Embed Size (px)
Citation preview

UNIVERSITY OF OSLO FACULTY OF DENTISTRY
Department of Endodontics Postgraduate Program in Endodontics Case Book Trude Handal Autumn Semester 2014

1 Table of contents
Endodontic treatment guidelines ............................................................................................... 1
Non-surgical cases Case 1 ............................................................................................................................................................... 6
Endodontic treatment of the mandibular right second molar with irreversible pulpitis and cracked tooth syndrome
Case 2 ............................................................................................................................................................ 12 Endodontic treatment of the mandibular right second molar with irreversible pulpitits and iatrogenic furcal perforation
Case 3 ............................................................................................................................................................ 17 Endodontic treatment of a mandibular right first incisor in a patient with DiGeorge Syndrome (velo-cardio-facial-syndrome)
Case 4 ............................................................................................................................................................ 22 Endodontic retreatment of the maxillary right second molar
Case 5 ............................................................................................................................................................ 28 Endodontic treatment of the maxillary left first molar
Case 6 ........................................................................................................ 3Error! Bookmark not defined. Endodontic retreatment of the maxillary right first incisor
Case 7 ........................................................................................................ Error! Bookmark not defined.8 Endodontic retreatment of the maxillary left first molar
Case 8 ............................................................................................................................................................ 42 Endodontic retreatment of the mandibular left first molar
Case 9 ............................................................................................................................................................ 47 Endodontic retreatment of the maxuíllary left first incisor
Case 10 ......................................................................................................................................................... 52 Endodontic treatment of a maxillary anterior tooth
Case 11 ......................................................................................................................................................... 56 Patient with persistent pain maxilla left side
Surgical cases Case 12 ......................................................................................................................................................... 62
Endodontic retreatment and apical surgery of the maxillary right canine Case 13 ......................................................................................................................................................... 69
Endodontic retreatment in conjunction with apical surgery of the mandibular right first molar with a separated instrument
Case 14 ......................................................................................................................................................... 76 Explorative surgery of the maxillary left second incisor with sinus tract
Case 15 ......................................................................................................................................................... 82 Endodontic retreatment of the maxillary left first molar and surgical retreatment of the maxillary left first and second premolar
Case 16 ......................................................................................................................................................... 88 Endodontic treatment and apical surgery of the mandibular left first molar
Case 17 ......................................................................................................................................................... 94 Surgical retreatment of the maxillary right first incisor
Case 18 ......................................................................................................................................................... 99 Evaluation of a root-filled mandibular right first molar and surgical retreatment of the maxillary left first molar with a sinus tract
Case 19 .......................................................................................................................................................106 Endodontic retreatment of the maxillary right first molar with a sinus tract
Case 20 .......................................................................................................................................................112 Treatment of multiple idiopathic cervical root resorption


1
Endodontic Treatment Guidelines
Treatment of Tooth with Apical Periodontitis Pre-operative radiograph.
Anaesthesia.
Removal of plaque, caries and leaking fillings.
Pre-endodontic tooth build-up if required for isolation.
Access cavity preparation.
Localization of canal orifices.
Application of rubber dam.
Disinfection of the working field with 0.5% chlorhexidine in 70% ethanol.
Measurement of working length, using apex locator and working length radiograph.
Instrumentation to desired apical length and size:
Goal: 0.5-1mm short of the anatomic apex
Frequent irrigation with:
0.5% sodium hypochlorite (NaOCl)
Alternative: 0.5 % chlorhexidine (from 2013)
Final irrigation with 17% ethylenediamine tetraacetic acid (EDTA)
Drying of the canals with paper points.
Mastercone radiograph.
Root filling:
Obturation techniques:
Lateral compaction, warm vertical compaction, apical plug with MTA
Sealers:
AH Plus
Seal Core materials:
Gutta-percha
Temporary IRM top filling with a 2 mm IRM plug in the canal orifice
Alternatively a final composite restoration
Removal of rubber dam.
Post-operative radiograph.

2
Treatment of Tooth with Apical Periodontitis The same treatment as for teeth without apical periodontitis, but two-appointment
treatment is the standard procedure: 2-3 weeks between 1st and 2nd appointment is
the standard, mainly due to practical reasons:
Intra-canal dressing with Ca(OH)2
Two-layered temporary top filling: Cavit G and IRM
In retreatment cases: Final irrigation with 17% EDTA and 2% chlorhexidine-di-
gluconate.
The periapical index (PAI) (Ørstavik et al. 1986) is used for radiographic evaluation.
Emergency treatment Acute irreversible pulpitis:
Pulpotomy
Eugenol pellet in pulp chamber
IRM top filling
NSAIDs when severe pain
Acute apical periodontitis:
Incision and drainage of abscess/pus if applicable
Preparation of canals and intracanal dressing (Ca(OH)2) as the optimal treatment
NSAIDs when indicated
Systemic antibiotics if systemic complaints and disseminating infection

3
Endodontic files for instrumentation of canals Hand files: K-files Stainless steel files (SS) Hedstrøm files Nickel-titanium files (NiTi files)
NiTi rotary files: Biorace Reciproc
Endodontic surgery All relevant radiographs mounted on viewer or screen.
Anaesthesia.
1 minute mouth rinse with Corsodyl®(Chlorhexidine 2mg/ml).
Incision:
A horizontal incision extending one to several teeth mesial and distal of the
involved tooth and one vertical-releasing incision, usually placed at the mesial
end of the prospective flap.
Retraction:
To hold the flap away from the surgical site, providing maximum access and
visibility, without causing harm to the flap or the surrounding tissues.
Osteotomy:
Involves removal of cortical and cancellous bone to gain direct access to the
apical portion. This is achieved routinely by using burs/rotary instruments.
Surgical curettage:
To remove all pathologic tissue, foreign bodies, and root and bone particles from
the periradicular area.
Biopsy:
Any soft tissue lesion removed during the surgical procedure should be
submitted for biopsy.
Microbiological sample:
With paper point directly in the periapical sample, placed in pre-reduced
anaerobic transport medium, or periapical tissue placed in 4% formalin for
scanning electron microscopy.

4
Root end resection:
By sectioning the apical segment of the root and/or bevelling it to the line of
sight/3 mm.
Ultrasonic root end preparation:
To provide a clean, well-shaped class I cavity.
Haemorrhage control:
Local anaesthetic solutions possessing vasoconstrictor properties; Stryphnon
gauze (Adrenalonchlorid 0,33 mg/cm2); Ferric sulphate (Fe2[SO4]3 with 15.5%
astringent and 21% stasis).
Root-end filling:
Using either IRM or MTA. Use of the MAP system (Micro-Apical Placement) or the
MTA pellet-forming block will ease the application of MTA.
Cleaning of surgical site:
Saline solution to remove debris, and tissue edges are re-approximated in their
correct position to promote healing by primary intention.
Compression of the repositioned tissue with a saline-moistened piece of gauze will
reduce the coagulum to a thin fibrin layer between the repositioned tissue and cortical
bone. Tissue margins should rest passively in the desired place before suturing.
Wound closure:
Using nonabsorbable suture material in sizes 4-0 and 6-0.
Post-operative radiograph is taken for control of procedures and as reference for follow-
up.
Postsurgical care:
A disposable ice pack is covered with a soft towel, and the patient instructed on
where and how to hold the ice pack firmly in position against the facial tissues
approximating the surgical site.
Unless contraindicated for some reason, the patient is instructed to take
Ibuprofen 400mg every 4 to 6 hours for the first 48hours. The patient is advised
to rinse with Corsodyl® twice a day until suture removal.
Suture removal:
The epithelial seal at the wound edges is evident within 2 days-suture removal
can take place earliest after 48h but nor later than 6-7 days.

5
Abbreviations Nd: not determined.
V&h: vertical and horisontal.

6
Case 1
Endodontic treatment of the mandibular right second molar with irreversible pulpitis and cracked tooth syndrome
Fig. 1. Frontal view.
Patient 43-year-old Caucasian female.
Chief complaint The patient complained about pain in the posterior region in the lower right jaw. She felt sudden pain and tenderness when chewing and biting. She also complained about increased sensitivity to thermal changes (both cold and warm stimuli) and discomfort during tooth brushing. The pain started after placement of a filling in the molar tooth in this jaw.
Medical record The patient had recurrent headaches and was medicated with Sarotex.
Dental history The patient was referred to the post-graduate clinic from the student clinic for evaluation and treatment of the mandibular right second molar. The tooth had previously been treated with an occlusal composite restoration due to occlusal caries three years earlier (2007), followed by a temporary restoration (IRM) in 2010 due to post-restoration pain. Since the pain
persisted, another temporary IRM filling, with concomitant reduction of cusp heights but without cuspal coverage was placed.
Fig. 2. Craze lines are visible at the buccal and distal aspect of the tooth.
Clinical findings September 15th2010 Soft tissue: Normal findings. Dental: Tooth 45: Sound. Tooth 46: Missing. Tooth 47: Occlusal temporary filling; several craze lines/fracture lines can be seen in the enamel (Fig 2.) When using a FracFinder on the different cusps of tooth 47, the patient felt sharp pain when the distal cusps were tested.
Clinical tests September 15th2010 44 45 47 EPT 16 16 43 Cold + + + Percussion - - +(v)∗ Palpation - - - PPD 4 4 4 Mobility - - - Biting - - + ∗v, vertical

7
Radiographic findings September 15th2010 Dental: Tooth 47 has a radiopaque occlusal filling. Periodontal: Marginal bone loss. Periapical: Teeth 45 and 46 have a continuous PDL space.
Fig. 3. Periapical radiograph 15.09.2010.
Diagnosis September 15th2010 Diagnosis Pulpal K04.01 acute irreversible pulpitis Periodontal K05.03 chronic marginal periodontitis Periapical Within normal limits Dental S02.50A cracked tooth
Treatment plan Treatment of the inflamed pulp tooth 47.
Problem list Cracked tooth.
Treatment September 15th2010 2 carpules of Xylocaine/adrenaline was applied to establish anaesthesia. Access opening and localisation of three canal orifices. Bleeding from all canals. The distal fracture line extended through the distal marginal ridge.
Mechanical: Bur, NiTi hand instrumentation #20, Biorace: MB: #40/0.04 (BR5) /16mm ML: #40/0.04 (BR5) /16mm D: #60/0.02 (BR7) /15 mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 4. Working length radiograph.
Intra-pulpal injection of anaesthetic was applied during the session due to pain when negotiating the canals. The patient was told that the tooth would have a less favourable prognosis unless a dental crown was made.
Treatment September 29th2010 The patient experiences fewer symptoms. The tooth is slightly tender to percussion, and the last two days she felt some tenderness when biting and tooth brushing. Several other teeth are also tender to percussion. Anaesthesia: 2 carpules of Xylocaine/adrenaline. The canals were obturated using gutta-percha (0.04 and 0.02 taper) and AH Plus and the tooth was sealed with IRM.

8
Fig. 5. Master cone radiograph.
Fig. 6. Post-obturation radiograph 29.09.2010.
Prognosis Endodontic: Good. Tooth: Uncertain due to cracks.
Follow up examination October 11th2011 (1 year) A dental crown has been made at the student clinic. She still feels some sensitivity to biting and tooth brushing. TMD symptoms.
Fig. 7. Follow-up radiograph 1 year.
Discussion The term “cracked tooth syndrome” (CTS), was first introduced by Cameron in 1964 (1). He defined a cracked tooth as an ”incomplete fracture in a vital posterior tooth that involves the dentine and occasionally extends into the pulp.” Diagnosis of incompletely fractured teeth with symptoms is time consuming and may represent a diagnostic problem. The discomfort or pain can mimic that arising from other pathologies, such as sinusitis, temporomandibular joint disorders, headaches, ear pain, or atypical orofacial pain (2). There may be a history of a course of extensive dental treatment involving repeated occlusal adjustments or replacement of restorations, which fail to eliminate symptoms. The American Association of Endodontists (AAE) categorized longitudinal tooth fractures into 5 major classes: craze line, fractured cusp, cracked tooth, split tooth, and vertical root fracture (VRF) (3). The diagnosis of CTS has been based in the past exclusively on tooth symptomatology. Common patient subjective findings with incompletely fractured teeth include: 1. Sustained pain during biting pressures, 2. Pain only upon release of biting pressure, 3. Occasional, momentary, sharp pain during mastication, 4. Sensitivity to thermal changes, 5. Sensitivity to mild stimuli, such as sweet or acidic foods, and 6. Persistent dull pain. Common clinical objective findings with incompletely fractured teeth: 1. Pain to selective percussion on specific tooth margins or cusps. The percussion may be in the long axis of the tooth or angled against a labial or cuspal slope, 2. Generalized discomfort to percussion, 3. Presence of craze or fracture lines on the facial or lingual surfaces or marginal ridges, 4.

9
Significant gaps between old restorations and tooth structure, 5. Cracked restorations, and 6. Evidence of the initial vertical loss of alveolar bone adjacent to the proximal root surface (4). A variety of protocols have been described in the contemporary literature for the definitive management of incomplete posterior tooth fractures, ranging from the application of directly bonded intra-coronal restorations and directly bonded extra-coronal restorations (5) and indirect extra-coronal restorations with varying amounts of tooth coverage (6). Seo et al. (7) analysed the characteristics, distribution, and associated factors of longitudinal fractures in 107 teeth from 103 patients. Eighty-seven teeth were diagnosed with a cracked tooth (81.3%), 14 were diagnosed with vertical root fracture (VRF, 13.1%), 4 had a split tooth (3.7%), and 2 had a fractured cusp (1.9%). I In 82.2% teeth showed a sensitive reaction on the bite test. The upper first molar (28.0%) was most frequently cracked, followed by the lower first molar (25.2%), the lower second molar (20.6%), and the upper second molar (16.8%). Longitudinal tooth fractures occurred mainly in restored teeth and in patients in their 40 years of age. Out of 107 of longitudinal fractured teeth, 33 (30.8%) were treated endodontically and 74 (69.2%) were not. VRF was associated with endodontic treatment. Roh et al. (8) reported on 154 cases of teeth with cracks. In their study cracked teeth were observed most frequently in the teeth with no restorations (60.4%) and with class I restorations (29.2%). The most prevalent age was in those over 40 years of age (31.2% in their 40s, 26.6% in their 50s) and the prevalence was similar in men (53.9%) and women (46.1%). Cracked teeth were found most frequently in the maxillary molars
(33.8% in first molar, 23.4% in second molar), followed by mandibular molars (20.1% in first molar, 16.2% in second molar). 96.1% of the cracked teeth responded to the bite test, and 81.1% of the cracked teeth were observed in the mesiodistal direction. In a material from Krell & Rivera (9) 796 out of 8175 cases seen in an endodontic practice during a six-year period were diagnosed as cracked teeth (9.7%). Mandibular second molars (243/796, 30%) had the largest incidence followed by mandibular first molars (231/796, 29%) and maxillary first molars (167/796, 21%). Of 127 patients specifically diagnosed with reversible pulpitis (RP), 27 converted to irreversible pulpitis (N=21) in 58 days or to necrotic pulp (N=6) in 149 days. The outcomes of this study suggested that if a crack is identified early enough in cases with a diagnosis of RP and a crown is placed, root canal treatment will be necessary in about 20% of these cases within a 6-month period. Tan el al. (10) assessed the survival rate of root filled cracked teeth over a 2-year period in a tertiary institute. Forty-nine patients who had root canal treatment completed on their cracked teeth at the National Dental Centre (Singapore) were recalled for a 2-year review. The survival rate of the root-filled cracked teeth was 85.5%. Cracked teeth that were the terminal teeth in the dental arch, teeth with pre-root filling periodontal pocketing and teeth with multiple cracks were more likely to be extracted. Opdam et al. (5) performed a seven-year clinical evaluation of painful cracked teeth restored with a direct composite restoration. Twenty teeth were restored without and 21 with cuspal coverage. After 7 years, 40 teeth could be evaluated. Three teeth without cuspal coverage needed an endodontic treatment, of which 2 failed as a result of

10
fracture. No failures in restorations with cuspal coverage occurred. They suggested that a direct bonded composite resin restoration could be a successful treatment for a cracked tooth. In a study by Brynjulfsen et al. (11), 32 patients with poorly localised orofacial pain were finally diagnosed with 46 incompletely fractured teeth. In cases with incompletely fractured mandibular teeth, the pain was felt throughout the arch and in tissues including neck, ear, chewing muscles and TMJ on the same side. The longer the duration of pain before the diagnosis of an incompletely fractured tooth was established, the more diffuse was the distribution of pain. Often symptoms projected to both jaws. Headaches occurred in the group of patients with symptoms for more than 5 years prior to treatment. Endodontic or restorative treatment relieved the symptoms in 90% of the patients during a two-year follow-up, whilst persisting symptoms in 10% were considered as part of an orofacial pain complex of unknown aetiology. The patient in the present case had an incomplete fractured tooth. Although treatment will succeed in many cases, some cracked teeth may eventually evolve into split teeth and require extraction. Placement of a cuspal-reinforced restoration, in this case a crown, providing optimum protection for the tooth, does not guarantee success, but is thought to be beneficial in most cases.
References 1. Cameron CE. Cracked-tooth
syndrome. J Am Dent Assoc 1964; 68: 405-411.
2. Türp JC, Gobetti JP. The cracked tooth syndrome: an elusive diagnosis. J Am Dent Assoc 1996; 127(10): 1502-1507.
3. American Association of Endodontists. Cracking the cracked tooth code: Detection and treatment of various longitudinal tooth fractures. Endodontics: Colleagues for Excellence 2008; summer: 1-8.
4. Gutmann JL, Rakusin H. Endodontic and restorative management of incompletely fractured molar teeth. Int Endod J 1994; 27: 343-348.
5. Opdam NJ, Roeters JJ, Loomans BA, Bronkhorst EM. Seven-year clinical evaluation of painful cracked teeth restored with a direct composite restoration. J Endod. 2008; 34(7): 808-811.
6. Signore A, Benedicenti S, Covani U, Ravera G. A 4–6 year retrospective clinical study of cracked teeth restored with bonded indirect resin composite onlays. Int J Prosthodontics 2007; 20: 609–616.
7. Seo DG, Yi YA, Shin SJ, Park JW. Analysis of factors associated with cracked teeth. J Endod 2012; 38(3): 288-292.
8. Roh BD, Lee YE. Analysis of 154 cases of teeth with cracks. Dent Traumatol 2006; 22(3): 118-23.
9. Krell KM, Rivera EM. A Six Year Evaluation of Cracked Teeth Diagnosed with Reversible Pulpitis: Treatment and Prognosis, J Endod 2007; 33(12): 1405-1407.
10. Tan L, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J 2006; 39(11): 886-889.
11. Brynjulfsen A, Fristad I, Grevstad T, Hals-Kvinnsland I. Incompletely fractured teeth associated with diffuse longstanding orofacial pain: diagnosis and treatment

11
outcome. Int Endod J 2002; 35: 461-466.

12
Case 2
Endodontic treatment of the mandibular right second molar with irreversible pulpitis and iatrogenic furcal perforation
Fig. 1. Frontal view.
Patient 59-year-old Caucasian male.
Chief complaint The patient complained of severe permanently pain which got worse in the evening/at night. He was suppressing the pain with analgesics (NSAIDs).
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate clinic from a general dental practitioner for endodontic treatment of the mandibular right second molar. The tooth had previously, and recently, been accessed by the referring dentist with the result of an iatrogenic furcal perforation.
Clinical findings January 28th2014 Soft tissue: Normal findings. Dental: Tooth 45: Dental crown.
46: Composite restoration ODB, occlusal temporary filling. 47: Dental crown, occlusal temporary filling (Fig. 2).
Fig. 2. Buccal/occlusal view.
Clinical tests January 28th2014 45 46 47 EPT nd∗ nd 80 Cold - - + Percussion - - +(v,h)∗ Palpation - - - PPD 4 3 3 Mobility - - - Biting - - - ∗nd, not determined ∗v, vertical ∗h, horizontal
Radiographic findings January 28th2014 Dental: Tooth 45: Radiopaque coronal restoration, poorly fitted crown with possible caries at the distal aspect, a post in the canal and a radiopaque root filling material. A radiolucency is seen between the post and the root filling.

13
Tooth 46: Radiopaque coronal restoration and a radiopaque root filling material. Tooth 47: Radiopaque coronal restoration, a radiolucency can be seen in the floor of the pulp chamber in the furcation area. Periodontal: Marginal bone loss. Periapical: Tooth 47 has a continuous PDL space (PAI I). Tooth 46 has a widened PDL space and an apical radiolucency mesial root (PAI 3). Tooth 45 has an apical radiolucency (PAI 4).
Fig. 3 Periapical radiograph 28.01.2014.
Diagnosis January 1st2014 Diagnosis Pulpal K04.01 acute irreversible pulpitis
Periodontal K05.03 chronic marginal periodontitis Periapical Within normal limits
Treatment plan Treatment of the inflamed pulp. Reparation of furcation perforation.
Problem list Communication of perforation to oral cavity. Weakened tooth.
Treatment January 28th2014 Two carpules of Xylocaine/adrenaline was applied to establish anaesthesia. Intrapulpal injection was necessary. Access opening and localisation of perforation and undiscovered MB canal orifice (Fig. 5). Mechanical: Bur, NiTi hand files #20, RECIPROC one file endo: MB: #40/18mm ML: #40/18mm D: #50 /18mm Chemical: 0.5% chlorhexidine, 17% EDTA. Reparation of furcal perforation with MTA seal. Intracanal medicament: Ca(OH)2. Temporary filling: Moistened cotton pellet, cavit, IRM.
Fig. 4. Working length radiograph.
Fig. 5. Furcal perforation.

14
Fig. 6. Reparation of furcal defect with grey MTA.
Treatment February 2nd2014 No symptoms, filled with gutta-percha and AH Plus, sealed with composite.
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph.
Prognosis Endodontic: Uncertain. Tooth: Uncertain
Follow-up examination September 2014 Not able to reach the patient for a scheduled control.
Discussion Perforations from the pulp to the surrounding periodontium may occur from resorptive defects, caries or iatrogenic events during endodontic treatment. Perforations create an artificial communication between the root canal system and the supporting tissues of the teeth (1). Ingle (2) reported that perforations were the second greatest cause of endodontic failure and account for 9.6% of all unsuccessful cases. Factors that affect treatment prognosis of perforation repair include the level, location and size of the perforation, the time delay before perforation repair and the material used to seal the perforation (3). The location of the perforation is of crucial importance. Close proximity to the gingival sulcus may lead to endodontic-periodontal problems through contamination of the perforation with bacteria from the oral cavity through the sulcus (4). Perforations near the crestal bone are susceptible to epithelial migration and rapid pocket formation and treatment of these has a low success rate (5). The purpose of treating furcal perforation is to seal the artificial communication between the endodontic space and the periradicular tissue to prevent alveolar bone resorption and damage to the periodontal ligament. These complications are not infrequent in cases of furcal and/or old perforations, which show a worse prognosis than fresh, small, coronal, and apical perforations. Mineral trioxide aggregate (MTA) is widely used to seal perforations because of its biocompatibility and sealability. Lodiene et al. (6) created furcation perforations in 82 extracted human maxillary and mandibular molars, and sealed them with either mineral trioxide aggregate (MTA), glass ionomer cement or resin composite. The bacterial

15
leakage method was used with Enterococcus faecalis as microbial tracer. They found that the percentage of leaking samples was significantly higher in the resin composite group. Scanning electron microscopy (SEM) inspection revealed the presence of bacteria in all leaking specimens. Bacteria were observed along the filling-dentine interface as well as in dentinal tubules at some distance from the filling. The authors concluded that teeth repaired with MTA were more resistant to bacterial leakage. Ford et al. (7) investigated the histologic response to intentional perforation in the furcations of 28 mandibular premolars in seven dogs. In half the teeth, the perforations were repaired immediately with either amalgam or MTA; in the rest the perforations were left open to salivary contamination before repair. All repaired perforations were left for 4 months before histologic examination of vertical sections through the site. In the immediately repaired group, all the amalgam specimens were associated with inflammation, whereas only one of six with MTA was; further, the five non-inflamed MTA specimens had some cementum over the repair material. After 4 months, all the amalgam specimens were associated with inflammation; in contrast only four of seven filled with MTA were inflamed. The authors suggest that MTA is a far more suitable material than amalgam for perforation repair, particularly when used immediately after perforation. Another study (8) assessed the ability of Portland cement, white Angelus-mineral trioxide aggregate (MTA), and MTA Bio to seal furcal perforations in extracted human molar teeth. Leakage existed in every sample and was very variable in all the experimental groups. The sealing ability promoted by the 3 cements was similar; no cement was able to produce a fluid-tight seal.
In a case series (9) MTA was used as repair material for furcal perforation Ten cases of furcal perforation were selected at the department of Endodontics, University of Florence. All the perforations were cleaned with NaOCl, EDTA, and ultrasonic tips and sealed with MTA without internal matrix. Finally, the teeth were endodontically treated and coronally restored. Clinical and radiographic follow-ups were done at 6 months, 1 year, 2 years, and 5 years. After 5 years, the absence of periradicular radiolucent lesions, pain and swelling along with functional tooth stability indicated a successful outcome of sealing perforations in 9 out of 10 teeth. One patient dropped out of the study after the 1-year follow-up and could not be contacted for further recalls. The results confirmed that MTA provides an effective seal of root perforations and clinical healing of the surrounding periodontal tissue.
References 1. Fuss Z, Trope M. Root
perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996; 12: 255–264.
2. Ingle JI. A standardized endodontic technique utilizing newly designed instruments and filling materials. Oral Surg Oral Med Oral Pathol 1961; 14: 83-91.
3. Tsatsas DV, Meliou HA, Kerezoudis NP. Sealing effectiveness of materials used in furcation perforation in vitro. Int Dent J 2005; 55: 133–141.
4. Simon J H, Glick D H, Frank A L. The relationship of endodontic-periodontic lesions. J Periodontol 1972; 43: 202–208.
5. Petersson K, Hasselgren G, Tronstad L. Endodontic treatment of experimental root

16
perforations in dog teeth. Endod Dent Traumatol 1985; 1: 22–28.
6. Lodiene G, Kleivmyr M, Bruzell E, Ørstavik D. Sealing ability of mineral trioxide aggregate, glass ionomer cement and composite resin when repairing large furcal perforations. British Dent J 2011; 210: 1-6.
7. Ford TR, Torabinejad M, McKendry DJ, Hong CU, Kariyawasam SP. Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995 Jun;79(6):756-63.
8. De-Deus G, Reis C, Brandão C, Fidel S, Fidel RA. The ability of Portland cement, MTA, and MTA Bio to prevent through-and-through fluid movement in repaired furcal perforations. J Endod. 2007 Nov; 33(11): 1374-1377.
9. Pace R, Giuliani V, Pagavino G. Mineral trioxide aggregate as repair material for furcal perforation: case series. J Endod. 2008; 34(9): 1130-1133.

