Embed Size (px)
Citation preview

IN THE NAME OF GOD

Pulpal and Periapical Disease
CHAPTER 3
Dr . Kheirandish Oral and maxillofacial pathology

Pulpitis
Periapical Granuloma
Periapical Cyst
Osteomyelitis
Osteomyelitis with Proliferative Periostitis
Alveolar Osteitis

PULPITIS
1. Mechanical damage
Traumatic accidents, iatrogenic damage, attrition, abrasion
2. Thermal injury
Large uninsulated metallic restorations, dental procedures
(cavity preparation, polishing)
3. Chemical irritation
Erosion , acidic dental materials
4. Bacterial effects
toxins or directly (caries)

I. Reversible pulpitis
I. Irreversible pulpitis
PULPITIS
Mimic pulpalgia : Myofascial pain
Trigeminal neuralgia
Atypical facial neuralgia
Migraine headaches
Cluster headaches
Nasal or sinus pathoses
Angina pectoris

Reversible pulpitis
Temperature extremes : short duration /mild-to-moderate
pain.
Cold,sweet or sour : pain
The pain does not occur without stimulation and subsides
within seconds after the stimulus is removed.
Electric pulp testing : lower levels
Mobility and sensitivity : absent.
Without treatment : Iirreversible

Irreversible pulpitis
Early stages :
o Sharp, severe pain on thermal stimulation
o Pain continues after the stimulus is removed
o Cold and heat
o Spontaneous or continuous pain
o Lies down
o Electric pulp testing : lower levels
o Early stages : localized pain / increasing discomfort : unable
to identify the offending tooth
Early stages
Later stages

Later stages :
o Increases pain
o Throbbing pressure
o Awake at night.
o Heat increases the pain
o Cold decrease pain
o Electric pulp testing : higher levels / -
o Mobility and sensitivity: absent
o Drainage (crown fracture, fistula formation) : symptoms resolve

CHRONIC HYPERPLASTIC PULPITIS
(pulp polyp)
Pulpal inflammation
Children and young adults
Large pulp exposures
Deciduous or succedaneous molars
Asymptomatic (masticatory function)


HISTOPATHOLOGIC FEATURES
Reversible pulpitis :
Hyperemia
Edema
Few inflammatory cells
Irreversible pulpitis :
Congestion of the venules
Chronic hyperplastic pulpitis :
Inflamed granulation tissue
Histopathologically resembles a pyogenic granuloma

TREATMENT AND PROGNOSIS
Reversible pulpitis
Removal the local irritant
Irreversible and chronic hyperplastic puIpitis
Root canal therapy
Extraction

PERIAPICAL GRANULOMA
(CHRONIC APICAL PERIODONTITIS)
Chronically inflamed granulation tissue
Apex of a nonvital tooth
Not true granulomatous inflammation microscopically
Apical periodontitis
Bacterial ( Yeasts / Cytomegalovirus / Epstein-Barr virus )
75% of apical inflammatory lesions

Early stages
Acute apical periodontitis
Constant dull / Throbbing pain
Vitality test : - / delayed positive
Pain : biting or percussion
Radiographic : -
Neutrophils
Prostaglandins ( activate osteoclasts )

Late stages
Asymptomatic
Radiographic : +
Response to thermal or electric pulp tests : -
Mobility or significant sensitivity to percussion
Chronic inflammatory cells (lymphocytes)
Reduce osteoclastic activity
Fibroblastic activity
Periapical cyst formation

Routine radiographic examination
Radiographic features are not diagnostic
Variable radiolucencies
Loss of apical lamina dura
Circumscribed or ill-defined
Root resorption
RG



Phoenix abscess : Secondary acute inflammatory changes
within a periapical granuloma
Unable to distinguish periapical granulomas from
periapical cysts
Greater than 200 mm2 : periapical cysts
Periapical inflammatory disease is not static and
granulomas can transform into cysts or abscesses

HISTOPATHOLOGIC FEATURES
Inflamed granulation tissue
Surrounded by a fibrous connective tissue wall
Lymphocytes ( neutrophils. plasma cells. Histiocytes )
Plasma cells :
Eosinophilic globules of gamma globulin (Russell
bodies)
Basophilic particles (Pyronine bodies)
Not specific

Rests of Malassez
Giant cells
Red blood cell extravasation
Hemosiderin pigmentation
Cholesterol clefts
Source of the cholesterol clefts is unclear (dying
inflammatory Cells / disintegrating red blood cells /
degenerating cystic epithelium)


