Embed Size (px)
Citation preview

Update in CardiologyFocus on Prevention
Andrew Teklinski, MD, MS, FACC
Cardiology
Munson Medical Center

Financial Disclosures
• None

CVD: Where are we at?

Carotid atherosclerosis
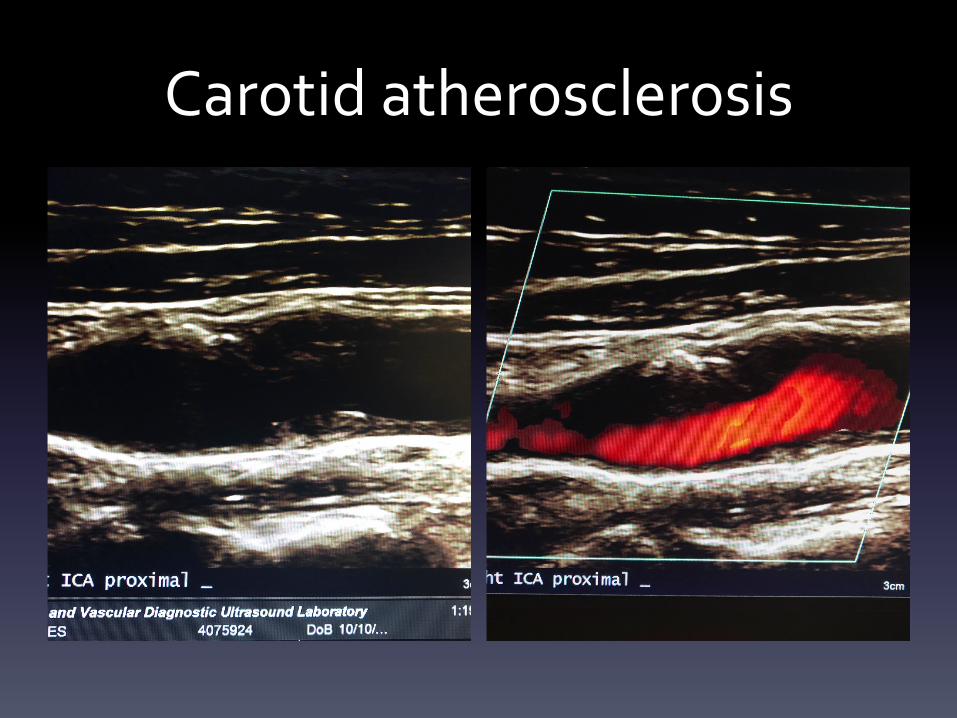
Carotid atherosclerosis

The Good News (Sort of)

The Good News

The Bad News
• CVD remains the leading cause of death in the US
– 840,768 deaths (635,260 cardiac) in 2016
– From 2006 to 2016, the US death rate from CVD decreased by 18.6% and
from CHD 31.8%
• Annual estimated cost of CVD in the US was $351.2 billion in 2014-2015,
with $213.8 billion in direct cost, including 46% for inpatient care
• About every 40 seconds an American will have an MI
• In the US in 2019, coronary events are expected in 1,055,000 individuals
including 720,000 new and 335,000 recurrent coronary events
Heart Disease and Stroke Statistics-2019 Update: A Report from the American Heart Association. Circulation 2019; Jan 31

The Changes To Our Current Plan• More accurate assessment of risk
– Coronary calcium scores
– Expanded risk assessment tools
• Prevention• Hypertension
• Diabetes
• Lipids
• Medical management
– Fish oil
– Anti inflammatory
– PCSK 9 inhibitors
– Anti coagulants
– ASA
– Antidiabetes meds
– Nonpharmacologic management
• Valvular disease

Lipid management guidelines (changes from 2013)
• 2013: Made use of pooled cohort equations for primary prevention, which provide good 10 year estimates of risk in most situations
– Variables: Race, gender, age, total cholesterol, HDL, Systolic BP, hypertension, diabetes, smoking
• 2018: Update
– Continued use of the pooled cohort equations
– Added concept of risk enhancers
• Family history
• Metabolic syndrome
• Chronic kidney disease
• Chronic inflammatory diseases: psoriasis, rheumatoid arthritis, HIV
• Certain ethnicity (South Asian descent: India, Bangladesh, Sri Lanka, Bhutan and the Madives; 4 fold higher risk than the general population and tend to develop it 10
years earlier)
• History of premature menopause or preecclampsia
• High levels of Lp(a) or apolipoprotein B
• Coronary artery calcium score
– May help as a “tiebreaker” for persons who are candidates for statin therapy in primary prevention, but unsure about committing to a long-term course of
statin therapy
• Added recommendations for ezetimibe (Zetia), evolocumab (Repatha) and alirocumab (Praluent) to secondary prevention patients unable to achieve LDL goals (<70) on statin alone.
• Use of non fasting lipid levels is acceptable in most circumstances

