Embed Size (px)
Citation preview
Neo-Adjuvant Systemic Treatment:
Current Modalities
Luc Y. Dirix
Medical Oncology
Oncologisch Centrum GvA, Antwerp.
October 14, 2006
Neo-Adjuvant or Pre-operative Systemic Chemotherapy in Patients with Primary
Operable Breast Cancer (POBC)• To improve surgical options
– Reduce size• Increase BCS• Decrease local recurrences
• To obtain improved long-term survival – Systemic therapy prior to S
• S releases and/or stimulates TC • CT more early
• To obtain information on response– In-vivo drug sensitivity test
• To answer biological questions
Pre-operative Systemic Therapy (PST) in Patients with Primary Operable
Breast Cancer (POBC)
A) Endpoints
B) Types of PST
C) Surgical Considerations
Pre-operative Systemic Therapy (PST) in Patients with Primary Operable
Breast Cancer (POBC) Endpoints
• Pathological assessment • MRI - PET • CTC - CEC• DTC
Neo-Adjuvant Chemotherapy
and pCR • NSABP definition pCR
– No residual invasive tumor in the breast – DCIS allowed – LNN
• Stringent definition of pCR – No invasive tumor in breast – No DCIS allowed – LNN are free
• Methodological issues

PST in POBC : Definitions of Pathological Response

PST in POBC : Role of MRI
• DCE-MRI accurately predicts response early on • Relation tumor diameter on pathology and DCE-
MRI 0.824 • DCE-MRI in is superior in predicting pCR
(PE, Mammography, US)• DCE-MRI over- and underestimates pCR • DCE-MRI effect of bevacizumab• Is MRI defined CR a prognostic factor ?• ACRIN,CALGB Intergroup 49808 : utility of MRI
(www.acrin.org, current protocol section)
PST in POBC : Role of F18FDG PET
• Early decrease in SUV in responders • Reliable in defining non-responders or PD• SUVp RR n = 50
• a RR -88% threshold pCR and pPR• Sensitivity 100%, Specificity 56.5%• AUC 0.788
• PET is able to differentiate pathological responders after 1-2 cycles CT with an accuracy of 91%, a sensitivity of 100%
• PET is a poor discriminator of pCR
PST in POBC : Role of DTC/CTC