17
Case 3
Endodontic treatment of a mandibular right first incisor in a patient with DiGeorge Syndrome (velo-cardio-facial syndrome)
Fig. 1. Frontal view
Patient 21-year-old Caucasian male.
Chief complaint Non-contributory.
Medical record The patient was diagnosed with DiGeorge Syndrome. He was quite anxious in new situations. Due to asthma he was medicated with Symbicort, Ventoline and Serevent. Because of congenital heart disease he was in need of prophylactic antibiotics before dental treatment.
Dental history The patient was referred to the post-graduate clinic from the public dentistry for endodontic treatment of the mandibular right lateral incisor. The mandibular right lateral incisor presented with a history of persistent fistula; tooth 42 had previously been treated endodontically, including cleaning/shaping to size #50 with rotary
Fig. 2. Fractured crown, tooth 42.
instruments (Biorace) and treatment with intracanal dressing of Ca(OH)2.
Clinical findings September 20th2011 Soft tissue: Gingivitis. Dental: Tooth 41: Composite build-up IP. Tooth 42: Fractured crown, occlusal temporary filling (Fig. 2). Tooth 43: Buccal enamel caries.
Clinical tests September 20th2011 41 42 43 EPT 25 80 15 Cold + - + Percussion - - - Palpation - + - PPD 3 3 3 Mobility - - - Biting - - -
Radiographic findings September 20th2011 Dental: Tooth 31 has a radiopaque root filling material. Teeth 41, 42 and 43 have radiopaque restorations related to the crowns.

18
Periodontal: Within normal limits. Periapical: A lateral radiolucency is seen between the roots of teeth 42 and 43 (PAI 4).
Fig. 3. Periapical radiograph 20.09.2011.
Diagnosis September 20th2011
Diagnosis Pulpal K04.11 necrotic pulp
K04.19 endodontically treated Periodontal K05.01 chronic gingivitis Periapical K04.51 chronic lateral periodontitis
Treatment plan Tooth 42: Endodontic treatment.
Problem list Cooperation/anxiety.
Treatment September 20th2011 Two carpules Xylocaine/adrenaline was applied to establish anaesthesia (infiltration). Access opening and localisation of untreated lingual canal orifice (bleeding from canal). Due to challenges with poor anaesthesia and patient hyperventilation (due to anxiety) treatment had to be ended. Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Treatment October 18th2011 Two carpules of Xylocaine/adrenaline was applied to establish anaesthesia (mandibular block and infiltration). Mechanical: Bur, NiTi hand files: B: #50/0.02/16mm L: #40/0.02/16.5mm Chemical: 1% NaOCl, 17% EDTA, 2% chlorhexidine-di-gluconate. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 4. Working-length radiograph.
Treatment November 8th2011 No symptoms. Filled with gutta-percha (0.02 taper) and AH Plus, sealed with IRM.
Fig. 5. Master cone radiograph.

19
Fig. 6. Post-obturation radiograph.
Prognosis Endodontic: Good. Tooth: Uncertain due to loss of tooth substance.
Follow-up examination October 15th2013 (2 years) No symptoms. A crown has been made. Lateral radiolucency has healed.
Fig. 7. Follow-up radiograph 2 years.
Discussion One of the most important factors in endodontic therapy is the mechanical preparation of the root canal. Despite the high success rates seen for appropriate endodontic procedures (1, 2), cleaning of complex root canals such as to those with lateral branches or apical ramifications is difficult.
Furthermore, cleaning narrow flattened canals or roots with a high degree of curvature is extremely ineffective (3). If accurate data on the size of the apex of root canals could be obtained, it might provide reliable standards for the amount of instrumentation normally required in this region. In an attempt to provide such data, Kerekes and Tronstad (4, 5, 6) measured the diameter of root canals by taking sections of anterior, premolar, and molar teeth at 1, 2, 3, 4, and 5 mm from the apex. Based on these data, they then estimated the smallest size of instruments that would ensure, with 90% probability for each tooth type, adequate preparation of the circular-shaped canals at the various distances from the apex. The internal anatomy of the mandibular incisors has been described in several studies that used clearing or cross-sectional methods (7-14). The results of these studies show that mandibular incisors with single canals are the most common reported anatomy. The second most prevalent anatomic variation includes the presence of 2 canals that ends in a single foramen (Vertucci type III) (7, 11, 15). In their study of one hundred freshly extracted central and lateral incisors, Kartal and Yanikoglo (15) concluded that the chance of a second canal in mandibular incisors is 50%. They also described two additional root canal types that are not defined in Vertucci´s classification (7). Despite the presence of single canals at the apical third of the mandibular incisors, the prevalence of oval canals is not uncommon (9). Several studies have shown the difficulty to achieve efficient cleaning of the mandibular incisors with oval root canal anatomy by using hand or rotary instruments (16-19).

20
Miyashita el al. (13) investigated canal configuration, thickness and curvature of the root canals, condition of any accessory canals, and location of the apical foramina in 1085 extracted mandibular incisors with no visual abnormalities. They found that more than 85 % of the root canals possessed a single canal (Type I). The majority of the lateral branches were small (>80% <#15 reamer, none >#30 reamer and 50 % of apical foramina were located distal to the apex. Based on data on the thickness of the root and main canal in the apical portion and curvature of the root canal the authors suggested that for adequate apical preparation, a #40 reamer must be able to reach the apical constriction. Milanezi de Almeida et al. (20) analysed root canal anatomy and prevalence of oval canals in 340 mandibular incisors by micro CT scanning. The occurrence of a single canal and Vertucci type III configuration represented 92% of the mandibular incisors studied. Within these anatomic configurations, oval-shaped canals in the apical third were not uncommon and were more prevalent in the type III anatomy.
References 1. Grossman LI, Shepard LI, Pearson
LA. Roentgenologic and clinical evaluation of endodontically treated teeth. Oral Surg 1964; 17: 368-374.
2. Yamamoto A, Sawada S, Ono Y, Beppu K, Yamada H, Takeuchi H, Yagasaki T, Takahashi T, Kasahara E, Yasuda E. Clinical long-term observation on endodontically treated teeth. J Conserv Dent 1986; 29: 74-84.
3. Kasahara E, Yasuda E, Yamada H, Miyazawa A. An evaluation of guidelines for the apical enlargement of maxillary
premolars. J Endodon 1991; 17(1): 1-7.
4. Kerekes K, Tronstad L. Morphometric observations on root canals of human anterior teeth. J Endodon 1977; 3: 24-29.
5. Kerekes K, Tronstad L. Morphometric observations on root canals of human premolars. J Endodon 1977; 3: 74-79.
6. Kerekes K, Tronstad L. Morphometric observations on root canals of human molars. J Endodon 1977; 3: 14-18.
7. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984; 58: 589–599.
8. Vertucci FJ. Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc 1974; 89: 369–371.
9. Wu MK, R’Oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 89: 739–743.
10. Mauger MJ, Schindler WG, Walker WA. An evaluation of canal morphology at different levels of root resection in mandibular incisors. J Endod 1998; 24: 607–609.
11. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol 1972; 33: 101–110.
12. Madeira MC, Hetem S. Incidence of bifurcations in mandibular incisors. Oral Surg Oral Med Oral Pathol 1973; 36: 589–591.
13. Miyashita M, Kasahara E, Yasuda E, et al. Root canal system of the mandibular incisor. J Endod 1997; 23: 479–484.

21
14. Boruah LC, Bhuyan AC. Morphologic characteristics of root canal of mandibular incisors in North-East Indian population: an in vitro study. J Conserv Dent 2011; 14: 346–350.
15. Kartal N, Yanikoglu FC. Root canal morphology of mandibular incisors. J Endod 1992; 18(11): 562–564.
16. Katz A, Tamse A. A combined radiographic and computerized scanning method to evaluate remaining dentine thickness in mandibular incisors after various intracanal procedures. Int Endod J 2003; 36: 682–686.
17. Wu MK, Wesselink PR. A primary observation on the preparation and obturation of oval canals. Int Endod J 2001; 34: 137–141.
18. Wu MK, van der Sluis LW, Wesselink PR. The capability of two hand instrumentation techniques to remove the inner layer of dentine in oval canals. Int Endod J 2003; 36: 218–224.
19. De-Deus G, Barino B, Zamolyi RQ, et al. Suboptimal debridement quality produced by the single-file F2 ProTaper technique in oval-shaped canals. J Endod 2010; 36: 1897–1900.
20. Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, Villas-Bôas MH, Amoroso-Silva PA, Brandão CG, Guimarães BM, , Gomes de Moraes I, Húngaro-Duarte MA. Micro–Computed Tomography Analysis of the Root Canal Anatomy and Prevalence of Oval Canals in Mandibular Incisors. J Endod 2013; 39: 1529–1533.

22
Case 4
Endodontic retreatment of the maxillary right second molar
Fig. 1. Frontal view.
Patient 56-year-old Caucasian male.
Chief complaint Non-contributory.
Medical record Ritalin, Paracetamol/codein due to back pain. Heavy smoker.
Dental history The patient was referred to the post-graduate clinic from the student clinic for endodontic retreatment of the maxillary right second molar. A post and crown was planned as restoration. The tooth had been treated endodontically for more than 10 years ago.
Clinical findings September 8th2010 Soft tissue: Gingivitis in the region 15 to 17. An aphthous lesion is seen at the buccal aspect between tooth 17 and 15. Dental: Tooth 15: MOD amalgam filling. Tooth 16: Missing. Tooth 17: MOD amalgam filling, buccal cuspal fracture (Fig. 2).
Fig. 2. Occlusal view.
Clinical tests September 8th2010 14 15 17 EPT 34 39 80 Cold + + - Percussion - - - Palpation - - - PPD 4 4 6 Mobility - - - Biting - - I
Radiographic findings September 8th2010 Dental: Tooth 17: Radiopaque MOD restoration. Tooth 16: Missing. Tooth 15: Radiopaque MOD restoration. A retained root corresponding to the wisdom tooth is seen. Periodontal: Generalized attachment loss. Periapical: Tooth 17 has an apical radiolucency (PAI 4). Tooth 15: A normal PDL space is seen around the root.

23
Diagnosis September 8th2010 Diagnosis Pulpal K04.11 necrotic pulp
K04.19 endodontically treated
Periodontal K05.03 chronic marginal periodontitis Periapical K05.40 chronic apical periodontitis
Treatment plan Non-surgical endodontic retreatment. The patient is told that the prognosis for the tooth is uncertain due to considerably loss of tooth substance.
Problem list Proper tooth isolation and aseptic due to severely damaged tooth (Fig. 2).
Fig. 3. Periapical radiograph 08.09.2010.
Treatment September 8th2010 1 carpule of Xylocaine/adrenaline was applied. The access cavity was refined with burs and all the caries and the former amalgam coronal restoration material was removed. Three orifices with gutta-percha were localised (Fig. 4). A pre-endodontic copper ring was adjusted and semented using IRM (Fig. 5).
Fig. 3. Access cavity.
Fig. 4. Copper ring assortment.
Fig. 5. Placement of copper ring.
Treatment September 15th2010 1 carpule of Septocaine was applied. Mechanical: Burs, prerace and biorace rotary files: MB: #50/0.04 (BR6)/18mm DB: #50/0.04 (BR6)/18mm P: #60/0.02 (BR7)/17mm Chemical: Chloroform, 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.

24
Fig. 6. Working length radiograph.
Treatment November 17th2010 No symptoms, filled with gutta-percha and AH Plus, sealed with IRM.
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph. Sealerpuff is noted, DB root.
Prognosis Endodontic: Good. Tooth: Uncertain.
Follow-up examination November 29th2011 No symptoms. Radiograph shows evidence of healing of the periapical radiolucency.
Fig. 9. Follow-up radiograph 1 year.
Discussion Endodontic therapy is a predictable treatment, resulting in up to 97% retention rate for the treated teeth (1, 2, 3). However, about 3% of endodontically treated teeth require further treatment, including extraction of the tooth. Long-term predictability of restored endodontically treated teeth is important for the decision of tooth retention versus extraction and implant placement. A distinction has to be made between a general treatment outcome and endodontic treatment outcome. Depending on the evaluation criteria used, a general treatment outcome of either natural tooth or dental implant may address retention, functionality, restorative, and, if applicable, periodontal and endodontic success (4). Endodontic treatment success is considered to be achieved by its objective of preventing or eliminating apical periodontitis (5, 6). Healing or continuation of periapical disease is widely regarded to be dependent on the absence or presence of microorganisms and thus on the antimicrobial debridement of the root canal system by cleaning, shaping, and subsequent root filling (7, 8). Nevertheless, additional factors have been found to influence the long-term endodontic outcome of a tooth. Sjögren et al. (9) suggested various factors, such

25
as pre-existing apical periodontitis or adequate length and level of the root canal filling. A variety of other endodontic treatment parameters, restorative factors, and biological variables are considered to influence the endodontic outcome (10). In a patient cohort with 200 teeth investigated by Chugal et al. (11), preoperative pulp and periapical diagnosis, periapical radiolucency size, and the patient’s sex were significantly correlated to the outcome of the endodontic treatment. The strongest influence on postoperative healing was found to be by the presence and magnitude of preoperative apical periodontitis. The apical limit of the obturation has also been identified as a parameter significantly influencing the true endodontic outcome by Bergenholtz et al. (12). In terms of the general treatment outcome, according to Ng et al. (10), four variables could improve the survival of endodontically treated teeth: a crown restoration after endodontic therapy, the presence of mesial and distal approximal contacts, that the tooth will not be used as an abutment for removable or fixed partial dentures, and if the tooth itself was not a molar. A definitive restoration is necessary because the root canal filling itself may not provide the necessary coronal seal that can prevent bacterial penetration and the invasion of oral microorganisms into the root canal system (13). A retrospective investigation of complete-mouth radiographs of patients seen in a university setting found the definitive coronal restoration to be more important for a successful endodontic outcome than the quality of the endodontic filling (14). Nevertheless, different studies showed that both a good coronal restoration and a good endodontic treatment provided the
highest endodontic success (15). Hence, an intact coronal restoration has been found indispensable for the long-term general treatment outcome of the endodontically treated tooth (16). Fuss et al. (17) studied 147 extracted teeth. The most common reason for extraction (44%) was a restorative consideration, with endodontic, endorestorative, and vertical root fracture (VRF) the next most frequent reasons (21%, 19%, and 11%, respectively). Vire (18) found that 59% of 116 extractions of endodontically treated teeth were due to prosthetic reasons, 32% to periodontal reasons, and 9% to endodontic failures. Zadik et al. (19) also analysed factors related to extraction of endodontically treated teeth. In this retrospective study 547 endodontically treated permanent teeth that were extracted in a multidisciplinary clinic in a 2-year period were analyzed. The most common reason for ectraction was nonrestorable caries (61.4%). Other reasons were: endodontic failure (12.1%), VRF and iatrogenic perforation or stripping (8.8% each), periodontal disease (4.6%), unrestorable cusp fracture (2.4%), orthodontic (1.3%) and prosthetic (0.2%) reasons, and trauma (0.5%). Setzer et al. (4) investigated preoperative factors that potentially can provide more information about the long-term survival and predictability of endodontically treated teeth, including age, sex, and restorative, periodontal, and endodontic factors. The authors found that significant positive correlations existed between ‘‘untoward events’’ (any form of retreatment or extraction) and ‘‘prognostic value according to periodontal status’’. They concluded that the only preoperative factors significant for the prognosis of restored endodontically treated molars

26
were related to periodontal prognostic value and attachment loss.
References 1. Salehrabi R, Rotstein I.
Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004; 30: 846–850.
2. Chen SC, Chueh LH, Hsiao CK, et al. An epidemiologic study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J Endod 2007; 33: 226–229.
3. Fonzar F, Fonzar A, Buttolo P, et al. The prognosis of root canal therapy: a 10-year retrospective cohort study on 411 patients with 1175 endodontically treated teeth. Eur J Oral Implantol 2009; 2: 201–208.
4. Setzer FC, Boyer KR, Jeppson JR, Karabucak B, Kim S. Long-Term Prognosis of Endodontically Treated Teeth: A Retrospective Analysis of Preoperative Factors in Molars. J Endod 2011; 37: 21-25.
5. Strindberg LZ. Dependence of the results of pulp therapy on certain factors. An analytical study based on radiographic and clinical follow-up examinations. Acta Odont Scand 1956; 14: 1–175.
6. Ørstavik D. Reliability of the periapical index scoring system. Scand J Dent Res 1988; 96:108–111.
7. Byström A, Happonen R-P, Sjögren U, et al. Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endod Dent Traumatol 1987; 3: 58–63.
8. Sjögren U, Figdor D, Persson S, et al. Influence of infection at the time of root filling on the
outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297–306.
9. Sjögren U, Hagglund B, Sundqvist G, et al. Factors affecting the long-term results of endodontic treatment. J Endod 1990; 16: 498–504.
10. Ng YL, Mann V, Gulabivala K. Tooth survival following non-surgical root canal treatment: a systematic review of the literature. Int Endod J 2010; 43: 171–189.
11. Chugal NM, Clive JM, Spangberg LS. A prognostic model for assessment of the outcome of endodontic treatment: effect of biologic and diagnostic variables. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001; 91: 342–352.
12. Bergenholtz G, Lekholm U, Milthon R, et al. Influence of apical overinstrumentatio and overfilling on retreated root canals. J Endod 1979; 5: 310–314.
13. Torabinejad M, Ung B, Kettering J. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J Endod 1990; 16: 566–569.
14. Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to technical quality of the root filling and the coronal restoration. Int Endod J 1995; 28: 12–18.
15. Tronstad L, Asbjornsen K, Døving L, et al. In- fluence of coronal restorations on the periapical health of en- dodontically treated teeth. Endod Dent Traumatol 2000;16: 218–221.
16. Iqbal MK, Johansson AA, Akeel RF, et al. A retrospective analysis of factors associated with the periapical status of restored,

27
endodontically treated teeth. Int J Prosthodont 2003; 16: 31–38.
17. Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted endodontically treated teeth. Int Endod J 1999; 32: 283-286.
18. Vire DE. Failure of endodontically treated teeth: classification and evaluation. J Endod 1991; 17: 338-342.
19. Zadik Y, Sandler V, Bechor R, Salehrabi R. Analysis of factors related to extraction of endodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(5): 31-35.

28
Case 5
Endodontic treatment of the maxillary left first molar
Fig. 1. Frontal view.
Patient 57-year-old Caucasian male.
Chief complaint Non-contributory.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate clinic from the student clinic for endodontic treatment of the maxillary left first molar.
Clinical findings January 19th2011 Soft tissue: Sinus tract at the buccal aspect of tooth 27, normal findings around tooth 26. Dental: Tooth 25: MOD amalgam restoration. Tooth 26: Fractured composite restoration, caries. Tooth 27: A mixture of amalgam, composite, and temporary filling material is seen.
Fig. 2. Buccal view. A sinus tract is seen at the distal aspect of tooth 27.
Clinical tests January 19th2011 25 26 27 EPT 50 80 80 Cold + - - Percussion - - - Palpation - - - PPD 4 4 12 Mobility - - - Biting - - -
Radiographic findings January 19th2011 Dental: Tooth 27 has a radiopaque MOD restoration, the root canal is filled with a weakly radiopaque filling material. Teeth 25 and 26 have MOD radiopaque filling materials. Periodontal: Moderate attachment loss. Periapical: Apical radiolucencies teeth 26 (PAI 3) and 27 (PAI 4). A normal PDL space is seen around the root of tooth 25.

29
Fig. 3. Periapical radiograph 19.01.2011.
Diagnosis January 19th2011 Diagnosis Pulpal K04.11 necrotic pulp
Periodontal K05.03 chronic marginal periodontitis Periapical K05.40 chronic apical periodontitis
Treatment plan Pre-endodontic treatment restoration and endodontic treatment tooth 26, extraction of tooth 27.
Problem list Obliteration, loss of tooth substance due to caries.
Treatment January 19th2011 1 carpule of Xylocaine/adrenaline was injected. Access opening and removal of caries and former restoration materials. Pre-endodontic composite restoration. Mechanical: Burs, Gates glidden, NiTi handfiles #20, Biorace rotary files: MB: #40/0.04 (BR5) /18mm MB2: #40/0.04(Br5)/20mm DB: #40/0.04 (BR5) /19mm P: #50/0.04 (BR6) /18mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 4. Working-length radiograph.
Treatment February 9th2011 No symptoms. Obturation tooth 26: Buccal roots filled with gutta-percha and AH Plus; Palatal root filled with MTA plug and thermoplastisised gutta-percha and AH Plus. Sealed with IRM.
Fig. 5. Master cone radiograph.
Fig. 6. Post-obturation radiograph.
Prognosis Endodontic: Good. Tooth: Good.