Coronary artery calcium score
• Non contrast CT scan
• Radiation dose of about 1 mSv ~ the same
radiation dose as a mammogram
• Not covered by insurance
• Costs $50-$300 out of pocket

Coronary CT
• Coronary calcium score
• Coronary CT angiogram

Prevention
• Medical management
– SGLT2 inhibitors
– GLP1 agonists
– PCSK9 Inhibitors
– Rivaroxiban
– ASA
– Eicosapent ethyl/omega 3
– Bempedoic acid

Omega 3 Fatty Acids• Bang and Dyerberg in 1970’s reported that Greenland Inuit, despite a diet
high in saturated fat and cholesterol, serum lipids , particularly
triglycerides, were significantly lower than in Danes and hypothesized
that it was the omega 3 fatty acids that were responsible
• Two families of dietary PUFA’s:
– omega 3
• Plant: alpha linolenic acid
• Marine: EPA, DPA and DHA
– omega 6
• Mechanism of action is complex, but involves inhibition of fatty acid
synthesis (lipogenesis) and stimulation of fatty acid oxidation

Omega 3 on lipid profile

Omega 3 FA Early Clinical Trials• GISSI Trial
– 11,234 Italian patients with recent MI (<3 months) and
randomized to 0.85 g/day of EPA and DHA for 3.5 years
– 21% reduction in mortality
– 44% reduction in sudden death
– Primary endpoint (death, non fatal MI and non fatal stroke(
was significantly reduced by 15%
– Results were thought to be mediated by an anti-arrhythmic
effect. Study was also criticized for its methodology

Omega 3 FA Early Clinical Trials
• JELIS Trial
– Japanese 14,981 primary prevention patients and 3664 secondary
prevention
– Group had high baseline Omega 3 FA intake
– Intervention: 1.8 mg QD of highly purified EPA to statin therapy
– 4.6 year follow up
– Incidence of major events reduced by 19%, including composite of
non fatal MI, CHD death, unstable angina and revascularization
– Benefit was seen only in secondary protection group
– ? Generalizability of the study
Omega 3
• REDUCE IT Trial
• ASCEND
• VITAL

Icosapent ethyl
• Pharmaceutical grade omega 3 fatty acid
• REDUCE-IT Trial
– High dose purified EPA –only (Vascepa) 4 GM/day
– Endpoints: CV death, non fatal MI, non fatal stroke, coronary revascularization or unstable angina
– 8,179 patients; median age 64, 71% men
– triglycerides 135-499 and LDL 41 to 100
– Prior CVD or DM
– Median follow up 4.9 years
– Total primary endpoints were reduced by 30% over placebo
• 61 per 1,000 patient years vs 89 per 1,000 patient years on placebo RR=0.7, 95% CI 0.62-0.78
• 20% reduction in CV death
• 31% reduction in MI
• 28% reduction in stroke
• Low risk of adverse events; increased risk of hospitalization for AF

ASCEND
• 15,480 patients with DM, but no CAD
• 1 GM n-3 fatty acids or olive oil placebo
• Outcomes: non fatal MI, CVA, TIA, vascular death
• 7.4 years of follow up
• No significant difference in rates of vascular
events, revascularization or death Effects of n-3 Fatty Acid Supplements in Diabetes Mellitis: N Engl J Med 2018; 379:1540-1550 DOI: 10.1056/NEJMoa1804989

VITAL Trial• 25,871 patients, men 50 and older, women 55 and older
• Primary endpoints
– Composite of MI, stroke, or death from CV causes. Secondary endpoints were
individual components of the composite
• Intervention: 1 GM QD of an omega-3 drug (Lovaza or Omacor) (or Vit D in
a separate arm of the study)
• 5.3 years of follow up
• However some secondary outcomes were promising
– MI risk 28% lower
• Greatest benefit in low consumption of omega 3 and in blacks
Marine N-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer: N Engl J Med2019; 380: 23-32 DOI: 10.1056/NEJMoa1811403