• CTC and PST • Pachman et al., n=30 epi-based PST• 100% CEC 600-273,150 cells/ml• R2 = 0.97 change TV and log fold decrease CEC
• REMAGUS 02 RPII study (PASCO 2006)• CTC CellSearch, n=60 • 1CTC in 15/56, >2CTC 8/56
• CEC and EPC and PST • Füstenberger et al., n=10• Decrease in CEnC correlated with PST• Increase in VEGF,EPC
• No data on DTC in BM and PST
Pre-operative Systemic Therapy (PST) in Patients with Primary Operable
Breast Cancer (POBC) A) Types of PST
– Chemotherapy • Anthracycline-based • Taxane based • Anti-HER2 • Anti-VEGF
– Endocrine therapy – Predictors of efficacy
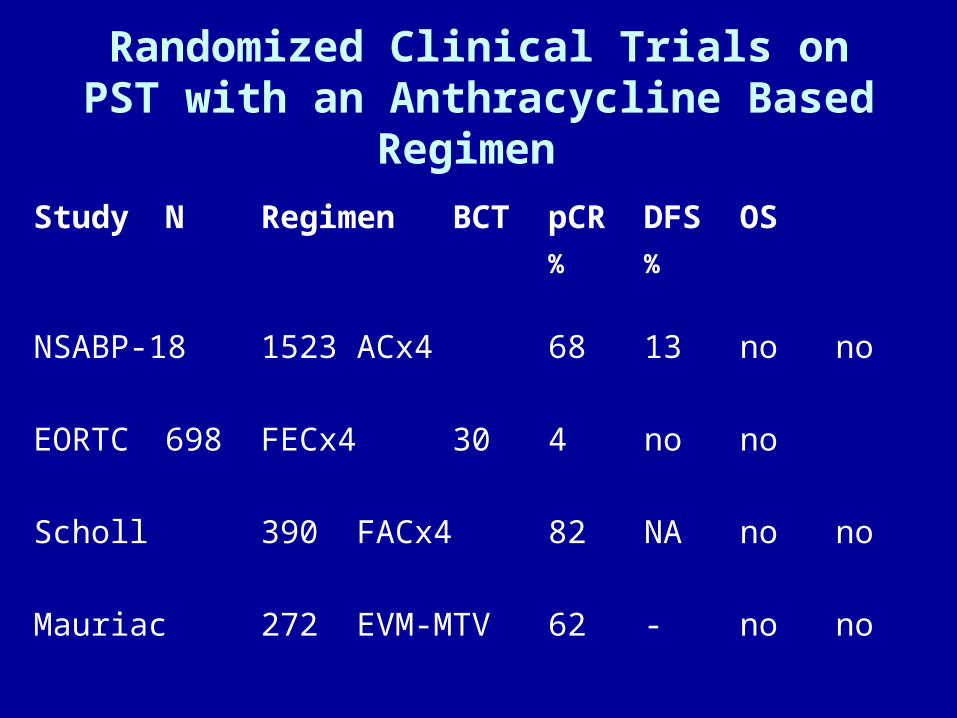
Randomized Clinical Trials on PST with an Anthracycline Based Regimen
Study N Regimen BCT pCR DFS OS
% %
NSABP-18 1523 ACx4 68 13 no no
EORTC 698 FECx4 30 4 no no
Scholl 390 FACx4 82 NA no no
Mauriac 272 EVM-MTV 62 - no no
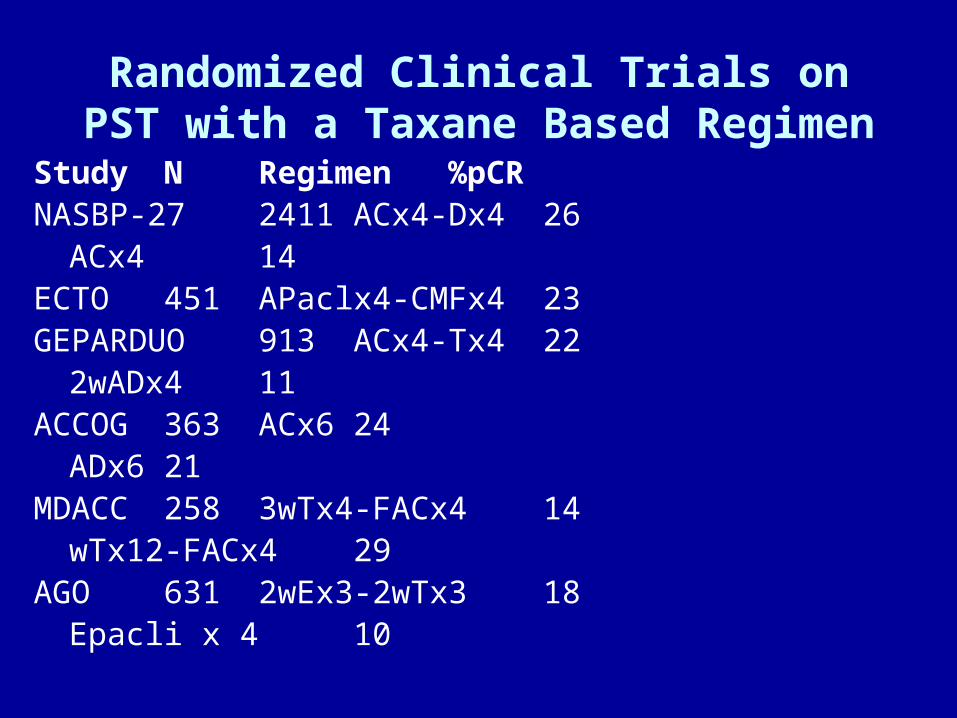
Randomized Clinical Trials on PST with a Taxane Based Regimen
Study N Regimen %pCR NASBP-27 2411 ACx4-Dx4 26