30
Follow-up examination January 27th2012 (1 year) No symptoms. Tooth 26 has been restored with a post and a dental crown. The patient has postponed the extraction of tooth 27 since he had no subjective complaints. Re-informed about the infection related to tooth 27 and recommended to have it extracted as soon as possible. Periapical radiograph shows no sign of regression of apical radiolucency related to tooth 26.
Fig. 7. Follow-up radiograph 1 year.
Follow-up examination June 24th2014 (3.5 years) No symptoms. Tooth 27 was extracted after the last follow-up examination. The apical periodontitis lesion on tooth 26 seems to have healed well.
Fig. 8. Follow-up radiograph 3.5 years.
Discussion The presence of microorganisms in a root canal is the main etiologic factor in the development and continuation of periapical lesions (1, 2, 3). Immunological reactions, in this case periapical lesions, are established in the periapex to combat the infectious agent and promote the repair of the affected region (4). These pathologies cause bone lysis to make room for their organisation and growth. The differential diagnosis of periapical pathologies is confirmed only by means of histological processing (5). Several authors disagree about the prevalence of these pathologies: the prevalence of cystic lesions ranges from 6% (6) to 54% (7), and that of granuloma, from 45% (8) to 97.0% (6, 9). A number of chemical mediators of inflammation, including the cytokines IL-1α, IL-1β, TNFα, prostaglandins and LPS, seem to be related to the pathogenesis of periapical lesions (10,11, 12, 13). These substances may stimulate root resorption in the same way that they stimulate bone resorption (14). Irregular resorbed areas are frequently situated in sites that are not within the reach of root-canal instruments or medication and may act as niches for extraradicular bacterial colonization (15, 16), besides causing technical problems for rootcanal treatment (17, 18). Radiographic examination is not always helpful in the diagnosis of small areas of external root resorption associated with teeth having apical periodontitis. Vier and Figuereido (19) examined 104 root apices from extracted teeth with periapical lesions by means of hematoxylin-eosin (HE) staining and scanning electron microscopy (SEM). Cysts accounted for 24.5% of the samples, 84% of which were associated with marked inflammation. The most prevalent

31
diagnosis was noncystic periapical abscess with varying degrees of severity (63.7%). Periapical granuloma was not a frequent finding. SEM analysis showed that 42.2% of the root apices had periforaminal resorption extending over 50% of their circumference. When the foraminal resorption was evaluated, 28.7% had resorption affecting >50% of the periphery. Only 8.9% of the samples showed no periforaminal or foraminal resorption. In a similar study examinating internal apical resorption the authors found that apical internal resorption was present in 74.7% of 75 examined roots associated with periapical lesions (20). Normally, the failure of root-canal treatment is related to the persistence of infection in the root-canal system (21, 22). The presence of root resorption in teeth with periapical lesions is important for infection control since these areas are niches for bacteria. Moreover, the apical limit of instrumentation may be altered in teeth with widely resorbed apices, since the cementum-dentine junction at the constriction can be missing (17, 18). In such circumstances, sealing the canal may be difficult and overflling is likely. Bacteria may also be found in the external surface of the root, forming a periapical bioflm (23, 24), thus confirming the importance of appreciating the existence of periforaminal root resorption.
References 1. Kakehashi S, Stanley H, Fitzgerald
R. The effects of surgical exposures of dental pulps in germ-free and conventional conventional laboratory rats. Oral Surg, Oral Med Oral Pathol 1965; 20: 340–349.
2. Fabricius L, Dahlen G, Holm S, Möller A (1982) Influence of combinations of oral bacteria on
periapical tissues of monkeys. Scand J Dent Res 1982; 90: 200–206.
3. Lin L, Pascan EA, Skribner J et al. Clinical, radiographic, and histologic study of endodontic treatment failures. Oral Surg Oral Med Oral Pathol 1991; 71: 603–161.
4. Torabinejad M, Bakland L. Immunopathogenesis of chronic periapical lesion. A review. Oral Surg, Oral Med Oral Pathol 1987; 46: 685–699.
5. Linenberg W, Waldron C, Delaune Jr G (1964) A clinical roentgenographic and histopathologic evaluation of periapical lesions. Oral Surg, Oral Med Oral Pathol 1964; 17: 467–472.
6. Block R, Brushell A, Rodrigues H et al. A histopathologic, histobacteriologic, and radiographic study of periapical endodontic surgical specimens. Oral Surg, Oral Med Oral Pathol 1976; 42: 656–678.
7. Priebe W, Lazansky J, Wuehrmann A. The value of the roentgenographic film in the differential diagnosis of periapical lesions. Oral Surg, Oral Med Oral Pathol 1954; 7: 979–983.
8. Lalonde E, Luebke R. The frequency and distribution of periapical cysts and granulomas. Oral Surg, Oral Med Oral Pathol 1968; 25: 861–868.
9. Nair P. Light and electron microscopic studies of root canal flora and periapical lesions. J Endod 1987; 13: 29-39.
10. Schein B, Schilder H. Endotoxin content in endodontically involved teeth. J Endod 1975; 1(1): 19-21.

32
11. Schonfeld SE, Greening AB, Glick DH, Frank AL, Simon JH, Herles SM. Endotoxic activity in periapical lesions. Oral Surg Oral Med Oral Pathol. 1982; 53(1): 82-87.
12. Wang CY, Stashenko P. Characterization of bone- resorbing activity in human periapical lesions. J Endod. 1993;19(3): 107-111.
13. Wang CY, Stashenko P. The role of interleukin-1 alpha in the pathogenesis of periapical bone destruction in a rat model system. Oral Microbiol Immunol. 1993; 8(1): 50-56.
14. Hammarström L, Lindskog S. Factors regulating and modifying dental root resorption. Proc Finn Dent Soc. 1992; 88 Suppl 1: 115-123.
15. Tronstad L, Barnett J, Cervone F. Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod and Dent Traumatol 1990; 6: 73-77.
16. Lomcali G, Sen B, Cancaya H. Scanning electron microscopic observations of apical root surfaces of teethwithapical periodontitis. Endod Dent Traumatol 1996; 12: 70-76.
17. Delzangles B. Scanning electronmicroscopic study of apical and intracanal resorption. J Endod 1989; 15: 281-285.
18. Malueg L,Wilcox L, JohnsonW. Examination of external apical root resorption with scanning electron microscopy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996; 82: 89-93.
19. Vier FV, Figueiredo JAP. Prevalence of different periapical lesions associated with human teeth and their correlation with the presence and extension of
apical external root resorption. Int Endodo J 2002; 35: 710-719.
20. Vier FV, Figueiredo JAP. Internal apical resorption and its correlation with the type of apical lesion. Int Endod J 2004; 37: 730–737.
21. Sjögren U, Figdor D, Persson S, Sundqvist G. In£uence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297-306.
22. Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol 1998; 85: 86-93.
23. Sunde PT, Olsen I, Debelian GJ, Tronstad L. Microbiota of periapical lesions refractory to endodontic therapy. J Endod 2002; 28: 304–310.
24. Wang J, Jang Y, Cheng W, Zhu C, Liang J. Bacterial flora and extraradicular biofilm associated with the apical segment of teeth with post-treatment apical periodontitis. J Endod 2012; 38(7): 954-959.

33
Case 6
Endodontic treatment of the maxillary right first incisor
Fig. 1. Frontal view.
Patient 34-year-old Caucasian male.
Chief complaint He complained about tenderness when chewing and biting on his upper right front tooth. He also had a sensation of slight mobility of this particular tooth. He could not remember any specific trauma to his front teeth.
Fig. 2. Buccal view. Discoloured tooth 11. PPD 6mm.
Fig. 3. Palatal view.
Medical record The patient had a pronounced dental anxiety. He was not using any medicaments.
Dental history The patient was referred to the post-graduate clinic from private practice for evaluation and treatment of the maxillary right first incisor.
Clinical findings November 3rd2010 Soft tissue: Normal findings Dental: Tooth 12: Sound Tooth 11: Discoloration, incisal composite filling. Tooth 21: Composite filling ID. Periodontal: A periodontal pocket of 6mm was probed at the buccal aspect of tooth 11 (Fig. 5).
Clinical tests November 3rd2010 12 21 11 EPT 20 80 10 Cold + - + Percussion - +(v) - Palpation - + - PPD 3 6 3 Mobility - I - Biting - + -
Radiographic findings November 3rd2010 Dental: Tooth 11has an incisal radiopaque restoration. Periodontal: Marginal periodontitis. Periapical: Tooth 11 has a periradicular radiolucency at the midroot to cervical level. Apically there is a continuous PDL space.

34
Fig. 4. Periapical radiograph.
Fig. 5. PPD 6mm.
Diagnosis November 3rd2010 Diagnosis Pulpal K04.11 necrotic pulp Periodontal K05.03 chronic marginal periodontitis Periapical K04.51 chronic lateral periodontitis
Treatment plan Tooth 11: Endodontic treatment of infected pulp.
Problem list Calcification. Root fracture?
Treatment November 3rd2010 2 carpules of Xylocaine/adrenaline was applied, intrapulpal injection was necessary during the treatment session. Access preparation and localisation of
canal orifice, pulp chamber obliteration. Bleeding from canal below the fracture line. Mechanical: Burs, Gates glidden, NiTi handfiles: #45/19mm Chemical: 1% NaOCl, 17% EDTA Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 6. Working-length radiograph.
Treatment November 24th2010 No symptoms. Tooth feels different, but is not tender on percussion compared to neighbouring teeth. Filled with gutta-percha and AH Plus, sealed with composite.
Fig. 7. Master cone radiograph.

35
Fig. 8. Post-obturation radiograph.
Prognosis Endodontic: Uncertain. Tooth: Uncertain.
Follow-up examination July 4th2011 (7 months) Asymptomatic. Reduction of periodontal pocket (4mm). Less mobility.
Fig. 9. Periapical control radiograph 04.07.2011.
Follow-up examination March 18th2013 (2.5 years) Asymptomatic. Periodontal pocket unchanged (4mm). Lateral radiolucency is seen in relation to fracture line. Observation.
Fig. 10. Periapical control radiograph 2.5 years.
Discussion An intra-alveolar fracture in the cervical part of the root is a rare injury; reported frequencies vary between 6% and 19% of intra-alveolar root fractures (1-5). The prognosis is considered to be poor due to a short mobile coronal fragment, with less probability of healing with hard tissue, and possible bacterial contamination of necrotic pulp tissue from the gingival crevice (6, 7). However, it has also been shown that cervical fractures may heal and a conservative approach, including a relatively long splinting period, has been recommended (8-11). Type of fracture healing was classified by Andreasen & Hjörting-Hansen (8): 1) Healing with interposition of hard tissue: healing with hard tissue, fragments are in close contact and the fracture line is not visible or indistinctly outlined; 2) Healing with interposition of bone and soft tissue (PDL) between the fragments: fragments are separated by ingrowth of hard tissue surrounded by periodontal ligament-like tissue; 3) Healing with interposition of soft tissue (PDL): fragments are close but separated by a distinct radiolucent line and there is rounding-up of the fracture edges; 4) No healing: persistent or a widened space between the fragments and the presence of a radiolucency in the alveolar bone adjacent to the root fracture.

36
Cvek et al. (12) evaluated 94 cervical root fractures .The teeth were divided into two groups according to type of fracture: 1: transverse fractures limited to the cervical third of the root (51 incisors) and 2: oblique fractures involving both the cervical and middle parts of the root (43 incisors). Healing of the fracture with hard tissue formation was observed in 17 teeth (18%), healing with interposition of periodontal ligament (PDL) and, in some cases, hard tissue between the fragments in 62 teeth (66%), and fifteen teeth (16%) showed no healing and a radiolucency adjacent to the fracture. Neither the frequency nor the type of fracture healing differed significantly between the two groups (transverse versus oblique). Andreasen et al. (13) analysed the long-term tooth loss after root fractures and assessed the influence of the type of healing and the location of the root fracture in 492 root-fractured teeth in 432 patients. The location of the root fracture had a strong significant effect on tooth survival. The 10-year tooth survival of apical root fractures was 89%, of mid-root fractures 78%, of cervical-mid-root fractures 67%, and of cervical fractures 33%. The fracture-healing type offered further prognostic information. No tooth loss was observed in teeth with hard tissue fracture healing regardless of the position of the fracture. For teeth with interposition of connective tissue, the location of the fracture had a significant influence on tooth loss. For teeth with connective tissue healing, the estimated 8-year survival of apical, mid-root, and cervical-mid-root fractures were all more than 80%, whereas the estimated 8-year survival of cervical fractures was 25%. Horizontal root fractures due to dental trauma generally do not result in pulp necrosis (14). The incidence of tooth survival in the cervical third is lower
(30%) than the incidence in the middle (86%) and apical thirds (96%) (14). In the present case, the tooth required endodontic treatment, probably because of infection via the periodontal pocket that resulted in necrosis of the coronal fragment. Clinical examination of root fractures should evaluate tooth colour, sensitivity to percussion, mobility, and sensitivity to thermal stimulation (15). This case showed slight mobility (grade 1), which can be explained by the cervical location of the fracture line. There was no response to the cold test, one can argue that this could be explained by the obliteration of the coronal pulp space; the dental crown showed yellow discoloration, which also may be a clinical sign of mineralization of the pulp chamber. Although in most cases of horizontal root fracture, testing the pulp elicits a positive response, a negative response may be recorded (16) when there is calcification. This negative response does not necessarily indicate a need for endodontic therapy. However, in this case, a radiolucency in the alveolar bone adjacent to fracture was evident, indicating the need for endodontic treatment. In the study by Cvek et al. (14) no healing, i.e. pulp necrosis and appearance of radiolucency in the periradicular bone, next to the root fracture, with or without widening of the space between fragments, occurred in 109 (20%) of the 534 intra-alveolar root fractured teeth.
References 1. Lindahl B. Transverse intra-
alveolar root fractures. Roentgen diagnosis and prognosis. Odontol Revy 1958; 9: 10–24.
2. Austin LT. A review of forty cases of retained fractured roots of

37
anterior teeth. J Am Dent Assoc 1930; 17: 1930–1932.
3. Zachrisson BU, Jacobsen I. Long-term prognosis of 66 permanent anterior teeth with root fracture. Scand J Dent Res 1975; 83: 345–354.
4. Ravn JJ. En klinisk og radiologisk undersögelse af 55 rodfrakturer i unge permanente incisiver. Tandlaegebladet 1976; 80: 391–396.
5. Andreasen FM, Andreasen JO, Bayer T. Prognosis of rootfractured permanent incisors - prediction of healing modalities. Endod Dent Traumatol 1989; 5: 11–22.
6. Feiglin B. Clinical management of transverse root fractures. Dent Clin North Am 1995; 39: 53–78.
7. Andreasen FM, Andreasen JO. Root fractures. In: Andreasen, JO, Andreasen, FM, editors. Textbook and color atlas of traumatic injuries to the teeth, 3rd edn. Copenhagen: Munksgaard; 1994: 301–314.
8. Andreasen JO, Hjörting-Hansen E. Intraalveolar root fractures. radiographic and histologic study of 50 cases. J Oral Surg 1967; 25: 414–426.
9. Andreasen JO. Treatment of fractured and avulsed teeth. ASDC J Dent Child 1971; 38: 29–48
10. Benati FW, Biggs JT. Management of traumatized incisor teeth with horizontal fractures. Okla Dent Assoc J 1994; 85: 30–3.
11. Yates JA. Root fractures in permanent teeth: a clinical review. Int Endod J 1992; 25:150–157.
12. Cvek M, Mejàre I, Andreasen JO. Healing and prognosis of teeth with intra-alveolar fractures involving the cervical part of the
root. Dent Traumatol 2002; 18: 57–65.
13. Andreasen JO, Ahrensburg ss, Tsilingaridis G. Root fractures: the influence of type of healing and location of fracture on tooth survival rates – an analysis of 492 cases. Dent Traumatol 2012; 28: 404–409.
14. Cvek M, Tsilingaridis G, Andreasen JO. Survival of 534 incisors after intra-alveolar root fracture in patients aged 7–17 years. Dent Traumatol 2008; 24: 379–387.
15. S. Patel, D. Ricucci, C. Durak, F. Tay. Internal root resorption: a review. J Endod 2010; 36: 1107–1121.
16. Andreasen FM, Andreasen JO, Cvek M. Root fractures. In: Andreasen JO, Andreasen FM, Andersson L, editors. Textbook and color atlas of traumatic injuries to the teeth, 4th edn. Kopenhagen: Blackwell Munksgaard; 2007: 337–371.

38
Case 7
Endodontic retreatment of the maxillary left first molar
Fig. 1. Frontal view.
Patient 29-year-old Caucasian male.
Chief complaint Non-contributory.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate clinic from the student clinic for endodontic retreatment of the maxillary right first molar. A crown is planned.
Clinical findings October 25th2011 Soft tissue: normal findings Dental: 25: Sound. 26: Discoloured and leaking composite filling (ODP) with underlying cavity/caries (Fig. 2). 27: Sound.
Fig. 2. Occlusal-palatal view.
Clinical tests October 25th2011 25 26 27 EPT Nd Nd Nd Cold + - + Percussion - - - Palpation - - - PPD 3 3 3 Mobility - - - Biting - - -
Radiographic findings October 25th2011 Dental: Tooth 26 has an MOD radiopaque filling material. The root canals seem poorly filled with a weakly radiopaque material. Periodontal: Within normal limits. Periapical: Widening of PDL space tooth 26, apical radiolucencies mesiobuccal and palatal root (PAI 3). Normal PDL space around tooth 25 and 27.
Fig. 3. Periapical radiograph 25.10.2011

39
Diagnosis October 25th2011 Diagnosis Pulpal K04.11 necrotic pulp
K04.19 endodontically treated
Periodontal within normal limits Periapical K05.40 chronic apical periodontitis
Treatment plan Non-surgical retreatment. A crown is planned after endodontic retreatment.
Problem list Obliteration.
Treatment October 25th2011 1 carpule of Xylocaine/adrenaline was applied to establish anaesthesia. Access preparation, caries removal and locating the untreated MB canal (MB2). Mechanical: Burs, NiTi handfiles #20, Biorace rotary files: MB2: #40/0.04 (Br5)/18mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 4. Working-length radiograph MB2.
Treatment November 2nd2011 1 carpule of Xylocaine/adrenaline was applied to establish anaesthesia. Gutta-percha was removed. Prepared the canals using NiTi hand files and BioRace rotary files: MB: #40/0.04 (Br5)/19.5mm DB: #40/0.04 (Br5)/19mm (step) P: #50/0.04 (Br6)/19.5mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 5. Working-length radiograph MB and P canals.
Fig. 6. Working length radiograph DB canal.
Treatment November 9th2011 No symptoms. Master cone radiograph. The canals were filled with AH Plus and gutta-percha with a cold lateral condensation technique. A small sealer puff is noted at the apex of the palatal root (Fig. 8).

40
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph 09.11.2011.
Prognosis Endodontic: Good. Tooth: Good.
Follow-up examination March 8th2012 (1 year) No symptoms. The tooth had been restored at the student clinic with a crown. Radiograph shows evidence of healing of the periapical radiolucency.
Fig. 9. Follow-up radiograph 1 year.
Follow-up examination April 15th2013 (2 years) No symptoms. Radiograph shows healing of the periapical radiolucency.
Fig. 10. Follow-up radiograph 2 years.
Discussion Successful root canal therapy requires a thorough knowledge of root and root canal morphology. Root canal anatomy variations present a constant challenge in successful diagnosis and endodontic treatment, especially the multirooted teeth. A classic study by Hess (1) showed pulp spaces to be complex systems. Numerous studies since then have continued to help define the anatomy, morphology, and dimension of the human dentition, with the common denominator being that certain root systems are more complex than others. One such system is found in the mesiobuccal (MB) root of maxillary molars (2-5). The broad buccolingual dimension of the mesiobuccal root and associated concavities on its mesial and distal surface is consistent with the majority of the mesiobuccal roots having two canals while there is usually a single canal in each of the distobuccal and palatal roots (6, 7). In a literature review of the root canal morphology of the human permanent maxillary first molar (8399 teeth from 34 studies) the incidence of two canals in the mesiobuccal root was 56.8% and of one canal was 43.1% in a weighted

41
average of all reported studies. The incidence of two canals in the mesiobuccal root was higher in laboratory studies (60.5%) compared to clinical studies (54.7%). Less variation was found in the distobuccal and palatal roots and the results were reported from fourteen studies consisting of 2576 teeth. One canal was found in the distobuccal root in 98.3% of teeth whereas the palatal root had one canal in over 99% of the teeth studied (8). The use of operating microscopes has facilitated the localization and handling of additional canals, especially the second mesiobuccal canal (MB2) in maxillary first molars. Buhrley et al. (9) investigated the effect of magnification on locating the MB2 canal in maxillary molars. The participating endodontists documented 312 cases of root canal therapy on maxillary first and second molars. Participants that used the microscope or dental loupes located the MB2 canal with a frequency of 57.4% and 55.3%, respectively. Those using no magnification located the MB2 canal with a frequency of 18.2% (9). Failure to detect and treat the second MB2 canal system will result in a decreased long-term prognosis (10). Stropko (11) observed that by scheduling adequate clinical time, by using the recent magnification and detection instrumentation aids and by having thorough knowledge of how and where to search for MB2, the rate of location can approach 93% in maxillary first molars.
References 1. W. Hess. 1925. The Anatomy of
the Root Canals of the Teeth of the Permanent Dentition. John Bale, Sons and Danielson, Ltd, London.
2. Bjorndal AM, Skidmore AE. 1987. Anatomy & Morphology of
Human Teeth (2nd ed.) Iowa City: University of Iowa Press.
3. Vertucci FJ. The endodontic significance of the mesiobuccal root of the maxillary first molar. US Navy Med 1974; 63: 29–31.
4. Weine FS, Healey, Gerstein H, et al. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol 1969; 28: 419–425.
5. F.J. Vertucci FJ. 1984. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984; 58: 589–599.
6. Walton R, Torabinejad M. 1996. Principles and practice of endodontics (2nd ed). W.B. Saunders Co, Philadelphia.
7. Ash M, Nelson S. 2003. Wheeler’s dental anatomy, physiology and occlusion (8th ed) Saunders, Philadelphia.
8. Cleghorn BM, Christie WH, Dong CC. Root and Root Canal Morphology of the Human Permanent Maxillary First Molar: A Literature Review. J Endod 2006; 32(9): 813-821.
9. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod 2002; 28: 324–327.
10. Wolcott J, Ishley D, Kennedy, Johnson S, Minnich S. Clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars J Endod 2002; 28: 477–479.
11. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod 1999; 25: 446–450.

42
Case 8
Endodontic retreatment of the mandibular left first molar
Fig. 1. Frontal view.
Patient 34-year-old Asian male.
Chief complaint Non-contributory.
Medical record Non-contributory.
Dental history The patient was referred to the postgraduate clinic from the student clinic for retreatment of the mandibular left first molar prior to prosthetics (crown). The tooth had been root filled approximately 15 years ago. Previous attempts to retreat the tooth had been made at the student clinic.
Clinical findings April 21st2010 Soft tissue: Normal findings. Dental: Tooth 35: Occlusal amalgam restoration. Tooth 36: Leaking amalgam restoration (MODL) with caries and occlusal temporary filling material. Tooth 37: Composite filling (MO).
Fig. 2. Occlusal view.
Clinical tests April 21st2010 35 36 37 EPT 22 80 66 Cold + - + Percussion - - - Palpation - - - PPD 3 3 3 Mobility - - - Biting - - -
Radiographic findings April 21st2010 Dental: Tooth 36 has an MOD radiopaque filling material. The tooth has an insufficient root filling. The root canals seem to be calcified apically. Periodontal: Within normal limits. Periapical: Normal PDL space around tooth 35, 36 and 37.

43
Fig. 3. Periapical radiograph.
Diagnosis April 21st2010 Diagnosis Pulpal K04.11 necrotic pulp
K04.19 endodontically treated
Periodontal Within normal limits Periapical Within normal limits
Treatment plan Non-surgical endodontic retreatment.
Problem list Negotiation of obliterated root canals.
Treatment April 21st2010 1 carpule of Septocaine was applied to establish anaesthesia. Access preparation and localisation of 3 canal orifices. Partially removing the old gutta-percha. Obliterated canals. Mechanical: Burs, Gates glidden, Hedstrøm hand files. Chemical: Chloroform, 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 4. Working length radiograph.
Treatment September 7th2010 1 carpule of Septocaine was injected. Access preparation and localisation of D canal, bleeding from canal. Attempt to negotiate mesial canals using ultrasound was unsuccessful. Mechanical: Burs, NiTi hand files: D: #50/0.02 23mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: Cavit, IRM.
Fig. 5. Working length radiograph. D canal.
Treatment September 12th2010 No symptoms. 1 carpule of Septocaine was injected. MB and ML canals were filled with ProRoot MTA, D canal was filled with gutta-percha and AH Plus using a cold lateral condensation technique. Moistened cotton pellet applied over MTA. Temporary filling: Cavit, IRM.

