Embed Size (px)
Citation preview

Journal of Cardiology xxx (2014) xxx–xxx
G Model
JJCC-907; No. of Pages 9
Review
Update in acute aortic syndrome: Intramural hematoma andincomplete dissection as new disease entities
Jae-Kwan Song (MD, PhD, FACC)*
Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Aortic intramural hematoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Issues regarding characteristic imaging findings. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
How does blood accumulate within the aortic wall in IMH? Rupture of vasa vasorum or micro-intimal tear . . . . . . . . . . . . . . . . . . 000
Different clinical features and outcomes: AD vs. IMH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Incomplete dissection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
Disclosure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 000
A R T I C L E I N F O
Article history:
Received 15 May 2014
Accepted 15 May 2014
Available online xxx
Keywords:
Acute aortic syndrome
Aortic dissection
Intramural hematoma
Computerized tomography
Transesophageal echocardiography
A B S T R A C T
Acute aortic syndrome is a relatively recent clinical entity. Non-invasive imaging methods, such as
computed tomography and transesophageal echocardiography, have contributed significantly to the
diagnosis of variant forms of classic aortic dissection, which have become important disease entities in
acute aortic syndrome. Imaging findings may result in risk stratification and application of different
treatment options, providing a rational approach to achieve a better outcome of this syndrome. This
review will focus on the imaging characteristics of two important variant forms of classic aortic
dissection, intramural hematoma and incomplete dissection, and the role of imaging methods in the
evaluation of differences in the hemodynamic status of false lumens that contributes to patient
prognosis.
� 2014 Published by Elsevier Ltd on behalf of Japanese College of Cardiology.
Contents lists available at ScienceDirect
Journal of Cardiology
jo u rn al h om ep age: ww w.els evier .c o m/lo c ate / j j c c
Introduction
The successful clinical introduction of various non-invasiveimaging modalities has contributed to the establishment of ‘acuteaortic syndrome’, a relatively recent clinical syndrome incorporat-ing several disease entities with similar clinical features (at thetime of clinical presentation) [1]. Aortic dissection (AD) with
* Correspondence to: Cardiac Imaging Center, Asan Medical Center Heart
Institute, University of Ulsan College of Medicine, 388-1 Poongnap-dong
Songpa-gu, Seoul 138-736, South Korea. Fax: +82 2 486 5918.
E-mail address: [email protected]
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
http://dx.doi.org/10.1016/j.jjcc.2014.05.005
0914-5087/� 2014 Published by Elsevier Ltd on behalf of Japanese College of Cardiolo
intimal flap and two aortic channels (true and false lumens) isthe most important disease entity in acute aortic syndrome. Theclinical characteristics of AD have been established, withstandardized treatment strategies depending on the affected siteof the aorta. For the past several decades, variant forms of classicAD, including aortic intramural hematoma (IMH) and incompletedissection have been increasingly diagnosed in routine clinicalpractice worldwide, and imaging findings characteristic of thesevariant forms have been established for their differential diagnosis.As imaging findings, rather than clinical features, are critical forthe differential diagnosis of acute aortic syndrome [1–4], carefulinterpretation of imaging results is necessary for accuratediagnosis and better clinical decision making, thus improving
drome: Intramural hematoma and incomplete dissection as new4.05.005
gy.
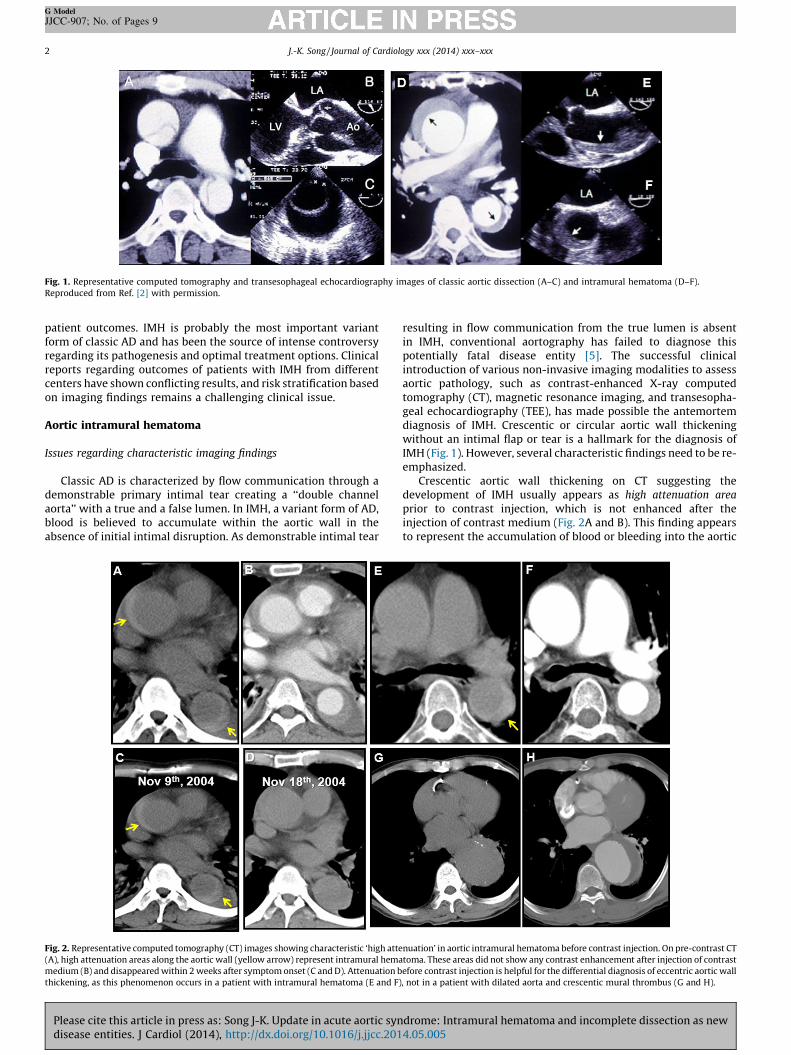
Fig. 1. Representative computed tomography and transesophageal echocardiography images of classic aortic dissection (A–C) and intramural hematoma (D–F).