TREATMENT AND PROGNOSIS
Root canal therapy
Goal of endodontics : reduce the microbial load
Extraction and curettage

Fail to heal :
Cyst formation
Persistent pulpal infection
Accumulation of endogenous debris
Associated periodontal disease
Penetration of the adjacent maxillary sinus
Fibrous scar formation

Periapical surgery:
larger than 2 cm
Endodontic therapy : -
All soft tissue removed during periapical surgical procedures
should be submitted for histopathologic examination.
Periapical fibrous scars :
facial and lingual cortical plates have been lost and lesions fill with
dense collagenous tissue rather than normal bone( Surgery - )

PERIAPICAL CYST
(RADICULAR CYST;
APICAL PERIODONTAL CYST)
Prevalence : 15%
Epithelium at the apex of a nonvital tooth presumably
can be stimulated by inflammation to form a true
epithelium-lined cyst ( periapical cyst ).
Keratinocyte growth factor (increased proliferation of
normally quiescent Epithelium)

Source of the epithelium :
Rest of Malassez
Crevicular epithelium
Sinus lining
Epithelial lining of fistulous tracts
Periapical pocket cysts
incomplete epithelial lining
Periapical true cysts
complete epithelium lined
(baglike structure)
PERIAPICAL CYST

Lateral radicular cyst
Along the lateral aspect
Rests of Malassez
Pulpal necrosis
Radiographically : mimic developmental lateral
periodontal cysts
Residual periapical cyst
Dystrophic calcification /radiopacity




Grow slowly
Nonvital
No symptoms
large size (swelling and mild sensitivity)
Mobility of adjacent teeth
Radiographic : resemble periapical granuloma
Greater size than periapical granulomas
Loss of lamina dura
Root resorption is common
Significant growth



Stratified squamous epithelium
Exocytosis
Spongiosis
Hyperplasia
Mucous cells
Ciliated pseudostratified columnar epithelium
HISTOPATHOLOGIC FEATURES


Rushton bodies (Arch-shaped calcifications)
Dystrophic calcification
Cholesterol clefts
Multinucleated giant cells
Red blood cells
Hemosiderin
Inflammatory infiltration (lymphocytes,neutrophils,plasma
cells,histiocytes,mast cells and eosinophils)
Hyaline bodies (pulse granuloma,giant-cell hyaline
angiopathy)
Chronic intraosseous inflammation


TREATMENT AND PROGNOSIS
Nonsurgical
Surgical
Extraction
Biopsy is indicated

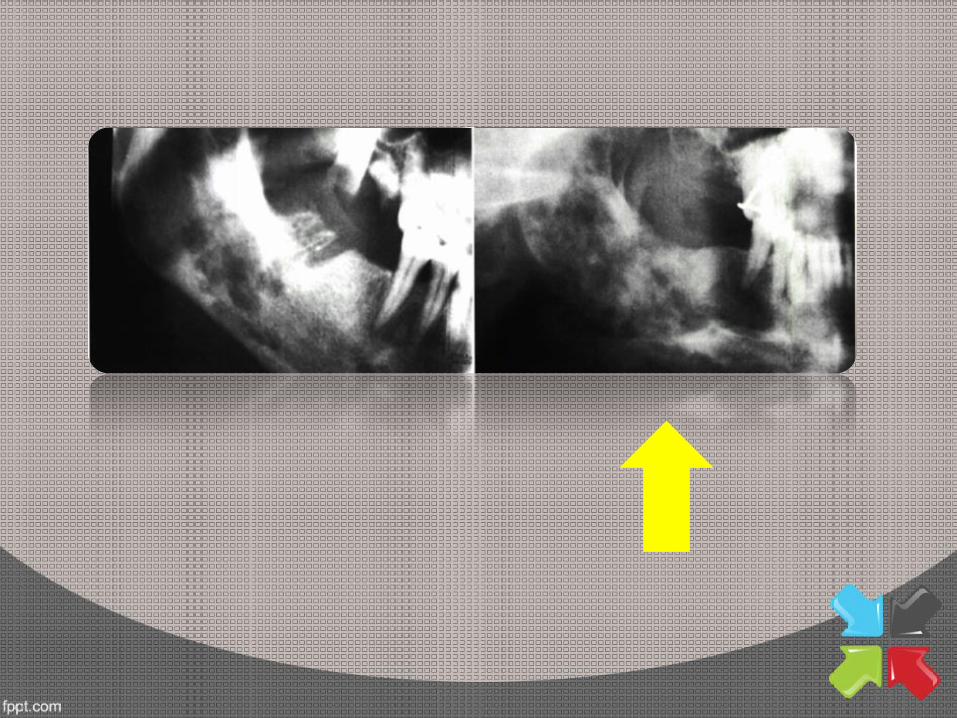
OSTEOMYELITIS
Osteomyelitis is an acute or chronic inflammatory process
in the medullary spaces or cortical surfaces of bone that
extends away from the initial site of involvement.
Bacterial infections
Lytic destruction of the involved bone
All ages
Male
Mandible

