Embed Size (px)
Citation preview
University of Kansas Medical Center Psychiatry Residency Training Program
Clinical Services/Goals and Objectives
University of Kansas Medical Center Psychiatry Adult Inpatient Service Psychiatry Adult Outpatient Service Psychiatry Consult Service Psychiatric Emergency Liaison Service (PLS) Methadone Clinic Pain Management Service Neurology Service Internal Medicine Service Kansas City Veterans Affairs Medical Center Psychiatry Adult Inpatient Service Psychiatry Intensive Substance Abuse Treatment Program Psychiatry Adult Outpatient Service Psychiatry Consult Service/Chief Resident Internal Medicine Service Dwight D. Eisenhower Veterans Administration Medical Center Neurology Service Psychiatry Adult Outpatient Clinic Colmery O’Neill Veterans Affairs Medical Center Acute Inpatient Psychiatry Service Geriatric Psychiatry Service Internal Medicine Service Johnson County Mental Health Center (Community Mental Health Affiliate) Adult Psychiatry Outpatient Service Community Psychiatry Wyandot Center for Community Behavioral Healthcare (Community Mental Health Affiliate) Adult Psychiatry Outpatient Service Marillac Child and Adolescent Psychiatry
UNIVERSITY OF KANSAS MEDICAL CENTER a. PSYCHIATRY ADULT INPATIENT SERVICE b. Required 4‐6 month rotation occurring mostly in the PGY1 and PGY2 year. c. KUMC inpatient faculty and staff include two FTE Psychiatrists, two FTE Ph.D.
Psychologists, one masters level licensed professional counselor who also administers psychological testing, and one FTE psychiatric social worker. Working together in two teams, they attend to patient needs and provide clinical training and supervision to residents.
d. Residents spend approximately 2‐3 hours in Multidisciplinary Treatment Planning two days per week, and meet with the team staff attending more informally on all other days to review patient progress and make rounds. All new patients are staffed within 24‐hours of admission. Residents spend the majority of their time taking primary care of patients under the supervision of their attending, learning psychopharmacology, individual and group psychotherapy, family therapy, crisis intervention, and electroconvulsive therapy. Residents have the opportunity to order and observe clinical correlation of commonly administered psychological and neuropsychological tests. They also teach and supervise medical students. Residents are expected to stay current with the medical management of medical and surgical comorbidities in their patients, and to use consultation services from medicine, surgery, and subspecialty programs as appropriate.
e. The ethnic and racial makeup of the inpatient population is about 58% female and 42% male; 72% Caucasian, 22% African American, 3% Hispanic, 1% Oriental or Asian, 1% Native American and 1% other. Ages range from 18 to the elderly with 22% age 18‐30, 59% age 31‐50, 12% age 51‐65, and 7% age 66‐100. A wide cross‐section of the diagnostic spectrum is represented among the patient population. Approximately 50% fall in the Mood Disorder group. Thirty‐one percent have schizophrenia or other psychotic disorders, 2% have organic disorders, 1% are substance abusers (many of whom have a dual diagnosis), and the remaining 17% comprise other diagnostic groups such as adjustment disorders, impulse control disorders, and personality disorders.
f. An average caseload consists of 4‐8 patients throughout the rotation. Treatment modalities include group psychotherapy, individual psychotherapy (utilizing primarily cognitive, interpersonal and psychodynamic approaches), medication, therapeutic structure, occupational therapy and recreational therapy.
g. Residents and medical students receive ongoing supervision by their attending through individual case review and rounds on a daily basis. Multidisciplinary treatment planning staffing includes teaching by various members and is held twice weekly. In addition, residents are required to have two hours of individual supervision per week with their assigned psychiatry supervisor.
