Embed Size (px)
DESCRIPTION
los mejores artículos de la psiquiatría psicosomática del 2015
Citation preview

Psychosomatics 2015:56:445–459 & 2015 The Academy of Psychosomatic Medicine. Published by Elsevier Inc. All rights reserved.
Original Research Reports
Updates in Psychosomatic Medicine: 2014
Oliver Freudenreich, M.D., Jeff C. Huffman, M.D., Michael Sharpe, M.D.,Scott R. Beach, M.D., Christopher M. Celano, M.D., Lydia A. Chwastiak, M.D., M.P.H.,
Mary Ann Cohen, M.D., Anne Dickerman, M.D., Mary Joe Fitz-Gerald, M.D.,Nicholas Kontos, M.D., Leena Mittal, M.D., Shamim H. Nejad, M.D., Shehzad Niazi, M.D.,
Marta Novak, M.D., Ph.D., med.habil., Kemuel Philbrick, M.D.,Joseph J. Rasimas, M.D., Ph.D., Jewel Shim, M.D., Scott A. Simpson, M.D., M.P.H.,
Audrey Walker, M.D., Jane Walker, Ph.D., Christina L. Wichman, D.O.,Paula Zimbrean, M.D., Wolfgang Söllner, M.D., Theodore A. Stern, M.D.
Background: The amount of literature published PsychosomaticMedicine in 15 subspecialties to create a
annually related to psychosomatic medicine is vast; thisposes a challenge for practitioners to keep up-to-date inall but a small area of expertise. Objectives: Tointroduce how a group process using volunteer expertscan be harnessed to provide clinicians with a manage-able selection of important publications in psychoso-matic medicine, organized by specialty area, for 2014.Methods: We used quarterly annotated abstractsselected by experts from theAcademy of PsychosomaticMedicine and the European Association ofReceived March 5, 2015; revised March 30, 2015; accepted March 31,2015. From Department of Psychiatry, Massachusetts GeneralHospital, Boston, MA (OF, JCH, SRB, CMC, NK, SHN, TAS);Psychological Medicine Research, Department of Psychiatry, Uni-versity of Oxford, Oxford, UK (MS, JW); Department of Psychiatryand Behavioral Sciences, University of Washington School ofMedicine, Seattle, WA (LAC); Department of Psychiatry, TheIcahn School of Medicine at Mount Sinai, New York, NY(MAC); Department of Psychiatry, Consultation-Liaison Service,New York-Presbyterian Hospital, Weill Cornell Medical College,New York, NY (AD); Department of Psychiatry, Louisiana StateUniversity Health Sciences Center, Shreveport, LA (MJF-G.);Divisions of Medical Psychiatry and Women’s Mental Health,Department of Psychiatry, Brigham and Women’s Hospital, Boston,MA (LM); Department of Psychiatry & Psychology, Mayo Clinic,Jacksonville, FL (SN); Department of Psychiatry, UniversityHealth Network and University of Toronto, Toronto, Canada(MN); Institute of Behavioral Sciences, Semmelweis University,Budapest, Hungary (MN); Department of Psychiatry and
Psychosomatics 56:5, September/October 2015
list of important articles. Results: In 2014, subspecialtyexperts selected 88 articles of interest for practitionersof psychosomatic medicine. For this review, 14 articleswere chosen. Conclusions: A group process can be usedto whittle down the vast literature in psychosomaticmedicine and compile a list of important articles forindividual practitioners. Such an approach is consistentwith the idea of physicians as lifelong learners andeducators.
(Psychosomatics 2015; 56:445–459)
Psychology, Mayo Clinic, Rochester, MN (KP); HealthPartners/Regions Hospital, St. Paul, MN (JJR); Department of Psychiatry,Kaiser Oakland Medical Center and the University of California,San Francisco, San Francisco, CA (JS); Denver Health MedicalCenter, University of Colorado School of Medicine, Denver, CO(SAS); Division of Child and Adolescent Psychiatry, Albert EinsteinCollege of Medicine/Montefiore Medical Center, Bronx, NY (AW);Department of Psychiatry and Behavioral Medicine, MedicalCollege of Wisconsin, Milwaukee, WI (CLW); Department ofPsychiatry and Surgery (Transplant), Yale New Haven Hospital,New Haven, CT (PZ); Department of Psychosomatic Medicineand Psychotherapy, Paracelsus Medical University, NurembergGeneral Hospital, Nuremberg, Germany (WS). Send correspondenceand reprint requests to Oliver Freudenreich, M.D., MGH Schizo-phrenia Program, Erich Lindemann Mental Health Center, 25Staniford Street, Boston, MA 02114; e-mail: [email protected]
& 2015 The Academy of PsychosomaticMedicine. Publishedby Elsevier Inc. All rights reserved.
www.psychosomaticsjournal.org 445

Updates in Psychosomatic Medicine
INTRODUCTION
The sheer amount of literature published each year inmedicine isoverwhelming.Humankind’s collectiveknowl-edge is growing exponentially, andmedical knowledge hasbeen estimated in 2010 to double every 3.5 years and hasbeen projected to double every 73 days by the year 2020.1
The area of psychosomatic medicine or consultation-liaisonpsychiatry isnoexception, and it hasbecomeall butimpossible for practitioners to keep up-to-date on newdevelopments across their field rather than just in a verynarrow area of their expertise. Yet, our patients expect usto remain informed about new developments in medicineand practice based on current knowledge.
To help practitioners of psychosomatic medicinekeep updated (and to maintain their accreditation) theAcademy of Psychosomatic Medicine (APM) in collab-oration with its sister organization the European Asso-ciation of Psychosomatic Medicine (EAPM) establisheda subcommittee of the APM Research and Evidence-Based Practice Committee, to publish annotated quar-terly updates in the field of psychosomaticmedicine. Thisarticle introduces the group process used to canvass theliterature; it provides all references selected by thesubcommittee for 2014; and in addition, it further distillsthe literature related to psychosomatic medicine toprovide an overview of important developments in 2014.
METHODS
Beginning in 2013, the evidence-based practice subcom-mittee of the APM, in collaboration with members fromthe EAPM, began publishing annotated updates ofimportant articles on the APMwebsite (in the Educationsection) quarterly.2 The quarterly updates are accessibleto anyone and not restricted to the APM members. In2014, these quarterly updates covered 15 subspecialties orsections of psychosomatic medicine. Each quarterlyupdate contained up to 3 articles per subspecialty areathat were published during that quarter (Epub ahead ofprint or published in the journal) and were selected by adesignated section expert from the APM or the EAPMwho volunteered to participate in this educationalendeavor in his or her area of expertise. In addition tothe PubMed article abstract, section experts annotatedthe articles using a structured format (Table 1).
For many subspecialty areas, although 1 expertauthor was the designated point person and primary
446 www.psychosomaticsjournal.org
contributing expert, 2 or more authors were respon-sible for canvassing the literature in their assignedtopic area and selecting articles of importance; inaddition, the primary experts were encouraged to useoutside consultants (i.e., colleagues with relevantexpertise) and APM special interest groups for articlesuggestions. Experts were instructed to preferentiallyselect high-quality articles. Consistent with the grad-ing scheme for the critical appraisal of literature thatwas developed by the Oxford Centre for Evidence-based Medicine, we operationalized high-qualityarticles as those that used a randomized controlledtrial design, represented a cohort study, or reported ameta-analysis.3 Table 2 summarizes the selectioncriteria for other types of articles that experts couldinclude in their updates because of high educationalvalue.
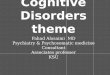
Authors were instructed to limit themselves to 3articles per quarter to avoid an uncritical inclusion ofarticles; if no articles were deemed high quality oreducationally valuable, none were selected for thequarter. For this 2014 update in psychosomaticmedicine, 2 authors (O. F. and T. A. S.) created aconsensus list of articles that they judged to be ofparticular relevance for general practitioners of psy-chosomatic medicine who want to educate themselvesabout major findings in psychosomatic medicine in2014. One of the authors (O. F.) is the chairperson ofthe subcommittee, who in this function had collectedand read all submitted articles and annotations beforeposting on the website; the other author (T. A. S.)functioned as a neutral judge, as he had not beeninvolved in the quarterly updates. For the annualupdate, articles were given preference if they reportedon innovations, investigated a clinical topic usinghigh-quality research methodology, represented con-sensus documents from important medical bodies, oreducated helpfully about an area of psychosomaticmedicine. The number of final articles was not limitedinitially but evolved during the consensus building.The overall process of selecting articles for thequarterly and the annual update is depicted in theFigure.
RESULTS
A total of 88 articles had been selected in 2014 by thecontributing APM/EAPM experts for annotation andpublication on the APM website. The articles were
Psychosomatics 56:5, September/October 2015

