Embed Size (px)
Citation preview

Update on clinical studies in Belgium
Jacques De Grève MD, PhDMedical OncologyOncologisch Centrum

Observations
Some academic, many “commercial” Profile similar between large community
hospitals and academic hospitals, except for initiating translational studies
Phase I-III and post-marketing The latter are often (masked) drug-pushing studies
Some increasing cross-center cooperation Which is very good
Very little non-drug research activity Surgical or radiotherapy

Caution
Confidential Biased overview
Information requested from 25 sources Information obtained from 12 investigators/centers

Overview
Prevention Surgical Neoadjuvant Adjuvant
Hormonal HER2 positive Chemotherapy Molecular
Metastatic Hormonal HER2 positive Chemotherapy Molecular

Prevention
IBIS studies: Role of AI in BC prevention in high risk profiles Some scientific value, but impact on clinical
practice improbable because of anticipated
Financial+toxicity cost Efficacy
= ASTRONOMICAL

Familial breast cancer
Search for novel breast cancer predisposing genes
Better method for counseling
BARD1
>1
J. De Grève et al, Current Opinion in Oncology, 11, 2008
UZBrussel

Copyright ©2004 BMJ Publishing Group Ltd.
Sermijn, E et al. J Med Genet 2004;41:e23
Awareness of the existence of a BRCA mutation in the subject's own family
Families ill-informed

Half of all pre-symptomatic mutation carriers do not engage in cancer prevention
Screening 50% BSO (all) 57.2% PM (No BC) 18% Chemoprevention (No mastectomy) 8.4% No action (No BC) 50%
Half of mutation carriers do nothing

Prospective study
Organized an active information of relevant family members on existence of mutation and subsequent prevention
Efficacy and psychological impact
E.Sermijn/M. Goossens, UZBrussel

SURGERY

SurgeryPedicled Perforator Flaps
Since 1989, major advance for reconstructive surgery
Only skin and subcutaneous tissue is utilized for reconstruction of defects with preservation of fascia, muscles and nerves according to basic plastic surgical principle of ” replacing like with like “
Muscle left in its native place to serve its original function and minimize donor site morbidity


Thoracodorsal artery perforator (TDAP) flap
Second generation perforator flaps Hamdi M, et al.
Pedicled perforator flaps in breast reconstruction: a new concept. Br. J. Plast. Surg. 2004 Sep; 57(6): 644-52
Other Thoracodorsal artery perforator (TDAP) flap Intercostal artery perforator (ICAP) flap Serratus anterior artery perforator (SAAP) flap Superior epigastric artery perforator (SEAP) flap
BJMO review (coming)
UGent

Indications
Immediate or delayed partial breast reconstruction following tumorectomy/ quadrantectomy
Post-mastectomy breast reconstruction in combination with an implant
Reconstruction of shoulder and thoracic defects after oncological resections
Should replace the classical latissimus dorsi flap in many indications in breast surgery





Satisfied women


Adjuvant radiotherapy
EORTC SUPREMO 22051-10052
Phase III randomized trial Role of adjuvant chest wall irradiation in
“intermediate risk” breast cancer following mastectomy
http://www.eortc.be
D. Vanden Wyngaert, ZNA

Neoadjuvant

Aout 2008
FRAGRANCE TRIALFRAGRANCE TRIAL
Postmenopausal patients (no age limits)Postmenopausal patients (no age limits)Non-candidates for CTNon-candidates for CTTT 2 cm 2 cmStages I, II & IIIStages I, II & IIIER and/or PgR+ER and/or PgR+
Letrozole 4 to 6 monthsLetrozole 4 to 6 months
SSUURRGGEERRYY
Frozen Frozen Biopsy 1Biopsy 1
D15D15D0D0
Frozen Frozen Biopsy 2Biopsy 2(optional)(optional)
Frozen Biopsy 3Frozen Biopsy 3
• F. Cardoso• Lab: M. Gloeckel, C. Desmedt,
V. Durbecq, C. SotiriouBiomarkers for response to AI