Canakinumab• CANTOS Trial
– Monoclonal antibody targeting interleukin-1 beta
– 10,061 patients with previous MI and elevated CRP (>2mg/l)
– 3 dose ranges (50,150 and 300mg) tested SQ Q3months
– Endpoints: non fatal MI, any non fatal stroke, CV death
– Showed reductions in CRP
– Only one dose (150mg Q 3 months) showed a statistically significant reduction in recurrent events
(p=0.005). There was no mortality benefit.
– Treatment was associated with higher incidence of fatal infection relative to placebo
• First drug targeting inflammation to show benefit in CV risk reduction
• Not approved by the FDA
• Cost is $73,000 per year
• QALY $6.4 million, $100,000 is considered acceptable
Anti inflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med 2017; 377-1119-1131 DOI: 10.1056/NEJMoa1707914

Omega 3 takeaways• May benefit patients with low intake of omega 3
or African American patients
• Icosapent ethyl demonstrated to show benefit in
the highest risk patients (known disease with
elevated triglycerides)
– Dose
– Higher ratio of EPA to docosahexanoic acid
Aspirin for primary prevention
• Patients at intermediate levels of risk
• All trials showed lower than expected rates of
vascular disease events:
• ASCEND
• ARRIVE
• ASPREE

Ebers papyrus

Aspirin

Aspirin
• Acetylsalicylic acid
– A precursor to ASA is found in leaves from the willow tree and has been used for 2400 years
– First synthesized in 1853 by Charles Gerhardt
– 1899 Bayer found that it was less irritating than other salicylates in use at the time and began marketing it under the name
“Aspirin”
• NSAID
• Used to treat pain, fever, inflammation
• Used in secondary prevention for CAD and CVA
• May reduce the risk of colorectal cancer
• Mechanism
– Irreversible inactivation of cyclooxygenase (COX) required for prostaglandin and thromboxane synthesis; Nobel prize to British
pharmacologist John Robert Vane for this discovery in 1982
– Blocks formation of thromboxin A2 in platelets, which inhibits platelet aggregation for the life of the platelet (8-9 days)
– May be some other effects mediated via COX 1 and 2 that mediate inflammation; affect mitochondria; induces formation of
nitric oxide and modulates signalling through NF-KB.
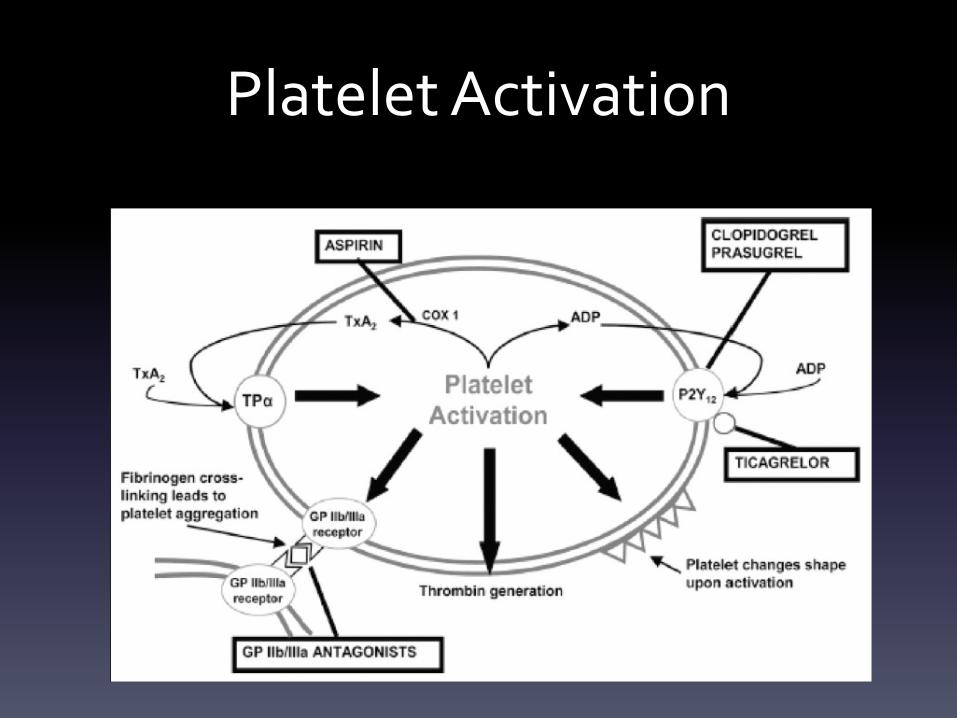
Platelet Activation