Reproduced from Ref. [2] with permission.
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx2
G Model
JJCC-907; No. of Pages 9
patient outcomes. IMH is probably the most important variantform of classic AD and has been the source of intense controversyregarding its pathogenesis and optimal treatment options. Clinicalreports regarding outcomes of patients with IMH from differentcenters have shown conflicting results, and risk stratification basedon imaging findings remains a challenging clinical issue.
Aortic intramural hematoma
Issues regarding characteristic imaging findings
Classic AD is characterized by flow communication through ademonstrable primary intimal tear creating a ‘‘double channelaorta’’ with a true and a false lumen. In IMH, a variant form of AD,blood is believed to accumulate within the aortic wall in theabsence of initial intimal disruption. As demonstrable intimal tear
Fig. 2. Representative computed tomography (CT) images showing characteristic ‘high atte
(A), high attenuation areas along the aortic wall (yellow arrow) represent intramural hema
medium (B) and disappeared within 2 weeks after symptom onset (C and D). Attenuation b
thickening, as this phenomenon occurs in a patient with intramural hematoma (E and F)
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
resulting in flow communication from the true lumen is absentin IMH, conventional aortography has failed to diagnose thispotentially fatal disease entity [5]. The successful clinicalintroduction of various non-invasive imaging modalities to assessaortic pathology, such as contrast-enhanced X-ray computedtomography (CT), magnetic resonance imaging, and transesopha-geal echocardiography (TEE), has made possible the antemortemdiagnosis of IMH. Crescentic or circular aortic wall thickeningwithout an intimal flap or tear is a hallmark for the diagnosis ofIMH (Fig. 1). However, several characteristic findings need to be re-emphasized.
Crescentic aortic wall thickening on CT suggesting thedevelopment of IMH usually appears as high attenuation area
prior to contrast injection, which is not enhanced after theinjection of contrast medium (Fig. 2A and B). This finding appearsto represent the accumulation of blood or bleeding into the aortic
nuation’ in aortic intramural hematoma before contrast injection. On pre-contrast CT
toma. These areas did not show any contrast enhancement after injection of contrast
efore contrast injection is helpful for the differential diagnosis of eccentric aortic wall
, not in a patient with dilated aorta and crescentic mural thrombus (G and H).
drome: Intramural hematoma and incomplete dissection as new4.05.005
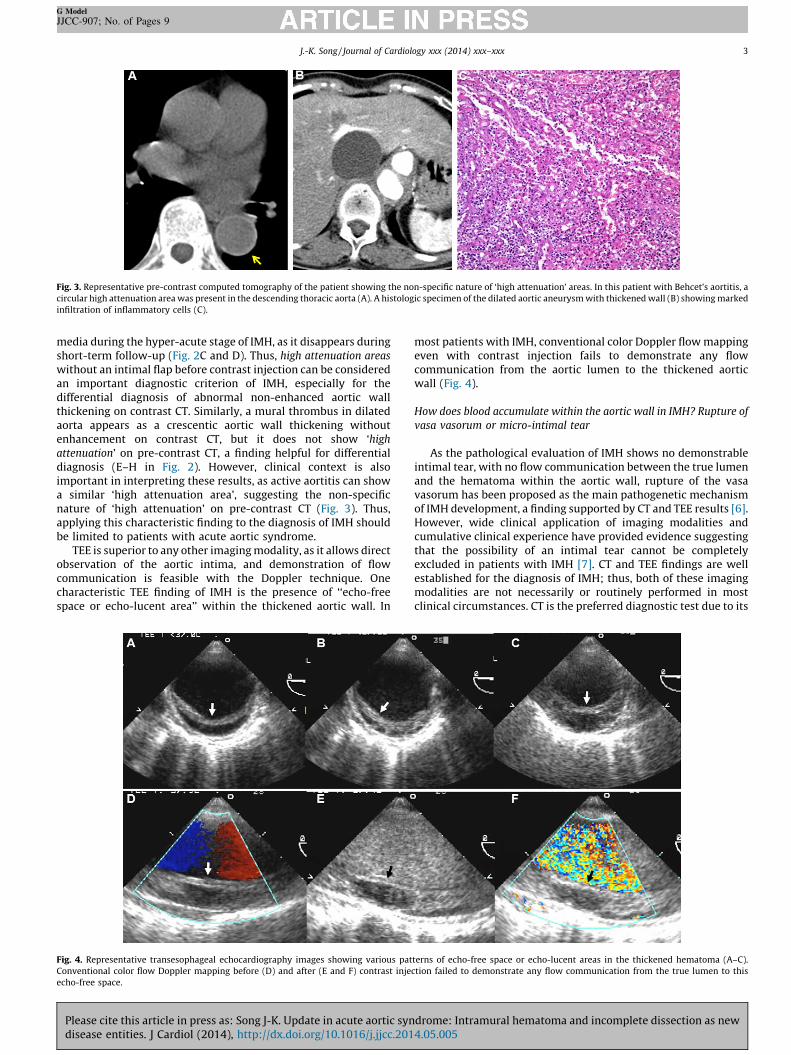
Fig. 3. Representative pre-contrast computed tomography of the patient showing the non-specific nature of ‘high attenuation’ areas. In this patient with Behcet’s aortitis, a
circular high attenuation area was present in the descending thoracic aorta (A). A histologic specimen of the dilated aortic aneurysm with thickened wall (B) showing marked
infiltration of inflammatory cells (C).