44
Fig. 6. Master cone radiograph.
Fig. 7. MTA in mesial canals.
Fig. 8. Filled with GP/AH+ distal canal.
Treatment November2nd2010 IRM plugs mesial canals, tooth filled with composite.
Fig. 9. IRM plugs.
Fig. 10. Tooth restored with composite.
Prognosis Endodontic: Uncertain. Tooth: Uncertain.
Follow-up examination February 6th2012 No symptoms. A crown with a post was made at the student clinic. No visible apical pathology on periapical radiograph.
Fig. 11. Follow-up radiograph 2 years.
Discussion Strindberg (1) stated in 1956 that the highest success rate is obtained when the root filling is confined to 1 mm from the radiographic apex. In the ideal endodontic case, the root canal is patent from the orifice to the apical foramen. However, this is not always the case. Canals may be obliterated by denticles or secondary dentin formation, or the anatomy of the root may prevent

45
proper instrumentation. There are various opinions in the literature regarding the prognosis for endodontic treatment of such canals. According to Strindberg (1) the prognosis is good even in teeth with nonvital pulps. Molven (2) studied, in vitro, forty-six root canals in which the pulps had been amputated or partially root filled 5 years or more previously and in which no root canals were visible in intraoral radiographs apical to the amputation or end of the root fillings. On radiographs taken after extraction, twenty-nine canals could be traced partially or for their whole length. When the canals were instrumented in the laboratory, using a standardized procedure, ten canals were found to be penetrable, twenty-six were diagnosed as non-penetrable, and complications occurred in ten canals (breakage of instrument/obstruction caused by filling material). A complete obliteration in the total length was not found in any canal. In a study by Åkerblom et al. (3), looking at the outcome of obliterated root-filled teeth that were root-filled only one third of the root length, clinical and radiographic follow-up examinations were performed for 2 to 12 years. The criteria for obliteration were: (a) The root canal was not patent for more than one-third of the root length, (b) No root canal lumen was visible on the radiographs apical to the instrumented portion. Teeth with obliterated root canals were treated endodontically without any surgical procedure. The overall success rate was found to be 89%. When the preoperative periapical status was taken into consideration, the success rate for roots with an intact periapical contour was 97.9%. An accessory canal is any branch of the main pulp canal that communicates with the external surface of the root. A lateral canal is an accessory canal located in the coronal or middle third of the root,
usually extending horizontally from the main root canal (4). Ramifications can be observed anywhere along the length of the root, but they occur more commonly in the apical portion and in posterior teeth (5). In 73.5% of the cases, ramifications are found in the apical third of the root, in 11% in the middle third, and in 15% in the coronal third (6). Ricucci et al. (7) reviews and reports on the histopathologic and histobacteriologic status of the tissue in lateral canals and apical ramifications (LC/AR) in diverse clinical conditions as well as in response to endodontic treatment. Serial sections from 493 human tooth specimens obtained by extraction or apical surgery. They found that LC/AR were observed in about 75% of the teeth. Chemo mechanical preparation partially removed necrotic tissue from the entrance of LC/AR, whereas the adjacent tissue remained inflamed, sometimes infected, and associated with periradicular disease. In cases in which lateral canals appeared radiographically ‘‘filled,’’ they were actually not obturated, and the remaining tissue in the ramification was inflamed and enmeshed with the filling material.
References
1. Strindberg LZ. The dependence of the results of pulp therapy on certain factors. An analytic study based on radiographic and clinical follow-up examinations. Acta Odontol Scand 1956; 14(Suppl 21).
2. Molven O. Nonpenetrable root canals as assessed by a standardized instrumentation procedure. Oral Surg Oral Med Oral Pathol 1973: 95(2): 232-237.
3. Akerblom A, Hasselgren G. The Prognosis for Endodontic

46
Treatment of Obliterated Root Canals J Endod 1988; 14: 565-567.
4. DeDeus QD. Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod 1975; 1: 361–6.
5. Vertucci FJ. Rootcanal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984; 58: 589–599.
6. Vertucci FL. Root canal
morphology and its relationship to endodontic procedures. End topics 2005; 10: 3-29.
7. Ricucci D, Siqueira JF. Fate of the Tissue in Lateral Canals and Apical Ramifications in Response to Pathologic Conditions and Treatment Procedures. J Endod 2010; 36: 1–15.

47
Case 9
Endodontic retreatment of the maxillary left first incisor
Fig. 1. Frontal view.
Patient 15-year-old Caucasian male.
Chief complaint Non-contributory.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate clinic from the public dentistry for retreatment of the maxillary left first incisor. The tooth had recently been rootfilled but the referring dentist was unhappy with the result. The patient had a trauma to his upper front teeth 7 years earlier (2004).
Clinical findings August 24th2011 Soft tissue: Normal findings. Dental: Teeth 11 and 21 have coronal composite build-ups. Tooth 21 has a palatal temporary filling.
Fig. 2. Buccal view.
Fig. 3. Palatal view.
Clinical tests August 24th2011 22 21 11 12 EPT 43 80 66 45 Cold + - - - Percussion - - - - Palpation - - - - PPD 2 3 2 2 Mobility - - - - Biting - - - -
Radiographic findings August 24th2011 Dental: Tooth 21 has a radiopaque coronal restoration and a radiopaque root filling material. Periodontal: Within normal limits. Periapical: Tooth 21 has an apical radiolucency (PAI 3).

48
Fig. 4. Periapical radiograph 24.08.2011.
Fig. 5. Working-length radiograph.
Diagnosis August 24th2011 Diagnosis Pulpal K04.19 endodontically treated Periodontal within normal limits Periapical K05.40 chronic apical periodontitis
Treatment plan Endodontic retreatment.
Problem list Apical resorption?
Treatment August 24th2011 Access opening and localization of gutta-percha. Iatrogenic push-out of gutta-percha during removal (Fig. 5). Mechanical: Bur, Gates Glidden, Hedstrøm handfiles, DeRace rotary files, NiTi handfiles: #60/24mm adjusted to 23.5mm Chemical: Chloroform, 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Treatment September 28th2011 Asymptomatic. Access and removal of remaining gutta-percha.
Mechanical: Bur, Hedstrøm handfiles, NiTi handfiles, root-canal enlargement: #90/23.5mm (Fig. 6). Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 6. Removal of GP with iatrogenic protrusion apically.
Treatment November 11th2011 Asymptomatic. Filled with gutta-percha and AH Plus, sealed with IRM.

49
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph.
Prognosis Endodontic: Uncertain. Tooth: Good.
Follow-up examination March 18th2013 (2 years) The patient is asymptomatic. Radiograph shows uncertain healing.
Fig.9. Follow-up radiograph 2 years.
Follow-up examination April 7th2014 (3 years) The patient is still asymptomatic. Radiograph shows improved, but uncertain healing.
Fig. 10. Follow-up radiograph 3 years.
Discussion Several follow-up studies (1-6) have concluded that apical overfilling is associated with an impaired prognosis. This opinion has been based on studies that include observation periods mostly in the range of 2-4 years. Strindberg (1) however, followed up some cases for up to 10 years, and he occasionally noticed a reduction in the volume of excess fillings over the longer periods.

50
Halse & Molven (7) re-examined 239 root-filled teeth after 10-17 years and concluded that apical overfilling per se had little influence on the long-term healing result as judged radiographically. In about 80% of the cases of overfilling, no excess root filling material could be traced at the reexamination. In a few cases only, the appearance of the excess material was nearly identical to that at the time of treatment, whereas the remaining overfillings (18%) showed a reduced size. Among the recorded variables only one seemed to have a major impact on the prognosis-namely, the presence or absence of an apical radiolucency at the time of treatment, indicating that infection was the important factor when failures occurred. Yusuf (8) found in his study of periapical granulomas that “foreign” material was present in 96/284 specimens. Whilst dentin and cementum chips often was associated with active inflammation, extruded root-filling materials were generally associated with the formation of scar tissue. Healing of the periapical lesion may occasionally occur by means of fibrous scar tissue, which appears as a periapical radiolucency indistinguishable from that seen in failed endodontic treatment (9). In one study (10) scar tissue healing was observed at the apices of teeth that had previously undergone periapical curettage; it was concluded that a periapical scar develops only after periapical surgery. However, in another histopathologic study, 2.5% of 2308 specimens were diagnosed as periapical scars, most of which occurred at the apices of conventionally rootfilled teeth (11). In the study by Nair et al. (9), the observation of scar tissue in 2 specimens indicated that after root canal treatment the periapical lesions healed with soft connective tissue with no signs of inlammation.
References 1. Strindberg LZ. The dependence of
the results of pulp therapy on certain factors. An analytic study based on radiographic and clinical follow-up examinations. Acta Odontol Scand 1956;14(suppl 21).
2. Grahnen H, Hansson L. The prognosis of pulp and root canal therapy. A clinical and radiographic follow-up examination. Odontol Rev 1961; 12: 146-165.
3. Storms JL. Factors that influence the success of endodontic treatment. J Can Dent Assoc 1969; 35: 83-97.
4. Seltzer S, Bender IB, Turkenkopf S. Factors affecting successful repair after root canal therapy. J Am Dent Assoc 1963; 67: 651-662.
5. Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endodont 1979; 5: 83-90.
6. Bergenholtz G, Lekholm U, Milthon R, Engstrom B. Influence of apical overinstrumentation and overfilling on re-treated root canals. J Endodont 1979; 5: 310-314.
7. Halse A, Molven O. Overextended gutta-percha and Kloroperka N-O root canal fillings. Radiographic findings after 10-17 years. Acta Odontol Scand. 1987; 45(3): 171-177.
8. Yusuf H. The significance of the presence of foreign material periapically as a cause of failure of root treatment.. Oral Surg Oral Med Oral Pathol. 1982; 54(5): 566-574.
9. Nair PNR, Sjögren U, Figdor D, Göran Sundqvist G. Persistent periapical radiolucencies of root-

51
filled human teeth, failed endodontic treatments, and periapical scars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87: 617-627.
10. Seltzer S, Bender IB, Smith J, Freedman I, Nazimov H. Endodontic failures: an analysis based on clinical, roentgenographic, and histologic findings. Oral Surg Oral Med Oral Pathol 1967; 23: 500-530.
11. Bhaskar SN. Periapical lesion: types, incidence, and clinical features. Oral Surg Oral Med Oral Pathol 1966; 21: 657-671.

52
Case 10
Endodontic treatment of a maxillary anterior tooth
Fig. 1. Frontal view.
Patient 61-year-old Caucasian female.
Chief complaint Pain in the mucosa above the maxillary left front tooth, sometimes-unprovoked radiating pain.
Medical record The patient has dental fear. She explains about traumatic experiences related to treatment of the upper front teeth after a trauma in childhood.
Dental history The patient was referred to the post-graduate clinic from private practice for endodontic treatment of the maxillary left first incisor. She had a trauma (traffic accident) to her anterior teeth as a child and the teeth were restored with aluminium crowns until the age of 18. After that the metallic-ceramic dental crowns (Fig. 1-3) were made.
Clinical findings May 27th2014 Soft tissue: Normal. Dental: Teeth 21 and 11 have dental crowns (Fig. 2, 3).
Fig. 2. Buccal view.
Fig. 3. Palatal view.
Clinical tests May 27th2014 23 22 21 11 EPT Nd Nd Nd Nd Cold + - - - Percussion - - +,h Palpation - - - - PPD 3 3 3 3 Mobility - - - Biting - - - -
Radiographic findings May 27th2014 Dental: Teeth 21 and 11 have radiopaque dental crowns. Periodontal: Within normal limits. Periapical: Tooth 21 has an apical radiolucency (PAI 3). Widened PDL space around the apex of tooth 11. A continuous PDL space is seen around the root of tooth 22.

53
Fig. 4. Periapical radiograph 27.05.2014.
Fig. 5. Locating the canal orifice.
Diagnosis May 27th2014 Diagnosis Pulpal K04.11 necrotic pulp Periodontal K05.01 chronic gingivitis Periapical K04.50 chronic apical periodontitis
Treatment plan Endodontic treatment of tooth 21.
Problem list Dental anxiety. Pulp canal obliteration in the coronal half of the canal space.
Treatment May 27th2014 The patient cried during the first visit. She was afraid that the crown would be destroyed, however, she wanted to treat the tooth due to pain. 1 carpule of Xylocaine/adrenaline was injected. Access opening and careful localisation of the canal orifice with the aid of radiographs (Fig. 5). Mechanical: Burs, LN burs. Chemical: 17% EDTA. Temporary filling: IRM.
Treatment June 3rd2014 1 carpule of Xylocaine/adrenaline was injected. Access opening and relocalization of canal orifice. Mechanical: Bur, NiTi hand instrumentation #20, RECIPROC one file endo: #40/0.04/23.5mm Chemical: 0.5% chlorhexidine, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 6. Working-length radiograph.

54
Treatment June 17th2014 No symptoms. Filled with gutta-percha and AH Plus, sealed with composite.
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph.
Prognosis Endodontic: Good. Tooth: Good.
Follow-up examination (phone call) September 9th2014 (3 months) The patient has no symptoms; no longer tender when palpating over the root.
Discussion Crown fractures of the permanent dentition comprise the most frequent form of traumatic dental injuries. Since enamel-dentin crown fractures expose a large number of dentinal tubules, pathways to the pulp are established for a variety of noxious agents present in the oral environment including bacteria and toxins (1-4). Therefore, to prevent pulpal injury, coverage of the exposed dentin would seem important. However, the effect of length of dentin exposure on pulpal response has been controversial. On the one hand this assumption is supported by a clinical study where pulpal necrosis (PN) was significantly increased in untreated crown fractured teeth with extensive dentin exposure (5). But, in teeth with functional, vital pulp tissue, dentin provides considerably resistance to bacterial ingress. Classical studies (6-8) suggest that persistent bacterial provocation of exposed dentin, even in conjunction with resin restoration (9), tends to result in pulpal inflammatory lesions of limited duration. Cavalleri and Zerman (10) did a follow-up study of 84 crown fractured permanent incisors with incomplete root formation over a 5-year period. Four of 67 teeth (6%) with fracture of the enamel and dentine without pulpal involvement showed PN and 1 tooth showed pulp canal obliteration (PCO) (1.5%). Eight of 14 teeth (57%) with fractures of the enamel and dentine with pulp involvement showed PN. Robertson (11) did a retrospective evaluation of patients with uncomplicated crown fractures and luxation injuries. A total of 241 patients with 545 injured teeth were available for clinical examination. In addition, 82 permanent incisors presenting with pulp canal obliteration were followed for a period of 7 to 22 years (mean 16 years). The findings showed little pulpal

55
response to crown fracture and subsequent restorative procedures as long as there was no concomitant periodontal injury (15-year follow-up). PCO was found in all luxation categories. According to the survival curve the 20-year pulp survival rate diagnosed radiographically was 84%. Although the risk of PN increased with time, routine endodontic intervention of teeth with on-going PCO of the root canal did not seem justified (11). Robertson et al. (12) investigated pulp-healing responses following crown fracture in 455 teeth with or without pulp exposure and luxation. The observation period ranged from 6 months to 17 years (mean 2-3 years). Crown fractures without luxation showed pulp survival (PS) in 99 %, PCO in 1 % and PN in 0 % of the cases. With concomitant luxation PS was observed in 70 %, PCO in 5 % and PN in 25 %. Their findings support the idea that in teeth with an intact pulpal circulation, dentin can provide considerable resistance to bacterial invasion (13).
References 1. Hørsted-Bindslev P, Simonsen A-
M, Larsen MJ. Monkey pulp reactions to restorative materials. Scand J Dent Res 1986; 94: 154-163.
2. Bergenholtz G, Cox CF, Loesche WJ, Syed SA. Bacterial leakage around dental restorations: its effect on the dental pulp. Oral Pathol 1982; 11: 439-450.
3. Brännström M, Nyborg H. Pulpal reactions to composite resin restorations. J Prosth Dent 1972; 27: 181-189.
4. Brännström M, Vojinovic O. Response of the dental pulp to invasion of bacteria around three filling materials. ASCD J Dent for children 1976; 43: 15-21.
5. Ravn JJ. Follow-up study of permanent incisors with enamel-dentin fractures after acute trauma. Scand J Dent Res 1981: 89: 355-365.
6. Lundy T, Stanley HR. Correlation of pulp histopathology and clinical symptoms in human teeth subjected to experimental irritation. Oral Surg 1969; 27: 187-201.
7. Lervik T, Mjör IA. Evaluation of techniques for the induction of pulpitis. J Biol Bucc 1977; 5: 137-148.
8. Warfvinge J, Bergenholtz G. Healing capacity of human and monkey dental pulps following experimentally induced pulpitis. Endod Dent Traumatol 1986; 2. 256-262.
9. Felton D, Bergenholtz G, Cox CF. Inhibition of bacterial growth under composite restorations following CLUMA pretreatment. Dent Res 1989; 68: 491-495.
10. Cavalleri G, Zerman N. Traumatic crown fractures in permanent incisors with immature roots: a follow-up study. Endod Dent Traumatol 1995; 11(6): 294-296.
11. Robertson A. A retrospective evaluation of patients with uncomplicated crown fractures and luxation injuries. Endod Dent Traumatol 1998; 14(6): 245-256.
12. Robertson A1, Andreasen FM, Andreasen JO, Norén JG. Long-term prognosis of crown-fractured permanent incisors. The effect of stage of root development and associated luxation injury. Int J Paediatr Dent. 2000; 10(3): 191-199.
13. Bergenholtz G. Pathogenic mechanisms in pulpal disease. J Endod 1990; 16: 98-101.

56
Case 11
Patient with persistent pain maxilla left side
Fig. 1. Frontal view.
Patient 32-year-old Caucasian male.
Chief complaint The patient is complaining about occasional throbbing pain (once a week) in the left side of maxilla. The pain mainly arises after consumption of red wine and the tooth pain often comes with a temporary headache. He describes the pain as ”nerve pain”. The pain started after a root canal treatment of the maxillary left first molar. The pain persisted after endodontic treatment and the tooth was later retreated two times without any relieve of symptoms. He is not using any pain medications.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate endodontic clinic from private practise for apicoectomy of the maxillary left first molar. Tooth 26 had been treated endodontically several times.
Clinical findings April 11th2014 Soft tissue: Normal findings. Dental: Tooth 25: Composite fillings. Tooth 26: Large composite restoration (MODP), temporary occlusal filling, chronic caries. Tooth 27: Composite fillings, chronic caries.
Fig. 2. Occlusal view.
Clinical tests April 11th2014 26 27 EPT Nd Nd Cold - + Percussion + + Palpation - - PPD 3 3 Mobility - - Biting - -
Radiographic findings April 11th2014 Dental: Teeth 25, 26, 27 have radiopaque restoration materials. Tooth 26 has a radiopaque root filling material.

57
Periodontal: Normal findings. Apical: Teeth 25 and 27 have continuous PDL spaces. Tooth 26 uncertain findings mesial root; flush root canal filling. Based on uncertain clinical and radiographic findings, the patient was referred for cone-beam CT (CBCT).
Fig. 3. Periapical radiograph.
Fig. 4. Periapical radiograph.
Diagnosis April 11th2014 Diagnosis Pulpal K04.19 endodontically treated
Periodontal within normal limits Periapical within normal limits Nerve disorders G50.10 atypical facial pain?
Treatment plan CBCT referral. Treatment alternative: Surgical retreatment of the mesial root of the
endodontically treated maxillary left first molar.
Problem list Neuropathic pain.
Prognosis Tooth: uncertain
Radiologic description (in Norwegian) from the Department of Maxillofacial Radiology, May 6th2014

58
Fig. 5. CBCT.
Follow-up examination May 27th2014 Information about CBCT findings. The patient is advised to have a permanent filling in tooth 26, preferably a dental crown, and a general caries check.
Follow-up examination (phone call) September 30th2014 Fewer symptoms from the tooth. He feels some ”discomfort” approximately once a month. He has not decided if he wants to keep the tooth and have a crown made. At present, he is waiting for his dentist to return after maternity leave.
Discussion Persistent pain associated with teeth after nonsurgical or surgical endodontic treatment has been used as an indicator of treatment failure (1, 2). However, pain may be experienced in a tooth or adjacent site in the absence of clinical or radiographic signs of dental disease. Failure to detect pathological change on
periapical radiographs may reflect limitations of the diagnostic method rather than an absence of an osteolytic lesion (3, 4). Superimposition of adjacent anatomical structures over the suspect tooth may further obscure the view. Conversely, residual periapical disease may be truly absent and the pain may be nonodontogenic. Nonodontogenic dentolalveolar pain is often difficult to diagnose because it is poorly understood (5, 6). Nonodontogenic pain in the dentoalveolar region can arise from four potential processes: 1) referred musculoskeletal pain disorder, 2) neuropathic pain disorder, 3) headache disorders presenting in the dentoalveolar region, and 4) a pathological process outside the immediate dentoalveolar region that refers pain to that area, such as sinus disease, salivary gland disorders, brain tumors, angina, throat cancer, and craniofacial vascular disorders (7, 8). Pain in a tooth site of neurogenic origin has been reported in the literature (9, 10) but only a few published studies (9-14) have investigated the occurrence of neuropathic pain after dental treatment. Evidence of the association between dental treatment and chronic neuropathic pain has been presented by Marbach (11), Schnurr & Brooke (12) and Vicker et al. (13), who reported that most patients diagnosed with atypical odontalgia related the onset of the pain to dental treatment, dental infection or dental trauma. Only three epidemiological studies (9, 10, 14) have investigated the prevalence of chronic neuropathic pain after dental treatment. The study by Marbach et al. (9) was conducted by a single endodontist, who mailed questionnaires to patients 1 month following nonsurgical endodontic treatment. Only female patients were included in their analyses because the

59
male sample was considered too small. Of the 256 female patients assessed, 20 (9%) reported persistent pain during the period of survey but only 11 female patients attended for clinical and radiographic examination to exclude an odontogenic cause of pain. Of the 11 patients, eight (3% of 256 female patients) were diagnosed with ‘phantom toothache’. Campbell et al. (10) carried out a similar survey of patients who had undergone surgical endodontic treatment 2 years previously and found that 59 (5%) of the 118 patients suffered from chronic pain that divided equally into two groups; post-traumatic stress dysaesthesia (absence of pain preoperatively) and phantom tooth pain (presence of pain preoperatively). In contrast, Berge (14) found none of the 1035 patients in their survey suffered from chronic neuropathic pain following surgical removal of third molars 5–6 years previously. Polycarpou et al. (15) investigated the prevalence of persistent pain after endodontic treatment and factors affecting its occurrence in cases with complete radiographic healing. 175 patients/teeth were reviewed 12–59 months following treatment. The prevalence of persistent pain after successful root canal treatment was 12% (21/175). A positive history of previous chronic pain experience or painful treatment in the orofacial region, and female gender were important risk factors associated with persistent pain after successful endodontic treatment. Marbach (16) has suggested that a deafferentation pain syndrome may be triggered by pulp amputation. Support for this theory comes from the work of Hu & Sessle (17) who showed that somato-sensory pathways alter as a result of removal of pulp tissue in cats. Nixdorf et al. (7) conducted
a systematic review of prospective studies that reported the frequency of nonodontogenic pain in patients who had undergone endodontic procedures. In their study, 3.4 % of patients experienced persistent pain of nonodontogenic origin for 6 months or more after root canal therapy. In rare cases, chronic persistent tooth pain does not respond to dental treatment. Some of these cases might be due to neuropathic pain disorders induced by nerve injuries sustained during endodontic procedures. Neuropathic pain is defined as a pain initiated or caused by a primary lesion in or dysfunction of the nervous system. Clinically, neuropathic pain is characterized by partial or complete somatosensory change in the innervation territory of a specific part of the peripheral or central nervous system along with the paradoxical presence of pain and hypersensitivity phenomena (18). Several studies have reported that endodontic procedures are related to the development of neuropathic tooth pain (NTP) (9, 10, 19-23). NTP is also known as atypical odontalgia (21) and phantom tooth pain (PTP) (9, 20). Some cases of chronic tooth pain related to endodontic procedures have been reported in which repeated dental treatments failed to provide pain relief (20, 21). One study reported that the incidence of NTP after endodontic procedures was greater than that after any other dental treatment such as tooth extraction and trauma (23). Furthermore, 3 retrospective studies have reported that 3%–12% of patients developed NTP after endodontic procedures (9, 10, 15). Oshima et al. (18) conducted another retrospective study of 271 patients who had chronic persistent tooth pain that did not respond to endodontic procedures despite the absence of

60
”major pathology”. Pain predominantly occurred in the maxilla (14 patients). In 10 patients (62.5%), NTP developed after retreatment. The majority of patients were female. Daily application of tricyclic antidepressants produced pain relief in 11 patients (68.8%).
References 1. Rahbaran S, Gilthorpe MS,
Harrison SV, Gulabivala K. Comparison of clinical outcome of periapical surgery in Endodontic and Oral Surgery units of a teaching Dental Hospital: a retrospective study. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, Endod 2001; 91: 700–709.
2. Hoskinson SE, Ng Y-L, Moles D, Hoskinson AE, Gulabivala K. Comparison of outcome or root canal treatment using two different protocols. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, Endod 2002; 93: 705–715.
3. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone. Part I. J Am Dent Assoc 1961; 62: 152–160.
4. Shoha RR, Dowson J, Richards AG. Radiographic interpretation of experimentally produced bony lesions. Oral Surg 1974; 38: 294–303.
5. Israel HA, Ward JD, Horrell B, et al. Oral and maxillofacial surgery in patients with chronic orofacial pain. J Oral Maxillofac Surg 2003; 61: 662–667.
6. deSiqueira SRDT, Nobrega JCM, Valle LBS, et al. Idiopathic trigeminal neuralgia: clinical aspects and dental procedures. Oral Surg Oral Med Oral Path Oral Rad Endod 2004; 98: 311–315.
7. Nixdorf DR, Moana-Filho EJ, Law AS, McGuire LA, Hodges JS, John MT. Frequency of Nonodontogenic Pain after Endodontic Therapy: A Systematic Review and Meta-Analysis. JOE 2010; 36 (9): 1494-1498.
8. Mattscheck D, Law AS, Nixdorf DR. Diagnosis of nonodonogentic toothache. In: Hargreaves KM, Cohen S, eds. Cohen’s pathways of the pulp. 10th ed. St. Louis, MO: Mosby Inc. 2011: 49–70.
9. Marbach JJ, Hulbrock J, Segal AG. Incidence of phantom tooth pain. Oral Surg, Oral Med, Oral Pathol. 1982; 53: 190–193.
10. Campbell RL, Parks KW, Dodds RN. Chronic facial pain associated with endodontic therapy. Oral Surg, Oral Med, Oral Pathol. 1990; 69: 287–290.
11. Marbach JJ. Phantom tooth pain. J Endod 1978; 4: 362–372.
12. Schnurr RF, Brooke RI. Atypical Odontalgia. Update and comment on long term follow up. Oral Surg, Oral Med, Oral Pathol 1992; 73: 445–448.
13. Vicker ER, Cousins MJ, Walker S, Chisholm K . Analysis of 50 patients with atypical odontalgia: a preliminary report on pharmacological procedures for diagnosis and treatment. Oral Surg, Oral Med, Oral Pathol, Endod 1998; 85: 24–32.
14. Berge TI. Incidence of chronic neuropathic pain subsequent to surgical removal of impacted third molars. Acta Odont Scand 2002; 60: 108–112.
15. Polycarpou N, Ng YL, Canavan D, Moles DR, Gulabivala K. Prevalence of persistent pain after endodontic treatment and factors affecting its occurrence in cases with complete radiographic

61
healing. Int Endod J. 2005; 38(3): 169-178.
16. Marbach JJ. Is Phantom tooth pain a deafferentation (neuropathic) syndrome? Part 1 Evidence derived from the pathophysiology and treatment. Oral Surgery, Oral Medicine, Oral Pathology 1993; 75. 95–105.
17. Hu JW, Sessle BJ. Effects of tooth pulp deafferentation on nociceptive neurons of the feline trigeminal subnucleus caudalis. Journal of Neurophysiology 1989; 61: 1197–1206.
18. Oshima K, Ishii T, Ogura Y, Aoyama Y, Katsuumi I. Clinical Investigation of Patients Who Develop Neuropathic Tooth Pain After Endodontic Procedures. J Endod 2009; 35: 958–961.
19. Vickers ER, Cousins MJ. Neuropathic orofacial pain: part 1—prevalence and pathophysiology. Aust Endod J 2000; 26: 19–26.
20. Battrum DE, Gutmann JL. Phantom tooth pain: a diagnosis of exclusion. Int Endod J 1996; 29: 190–194.
21. Lilly JP, Law AS. Atypical odontalgia misdiagnosed as odontogenic pain: a case report and discussion of treatment. J Endod 1997; 23: 337–339.
22. Matwychuk MJ. Diagnostic challenges of neuropathic tooth pain. J Can Dent Assoc 2004; 70: 542–546.
23. Lynch ME, Elgeneidy AK. The role of sympathetic activity in neuropathic orofacial pain. J Orofac Pain 1996; 10: 297–305.