RANDOMIZE
NEO-ALTTO
Stratification:—T< 5 cm versus T> 5 cm—ER or PgR + versus both ER and PgR –—N0-1 versus N ≥2—Conservative surgery or not
lapatinib
trastuzumab
lapatinib
trastuzumab
paclitaxel
paclitaxel
paclitaxel
Surgery
FEC3
lapatinib
trastuzumab
lapatinib
trastuzumab
18 weeks 9 weeks 34 weeks
52 weeks of anti-ErbB2 therapy
Invasive breast cancerHER2+ T>2 cm (inflammatory BC excluded)
LVEF 50%
N=450
Biomarkers for response

Adjuvant

Adjuvant studies SOLE
IBCSG 35-07 / BIG 1-07 Postmenopausal women with HR positive, N+ early
stage breast cancer
Phase III trial of continuous letrozole versus intermittent letrozole following 4 to 6 years of prior adjuvant endocrine therapy
N=4600
Guy Jerusalem, Liège

Rationale
ER+ cancers relapse continuously Extended adjuvant results Adjuvant tamoxifen: 10 years is better than 5
years AI reimbursed for 5 years or extended
adjuvant


N+

Hormonal adjuvant EORTC 10031(SOFT)
• Premenopausal 35y
• Tamoxifen vs
• OFS + tamoxifen vs
• OFS + exemestane

Adjuvant studies ALTTO
Lapatinib dual EGFR/HER2 neu inhibitor EGFR effect irrelevant in BC Good drug after H failure, especially with BM’s
A randomised phase III comparison Adjuvant lapatinib, trastuzumab, their sequence and their
combination in patients with HER2/ErbB2 positive primary breast cancer
Open Q how efficacies versus toxicities will differ
BIG 2-06/N063D/DGF106708

•Patients with ER or PgR-positive tumours receive Patients with ER or PgR-positive tumours receive endocrine therapyendocrine therapy selected accordingly to menopausal status; endocrine therapy will be started selected accordingly to menopausal status; endocrine therapy will be started after the end of chemotherapy, will be administered concurrently with targeted therapies and will be planned for at least 5 yearsafter the end of chemotherapy, will be administered concurrently with targeted therapies and will be planned for at least 5 years• RadiotherapyRadiotherapy if indicated if indicated
DESIGN 1: Completion of ALL (neo)adjuvant chemotherapy prior to targeted therapyDESIGN 1: Completion of ALL (neo)adjuvant chemotherapy prior to targeted therapy
TrastuzumabTrastuzumab3-weekly3-weekly
(For 52 weeks)(For 52 weeks)
LapatinibLapatinib
(For 52 weeks)(For 52 weeks)
Trastuzumab Trastuzumab Weekly Weekly
(For 12 weeks)(For 12 weeks)
Lapatinib Lapatinib 3-weekly3-weekly
++Trastuzumab Trastuzumab (For 52 weeks)(For 52 weeks)
Centrally-determined HER2 +Centrally-determined HER2 +
Surgery, complete (neo)adjuvant anthracycline-based chemotherapy Surgery, complete (neo)adjuvant anthracycline-based chemotherapy (selected from an approved list)(selected from an approved list)
LVEF LVEF 50%50%
Locally-determined HER2-positive invasive breast cancerLocally-determined HER2-positive invasive breast cancer
Washout (6 weeks)Washout (6 weeks)
Lapatinib Lapatinib (34 weeks)(34 weeks)
ALTTO (Adjuvant Lapatinib and/or Trastuzumab Treatment Optimization) study