TABLE 1. Annotation Format for APM Quarterly Updates
The findingConcise summary of the studyThis should include the (one) main finding in the topic expert'sown words
This should include the population studied, the study designused, and the main outcome variable
Strength and weaknessesComments regarding the appropriateness of the study'smethodology
This should include patient selection and measurement issuessuch as rating scales used
This should include the study's power and generalizability
RelevanceBackground and the larger context of the study that illustrateswhy it is important
This should include applicability for psychosomatic medicine
APM ¼ Academy of Psychosomatic Medicine.
Freudenreich et al.
related to 15 subspecialties: cardiac psychiatry,4–9
collaborative care/integrated behavioral health,10,11
emergency psychiatry,12,13 HIV psychiatry,14–20
neuropsychiatry,21–31 pediatric psychosomatic medi-cine,32–36 psychodermatology,37–45 psychonephrol-ogy,46–55 psycho-oncology and palliative care,56–64
serious mental illness,65–72 somatic symptom disor-ders,73 suicide,74–78 transplant psychiatry,79–85 traumaand critical care psychiatry,86,87 and women’s mentalhealth.11,88–91 In addition, 14 articles with substantialeducational value for general practitioners of psycho-somaticmedicine psychiatrywere selected as describedearlier. The full annotations for those articles (asprovided by the original authors, with some editingfor uniformity) are provided later, and their mainfindings are summarized in Table 3.
TABLE 2. Selection Criteria for Articles Included in the APMQuarterly Updates
High-quality evidenceRandomized, controlled trialCohort studyMeta-analysis
Publications in high-impact journals that practitioners should beaware of
Novel findings or approaches that might change practiceSummary statements or expert guidelines by large organizationsArticles with high educational value
APM ¼ Academy of Psychosomatic Medicine.
Cardiac Psychiatry
Depression As a Risk Factor for Poor Prognosis AmongPatients With Acute Coronary Syndrome: SystematicReview and Recommendations: A Scientific StatementFrom the American Heart Association
Lichtman JH, Froelicher ES, Blumenthal JA, CarneyRM, Doering LV, Frasure-Smith N, et al: Circulation2014; 129:1350–1369
The Finding: Despite moderate heterogeneity ofindividual studies, this comprehensive systematic
Psychosomatics 56:5, September/October 2015
review found clear connections between depressionand adverse outcomes after acute coronary syn-drome (ACS). Based on this review and additionalaspects of this association (e.g., a plausible mecha-nism connecting depression and adverse outcomes),the committee concluded that depression should beconsidered a risk factor for adverse events afterACS.
Strengths andWeaknesses: The strengths includeda careful and comprehensive systematic review andconsideration ofmultiple criteria required to reach riskfactor status. The authors also carefully outlined anddiscussed sources of heterogeneity. The weaknesses ofthe review included incorporation only of articleswritten in English, only considering post-ACS out-comes (rather than onset of cardiac illness or otherconditions), and the inherent limitations and hetero-geneity of the reviewed studies. Regarding the assign-ment as a risk factor, an important weakness was thatthe authors did not include the criterion that treat-ment/reduction of the risk factor leads to improvedprognosis (not yet proven) and that it includes only avery specific condition rather than coronary arterydisease overall.
Relevance: This article may prove controversialfor the reasons listed earlier. However, there is littledoubt that depression is linked with cardiac mortalityafter ACS. Although there has not yet been anadequately powered study proving that treatment ofdepression leads to a reduction inmortality, there havebeen several studies showing that management ofdepression in patients with cardiac disease leads toimproved health-related quality of life and function.Whether one considers depression a “risk factor,” it isclearly important to address in patients post-ACS.
www.psychosomaticsjournal.org 447

APM and EAPM Members
Outside ConsultantsPsychosoma�c Medicine
Topic Area Experts
TOPICAREAS
Cardiopsychiatry
Emergency psych Psychooncology
Transplant psychiatryPsychonephrology
HIV psychiatry
Ped psychosom med
Neuropsychiatry
Trauma
Women’s mental healthSuicide; SSS; SMIPsychodermatology
QUARTERLYUPDATES
(APM Website*)Q1 Q2 Q3 Q4
ANNUALUPDATE
(Psychosoma�cs)
Updates inPsychosoma�c Medicine
FIGURE. APM/EAPM Quarterly and Annual Updates in Psychosomatic Medicine. The 2014 Topic Areas and Article Selection. APM ¼Academy of Psychosomatic Medicine, EAPM ¼ European Association of Psychosomatic Medicine, SSS ¼ Somatic SymptomDisorder, SMI¼SeriousMental Illness. *APMwebsite (education section, annotated abstracts): http://www.apm.org/library/articles/index.shtml.
Updates in Psychosomatic Medicine
HIV Psychiatry
Asymptomatic HIV-Associated NeurocognitiveImpairment Increases Risk for Symptomatic Decline
Grant I, Franklin DR, Jr., Deutsch R, Woods SP,Vaida F, Ellis RJ, et al: Neurology 2014; 82:2055–2062
The Finding: In this longitudinal cohort study(the CHARTER cohort), a diagnosis of “asympto-matic neurocognitive impairment” (ANI) at thebeginning of the study predicted, over a medianfollow-up of 45.2 months, progression to problems ineveryday functioning. Combining self-report andperformance-based measure, the presence of ANIconferred a relative risk (RR) of 3.0 (CI: 2.1–4.4)when compared with patients without impairment atbaseline.
Strength and Weaknesses: This is an importantlongitudinal study (as opposed to a cross-sectional
448 www.psychosomaticsjournal.org
study) with a sufficiently large sample (N ¼ 121) ofpatients diagnosed as having ANI and 226 diagnosedas being cognitively intact. The CHARTER cohort’slongitudinal design might be biased toward thosewho can commit to participating in a longitudinalstudy (i.e., removing people at the extremes offunction: those who work and those who areimpaired).
Relevance: In patients with HIV infection, pre-serving cognition remains elusive for some, in whom,despite seemingly effective HIV treatment, functionalimpairments fromHIV-associated neurocognitive dis-order develop. It is a high priority to develop treatmentstrategies (either new drugs or optimizing currentregimens for central nervous system protection) forpatients who are labeled as having “ANI” (mostpatients withHIV-associated neurocognitive disorder)using the Frascati criteria. In this scheme, ANIindicates measurable cognitive impairment that is
Psychosomatics 56:5, September/October 2015