62
Case 12
Endodontic retreatment and apical surgery of the maxillary right canine
Fig. 1. Frontal view.
Patient 65-year-old Caucasian female.
Chief complaint Tender to palpation.
Medical record Non-contributory.
Dental history Tooth 13 was endodontically treated by general practitioner 5 years ago (due to apical periodontitis). History of a sinus tract. Tooth 12 is going to be extracted and an implant or a dental bridge is planned. The patient was referred to the post-graduate endodontic clinic for retreatment and complementary apical surgery of tooth 13.
Clinical findings May 18th2011 Soft tissue: A sinus tract is evident apically region 13. Dental: Teeth 11, 12 and 13 have dental crowns.
Fig. 2. Buccal view.
Clinical tests May 18th2011 11 12 13 EPT 80 80 80 Cold + - - Percussion - +(v) - Palpation + + - PPD 3 3 3 Mobility - - Biting - - -
Radiographic findings May 18th2011 Dental: Teeth 13 and 12 have radiopaque dental crowns. A radiopaque root filling material is seen in both teeth. Periodontal: Attachment loss. Apical: An apical radiolucency is seen around the root of tooth 13 (PAI 4). Widened PDL space apically around the root of tooth 12.

63
Fig. 3. Periapical radiograph.
Diagnosis May 18th2011 Diagnosis Pulpal K04.19 endodontically treated
Periodontal K05.03 chronic marginal periodontitis Periapical K05.40 chronic apical periodontitis
Treatment plan Orthograde retreatment and complementary apical surgery tooth 13.
Problem list Gingival recession and aesthetics.
Treatment May 18th2011 1 carpule of Septocaine was injected. Access opening and localization of gutta-percha (GP). Not able to remove all GP apically. Mechanical: Burs, Gates glidden, Prerace, NiTi hand files: #60/23mm adjusted to 22.5 mm Chemical: Chloroform, 1% NaOCl, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 4. Working length radiograph.
Treatment August 31th2011 The patient is asymptomatic. Access opening and attempt to remove GP in the apical part of the canal. Apical perforation and bleeding at the tip of paper point. Adjustment of working length and enlargement. Mechanical: Burs, Hedstrøm- and NiTi hand files: #70/21.5mm Chemical: Chloroform, 1% NaOCl, 17% EDTA. Filled with gutta-percha and AH Plus Sealed with IRM plug and composite.
Fig. 5. Master cone radiograph.

64
Fig. 6. Post-obturation radiograph.
Surgery September 28th2011 The patient was given a chlorhexidine mouth rinse and local anaesthetic was injected. A marginal incision was made running from tooth 11 to tooth 14 with a vertical releasing incision on the distal aspect of 14. Elevation of the mucoperiosteal flap revealed pathological fenestration and extruded GP. Osteotomy and curettage of granulation tissue. Biopsy. Root-end resection 3mm and retrograde preparation with ultrasonic instruments. Haemostasis using resorbable surgicel and ferric sulphate. A retrograde filling of white MTA was applied. The operation site was rinsed with sterile saline and the flap sutured in place with supramide 4.0. Administration of Ibux 400mg. Postoperative instructions.
Fig. 7. Marginal incision. Pathologic fenestration apically, tooth 13.
Fig. 8. Osteotomy. Extruded GP is visible.
Fig. 9. Root end resection 3mm.
Fig. 10. Periapical radiograph, root-end preparation.
Fig. 11. Root-end filling using white MTA.

65
Fig.12. Periapical radiograph to see placement of root-end filling.
Fig. 13. Suturing.
Prognosis Endodontic/surgery: Good. Tooth: Good.
Follow-up examination October 11th2011 (2 weeks) The patient had no postoperative complaints. Suture removal.
Fig. 14. Follow-up (2 weeks).
Follow up examination January 26th2012 (4 months) Asymptomatic. Healing of apical radiolucency.
Fig. 15. Periapical control radiograph 4 months.
Follow up examination May 14th2013 (2 years) Asymptomatic. The apical radiolucency seems to have healed well.
Fig. 16. Periapical control radiograph 2 years.
Radiograph from general practitioner September 4th2013
Fig. 17. Periapical radiograph 04.09.2013.

66
Discussion Non-surgical endodontic treatment is a predictable and reliable treatment with high success rates ranging from 86%–98% (1, 2). Nevertheless, for a variety of reasons, endodontic failure still occurs, and presence of clinical signs and symptoms along with radiographic evidence of periapical bone destruction indicates the need for retreatment (3, 4). Etiologic factors of endodontic failure can be placed into 4 groups (5): (1) persistent or reintroduced intraradicular microorganism, (2) extraradicular infection, (3) foreign body reaction, and (4) true cysts. Among those, many studies reported that microorganisms in the root canals or periradicular lesions play a major role in the persistence of apical periodontitis after a root canal treatment (6-8). Non-microbial factors have also been suggested as a potential cause of post-treatment disease (9), but evidence is relatively weak as it comes from a few case reports. Endodontic failure related to microorganisms can be caused by procedural errors such as root perforation, ledge formation, separated instruments, and missed canals, as well as anatomical difficulties such as apical ramification, isthmuses, and other morphologic irregularities (8, 10). Song et al. (11) examined the clinical causes of failure and the limitation of previous endodontic treatment by examining the root apex and resected root surface at 26x magnification during endodontic microsurgery. A total of 493 roots were analysed. The most common possible cause of failure was a leaky canal (30.4%), followed by a missing canal (19.7%), under filling (14.2%), anatomical complexity (8.7%), overfilling (3.0%), iatrogenic problems (2.8%), apical calculus (1.8%) and apical cracks (1.2%).
Post-treatment disease has been demonstrated to be highly associated with intraradicular infection by studies using microscopy (12-14), culture (15, 16) or molecular methods (17, 18, 19). The outcome of treatment has been shown to be poorer when bacteria persist in the root canals at the time of filling (20, 21). This may indicate that residual bacteria can survive in treated canals for many years and induce or sustain periradicular tissue inflammation. Extraradicular infections are usually associated with acute inflammation, clinically characterised by an abscess with accompanying pain and swelling, or a sinus tract. However, it has been suggested that in some cases an extraradicular infection may be associated with chronic inflammation and lead to endodontic treatment failure. This condition may be associated with a biofilm formation on the external root surface (22), sometimes showing calculus-like calcifications (23), or forming cohesive actinomycotic colonies within the body of the lesion (24). There are some few case reports that suggest that some lesions may not heal because of endogenous or exogenous non-microbial factors (25). Endogenous causes include cholesterol crystals and true cysts, whereas exogenous causes comprise foreign-body reactions to apically extruded filling materials, paper points or food (14, 26). Nevertheless, in most of these cases it is difficult to rule out the concomitant presence of infection as the cause of the disease.
References 1. Friedman S, Abitbol S, Lawrence
HP. Treatment outcome in endodontics: the Toronto Study—phase 1: initial treatment. J Endod 2003; 29: 787–793.

67
2. Setzer FC, Boyer KR, Jeppson JR, Karabucak B, Kim S. Long-term prognosis of endodontically treated teeth: a retrospective analysis of preoperative factors in molars. J Endod 2011; 37: 21–25.
3. Barbizam JV, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J Endod 2002; 28: 365–366.
4. De Cleen MJ, Schuurs AH, Wesselink PR, Wu MK. Periapical status and prevalence of endodontic treatment in an adult Dutch population. Int Endod J 1993; 26: 112–119.
5. Nair R. Pathology of apical periodontitis. In: Ørstavik D, Pitt Ford TR, eds. Essential Endodontology: Prevention and Treatment of Apical Periodontitis, 2nd ed. Boston, MA: Blackwell Science; 2008: 68–88.
6. Sundqvist G, Figdor D, Persson S, Sjogren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 86–93.
7. Gomes BPFA, Pinheiro ET, Jacinto RC, Zaia AA, Ferraz CCR, Souza-Filbo FJ. Microbial analysis of canals of root-filled teeth with periapical lesions using polymerase chain reaction. J Endod 2008; 34: 537–540.
8. Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod 1992; 18: 625–627.
9. Siqueira JF, Rocas IN, Ricucci D, Hülsmann N. Causes and management of post-treatment
apical periodontitis. Brit Dent J 2014; 216: 305-312.
10. Lin LM, Rosenberg PA, Lin J. Do procedural errors cause endodontic treatment failure? J Am Dent Assoc 2005; 136: 187–193.
11. Song M, Kim HC, Lee W, Kim E. Analysis of the Cause of Failure in Nonsurgical Endodontic Treatment by Microscopic Inspection during Endodontic Microsurgery. J Endod 2011; 11: 1516-1519.
12. Nair P N, Sjögren U, Krey G, Kahnberg K E, Sundqvist G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. J Endod 1990; 16: 580–588.
13. Ricucci D, Siqueira J F Jr. Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod 2010; 36: 1277–1288.
14. Ricucci D, Siqueira J F Jr., Bate A L, Pitt Ford T R. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod 2009; 35: 493–502.
15. Sundqvist G, Figdor D, Persson S, Sjögren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 86–93.
16. Pinheiro E T, Gomes B P, Ferraz C C, Sousa E L, Teixeira F B, Souza-Filho F J. Microorganisms from canals of root-filled teeth with periapical lesions. Int Endod J 2003; 36: 1–11.

68
17. Siqueira J F Jr, Rôças I N. Polymerase chain reaction-based analysis of microorganisms associated with failed endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 97: 85–94.
18. Rôças I N, Siqueira J F Jr. Characterization of microbiota of root canal-treated teeth with posttreatment disease. J Clin Microbiol 2012; 50: 1721–1724.
19. Schirrmeister J F, Liebenow A L, Pelz K et al. New bacterial compositions in root-filled teeth with periradicular lesions. J Endod 2009; 35: 169–174.
20. Fabricius L, Dahlén G, Sundqvist G, Happonen R P, Möller A J R. Influence of residual bacteria on periapical tissue healing after chemomechanical treatment and root filling of experimentally infected monkey teeth. Eur J Oral Sci 2006; 114: 278–285.
21. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297–306.
22. Tronstad L, Barnett F, Cervone F. Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod Dent Traumatol 1990; 6: 73–77.
23. Ricucci D, Martorano M, Bate A L, Pascon E A. Calculus-like deposit on the apical external root surface of teeth with post-treatment apical periodontitis: report of two cases. Int Endod J 2005; 38: 262–271.
24. Happonen R P. Periapical actinomycosis: a follow-up study of 16 surgically treated cases. Endod Dent Traumatol 1986; 2: 205–209.
25. Nair P N. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med 2004; 15: 348–381.
26. Koppang H S, Koppang R, Solheim T, Aarnes H, Stolen S O. Cellulose fibres from endodontic paper points as an etiological factor in postendodontic periapical granulomas and cysts. J Endod 1989; 15: 369–372.

69
Case 13
Endodontic retreatment in conjunction with apical surgery of the mandibular right first molar with a separated instrument
Fig. 1. Frontal view.
Patient 54-year-old Caucasian male.
Chief complaint He has no symptoms at present, but he complains about several episodes of pain and swelling in the lower right mandible. His dentist/doctor has prescribed antibiotics (AB) at several occasions due to tooth pain.
Medical record The patient is diagnosed with Bechterev. He has dental fear. Medicaments: Celebra, Prednisolone.
Dental history Concomitant with the last AB regimen the patient was referred to the postgraduate clinic from private practice for retreatment of the mandibular right first molar. Tooth 46 was endodontically treated many years ago. At several occasions the last year, the patient received dental emergency treatment consisting of AB prescriptions for tooth pain related to the specific tooth.
Clinical findings September 28th2010 Soft tissue: Normal findings Dental: Tooth 44 has an occlusal amalgam filling and a buccal composite filling. Buccal caries is noted along the composite margins. A craze line is seen at the buccal aspect, running in an occlusal-cervical direction. Tooth 45 has a dental crown. Tooth 46 has a composite restoration with a small buccal amalgam filling, and there is caries along the margins of the restorations.
Fig. 2. Buccal view.
Fig. 3. Lingual view.

70
Clinical tests September 28th2010
44 45 46 EPT 25 12 80 Cold + + - Percussion - - - Palpation - - - PPD 3 3 3 Mobility - - - Biting - - -
Radiographic findings September 28th2010 Dental: Tooth 46 has a radiopaque filling material. A radiopaque root canal filling material and a separated instrument in the mesial root is seen. Tooth 45 has a radiopaque dental crown and a radiopaque root filling material. Periodontal: Within normal limits Apical: An apical radiolucency around the root of tooth 46 is seen (PAI 4). A normal PDL space is seen around the root of tooth 45.
Fig. 4. Periapical radiograph 28.09.2010.
Diagnosis September 28th2010 Diagnosis Pulpal K04.19 endodontically treated
Periodontal Within normal limits Periapical K04.50 chronic apical periodontitis
Treatment plan Non-surgical retreatment of the endodontically treated right mandibular first molar and observation.
Problem list Instrument removal and negotiation of apical third.
Treatment September 28 th2010 1 carpule of Septocaine was injected. Access opening and localization of old GP and of untreated DL canal. Mechanical: Burs, Gates glidden, Hedstrøm files, NiTiFlex hand files: MB: #40/18.5mm ML: #40/20.5 DB: #40 /18.5mm DL: #40/21.5mm Chemical: Chloroform, 1% NaOCl, 17% EDTA. Intracanal medicament: CaOH2 Temporary filling: Cavit, IRM
Fig. 5. Working length radiograph.
Treatment October 26th2010 History: The patient experienced a flare-up three days ago during physical workout. Emergency treatment at the student clinic: Prescription of phenoxymethylpenicillin and paracetamol/codein. At present: Tooth is tender on biting only.

71
Fig. 6. Periapical radiograph 26.10.2010.
Mechanical: NiTiFlex hand files, adjusting working lengths according to apex locator: MB: #40/18.5mm ML: #40/21mm DB: #40 /21mm DL: #40/23mm Chemical: 1% NaOCl, 17% EDTA, 2% chlorhexidine-di-gluconate. Intracanal medicament: Chlorhexidine-di-gluconate /CaOH2. Temporary filling: Cavit, IRM.
Treatment November 23rd2010 The patient has no symptoms. Tooth 46 filled with gutta-percha and AH Plus. Sealed with IRM.
Fig. 7. Master cone radiograph.
Fig. 8. Post-obturation radiograph 23.11.2010.
Prognosis Endodontic: Uncertain. Tooth: Uncertain.
Follow-up examination August 23rd2011 (8 month) The patient describes another history of flare-up and antibiotic treatment in June 2011 at private practice. Radiographic findings 23.08.2011: Radiolucency seemed unchanged from November 2010. Treatment plan: Surgical retreatment of the endodontically treated mandibular right first molar.
Fig. 9. Periapical radiograph 23.08.2011.
Fig. 10. Orthopanthogram 23.08.2011.

72
Surgical treatment September 21th2011 The patient was given a chlorhexidine mouth rinse and local anaesthetic was injected. A marginal incision was made running from tooth 43 to tooth 46 with vertical releasing incisions at the distal aspect of 46 and mesial aspect of 43. Elevation of the mucoperiosteal flap. Osteotomy and curettage of granulation tissue. Biopsy. Root-end resection and retrograde preparation with ultrasonic instruments. Fractured instrument in mesial root removed simultaneously with resected root. Adrenalin and ferric sulphate haemostasis. Retrograde filling of IRM was applied. The operation site was rinsed with sterile saline and the flap sutured in place with supramide 4.0 and 5.0. Postoperative instructions.
Fig. 11. Buccal view of operation site.
Fig. 12. Enucleation of lesion.
Fig. 13. Root resection 3mm.
Fig. 14. Root-end preparation.
Fig. 15. Root-end filling with IRM.
Prognosis Surgery: Good. Tooth: Good.
Follow up examination September 27th2011 (1 week) The patient experienced mild post-operative discomfort. Suture removal. A secondary healing pattern was observed in the posterior region and the patient was advised to rinse with chlorhexidine for another week.

73
Follow up examination October 8th2013 (2 years) Asymptomatic, a crown is now planned. Radiograph shows healing of apical radiolucency.
Fig. 16. Periapical control radiograph 2 years.
Discussion Procedural accidents have a negative effect on healing and might contribute to the persistence of infections in inaccessible apical areas, requiring surgical intervention. The failure of nonsurgical root canal treatment is commonly related to the presence of residual bacteria (persistent infection) or the reinfection of a previously disinfected root canal environment (secondary infection) (1). Unsuccessful outcomes can be attributed to persistent intraradicular infections found in previously un-instrumented canals, dentinal tubules, or the complex irregularities of the root canal system (2, 3, 4). The extraradicular causes of endodontic failures include periapical actinomycosis, a foreign-body reaction caused by extruded endodontic materials, the accumulation of endogenous cholesterol crystals in the apical tissues, and an unresolved cystic lesion (5-8). Previous procedural accidents may have a negative effect on healing. Besides, they might contribute to the establishment of infections at inaccessible apical areas, requiring a surgical intervention (9). In different European countries, epidemiological studies have shown an
elevated number of teeth to be retreated resulting in periapical radiolucencies from poor root-canal therapies (10). Gorni & Gagliani (11) studied 254 molars, 107 premolars, and 91 single-root anterior teeth and found that the success rate was significantly lower in teeth with altered root canal morphology (47%) compared with teeth in which no significant anatomical changes were made by the former endodontic treatment (86,8%). Formerly treated teeth with persistent periapical lesions might be preserved with nonsurgical retreatment, assuming the tooth is restorable and periodontally sound. Bergenholtz et al. (12) reported a success rate of 78% in teeth with periapical pathologies and 94% in teeth without. Sundqvist et al. (13) reported an overall success rate of 74% of 50 cases examined after retreatment. They found that the success rate in bacteria-free canals was almost 80%; whereas in teeth with particular bacterial species the outcome was significantly lower (66%). In a study by Sjögren et al. (14), similar results were achieved and further considerations were made regarding the size of the lesions: the greater the lesion, the lower the success rate. Chugal et al. (15) confirmed these results. Some authors have reported better clinical results with surgical procedures compared with orthograde retreatment (16), although others have reported similar clinical outcomes using both techniques with slight differences related only to the time element. Kvist & Reit (17) did a randomized clinical study comparing surgical and nonsurgical procedures. They failed to show any systematic difference in the outcome of surgical and nonsurgical endodontic retreatment. Surgical retreatment seemed to result in more rapid periapical bone fill, but also might imply a higher risk of ”late failures”.

74
Torabinejad el al. (18) performed a systematic review to compare the outcomes of nonsurgical and surgical retreatment. They concluded that while endodontic surgery demonstrates more favourable initial healing, this declines with increasing recall periods. Conversely, nonsurgical retreatment shows improved outcomes with increasing recall time.
References 1. Siqueira JF Jr. Reaction of
periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics 2005;10: 123–147.
2. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod 1999; 25: 446–450.
3. Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J 2006; 39: 249–281.
4. Ricucci D, Siqueira JF Jr. Anatomic and microbiologic challenges to achieving success with endodontic treatment: a case report. J Endod 2008; 34: 1249–1254.
5. Tronstad L, Barnett F, Cervone F. Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod Dent Traumatol 1990; 6: 73–77.
6. Nair PN, Sjögren U, Krey G, Sundqvist G. Therapy-resistant foreign body giant cell granuloma at the periapex of a root-filled human tooth. J Endod 1990; 16: 589–595.
7. Nair PN. Cholesterol as an aetiological agent in endodontic failures: a review. Aust Endod J 1999; 25: 19–26.
8. Nair PN, Pajarola G, Schroeder HE. Types and incidence of
human periapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996; 81: 93–102.
9. Wu MK, Dummer PM, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. Int Endod J 2006; 39: 343–356.
10. Eriksen HM. Endodontology-epidemiological considerations. Endod Dent Traumatol 1991; 7: 189–195.
11. Gorni FGM, Gagliani MM. The Outcome of Endodontic Retreatment: A 2-yr Follow-up. J Endod 2004; 30: 1-4.
12. Bergenholtz G, Lekholm U, Milthon R, et al. Retreatment of endodontic fillings. Scand J Dent Res 1979; 87: 217–224.
13. Sundqvist G, Fidgor D, Persson S, et al. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative retreatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 86–93.
14. Sjögren U, Hagglund B, Sundqvist G, et al. Factors affecting the longterm results of endodontic treatment. J Endodon 1990; 16: 498–504.
15. Chugal NM, Clive JM, Spångberg LS. A prognostic model for assessment of the outcome of endodontic treatment: effect of biologic and diagnostic variables. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001; 91: 342–352.
16. Danin J, Stromberg T, Forsgren H, et al. Clinical management of nonhealing periradicular pathosis. Surgery versus endodontic retreatment. Oral

75
Surg Oral Med Oral Pathol Oral Radiol Endod 1996; 82: 213–217.
17. Kvist T, Reit C. Results of endodontic retreatment: a randomized clinical study comparing surgical and nonsurgical procedures. J Endodon 1999; 25: 814–817.
18. Torabinehad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 2009: 35: 930-937.

76
Case 14
Explorative surgery of the maxillary left second incisor with sinus tract
Patient 72-year-old Caucasian male.
Chief complaint The patient complains about spontaneous pain and tenderness when chewing in the front region of the upper left maxilla. The pain is worse in the morning.
Medical record Non-contributory.
Dental history The patient was referred to the postgraduate clinic from a specialist in endodontics for apicoectomy of the maxillary left lateral incisor. The tooth was root filled one year ago (2010) by the referring specialist due to apical periodontitis. One year later (2011) the patient presented with pain and a sinus tract was evident.
Clinical findings October 19th2011 Soft tissue: A draining sinus tract was evident at the distal aspect of tooth 22. Dental: Tooth 22 had a distopalatal composite filling.
Clinical tests October 19th2011 22 EPT Nd Cold Nd Percussion +v,h Palpation + PPD Mobility I Biting +
Radiographic findings October 19th2011 Dental: Tooth 22 has a non-radiopaque distal filling and a radiopaque coronal filling material. The root canal is filled with a homogeneous radiopaque material. Periodontal: Moderate attachment loss. Periapical: Tooth 22 has an apical circumferential radiolucency (PAI 5).
Fig. 1. Periapical radiograph 19.10.2011.