Locally-determined HER2-positive invasive breast cancerLocally-determined HER2-positive invasive breast cancer
Centrally-determined HER2 +Centrally-determined HER2 +
Surgery, complete (neo)adjuvant Surgery, complete (neo)adjuvant chemotherapychemotherapy (selected from an approved list)(selected from an approved list)
LVEF LVEF 50% 50%
5252
WWEEEEKSKS
Lapatinib Lapatinib + +
TrastuzumabTrastuzumab3-weekly3-weekly
40 weeks40 weeks
Lapatinib Lapatinib ++
TrastuzumabTrastuzumabWeekly Weekly
12 weeks12 weeks
TrastuzumabTrastuzumabWeeklyWeekly
12 weeks12 weeks
LapatinibLapatinib
52 weeks52 weeks
3-weekly 3-weekly TrastuzumabTrastuzumab
40 weeks40 weeks
LapatinibLapatinib
34 weeks34 weeks
PaclitaxelPaclitaxelWeeklyWeekly
12 weeks12 weeks
+/-+/-Radio-Radio-therapytherapy
PaclitaxelPaclitaxelWeeklyWeekly
12 weeks12 weeks
+/-+/-Radio-Radio-therapytherapy
PaclitaxelPaclitaxelWeeklyWeekly
12 weeks12 weeks
+/-+/-Radio-Radio-therapytherapy
Washout 6 Washout 6 weeksweeks
DESIGN 2: DESIGN 2: Paclitaxel concurrent with targeted therapy after any A-based (neo)adjuvant CTPaclitaxel concurrent with targeted therapy after any A-based (neo)adjuvant CT
PaclitaxelPaclitaxelWeekly Weekly
12 weeks12 weeks
+/-+/-Radio-Radio-therapytherapy
TrastuzumabTrastuzumabWeeklyWeekly
12 weeks12 weeks
ALTTO (Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation) study

Adjuvant studies MINDACT
EORTC 10041 BIG3-04 Fatima Cardoso/ Martine Piccart
Can microarray expression profiling help avoid chemotherapy in N- disease?
Phase III
Compares the 70-gene expression signature with common clinical-pathological criteria in selecting patients for adjuvant chemotherapy in node-negative breast cancer

Aout 2008
Evaluate Clinical-Pathological risk and 70-gene signature risk
Clinical-pathological and 70-gene both
HIGH risk
Discordant casesClin-Path HIGH70-gene LOW
Clin-Path LOW70-gene HIGH
Clinical-pathological and 70-gene both LOW
risk
Use Clin-Path risk to decide Chemo or not
Use 70-gene risk to decide Chemo or not
55% 32% 13%
R1
Chemotherapy
N=3300 N=780
Endocrine therapy
EORTC-BIG MINDACT TRIAL DESIGN6,000 Node negative women
N=1920
MD: M. Piccart; F. Cardoso;

HER2+ adjuvant BACH study
Caelyx-endoxan-herceptin
vs AC -> taxol-herceptin
+ cardiac substudy strain rate
UZLeuven

Beatrice
International multi-centre phase III trial of adjuvant Bevacizumab in triple negative breast cancer

Beatrice

Aout 2008
LOCAL RELAPSE [IBCSG 27-02, BIG 1-02]Chemotherapy for Radically Resected Loco-regional Relapse
RANDOMIZE
SURGERY
Strata:
-Prior CT
-ER+ and/or PgR+
-Location of recurrence
Observation (+/- Radiation Therapy)
Chemotherapy (+/- Radiation Therapy)
ER+ and/or PgR+: hormonal therapy
ER+ and/or PgR+: hormonal therapy
Recrutement total prévu: 977 patientes
(MD: F. Cardoso)
« PSEUDO-ADJUVANT »

Metastatic

Hormones

HR+ MBCIGF1-receptor targeting
IGF1R important co-regulator of other GF pathways and endocrine pathways, including causing resistance
CP-751,871 = IGF1R Moab Pfizer
Multiple myeloma: 9/ 27 RR in combination with dexamethasone 2 PR in dexa resistant patients

HR+ MBCIGF1-receptor targeting
RANDOMIZED PHASE 2 in 1st-line
COMBINATION WITH EXEMESTANE
vs EXEMESTANE ALONE AS FIRST LINE
Hans Wildiers

Copyright ©2007 AlphaMed Press
Stanway, S. J. et al. Oncologist 2007;12:370-374
Steroidogenesis in postmenopausal women and site of action of STX64 (BN83495)
• Steroid sulfatase (STS) activity much higher than aromatase activity in breast tumors
• High levels of STS mRNA associated with a poor prognosis
• STS hydrolyzes steroid sulfates, such as estrone sulfate and dehydroepiandrosterone sulfate (DHEAS), to estrone and DHEA, which can be converted to steroids with potent estrogenic properties, that is, estradiol and androstenediol, respectively.