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx 3
G Model
JJCC-907; No. of Pages 9
media during the hyper-acute stage of IMH, as it disappears duringshort-term follow-up (Fig. 2C and D). Thus, high attenuation areas
without an intimal flap before contrast injection can be consideredan important diagnostic criterion of IMH, especially for thedifferential diagnosis of abnormal non-enhanced aortic wallthickening on contrast CT. Similarly, a mural thrombus in dilatedaorta appears as a crescentic aortic wall thickening withoutenhancement on contrast CT, but it does not show ‘high
attenuation’ on pre-contrast CT, a finding helpful for differentialdiagnosis (E–H in Fig. 2). However, clinical context is alsoimportant in interpreting these results, as active aortitis can showa similar ‘high attenuation area’, suggesting the non-specificnature of ‘high attenuation’ on pre-contrast CT (Fig. 3). Thus,applying this characteristic finding to the diagnosis of IMH shouldbe limited to patients with acute aortic syndrome.
TEE is superior to any other imaging modality, as it allows directobservation of the aortic intima, and demonstration of flowcommunication is feasible with the Doppler technique. Onecharacteristic TEE finding of IMH is the presence of ‘‘echo-freespace or echo-lucent area’’ within the thickened aortic wall. In
Fig. 4. Representative transesophageal echocardiography images showing various pat
Conventional color flow Doppler mapping before (D) and after (E and F) contrast inje
echo-free space.
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
most patients with IMH, conventional color Doppler flow mappingeven with contrast injection fails to demonstrate any flowcommunication from the aortic lumen to the thickened aorticwall (Fig. 4).
How does blood accumulate within the aortic wall in IMH? Rupture of
vasa vasorum or micro-intimal tear
As the pathological evaluation of IMH shows no demonstrableintimal tear, with no flow communication between the true lumenand the hematoma within the aortic wall, rupture of the vasavasorum has been proposed as the main pathogenetic mechanismof IMH development, a finding supported by CT and TEE results [6].However, wide clinical application of imaging modalities andcumulative clinical experience have provided evidence suggestingthat the possibility of an intimal tear cannot be completelyexcluded in patients with IMH [7]. CT and TEE findings are wellestablished for the diagnosis of IMH; thus, both of these imagingmodalities are not necessarily or routinely performed in mostclinical circumstances. CT is the preferred diagnostic test due to its
terns of echo-free space or echo-lucent areas in the thickened hematoma (A–C).
ction failed to demonstrate any flow communication from the true lumen to this
drome: Intramural hematoma and incomplete dissection as new4.05.005

Fig. 5. Representative transesophageal echocardiography (TEE) of the patient demonstrating a ‘micro-intimal tear’. Initial computed tomography (CT) showed markedly
thickened hematoma without contrast enhancement (C). However, TEE showed flow communication from the true lumen to the thickened hematoma through a small intimal
tear (A and B). Follow-up CT showed marked contrast enhancement (*), suggesting flow communication from the true lumen (D). Ao, aorta; LV, left ventricle; RV, right
ventricle; TL, true lumen.
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx4
G Model
JJCC-907; No. of Pages 9
rapid accessibility and non-invasiveness suitable for the clinicalsetting of acute aortic syndrome. However, in rare cases, TEEevaluation of the aortic intima may provide evidence of ‘micro-tear’ or ‘a small intimal tear’ not visible on contrast CT (Fig. 5) [7].Moreover, traumatic aortic injury caused by a diagnostic ortherapeutic vascular catheter can result in a similar crescenticaortic wall thickening mimicking typical IMH (Fig. 6) [8–10]. Thesefindings suggest that a ‘micro-intimal tear’, rather than rupture ofthe vasa vasorum, is the initiating event for IMH development,with the tear not large enough to be visualized or detected byroutine CT or conventional TEE [1].
One recent clinical study reported that, during surgery, anintimal tear could be localized in 47% (77/165) of patients withtypical CT images suggesting IMH [11]. The prevalence of anintimal tear was significantly lower in patients with IMH than intypical AD patients (47% vs. 80%, p < 0.01), and the mean tear sizewas significantly smaller in the IMH group (1.8 � 1.0 cm vs.2.9 � 1.2 cm, p < 0.01). These findings suggest that, similar to classicAD, IMH develops from an intimal tear and, with negligible re-entryinto the true lumen, results in a thrombosed false lumen. Thus, IMHshould be referred to as ‘thrombosed-type AD’, with the sametreatment strategy applied to both patients with IMH and those withAD. Recent advances in CT techniques, resulting in higher resolutionaortic images, have allowed the detection of an aortic ‘intimal defect’in patients with otherwise typical IMH. Intimal defects detected by CTshow a wide clinical spectrum, from focal contrast enhancementwithin a thick hematoma or adjacent to the intima to a relatively largeulcer-like projection (Fig. 7) [12,13]. Although prognosis was worse inpatients with than without these intimal defects on CT, with the
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
former showing a higher frequency of progression to classic AD ordevelopment of an aortic aneurysm, hematoma resorption was themost common pattern of remodeling, even in patients with intimaldefects, indicating that these patients do not require urgentintervention. Moreover, no study to date has shown correlationsbetween aortic intimal defects on CT images and operative findings.Therefore, the true prevalence of intimal tear in patients with IMHcannot be estimated using CT images. In addition to an intimal tear, anaortic branch artery pseudoaneurysm or a simple penetrating ulcercan yield similar images on CT [14], reinforcing suggestions thatimaging results be interpreted cautiously. Despite these limitations,cumulative clinical experience has provided important evidenceindicating that patients with IMH may have a micro-intimal tear thatcannot be easily detected by CT or TEE in routine clinical practice.Thus, IMH can be considered as an ‘AD with a closed and thrombosedfalse lumen’ [15,16].