TABLE 3. Updates in Psychosomatic Medicine 2014: 14 Key Findings
SubspecialtyDomain
Reference No. Major Finding/Relevance
Cardiacpsychiatry
4 The American Heart Association officially concluded that depression should be considereda risk factor for adverse events after an acute coronary syndrome (ACS). Depression inpost-ACS patients is ignored to the detriment of the patient and must be addressed.
HIV psychiatry 17 An asymptomatic form of HIV-associated neurocognitive disorder termed asymptomaticneurocognitive impairment (ANI) increases the risk for cognitive decline that becomessymptomatic. Patients with HIV infection who have ANI have to be identified, andattempts should be made to protect cognition.
18 The old standby first-generation NNRTI antiretroviral agent efavirenz, which is a component ofstandard treatment for HIV infection, is associated with an increased risk of suicidality. Itremains yet to be seen if next-generation NNRTIs have a lower risk for neuropsychiatriccomplications.
Neuropsychiatry 23 Cognitive deficits 6 months after a stroke were common. After a stroke (regardless of location),serial testing including formal neuropsychologic testing where there is a discrepancy betweensubjective complaints and “bedside” screening is needed.
31 A simple bedside test of attention (months of year backward) was both sensitive and specific fordelirium in hospitalized (but not in intensive care) patients. Quality initiatives in hospitalsshould pay attention to this simple test.
Psychodermatol-ogy
39 Psychotropic medications can cause a variety of dermatologic side effects. Consultationpsychiatrists would benefit from this review that details reported reactions for all majormedications and has a small section on treatment and prevention.
Psycho-oncologyand palliativecare
60 The investigators failed to recruit to a placebo-controlled trial for depression in patients withcancer. Given the importance of clinical psychiatric research in medical settings, the experienceof the authors and the discussion are informative for any C-L psychiatrist who works inacademic settings or who considers conducting a clinical trial in a medical setting.
63 Patients with cancer with major depression had substantially greater improvement in depressionwhen treated withmanualized depression care when comparedwith usual treatment. This large,randomized effectiveness trial convincingly showed the power of intensive and integratedcollaborative care to address depression in patients with cancer. Such coordinated andinterdisciplinary treatment sets the standard for care.
Serious mentalillness
68 Patients with serious mental illness admitted for diabetes had an increased risk for (a costly) earlyrehospitalization. This finding points to need for better coordinated and integrated medical-psychiatry care for patients with serious mental illness and diabetes.
Suicide 75 A 41-year longitudinal study established traumatic brain injury as a risk factor for suicide (andalso for other violent deaths). This is an important clinical finding that clinicians should keep inmindwhen assessing post-TBI patients, be it returning veterans, people with sports-related headinjuries, or other groups where head injuries are likely (e.g., patients who are homeless).
76 The US Preventive Services Task Force concluded that there was no clear evidence for benefitfrom routinely screening asymptomatic primary care patients for suicide risk. This is animportant reminder that indiscriminant, broad screening (in this case for suicidality) can lead towasted resources with little to show for it.
Transplantpsychiatry
80 In this prospective study, cognitive decline developed in patients after liver transplantation eventhough hepatic encephalopathy resolved after transplantation. Not all cognitive dysfunctionseen in patients after liver transplantation is thus explained by hepatic encephalopathy.
Trauma andcritical carepsychiatry
86 This randomized trial found ramelteon to be an effective prevention of delirium in hospitalizedpatients. Replication is needed before ramelteon can become standard delirium prophylaxis.Whether ramelteon is safer and more effective than melatonin in this setting is also unknown.
Women's mentalhealth
90 In this cohort study, antidepressants were not associated with an increased risk for cardiacmalformations once cofounders (e.g., depression severity) were taken into account. This studyadds to the large body of literature suggesting that either antidepressants are not teratogenic orthe absolute risk is very low.
C-L ¼ consultation liaison; NNRTI ¼ non–nucleoside reverse transcriptase inhibitors; traumatic brain injury.
Freudenreich et al.
Psychosomatics 56:5, September/October 2015 www.psychosomaticsjournal.org 449

Updates in Psychosomatic Medicine
clinically silent and has no functional relevance. Thereis still value in diagnosing ANI: “Asymptomatic”might not sound alarming but, as shown in the study, itis a risk factor for cognitive deterioration, and thosepatients need to be identified even when they are“asymptomatic.”
Association Between Efavirenz as Initial Therapy forHIV-1 Infection and Increased Risk for SuicidalIdeation or Attempted or Completed Suicide: AnAnalysis of Trial Data
Mollan KR, Smurzynski M, Eron JJ, Daar ES,Campbell TB, Sax PE, et al: Ann Intern Med 2014;161:1–10
The Finding: Using data from 4 AIDS ClinicalTrials Group studies of treatment-naive patients withHIV infection who were started with treatment onrandomized antiretroviral treatment regimens, it wasfound that the risk of suicidality (defined as suicidalideation or attempted or completed suicide) was twiceas high for patients randomly assigned to an efavirenz-containing regimen when compared with thoseassigned to efavirenz-free regimens. Of the observed9 suicides, 8 were in the efavirenz group.
Strength and Weaknesses: This is the first analysisusing data about suicidality from random assignmentto treatment regimens with or without efavirenz. Still,3 of the 4 trials were open label; with suicide alreadylisted in the prescribing information as a complication,reporting bias is possible. In addition, suicidality wasnot assessed with a standard rating scale, and patientswho were deemed to be at a higher risk for suicidalitymight not have been referred to these 4 trials to beginwith. Finally, efavirenz was not compared withregimens containing other non–nucleoside reversetranscriptase inhibitors or integrase inhibitors.
Relevance: The non–nucleoside reverse transcrip-tase inhibitors efavirenz (Sustiva) has been an impor-tant cornerstone medication for the treatment ofHIV/AIDS because of its excellent antiretroviralefficacy. It is also included in the most widely usedsingle-pill regimen (Atripla). However, its use hasalways been complicated by a higher rate of neuro-psychiatric side effects and by anecdotal observationsof serious events (such as thoughts of suicide). Thisanalysis, using data from randomized trials, providesthe best evidence yet that these clinical observationsare true and that there is some risk of suicidal
450 www.psychosomaticsjournal.org
thinking (and death from suicide) owing to use ofefavirenz. Thus, careful clinical monitoring for psy-chiatric problems is needed for patients starting withthe treatment with efavirenz. It remains yet to be seenif next-generation non–nucleoside reverse transcrip-tase inhibitorss have a lower risk for neuropsychiatriccomplications.
Neuropsychiatry
The Cognitive Burden of Stroke Emerges EvenWith anIntact National Institutes ofHealth Stroke Scale Score:A Cohort Study
Kauranen T, Laari S, Turunen K, Mustanoja S,Baumann P, Poutiainen E: J Neurol NeurosurgPsychiatry 2014; 85:295–299
The Finding: Cognitive deficits at 6 months afterstroke (without regard for localization) were commonin a working-age cohort. Further, a screening instru-ment used at the time of discharge was of limited use inpredicting this.
Strengths and Weaknesses: Strict definitions forcognitive impairment were used; along with therelatively young sample, this makes the study’s find-ings striking. However, the baseline cognitive status ofthe patients was unknown, and although presumed tobe buoyed by age, relative youth plus stroke suggestsunfavorable CNS vasculopathy burden; thus, mitigat-ing assumptions about baseline cognition.
Relevance: This study highlights the need forserial cognitive screening in persons with acute,subacute, and remote stroke. The importance offormal neuropsychologic testing when subjectivefunctioning and “bedside” screening are incongruentis suggested.
Attention! A Good Bedside Test for Delirium?
O’Regan NA, Ryan DJ, Boland E, Connolly W,McGlade C, Leonard M, et al: J Neurol NeurosurgPsychiatry 2014; 85:1122–1131
The Finding: Simple attention screening (monthsof year backward) is a sensitive and surprisinglyspecific detector of delirium in hospitalized (non-intensive care) populations. It is enhanced by combin-ing it with screens for subjective confusion or avisuospatial attention task or both.
Strengths andWeaknesses: This article highlightedthe continued problems that exist in delirium detection
Psychosomatics 56:5, September/October 2015