Osteoradionecrosis (hypoxia,hypocellularity and
hypovascularity)
Uncommon in developed countries
Developd countries : Odontogenic infections or
traumatic fracture
Africa : acute necrotizing ulcerative gingivitis (ANUG)
or NOMA.

Predispose people to osteomyelitis:
o Chronic systemic diseases
o Immunocompromised status
o Disorders associated with decreased vascularity
o Tobacco
o Alcohol
o IV drug abuse
o Diabetes mellitus
o Malaria
o Sickle cell anemia
o Malnutrition
o Malignancy
o AIDS
o Radiation
o Diseases (e.g., osteopetrosis, late Paget's disease,
end-stage cementoosseous dysplasia)

Acute suppurative osteomyelitis
Young patients
Signs and symptoms
Acute inflammatory process
1 month in duration
Swelling: may be present
Fever
Leukocytosis
Lymphadenopathy
Significant sensitivity

Radiographs : unremarkable / ill-defined radiolucency
Paresthesia of the lower lip
Necrotic bone
Sequestrum
Fragment of necrotic bone
Spontaneous exfoliation
Involucrum
Necrotic bone surrounded by new vital bone


Chronic suppurative osteomyelitis
If acute osteomyelitis is not resolved or primarily without a
previous acute episode.
Granulation tissue
Dense scar tissue
Swelling

Pain
Sequestrum formation
Tooth loss
Pathologic fracture
Radiographs : patchy, ragged. and ill-defined radiolucency
(central radiopaque)

HISTOPATHOLOGIC FEATURES
ACUTE SUPPURATIVE OSTEOMYELITIS
Biopsy not common (lack of a soft tissue component)
Necrotic bone
Loss of the osteocytes
Peripheral resorption
Bacterial colonization
Acute inflammatory cells
CHRONIC SUPPURATIVE OSTEOMYELITIS
Significant soft tissue component Chronically inflamed fibrous connective
Scattered sequestra
Abscess formation

TREATMENT AND PROGNOSIS
ACUTE SUPPURATIVE OSTEOMYELITIS
Antibiotic therapy
CHRONIC SUPPURATIVE OSTEOMYELITIS
Surgical Intervention
Antibiotic therapy

OSTEOMYELITIS WITH PROLIFERATIVE
PERIOSTITIS (PERIOSTITIS OSSIFICANS)
Garre sosteomyelitis
Periosteal reaction to the presence of inflammation
Periosteum : Several rows of reactive vital bone that
parallel each other
Children and young adults (13 y/o)
premolar and molar (mandible)
Radiopaque laminations of bone (NO=1 to 12 )


Dental caries
( periapical inflammatory disease, Periodontal infections,
fractures, buccal bifurcation cysts, and nonodontogenic
infections)
Causes of periosteal new bone formation :
Osteomyelitis
Trauma
Cysts
Fluorosis
Avitaminosis C
Congenital syphilis
Neoplasms (Ewing sarcoma, Langerhans cell histiocytosis, and
osteogenic sarcoma)
o CT scanning
o Panoramic
o Lateral oblique
o Occlusal
o posteroanterior

ALVEOLAR OSTEITIS
(DRY SOCKET; FIBRINOLYTIC ALVEOLITIS)
• Destruction of the initial clot ( plasminogen to plasmin)
• Mandible (posterior areas) :Impacted mandibular third molars
• 20 - 40 y/o
o Poor oral hygiene o Inexperienced surgeons o Traumatic extractions o Oral contraceptive o Presurgical infections o Tobacco

• Dirty gray clot
• Bare bony socket
• Sensitive bone
• Severe pain
• Foul odor
• 3 to 4 days
• 10 to 40 days

High risk patients :
Oral contraceptives
Smoke
Pericoronitis
Traumatic extractions
History of alveolar osteitis

TREATMENT AND PROGNOSIS
Curettage of the socket is not recommended,
Eugenol (every 24 hours for the first 3 days)