Differences in the hemodynamic status of the false lumen mayresult in the differentiation of classic AD and IMH, and can explainbetter the long-term outcomes in patients with retrograde type AAD. In about one-fourth of these patients with type A AD, anintimal tear is present in the upper part of the descending aorta andthere is retrograde extension of the dissection into the ascendingaorta [17]. Imaging findings characteristic of this condition includean IMH-like crescentic aortic wall thickening in the ascendingaorta and a ‘double channel aorta’ in the descending aorta (Fig. 8).Thus, the ascending aorta in this condition is a typical example of athrombosed false lumen, and medical treatment alone resulted incomplete resorption of the thrombosed false lumen, with a bettersurvival rate than that in patients with typical type A antegrade AD
drome: Intramural hematoma and incomplete dissection as new4.05.005
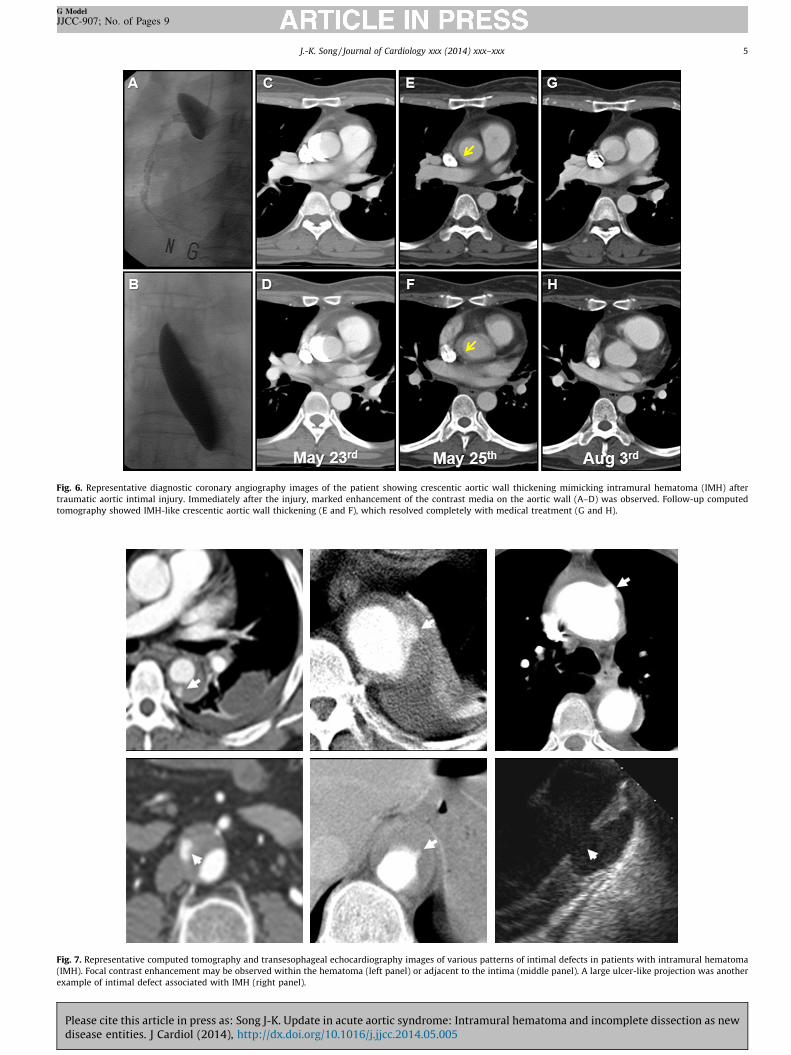
Fig. 6. Representative diagnostic coronary angiography images of the patient showing crescentic aortic wall thickening mimicking intramural hematoma (IMH) after
traumatic aortic intimal injury. Immediately after the injury, marked enhancement of the contrast media on the aortic wall (A–D) was observed. Follow-up computed
tomography showed IMH-like crescentic aortic wall thickening (E and F), which resolved completely with medical treatment (G and H).
Fig. 7. Representative computed tomography and transesophageal echocardiography images of various patterns of intimal defects in patients with intramural hematoma
(IMH). Focal contrast enhancement may be observed within the hematoma (left panel) or adjacent to the intima (middle panel). A large ulcer-like projection was another
example of intimal defect associated with IMH (right panel).
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx 5
G Model
JJCC-907; No. of Pages 9
Please cite this article in press as: Song J-K. Update in acute aortic syndrome: Intramural hematoma and incomplete dissection as newdisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.2014.05.005
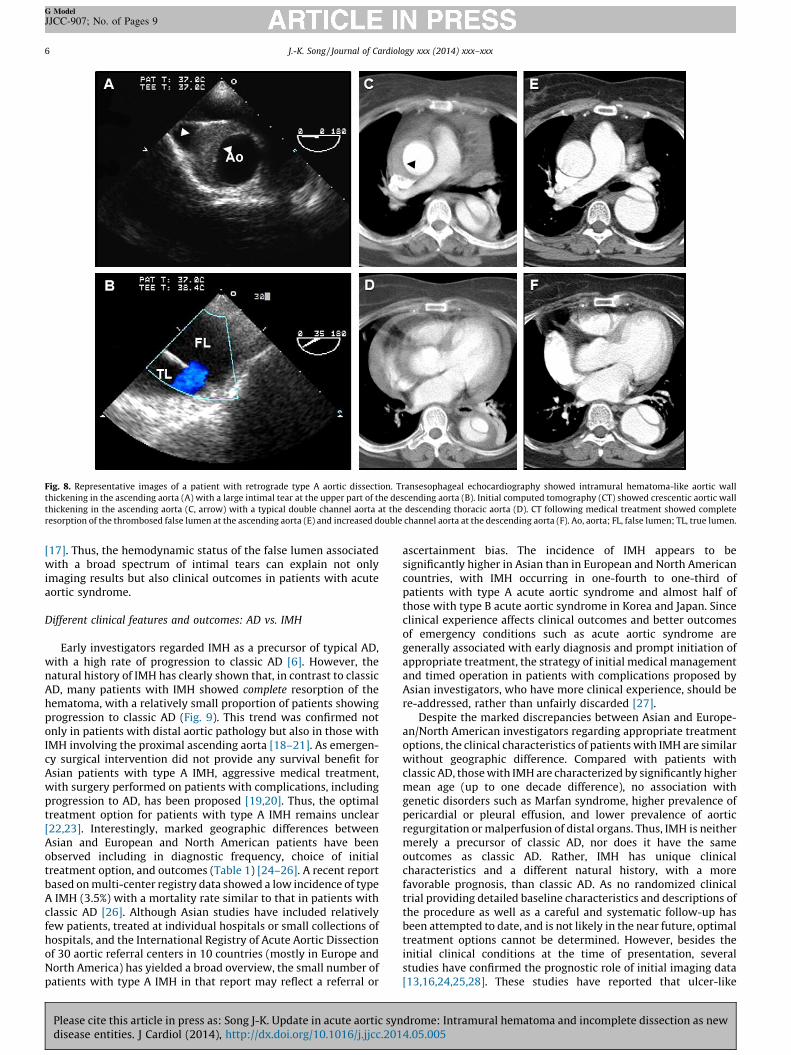
Fig. 8. Representative images of a patient with retrograde type A aortic dissection. Transesophageal echocardiography showed intramural hematoma-like aortic wall
thickening in the ascending aorta (A) with a large intimal tear at the upper part of the descending aorta (B). Initial computed tomography (CT) showed crescentic aortic wall
thickening in the ascending aorta (C, arrow) with a typical double channel aorta at the descending thoracic aorta (D). CT following medical treatment showed complete
resorption of the thrombosed false lumen at the ascending aorta (E) and increased double channel aorta at the descending aorta (F). Ao, aorta; FL, false lumen; TL, true lumen.