Freudenreich et al.
in the general hospital setting, reviewed proposedremedies, and made a convincing argument for amuch simpler solution than has been proffered pre-viously. The study design was ambitious (all assess-ments of the 4200 patients took place on the sameday; this included screening followed by a secondscreening with the Confusion Assessment Method,followed by psychiatric assessment) but it appears tohave been carried out rigorously. The authors did anexcellent job of identifying the potential limitingfactors of the study. The biggest quibble is thatattention is far from a specific delirium finding andprobably ought not be taken as such in a cross-sectional assessment. However, as noted by theauthors, very, very few patients with documenteddementia in this study did not have delirium. The factthat patients with cognitive impairment were moresusceptible to delirium may have mitigated the usualinsensitivity of attention impairment as a diagnosticscreen. In addition, technically, months of the yearbackward is not a pure test of attention, as it usesworking memory as well.
Relevance: Delirium detection in the generalhospital remains poor and is often thought to requiresignificant investment in time and effort. This articlemay have quality improvement implications as itoffers a straightforward and brief bedside method ofdetecting delirium.
Psychodermatology
Dermatologic Side Effects of PsychotropicMedications
Mitkov MV, Trowbridge RM, Lockshin BN,Caplan JP: Psychosomatics 2014; 55:1–20
The Finding: The authors presented a broadoverview of the most common dermatologic sideeffects associated with psychotropic medications. Ingeneral, dermatologic symptoms are most commonlyassociated with antiepileptic medications; the mostserious dermatologic adverse effects are also due tothis class of medications. The authors described themost common dermatologic conditions, their onsetand clinical course, risk factors for cutaneous drugreactions, as well as recommendations on how todiagnose these problems.
Strengths and Weaknesses: The primary strengthof this article was that it presented a comprehensive
Psychosomatics 56:5, September/October 2015
overview of the most common dermatologic sideeffects of psychotropic medication and served as goodresource for psychiatrists for information and guid-ance on recognition, diagnosis, and evaluation of theseconditions. A weakness was that a significant amountof the data on cutaneous drug reactions and psycho-tropic medications were based on case reports orretrospective data, which limited the quality of theevidence.
Relevance: Dermatologic side effects are notuncommonly associated with psychotropic medica-tions, and it is important for practitioners of psycho-somatic medicine to be aware of the potential fordermatologic adverse effects, particularly with certainmedications (i.e., mood stabilizers) and in higher riskgroups. Risk mitigation is already possible for somemedications (e.g., HLA genotyping before carbama-zepine use).
Psycho-Oncology and Palliative Care
Conducting an Antidepressant Clinical Trial inOncology: Challenges and Strategies to Address Them
Park EM, Raddin RS, Nelson KM, Hamer RM,Mayer DK, Bernard SA, et al: Gen Hosp Psychiatry2014; 36:474–476
The Finding: The researchers planned a 4-armclinical trial to compare the efficacy of citalopramwithplacebo and mirtazapine with placebo for depressedpatients with cancer (participants were to be stratifiedaccording to their symptom profile). They were unableto recruit any participants and, after removing theplacebo arms, were still unable to recruit sufficientnumbers. They described the reasons for poor recruit-ment (summarized in 4 categories: diagnostic ambi-guity, participant recruitment and retention, practicalbarriers, and placebo concerns) and the possiblesolutions.
Strengths and Weaknesses: This article’s strengthwas that it was one of only a few that described thepractical aspects of conducting a real clinical researchstudy in psycho-oncology. Its weakness was that theresearchers were not able to put their potentialsolutions to the test.
Relevance: This description of the challengesof doing clinical research in psychiatry in a medi-cal setting is relevant to all consultation-liaisonpsychiatrists.
www.psychosomaticsjournal.org 451

Updates in Psychosomatic Medicine
Integrated Collaborative Care for Comorbid MajorDepression in Patients With Cancer (SMaRTOncology-2): A Multicentre Randomised ControlledEffectiveness Trial
Sharpe M, Walker J, Holm Hansen C, Martin P,Symeonides S, Gourley C, et al: Lancet 2014;384:1099–1108
The Finding: An integrated, systematic, multi-component collaborative care–based treatment pro-gram for major depression was significantly betterthan usual care in achieving a treatment response inpatients with cancer. The treatment program wasrelatively inexpensive.
Strengths and Weaknesses: The strengths of thistrial included its rigorous methods, recruitment byscreening, and high follow-up rate. The main weak-ness was that, as is usually the case with such trials, theparticipants could not be masked to interventionallocation.
Relevance: The findings suggested that systematicand intensive integrated collaborative care treatmentprograms could achieve striking results for patientswith comorbid depression.
Serious Mental Illness
The Effect of Serious Mental Illness on the Risk ofRehospitalization Among Patients With Diabetes
Chwastiak LA,DavydowDS,McKibbinCL, SchurE, Burley M, McDonell MG, et al: Psychosomatics2014; 55:134–143
The Finding: AmongMedicare beneficiaries, reho-spitalization within 30 days of discharge occurs inalmost 20% of patients, costing the health care systeman estimated $17.4 billion. A key component of thecomprehensive strategy of the Centers for Medicareand Medicaid Services to reduce costs focuses onreducing 30-day rehospitalizations for heart failure,acute myocardial infarction, and pneumonia. In thisstudy, of all admissions to community hospitals inWashington State for diabetes between 2010 and 2011,a diagnosis of serious mental illness was independentlyassociated with an increased risk of early medicalrehospitalization.
Strength and Weaknesses: This observationalcohort study comprised a very large (82,060 adultsin Washington State), population-based sample ofpatients who had a medical-surgical hospitalization
452 www.psychosomaticsjournal.org
between 2010 and 2011 with any discharge diagnosisindicating diabetes mellitus. The study sample wasrepresentative of patients in Washington State withdiabetes, as data were obtained from all communityhospitals in the state. The study limitations wererelated to the use of administrative data. First, theremay have been misclassification of patients withserious mental illness disorders, resulting in theirinclusion in the reference group. Moreover, theadministrative data set used for these analyses didnot include information about health behaviors (suchas smoking, sedentary lifestyle, and poor diet) orlaboratory or pharmacy data—so the effect of theseimportant factors could not be evaluated.
Relevance: These findings may indicate poorquality of medical care for patients with diabeteswho also have comorbid serious mental illness, ormaybe further evidence that patients with seriousmental illness interact with the health care systemdifferently, and have unique barriers to adherencewithmedical care and follow-up. Improving the coordina-tion or integration of outpatient medical and psychi-atric care for these complex patients may decrease therisk of early rehospitalizations.
Suicide
Suicide, Fatal Injuries, and Other Causes of PrematureMortality in Patients With Traumatic Brain Injury: A41-Year Swedish Population Study
Fazel S,WolfA,PillasD,LichtensteinP,LangstromN:JAMA Psychiatry 2014; 71:326–333
The Finding: Drawing on an extended longitudinalfollow-up (4 to 440 y) of more than 218,000 Swedishindividuals who had a traumatic brain injury (TBI),this study showed that people who survived 6 monthsor more beyond a TBI were 3 times more likely to dieprematurely of suicide, assault, or other injuries. Ofparticular interest to psychiatrists, post-TBI patientswere twice as likely to die of suicide as compared withtheir uninjured siblings.
Strengths and Weaknesses: This study relied onimpressive numbers and on extensive longitudinaldata, taking advantage of comprehensive nationwidepopulation-based registers in Sweden that alsoallowed for comparison with general populationcontrols and a substantial number (4237,000) ofuninjured siblings; this extensive database enabled
Psychosomatics 56:5, September/October 2015