h. Faculty who rotate on the inpatient service have various areas of interest, including forensic psychiatry, eating disorders, substance abuse issues, affective and anxiety disorders and mental retardation.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: ADULT INPATIENT PSYCHIATRY LEVEL: PGY1 AND PGY2 DURATON: 6‐8 MONTHS (PG1); 10‐12 MONTHS (PG2) SITE: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KU HOSPITAL
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
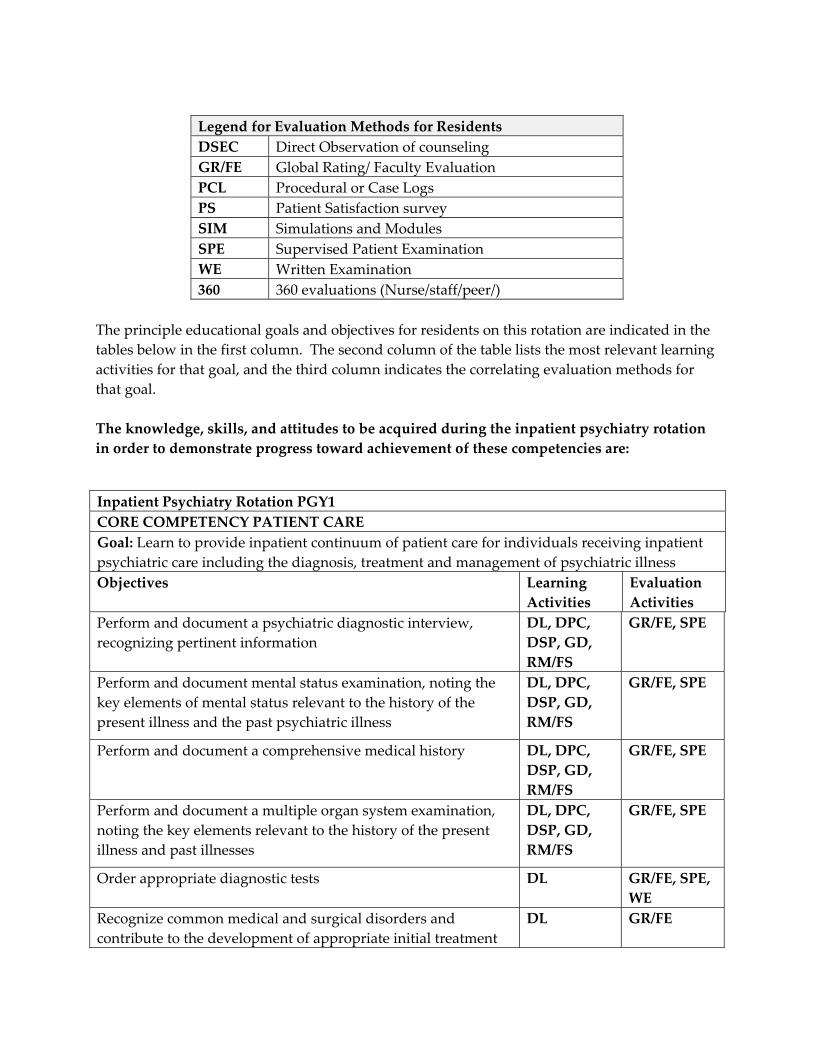
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. The knowledge, skills, and attitudes to be acquired during the inpatient psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Inpatient Psychiatry Rotation PGY1 CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illness Objectives Learning
Activities Evaluation Activities
Perform and document a psychiatric diagnostic interview, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Order appropriate diagnostic tests DL GR/FE, SPE, WE
Recognize common medical and surgical disorders and contribute to the development of appropriate initial treatment
DL GR/FE
5
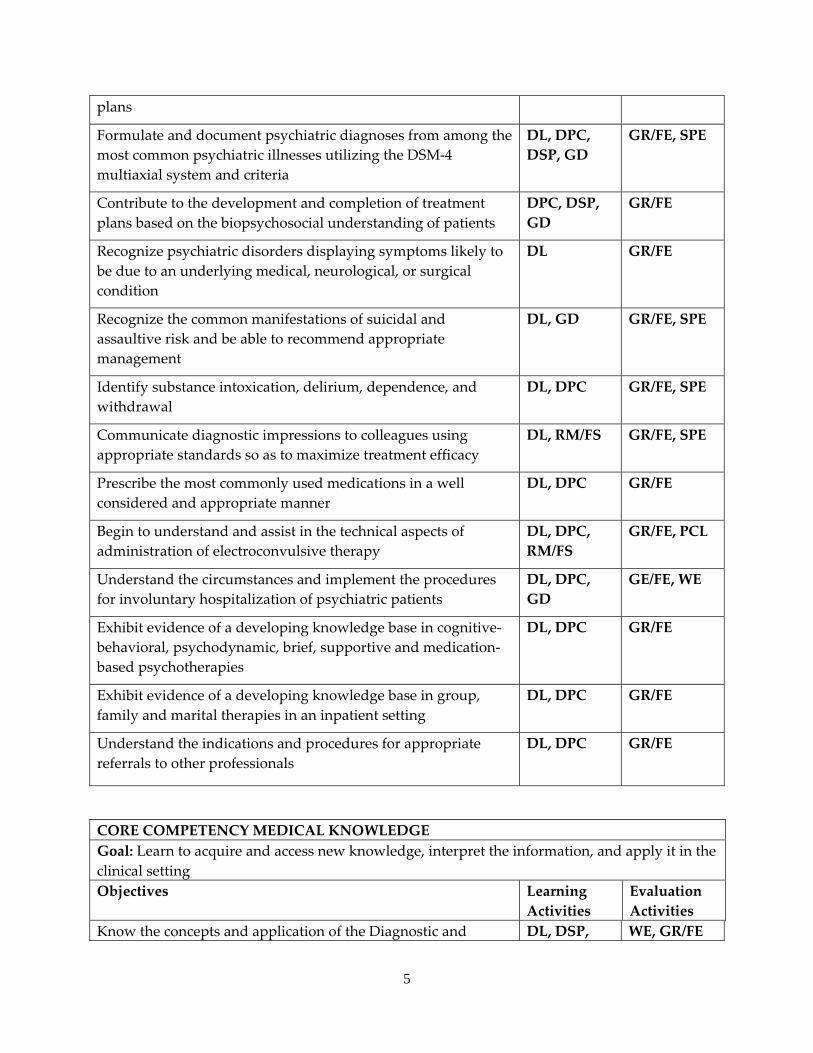
plans
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DL, DPC, DSP, GD
GR/FE, SPE
Contribute to the development and completion of treatment plans based on the biopsychosocial understanding of patients
DPC, DSP, GD
GR/FE
Recognize psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL GR/FE
Recognize the common manifestations of suicidal and assaultive risk and be able to recommend appropriate management
DL, GD GR/FE, SPE
Identify substance intoxication, delirium, dependence, and withdrawal
DL, DPC GR/FE, SPE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe the most commonly used medications in a well considered and appropriate manner
DL, DPC GR/FE
Begin to understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GE/FE, WE
Exhibit evidence of a developing knowledge base in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Exhibit evidence of a developing knowledge base in group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and DL, DSP, WE, GR/FE
6
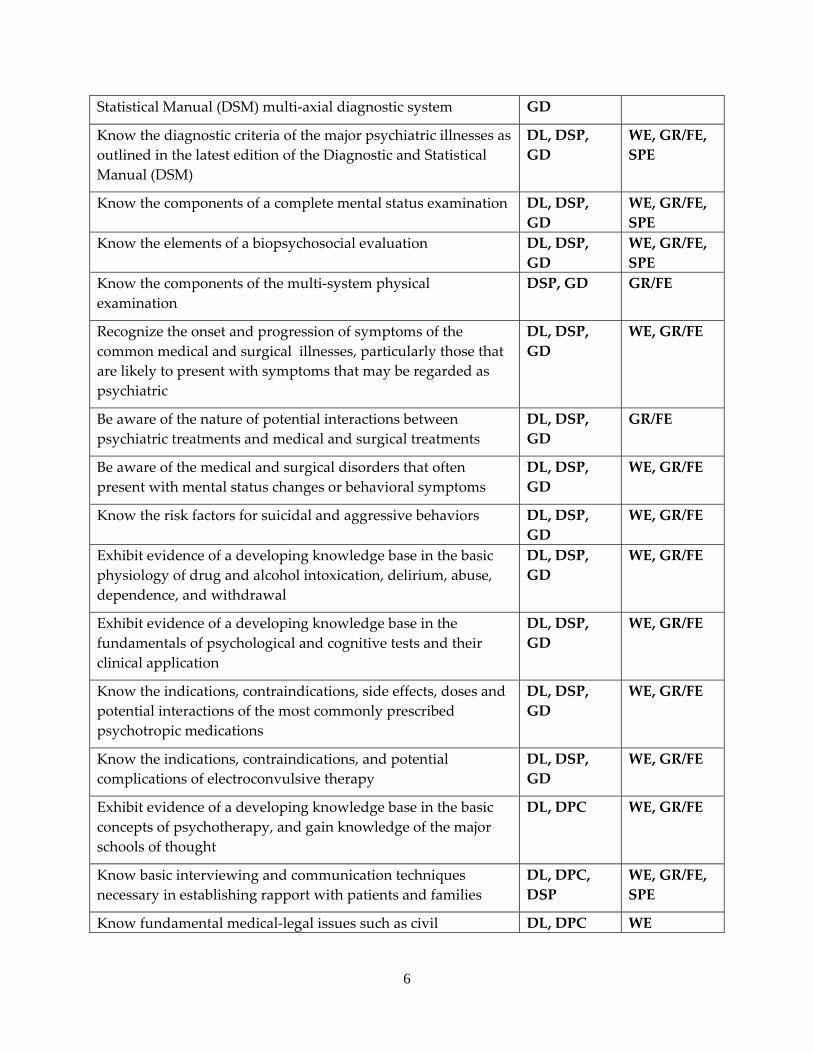
Statistical Manual (DSM) multi‐axial diagnostic system GD
Know the diagnostic criteria of the major psychiatric illnesses as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Recognize the onset and progression of symptoms of the common medical and surgical illnesses, particularly those that are likely to present with symptoms that may be regarded as psychiatric
DL, DSP, GD
WE, GR/FE
Be aware of the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Be aware of the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of the most commonly prescribed psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil DL, DPC WE
7
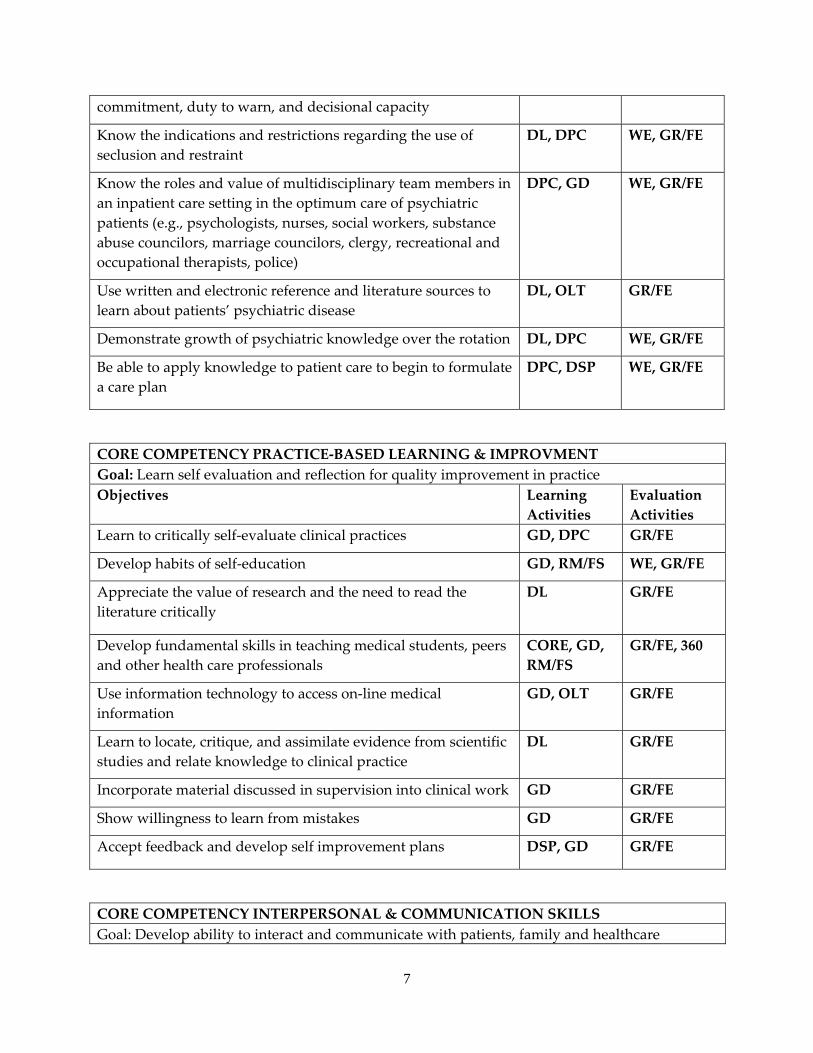
commitment, duty to warn, and decisional capacity
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and occupational therapists, police)
DPC, GD WE, GR/FE
Use written and electronic reference and literature sources to learn about patients’ psychiatric disease
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
Be able to apply knowledge to patient care to begin to formulate a care plan
DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Learn to critically self‐evaluate clinical practices GD, DPC GR/FE
Develop habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Develop fundamental skills in teaching medical students, peers and other health care professionals
CORE, GD, RM/FS
GR/FE, 360
Use information technology to access on‐line medical information
GD, OLT GR/FE
Learn to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare
8
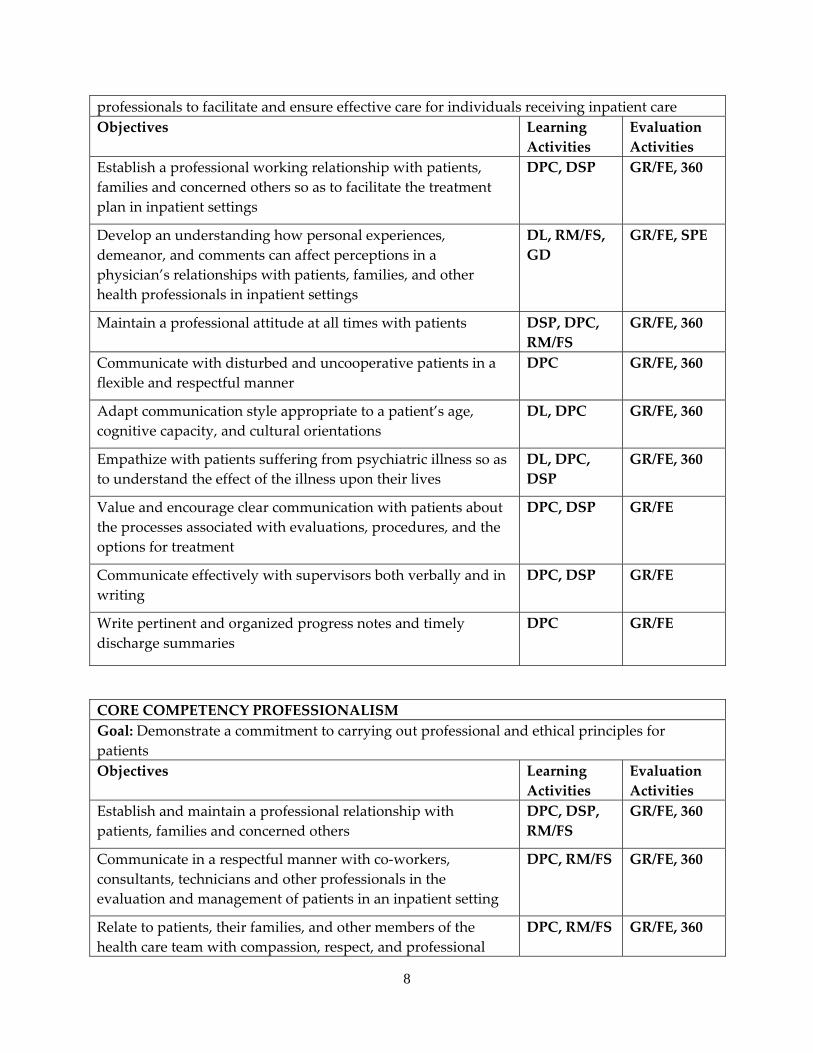
professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, RM/FS, GD
GR/FE, SPE
Maintain a professional attitude at all times with patients DSP, DPC, RM/FS
GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors both verbally and in writing
DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional
DPC, RM/FS GR/FE, 360
9
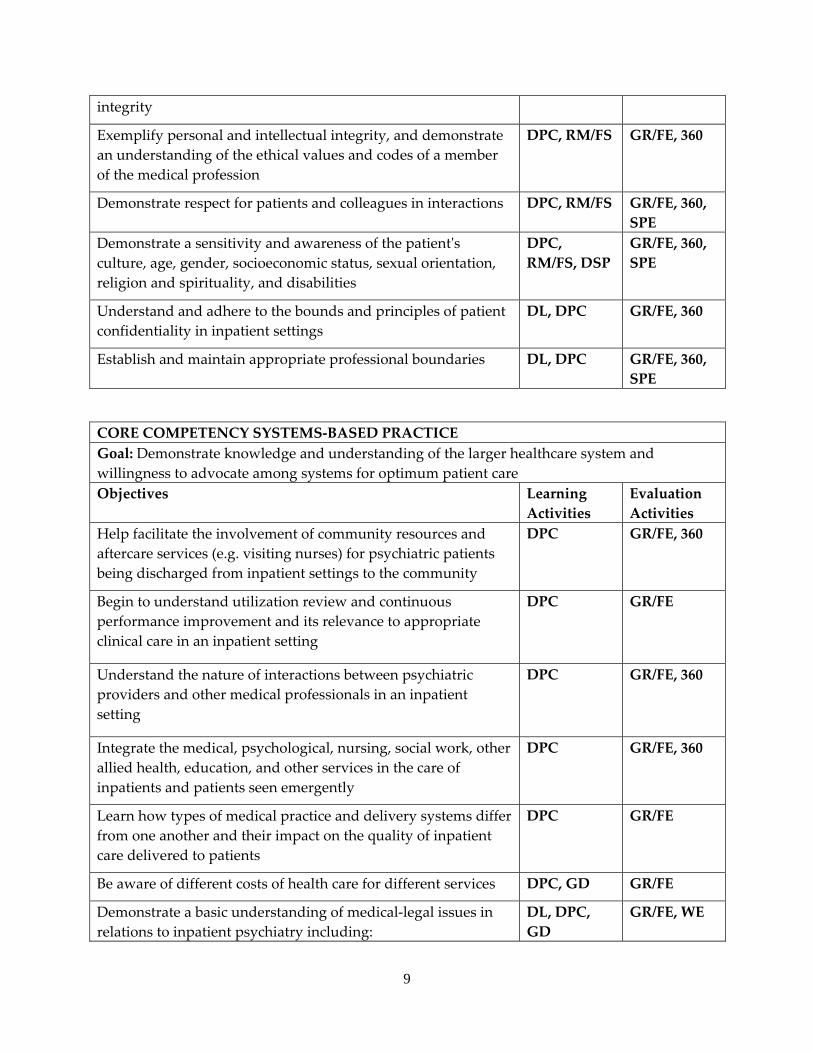
integrity
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/FE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC GR/FE, 360