ASPREE
• Adults older than 70 (>= 65 for blacks and Hispanics), free from CVD, dementia or disability
• N=19,114
• Low dose ASA (100 mg QD)
• 4.7 year follow up
• Outcome:
– Fatal CHD, non fatal MI, stroke, HF hospitalization
• ASA 10.7 events per 1,000 person-years; placebo 11.3 events per 1,000 person years HR=0.95; 95% CI 0.83-1.08
– Major hemorrhage
• ASA 8.6 events per 1,000 person-years; placebo 6.2 events per 1,000 person years. HR=1.38; 95% CI, CI 1.16-1.82
– Cancer related death
• ASA 3.1% ; placebo 2.3%; HR 1.31,95% CI 1.1-1.56
Effect of Aspirin on Cardiovascular Events and Bleeding in the Health ElderlyNEJM 2018; 379;1509-1518 DOI:10.1056/NEJMoa1805819

ARRIVE
• Men aged <55, women <60 and at moderate risk of CV
• N=12,546
• Outcome
– CV death, MI, USA, CVA or TIA
• ASA 4.29%; placebo 4.48%; HR=0.96, 95% CI, 0.81-1.13
– GI bleeding
• ASA 0.97%; placebo 0.46%; HR 2.11, 95% CI 0.79-0.97
Lancet. 2018 Sep 22; 392 (10152): 1036-1046

ASCEND• Patients with diabetes but no evidence of CAD
• N=15,480
• ASA dose 100 mg QD
• Outcome
– MI, CVA, TIA, vascular death excluding intracranial hemorrhage
• ASA 8.5%; placebo 9.6%; rate ratio=0.88; 95% CI, 0.79-0.97
– Major bleeding
• ASA 4.1%; placebo, 3.2%; rate ratio=1.29; 95% CI, 1.09-1.52
• No cancer difference in ASA vs placebo
The ASCEND Study Collaborative Group. NEJM 2018;DOI:10.1056/NEJMoa804988

Conclusions• No benefit at all
• -or-
• May have benefit in certain circumstances
• ACC:
– Should not be used at all in patients 70 years or older or in patients at
high bleeding risk
– May be considered for patients 40-70 years of age at high risk of CVD
and low risk of bleeding
• e.g. Positive coronary calcium score, strong family history, very high lipids
and statin intolerant, high ASCVD risk (>20%)
Considerations for ASA in primary prevention
• Be sure benefit outweighs risk
• Evaluate risk factors
– ASCVD risk score (greater than 20%), FH of premature ASCVD, and possibly
an elevated coronary calcium score
• Consider risk of bleeding
– Comorbidities, PUD c/b bleeding, recent ulcers, recent GIB, kidney disease,
other NSAID use
• ASA should be considered once other options have been implemented,
i.e., lipid lowering, BP reduction, and smoking cessation
• Strong family history of colon CA may favor ASA use

Rivaroxiban (Xarelto)
• Factor Xa inhibitor, inhibiting thrombin
formation
• Approved for use in 2011
• Indications include
– Stroke prophylaxis in non valvular AF
– DVT prophylaxis
– DVT/PE treatment