Freudenreich et al.
uncommon statistical power to examine relativelyinfrequent events. Unfortunately, the study was notable to either specify the type of TBI or quantify theseverity of the TBI.
Relevance: This study underscored the utility ofregarding post-TBI patients as having chronic medicalproblems that deserve ongoing attention, perhapsparticularly those who are also prone to impulsivity,risk-taking behaviors, or substance abuse. Returningveterans, youth involved in contact sports, and indi-viduals who live in environments where assaults weremore common comprised a population that was at anincreased risk of having a TBI and may invitepsychiatric attention when they pursue medicalattention.
Screening for Suicide Risk in Adolescents, Adults, andOlder Adults in Primary Care: U.S. Preventive ServicesTask Force Recommendation Statement
LeFevre ML: Ann Intern Med 2014; 160:719–726The Finding: Although the United States Preven-
tive Services Task Force recommended that primarycare clinicians should remain attentive to screeningpatients in high-risk groups (such as immediatelyfollowing dismissal from an emergency departmentvisit for a suicidal act or following a psychiatrichospitalization), there was insufficient evidence ofbenefit to support routine screening for suicide riskin primary care. The American Academy of FamilyPhysicians and the Canadian Task Force on Preven-tive Health Care reached similar conclusions. TheUnited States Preventive Services Task Force contin-ues to support screening for depression in primarycare, provided such screening is coupled with adequateresources to ensure accurate diagnosis, treatment, andfollow-up. However, the United States PreventiveServices Task Force concluded that there was no clearevidence that screening for suicide risk in asympto-matic primary care patients yielded improved healthoutcomes.
Strengths and Weaknesses: Given that suicide wasthe 10th leading cause of death in the United States in2010, this update of the 2004 United States PreventiveServices Task Force recommendations is timely.Unfortunately, available studies for review weresparse, the accuracy of the screening instruments usedvaried widely, and no 2 studies used the sameinstrument.
Psychosomatics 56:5, September/October 2015
Relevance: Recent emphases on patient safety andthe recognition of the potential adverse effects ofdepression in select groups of medical and surgicalpatients have increased the attention given to suicidescreening in and out of the hospital. Awareness of thepaucity of evidence for benefit from routine screeningfor suicide risk in primary care patients may enableconsultation psychiatrists to inform these efforts, suchthat the energy and work invested are directed towardhigh-risk individuals where intervention may favor-ably influence outcome.
Transplant Psychiatry
New-Onset Cognitive Dysfunction Impairs the Qualityof Life in Patients After Liver Transplantation
Tryc AB, PflugradH, Goldbecker A, Barg-HockH,Strassburg CP, Hecker H, et al: Liver Transpl 2014;20:807–814
The Finding: A total of 50 patients were inves-tigated prospectively before orthotopic liver trans-plantation (OLT), at 6 months, and at 12 monthsafter OLT. A battery of psychometric tests was used:the psychometric hepatic encephalopathy score, theinhibitory control test, the critical flicker frequency,and the Repeatable Battery for the Assessment ofNeuropsychological Status. The hepatic encephal-opathy group performed significantly worse on alltests in comparison with the nonhepatic encephal-opathy group before OLT (psychometric hepaticencephalopathy score, p o 0.01; inhibitory controltest, p o 0.04; and critical flicker frequency, p o0.01). At 6 months after OLT, the hepatic encephal-opathy group still had lower mean scores for criticalflicker frequency (p o 0.04) and psychometrichepatic encephalopathy score (p o 0.09) in compar-ison with the nonhepatic encephalopathy group. Overtime, the patients in the hepatic encephalopathygroup improved on the Repeatable Battery for theAssessment of Neuropsychological Status (T1 vsT3, p o 0.06), whereas a cognitive decline wasmeasured with Repeatable Battery for the Assess-ment of Neuropsychological Status for the non-hepatic encephalopathy group (T1 vs T2, p o 0.02,and T1 vs T3, po 0.02). At 12 months after OLT, nosignificant differences between the groups weredetectable. Approximately 70% of the patientsshowed a decline in cognition, exceeding 10% in
www.psychosomaticsjournal.org 453

Updates in Psychosomatic Medicine
at least one cognitive domain. Hepatic encephalop-athy–related cognitive dysfunction was mostlyresolved within the first 6 months after OLT, andno patient was diagnosed with minimal hepaticencephalopathy according to psychometric hepaticencephalopathy score and inhibitory control testtargets 12 months after OLT.
Strength and Weaknesses: The strengths of thestudy involved its prospective design, extensive cognitivebattery, and length of follow-up (12 mo). All patientsreceived a standard triple-immunosuppression regimenafter OLT, which took away 1 possible confoundingfactor. The main limitation of the study was its lack ofinformation about the possible causes of cognitivedecline posttransplantation.
Relevance: This study addressed the importanttopic of cognitive impairment after liver transplanta-tion. Patients with liver transplant often have cognitiveimpairment related to hepatic encephalopathy whileon the transplant waiting list; however, they often havesignificant risk factors for other cognitive disorders:long history of alcohol abuse, cardiovascular disease,medications, and age. Differentiating reversible fromprogressive cognitive decline before and after livertransplantation is often extremely difficult. This studybrings valuable information regarding the evolution ofthe hepatic encephalopathy after liver transplantationand raises attention to the cognitive decline posttrans-plantation, which is not related to hepatic encephal-opathy. The findings of the study suggested that 1 yearafter OLT, cognitive dysfunctions should not beinterpreted as residual symptoms but instead beviewed as new-onset cognitive disturbances.
Trauma and Critical Care Psychiatry
Preventative Effects of Ramelteon on Delirium: ARandomized Placebo-Controlled Trial
HattaK,Kishi Y,WadaK,Takeuchi T,Odawara T,Usui C, et al: JAMA Psychiatry 2014; 71:397–403
The Finding: In a randomized rater-blinded pla-cebo-controlled trial thatwas conducted in 4 universityhospitals and 1 general hospital involving 67 patients(24 patients in intensive care units and 43 admitted toregular acute care wards) between the ages of 65 and89 years, ramelteon was associated with a lower risk ofdelirium (3% vs 32%; p ¼ 0.003). After risk factorswere controlled for, ramelteonwas still associatedwith
454 www.psychosomaticsjournal.org
a lower incidence of delirium (p ¼ 0.01; odds ratio ¼0.07 [95% CI: 0.008–0.54].
Strength and Weaknesses: The primary strength ofthis study was its randomized, placebo-controlled design.Despite a relatively low number of patients in the trial,both the groups were reasonably similar concerning riskfactors for development of delirium.The limitations of thestudy included that this was not a double-blind study butwas rater-blinded. In addition, although the number ofpatients enrolled was more than that needed for poweranalysis, the study had a relatively small sample size.Other weaknesses include the exclusion of patients withhepatic dysfunction, diagnoses ofmooddisorders (includ-ingbipolarmooddisorderanddepression), and thosewithpsychotic disorders. These groups represented not onlythose patientswhooften have sleep/wake dysfunction andcircadian rhythm disturbances but also those who havealso been shown to be at a higher risk for the developmentofdeliriumin the intensive careunit setting; their exclusionfrom the study deviates from real clinical practice.
Relevance: During the last several years, varyingstrategies regarding delirium prevention, particularly inintensive care unit patients, have been studied, includinguse of dopamine antagonists, cholinesterase inhibitors,and even benzodiazepines, all with varying results. Thisparticular study, despite its limitations, was one that isthe first to show a significant prophylactic effect on theincidence of delirium in elderly intensive care unitpatients with the use of the melatonin analogue ramel-teon. Interestingly, no published studies exist to show iframelteon is more effective (or if more safe) thanmelatonin is in clinical trials with human subjects.
Women’s Mental Health
Antidepressant Use in Pregnancy and the Risk ofCardiac Defects
Huybrechts KF, Palmsten K, Avorn J, Cohen LS,Holmes LB, Franklin JM, et al: N Engl J Med 2014;370:2397–2407
The Finding: This cohort study of 64,389 womennested within a large population-based cohort study ofwomen enrolled in the nationwide Medicaid AnalyticeXtract found no substantial increase in risk of cardiacmalformations in infants of women with depressionwho use antidepressants (selective serotonin reuptakeinhibitors, serotonin-norepinephrine reuptake inhibi-tors, bupropion, and tricyclic antidepressants) in the
Psychosomatics 56:5, September/October 2015