Begin to understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Learn how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate a basic understanding of medical‐legal issues in relations to inpatient psychiatry including:
DL, DPC, GD
GR/FE, WE
10
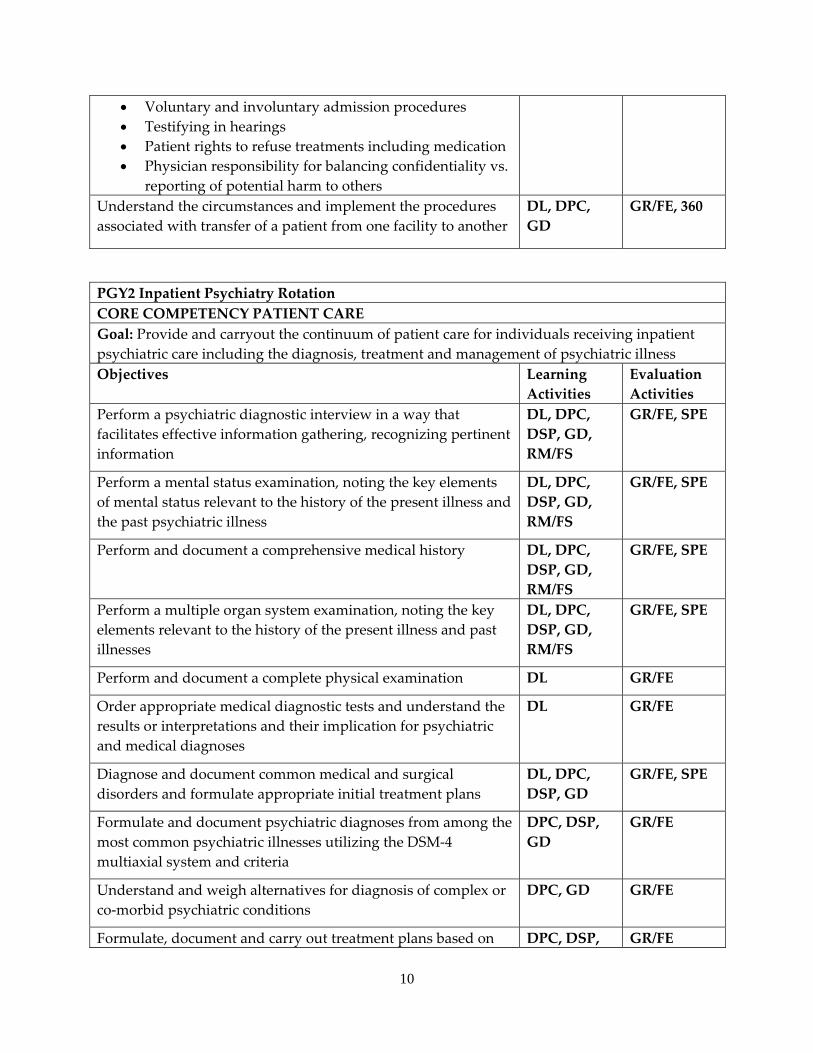
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360
PGY2 Inpatient Psychiatry Rotation CORE COMPETENCY PATIENT CARE Goal: Provide and carryout the continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illnessObjectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview in a way that facilitates effective information gathering, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a complete physical examination DL GR/FE
Order appropriate medical diagnostic tests and understand the results or interpretations and their implication for psychiatric and medical diagnoses
DL GR/FE
Diagnose and document common medical and surgical disorders and formulate appropriate initial treatment plans
DL, DPC, DSP, GD
GR/FE, SPE
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DPC, DSP, GD
GR/FE
Understand and weigh alternatives for diagnosis of complex or co‐morbid psychiatric conditions
DPC, GD GR/FE
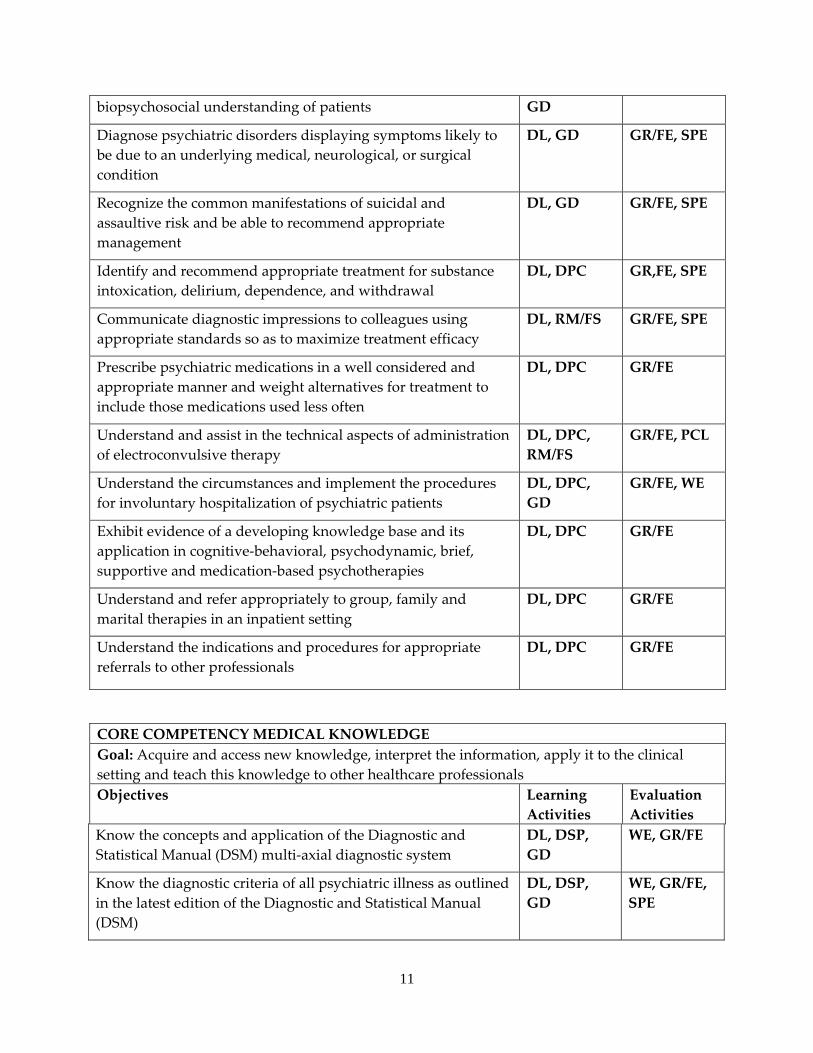
Formulate, document and carry out treatment plans based on DPC, DSP, GR/FE
11
biopsychosocial understanding of patients GD
Diagnose psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL, GD GR/FE, SPE
Recognize the common manifestations of suicidal and assaultive risk and be able to recommend appropriate management
DL, GD GR/FE, SPE
Identify and recommend appropriate treatment for substance intoxication, delirium, dependence, and withdrawal
DL, DPC GR,FE, SPE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe psychiatric medications in a well considered and appropriate manner and weight alternatives for treatment to include those medications used less often
DL, DPC GR/FE
Understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GR/FE, WE
Exhibit evidence of a developing knowledge base and its application in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Understand and refer appropriately to group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionals Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and Statistical Manual (DSM) multi‐axial diagnostic system
DL, DSP, GD
WE, GR/FE
Know the diagnostic criteria of all psychiatric illness as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
12
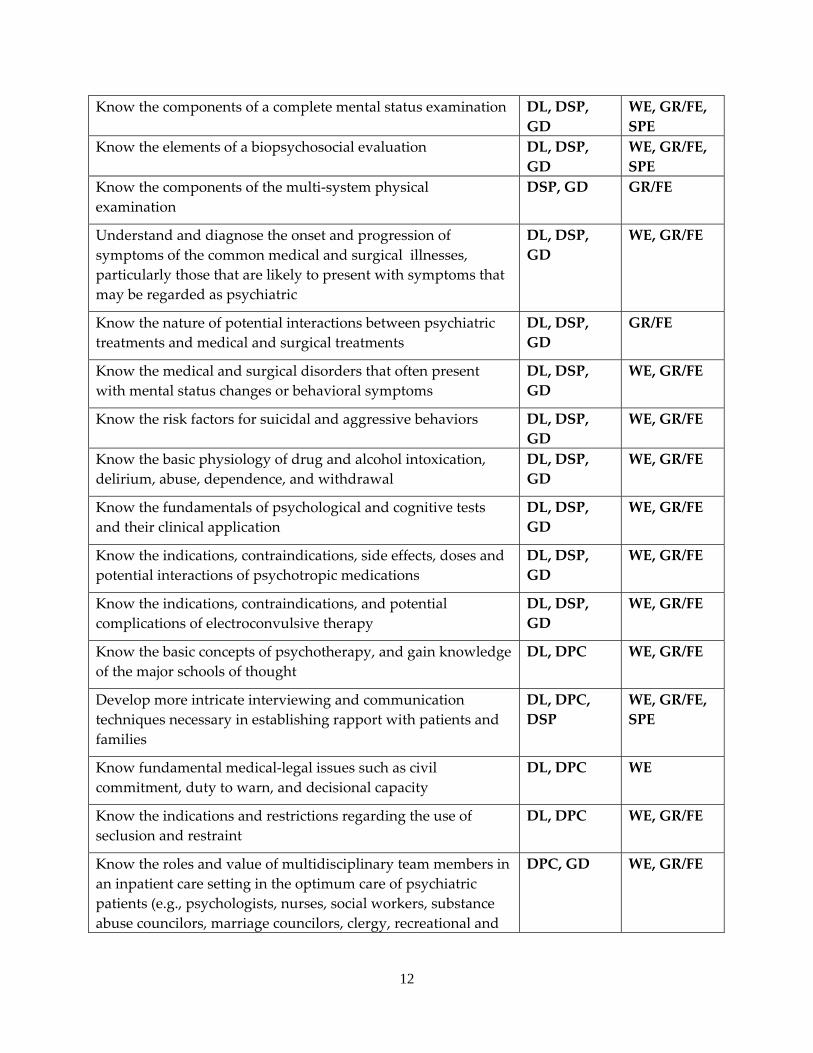
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Understand and diagnose the onset and progression of symptoms of the common medical and surgical illnesses, particularly those that are likely to present with symptoms that may be regarded as psychiatric
DL, DSP, GD
WE, GR/FE
Know the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Know the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Know the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Know the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Develop more intricate interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil commitment, duty to warn, and decisional capacity
DL, DPC WE
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and
DPC, GD WE, GR/FE
13
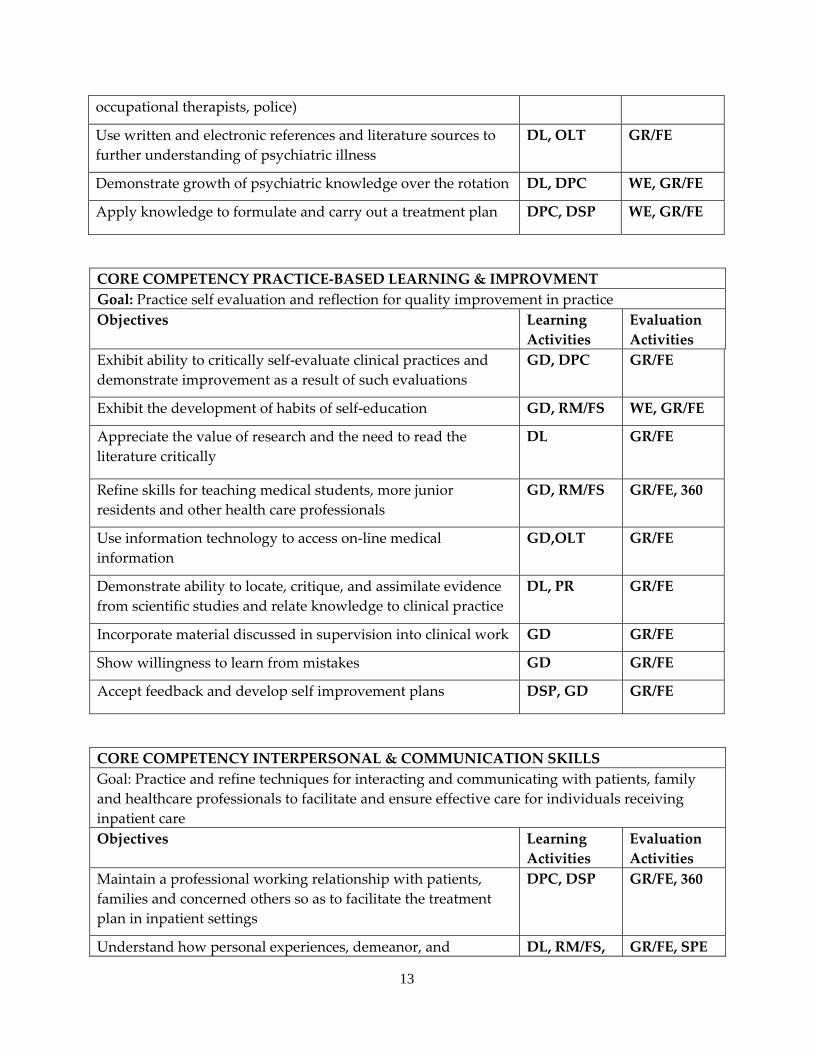
occupational therapists, police)
Use written and electronic references and literature sources to further understanding of psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
Apply knowledge to formulate and carry out a treatment plan DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Exhibit ability to critically self‐evaluate clinical practices and demonstrate improvement as a result of such evaluations
GD, DPC GR/FE
Exhibit the development of habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Refine skills for teaching medical students, more junior residents and other health care professionals
GD, RM/FS GR/FE, 360
Use information technology to access on‐line medical information
GD,OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, PR GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Maintain a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