ACx4 14ECTO 451 APaclx4-CMFx4 23GEPARDUO 913 ACx4-Tx4 22
2wADx4 11ACCOG 363 ACx6 24
ADx6 21MDACC 258 3wTx4-FACx4 14
wTx12-FACx4 29AGO 631 2wEx3-2wTx3 18
Epacli x 4 10
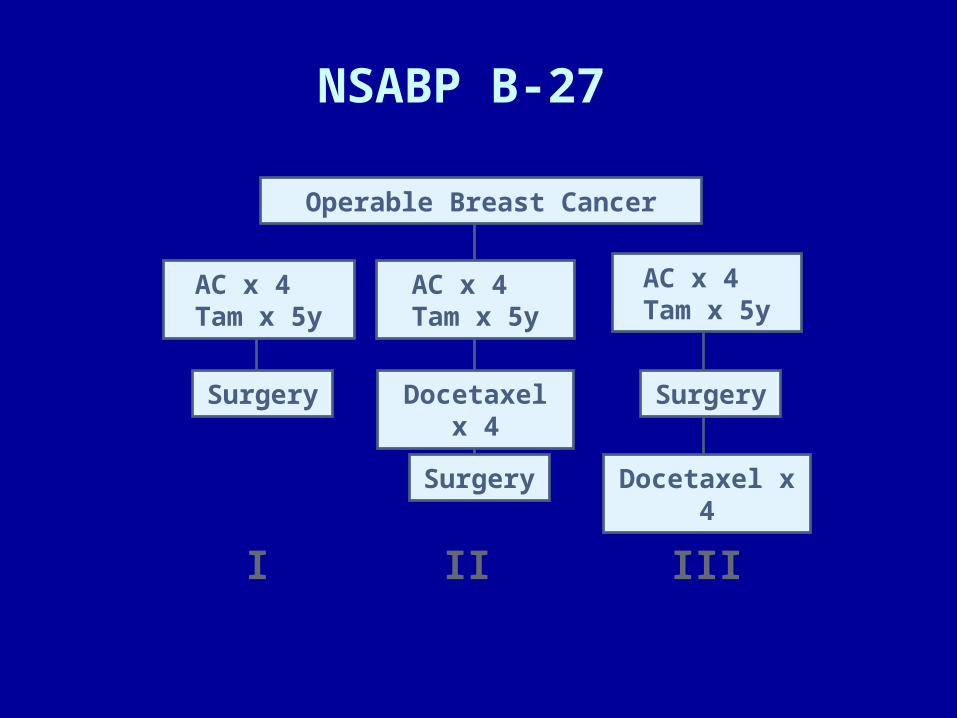
NSABP B-27
I II III
Operable Breast Cancer
AC x 4 Tam x 5y
Surgery Docetaxel x 4
Surgery
Surgery
Docetaxel x 4
AC x 4 Tam x 5y
AC x 4 Tam x 5y
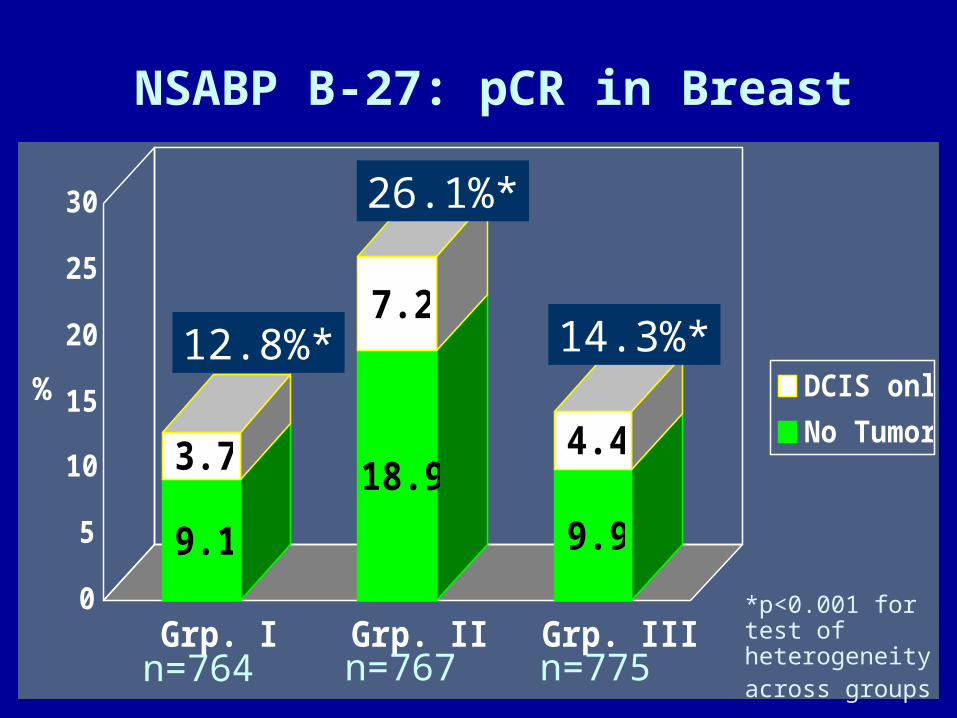
NSABP B-27: pCR in Breast
9.1
3.7 18.9
7.2
9.9
4.4
0
5
10
15
20
25
30
Grp. I Grp. II Grp. III
DCIS only
No Tumor%
*p<0.001 for test of heterogeneity across groups n=764 n=767
12.8%*
26.1%*
14.3%*
n=775
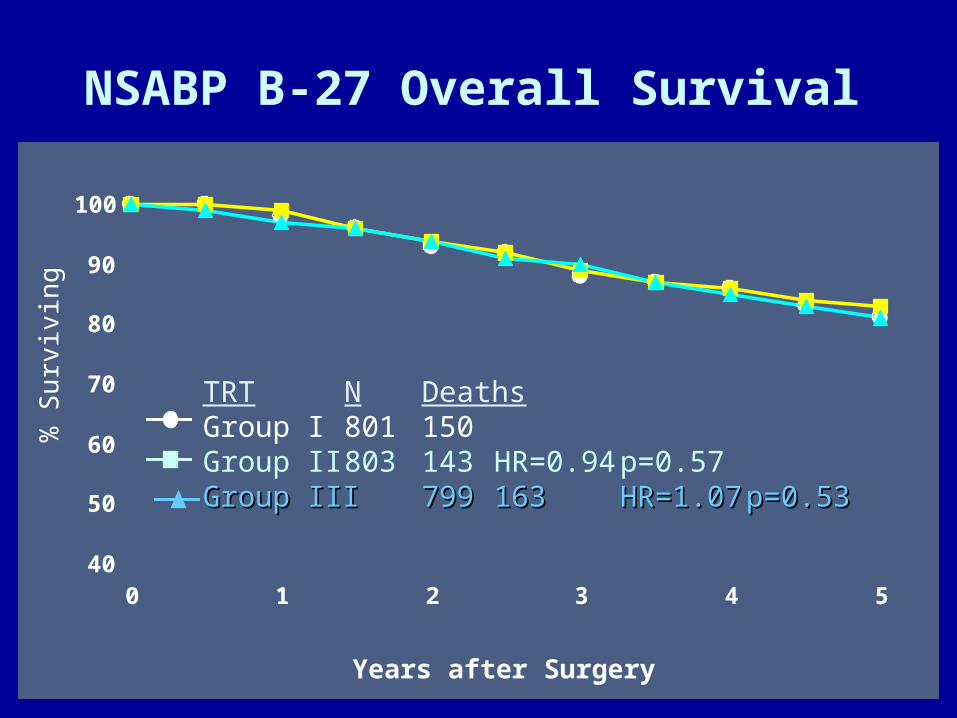
NSABP B-27 Overall Survival
40
50
60
70
80
90
100
0 1 2 3 4 5
% Surviving
Years after Surgery
TRT N DeathsGroup I 801 150Group II 803 143 HR=0.94 p=0.57Group IIIGroup III 799799 163163 HR=1.07HR=1.07 p=0.53p=0.53
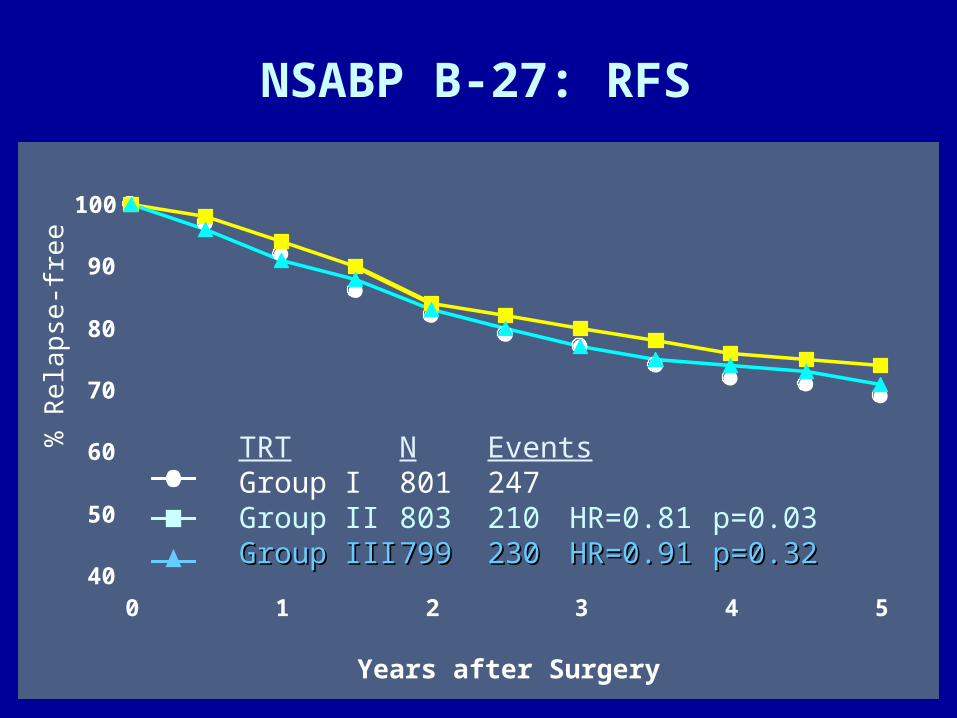
NSABP B-27: RFS
40
50
60
70
80
90
100
0 1 2 3 4 5
% Relapse-free
Years after Surgery