Jan 2008
Steroid sulfatase inhibitor
• Post-menopausal with ER positive, LABC or MBC• 2nd line HT (adjuvant HT allowed but progressed > 12 ms)• Only 1 prior CT and Herceptin (discontinued at least for 4 months prior) • Measurable (RECIST) and non-measurable (only until OBD)• Progressive CNS excluded
METASTATIC SETTING: HR + Hormonal TherapyIPSEN BN83495 TRIAL (Phase 1)
Bordet

HOBO-trial
Phase II study in patients with hormone receptor positive breast cancer with Bortezomib (Velcade) in the reversal of endocrine resistance
L. Dirix, Sint AugustinusAlso many interesting translational studies in inflammatory breast cancer

HER2 positive disease

Metastatic disease (MBC) HER2-positive EGF 104383
Phase III study
Paclitaxel plus Trastuzumab plus Lapatinib
vs Paclitaxel plus Trastuzumab plus placebo

Aout 2008
Pfizer A 6181067: Herceptin + Sutent
•Phase II
•CT not indicated but Herceptin indicated
•Prior treatment with trastuzumab and/or lapatinib in the neoadjuvant, adjuvant or metastatic setting is permitted
Pfizer A 6181113: Docetaxel + Herceptin + SU011248 (Sutent)
•Phase II
• F. Cardoso
METASTATIC SETTINGHER-2 BC 1st Line

Aout 2008
METASTATIC SETTING HER-2 BC
2nd or more Line Local relapse and/or inflammatory MBC
Lapatinib +/- PazopanibPhase III randomised double blindMust have received CT and TrastuzumabMain endpoint: PFS
Controlled CNS mets allowed
GSK: VEG108838

HSP90

Metastatic studies HER2-positive MedImmune Protocol No. MI-CP153
Phase 2
Antitumor Activity and Safety of IPI-504, Small Molecule Inhibitor of Heat Shock Protein 90
(Hsp90)
Progressed on HER2-targeted Therapy
Marleen Borms, AZ GroeningeUZLeuven

Aout 2008
METASTATIC SETTING HER-2 BC
Herceptin + Velcade
• Bordet-sponsored trial and based on their prior preclinical experiments1
• Phase I
• No limit of previous lines of HT nor CT
• Previous Herceptin or lapatinib allowed
• All MBC HER-2 for whom Herceptin alone would be the choice
F. Cardoso
1Cardoso F, et alBortezomib increases the efficacy of trastuzumab (Herceptin) in HER-2-positive breast cancer cells in a synergistic mannerMol Cancer Ther. 2006 Dec;5(12):3042-51

Ertumaxomab
•Bispecific antibody targeting HER2/neu and CD3
•Formation of a tri-cell complex
•tumour cell, T cell and accessory cell
•Antitumour efficacy against HER2/neu low-expressing tumours resistant to trastuzumab
• Phase I study in MBC : strong immune responses
• Phase II studies MBC even without HER2/neu gene amplification

Aout 2008
METASTATIC SETTINGBiological Therapy Alone
HR + & HER-2 1 or 2/FISH BC
Ertumaxomab (trifunctional HER MoAb) (Fresenius)
Phase I I
HR + but HT Resistant
HER-2 + ou ++ but FISH neg
F. Cardoso

Aout 2008
METASTATIC SETTING
1. Lapatinib + Temozolomide (LAPTEM) 2. Lapatinib + Capecitabine
BRAIN METASTASES
HER-2+
Bordet