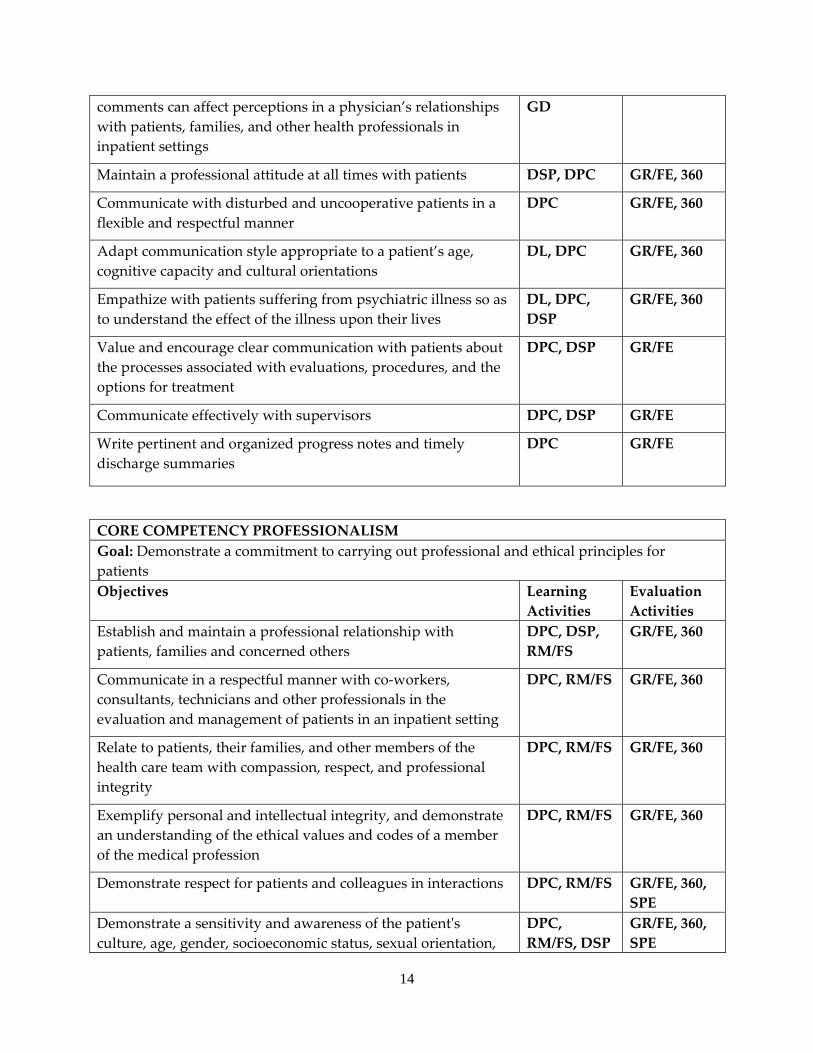
Understand how personal experiences, demeanor, and DL, RM/FS, GR/FE, SPE
14
comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
GD
Maintain a professional attitude at all times with patients DSP, DPC GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation,
DPC, RM/FS, DSP
GR/FE, 360, SPE
15
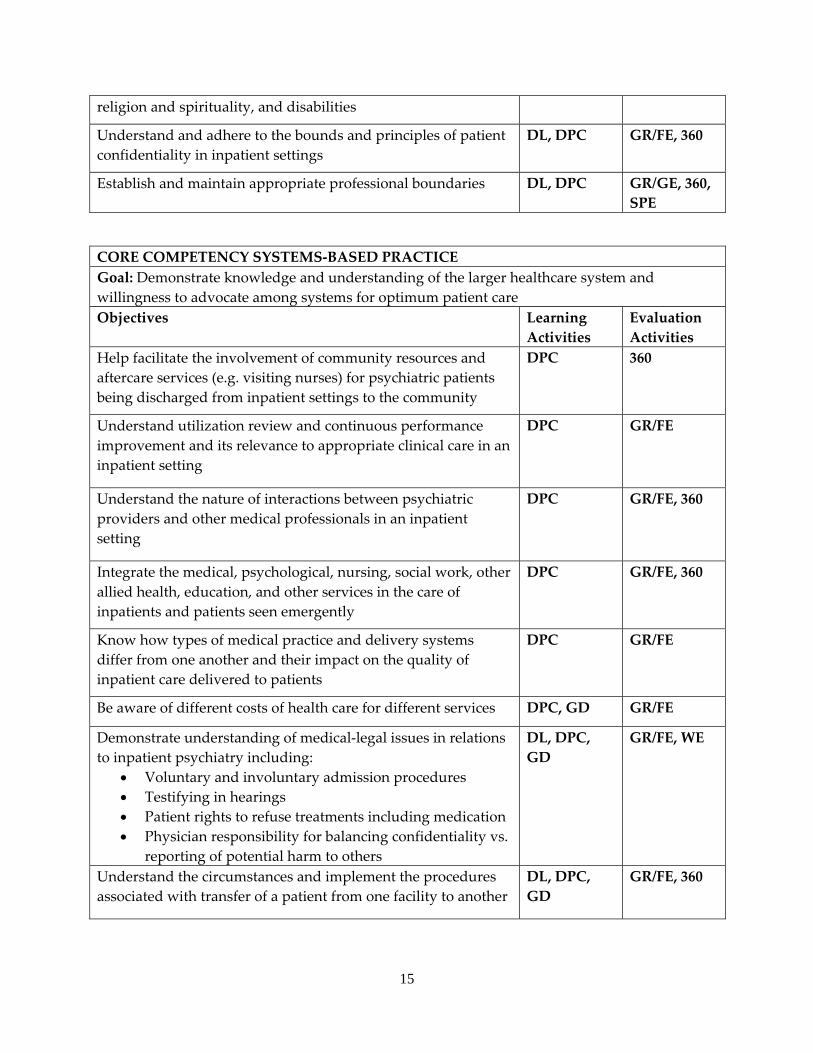
religion and spirituality, and disabilities
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/GE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC 360
Understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Know how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate understanding of medical‐legal issues in relations to inpatient psychiatry including:
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others
DL, DPC, GD
GR/FE, WE
Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360
16
PSYCHIATRY ADULT OUTPATIENT SERVICE a. Required continuous 12 month rotation occurring mostly in the PGY3 year and
occasionally in the PGY2 year. Most residents are assigned on a half‐time basis for the 12 months to the KUMC clinic and half time for 6 months to a community Mental Health Center (Johnson County or Wyandot) and half time for 6 months to a VA outpatient clinic (Kansas City or Leavenworth).
b. The regular outpatient clinic faculty at KUMC consists of two full‐time psychiatrists and four part‐time psychiatrists, one of whom is always present and directly supervising residents in the clinic. The clinic also consists of one full‐time psychologist and one full time social worker.
c. The residents spend 1.5 hours a week in formal didactic or interviewing skill conferences. This is in addition to their other weekly didactic requirements. All patients seen by residents are discussed by the resident with the faculty while the patient is in the clinic and the patient briefly interviewed by the faculty. Faculty review, add comments and sign all resident documentation. Caseloads are carefully monitored and controlled for both breadth and variety of experience.
d. The clinic population is 48% men and 52% women. The average patient age is 43 (42 for men; 43 for women) with a range of 18‐88. The percentage of Caucasian patients is 81%, 14% African‐American, and 5% other ethnic groups. Frequent diagnoses include major affective disorders, substance abuse/dependence, developmental disabilities, and various psychotic disorders including schizophrenia, panic disorder, obsessive compulsive disorder, PTSD, eating disorders, adjustment disorders, and a variety of personality disorders. Residents have experience in medication management and various types of individual psychotherapy.
e. An average caseload at KUMC is 125‐150 patients. The composition includes approximately 5‐10 patients in individual psychotherapy, 20‐30 patients primarily receiving medication management; and approximately 100‐110 patients treated with a combination of diagnosis specific psychotherapy and medication.
f. There is a vital exchange between the residents and staff regarding clinic issues, i.e., malpractice, ethics, commitment laws, patient information, fees and payment schedules, insurance and managed care dilemmas. The senior residents are encouraged to be active participants in the practical problems and policy decisions that this university clinic encounters. The faculty has an eclectic approach addressing psychodynamic, cognitive‐behavioral, interpersonal, and family therapy. Opportunities for writing case report, analyzing data, and participating in investigations are encouraged.
17
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: OUTPATIENT ADULT PSYCHIATRY LEVEL: PGY3 DURATON: 12 MONTHS, HALF‐TIME (PGY3) SITE: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KU HOSPITAL By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
7. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
8. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
9. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
10. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
11. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
12. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents
18
DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the outpatient adult psychiatry rotation include but are not limited to those listed below
Outpatient Adult Psychiatry PGY3 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to adult ambulatory patient Objectives Learning
Activities Evaluation Activities
Diagnose and treat a variety of outpatients with a broad range of acute and chronic psychiatric disorders, seen briefly, regularly or frequently for both focused and long‐term management, using a variety of psychopharmacologic, psychotherapeutic, and social rehabilitative treatments
DL, DPC, DSP, GD
GR/FE, SPE, PCL, WE
Practice conceptualizing psychopathology in terms of each patient’s developmental, biological, psychological and social patterns and formulate patient specific treatment plans based on this understanding
DL, DPC, GD
GR/FE, SPE
Show consideration for and respond therapeutically to personality features and coping techniques that affect the course of a patient’s illness
DL, DPC, GSE
GR/FE, SPE
Provide psychiatric consultative services and/or ongoing care for outpatients referred by other physicians and non‐medical therapists
DL, DPC GR/FE
Demonstrate skills in the prescription of psychotropic medications, with specific attention to the needs of ambulatory patients followed by other providers
DL, DPC GR/FE
19
prescribing psychotropic and non‐psychotropic medications
Gain experience and competence in prescribing and monitoring electroconvulsive therapy as an outpatient maintenance treatment for appropriate patients
DL, DPC GR/FE
Perform supportive, psychodynamic, and cognitive‐behavioral psychotherapies as both brief and long‐term treatments
DL, DPC GR/FE, PCL
Gain familiarity and identify patients who might benefit from family, couples, group and other individual evidence‐based psychotherapies
DL, DPC GR/FE, PCL
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Continue to acquire and access new knowledge, interpret the information and apply it in the outpatient clinical setting Objectives Learning
Activities Evaluation Activities
Know in detail the diagnostic criteria and the usual progression of symptoms of all the DSM‐IV‐TR disorders emphasizing those commonly diagnosed and treated in an outpatient setting
DL, DPC, GD
GR/FE, SPE, WE
Expand and demonstrate knowledge of sub‐populations and their psychiatric disorders commonly seen in outpatient psychiatric setting including:
• older adults • those with mental retardation/developmental
disabilities and psychiatric illness • those with Axis II disorders • those with co‐morbid substance abuse • those with complex medical/surgical/psychiatric
co‐morbidities
DL, DPC, GD, RM/FS
GR/FE, WE, SPE
Pay attention to the impact of economic, ethnic, gender, religious/spiritual, sexual orientation and family factors on a patient’s physical and psychological development
DL, DPC GR/FE
Demonstrate knowledge of generally accepted diagnostic, psychological, and cognitive tests, and their clinical applications particularly as they pertain to the outpatient setting
DL, DPC GR/FE, WE, SPE
Know the value and application of clinical rating scales of DL, DPC GR/FE, WE
20
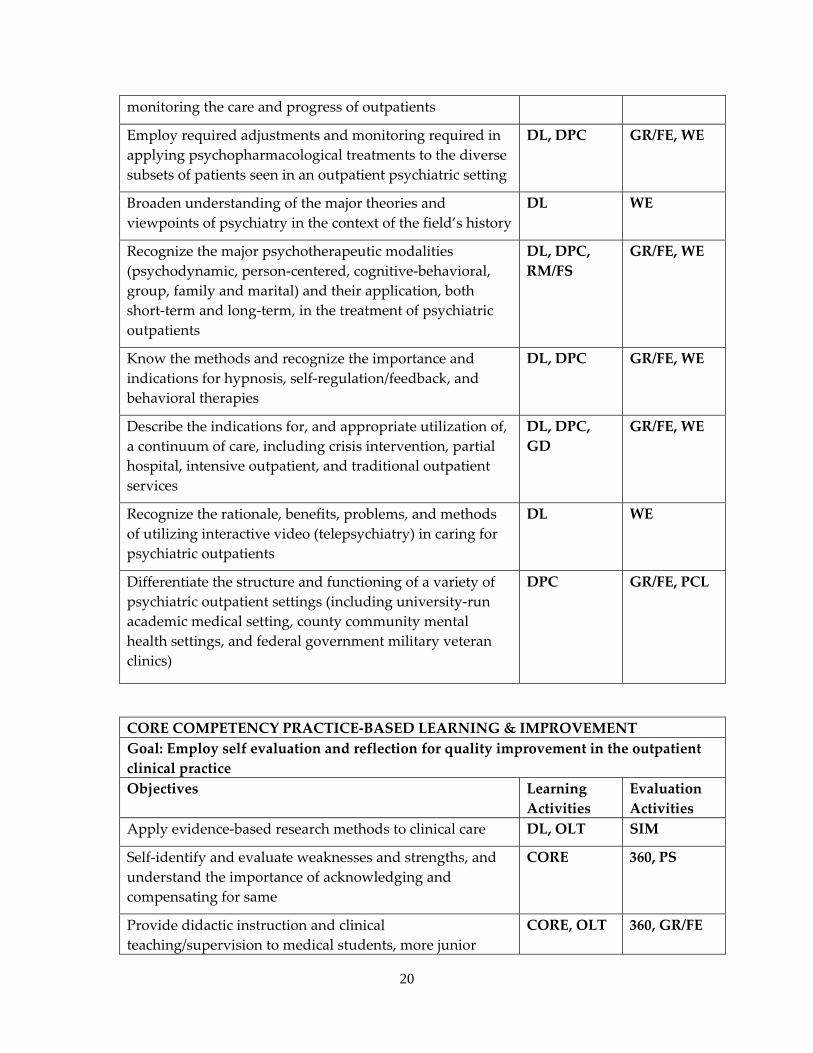
monitoring the care and progress of outpatients
Employ required adjustments and monitoring required in applying psychopharmacological treatments to the diverse subsets of patients seen in an outpatient psychiatric setting
DL, DPC GR/FE, WE
Broaden understanding of the major theories and viewpoints of psychiatry in the context of the field’s history
DL WE
Recognize the major psychotherapeutic modalities (psychodynamic, person‐centered, cognitive‐behavioral, group, family and marital) and their application, both short‐term and long‐term, in the treatment of psychiatric outpatients
DL, DPC, RM/FS
GR/FE, WE
Know the methods and recognize the importance and indications for hypnosis, self‐regulation/feedback, and behavioral therapies
DL, DPC GR/FE, WE