Freudenreich et al.
first trimester when compared with women withdepression without antidepressant use. This associa-tion was further attenuated by adjusting for a varietyof factors including severity of depression, otherindications for antidepressant use, sociodemographicfactors, and health care use factors. In the unadjustedanalysis, the RR of any cardiac defect with the useof a selective serotonin reuptake inhibitor was 1.25(CI: 1.13–1.38). However, these findings were attenu-ated by adjustment for women with depression only(RR¼ 1.12, with CI: 1.00–1.26) and a cohort that wasfully adjusted for depression, depression severity, andother confounders (RR ¼ 1.06; 95% CI: 0.93–1.22).
Strength and Weaknesses: The strengths of thisstudy included its large sample size within a nationaldatabase of Medicaid enrollees with the ability to linkmaternal and infant records as well as the use ofpropensity score matching to adjust for a large set ofpotential confounders. All major antidepressants wereincluded. Additionally, this study controlled for thepresence and severity of depression. Although epide-miologic studies have often been challenged by defin-ing exposure and the timing of that exposure duringpregnancy, these investigators enlisted secondaryanalyses limiting exposure to the first trimester andrequired women to have a filled prescription or refilledprescription that did not alter the findings substan-tially. The findings were further bolstered by thereplication of prior reports’ findings of associationsbetween well-known risk factors for cardiac malfor-mation, such as diabetes, use of anticonvulsant, andmultifetal pregnancy.
Some of the limitations of this study included itsuse of aMedicaid population that is younger andmoreracially diverse than populations in prior studies were,though the authors found no effect related to age orrace. The data also included only live births, thusexcluding pregnancies resulting in stillbirth, termina-tion, or spontaneous abortion that could have been theresult of more severe cardiac malformation. Addi-tionally, the information on important lifestyle factors(such as smoking, alcohol use, and obesity) was limitedor absent.
Relevance: The use of psychotropics, especiallyantidepressants, during pregnancy is still the focus ofmuch scrutiny. Additionally, the role of untreated orunremitted symptoms of mental illness on pregnancyoutcomes and infant outcomes has a growing body ofliterature. The decision about whether to initiate or
Psychosomatics 56:5, September/October 2015
continue treatment with an antidepressant duringpregnancy should be made with careful consider-ation that balances the risk of that medication withthe risk of the untreated symptoms, and this studyadds to this discussion by carefully analyzing therisks of cardiac malformation associated with anti-depressants.
This study calls into question previous findingsfrom earlier epidemiologic studies that implicatedparoxetine with a higher risk of right ventricularoutflow tract obstructions in infants exposed in utero,which resulted in the Food and Drug Administrationeventually reclassifying the drug to Category D.Similarly, sertraline, one of the most commonlyprescribed selective serotonin reuptake inhibitors usedin pregnancy, was previously associated with ventric-ular septal defects. Given the increasing prevalence ofantidepressant use (among other psychotropics) dur-ing pregnancy, this study adds to the large body ofliterature suggesting low absolute and RR of anti-depressant use during pregnancy and specificallyargued against teratogenic effects associated withcommon antidepressants.
CONCLUSION
A concerted effort by members of the APM and theEAPM identified important findings in psychosomaticmedicine that should be of interest for all psychoso-matic medicine psychiatrists, even if some content liesoutside the main thrust of the consultative work forindividual practitioners. The group process for can-vassing the vast medical literature and creating anno-tated versions of relevant articles by experts (furthercondensed in our list of 14 key findings for 2014) is oneapproach to synthesize medical information. Theutility is 2-fold: one, clinicians and experts alikeremain engaged as students and life-long learnersand two, experts function as peer educators and servean important professional function.
The strengths of our selection approach lies in agroup effort by experts to find the most relevantarticles. Our approach for selecting the quarterlyupdate articles also had weaknesses. Although thework group covered many topics in psychosomaticmedicine, not all topics were covered (e.g., gastro-enterology and hepatology; chronic pain), and theselection of only a few articles favors small areas ofpsychosomatic medicine (HIV psychiatry) over larger
www.psychosomaticsjournal.org 455

Updates in Psychosomatic Medicine
areas (e.g., cardiopsychiatry) that are underrepre-sented. However, articles were also selected basedon quality, and some areas did not have high-qualitypublications this past year and were noncompetitive.Further, even though key principles of article selectionwere outlined, the experts had leeway in making theirultimate article selections, and some selections mayappear idiosyncratic. Last, limiting the number ofselected articles per quarter to 3 main articles forcedexperts to make choices.
In addition, any attempt to further reduce thenumber of relevant articles to 14 in this review for thewhole field would omit some articles that could veryreasonably have been considered. Our final selectionattempts to provide practitioners of psychosomaticmedicine with articles that capture current trends inthe various subspecialties and practical articles to informtheir clinical practice and help prepare for boardexaminations. Still, although our approach is not thebest or only approach, it is a possible approach that usesa group process and the wisdom of a group of experts tomake lifelong learning possible as a physician. TheAPM’s approach of eliciting quarterly, annotatedupdates from area experts could in principle be adoptedby groups of clinicians (at a hospital or practice or
456 www.psychosomaticsjournal.org
organization) who come together voluntarily and divvyup the literature. Without an attempt to synthesize theliterature, individual clinicianswould drown in the sea ofinformation.This groupof cliniciansplans on continuingthe quarterly updates and make the annual updates aregular feature in psychosomatics.
Acknowledgment: We would like to thank otherAPM and EAPM members who have contributedarticles for consideration but who were not listed asauthors. We particularly want to thank APM’s webperson Grace Bachmann who developed the overalllayout for the web-based updates and who carefullyread, edited, and put the abstracts and annotations onthe APM website each quarter.
Disclosure: Oliver Freudenreich has received grantsupport from Psychogenics and Forum, has receivedhonoraria from Global Medical Education and theMGH Psychiatry Academy, has received consultantfees from Beacon Health Strategies and OptimalMedicine, and has received royalties from UpToDate.Theodore A. Stern is an employee of the Academy ofPsychosomatic Medicine for serving as the editor inchief of Psychosomatics. The other authors had nodisclosures.
References
1. Densen P: Challenges and opportunities facing medicaleducation. Trans Am Clin Climatol Assoc 2011; 122:48–58
2. Academy of Psychosomatic Medicine. Available fromhttp://www.apm.org/library/articles/index.shtml. Accessedon 3/30/15
3. Oxford Centre for Evidence-based Medicine. Availablefrom: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/. Accessed on 3/30/15
4. Lichtman JH, Froelicher ES, Blumenthal JA, et al: Depres-sion as a risk factor for poor prognosis among patients withacute coronary syndrome: systematic review and recom-mendations: a scientific statement from the AmericanHeartAssociation. Circulation 2014; 129:1350–1369
5. EdmondsonD,Kronish IM,WassonLT,Giglio JF,DavidsonKW, Whang W: A test of the diathesis-stress model in theemergency department: who develops PTSD after an acutecoronary syndrome? J Psychiatr Res 2014; 53:8–13
6. Mastenbroek MH, Versteeg H, Jordaens L, Theuns DA,Pedersen SS: Ventricular tachyarrhythmias andmortality inpatients with an implantable cardioverter defibrillator:impact of depression in the MIDAS cohort. PsychosomMed 2014; 76:58–65
7. Donohue JM, Belnap BH, Men A, et al: Twelve-monthcost-effectiveness of telephone-delivered collaborative
care for treating depression following CABG surgery: arandomized controlled trial. Gen Hosp Psychiatry 2014;36:453–459
8. Ye S, Shaffer JA, Rieckmann N, et al: Long-termoutcomes of enhanced depression treatment in patientswith acute coronary syndromes. Am J Med 2014; 127:1012–1016
9. Kessing D, Pelle AJ, Kupper N, Szabo BM, Denollet J:Positive affect, anhedonia, and compliance with self-care inpatients with chronic heart failure. J Psychosom Res 2014;77:296–301
10. Katon W, Russo J, Reed SD, et al: A randomized trial ofcollaborative depression care in obstetrics and gynecologyclinics: socioeconomic disadvantage and treatment response.Am J Psychiatry 2015; 172:32–40
11. Melville JL, Reed SD, Russo J, et al: Improving care fordepression in obstetrics and gynecology: a randomizedcontrolled trial. Obstet Gynecol 2014; 123:1237–1246
12. McCullumsmithC, Clark B, Blair C, CropseyK, SheltonR:Rapid follow-up for patients after psychiatric crisis. Com-munity Ment Health J 2015; 51:139–144
13. Buswell M, Lumbard P, Prothero L, et al: Unplanned,urgent and emergency care: what are the roles that EMSplays in providing for older people with dementia? An
Psychosomatics 56:5, September/October 2015