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx6
G Model
JJCC-907; No. of Pages 9
[17]. Thus, the hemodynamic status of the false lumen associatedwith a broad spectrum of intimal tears can explain not onlyimaging results but also clinical outcomes in patients with acuteaortic syndrome.
Different clinical features and outcomes: AD vs. IMH
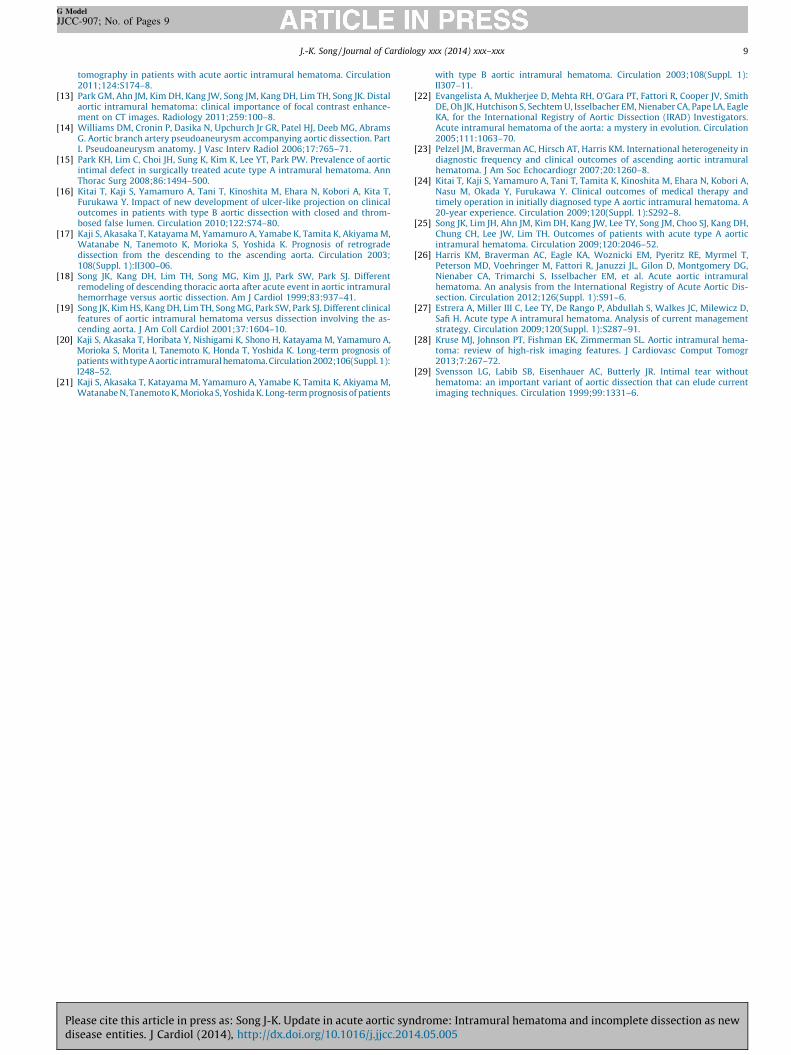
Early investigators regarded IMH as a precursor of typical AD,with a high rate of progression to classic AD [6]. However, thenatural history of IMH has clearly shown that, in contrast to classicAD, many patients with IMH showed complete resorption of thehematoma, with a relatively small proportion of patients showingprogression to classic AD (Fig. 9). This trend was confirmed notonly in patients with distal aortic pathology but also in those withIMH involving the proximal ascending aorta [18–21]. As emergen-cy surgical intervention did not provide any survival benefit forAsian patients with type A IMH, aggressive medical treatment,with surgery performed on patients with complications, includingprogression to AD, has been proposed [19,20]. Thus, the optimaltreatment option for patients with type A IMH remains unclear[22,23]. Interestingly, marked geographic differences betweenAsian and European and North American patients have beenobserved including in diagnostic frequency, choice of initialtreatment option, and outcomes (Table 1) [24–26]. A recent reportbased on multi-center registry data showed a low incidence of typeA IMH (3.5%) with a mortality rate similar to that in patients withclassic AD [26]. Although Asian studies have included relativelyfew patients, treated at individual hospitals or small collections ofhospitals, and the International Registry of Acute Aortic Dissectionof 30 aortic referral centers in 10 countries (mostly in Europe andNorth America) has yielded a broad overview, the small number ofpatients with type A IMH in that report may reflect a referral or
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
ascertainment bias. The incidence of IMH appears to besignificantly higher in Asian than in European and North Americancountries, with IMH occurring in one-fourth to one-third ofpatients with type A acute aortic syndrome and almost half ofthose with type B acute aortic syndrome in Korea and Japan. Sinceclinical experience affects clinical outcomes and better outcomesof emergency conditions such as acute aortic syndrome aregenerally associated with early diagnosis and prompt initiation ofappropriate treatment, the strategy of initial medical managementand timed operation in patients with complications proposed byAsian investigators, who have more clinical experience, should bere-addressed, rather than unfairly discarded [27].