Describe the indications for, and appropriate utilization of, a continuum of care, including crisis intervention, partial hospital, intensive outpatient, and traditional outpatient services
DL, DPC, GD
GR/FE, WE
Recognize the rationale, benefits, problems, and methods of utilizing interactive video (telepsychiatry) in caring for psychiatric outpatients
DL WE
Differentiate the structure and functioning of a variety of psychiatric outpatient settings (including university‐run academic medical setting, county community mental health settings, and federal government military veteran clinics)
DPC GR/FE, PCL
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Employ self evaluation and reflection for quality improvement in the outpatient clinical practice Objectives Learning
Activities Evaluation Activities
Apply evidence‐based research methods to clinical care DL, OLT SIM
Self‐identify and evaluate weaknesses and strengths, and understand the importance of acknowledging and compensating for same
CORE 360, PS
Provide didactic instruction and clinical teaching/supervision to medical students, more junior
CORE, OLT 360, GR/FE
21
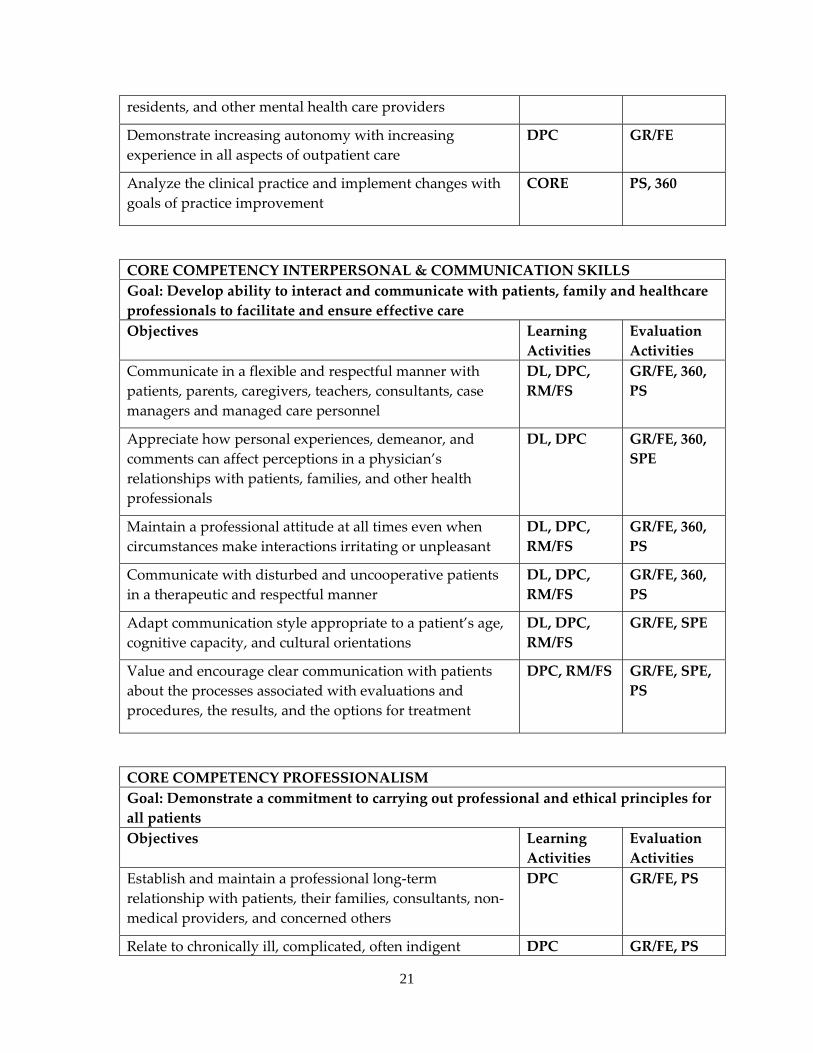
residents, and other mental health care providers
Demonstrate increasing autonomy with increasing experience in all aspects of outpatient care
DPC GR/FE
Analyze the clinical practice and implement changes with goals of practice improvement
CORE PS, 360
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care Objectives Learning
Activities Evaluation Activities
Communicate in a flexible and respectful manner with patients, parents, caregivers, teachers, consultants, case managers and managed care personnel
DL, DPC, RM/FS
GR/FE, 360, PS
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times even when circumstances make interactions irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360, PS
Communicate with disturbed and uncooperative patients in a therapeutic and respectful manner
DL, DPC, RM/FS
GR/FE, 360, PS
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, RM/FS GR/FE, SPE, PS
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for all patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional long‐term relationship with patients, their families, consultants, non‐medical providers, and concerned others
DPC GR/FE, PS
Relate to chronically ill, complicated, often indigent DPC GR/FE, PS
22
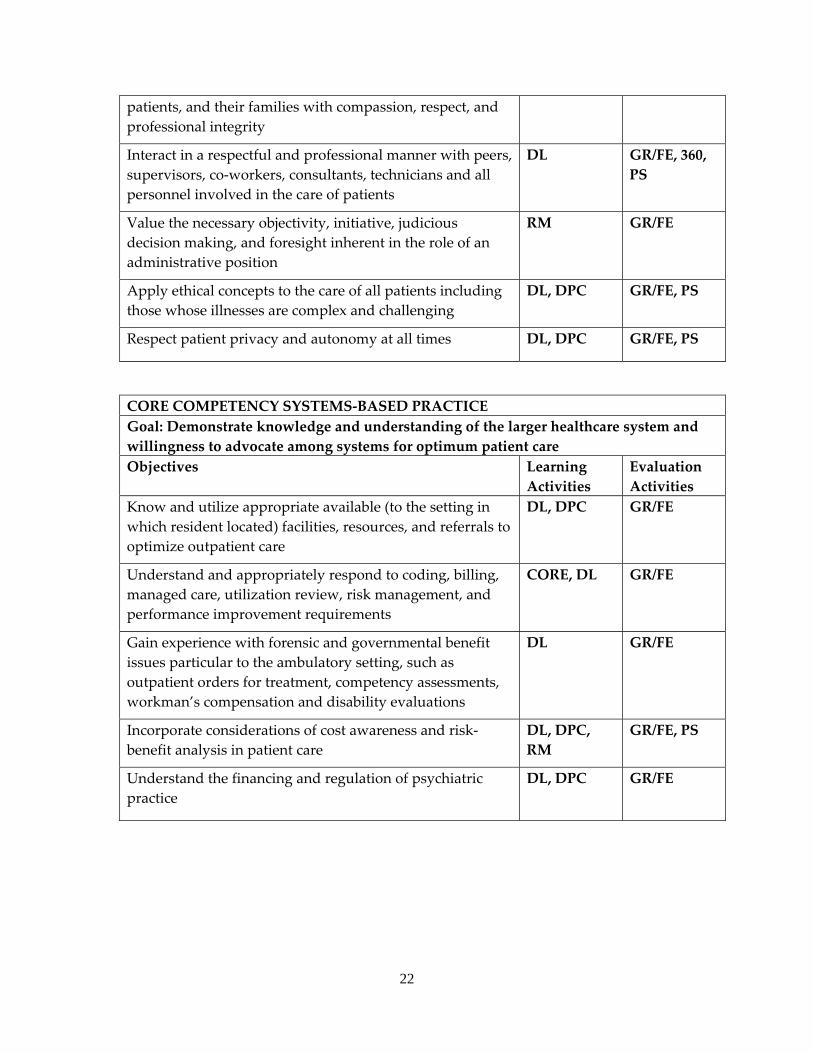
patients, and their families with compassion, respect, and professional integrity
Interact in a respectful and professional manner with peers, supervisors, co‐workers, consultants, technicians and all personnel involved in the care of patients
DL GR/FE, 360, PS
Value the necessary objectivity, initiative, judicious decision making, and foresight inherent in the role of an administrative position
RM GR/FE
Apply ethical concepts to the care of all patients including those whose illnesses are complex and challenging
DL, DPC GR/FE, PS
Respect patient privacy and autonomy at all times DL, DPC GR/FE, PS
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Know and utilize appropriate available (to the setting in which resident located) facilities, resources, and referrals to optimize outpatient care
DL, DPC GR/FE
Understand and appropriately respond to coding, billing, managed care, utilization review, risk management, and performance improvement requirements
CORE, DL GR/FE
Gain experience with forensic and governmental benefit issues particular to the ambulatory setting, such as outpatient orders for treatment, competency assessments, workman’s compensation and disability evaluations
DL GR/FE
Incorporate considerations of cost awareness and risk‐benefit analysis in patient care
DL, DPC, RM
GR/FE, PS
Understand the financing and regulation of psychiatric practice
DL, DPC GR/FE
23
a. PSYCHIATRY CONSULT SERVICE b. Required 2 month rotation occurring in the PGY4 year. PGY2 residents are assigned
to 1‐2 months in conjunction with ECT. c. Faculty consists of two full‐time psychiatrists and two part‐time psychiatrists. In
addition, other psychiatrists on faculty may be consulted in individual cases because of special areas of expertise.