TRT N EventsGroup I 801 247Group II 803 210 HR=0.81 p=0.03Group IIIGroup III 799799 230230 HR=0.91HR=0.91 p=0.32p=0.32
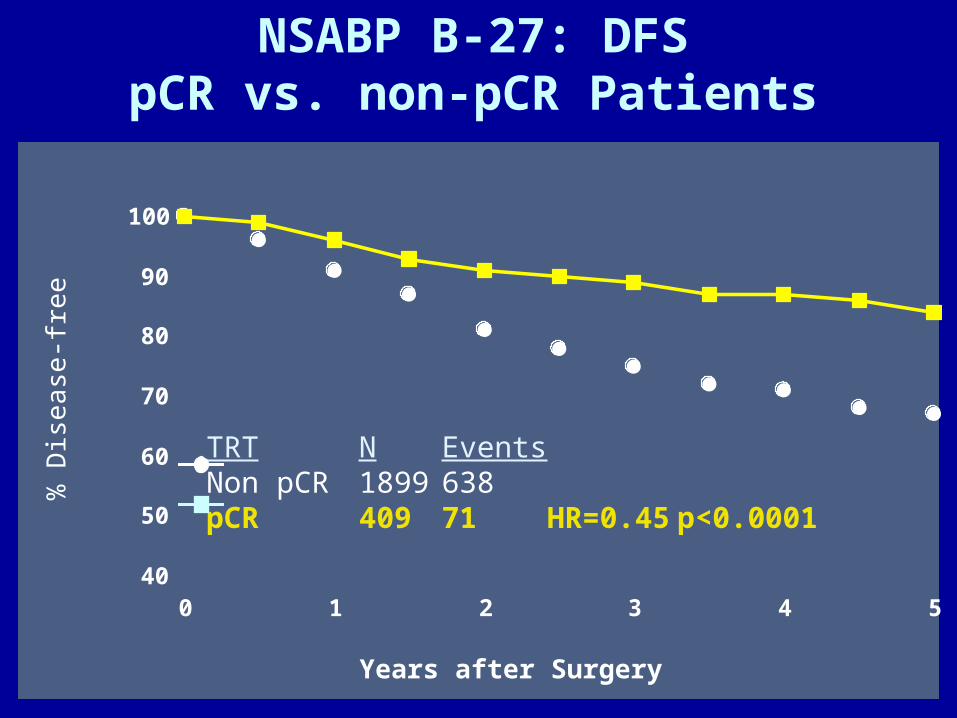
NSABP B-27: DFSpCR vs. non-pCR Patients
40
50
60
70
80
90
100
0 1 2 3 4 5
% Disease-free
Years after Surgery
TRT N EventsNon pCR 1899 638pCR 409 71 HR=0.45 p<0.0001
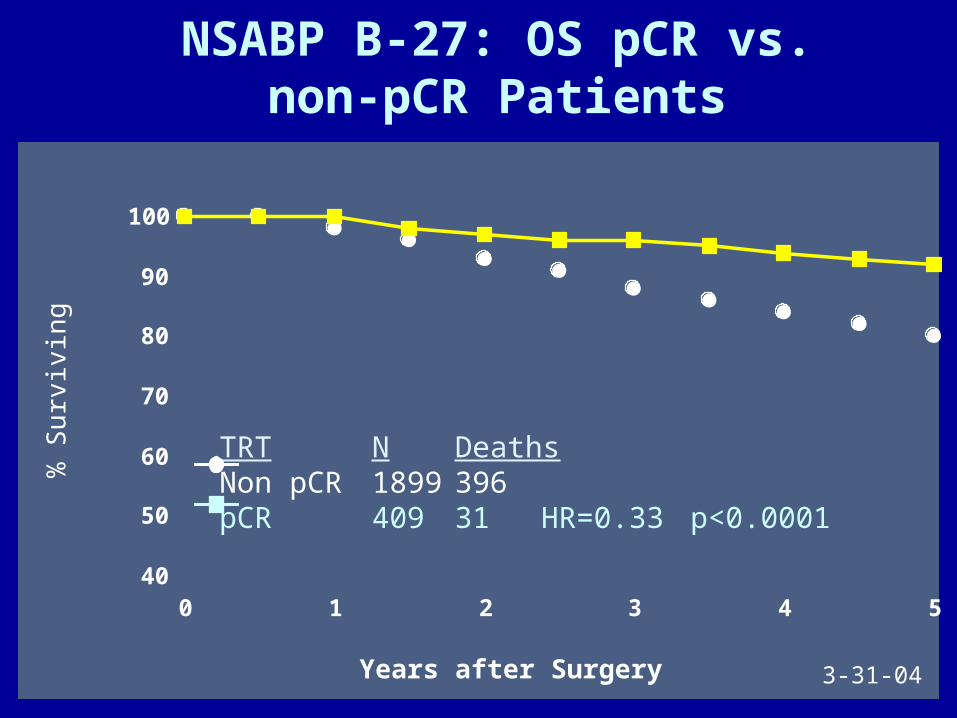
NSABP B-27: OS pCR vs. non-pCR Patients
40
50
60
70
80
90
100
0 1 2 3 4 5
% Surviving
Years after Surgery
TRT N DeathsNon pCR 1899 396pCR 409 31 HR=0.33p<0.0001
3-31-04
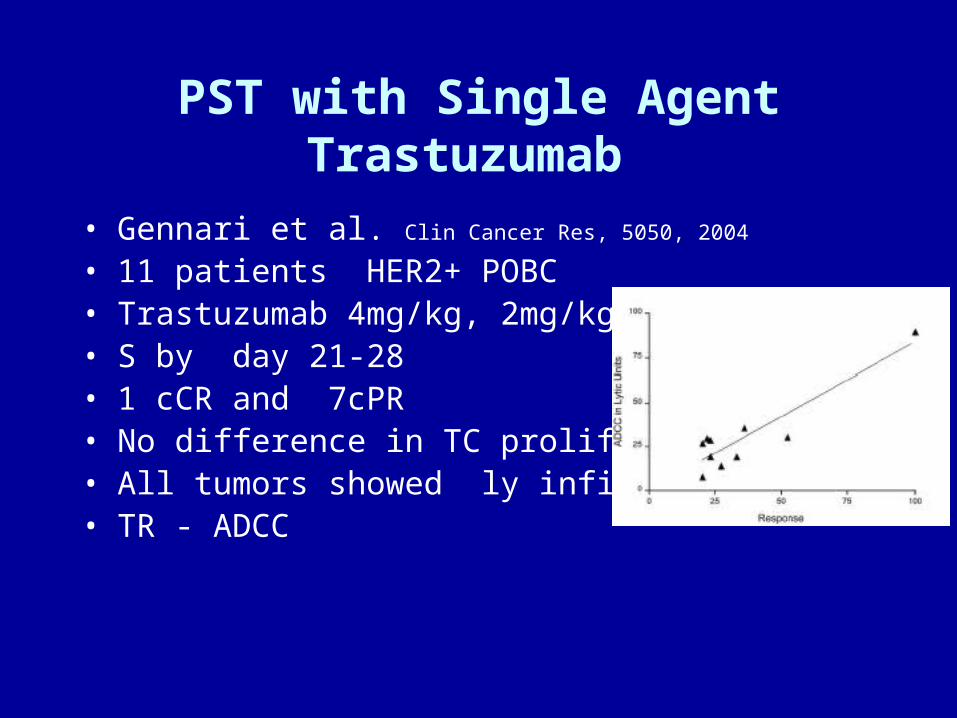
PST with Single Agent Trastuzumab
• Gennari et al. Clin Cancer Res, 5050, 2004
• 11 patients HER2+ POBC • Trastuzumab 4mg/kg, 2mg/kg/we• S by day 21-28 • 1 cCR and 7cPR• No difference in TC proliferation • All tumors showed ly infiltration • TR - ADCC
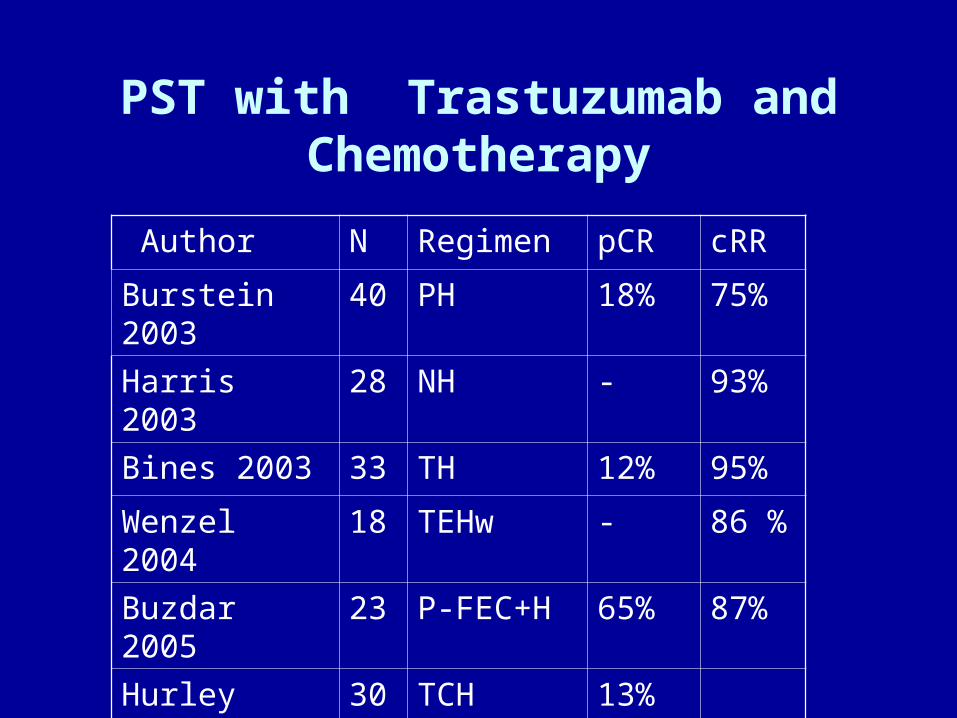
PST with Trastuzumab and Chemotherapy
Author N Regimen pCR cRR
Burstein 2003 40 PH 18% 75%
Harris 2003 28 NH - 93%
Bines 2003 33 TH 12% 95%
Wenzel 2004 18 TEHw - 86 %