Metastatic HER2 + BC 3144A1-203-WW
HKI-272: irreversible inhibitor of EGFR/HER2neu
Phase I/II study and after Herceptin failure
HKI-272 with paclitaxel in subjects with solid tumours and breast cancer
HKI-272 (Neratinib) + Vinorelbine
AZ Groeninge en Bordet

Metastatic Triple Negative BC BIBW 2992 (Boehringer)
• Dual irreversible EGFR/HER2neu inhibitor
• Phase II
• HER-2 Neg, HR negative (Triple Negative)
• Asymptomatic brain mets allowed

Eribulin
Synthetic analogue of halichondrin B Substance derived from a marine sponge
(Lissodendoryx sp.) Binds to vinca domain of tubulin and
inhibits the polymerization of tubulin Inhibition of mitotic spindle assembly,
induction of cell cycle arrest at G2/M phase

MBC, 2nd line E7389 (Eribulin)
Phase 3, Multiple centers
1. Eribulin versus ‘treatment of physician’s choice’ in
patients with locally recurrent or metastatic breast cancer, previously treated with at least two and maximum five prior chemotherapy regimens, including an anthracycline and a taxane
2. Eribulin versus Capecitabine in patients with locally advanced or metastatic breast cancer previously treated with anthracyclines and taxanes and refractory to the most recent chemotherapy

Jan 2008
METASTATIC SETTING Triple Negative
1st LineMERCK 20027-051 BALI-1
Phase-II randomized• WEEKLY CETUXIMAB + six 3-WEEKLY cycles of CISPLATIN
• Maximum of six 3-WEEKLY CYCLES OF CISPLATIN
Main endpoint: RR
Only 1 prior anthracycline or taxane (adjuvant or MBC)
• MD: A. Awada

IMC-1121B
A multicenter phase III-study in first-line
Anti-vascular endothelial growth factor receptor-2 (VEGFR-2) monoclonal antibody
IMC-1121B plus Docetaxel
vs placebo plus Docetaxel
V. Cocquyt

SUCON trial
SUtent CONsolidation
A belgian multicenter phase II randomized trial in her2 negative metastatic breast cancer evaluating consolidation antiangiogenic therapy with SU11248 after response to taxane chemotherapy induction.
H. Wildiers

SUCON trial

Biomarking in Top trial
Anthracycline in triple negative:
Looking for biomarkers for sensitivity/resistance Expression profiling Genetic predisposition genes Epigenetic profiling
Bordet-ULB-UCL-VUB

PARP1 inhibitor
High activity in genetic ovarian cancer*
Under study:
SA activity under study in genetic breast cancer
Activity with cisplatinum in breast cancer
* AZD2281 (KU-0059436), a PARP (poly ADP-ribose polymerase) inhibitor with single agent anticancer activity in patients with BRCA deficient ovarian cancer: Results from a phase I study. P. C. Fong, D. S. Boss, C. P. Carden, M. Roelvink, J. De Greve, et al J Clin Oncol 26: 2008 (May 20 suppl; abstr 5510)

L. D. Wood et al., Science 318, 1108 -1113 (2007)
Future is: genomics

Thank you for the information
Bordet: F. Cardoso AZ Groeninge: M. Borms Hasselt: J. Janssens UGent: H. Thierens, V.Cocquyt, M. Hamdi UZBrussel: C. Fontaine UZLeuven : H. Wildiers en P. Neven UZAntwerpen: W. Tjalma (overview) Klina: D. Verhoeven, OLV-Aalst Sint-Nicolaas ZNA (Vandenwyngaert)


P
rop
idiu
m io
did
e
Annexin V Annexin V Annexin V
Control Fulvestrant Estradiol
B
Estrogen Induces Apoptosis and Tumor Regression in a BreastCancer Cell Line Resistant To Estrogen Deprivation
0
2
4
6
8
10
12
14
16
2 4 6 8 10
AUTONOMOUSGROWTH
ESTRADIOL
FULVESTRANT
A
DN
A (
g/w
ell)
Days
G1-blockade Apoptosis
0.0
0.2
0.4
0.6
0 2 4 6 8
Aver
age
tum
our a
rea
(cm
2 )
Weeks
AUTONOMOUSGROWTH
FULVESTRANT
ESTRADIOL
CIn vivo
In vitro
Lewis et al, J Natl Cancer Inst. 2005; 97:1746-59