Despite the marked discrepancies between Asian and Europe-an/North American investigators regarding appropriate treatmentoptions, the clinical characteristics of patients with IMH are similarwithout geographic difference. Compared with patients withclassic AD, those with IMH are characterized by significantly highermean age (up to one decade difference), no association withgenetic disorders such as Marfan syndrome, higher prevalence ofpericardial or pleural effusion, and lower prevalence of aorticregurgitation or malperfusion of distal organs. Thus, IMH is neithermerely a precursor of classic AD, nor does it have the sameoutcomes as classic AD. Rather, IMH has unique clinicalcharacteristics and a different natural history, with a morefavorable prognosis, than classic AD. As no randomized clinicaltrial providing detailed baseline characteristics and descriptions ofthe procedure as well as a careful and systematic follow-up hasbeen attempted to date, and is not likely in the near future, optimaltreatment options cannot be determined. However, besides theinitial clinical conditions at the time of presentation, severalstudies have confirmed the prognostic role of initial imaging data[13,16,24,25,28]. These studies have reported that ulcer-like
drome: Intramural hematoma and incomplete dissection as new4.05.005
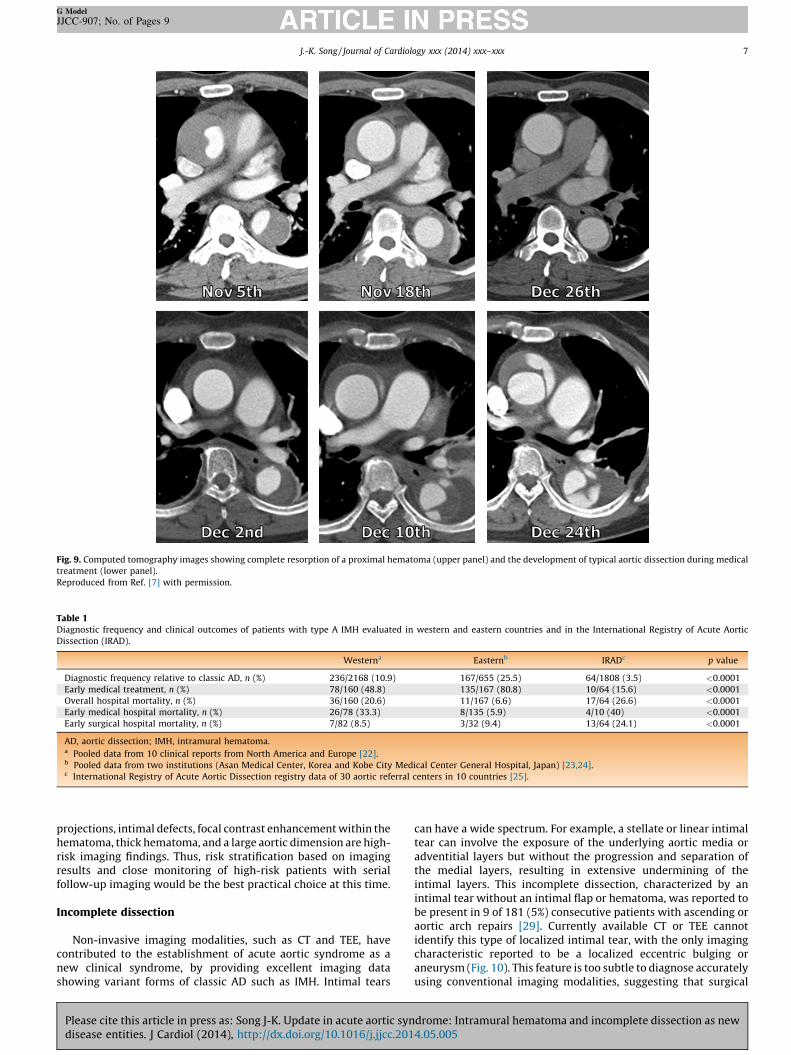
Fig. 9. Computed tomography images showing complete resorption of a proximal hematoma (upper panel) and the development of typical aortic dissection during medical
treatment (lower panel).
Reproduced from Ref. [7] with permission.
Table 1Diagnostic frequency and clinical outcomes of patients with type A IMH evaluated in western and eastern countries and in the International Registry of Acute Aortic
Dissection (IRAD).
Westerna Easternb IRADc p value
Diagnostic frequency relative to classic AD, n (%) 236/2168 (10.9) 167/655 (25.5) 64/1808 (3.5) <0.0001
Early medical treatment, n (%) 78/160 (48.8) 135/167 (80.8) 10/64 (15.6) <0.0001
Overall hospital mortality, n (%) 36/160 (20.6) 11/167 (6.6) 17/64 (26.6) <0.0001
Early medical hospital mortality, n (%) 26/78 (33.3) 8/135 (5.9) 4/10 (40) <0.0001
Early surgical hospital mortality, n (%) 7/82 (8.5) 3/32 (9.4) 13/64 (24.1) <0.0001
AD, aortic dissection; IMH, intramural hematoma.a Pooled data from 10 clinical reports from North America and Europe [22].b Pooled data from two institutions (Asan Medical Center, Korea and Kobe City Medical Center General Hospital, Japan) [23,24].c International Registry of Acute Aortic Dissection registry data of 30 aortic referral centers in 10 countries [25].