Buzdar 2005 23 P-FEC+H 65% 87%
Hurley 2005 30 TCH 13%
Coudert 2006 33 TH 47% 96%
PST with Trastuzumab: RCT
• 42 pts HER-2 + BC (4T1,28T2,9T31T4)
• 4xPac 225mg/sqm/24h, 4xFEC(d1,4)+/-H
• pCR = in breast and LNN = no invasive T
• 2 pts FISH negative
• pCR 26.3% vs 65,2% (43%-84%)
• pCR irrespective of ER status
• 10% decrease in LVEF in five and seven
Wedam, S. B. et al. J Clin Oncol; 24:769-777 2006
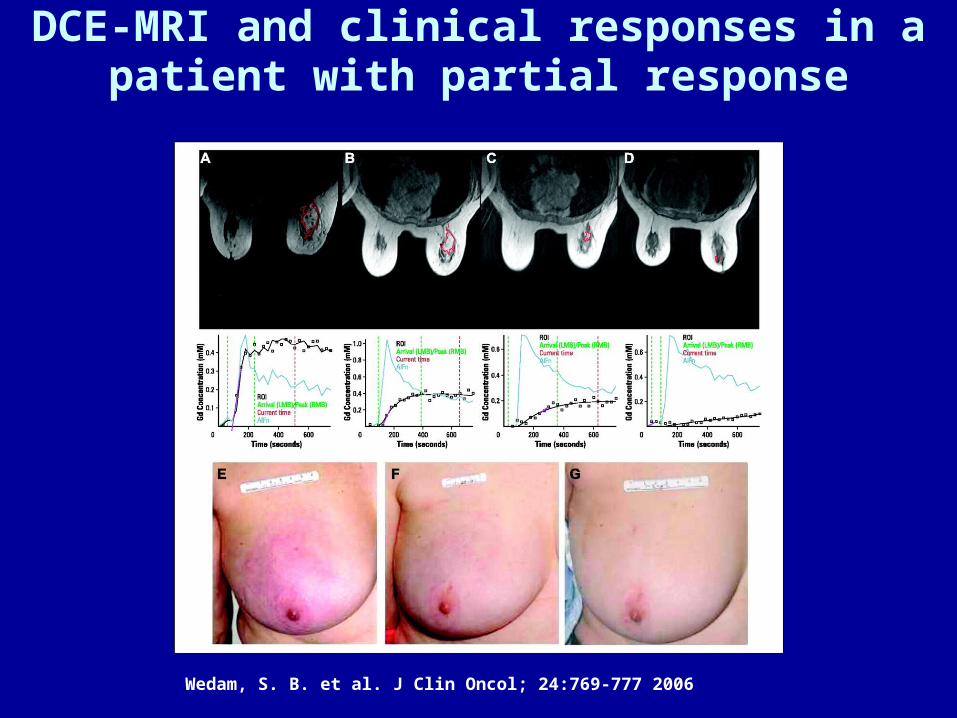
DCE-MRI and clinical responses in a patient with partial response
Wedam, S. B. et al. J Clin Oncol; 24:769-777 2006
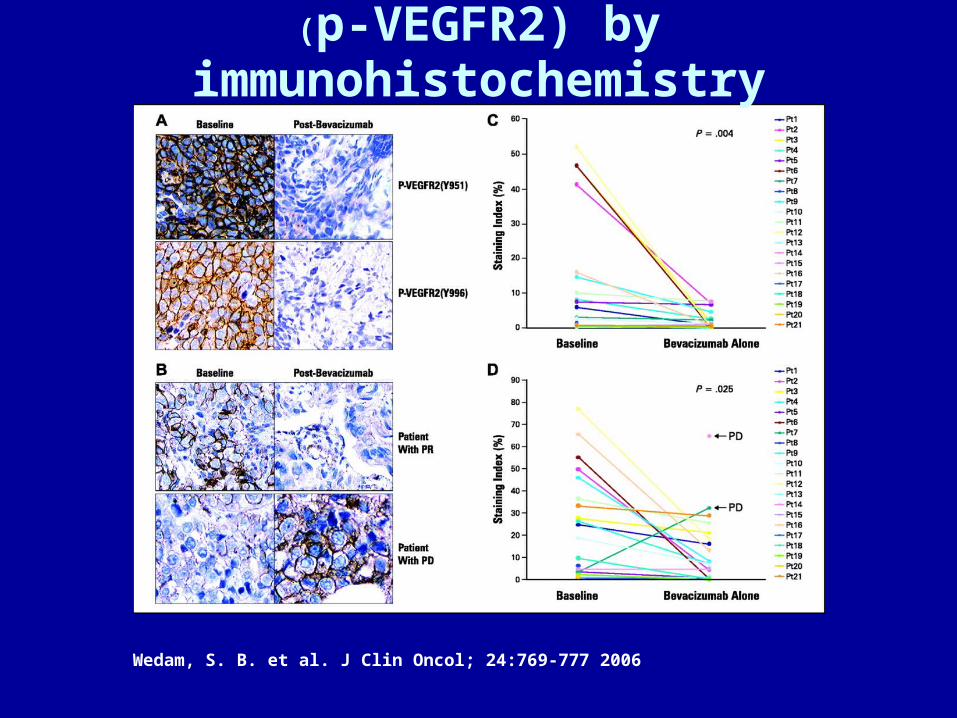
(p-VEGFR2) by immunohistochemistry
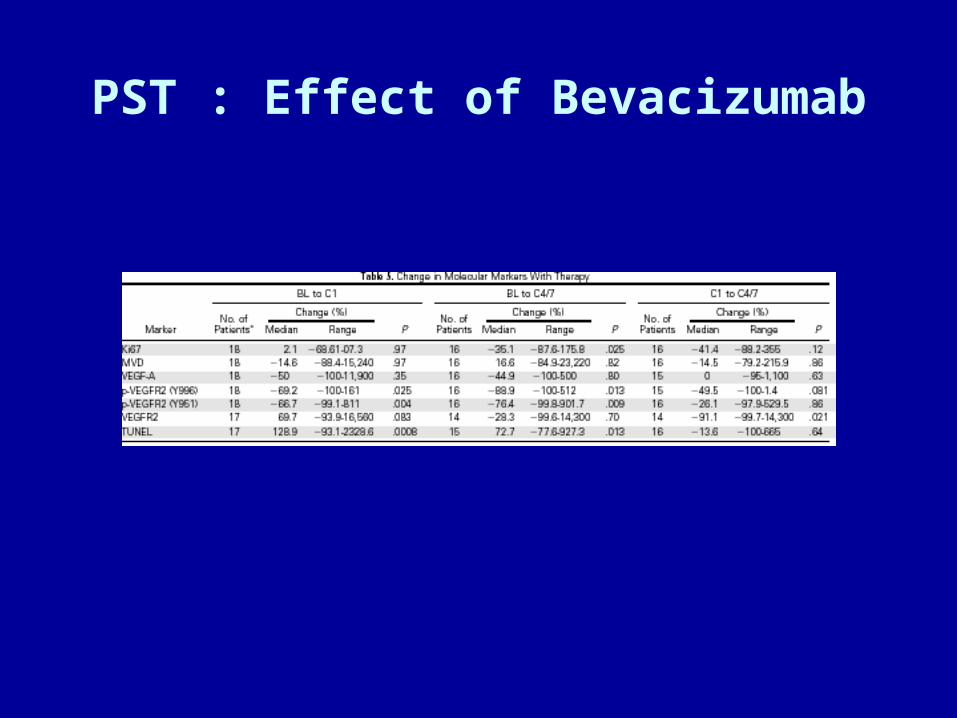
PST : Effect of Bevacizumab
Candidate Single Gene Predictive Markers : HR
QuickTime™ en eenTIFF (ongecomprimeerd)-decompressor
zijn vereist om deze afbeelding weer te geven.
Neo-Adjuvant Chemotherapy and pCR
QuickTime™ en eenTIFF (ongecomprimeerd)-decompressor
zijn vereist om deze afbeelding weer te geven.