Rivaroxiban
• COMPASS Trial
• ASA combined with low dose rivaroxiban (2.5 mg BID)
compared with ASA alone
• Reduced CV events by 24% in patients with CAD
• Reduced CV events by 28% in patients with PAD
• 51% increased risk of major bleeding, but not fatal
bleeds or ICH
N Engl J Med 2017 Oct 5;377[14];1319-30
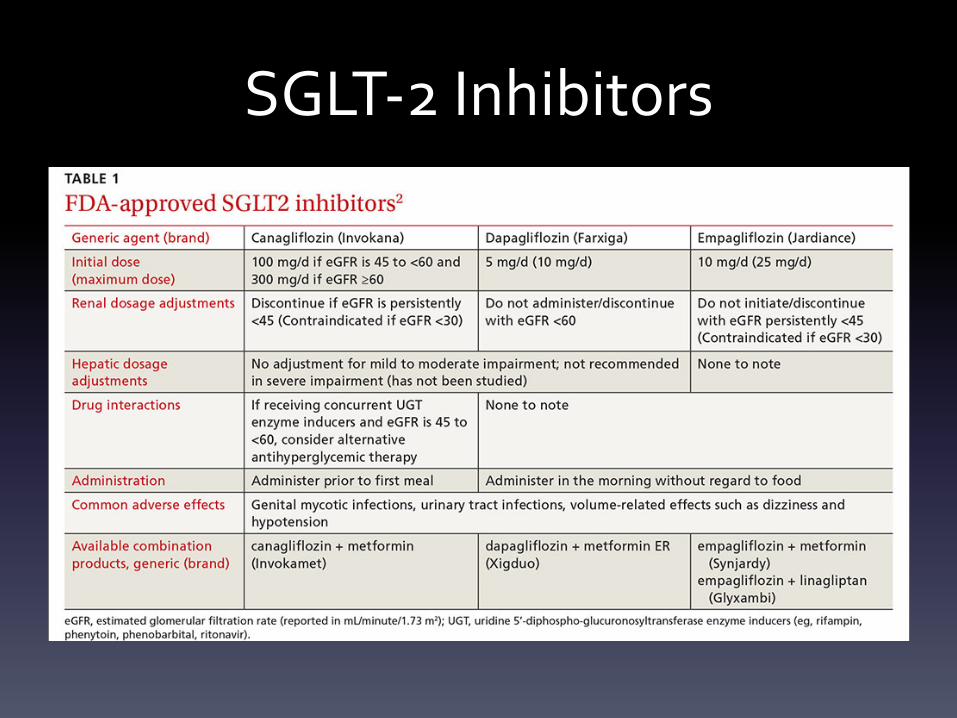
SGLT-2 Inhibitors


SGLT-2 Inhibitors
• Empagliflozin
– EMPA-REG Trial
• Dapagliflozin
– DECLARE TIMI 58Trial

Empagliflozin (Jardiance)
• SGLT-2 Inhibitor
• EMP-REG Outcome Trial
– 7,020 patients with type 2 DM and CAD
– Compared with placebo
• Reduced all-cause mortality over 3.1 years of follow up
• Reduced C-V mortality by 38%
• Reduced HF hospitalizations by 35%
N Engl J Med. 2015 Nov 26;373[22]:2117-28
Empagliflozin• EMPA-HEART Cardiolink 6 Trial
– Randomized trial of 97 patients with type 2 DM and CAD
– In 6 months of treatment
• Reduced LV mass by 4.71 gm vs 0.39 gm with placebo
• Systolic BP decreased 7.9 mm Hg vs 0.7 mm Hg with placebo
• Hematocrit increased by 1.91% relative to placebo
• Mechanism of benefit is unclear, but this study suggests
there is a direct effect on cardiac remodeling plus other
non cardiac mechanisms

Dapagliflozin (Farxiga)
• DECLARE-TIMI 58 Trial
– 17,160 patients with type 2 DM from 33 countries
– 7,000 with CAD
– 10,000 with risk factors for CAD
– At least 40 years of age
• MACE rate similar to placebo
• 17% lower rate of CV death, 33% hospitalization for HF
• Less robust benefit than empagliflozin
N Engl J Med 2019; 380 :347-357. DOI: 10.1056/NEJMoa1812389
CANVAS Program
• Two sister trials (CANVAS and CANVAS-R)
• 10,142 patients with Type 2 DM and kidney disease
• 100 mg QD of canagliflozin or placebo
• Primary outcome: composite of doubling of serum creatinine or death from cardiovascular cause
• Trial was event driven and stopped early
• Event rate was significantly lower in the canagliflozin group (43.2 vs 61.2 per 1000 patient years).
– 30 percent lower relative risk
– Patients in the treatment group had a lower risk of CV death, hospitalization for heart failure, MI or stroke
– The relative risk of the composite of end stage kidney disease, doubling of the serum creatinine or renal
death was 34% lower with treatment
– Rates of adverse events was similar in both groups except for an increased risk of amputation
N Engl J Med 2019; Apr 14

Use of SGLT-2 Inhibitors

SGLT-2
• Currently, empagliflozin and canagliflozin are
the SGLT-2 inhibitors indicated for the
reduction of CV events in adults with type 2
DM and established CVD

Glucagon-like Peptide-1 Receptor Agonists (GLP-1)
• Agonists of the GLP-1 receptor
• Indicated for the treatment of Type 2 DM
• Currently approved medications include:
– exenatide (Byetta) approved 2005
– liraglutide (Victoza) approved 2010
– lixisenatide (Lyxumia) approved 2016
– abliglutide (Tanzeum) approved 2014
– dulaglutide (Trulicity) approved 2014
– semaglutide (Ozempic) approved 2017