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx 7
G Model
JJCC-907; No. of Pages 9
projections, intimal defects, focal contrast enhancement within thehematoma, thick hematoma, and a large aortic dimension are high-risk imaging findings. Thus, risk stratification based on imagingresults and close monitoring of high-risk patients with serialfollow-up imaging would be the best practical choice at this time.
Incomplete dissection
Non-invasive imaging modalities, such as CT and TEE, havecontributed to the establishment of acute aortic syndrome as anew clinical syndrome, by providing excellent imaging datashowing variant forms of classic AD such as IMH. Intimal tears
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
can have a wide spectrum. For example, a stellate or linear intimaltear can involve the exposure of the underlying aortic media oradventitial layers but without the progression and separation ofthe medial layers, resulting in extensive undermining of theintimal layers. This incomplete dissection, characterized by anintimal tear without an intimal flap or hematoma, was reported tobe present in 9 of 181 (5%) consecutive patients with ascending oraortic arch repairs [29]. Currently available CT or TEE cannotidentify this type of localized intimal tear, with the only imagingcharacteristic reported to be a localized eccentric bulging oraneurysm (Fig. 10). This feature is too subtle to diagnose accuratelyusing conventional imaging modalities, suggesting that surgical
drome: Intramural hematoma and incomplete dissection as new4.05.005

Fig. 10. Representative pathologic specimen (A, courtesy of Dr. Vilacosta), diagram (B), and computed tomography (CT) images of incomplete dissection. Limited intimal tear
usually results in an eccentric bulge, which can be visualized by CT. Initial CT of this patient, who visited our emergency department due to severe aortic pain, showed
localized bulging with no evidence of AD or intramural hematoma (middle panel). CT following medical treatment showed progression of the aneurysmal bulging with
development of hemopericardium (right panel).
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx8
G Model
JJCC-907; No. of Pages 9
exploration be performed in patients with aortic pain and aorticroot dilatation who show unexplained aortic regurgitation orpericardial effusion [29]. Further investigations are necessary toevaluate the clinical significance and outcomes of patients withincomplete dissection.
Conclusion
Non-invasive imaging modalities such as CT and TEE havecontributed to a better understanding of acute aortic syndrome,resulting in the inclusion of IMH and atypical dissection as newdisease entities. Differences in imaging findings may be due todifferences in the hemodynamic status of the false lumen, resultingfrom the wide spectrum of intimal tears, from a localized or ‘micro-intimal tear’ to a large tear with flow communication resulting in a‘double channel aorta.’ Further investigation is required todetermine whether the application of different treatment optionsfollowing risk stratification based on imaging results is rationaland can improve the clinical outcomes of patients with thissyndrome.
Funding
None declared.
Disclosure
None declared.
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
References
[1] Vilacosta I, Aragoncillo P, Canadas V, San Roman JA, Ferreiros J, Rodrıguez E.Acute aortic syndrome: a new look at an old conundrum. Heart 2009;95:1130–9.
[2] Song JK. Diagnosis of aortic intramural haematoma. Heart 2004;90:368–71.[3] Nienaber CA. The role of imaging in acute aortic syndromes. Eur Heart J
Cardiovasc Imaging 2013;14:15–23.[4] Baliga RR, Nienaber CA, Bossone E, Oh JK, Isselbacher EM, Sechtem U, Fattori R,
Raman SV, Eagle KA. The role of imaging in aortic dissection and relatedsyndromes. J Am Coll Cardiol Imaging 2014;7:406–24.
[5] Bansal RC, Chandrasekaran K, Ayala K, Smith DC. Frequency and explanation offalse negative diagnosis of aortic dissection by aortography and transesopha-geal echocardiography. J Am Coll Cardiol 1995;25:1393–401.
[6] Mohr-Kahaly S, Erbel R, Kearney P, Puth M, Meyer J. Aortic intramuralhemorrhage visualized by transesophageal echocardiography: findings andprognostic implications. J Am Coll Cardiol 1994;23:658–64.
[7] Agricola E, Slavich M, Bertoglio L, Fisicaro A, Oppizzi M, Marone E, Melissano G,Tufaro V, Margonato A, Chiesa R. The role of contrast enhanced transesopha-geal echocardiography in the diagnosis and in the morphological and func-tional characterization of acute aortic syndromes. Int J Cardiovasc Imaging2014;30:31–8.
[8] Song JK. Aortic intramural hematoma: aspects of pathogenesis 2011. Herz2011;36:488–97.
[9] Vilacosta I, Castillo JA, Peral V, Batlle E, Rollan MJ, Sanchez-Harquindey L.Intramural aortic haematoma following intra-aortic balloon counterpulsation.Documentation by transoesophageal echocardiography. Eur Heart J 1995;16:2015–6.
[10] Vilacosta I, de Dios RM, Pinto AG. Aortic intramural hematoma during coro-nary angioplasty: insights into the pathogenesis of intramedial hemorrhage. JAm Soc Echocardiogr 2000;13:403–6.
[11] Uchida K, Imoto K, Karube N, Minami T, Cho T, Goda M, Suzuki SI, Masuda M.Intramural hematoma should be referred to as thrombosed-type aortic dis-section. Eur J Cardiothorac Surg 2013;44:366–9.
[12] Kitai T, Kaji S, Yamamuro A, Tani T, Kinoshita M, Ehara N, Kobori A, Kim K, KitaT, Furukawa Y. Detection of intimal defect by 64-row multidetector computed
drome: Intramural hematoma and incomplete dissection as new4.05.005
J.-K. Song / Journal of Cardiology xxx (2014) xxx–xxx 9
G Model
JJCC-907; No. of Pages 9
tomography in patients with acute aortic intramural hematoma. Circulation2011;124:S174–8.