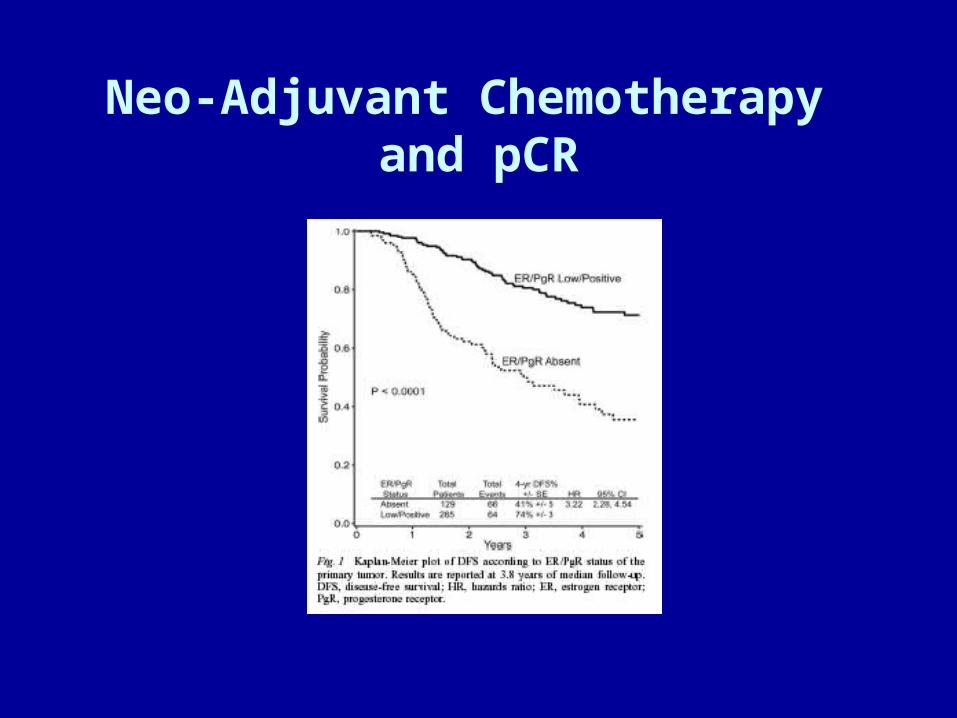
Neo-Adjuvant Chemotherapy and pCR
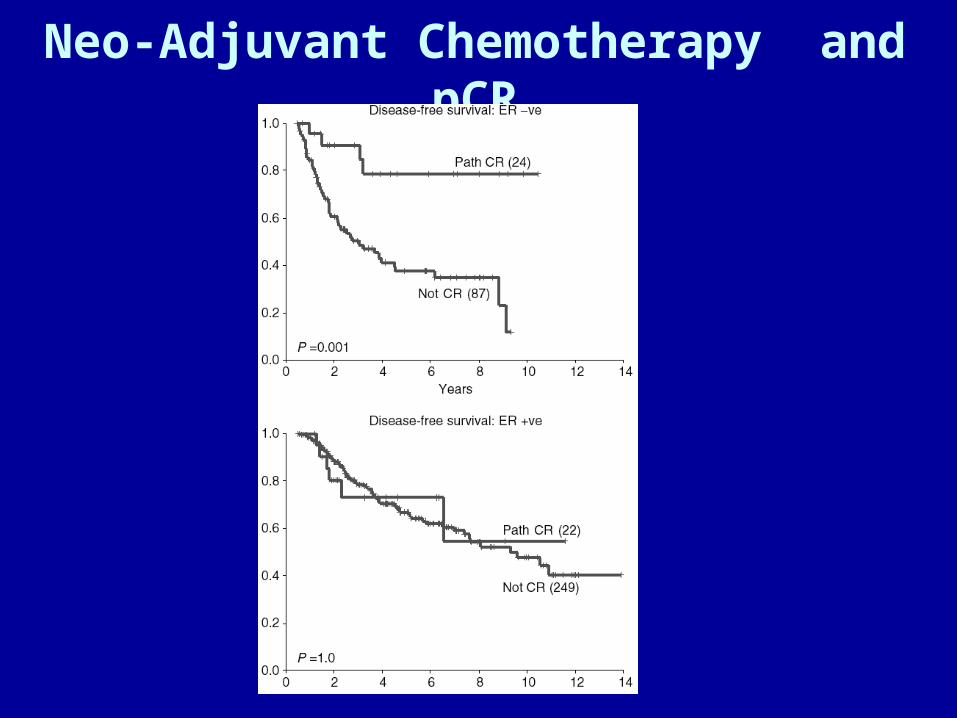
Neo-Adjuvant Chemotherapy and pCR

Hess, K. R. et al. J Clin Oncol; 24:4236-4244 2006
Learning curve for Diagonal Linear Discriminant Analysis-30 classifier
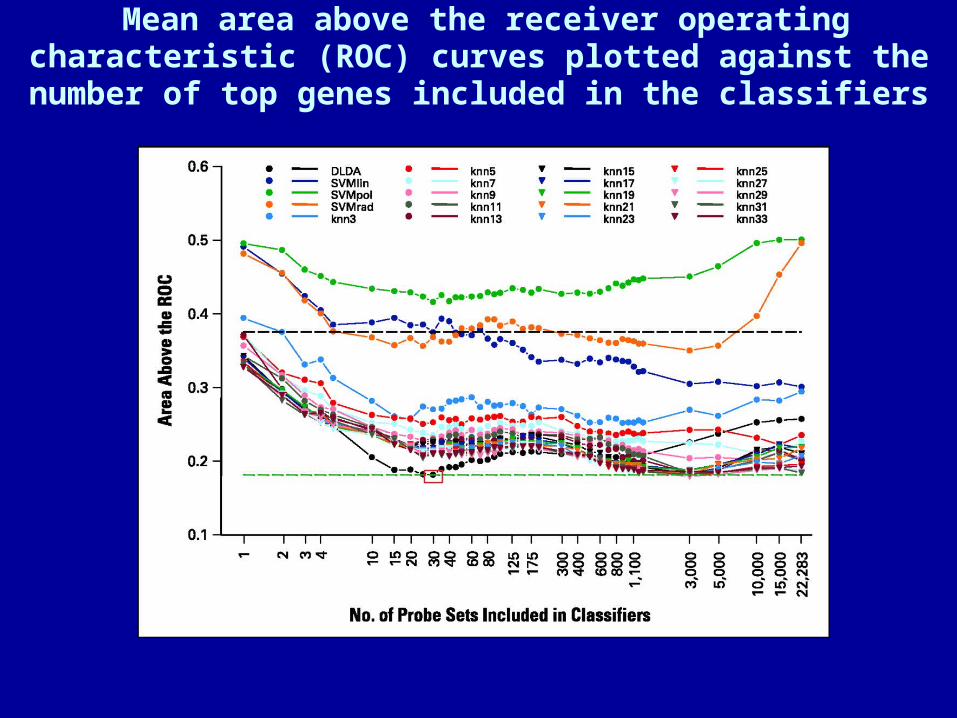
Mean area above the receiver operating characteristic (ROC) curves plotted against the number of top genes
included in the classifiers
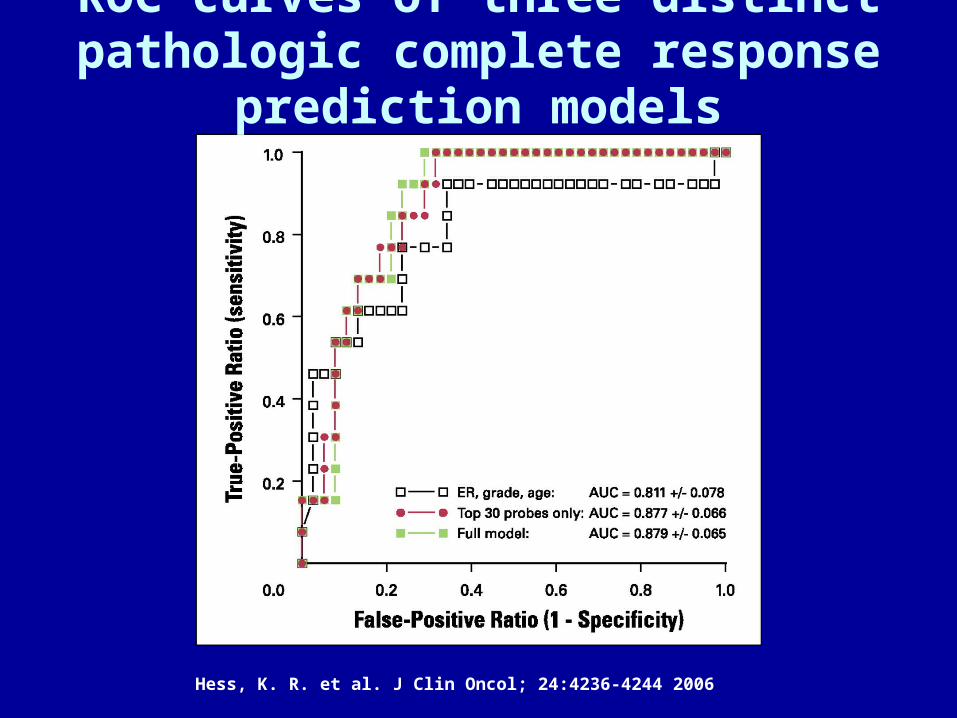
Hess, K. R. et al. J Clin Oncol; 24:4236-4244 2006
ROC curves of three distinct pathologic complete response prediction models
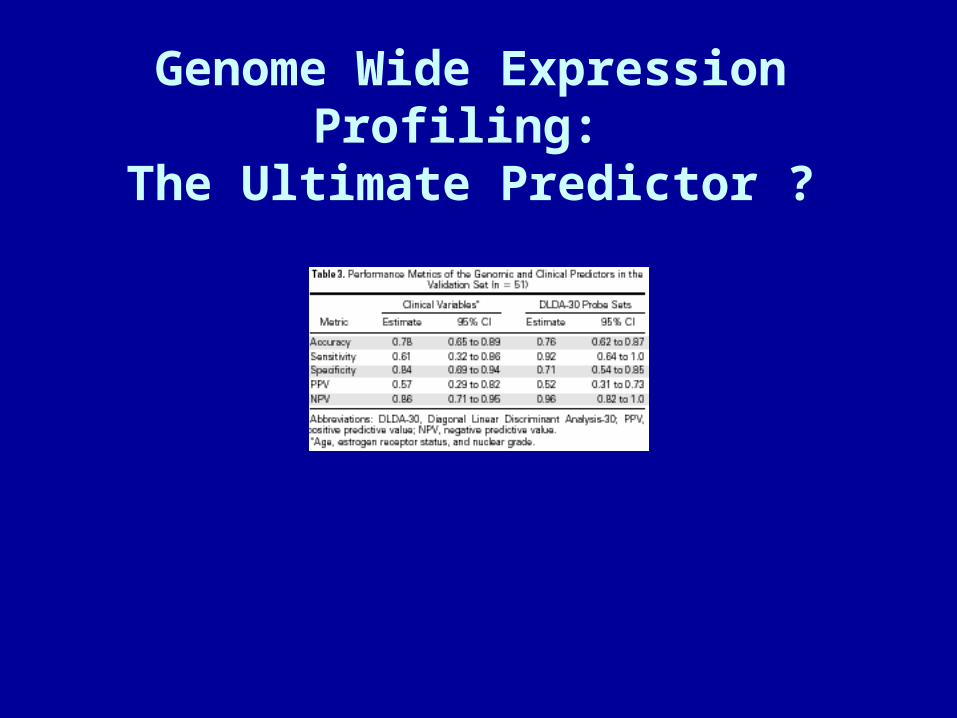
Genome Wide Expression Profiling: The Ultimate Predictor ?
PST with Chemotherapy & BCS
BCT after AT -CMF (ECTO)
BCS LNN-
• S-Ax4-CMFx4 38% 35%• ATx4-CMFx4-S 61% 71%
PST in Patients with POBC• Breast conserving treatment is feasible and safe.• Pre-treatment assessment (SLN) is advisable.• pCR is possible both in breast and LNN. • Surgery is not be omitted even in cCR. • A taxane-anthracycline combination seems optimal. • Sequential therapy seems preferable . • Addition of Herceptin increases pCR if HER-2 ampl.• Optimal duration of PST is unclear.• PET and DCE-MRI allow for recognition of non-
responders. • Is pCR a surrogate for “activity” on CTC-DTC? • pCR in nodes remains a prognostic factor• pCR predicts survival (most convincingly if ER-)



![[ e„wËÔi †M‡RU ] - WordPress.com€¦ · Scholarship of SSC-2015/308 cvZv-1 [ e„wËÔi †M‡RU ] gva¨wgK I D”P gva¨wgK wk¶v †evW, PÆMvg 2015 mv‡ji gva¨wgK ¯‹zj](https://img.pdfslide.us/doc/110x75/5f10b96f7e708231d44a82e9/-eawi-amaru-scholarship-of-ssc-2015308-cvzv-1-eawi-amaru.jpg)