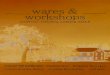
Effect of intermittent letrozole treatment in MCF-7Ca xenografts
1
1
1
1
1
1
5.4
3.1
4.1
1
0.2
0.2
6.7
3.7
5.9
1
0
0.1
1.99
2.1
0.9
0.9
0.9
0.9
0.3
1.3
0.8
0.9
2.7
2.4
1.1
1.7
1.1
1
0.8
1.1
Her-2
p-Her-2
p-MAPK
MAPK
Aromatase
ERα
ß-Actin
Off Letrozole
Letrozole
0
250
500
750
1000
1250
1500
1750
2000
2250
2500
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Mea
n Tu
mor
Vol
ume
(mm
3 )
Control
Back onLetrozole
Weeks
Control
Letrozole-22 wk
Letrozole-33 wk
Off – 28 wk
Off – 33 wkBack On Letro
zole
28 weeks
Sabnis et al. Cancer Res. 2008;68,4518.

Patient Population• Postmenopausal• Disease-free after 4 to 6 years of prior
adjuvant endocrine therapy (SERM and/or AI)
• Endocrine-responsive breast cancer at diagnosis
• Node-positive breast cancer at diagnosis
S LE

• 10 of a total of 25 accepted sites in Belgium are actively recruting. Last month Belgium as a country take the lead compared to all other countries concerning the recrutment.
• The trial allows free drug access for all postmenopausal lymph node positive patients who are candidates for extended adjuvant treatment and who received an aromatase inhibitor within the first 5 years (and who consequently can not obtained a reimbursement for extended adjuvant treatment).
• Contact: [email protected]

Patient Visit Schedule• All patients will be followed every 6 months
for years 1 to 5, and thereafter yearly for assessment of disease status and for survival data collection.
S LE

Aout 2008
« EN PRATIQUE »: ADJUVANT
Phase III trial (4800 pts): 5 years continuous letrozole vs of intermittent letrozole following 4 to 6 years of prior adjuvant HT (tam and/or AI)
Postmenopausal women with HR positive; Node positive only
Main endpoint: DFS; tumor block required; QoL substudy

Participating centers2-2006: 15 centres• UZ Gasthuisberg Leuven (R Paridaens and H Wildiers and P Neven)• AZ St-Augustinus Wilrijk (L Dirix)• Imelda Bonheiden (W. Wynendaele)• AZ St jan Brugge (E. Decuypere)• ZOL (J Mebis, D Luyten, G Debrock)• St-Elisabeth Turnhout (M Martens)• St-Elisabeth Namen (P Vuylsteke and Jean-Charles Goemine)• UZ Gent (H Denys and Dr V Cocquyt)• UCL Brussels and Mont-Godinne (JP Machiels and J Kerger)• Charleroi (JL Canon)• UZBrussel (J De Greve)• Liege (G Jerusalem)
8-2007: 5 new centres• Cliniques du Sud-Luxembourg, Arlon (P Glorieux)• CHR de Huy (J Collignon, J Bury, M Reginster)• CHC Clinique Saint Joseph (C Focan, M P Graas, F Kreutz)• UCL Ottignies Louvain-la-Neuve (L Duck)• AZ Nikolaas (W Lybaert, I Deleu, E Everaert)

Aout 2008
METASTATIC SETTING HER-2 Neg BC
1st Line MBCWX‑671 + Capecitabine vs. Placebo + Capecitabine (Wilex)
Phase II randomisedMain endpoint: PFSMeasurable disease (RECIST)Bone or skin only not allowed
SNS mets not allowed
• F. Cardoso
Serine protease inhibitor inhibits the uPA system