Freudenreich et al.
integrative review of policy, professional recommendationsand evidence Emerg Med J 2014 [Epub ahead of print]
14. BlankMB,HimelhochSS,BalajiAB, et al: Amultisite studyof the prevalence of HIV with rapid testing in mental healthsettings. Am J Public Health 2014; 104:2377–2384
15. Parker R, Stein DJ, Jelsma J: Pain in people living withHIV/AIDS: a systematic review. J Int AIDS Soc 2014;17:18719
16. Ferrara M, Umlauf A, Sanders C, et al: The concomitantuse of second-generation antipsychotics and long-termantiretroviral therapy may be associated with increasedcardiovascular risk. Psychiatry Res 2014; 218:201–208
17. Grant I, Franklin DR Jr., Deutsch R, et al: AsymptomaticHIV-associated neurocognitive impairment increases riskfor symptomatic decline. Neurology 2014; 82:2055–2062
18. Mollan KR, Smurzynski M, Eron JJ, et al: Associationbetween efavirenz as initial therapy for HIV-1 infection andincreased risk for suicidal ideation or attempted or com-pleted suicide: an analysis of trial data. Ann Intern Med2014; 161:1–10
19. Caniglia EC, Cain LE, Justice A, et al: Antiretroviralpenetration into the CNS and incidence of AIDS-definingneurologic conditions. Neurology 2014; 83:134–141
20. Mugavero MJ, Westfall AO, Cole SR, et al: Beyond coreindicators of retention in HIV care: missed clinic visits areindependently associated with all-cause mortality. ClinInfect Dis 2014; 59:1471–1479
21. Marin RS, Gorovoy IR: Echothymia: environmentaldependency in the affective domain. J NeuropsychiatryClin Neurosci 2014; 26:92–96
22. Cagnie B, Coppieters I, Denecker S, Six J, Danneels L,Meeus M: Central sensitization in fibromyalgia? A system-atic review on structural and functional brain MRI SeminArthritis Rheum 2014; 44:68–75
23. Kauranen T, Laari S, Turunen K, Mustanoja S, BaumannP, Poutiainen E: The cognitive burden of stroke emergeseven with an intact NIH Stroke Scale Score: a cohort study.J Neurol Neurosurg Psychiatry 2014; 85:295–299
24. NowrangiMA, Lyketsos C, Rao V,Munro CA: Systematicreview of neuroimaging correlates of executive functioning:converging evidence from different clinical populations.J Neuropsychiatry Clin Neurosci 2014; 26:114–125
25. Hoepner R, LabuddaK,May TW, SchondienstM, Bien CG,Brandt C: Distinguishing between patients with pure psycho-genic nonepileptic seizures and those with comorbid epilepsyby means of clinical data. Epilepsy Behav 2014; 35:54–58
26. Nixon NL, Liddle PF, Nixon E, Worwood G, Liotti M,Palaniyappan L: Biological vulnerability to depression:linked structural and functional brain network findings.Br J Psychiatry 2014; 204:283–289
27. Caceda R, Nemeroff CB, Harvey PD: Toward an under-standing of decision making in severe mental illness.J Neuropsychiatry Clin Neurosci 2014; 26:196–213
28. LaFrance WC Jr, Baird GL, Barry JJ, et al: Multicenterpilot treatment trial for psychogenic nonepileptic seizures: arandomized clinical trial. JAMA Psychiatry 2014; 71:997–1005
Psychosomatics 56:5, September/October 2015
29. Okun MS: Deep-brain stimulation—entering the era ofhuman neural-network modulation. N Engl J Med 2014;371:1369–1373
30. Demartini B, Petrochilos P, Ricciardi L, Price G, EdwardsMJ, Joyce E: The role of alexithymia in the development offunctional motor symptoms (conversion disorder). J NeurolNeurosurg Psychiatry 2014; 85:1132–1137
31. O’ReganNA, RyanDJ, Boland E, et al: Attention! A goodbedside test for delirium? J Neurol Neurosurg Psychiatry2014; 85:1122–1131
32. Kunin-Batson A, Kadan-Lottick N, Neglia JP: The con-tribution of neurocognitive functioning to quality of lifeafter childhood acute lymphoblastic leukemia. Psychoon-cology 2014; 23:692–699
33. Smith BA,Cogswell A,GarciaG:VitaminDand depressivesymptoms in children with cystic fibrosis. Psychosomatics2014; 55:76–81
34. Reddick WE, Taghipour DJ, Glass JO, et al: Prognosticfactors that increase the risk for reduced white mattervolumes and deficits in attention and learning for survivorsof childhood cancers. Pediatr Blood Cancer 2014; 61:1074–1079
35. Reilly C, Atkinson P, Das KB, et al: Neurobehavioralcomorbidities in children with active epilepsy: a population-based study. Pediatrics 2014; 133:e1586–e1593
36. Szigethy E, Bujoreanu SI, Youk AO, et al: Randomizedefficacy trial of two psychotherapies for depression in youthwith inflammatory bowel disease. J AmAcadChildAdolescPsychiatry 2014; 53:726–735
37. Grant JE, Odlaug BL, Schreiber LR, Kim SW: The opiateantagonist, naltrexone, in the treatment of trichotillomania:results of a double-blind, placebo-controlled study. J ClinPsychopharmacol 2014; 34:134–138
38. Gupta MA, Gupta AK, Vujcic B: Increased frequency ofAttention Deficit Hyperactivity Disorder (ADHD) in acneversus dermatologic controls: analysis of an epidemiologicdatabase from theUS. JDermatologTreat 2014; 25:115–118
39. Mitkov MV, Trowbridge RM, Lockshin BN, Caplan JP:Dermatologic side effects of psychotropic medications.Psychosomatics 2014; 55:1–20
40. Wu BY, Wu BJ, Lee SM, Sun HJ, Chang YT, Lin MW:Prevalence and associated factors of comorbid skin diseases inpatients with schizophrenia: a clinical survey and nationalhealth database study.GenHospPsychiatry 2014; 36:415–421
41. Soderfeldt Y, Gross D: Information, consent and treatmentof patients with Morgellons disease: an ethical perspective.Am J Clin Dermatol 2014; 15:71–76
42. Eskin M, Savk E, Uslu M, Kucukaydogan N: Socialproblem-solving, perceived stress, negative life events,depression and life satisfaction in psoriasis. J Eur AcadDermatol Venereol 2014; 28:1553–1559
43. McGuire JF, Ung D, Selles RR, et al: Treating tricho-tillomania: a meta-analysis of treatment effects and mod-erators for behavior therapy and serotonin reuptakeinhibitors. J Psychiatr Res 2014; 58:76–83
44. Rufer M, Bamert T, Klaghofer R, Moritz S, Schilling L,Weidt S: Trichotillomania and emotion regulation: is
www.psychosomaticsjournal.org 457