[13] Park GM, Ahn JM, Kim DH, Kang JW, Song JM, Kang DH, Lim TH, Song JK. Distalaortic intramural hematoma: clinical importance of focal contrast enhance-ment on CT images. Radiology 2011;259:100–8.
[14] Williams DM, Cronin P, Dasika N, Upchurch Jr GR, Patel HJ, Deeb MG, AbramsG. Aortic branch artery pseudoaneurysm accompanying aortic dissection. PartI. Pseudoaneurysm anatomy. J Vasc Interv Radiol 2006;17:765–71.
[15] Park KH, Lim C, Choi JH, Sung K, Kim K, Lee YT, Park PW. Prevalence of aorticintimal defect in surgically treated acute type A intramural hematoma. AnnThorac Surg 2008;86:1494–500.
[16] Kitai T, Kaji S, Yamamuro A, Tani T, Kinoshita M, Ehara N, Kobori A, Kita T,Furukawa Y. Impact of new development of ulcer-like projection on clinicaloutcomes in patients with type B aortic dissection with closed and throm-bosed false lumen. Circulation 2010;122:S74–80.
[17] Kaji S, Akasaka T, Katayama M, Yamamuro A, Yamabe K, Tamita K, Akiyama M,Watanabe N, Tanemoto K, Morioka S, Yoshida K. Prognosis of retrogradedissection from the descending to the ascending aorta. Circulation 2003;108(Suppl. 1):II300–06.
[18] Song JK, Kang DH, Lim TH, Song MG, Kim JJ, Park SW, Park SJ. Differentremodeling of descending thoracic aorta after acute event in aortic intramuralhemorrhage versus aortic dissection. Am J Cardiol 1999;83:937–41.
[19] Song JK, Kim HS, Kang DH, Lim TH, Song MG, Park SW, Park SJ. Different clinicalfeatures of aortic intramural hematoma versus dissection involving the as-cending aorta. J Am Coll Cardiol 2001;37:1604–10.
[20] Kaji S, Akasaka T, Horibata Y, Nishigami K, Shono H, Katayama M, Yamamuro A,Morioka S, Morita I, Tanemoto K, Honda T, Yoshida K. Long-term prognosis ofpatients withtype A aortic intramural hematoma.Circulation 2002;106(Suppl. 1):I248–52.
[21] Kaji S, Akasaka T, Katayama M, Yamamuro A, Yamabe K, Tamita K, Akiyama M,Watanabe N, Tanemoto K, Morioka S, Yoshida K. Long-term prognosis of patients
Please cite this article in press as: Song J-K. Update in acute aortic syndisease entities. J Cardiol (2014), http://dx.doi.org/10.1016/j.jjcc.201
with type B aortic intramural hematoma. Circulation 2003;108(Suppl. 1):II307–11.
[22] Evangelista A, Mukherjee D, Mehta RH, O’Gara PT, Fattori R, Cooper JV, SmithDE, Oh JK, Hutchison S, Sechtem U, Isselbacher EM, Nienaber CA, Pape LA, EagleKA, for the International Registry of Aortic Dissection (IRAD) Investigators.Acute intramural hematoma of the aorta: a mystery in evolution. Circulation2005;111:1063–70.
[23] Pelzel JM, Braverman AC, Hirsch AT, Harris KM. International heterogeneity indiagnostic frequency and clinical outcomes of ascending aortic intramuralhematoma. J Am Soc Echocardiogr 2007;20:1260–8.
[24] Kitai T, Kaji S, Yamamuro A, Tani T, Tamita K, Kinoshita M, Ehara N, Kobori A,Nasu M, Okada Y, Furukawa Y. Clinical outcomes of medical therapy andtimely operation in initially diagnosed type A aortic intramural hematoma. A20-year experience. Circulation 2009;120(Suppl. 1):S292–8.
[25] Song JK, Lim JH, Ahn JM, Kim DH, Kang JW, Lee TY, Song JM, Choo SJ, Kang DH,Chung CH, Lee JW, Lim TH. Outcomes of patients with acute type A aorticintramural hematoma. Circulation 2009;120:2046–52.
[26] Harris KM, Braverman AC, Eagle KA, Woznicki EM, Pyeritz RE, Myrmel T,Peterson MD, Voehringer M, Fattori R, Januzzi JL, Gilon D, Montgomery DG,Nienaber CA, Trimarchi S, Isselbacher EM, et al. Acute aortic intramuralhematoma. An analysis from the International Registry of Acute Aortic Dis-section. Circulation 2012;126(Suppl. 1):S91–6.
[27] Estrera A, Miller III C, Lee TY, De Rango P, Abdullah S, Walkes JC, Milewicz D,Safi H. Acute type A intramural hematoma. Analysis of current managementstrategy. Circulation 2009;120(Suppl. 1):S287–91.
[28] Kruse MJ, Johnson PT, Fishman EK, Zimmerman SL. Aortic intramural hema-toma: review of high-risk imaging features. J Cardiovasc Comput Tomogr2013;7:267–72.
[29] Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear withouthematoma: an important variant of aortic dissection that can elude currentimaging techniques. Circulation 1999;99:1331–6.
drome: Intramural hematoma and incomplete dissection as new4.05.005











![Duodenal intramural hematoma due to early postoperative ......Oral anticoagulants such as warfarin are widely used and the most common complication is bleeding.[9] ... (Sao Paulo)](https://img.pdfslide.us/doc/110x75/602fcbba08aab1610f1e229d/duodenal-intramural-hematoma-due-to-early-postoperative-oral-anticoagulants.jpg)



![Rapid Diagnosis and Management of Thoracic Aortic ...€¦ · dissection[3–5]; however, the diagnostic accuracy of bi-plane versus multiplane TEE for aortic dissection and intramural](https://img.pdfslide.us/doc/110x75/5eab1bba8447411721456a13/rapid-diagnosis-and-management-of-thoracic-aortic-dissection3a5-however.jpg)