77
Fig. 2. Sinus tract.
Diagnosis October 19th2011 Diagnosis Pulpal K04.19 endodontically treated
Periodontal K05.03 chronic marginal periodontitis Periapical K04.69 chronic apical periodontitis
with sinus tract
Treatment plan Explorative surgery tooth 22.
Problem list Root fracture?
Surgery October 19th2011 1. Local anaesthetic (xylocaine/adrenaline), 2. Sulcular flap from tooth 24 to tooth 11D, vertical releasing incision 11D, 3. Curettage of granulation tissue and removal of ”sulphur granules”, 4. Biopsy and microbiological sample, 5. Root resection mid-root level due to incomplete root fracture (visualized with the aid of methylene blue), 6. Haemostasis, and 7. Suturing. A sinus tract draining through the alveolar bone incisally between tooth 22 and tooth 23 was evident (Fig. 3).
Fig. 3. Draining sinus tract.
An incomplete vertical root fracture was evident in the apical part of the root; resection was done at the mid-root level (Fig. 3.). Tooth 22 was kept in place as temporary restoration and the tooth was stabilized with a dentine adhesive and a composite restoration to the neighbouring teeth.
Fig. 4. Root resection. "Sulphur granules" is seen in the soft tissue lesion.

78
Fig. 5. Dissected "sulphur granules".
Fig. 6. Suturing.
Follow-up treatment October 25th2011 Suture removal. The patient was asymptomatic.
Prognosis The tooth has to be extracted.
Follow-up examination August 29th2014 The patient has a well-functioning brigde replacing tooth 22.
Fig. 7. Periapical radiograph 29.08.2014.
Bacteriological findings (with DNA-DNA hybridization); Diagnostic service, Institute of Oral Biology
• Porphyromonas gingivalis in high concentrations.
• Gram-negative enteric bacilli in high concentrations
• Additional findings: o Treponema socranskii
subsp. socranskii o Eubacterium saburreum o Prevotella nigrescens o Fusobacterium nucleatum
subsp. vincentii o Campylobacter rectus o Actinomyces viscosus o Actinomycis gerenceriae o Streptococcus
intermeduíus o Fusobacterium nucleatum
subsp. polymorphum o Porphyromonas
endodontalis

79
Results SEM (scanning electron microscopy); Institute of Oral Biology, Steinar Stølen
Fig. 8. SEM photo shows Gram-negative bacilli on root cementum.
Fig. 9. SEM of cut surface of sulphur granule. The granule consists of an abundance of bacteria. Rod-like organisms are prominent.
Discussion Microorganisms are able to survive and induce persistent infection in extraradicular areas (1, 2). The endodontic treatment of teeth with periapical lesions is less successful than that of teeth with vital pulp or with pulp necrosis without radiographically visible periapical lesions (3). Some studies have revealed that bacteria can form a biofilm surrounding the apical foramina and external root surfaces that is associated with persistent periapical infections (4).
Wang et al. (5) evaluated the presence of extraradicular biofilm on the external surface of the root apex in teeth with different pulp and periapical pathological conditions. They found that teeth with vital pulp and pulp necrosis without radiographically visible periapical lesions did not have exposed apical root cementum or extraradicular bacteria. The detection rates of extraradicular biofilm in teeth with primary chronic periapical periodontitis and persistent periapical periodontitis were 30% and 100%, respectively. Actinomycosis is a chronic, granulomatous infectious disease characterized by suppuration, abscess formation, and draining sinus tracts. In tissues, Actinomyces species grow in microscopic or macroscopic clusters, that sometimes exude from soft tissues through sinus tracts, and because of their yellowish appearance, they are commonly referred to as sulphur granules, even though there is no clear evidence that they contain sulphur at all (1, 6). It has been recognized that granules can provide the bacteria with protection against phagocytosis or other immunologic mechanisms. The patient in the present case had a persistent sinus tract. A sinus tract is defined as a passage of pus from an abscess cavity to and external environment through a tissue membrane such as the oral mucosa or the skin. The reason that a sinus tract develops is not fully understood. Mortensen et al. (7) investigated 1600 teeth with periapical lesions; 136 (9.0%) teeth had sinus tracts. They found that the size of the radiolucency seemed to matter, because teeth with periapical lesions smaller than 5 mm had sinus tracts in 5% of cases, whereas teeth with periapical lesions greater than or equal to 5 mm had sinus tracts in 19%.

80
Some studies have suggested that the odontogenic sinus tract is lined with epithelium (8, 9). Valderhaug (10) studied experimentally induced sinus tracts in monkeys. He found that most of the sinus tracts were completely or partly lined with epithelium. However, studies by Grossman (11) and Bender and Seltzer (12) state that the sinus tract is not lined with epithelium, but lined with granulation tissue. According to Grossman (11) sinus tracts can heal and closure occur after root-canal treatment. In this case the sinus tract persisted after treatment of the tooth. It was an indication of treatment failure and a surgical approach had to be done. For non surgical endodontic treatment, it has been shown that the presence of a sinus tract will not influence the long-term outcome of endodontic treatment (13-17). However, another study fond that the presence of a sinus tract was found to be a significant prognostic indicator (18). In surgical endodontic, studies have reported a comparable treatment outcome (19, 20).
References 1. Sunde PT, Olsen I, Debelian GJ,
Tronstad L. Microbiota of periapical lesions refractory to endodontic therapy. J Endod 2002; 28: 304– 310.
2. Tronstad L, Sunde PT. The evolving new understanding of endodontic infections. Endod Top 2003; 6: 57–77.
3. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297–306.
4. Signoretti FG, Endo MS, Gomes BP, Montagner F, Tosello FB, Jacinto RC. Persistent extraradicular infection in root-
filled asymptomatic human tooth: Scanning electron microscopic analysis and microbial investigation after apical microsurgery. J Endod 2011; 37: 1696–1700.
5. Wang J, Jiang Y, Chen W, Zhu C, Liang J. Bacterial Flora and Extraradicular Biofilm Associated with the Apical Segment of Teeth with Post-treatment Apical Periodontitis. J Endod 2012; 38: 954–959.
6. Happonen RP. Periapical actinomycosis: a follow-up study of 16 surgically treated cases. Endod Dent Traumatol 1986: 2: 205-209.
7. Mortensen H, Winther JE, Birn H. Periapical granulomas and cysts. Scand J Dent Res 1970; 78: 241–250.
8. Harrison JW, Larson WJ. The epithelized oral sinus tract. Oral Surg 1976; 42: 511–517.
9. Baumgartner JC, Pickett AB, Muller JT. Microscopic examination of oral sinus tracts and their associated periapical lesions. J Endod 1984; 10: 146-152.
10. Valderhaug J. A histologic study of experimentally produced intra-oral odontogenic fistulae in monkeys. Int J Oral Surg 1973; 2: 54–61.
11. Grossman LI. Endodontic practice. Philadelphia: Lea & Febiger. 1965; 78 –92.
12. Bender IB, Seltzer S. The oral fistula: its diagnosis and treatment. Oral Surg 1961; 14: 1367– 1376.
13. Strindberg LZ. The dependence of the results of pulp therapy on certain factors. Acta Odont Scand 1956; 14(Suppl 21): 1–175.
14. Sjögren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the

81
long-term result of endodontic treatment. J Endod 1990; 16: 498-482.
15. Chugal NM, Clive JM, Spångberg LSW. A prognostic model for assessment of the outcome of endodontic treatment: effect of biologic and diagnostic variables. Oral Surg Oral Med Oral Path Oral Radiol Endod. 2001; 91: 342-352.
16. Farzaneh M, Abitol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phases I and II: Orthograde retreatment. J Endod 2004; 30: 627-633.
17. Ricucci D,Russo J, Rutberg M, DMD,c Burleson JA, Spångberg LSW. A prospective cohort study of endodontic treatments of 1,369 root canals: results after 5 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 112: 825-842.
18. Ng YL, Mann V, gulabivala K. A prospective study of the factors effecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 2011; 344: 583-609.
19. Wang N, Knight K, Dao T, Friedman S. Treatment outcome in endodontics-The Toronto Study. Phases I and II: apical surgery. J Endod. 2004; 30: 751-761.
20. Rahbaran S, Gilthorpe MS, Harrison SD, Gulabivala K. Comparison of clinical outcome of periapical surgery in endodontic and oral surgery units of a teaching dental hospital: a retrospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 91: 700-709.

82
Case 15
Endodontic retreatment of the maxillary left first molar and surgical retreatment of the maxillary left first and second premolar
Fig. 1. Frontal view.
Patient 66-year-old Caucasian female.
Chief complaint The patient reported of previous pain and antibiotic regiments related to tooth 25. She also complains that several teeth in the left maxilla are tender when biting.
Medical record The patient was diagnosed with fibromyalgia and was medicated with Ibuprofen.
Dental history The patient was referred to the post-graduate clinic from the student clinic for apicoectomy of the maxillary left second premolar.
Clinical findings November 16th2010 Soft tissue: Normal findings. Dental: Teeth 24, 25 and 26 have dental crowns.
Fig. 2. Buccal view.
Clinical tests November 16th2010 24 25 26 EPT Nd Nd Nd Cold - - - Percussion h v&h V Palpation - - - PPD 4 4 4 Mobility - I - Biting + + +
Radiographic findings November 16th2010 Dental: Teeth 24 and 25 have radiopaque dental crowns, a post in the canal and radiopaque root filling materials. Tooth 26 has a radiopaque dental crown and a radiopaque root filling material. Periodontal: Moderate attachment loss. Periapical: An apical radiolucency is seen around the root of tooth 25 (PAI 4). Widened PDL space around the root of tooth 24, flush root filling. Discontinued lamina dura around the buccal roots of tooth 26; apical radiolucency MB root (PAI 3).

83
Fig. 3. Periapical 16.11.2010.
Fig. 4. Periapical radiograph 16.11.2010.
Diagnosis November 16th2010
Diagnosis Pulpal 24, 25, 26
K04.19 endodontically treated
Periodontal K05.03 chronic marginal periodontitis Periapical 25, 26
K05.40 chronic apical periodontitis
Treatment plan Endodontic retreatment of tooth 26. Surgical retreatment of tooth 25 and inspection of tooth 24.
Problem list Post removal 26. Apical lesion 24? Root fracture.
Treatment November 16th2010 1 carpule of Xylocaine/adrenaline was applied to establish anaesthesia. Access opening and localization of gutta-percha and a post in the palatal root canal. Mechanical: Burs, Gates Glidden,
NiTiFlex hand files: MB: #45/18mm DB: #45 /18.5mm P: no treatment Chemical: 1% NaOCl, 17% EDTA, 2% clorhexidine-di-gluconate. Intracanal medicament: CaOH2 Temporary filling: Cavit, IRM.
Fig. 5. Working length radiograph.
Treatment December 14th2010 Filled with thermoplasticized gutta-percha (Beefill) and AH Plus. Sealed with IRM.
Fig. 6. Master cone radiograph.
Fig. 7. Post-obturation radiograph.

84
Prognosis: Endodontic: Good. Tooth: Good.
Surgery April 6th2011 Anaesthetic, mucoperiosteal flap, osteotomy, surgical curettage, biopsy, root-end resection, ultrasonic root-end preparation. Haemorrhage control: adrenalin, ferric sulphate. Root-end filling using MTA Wound closure using non-absorbable suture material in sizes 4-0 and 5-0. Postoperative radiograph. Postsurgical care.
Fig. 8. Pathologic fenestration/extruded GP tooth 24.
Fig. 9. Root-end resection 3mm.
Fig. 10. Root-end preparation.
Fig. 11. Root-end filling with white MTA.
Fig. 12. Root-end filling checked on periapical radiograph.
Fig. 13. Suturing.
Histologic findings (Laboratorium of pathology, HS Koppang) Granulation tissue with moderate to intense chronic inflammation.

85
Prognosis Surgery: Good. Teeth: Good.
Follow-up examination April 13th2011 (1 week) Few post-operative complaints. Suture removal.
Fig. 14. One week post-operatively.
Follow-up examination September 21th2011 (5month´s) The patient is asymptomatic. No pain to percussion. The radiograph shows that the lesion is healing.
Fig. 15. Periapical control radiograph 5 months post-operatively.
Discussion Surgical endodontic treatment has historically been considered as an alternative to root canal treatment, or the preferred choice when root canal treatment is difficult or impossible (1). However, unless the root canal space is effectively cleaned, shaped and filled during preliminary root canal treatment or root-end preparation, it remains as a
source of infection that may allow inflammation to continue after surgical endodontics. The surgical intervention aims thus to remove the infected root-end and seal any remaining bacteria in the root canal system from the periradicular tissues. It has been discussed whether a root-end filling after root-end resection is necessary, or if the root canals are sufficiently filled with GP (2, 3). Some studies have found that healing occurs whether or not a root-end filling is placed (2, 4). However, ex vivo studies have suggested that a root-end filling is necessary to prevent leakage from the root canal and dentinal tubules (5, 6). In the last 10 years, mineral trioxide aggregate (MTA) has received special attention. MTA was introduced in the early 1990s as a new root-end filling material (7). MTA has showed in leakage studies that the material provides a remarkable seal (7, 8) and a favourable endodontic response with the potential to induce or attach to the newly regenerating periodontal ligament (8,9). Two randomized clinical trials (RCTs) comparing MTA and intermediate restorative material (IRM) have reported success rates of 84–92% for MTA and 76– 86% for IRM after 1 year (11, 12) and 92% for MTA and 87% for IRM after 2 years (11). Christiansen el al. (13) performed a randomized clinical to compare healing after root-end resection with a root-end filling of mineral trioxide aggregate (MTA) or smoothing of the orthograde gutta-percha (GP) root filling. Teeth treated with MTA had significantly better healing (96%) than teeth treated by smoothing of the orthograde GP root filling only (52%). Wälivaara el al. (14) investigated the periapical tissue response of 4 different retrograde root-filling materials: intermediate restorative material (IRM), thermoplasticized gutta-percha,

86
reinforced zinc oxide cement (Super- EBA), and mineral trioxide aggregate (MTA), in conjunction with an ultrasonic root-end preparation technique in an animal model. New root cement on the resected dentin surfaces was seen on all sections regardless of the used material. The IRM and MTA produced fewer signs of leakage, less unhealed periapical tissue, and a concomitant decreased inflammatory infiltration. New hard tissue formation, directly on the surface of the material, was seen only in the MTA sections. There was, however, no statistical difference in outcome among the tested materials.
References 1. Gutmann JL & Harrison JW.
Posterior endodontic surgery: anatomical considerations and clinical techniques. Int Endod J. 1985; 18(1): 8-34.
2. Nordenram A, Svärdström G. Results of apicectomy. Sven Tandlak Tidskr. 1970; 63(9): 593-604.
3. Johnson BR. Considerations in the selection of a root-end filling material. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87(4): 398-404.
4. Rapp EL, Brown Jr CE, Newton CW. An analysis of success and failure of apicoectomies. J Endodontics 1991; 17: 508–512.
5. Beatty RG, Vertucci FJ, Zakariasen KL. Apical sealing efficacy of endodontic obturation techniques. Int Endod J 1986; 19(5): 237-241.
6. Vignaroli PA, Anderson RW, Pashley DH. Longitudinal evaluation of the microleakage of dentin bonding agents used to seal resected root apices. J Endod 1995; 21(10): 509-512.
7. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a
mineral trioxide aggregate when used as a root end filling material. J Endod 1993; 19: 591-595.
8. Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR. Comparative investigation of marginal adaptation of mineral trioxide aggregate and other commonly used root-end filling materials. J Endod 1995; 21(6): 295-299.
9. Torabinejad M, Hong CU, Lee SJ, Monsef M, Pitt Ford TR. Investigation of mineral trioxide aggregate for root-end filling in dogs. J Endod 1995; 21(12): 603-608.
10. Torabinejad M, Pitt Ford TR, McKendry DJ, Abedi HR, Miller DA, Kariyawasam SP. Histologic assessment of mineral trioxide aggregate as a root-end filling in monkeys. J Endod 1997; 23(4): 225-228.
11. Chong BS, Pitt Ford TR, Hudson MB. A prospective clinical study of Mineral Trioxide Aggregate and IRM when used as root-end filling materials in endodontic surgery. Int Endod J. 2003 Aug;36(8):520-526.
12. Lindeboom JA, Frenken JW, Kroon FH, van den Akker HP. A comparative prospective randomized clinical study of MTA and IRM as root-end filling materials in single-rooted teeth in endodontic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005 Oct;100(4):495-500.
13. Christiansen R, Kirkevang LL, Hørsted-Bindslev P, Wenzel A. Randomized clinical trial of root-end resection followed by root-end filling with mineral trioxide aggregate or smoothing of the orthograde gutta-percha root

87
filling--1-year follow-up. Int Endod J 2009; 42(2): 105-114.
14. Wälivaara DÅ, Abrahamsson P, Isaksson S, Salata LA, Sennerby L, Dahlin C. Periapical tissue response after use of intermediate restorative material, gutta-percha, reinforced zinc oxide cement, and mineral trioxide aggregate as retrograde root-end filling materials: a histologic study in dogs. J Oral Maxillofac Surg 2012; 70(9): 2041-2047.

88
Case 16
Endodontic treatment and apical surgery of the mandibular left first molar
Fig. 1. Frontal view.
Fig. 2. Occlusal view.
Patient 70-year-old Caucasian male.
Chief complaint The patient complains about occasional, sporadic pain in the posterior region in lower left mandible. The posterior molar tooth is tender when biting.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate clinic from private practise for endodontic treatment of the mandibular left first molar. Tooth 35 was treated 2 years earlier (2009) at the Department of Oral and Maxillofacial Surgery; apicoectomy without root-end filling.
Clinical findings January 12th2011 Soft tissue: Normal findings. Dental: Tooth 34 is sound. Tooth 35 has a MODL composite restoration. Tooth 36 has a dental crown (Fig. 2).
Clinical tests January 12th2011 34 35 36 EPT 28 80 Nd Cold + - + Percussion - - +,v Palpation - - - PPD 3 3 3 Mobility - - - Biting - - +
Radiographic findings January 12th2011 Dental: Tooth 36 has radiopaque coronal restoration. Tooth 35 has a radiopaque MOD restoration and a radiopaque root filling material. Periodontal: Moderate attachment loss. Apical: Tooth 46 has an apical radiolucency mesial root (PAI 3). Tooth 35 has an apical radiolucency (PAI 3).

89
Fig. 3. Periapical radiograph 12.01.2011.
Diagnosis January 12th2011 Diagnosis Pulpal K04.11 necrotic pulp Periodontal K05.03 chronic marginal periodontitis Periapical K05.40 chronic apical periodontitis
Treatment plan Non-surgical endodontic treatment of tooth 36.
Treatment January 12th2011 2 carpules of Xylocaine/adrenaline was applied to establish anaesthesia. Access opening, bleeding from DB and MB canal, ML necrotic. Mechanical: Burs, NiTiFlex hand files #20, Biorace MB: #40/0.04 (BR5)/18mm ML: #40/0.04 (BR5)/18mm D: #50/0.04 (BR6) /19mm Chemical: 1% NaOCl, 17% EDTA. Intracanal medicament: CaOH2. Temporary filling: Cavit, IRM.
Fig. 4. Working length radiograph.
Treatment February 2nd2011 No symptoms. Tooth filled with gutta-percha and AH Plus. Sealed with IRM.
Fig. 5. Master cone radiograph.
Fig. 6. Post-obturation radiograph.
Prognosis Endodontic: Good. Tooth: Good.
Follow-up examination February 29th 2012 (1 year) Control at 1 year with x-ray indicated that the tooth was healing.
Fig. 7. Periapical control radiograph 1 year.

90
Follow-up examination April 2nd2014 (3 years) The patient contacted the clinic due to a small discomfort and swelling of the gingiva next to tooth 36 (Fig. 8).
Fig. 8. Gingival swelling.
Clinical examination revealed a buccal swelling over the mesial root of tooth 36. Normal probing depths. X-ray showed apical radiolucency. An OPG was ordered. Medications: 8 months ago the patient started taking Calcigran Forte 1000mg/day and Alendronat 70mg once a week. Treatment plan: Apical surgery tooth 36.
Fig. 9. Periapical radiograph 2 years.
Fig. 10. OPG 02.04.2014.
Surgery April 22nd2014 5 carpules of Xylocaine/adrenalin was applied to establish anaesthesia. Marginal incision from 34-36 with vertical releasing incisions 34 mesially and 36 distally. Enucleation of granuloma overlying mesial root /surgical curettage. Detection of a vertical root fracture (VRF) mesial root. Discussion of treatment alternatives. The patient is reluctant upon extracting the tooth immediately. Root resection of mesial root was discussed as a treatment alternative with the conclusion that unfavourable occlusal loading could weaken the prognosis of the remaining distal root. It was decided to postpone the extraction and leave the tooth until symptoms. Wound closure using non-absorbable suture material in sizes 4-0. Postsurgical care.
Fig. 11. Clinical photo showing VRF mesial root.

91
Follow-up examination April 29th2014 (1 week) No symptoms. Suture removal.
Follow-up examination May 13th2014 (1 month) Recurrent swelling at the buccal aspect over the mesial root. Tender on biting. Referred to Department of Maxillofacial Surgery, Ullevål hospital the same day for removal of tooth 36.
Discussion Vertical root fracture (VRF) is a longitudinally oriented fracture of the root that originates from its apical end and propagates coronally and is defined as one of the crack types (1). The prevalence of VRFs is reported to range from 11%–20% in extracted endodontically treated teeth (2). According to the literature, vertical root fracture is the third most common reason for extraction of an endodontically treated tooth (3). The final diagnosis of VRF can be complicated due to lack of specific signs, symptoms, and/or radiographic features and because several etiologic factors might be involved. Thus, the differential diagnosis from other pathologic entities might be difficult (4, 5, 6, 7, 8, 9, 10, 11). Tamse et al. (4) did an evaluation of 92 endodontically treated VRF teeth. They found that premolars were the predominant group (52%), and the maxillary second premolar accounted for 27%. In the mandible, the fracture was found in the mesial root in 17 of 22 molars (77%), whereas the distal root was fractured in only five teeth. In the maxillary molars, the fracture was in the mesiobuccal root (55.5%) and palatal root (33.3%). Only one distobuccal root was fractured. Pain (51%) or abscess (31%) was the major complaint. The most predominant clinical sign was deep pockets in 62 cases (67.4%),
usually located at the buccal side of the tooth or the root involved. Other signs and symptoms were sensitivity to percussion, mobility, and a coronally located fistula. There was a combination of both a deep pocket and a fistula in 22 cases (23.9%). The most significant finding of bone rarefaction was that a lateral radiolucency plus the combination of periapical and lateral radiolucency was present in 58 cases (63%). Radiographic features of vertical root fractures vary widely. These may be observed on radiographs as diffuse widening of periodontal ligament, dislodgement of retro-filling material, vertical bone loss, separation of root fragments or displacement of apical portions of root. Presence of “radiographic halo” has been shown as a major finding in cases of vertical root fractures (12). A VRF might also be observed directly on a conventional radiograph in the event the x-ray beam is in the same plane as the fracture to be observed (13, 17). In a systematic review by Tsesis et al. (14), the authors concluded that evidence-based data concerning the diagnostic accuracy and clinical effectiveness of clinical and radiographic dental evaluation for the diagnosis of VRF in endodontically treated teeth are lacking. Often, exploratory surgery is resorted in order to visualize the fracture. Raising a full thickness flap to directly visualize the root(s) under light, magnification, and with methylene blue staining does this. There is no substitute for direct visualization if the diagnostic and prognostic assessments remain questionable (15). The inability of conventional imaging techniques to consistently visualize VRFs precisely necessitates the development of alternative imaging

92
modalities to improve their detection (16). Cone-beam computed tomography (CBCT), also called digital volume tomography (DVT), is a relatively new imaging modality in maxillofacial imaging, which involves three-dimensional (3D) slice acquisition at significantly reduced radiation doses. Presently CBCT has been shown to be promising in the early detection of vertical root fractures. Edlund et al. (17) designed a clinical pilot study to determine the diagnostic accuracy of CBCT for detection of suspected VRFs in endodontically treated teeth by using exploratory surgery to confirm the presence or absence of a fracture. Thirty-two teeth in 29 patients with clinical signs and symptoms suggestive of VRF were included in the study. Sensitivity of CBCT for detection of VRF was 88%, and the specificity was 75%. Positive predictive value (PPV), the proportion of teeth with fractures that were correctly diagnosed, was determined to be 91%, and negative predictive value (NPV), the proportion of teeth with no fractures that were correctly diagnosed, was 67%. The overall accuracy was 84%. Similar findings have been published in a few case reports (18, 19, 20). It has been shown that the presence root canal filling does not significantly influence the accuracy but reduces specificity in detection of vertical root fracture by CBCT (21, 22).
References 1. Colleagues for excellence.
Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Chicago: American Association of Endodontics; 2008.
2. Fuss Z, Lustig J, Tamse A. Prevalence of vertical root
fractures in extracted endodontically treated teeth. Int Endod J 1999; 32: 283–286.
3. Toure B, Faye B, Kane AW, Lo CM, Niang B, Boucher Y. Analysis of reasons for extraction of endodontically treated teeth: A prospective study. J Endod 2011; 37: 1512-1515.
4. Tamse A, Fuss Z, Lustig J, Kaplavi J. An evaluation of endodontically treated vertically fractured teeth. J Endod 1999; 25: 506–508.
5. Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical root fractured teeth: impact of operative procedures. J Endod 2001; 27: 46–48.
6. Cohen S, Blanco L, Berman L. Vertical root fractures: clinical and radiographic diagnosis. J Am Dent Assoc 2003; 134: 434–441.
7. Meister F Jr, Lommel TJ, Gerstein H. Diagnosis and possible causes of vertical root fractures. Oral Surg Oral Med Oral Pathol 1980; 49: 243–25.
8. Moule AJ, Kahler B. Diagnosis and management of teeth with vertical root fractures. Aust Dent J 1999; 44: 75–87.
9. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod 1992; 18: 332–335.
10. Tamse A. Iatrogenic vertical root fractures in endodontically treated teeth. Endod Dent Traumatol 1988; 4: 190–196.
11. Tamse A, Fuss Z, Lustig J, Ganor Y, Kaffe I. Radiographic features of vertically fractured, endodontically treated maxillary premolars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88: 348–352.