d. All patients for whom psychiatric consultation is requested are seen by the resident and faculty psychiatrist. The resident’s initial workup of each patient is followed by an interview by the faculty psychiatrist with the resident observing. Each case is discussed in detail, including symptomology, differential diagnosis, complications of underlying medical illness, treatment plan and recommendations to the primary care physician/treatment team. The resident’s documentation is reviewed. A broad range of adult surgical and medical cases is seen in the course of each resident’s rotation. Residents are required to attend the weekly didactic series and Psychiatry Grand Rounds.
e. Approximately 1200 patients are seen in consultation every 12 months for an average of 200 patients seen by each resident during their 2 month rotation on the consultation‐liaison service. The population of these patients is about 45% male and 55% female; they are all 17 years of age or older, approximately 70% Caucasian, 20% African American and 10% Hispanic and other ethnic groups. There is a full range of psychiatric and medical‐surgical diagnoses with special instruction and ongoing evaluation of burn patients, cancer patients, bone‐marrow transplant, organ transplant patients, patients with chronic pain and in need of palliative care management, renal dialysis patients, patients who have attempted suicide, long‐term inpatients with orthopedic trauma or surgery, violent and homicidal patients. Patients are also seen who have been transferred from Osawatomie State Hospital and the Kansas State Penitentiary and who need to continue their psychiatric care while their medication issues are addressed. Other frequently occurring consultation requests are for evaluation and treatment of drug and alcohol abuse and dependence, capacity determinations, and patients with puzzling diagnostic medical problems. Attention is given to psychiatric diagnosis, pharmacotherapy, psychosocial interventions, and arrangement of appropriate inpatient or outpatient psychiatric follow‐up.
f. On the average 20‐30 new patients are seen each week by each resident in addition to daily follow‐up on anywhere from 5 to 20 patients who had previously been seen for initial evaluation.
g. Residents are supervised daily in all aspects of each patient’s psychiatric care and treatment recommendations. This includes an opportunity for the faculty to observe the resident interviewing patients, and vice versa. In addition to daily supervision, the residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision.
24
h. One member of the psychiatry consult faculty has a special interest in oncology, pain management, and HIV related illnesses. Three of the psychiatrists are fully‐trained in psychiatry and internal medicine. Dual faculty appointments are held with the Department of Internal Medicine at Kansas University Medical Center.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: PSYCHIATRY CONSULTS‐ECT LEVEL: PGY2 DURATON: 1 MONTH SITE: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KU HOSPITAL By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling
25
CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the rotation include but are not limited to those listed below:
The knowledge, skills, and attitudes to be acquired during the geriatric psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Consult Psychiatry Rotation CORE COMPETENCY PATIENT CARE Goal: Provide and carryout the continuum of patient care for medically ill individuals receiving concurrent psychiatric care including the diagnosis, treatment and management of psychiatric illnessObjectives Learning
Activities Evaluation Activities
Understand and assist in the technical aspects of administration of electroconvulsive therapy (ECT) Specifically, residents will be able to:
• describe selection of appropriate patients for ECT, including psychiatric indications and medical/psychiatric contraindications;
• educate patients and their families about the risks and benefits of and alternatives to ECT;
• obtain informed consent for ECT from patients;
DL, DPC, RM/FS
GR/FE, PCL, WE
26
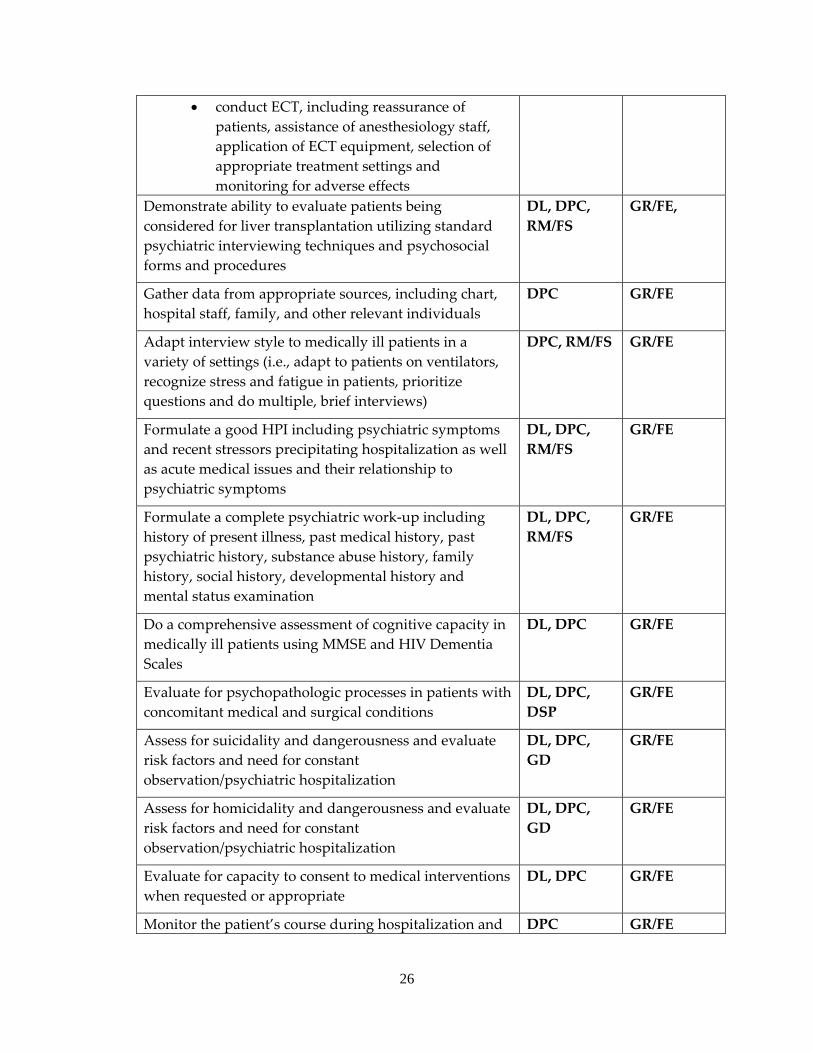
• conduct ECT, including reassurance of patients, assistance of anesthesiology staff, application of ECT equipment, selection of appropriate treatment settings and monitoring for adverse effects
Demonstrate ability to evaluate patients being considered for liver transplantation utilizing standard psychiatric interviewing techniques and psychosocial forms and procedures
DL, DPC, RM/FS
GR/FE,
Gather data from appropriate sources, including chart, hospital staff, family, and other relevant individuals
DPC GR/FE
Adapt interview style to medically ill patients in a variety of settings (i.e., adapt to patients on ventilators, recognize stress and fatigue in patients, prioritize questions and do multiple, brief interviews)