Updates in Psychosomatic Medicine
symptom severity related to alexithymia? Psychiatry Res2014; 218:161–165
45. Crosta ML, Caldarola G, Fraietta S, et al: Psychopathol-ogy and eating disorders in patients with psoriasis. G ItalDermatologia Venereologia 2014; 149:355–361
46. ZaidanM, Stucker F, Stengel B, et al: Increased risk of solidrenal tumors in lithium-treated patients. Kidney Int 2014;86:184–190
47. McPherson S, Barbosa-Leiker C, Daratha K, et al: Asso-ciation of co-occurring serious mental illness with emer-gency hospitalization in people with chronic kidney disease.Am J Nephrol 2014; 39:260–267
48. Garcia-Llana H, Remor E, del Peso G, Celadilla O, SelgasR: Motivational interviewing promotes adherence andimproves wellbeing in pre-dialysis patients with advancedchronic kidney disease. J Clin Psychol Med Settings 2014;21:103–115
49. Roxanas M, Grace BS, George CR: Renal replacementtherapy associated with lithium nephrotoxicity in Australia.Med J Aust 2014; 200:226–228
50. Zheng G, Wen J, Zhang L, et al: Altered brain functionalconnectivity in hemodialysis patients with end-stage renaldisease: a resting-state functional MR imaging study.Metab Brain Dis 2014; 29:777–786
51. Zhang J, Zhang P, Ni X, et al: Vitamin D status in chronicdialysis patients with depression: a prospective study. BMCPsychiatry 2014; 14:125
52. Bliwise DL, Zhang RH, Kutner NG: Medications associ-ated with restless legs syndrome: a case-control study in theUS Renal Data System (USRDS). Sleep Med 2014; 15:1241–1245
53. Salter ML, Gupta N, King E, et al: Health-related andpsychosocial concerns about transplantation amongpatients initiating dialysis. Clin J Am Soc Nephrol 2014; 9:1940–1948
54. Manns B, Hemmelgarn B, Lillie E, et al: Setting researchpriorities for patients on or nearing dialysis. Clin J Am SocNephrol 2014; 9:1813–1821
55. Jones ER, Goldman RS: Managing disruptive behavior bypatients and physicians: a responsibility of the dialysisfacility medical director. Clin J Am Soc Nephrol 2014[Epub ahead of print]
56. Zimmermann C, Swami N, Krzyzanowska M, et al:Early palliative care for patients with advanced cancer: acluster-randomised controlled trial. Lancet 2014;383:1721–1730
57. O’Neill S, Posada-Villa J, Medina-Mora ME, et al: Asso-ciations between DSM-IV mental disorders and subsequentself-reported diagnosis of cancer. J Psychosom Res 2014;76:207–212
58. Chang CK, Hayes RD, Broadbent MT, et al: A cohortstudy on mental disorders, stage of cancer at diagnosis andsubsequent survival. BMJ Open 2014; 4:e004295
59. Riblet N, Larson R, Watts BV, Holtzheimer P: Reevaluat-ing the role of antidepressants in cancer-related depression:a systematic review and meta-analysis. Gen Hosp Psychia-try 2014; 36:466–473
458 www.psychosomaticsjournal.org
60. Park EM, Raddin RS, Nelson KM, et al: Conducting anantidepressant clinical trial in oncology: challenges andstrategies to address them. Gen Hosp Psychiatry 2014;36:474–476
61. Fujimori M, Shirai Y, Asai M, Kubota K, Katsumata N,Uchitomi Y: Effect of communication skills training pro-gram for oncologists based on patient preferences forcommunication when receiving bad news: a randomizedcontrolled trial. J Clin Oncol 2014; 32:2166–2172
62. Walker J, Hansen CH, Martin P: Prevalence, associations,and adequacy of treatment of major depression in patientswith cancer: a cross-sectional analysis of routinely collectedclinical data. Lancet Psychiatry 2014; 1:343–350
63. Sharpe M, Walker J, Holm Hansen C, et al: Integratedcollaborative care for comorbid major depression inpatients with cancer (SMaRT Oncology-2): a multicentrerandomised controlled effectiveness trial. Lancet 2014;384:1099–1108
64. Walker J, Hansen CH, Martin P, et al: Integratedcollaborative care for major depression comorbid with apoor prognosis cancer (SMaRT Oncology-3): a multicentrerandomised controlled trial in patients with lung cancer.Lancet Oncology 2014; 15:1168–1176
65. EvinsAE,CatherC, Pratt SA, et al: Maintenance treatmentwith varenicline for smoking cessation in patients withschizophrenia and bipolar disorder: a randomized clinicaltrial. J Am Med Assoc 2014; 311:145–154
66. Druss BG, Ji X, Glick G, von Esenwein SA: Randomizedtrial of an electronic personal health record for patients withserious mental illnesses. Am J Psychiatry 2014; 171:360–368
67. Benros ME, Pedersen MG, Rasmussen H, Eaton WW,Nordentoft M, Mortensen PB: A nationwide study on therisk of autoimmune diseases in individuals with a personalor a family history of schizophrenia and related psychosis.Am J Psychiatry 2014; 171:218–226
68. Chwastiak LA, Davydow DS, McKibbin CL, et al: Theeffect of serious mental illness on the risk of rehospitaliza-tion among patients with diabetes. Psychosomatics 2014;55:134–143
69. Bergamo C, Sigel K, Mhango G, Kale M, Wisnivesky JP:Inequalities in lung cancer care of elderly patients withschizophrenia: an observational cohort study. PsychosomMed 2014; 76:215–220
70. Viverito K, Owen R,Mittal D, Li C, Williams JS: Manage-ment of new hyperglycemia in patients prescribed antipsy-chotics. Psychiatr Serv 2014; 65:1502–1505
71. Green CA, Yarborough BJ, Leo MC, et al: The STRIDEweight loss and lifestyle intervention for individuals takingantipsychotic medications: a randomized trial. Am J Psy-chiatry 2015; 172:71–81
72. Correll CU, Robinson DG, Schooler NR, et al: Cardio-metabolic risk in patients with first-episode schizophreniaspectrum disorders: baseline results from the RAISE-ETPstudy. JAMA Psychiatry 2014; 71:1350–1363
73. Carson AJ, Stone J, Hansen CH, et al: Somatic symptomcount scores do not identify patients with symptomsunexplained by disease: a prospective cohort study of
Psychosomatics 56:5, September/October 2015

Freudenreich et al.
neurology outpatients. J Neurol Neurosurg Psychiatry2015; 86:295–301
74. Milner A, Page A, Morrell S, et al: The effects ofinvoluntary job loss on suicide and suicide attempts amongyoung adults: evidence from a matched case-control study.Aust N Z J Psychiatry 2014; 48:333–340
75. Fazel S, Wolf A, Pillas D, Lichtenstein P, Langstrom N:Suicide, fatal injuries, and other causes of prematuremortality in patients with traumatic brain injury: a 41-year Swedish population study. JAMA Psychiatry 2014;71:326–333
76. LeFevre ML: Screening for suicide risk in adolescents,adults, and older adults in primary care: U.S. PreventiveServices Task Force recommendation statement. AnnIntern Med 2014; 160:719–726
77. Tsai AC, Lucas M, Sania A, Kim D, Kawachi I: Socialintegration and suicide mortality among men: 24-yearcohort study of U.S. health professionals. Ann InternMed 2014; 161:85–95
78. Kang HK, Bullman TA, Smolenski DJ, Skopp NA, GahmGA, Reger MA: Suicide risk among 1.3 million veteranswho were on active duty during the Iraq and Afghanistanwars. Ann Epidemiol 2015; 25:96–100
79. Artherholt SB, Hong F, Berry DL, Fann JR: Risk factorsfor depression in patients undergoing hematopoietic celltransplantation. Biol Blood Marrow Transplant 2014;20:946–950
80. Tryc AB, Pflugrad H, Goldbecker A, et al: New-onsetcognitive dysfunction impairs the quality of life in patientsafter liver transplantation. Liver Transpl 2014; 20:807–814
81. Sorensen LG, Neighbors K, Martz K, Zelko F, BucuvalasJC, Alonso EM: Longitudinal study of cognitive andacademic outcomes after pediatric liver transplantation.J Pediatr 2014; 165:65–72.e62
Psychosomatics 56:5, September/October 2015
82. FoxKR, PoslusznyDM,DiMartini AF, et al: Predictors ofpost-traumatic psychological growth in the late years afterlung transplantation. Clin Transplant 2014; 28:384–393
83. Burkhalter H, Wirz-Justice A, Denhaerynck K, et al: Theeffect of bright light therapy on sleep and circadian rhythmsin renal transplant recipients: a pilot randomized, multi-centre wait-list controlled trial. Transpl Int 2015; 28:59–70
84. LadnerDP,DewMA,Forney S, et al: Long-term quality oflife after liver donation in the adult to adult living donorliver transplantation cohort study (A2ALL). J Hepatol2015; 62:346–353
85. Sanchez R, Bailles E, Peri JM, et al: Cross-sectionalpsychosocial evaluation of heart transplantation candi-dates. Gen Hosp Psychiatry 2014; 36:680–685
86. Hatta K, Kishi Y, Wada K, et al: Preventive effects oframelteon on delirium: a randomized placebo-controlledtrial. JAMA Psychiatry 2014; 71:397–403
87. Gacouin A, Tadie JM, Uhel F, et al: At-risk drinking isindependently associated with ICU and one-year mortalityin critically ill nontrauma patients*. Crit Care Med 2014;42:860–867
88. Freeman EW, Sammel MD, Boorman DW, Zhang R:Longitudinal pattern of depressive symptoms around nat-ural menopause. JAMA Psychiatry 2014; 71:36–43
89. Joffe H, Guthrie KA, LaCroix AZ, et al: Low-doseestradiol and the serotonin-norepinephrine reuptake inhib-itor venlafaxine for vasomotor symptoms: a randomizedclinical trial. JAMA Intern Med 2014; 174:1058–1066
90. HuybrechtsKF, PalmstenK,Avorn J, et al: Antidepressantuse in pregnancy and the risk of cardiac defects. N Engl JMed 2014; 370:2397–2407
91. Bech BH, Kjaersgaard MI, Pedersen HS, et al: Use ofantiepileptic drugs during pregnancy and risk of sponta-neous abortion and stillbirth: population based cohortstudy. Br Med J 2014; 349:g5159
www.psychosomaticsjournal.org 459