93
12. Khasnis SA, Kidiyoor KH, Patil AB, Kenganal SB. Vertical root fractures and their management. J Conserv Dent 2014; 17(2): 103-110.
13. Rud J, Omnell KA. Root fractures due to corrosion: diagnostic aspects. Scand J Dent Res 1970; 78: 397–403.
14. Tsesis I, Rosen E, Tamse A, Taschieri S, Kfir A. Diagnosis of Vertical Root Fractures in Endodontically Treated Teeth Based on Clinical and Radiographic Indices: A Systematic ReviewJ Endod 2010; 36: 1455–1458.
15. Cohen S, Blanco L, Berman L. Vertical root fractures: clinical and radiographic diagnosis. J Am Dent Assoc 2003; 134: 434–441.
16. Nair MK, Nair UDP, Grondahl HG, Webber RL, Wallace JA. Detection of artificially induced vertical radicular fractures using tuned aperture computed tomography. Eur J Oral Sci 2001; 109: 375–379.
17. Edlund M, DDS, Nair MK, Nair PN. Detection of Vertical Root Fractures by Using Cone-beam Computed Tomography: A Clinical Study. J Endod 2011; 37: 768–772.
18. Zou X, Liu D, Yue L, Wu M. The ability of cone beam computed tomography to detect vertical root fracture s in endodontically treated and non endodontically treated teeth: A report of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 111: 797-801.
19. Tang L, Zhou XD, Wang Y, Zhang L. Detection of vertical root fracture using cone beam computed tomography: Report of
two cases. Dent Traumatol 2011; 27: 484-488.
20. Metska ME, Aartman IHA, Wesselink PR. Ozok AR. Detection of vertical root fracture in vivo in endodontically treated teeth by cone beam computed tomography scans. J Endod 2012; 38: 1344-1347.
21. Hassan B, Metska ME, Ozok AR, Stelt PV, Wesselink PR. Detection of vertical root fracture in endodontically treated teeth by cone beam computed tomography scan. J Endod 2009; 35: 719-722.
22. Hassan B, Metska ME, Ozok AR, Stelt PV, Wesselink PR. Comparison of five cone beam computed tomography systems for detection of vertical root fractures. J Endod 2010; 36: 126-129

94
Case 10
Surgical retreatment of the maxillary right first incisor
Fig. 1. Frontal view.
Patient 18-year-old Asian female.
Chief complaint Non-contributory.
Medical record Non-contributory.
Dental history A specialist in pedodontics endodontically treated tooth 11 in 2009 due to a large apical radiolucency. There was a trauma in childhood. The tooth had a crown cemented soon after finishing of the root filling. The patient was referred to the postgraduate clinic from the public dentistry for surgical retreatment due to a persisting apical lesion.
Fig. 2. Buccal view.
Fig. 3. Palatal view.
Clinical findings February 2nd2011 Soft tissue: Gingivitis. Dental: Tooth 11 has a dental crown. Teeth 12 and 21 have palatal erosive tooth loss, otherwise sound.
Clinical tests February 2nd2011 12 11 21 EPT 32 80 22 Cold + - + Percussion - - - Palpation - + - PPD 2 3 2 Mobility - - - Biting - - -

95
Radiographic findings February 2nd2011 Dental: Tooth 11 has a radiopaque dental crown and a radiopaque root-filling material. Periodontal: Gingivitis. Apical: Tooth 11 has an apical radiolucency (PAI 4), and overfilling of gutta-percha is suspected. Normal PDL space around teeth 12 and 21.
Fig. 4. Periapical radiograph.
Diagnosis February 2nd2011 Diagnosis Pulpal K04.19 endodontically treated
Periodontal K05.01 chronic gingivitis Periapical K04.50 chronic apical periodontitis
Treatment plan Apicoectomy with retrograde filling of tooth 11. Treatment alternative: non-surgical retreatment and observation.
Problem list Thin gingival biotype. Gingival recession and aesthetics.
Surgical treatment May 25th2011 At the day of surgery, clinical inspection showed a sinus tract tooth 11.
Fig. 5. A sinus tract was present apically around tooth 11, 25.05.2011.
The patient was given a chlorhexidine mouth rinse and local anaesthetic (Xylocaine/adrenaline) was injected. A papilla-base incision was made running from tooth 22 to tooth 13 with a vertical releasing incision on the distal aspect of 13. Elevation of the mucoperiosteal flap revealed pathologic fenestration and extruded gutta-percha. Osteotomy and curettage of granulation tissue. Biopsy. Root-end resection and retrograde preparation with ultrasonic instruments. Haemostasis with ferric sulphate. A retrograde filling of white MTA was applied. The operation site was rinsed with sterile saline and the flap sutured in place with supramide and dafilon 5.0 and 6.0. Prescription of Apocillin 660mg x4 for 7 days. Postoperative instructions. Complications during surgery: Flap-tearing and difficulties in suturing.

96
Fig. 6. Photo after root-end preparation.
Fig. 7. Photo showing retrograde filling with MTA.
Fig. 8. Post-operative radiograph before suturing.
Fig. 9. Suturing.
Prognosis Endodontic: Good. Tooth: Good. Surgery: Unpredictable tissue healing.
Follow-up examination May 31th2011 (one week) Suture removal. The patient had not experienced any postoperative problems. The sinus tract was closed but secondary healing was observed in the midline.
Follow-up examination June 8 th2011 (2 weeks) The wound healing was good. There was a small gingival recession. The patient had not noticed any changes in gingival levels.
Fig. 10. Photo 2 weeks post-operatively.
Follow-up examination January 19th2012 (7 months) No further gingival recessions. The tooth was asymptomatic. Radiographic signs of healing with a continuous PDL space surrounding the apex.

97
Fig. 11. Photo 7 months post-operatively.
Fig. 12. Periapical control radiograph 7 months after surgery.
Discussion When designing a tissue flap, various modes of incision can be selected, including horizontal, sulcular, submarginal, and vertical releasing incisions. The tissue flap in its entirety can be a full-thickness or a combination of a full- and a split-thickness flap (1). Certain basic principles must be considered before deciding on the type of incision and the flap design: regional anatomy, proper access to the periapical pathosis, periodontal conditions, state of coronal tooth structure, the nature and extent of coronal restorations and operators choice. The papilla base incision (PBI) for the marginal mucoperiosteal flap was suggested to prevent loss of interdental papilla height. This incision allows the preservation of the entire papilla, thus eliminating any substantial loss of
height as a result of the surgical or healing process (2). In 2003 Velvart et al. (3) investigated papilla healing in twelve patients after apical surgery in anterior and molar teeth using the PBI and sulcular full-thickness flap. After 1- and 3- months the PBI allowed recession-free healing whilst complete mobilization of the papilla led to a marked loss of the papilla height. Velvart et al. (4) compared the long-term loss of papilla height when using either the PBI or the standard papilla mobilization incision in marginal full thickness flap procedures. They found a significant difference between the two incision techniques for all recall appointments (1-, 3-, and 12-months). Von Arx et al. (5) evaluated gingival recession following apical surgery of 70 anterior teeth (central and lateral incisors, canines, and first premolars). They concluded that gingival biotype, pre-treatment periodontal pocket, and type of incision might significantly influence changes in gingival margin (GM) and clinical attachment level (CAL). In their study the submarginal incision showed significantly less gingival recession compared with the intrasulcular incision, papilla-base incision or papilla-saving incision. In a study by von Arx et al. (6) long-term changes in periodontal parameters were evaluated after apical surgery of 186 teeth. Significant changes in GM and CAL were observed at facial sites during the first year after surgery. However, none of the periodontal parameters changed significantly between 1 and 5 years after apical surgery. The type of incision technique was found to be the major factor affecting changes in GM and CAL between baseline and 1 year after surgery. Age, smoking, and type of periapical healing were the variables influencing the periodontal parameters

98
over the longer observation period of up to 5 years. It has been demonstrated that the gingival biotype could be related to complications following flap-procedures. The thin biotype is more prone to gingival recession and an unpredictable tissue healing should be expected (7). The type of incision may be a predictor for complications following surgery of a tooth with a thin biotype: higher probability of recession for intra-sulcular incision, more scarring for submarginal incision, more complications during flap elevation susch as flap tearing, and dehiscence and difficulties in suturing (8).
References 1. Velvart P, Peters CI, Peters OA.
Soft tissue management: flap design, incision, tissue elevation and tissue retraction. Endod Topics 2005: 11: 78–97.
2. Velvart P. Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. Int Endod J 2002: 35: 543-460.
3. Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-thickness flap and papilla base flap in endodontic surgery. Int Endod J 2003: 36: 653–659.
4. Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of long term papilla healing following sulcular full thickness flap and papilla base flap in endodontic surgery. Int Endod J 2004: 37: 687–693.
5. von Arx T, Salvi GE, Janner S, Jensen SS. Gingival recession following apical surgery in the esthetic zone: a clinical study with 70 cases. Eur J Esthet Dent 2009: 4: 28–45.
6. von Arx T, Alsaeed M, Giovanni ES. Five-year changes in periodontal parameters after apical Surgery. J Endod 2011: 37: 910-918.
7. Kao RT, Fagan MC, Conte GJ. Thick vs. thin gingival biotypes: a key determinant in treatment planning for dental implants. J Calif Dent Assoc. 2008; 36(3): 193-198.
8. Tsesis I, Beitlitum I, Rosen E. Prevention and management of soft tissue complications in endodontic surgery. In: Complications in endodontic surgery. 2014; Springer-Verlag Berling Heidelberg (eBook).

99
Case 18
Evaluation of a root-filled mandibular right first molar and surgical retreatment of the maxillary left first molar with a sinus tract.
Fig. 1. Frontal view.
Patient 45-year-old Asian male.
Chief complaint The patient complains about previous pain and sinus tract related to a mandibular left molar tooth. He tells that the tooth was root-filled in 2012 and that his dentist has prescribed antibiotics at several occasions after finishing the root filling. At present the tooth is tender when chewing. He also complains about tenderness when chewing in the posterior region in the upper left maxilla. He has noticed a draining sinus tract in this area.
Medical record Podagra (hyperuricaemia), allergy (pollen), sleeping disorder. He has mild dental fear. Medications: Ritalin, Zyrtec.
Dental history The patient was referred to the postgraduate clinic from private practice for endodontic evaluation and treatment of the mandibular right first molar and the maxillary left first molar.
Tooth 46 was root-filled by the referring dentist 2 years ago and has a history of pain, swelling and sinus tract. Tooth 26 was root-filled by a specialist in endodontics 4 years ago and a crown has recently been made.
Clinical findings February 7th2014 Soft tissue: Sinus tract region 26. Dental: Tooth 46 has an ODL composite restoration. Tooth 26 has a dental crown, tooth 27 has a composite restoration with poor margins and caries. Generalized erosive tooth surface loss.
Fig. 2. Occlusal view tooth 46.
Fig. 3. Buccal view tooth 26; sinus tract.

100
Clinical tests February 7th2014 25 26 27 46 EPT 25 Nd Nd Nd Cold + - - - Percussion - + - + Palpation - + - + PPD 3 4 4 4 Mobility - - - - Biting - + - +
Radiographic findings February 7th2014 Dental: Tooth 46 has a radiopaque MOD filling and a radiopaque root filling material. Tooth 26 has a radiopaque dental crown and a radiopaque root-filling material. Periodontal: Chronic marginal periodontitis. Apical: Tooth 46 has apical radiolucencies mesial and distal root (PAI 4) and a lateral radiolucency distal root. Tooth 26 has apical radiolucencies mesial and distal root (PAI 3) and an interradicular radiolucency.
Fig. 4. Periapical radiograph.
Fig. 5. Periapical radiograph.
Fig. 6. Periapical radiograph.
Fig. 7. A sinus tract originating from tooth 26.
Diagnosis February 7th2014 Diagnosis Pulpal 26,46
K04.19 endodontically treated
Periodontal K05.03 chronic marginal
periodontitis Apical 26 Apical 46
K04.62 chronic apical periodontitis with sinus tract K04.50 chronic apical periodontitis
Dental 46 S02.50 cracked tooth
Treatment plan Access preparation and visual inspection with magnification of tooth 46; longitudinal fracture? Surgical retreatment of the buccal roots of the endodontically treated maxillary left first molar.

101
Problem list Anxiety. Longitudinal fracture tooth 46? Interradicular radiolucency tooth 26.
Treatment February 7th2014 Rubberdam was applied. Access preparation and identification of a crack affecting the distal marginal ridge of the mandibular right first molar; the crack has propagated into the distal root. The patient is told that the prognosis is poor and removal of the tooth is recommended.
Fig. 8. Occlusal view of the cracked tooth affecting the distal marginal ridge and extending into the distal root.
Follow-up April 29th2014 (by phone) The patient postponed the removal of tooth 46 and sent a photo showing a fracture of the tooth (Fig. 9). He was advised to contact his dentist for removal of 46.
Fig. 9. Propagation of crack resulted in a split tooth 46.
Surgery March 25th2014 The patient was given a chlorhexidine mouth rinse and local anaesthetic was injected. A marginal incision was made running from tooth 27 to tooth 25, with vertical releasing incisions 25 mesially and 27 distally. Elevation of the mucoperiosteal flap. Osteotomy and curettage of granulation tissue. Adrenaline and ferric sulphate haemostasis. A retrograde filling of white MTA was applied. The operation site was rinsed with sterile saline and the flap sutured in place with supramide 4.0 and 5.0. Postoperative instructions. Paracetamol. Complications during surgery: Large defect in furcation area. Limitations to visibility and accessibility of the root tips.
Fig. 10. Retro-preparation radiograph.
Fig. 11. Retro-filling.
Prognosis Endodontic: Uncertain. Tooth: Uncertain.

102
Follow-up examination March 27th2014 (2 days) The patient experienced post-operative discomfort; swelling and mild pain/malaise and fever. He contacted us due to a planned flight abroad the same day. Clinically: heat, pain, redness, and swelling are noted in the cheek at the operation site. Secondary healing region 25. Prescription of phenoxymethylpenicillin (660mgx4 for 7 days).
Follow-up examination April 1th2014 (1 week) Asymptomatic. Suture removal. Minor swelling in the cheek.
Follow-up examination April 11th2014 (10 days) No swelling. Satisfactory healing at the operation site.
Follow-up examination June 17th2014 (3 months) The patient has no complaints. Radiograph shows initial healing of apical radiolucencies. Interradicular radiolucency seems unchanged.
Fig. 12. Photo region 26; 3 months post-operatively.
Fig. 13. Periapical radiograph 3 months.
Follow-up examination September 5th2014 (6 months) No symptoms. Tooth 26 not tender to percussion or palpation. PPD 4mm at the buccal aspect. Interradicular radiolucency seems unchanged on the periapical radiograph.
Fig. 14. Periapical control radiograph 6 months.
Discussion The persistence of microorganisms plays a significant role in endodontic treatment failures (1). Although several factors might be involved with endodontic treatment failure, this usually results from the presence of bacteria in the apical portion of the root canal (2-4). The absence of coronal sealing, micro leakage, failures in chemo mechanical preparation, and limit and quality of root filling favour the survival of microorganisms after endodontic treatment or reinfection of the canal and may lead to endodontic treatment failure (2, 4, 5). There is great variation in the composition of the microbiota

103
associated with endodontic failure and the levels of the bacterial species detected in root canals, which may occur as a result of the different diagnostic techniques used (6-10). This microbiota has been described as being mainly composed of facultative anaerobic gram-positive species. Enterococcus is the genus most frequently described, and Enterococcus faecalis is the species more commonly found in these lesions (6-10). However, recent studies have questioned the hypothesis that E. faecalis is the main species associated with endodontic failures (11-16). Murad et al. (17) investigated the composition of the root canal microbiota from 36 root canals with persistent endodontic infection. The presence, levels, and proportions of 79 bacterial species were determined by checkerboard DNA-DNA hybridization. The highest mean levels were found for the following species: E. faecium, Dialister pneumosintes, Staphylococcus epidermidis and Helicobacter pylori. No correlation was found between any of the species tested and clinical findings; however, periapical lesions with the largest areas presented higher counts of gram-negative and rod species. The levels of gram-negative species were statistically significantly higher than those of the gram-positive species. Sodium hypochlorite (NaOCl) is the main irrigating solution used in root canal preparation to dissolve vital and necrotic tissue and eliminate the bacteria of instrumented root canals (18, 19). Concomitant with the focus on E. faecalis as a key organism in persistent infections, modifications like the addition of chlorhexidine (CHX) were introduced. Many authors have stressed the importance of using antimicrobial irrigants during chemo mechanical
preparation to ensure complete disinfection when this particular organism is suspected. CHX is a broad-spectrum antimicrobial agent that has been reported to be an effective medicament in endodontic therapy. It has been recommended as a final irrigating solution in view of its antimicrobial action (20), proven substantivity (21), and capacity to inhibit the adherence of certain bacteria to dentin (22). Basrani et al. (23) studied the efficacy of CHX and calcium hydroxide (Ca(OH)2-containing medicaments against E. faecalis in vitro. They concluded that CHX was significantly more effective against E. faecalis than Ca(OH)2. In another study by Zamany et al. (23), the authors demonstrated that an additional rinse with 2% chlorhexidine resulted in enhanced disinfection of the root canal system.
References 1. Sjögren U, Fidgor D, Persson S, et
al. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997; 30: 297–306.
2. Sjögren U. Siqueira Jr JF. Aetiology of root canal treatment failure: why well treated teeth can fail. Int Endod J 2001; 34: 1–10.
3. Wu MK, Dummer PM, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. Int Endod J 2006; 39: 343–356.
4. Sundqvist G, Fidgor D, Persson S, et al. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol 1998; 85: 86–92.

104
5. Siqueira Jr JF, Rôças IN, Uzeda M, et al. Comparison of 16S rDNA-based PCR and checkerboard DNA-DNA hybridization for detection of selected endodontic pathogens. J Med Microbiol 2002; 51: 1090–1096.
6. Molander A, Reit C, Dahlen G, et al. Microbiological status of root-filled teeth with apical periodontitis. Int Endod J 1998; 31:1–7.
7. Hancock HH, Sigurdsson A, Trope M, et al. Bacteria isolated after unsuccessful endodontic treatment in a North American population. Oral Surg Oral Med Oral Pathol 2001; 91: 579–585.
8. Fouad AF, Zerella J, Barry J, et al. Molecular detection of Enterococcus species in root canal therapy-resistant endodontic infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99: 112–118.
9. Gomes BP, Pinheiro ET, Jacinto RC, et al. Microbial analysis of canals of toot-filled teeth with periapical lesions using polymerase chain reaction. J Endod 2008; 34: 537–540.
10. Rocas IN, Jung II-Y, Lee CY, et al. Polymerase chain reaction identification of microorganisms in previously root-filled teeth in a South Korean population. J Endod 2004; 30: 504–508.
11. Blome B, Braun A, Sobarzo V, Jepsen S. Molecular indentification and quantification of bacteria from endodontic infections using real-time polymerase chain reaction. Oral Microbiol Immunol 2008; 23: 384–390.
12. Schirrmeister JF, Liebenow AL, Pelz K, et al. New bacterial compositions in rootfilled teeth
with periradicular lesions. J Endod 2009; 35: 169–174.
13. Fujii R, Saito Y, Tokura Y, et al. Characterization of bacterial flora in persistent apical periodontitis lesions. Oral Microbiol Immunol 2009; 24: 502–505.
14. Rocas IN, Siqueira JF Jr. Characterization of microbiota of root canal-treated teeth with posttreatment disease. J Clin Microbiol 2012; 50: 1721–1724.
15. Wang J, Jiang Y, Chen W, et al. Bacterial flora and extraradicular biofilm associated with the apical segment of teeth with port-treatment apical periodontitis. J Endod 2012; 38: 954–959.
16. Hong BY, Lee TK, Lim SM, et al. Microbial analysis in primary and persistent endodontic infections by using pyrosequencing. J Endod 2013; 39: 1136–1140.
17. Murad CF, Sassone LM, Faveri M, Hirata Jr R, Figueiredo L, and Feres M, DDS, MSc, PhDMicrobial Diversity in Persistent Root Canal Infections Investigated by Checkerboard DNA-DNA Hybridization. J Endod 2014; 40: 899–906.
18. Bystrom A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J 1985; 18(1): 35–40.
19. Siqueira JF Jr, Rôças IN, Santos SR et al. Efficacy of instrumentation techniques and irrigation regimens in reducing the bacterial population within root canals. J Endod 2002; 28(3): 181–184.
20. Mohammadi Z, Abbott PV. The properties and applications of chlorhexidine in endodontics. Int Endod J 2009; 42(4): 288–302.
21. Mohammadi Z, Abbott PV. Antimicrobial substantivity of

105
root canal irrigants and medicaments: a review. Aust Endod J 2009; 35(3): 131–139.
22. Kishen A, Sum CP, Mathew S et al. Influence of irrigation regimens on the adherence of Enterococcus faecalis to root canal dentin. J Endod 2008; 34(7): 850–854.
23. Basrani B, Tjaderhane L, Santos JM, Pascon E, Grad H, Lawrence HP, Friedman S. Efficacy of chlorhexidin- and calcium hydroxide-containing medicaments against Enterococcus faecalis in vitro. Oral Surg Oral Med Oral Pathol Oral Rsdiol Oral Endod 2003; 96(5): 618-624.
24. Zamany A, Safavi K, Spangberg LS. The effect of chlorhexidine as an endodontic disinfectant. Oral Surg Oral Med Oral Pathol Oral Radiol Oral Endod 2003; 96(5): 578-581.

106
Case 19
Endodontic retreatment of the maxillary right first molar with a sinus tract
Fig. 1. Frontal view.
Patient 60-year-old Caucasian female.
Chief complaint She had noticed a swelling on the gingiva in the molar region in the right maxilla.
Medical record Medical condition: Hypothyroidism. Medications: Esidrex, Levaxin.
Dental history Tooth 16 had been treated endodontically more than 10 years ago. In 2012 she had a bridge made at the student clinic, keeping the pre-existing casted conus tooth 16. The patient was referred to the postgraduate clinic from the student clinic for endodontic retreatment of the maxillary right first molar.
Clinical findings January 31st2014 Soft tissue: A sinus tract in relation to tooth 16 was observed (Fig. 2). Dental: A dental bridge restoration comprising teeth 141516.
Fig. 2. Photo showing sinus tract tooth 16.
Clinical tests January 31st2014 14 16 EPT Nd Nd Cold + - Percussion - - Palpation - + PPD 3 6 Mobility - - Biting - -
Radiographic findings January 31st2014 Dental: A radiopaque dental bridge abutment teeth 14 and 16, and replacement tooth 15 is seen. Tooth 16 has a radiopaque root filling material. Periodontal: Attachment loss. Apical: An apical radiolucency is seen surrounding the mesial root of tooth 16. Normal PDL space around the root apex of tooth 14 (Fig. 3). The radiopaque gutta-percha point in the sinus tract can be seen in Fig. 4.