GLP-1
• GLP-1 is a peptide hormone secreted by the
enteroendocrine cells of the distal small intestine
and colon, alpha cells of the pancreatic islets and
neurons in the CNS
• It is secreted in response to nutrient ingestion
and mediates regulatory effects on glucose
assimilation and homeostasis

GLP-1 Agonists MOA

GLP-1 Trials
• LEADER
– 9,340 adults with increased cardiovascular risk (CAD, CVA, PAD, CKD>3, HF 2-3 or age > 60 with at least 1
CRF) and type 2 DM
– Liraglutide vs placebo vs 3.5 years
– Primary composite outcome: death from CV causes, non fatal MI or non fatal CVA
– Primary CV outcome was decreased relative to placebo, HR 0.87 (95% CI 0.78-0.97, P=0.01)
– Outcome was driven mostly by reduction in fatal events
• CV mortality HR 0.78 (95% CI 0.66-0.93, p=0.007)
• Total mortality (death from any cause) HR 0.85 (95% CI 0.74-0.97, p=0.02
• However, individual rates of non fatal MI, non fatal CVA and hospitalization for HF were no
different
• Theorized that benefit may be related to mechanism other than an antiatherosclerotic effect
Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311-22.

Other GLP-1 Trials
• EXSCEL
– 14,752 high risk patients with type 2 DM
– Exenatide vs placebo
– No statistically significant benefit on CV event reduction
• ELIXA
– 6068 patients with type 2 DM and CV disease
– Lixisenatide vs placebo
– No statistically significant benefit on CV risk reduction
Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med2015;373:2247-57.
Rationale and design of the EXenatide Study of Cardiovascular Event Lowering (EXSCEL) trial. Am Heart J 2016;174:103-10.

GLP-1 agonists
• Currently, only liraglutide has the indication
for reduction in the risk of major adverse
cardiac events (MACE) in adults with type 2
DM and established CV disease

SGLT-2/GLP-1
• Should be considered for patients with type 2 DM and
cardiovascular disease; metformin should probably be baseline
therapy
• Will require more coordination of care between primary care and
cardiology
– When to add these meds?
– Who makes the decision?
– Monitoring of treatment?
– Answer: Probably not the cardiologist (we are not good at this!)

Hypertension Guidelines
• 2017
ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/
ASPC/NMA/PCNA
• Led by ACC and AHA
• Special care was taken to govern conflicts of
interest and relationships with industry

Important Points• Recognize patterns of blood pressure abnormalities
– “Masked” HTN (aka ‘reverse white coat HTN’):
• Defined as normal BP in the office, but elevated outside
• Affects 15-25% of the population
• Similar risk for CV disease compared with those with sustained HTN
• Suspect it in patients with target organ damage of HTN, but with
normal BP
• More common in African Americans, DM and chronic renal failure
• Gold standard for diagnosis is ambulatory BP monitor

BP Patterns
Office/clinic/Healthcare setting
• No HTN
• HTN
• No HTN
• HTN
Home/Nonhealthcare setting
• No HTN
• HTN
• HTN
• No HTN
Normotensive
Sustained HTN
Masked HTN
White Coat HTN

Paul K. Whelton et al. JACC 2018;71:e127-e248
2018 American College of Cardiology Foundation and the American Heart Association, Inc.

BP classification
• Normal, elevated, stage 1 and stage 2
• Prehypertension and high normal are no
longer used

Overview of BP Diagnosis and Management
Paul K. Whelton et al. JACC 2018;71:e127-e248
2018 American College of Cardiology Foundation and the American Heart Association, Inc.

Theres an APP for that


HTN Take aways
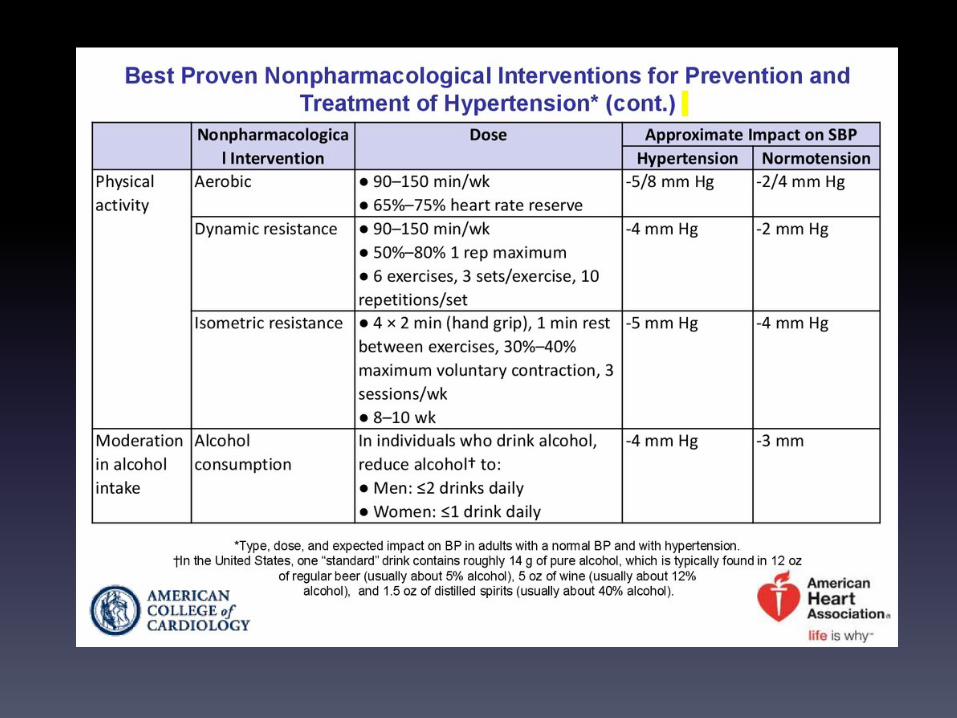
• Non pharmacologic therapy will be the recommended treatment
for the majority of patients with newly diagnosed HTN
• Formal assessment of risk drives treatment thresholds and targets.
• For most patients, BP goal is 130/80 or less
• Four agents are recommended: thiazides, calcium channel
blockers, ACE and ARB, with thiazides being the first line agents
• Concepts of prehypertension and high normal are removed

HTN
• Renal artery denervation
– RF Ablation
– US ablation
• Radiance II Trial
– Patients 18-75 with either controlled BP on meds, or
uncontrolled and on meds are eligible
RADIANCE Trial

PCSK-9 Inhibitors
• Evolocumab (Repatha)
• Alirocumab (Praluent)
• Both given by injection 1-2 per month
• Average LDL reduction of 50-60% on monotherapy
• Indications
– CAD: Inability to achieve goals of treatment on maximal therapy or
maximally tolerated therapy
– Primary prevention: LDL>190, usually with some evidence of familial
hypercholesterolemia (FH), and inability to achieve goals with maximal
therapy or maximally tolerated therapy

PCSK 9 MOA
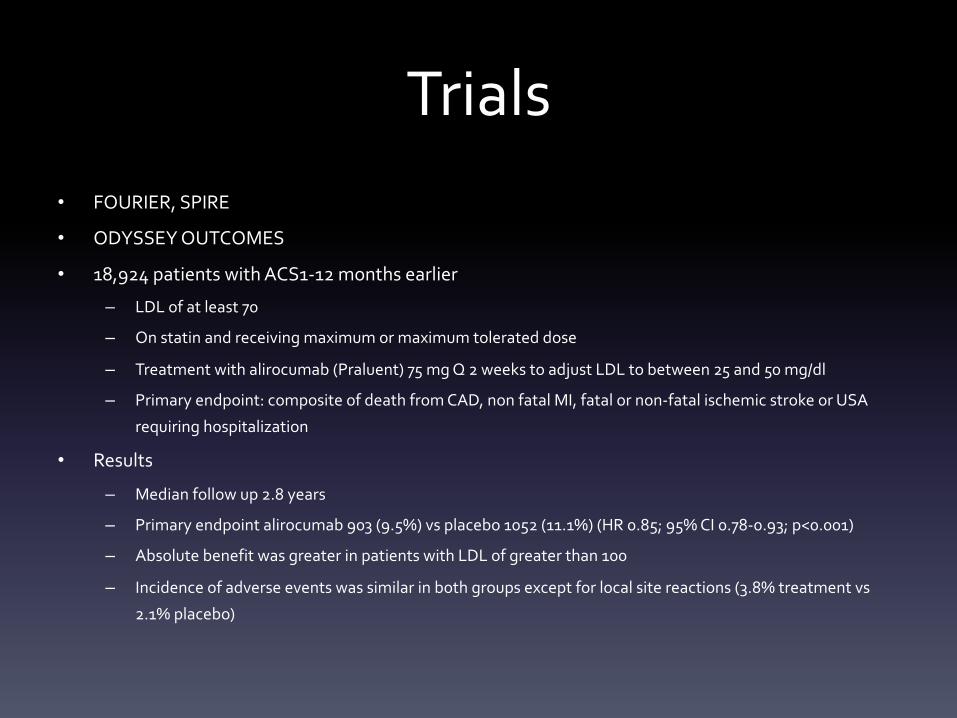
Trials• FOURIER, SPIRE
• ODYSSEY OUTCOMES
• 18,924 patients with ACS1-12 months earlier
– LDL of at least 70
– On statin and receiving maximum or maximum tolerated dose
– Treatment with alirocumab (Praluent) 75 mg Q 2 weeks to adjust LDL to between 25 and 50 mg/dl
– Primary endpoint: composite of death from CAD, non fatal MI, fatal or non-fatal ischemic stroke or USA
requiring hospitalization
• Results
– Median follow up 2.8 years
– Primary endpoint alirocumab 903 (9.5%) vs placebo 1052 (11.1%) (HR 0.85; 95% CI 0.78-0.93; p<0.001)
– Absolute benefit was greater in patients with LDL of greater than 100
– Incidence of adverse events was similar in both groups except for local site reactions (3.8% treatment vs
2.1% placebo)
PCSK 9• Advantages
– Clinically proven to reduce LDL and subsequently
reduce CV events, either alone or in addition to
standard therapy
– Fairly simple and convenient to use
– Low incidence of SE