107
Fig. 3. Periapical radiograph 31.01.2014.
Fig. 4. The sinus tract originates from tooth 16.
Diagnosis January 31st2014 Diagnosis Pulpal K04.19 endodontically treated
Periodontal K05.03 chronic marginal
periodontitis Apical K04.62 chronic apical periodontitis
with sinus tract
Treatment plan Non-surgical retreatment of the mesial root of the endodontically treated maxillary right first molar Observation of sinus tract. If no healing apicoectomy is planned.
Problem list Previous transportation of mesiobuccal canal. Negotiating the apical third beyond the curvature. Sinus tract.
Treatment January 31st2014 Access opening and localisation of MB canal orifice with the old GP. Mechanical: Burs, NiTiFlex hand files MB: #55/18mm Not able to negotiate beyond the curvature. Unable to localize a second MB canal. Chemical: 2% Chlorhexidine, 17% EDTA. Intracanal medicament: Ca(OH)2. Temporary filling: IRM.
Fig. 5. Working length radiograph.
Treatment February 18th2014 Asymptomatic. Regression of sinus tract is seen (Fig. 6).
Fig. 6. Photo showing recession of sinus tract.
The tooth was filled with gutta-percha and AH Plus. Sealed with composite.
Fig. 7. Master cone radiograph.

108
Fig. 8. Post-obturation radiograph.
Prognosis Endodontic: Uncertain. Tooth: Good.
Follow-up examination May 6th2014 (3 months) No symptoms but the patient noticed that the sinus tract is still there. Surgery is planned. Problem list: Reduced bone level.
Fig. 9. Periapical radiograph 06.05.2014.
Fig. 10. Persisting sinus tract 3 months.
Surgery May 13th2014 The patient was given a chlorhexidine mouth rinse and local anaesthetic was injected. A marginal incision was made running from pontic 25 to tooth 17 with
a vertical releasing incision on the mesial aspect of tooth 25. Elevation of the mucoperiosteal flap. Osteotomy and curettage of granulation tissue. Small sinus perforation. Gauze sponge sutured in place before root-end resection and retrograde preparation with ultrasonic instruments. Haemostasis using Xylocaine/adrenaline. A retrograde filling of white MTA was applied. The operation site was rinsed with sterile saline and the flap sutured in place with supramide 4.0 and 5.0. Postoperative instructions.
Fig. 11. Gauze sponge sutured in place to protect sinus.
Fig. 12. Root resection.
Prognosis Surgery: Good. Tooth: Good.
Follow-up examination September 5th2014 (4 months) No symptoms. Closed sinus tract.

109
Fig. 13. Control 4 months.
Fig. 14. Periapical control radiograph (4 months).
Discussion When planning periapical surgery in maxillary premolars and molars, the proximity of the maxillary sinus has to be considered. The maxillary sinus is an osseous cavity with the shape of a pyramid, the base being the nasal antral wall and the rounded tip lying in the zygomatic bone (1). The maxillary sinus is lined by a ciliary epithelium containing beaker cells. This lining transports bacteria and other possible foreign material toward the maxillary ostium on a thin mucous layer. The maxillary ostium represents the opening to the nasal cavity, lying below the middle nasal concha. A healthy maxillary sinus is aseptic in 80 to 100% of the population, containing neither bacteria nor any other foreign material (2). The main purposes of the maxillary sinus have been postulated as a space for conditioning of the breathing air, a means of reducing the weight of the skull, and a resonance chamber for the human voice (1). It also functions as an immunologic barrier (2).
There is a very close anatomic relationship between the root tips of the maxillary posterior teeth and the sinus floor. Eberhardt et al. (3) measured the distances between maxillary molar and premolar roots and the maxillary sinus. Their findings showed that the mean distance of the maxillary posterior teeth to the floor of the maxillary sinus is 1.97 mm. Thus, endodontic surgery of premolars and molars can produce an accidental oroantral communication (2, 4, 5, 6, 7 and 8) referred to as OAC. The OAC may result in acute or chronic sinusitis through displacement of bacteria from the infected periapical tissue, resected root tips, or bony drilling dust into the sinus (2). Hauman et al. (9) addressed anatomic and clinical aspects of the maxillary sinus in their review article. A key finding was that the borders of the maxillary sinus are projected as a thin radio-opaque line on periapical radiographs. In some cases with chronic periapical periodontitis, this line can be well-defined and easy to trace, although in others the radio-opaque line appears less defined or blurred. Oberli et al. (2007) attempted to find out whether conventional periapical radiographs can be used to determine the risk of creating an oroantral communication (OAC) while performing periapical surgery on maxillary premolars and molars. Perforation of the sinus membrane (also referred to as the Schneiderian membrane) occurred in 12 cases (9.6%). Exposure of the membrane without rupture occurred in 15 cases (12%). It was found that the distance between the apex or the apical lesion and the sinus floor did not serve as a predictor of a possible sinus membrane rupture. On the other hand, if the radiograph showed a distinct distance between the lesion and the sinus floor, there was an 82.5% probability that OAC would not occur.

110
Additionally, a blurred radiographic outline of the periapical lesion did not indicate an increased risk of sinus membrane rupture. They concluded that conventional periapical radiographs couldn’t be used as predictors for perforation of the maxillary sinus during periapical surgery. However, radiographs with a specific distance between the periapical lesion and the sinus floor point toward a very low risk of accidental sinus perforation during periapical surgery (10). Another issue is whether an OAC must be considered a “surgical accident” (6). A review article of the literature on periapical surgery by Garcia et al. (11) confirms that none of the included studies found a significant difference in the healing outcome or the postoperative sequel when accidental OAC had occurred. However, the importance of prevention of introduction of foreign bodies, drilling dust, or bacteria into the maxillary sinus during the surgery is emphasised. In case of OAC, Jerome and Hill (12) suggested protecting the OAC with a gauze pad once the root tip had been resected. Furthermore, magnifying surgical aids such as loupes, endoscopes, and microscopes permit the surgeon to make a precise diagnosis and perform minimally invasive low trauma surgery (13, 14). The occurrence of intraoperative OAC during periapical surgery is not a severe surgical accident. A proper operation technique avoiding dislocation of drilling dust, root tips, infected tissue, and haemostatic and filling material into the maxillary sinus will allow healing without complications even if OAC should occur.
References 1. Waite DE. Maxillary sinus. Dent
Clin North Am 1971; 15: 349-386.
2. Watzek G, Bernhart T, Ulm C. Complications of sinus perforations and their management in endodontics. Dent Clin North Am 1997; 41: 563-583.
3. Eberhardt JA, Torabinejad M, Christiansen EL. A computed tomographic study of the distances between the maxillary sinus floor and the apices of the maxillary posterior teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1992; 73: 345-346.
4. Freedman A, Horowitz I. Complications after apicoectomy in maxillary premolar and molar teeth. Int J Oral Maxillofac Surg 1999; 28: 192-194.
5. Rud J, Rud V. Surgical endodontics of upper molars: relation to the maxillary sinus and operation in acute state of infection. J Endod 1998; 24: 260-261.
6. Lin L, Chance K, Shovlin F, Skribner J, Langeland K. Oroantral communication in periapical surgery of maxillary posterior teeth. J Endod 1985; 11: 40-44.
7. Ericson S, Finne K, Persson G. Results of apicoectomy of maxillary canines, premolars and molars with special reference to oroantral communication as a prognostic factor. Int J Oral Surg 1974; 3: 386-393.
8. Ioannides C, Borstlap WA. Apicoectomy on molars: a clinical and radiographical study. Int J Oral Surg 1983; 12: 73-79.
9. Hauman CHJ, Chandler NP, Tong DC. Endodontic implications of

111
the maxillary sinus: a review. Int Endod J 2002; 35: 127-141.
10. Oberli K, Bornstein MM, vonArx T. Periapical surgery and the maxillary sinus: radiographic parameters for clinical outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103: 848-853.
11. Garcia B, Martorell L, Martí E, Peñarrocha M. Periapical surgery of maxillary posterior teeth. A review of the literature. Med Oral 2006; 11: 146-150.
12. Jerome CE, Hill AV. Preventing root tip loss in the maxillary sinus during endodontic surgery. J Endod 1995; 21: 422-424.
13. von Arx T, Montagne D, Zwinngi C, Lussi A. Diagnostic accuracy of endoscopy in periradicular surgery—a comparison with scanning electron microscopy. Int Endod J 2003; 36: 691-699.
14. von Arx T, Hunenbart S, Buser D. Endoscope- and videoassisted endodontic surgery. Quintessence Int 2002; 33: 255-259.

112
Case 20
Treatment of multiple idiopathic cervical root resorption
Fig. 1. Frontal view.
Patient 51-year-old Russian male.
Chief complaint Firstly, he complains about lots of past problems with his teeth in the left maxilla that finally had to be extracted. At present he feels discomfort in the gingiva around tooth 14 as well as sensitivity to cold in this area. He thinks the problems started when a crown was made 4 years earlier, and that the gingival discomfort got worse as time went by. Secondly, he complains of sensitivity to cold in the posterior left side of the mandible. He further tells that he is grinding his teeth and that his dentist told him that he is a bruxist.
Medical record Non-contributory.
Dental history The patient was referred to the post-graduate endodontic clinic from private practise because of suspicion of a resorption (internal) on tooth 14 below a crown made 4 years earlier. It was observed on a routine x-ray. There was
no history of trauma or orthodontic treatment.
Clinical findings August 30th2013 Soft tissue: An aphthous lesion was observed at the buccal aspect between tooth 13 and tooth 14. A gingival pocket of 5mm was probed at the mesiopalatal aspect of tooth 14. Sensitivity to airspray and explorer was noted on the mesiobuccal side of tooth 37 and palatal side of tooth 15. Dental: Tooth 13 has a composite filling. Tooth 14 has a dental crown and a mesiopalatal subgingival cavity. Tooth 15 has a composite filling. Tooth 37 has an occlusal amalgam filling and a small mesiobuccal.
Fig. 2. Buccal view tooth 14, 15.
Fig. 3. Buccal view tooth 37.

113
Clinical tests August 30th2013 13 14 15 37 EPT nd nd nd nd Cold + + + + Percussion - v&h - - Palpation - + - - PPD 3 5 3 3 Mobility - - - - Biting - - - -
Radiographic findings August 30th2013 Dental: Tooth 14 has a dental crown and a radiolucency is seen in the cervical area of the tooth. Tooth 15 has a MOD composite filling. Tooth 37 has an occlusal radiopaque filling and a possible pathologic radiolucency is seen at the mesial aspect of the tooth. Periodontal: Chronic marginal periodontitis. Apical: Tooth 14 has a lateral radiolucency, mesial aspect, in the coronal third of the root. Teeth 15 and 37 have a continuous PDL space. Based on clinical and radiographic findings, and with the suspicion of an additional resorptive lesion on tooth 37, the patient was referred for cone-beam CT. In addition to cervical resorption on teeth 14 and 37, a cervical resorption on tooth 15 was identified on the CT scans.
Fig. 4. Periapical radiograph with gutta-percha inserted in the periodontal pocket.
Fig. 5. Bite-wing to visualize suspected cavity 37m.
Fig 6. Orthopanthogram.
Radiologic description (in Norwegian) from the Department of Maxillofacial Radiology

114
Fig. 7. CT scan; axial view of the maxillary right first and second premolar with cervical resorption.
Fig. 8. CT scan; sagittal view of mandibular left second molar with cervical resorption. The resorption has not perforated the pulp.
Diagnosis Diagnosis Pulpal within normal limits Periodontal K05.03 chronic marginal
periodontitis Periapical within normal limits Pathologic resorption
K03.38 cervical resorption MIR Multiple idiopathic resorption
Treatment plan Flap-elevation to fill the defects in teeth 37 and 15 externally with composite Surgical extraction of tooth 14. Treatment alternatives were thoroughly discussed: pulpectomy tooth 37 before surgery? Root canal treatment and filling of resorption defect tooth 14?
Problem list Extension of lesion tooth 37. Preservation of bone tooth 14 prior to implant therapy.
Surgery November 19th2013 Surgery tooth 37: Marginal incision from 37 to 35. Cleaning of resorption lacunae: topical application of a 90% aqueous solution of trichloroacetic acid and curettage. Placement of a composite restoration. Suturing. The lesion was more advanced in apical direction than observed on CT scans, displaying fibro-osseous characteristics with deposition of ectopic bonelike calcifications both within the resorbing tissue and directly on the dentin surface. No pulpal perforation.
Prognosis Tooth: Uncertain.
Follow-up examination November 26th2013 (1 week) The patient is having pain. He describes increased sensitivity to cold and warm drinks region 37. Clinically there is drainage of pus from a periodontal pocket at the buccal aspect. Tooth 37 is sensitive to percussion. Treatment: Sterile saline rinse, observation.
Follow-up and treatment December 6th2013 The patient complains about intense pain and increased sensitivity region 37. The pain is worse in the evening; jaw pain that is radiating to the ear. He uses paracetamol/codein at a daily basis. Clinically tooth 37 is hypersensitive to cold stimulus (endo ice), lingering pain. Optimal healing is noted after surgery. Diagnosis: K04.01 acute irreversible pulpitis. The patient is not interested in a root filling. It was decided to extract the tooth non-surgically (Fig. 10, 11).

115
Fig. 9. Periapical radiograph tooth 37, 06.12.2013.
Fig. 10. Buccal view of extracted tooth 37.
Fig. 11. Palatal view of extracted tooth 37.
Histological findings tooth 37 (Laboratorium of pathology, AK Goplen) Diagnosis: “Changes consistent with resorption of cementum and with virtually empty pulp”.
Surgery February 4th2014 Surgery teeth 14 and 15: A palatal marginal incision was made from the canine to the molar region (13-16). Tooth 15: Small resorption defect, minimal osteotomy required, cleaning of
resorption lacunae and placement of composite filling. Tooth 14: Tooth/root sectioning and removal.
Fig. 12. Photo of resorption defects.
Fig. 13. Suturing.
Prognosis Tooth 15: Uncertain.
Follow-up examination February 11th2014 (1 week) Removal of sutures. Healing. No symptoms.
Follow-up examination May 27th2014 The patient describes mild sensitivity to cold in the right maxilla. Two implants are placed in region 14 and 36. Clinically: Teeth 15 and 16 are sensitive to air spray, more pronounced on tooth 16. PPD 4mm tooth 15, palatal aspect. No symptoms on palpation and percussion. A new recall is planned in 6 months.

116
Fig. 14. Periapical radiograph 27.05.2014.
Fig. 15. Periapical radiograph 27.05.2014.
Discussion Invasive cervical resorption (ICR) is defined as ‘a localized resorptive process that commences on the surface of root below the epithelial attachment and the coronal aspect of the supporting alveolar process, namely the zone of the connective tissue attachment’ (1). Characterized by its cervical location and invasive nature, this resorptive process leads to the progressive and usually destructive loss of tooth structure. The resorbed tissue is replaced by highly vascular tissue that may become visible through thin residual enamel as pinkish discoloured tooth (2). Clinically, invasive external resorption is associated with inflammation of the periodontal tissues and does not have any pulpal involvement (3). The pulp remains protected by a thin layer of predentin until late in the process and it has been postulated that bacteria in the sulcus sustain the inflammatory response in the periodontium (1, 4). This feature differentiates cervical
external resorption from another type of inflammatory resorption called external inflammatory resorption, which is continued by necrotic pulp tissues and an infected root canal content (5). The aetiology of invasive cervical resorption is inconclusive, however, several potential predisposing factors have been identified (1): A. Physical trauma a) Orthodontic treatment b) Orthognathic surgery c) Transplanted teeth d) Trauma e) Bruxism f) Guided tissue regeneration B. Chemical Agents a. Intracoronal bleaching b. Secondary bone grafting in unilateral complete cleft palate patient. c. Tetracycline conditioning of root The clinical presentation of invasive cervical resorption varies considerably depending on the extent of the resorptive process. The condition is usually painless and while a pink discoloration of the crown indicates the resorptive process, some teeth give no visual signs and diagnosis is usually the result of a routine or sometimes a chance radiologic examination. Multiple resorptions can occur, particularly when there has been a history of orthodontic treatment and a full mouth radiographic examination should follow the identification of any tooth showing evidence of invasive cervical resorption. Based on the invasiveness of the lesion, Heithersay (4) introduced a clinical classification of invasive cervical resorption (6): Class 1- Denotes a small invasive resorptive lesion near the cervical area with a shallow penetration into dentine Class 2- Denotes a well-defined resorptive lesion that has penetrated close to the coronal pulp chamber but

117
shows little or no extensions into the radicular dentine Class 3- Denotes a deeper invasion of dentine by resorbing tissue, not only involving the coronal dentine but also extending into the coronal third of the root Class 4- Denotes a large invasive resorptive process that has extended beyond the coronal third of the root Early defects are commonly detected as chance findings on radiographs. The severity of the lesion determines its radiographic appearance. The lesion classically presents as an asymmetrical radiolucency with ragged or irregular margins in the cervical region of the tooth. Early lesions might be radiolucent; however, more advanced lesions might have a mottled appearance caused by the osseous nature of the advanced lesion. The outline of the root canal should be visible and intact, indicating that the lesion lies on the outer surface of the root (7). It has been shown that conventional radiographic techniques reveal limited information on the true extent and nature of the resorptive lesion (8). In recent literature, cone beam computed tomography (CBCT), has been used to assess ICR lesions. The position, depth in relation to the root canal, and ultimately the restorability of the tooth can be assessed objectively before any treatment is carried out (8, 9). Heithersay (10) reported on a non-surgical treatment regime that were applied to 101 teeth from 94 patients displaying varying degrees of invasive resorption and followed up for a minimum of 3 years. It involved the topical application of a 90% aqueous solution of trichloroacetic acid to the resorptive tissue, curettage, endodontic treatment where necessary, and
restorations with glass-ionomer cement. The result was complete success in Class 1 and Class 2 resorption. Of the 63 teeth classified with Class 3, 61 (96,8%) showed resorption control. When all factors (resorption control, angular bone loss, periapical changes and extraction) were included in the assessment, the overall success rate of Class 3 treatment was 77,8%. In Class 4 resorption 16 teeth were treated and the results showed a survival rate of 50% and a success rate as judged above 12,5%. This represents an unsatisfactory outcome for this treatment regimen when applied to Class 4 resorption, and alternative prosthodontic replacement is generally suggested (2). Multiple idiopathic cervical root resorption (MICRR) is an uncommonly reported phenomenon that may affect varying numbers of teeth. The condition was first identified 80 years ago by Mueller who reported the first case of idiopathic cervical root resorption in 1930 (11), and since that time approximately 30 cases have been reported (12-25); the number of involved teeth ranges from three to more than 20 per subject (13). The distribution varies from a single region (e.g. mandibular incisors) to most teeth within one arch or more generally distributed throughout the entire dentition. A similar condition involving apical resorption has also been described (26). Most affected individuals are healthy, with non-contributory medical histories. A predilection for young females has been reported (12, 27). An attempt has also been made to link multiple idiopathic cervical root resorption to feline invasive cervical resorption (14, 28). These studies raised the question of a possible role of a feline virus as an etiologic co-factor in MICRR.

118
Liang et al. (12) reviewed the literature on MICRR. They reported the history, clinical findings and radiographic appearance of four unreported cases of multiple idiopathic cervical root resorption and did a systematic literature review of this condition. MICRR was an incidental finding on routine clinical and radiographic examination. No correlation was seen between this type of resorption and any medical or dental finding. Radiographically, the lesions were found to begin at the cemento-enamel junction and then either progress to involve the entire cervical region or, at some point, spontaneously arrest. Those cases that progressed to involve the entire cervical region required extraction. The number of teeth that demonstrated this condition ranged from 5 to 24 per patient. More teeth became involved as the condition was followed in time. There was no detectable frequency of occurrence for any particular dental region or tooth among the involved teeth. Of a total of 18 patients, 13 were females whose ages ranged from 7 years to 68 years. Ten of the 18 patients were Caucasian. In the present case, there was no obvious etiologic factor identified, and the lesion was considered to be idiopathic form.
References 1. Tronstad L. Root resorption:
etiology, terminology and clinical manifestations. Endod Dent Traumatol 1988; 4: 241–252.
2. Heithersay G. Invasive cervical resorption. Endod Topics 2004; 7: 73–92.
3. Frank AL, Torabinejad M. Diagnosis and treatment of extracanal invasive resorption. J Endod 1998; 24(7): 500-504.
4. Heithersay GS. Clinical, radiologic, and histopathologic features of invasive cervical resorption. Quintessence Int 1999; 30: 27-37.
5. Andreasen JO. External root resorption: its implication in dental traumatology, paedodontics, periodontics, orthodontics and endodontics. Int Endod J 1985; 18(2): 109-118.
6. Heithersay GS. Treatment of invasive cervical resorption: An analysis of results using topical application of trichloroacetic acid, curettage, and restoration. Quintessence Int 1999; 30: 96-110.
7. Patel S, Kanagasingam S, Ford TP. External Cervical Resorption: A Review. J Endod 2009; 35: 616–625.
8. Patel S, Dawood A, Whaites E, Pitt Ford T. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J 2007; 40: 818–830.
9. Cohenca N, Simon JH, Mathur A, Malfaz JM. Clinical indications for digital imaging in dento-alveolar trauma: part 2—root resorption. Dent Traumatol 2007; 23: 105–113.
10. Heithersay GS. Treatment of invasive cervical resorption: An analysis of results using topical application of trichloroacetic acid, curettage, and restoration. Quintessence Int 1999; 30: 96-110.
11. Mueller E, Rony HR. Laboratory studies of an unusual case of resorption. J Am Dent Assoc 1930; 17: 326–334.
12. Liang H, Burkes EJ, Frederiksen NL. Multiple idiopathic cervical

119
root resorption: systematic review and report of four cases. Dentomaxillofac Radiol 2003; 32: 150–155.
13. Iwamatsu-Kobayashi Y, Satoh-Kuriwada S, Yamamoto T, Hirata M, Toyoda J, Endo H, Kindaichi K, Komatsu M. A case of multiple idiopathic external root resorption: a 6-year follow-up study.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100(6): 772-779.
14. vonArx T, Schawalder P, Ackermann M, Bosshardt DD. Human and feline invasive cervical resorption: the missing link?--Presentation of four cases J Endod. 2009; 35(6): 904-913.
15. Yu VSH, Messer HH, Tan KB. Multiple idiopathic cervical resorption: case report and discussion of management options. Int Endod J 2011; 44: 77–85.
16. Jiang YH, Lin Y, Ge J, Zheng JW, Zhang L, Zhang CY. Multiple idiopathic cervical root resorption: report of one case with 8 teeth involved successively. Int J Clin Exp Med. 2014; 7(4): 1155-1159.
17. D.I. George, R.L. Miller. Idiopathic resorption of teeth: a report of three cases. Am J Orthod 1986: 89: 13–20.
18. P.H. Kim, H.B. Heffez. Multiple idiopathic resorption in the primary dentition. Review of the literature and case report Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88: 501–505.
19. H.G. Carr Multiple idiopathic resorption of teeth Br Dent J 1958; 105: 455–456.
20. D.A. Kerr, R.M. Courtney, E.J. Burkes Multiple idiopathic root resorption Oral Surg Oral Med Oral Pathol 1979; 29: 552–565.
21. R. Hopkins, D. Adams Multiple idiopathic resorption of the teeth Br Dent J 1979; 146: 309–312.
22. Lydiatt DD, Hollins RR, Peterson G. Multiple idiopathic root resorption: diagnostic considerations Oral Surg Oral Med Oral Pathol 1989; 67: 208–210.
23. Moody AB, Speculand B, Smith AJ, Basu MK . Multiple idiopathic external resorption of teeth Int J Oral Maxillofac Surg 1999; 19: 200–202.
24. Moody GH, Muir KF. Multiple idiopathic root resorption. J Clin Periodontol 1991; 18: 577–580.
25. Beckett HA, Gilmour AG. Multiple idiopathic cervical root resorption in a male. Br Dent J 1993; 175: 33–34.
26. Cholia SS, Wilson PH, Makdissi J. Multiple idiopathic external apical root resorption: report of four cases. Dentomaxillofac Radiol 2005; 34(4): 240-246.
27. Macdonald-Jankowski D. Multiple idiopathic cervical root resorption most frequently seen in younger females. Evid Based Dent 2005; 6(1): 20.
28. DeLaurier A, Boyde A, Jackson B, Horton MA, Price JS. Identifying early osteoclastic resorptive lesions in feline teeth: a model for understanding the origin of multiple idiopathic root resorption. J Periodontal Res 2009; 44(2): 248-257.









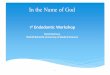



![Diagnostic biomarker candidates for pulpitis revealed by … · 2020. 10. 12. · pulpitis is considered reversible or irreversible [10]. However, histopathological examinations have](https://img.pdfslide.us/doc/110x75/61177d015a9fb078113cd46d/diagnostic-biomarker-candidates-for-pulpitis-revealed-by-2020-10-12-pulpitis.jpg)