PCSK 9• Disadvantages
– Expense
• Initially both were about $1,400/mo ~ $14,000/year
– Not cost effective at this price
• More recently
– Both have reduced prices to about $450/month
– Appears to be cost effective for the highest risk patients
• Hoops to jump through
– Paperwork demonstrating prior treatments
• Usually need atorva, rosuvastatin and ezetimibe trials
• LDL levels
• Document failure to achieve goals on treatment or intolerance
• 80% of plans still require cardiology/endocrin/lipid doc to sign off for insurance approval

TAVR
• Trans catheter aortic valve replacement
• Indicated for intermediate and high risk
patients with severe AS
• PARTNER 3 and Evolut Low Risk Trials

Partner 3• 1,000 patients, mean age 73 with severe AS and a mean STS score of 1.9% (low risk)
• Randomly assigned to TAVR with a Sapien 3 valve or surgical valve replacement
• Outcomes at 1 year:
– Death/stroke/rehospitalization
• TAVR 8.5% SAVR 15.1%
– Mortality
• TAVR 1% SAVR 2.5%
– All stroke
• TAVR 1.2% SAVR 3.1%
– Death or disabling stroke
• TAVR 1% SAVR 2.9%
– Rehospitaliztion
• TAVR 7.3% SAVR 11%
• Similar results in Evolut Low risk Trial, although it showed higher rates of AR and pacemaker
implant than the surgical gruop
Mack M, et al. N Engl J Med 2019; doi: 10.1056/NEJMoa 1814052

TAVR
• About 50% of patients in the US are getting TAVR vs SAVR,
and this is expected to grow
• Questions remain regarding long term durability
• Factors favoring SAVR:
– Younger, < 60
– Bicuspid aortic valves
– Other valve, CAD or aortic disease
– Severely calcified annulus

Summary
• Exciting time in cardiovascular disease, especially prevention
• More effective tools for risk assessment.
• Use of imaging for assessing presence or absence of disease
• Renewed focus on lifestyle
• New and effective therapeutics available or in the pipeline
• Need for coordination between cardiology and primary care to
provide maximum benefit for the patient
![Unique Fundraiserscharitymania.com/Documents/CharityMania-Brochure.pdf · tiebreaker. See website for tiebreaker examples. [4] A football team that does not play (i.e. has a bye)](https://img.pdfslide.us/doc/110x75/5e212fdf95fceb21fb2b8700/unique-fun-tiebreaker-see-website-for-tiebreaker-examples-4-a-football-team.jpg)
























![Polymorphic forms of human apolipoprotein[a]: inheritance and](https://img.pdfslide.us/doc/110x75/58a2fe571a28abeb428c0e16/polymorphic-forms-of-human-apolipoproteina-inheritance-and-.jpg)