DPC, RM/FS GR/FE
Formulate a good HPI including psychiatric symptoms and recent stressors precipitating hospitalization as well as acute medical issues and their relationship to psychiatric symptoms
DL, DPC, RM/FS
GR/FE
Formulate a complete psychiatric work‐up including history of present illness, past medical history, past psychiatric history, substance abuse history, family history, social history, developmental history and mental status examination
DL, DPC, RM/FS
GR/FE
Do a comprehensive assessment of cognitive capacity in medically ill patients using MMSE and HIV Dementia Scales
DL, DPC GR/FE
Evaluate for psychopathologic processes in patients with concomitant medical and surgical conditions
DL, DPC, DSP
GR/FE
Assess for suicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric hospitalization
DL, DPC, GD
GR/FE
Assess for homicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric hospitalization
DL, DPC, GD
GR/FE
Evaluate for capacity to consent to medical interventions when requested or appropriate
DL, DPC GR/FE
Monitor the patient’s course during hospitalization and DPC GR/FE
27
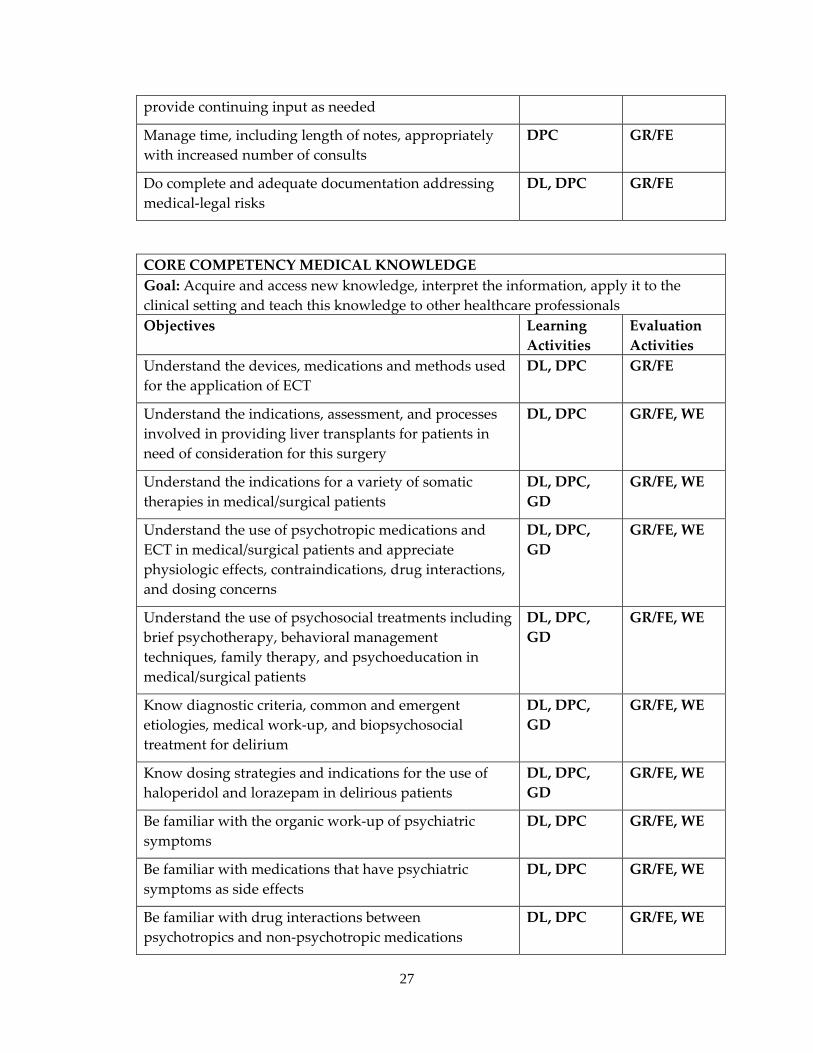
provide continuing input as needed
Manage time, including length of notes, appropriately with increased number of consults
DPC GR/FE
Do complete and adequate documentation addressing medical‐legal risks
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionals Objectives Learning
Activities Evaluation Activities
Understand the devices, medications and methods used for the application of ECT
DL, DPC GR/FE
Understand the indications, assessment, and processes involved in providing liver transplants for patients in need of consideration for this surgery
DL, DPC GR/FE, WE
Understand the indications for a variety of somatic therapies in medical/surgical patients
DL, DPC, GD
GR/FE, WE
Understand the use of psychotropic medications and ECT in medical/surgical patients and appreciate physiologic effects, contraindications, drug interactions, and dosing concerns
DL, DPC, GD
GR/FE, WE
Understand the use of psychosocial treatments including brief psychotherapy, behavioral management techniques, family therapy, and psychoeducation in medical/surgical patients
DL, DPC, GD
GR/FE, WE
Know diagnostic criteria, common and emergent etiologies, medical work‐up, and biopsychosocial treatment for delirium
DL, DPC, GD
GR/FE, WE
Know dosing strategies and indications for the use of haloperidol and lorazepam in delirious patients
DL, DPC, GD
GR/FE, WE
Be familiar with the organic work‐up of psychiatric symptoms
DL, DPC GR/FE, WE
Be familiar with medications that have psychiatric symptoms as side effects
DL, DPC GR/FE, WE
Be familiar with drug interactions between psychotropics and non‐psychotropic medications
DL, DPC GR/FE, WE
28
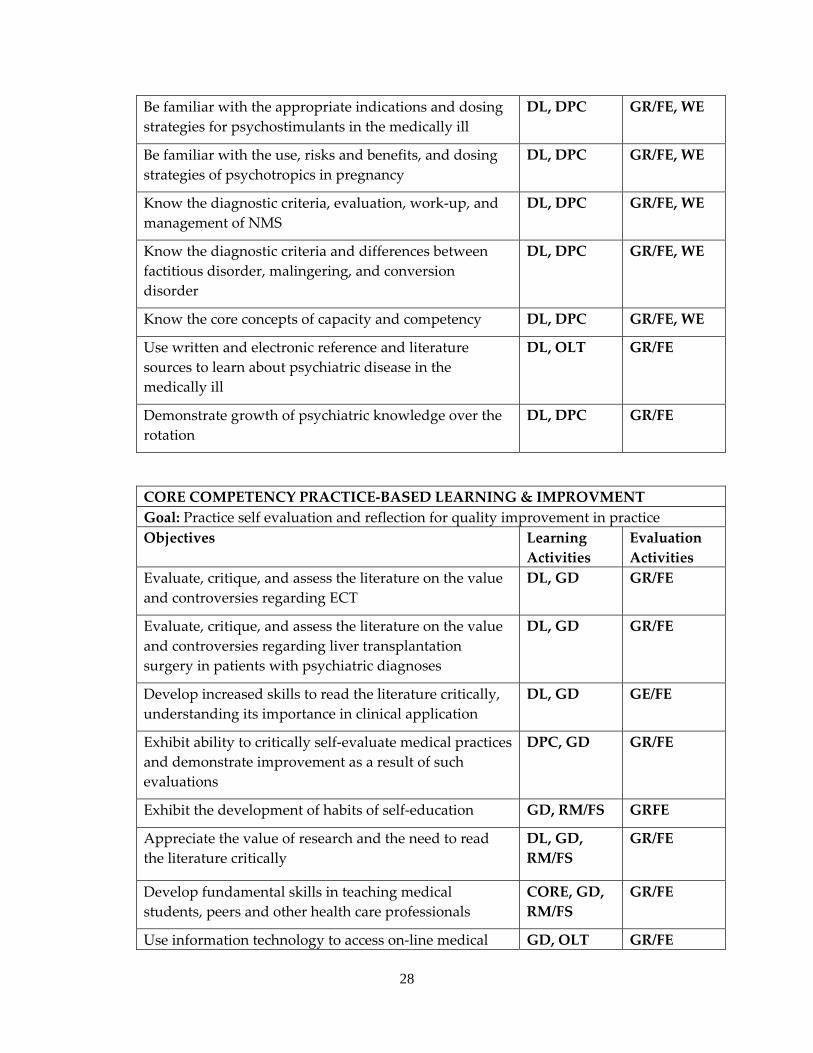
Be familiar with the appropriate indications and dosing strategies for psychostimulants in the medically ill
DL, DPC GR/FE, WE
Be familiar with the use, risks and benefits, and dosing strategies of psychotropics in pregnancy
DL, DPC GR/FE, WE
Know the diagnostic criteria, evaluation, work‐up, and management of NMS
DL, DPC GR/FE, WE
Know the diagnostic criteria and differences between factitious disorder, malingering, and conversion disorder
DL, DPC GR/FE, WE
Know the core concepts of capacity and competency DL, DPC GR/FE, WE
Use written and electronic reference and literature sources to learn about psychiatric disease in the medically ill
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Evaluate, critique, and assess the literature on the value and controversies regarding ECT
DL, GD GR/FE
Evaluate, critique, and assess the literature on the value and controversies regarding liver transplantation surgery in patients with psychiatric diagnoses
DL, GD GR/FE
Develop increased skills to read the literature critically, understanding its importance in clinical application
DL, GD GE/FE
Exhibit ability to critically self‐evaluate medical practices and demonstrate improvement as a result of such evaluations
DPC, GD GR/FE
Exhibit the development of habits of self‐education GD, RM/FS GRFE
Appreciate the value of research and the need to read the literature critically
DL, GD, RM/FS
GR/FE
Develop fundamental skills in teaching medical students, peers and other health care professionals
CORE, GD, RM/FS
GR/FE
Use information technology to access on‐line medical GD, OLT GR/FE
29
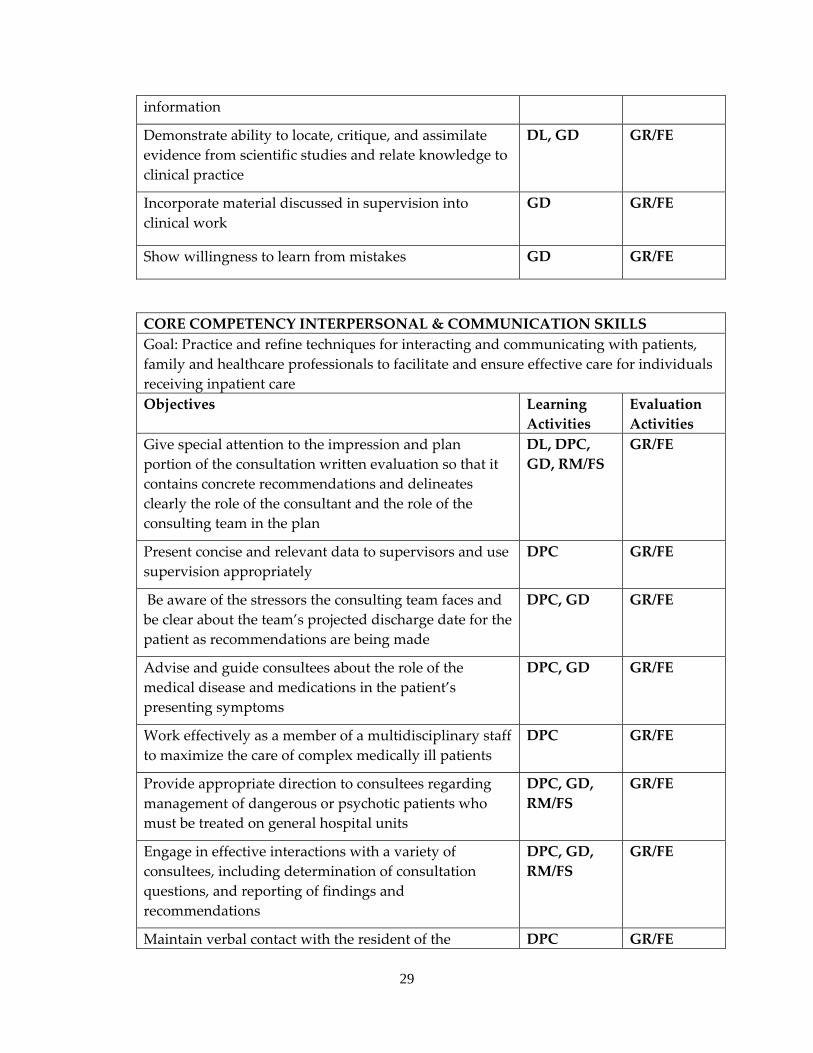
information
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, GD GR/FE
Incorporate material discussed in supervision into clinical work
GD GR/FE
Show willingness to learn from mistakes GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Give special attention to the impression and plan portion of the consultation written evaluation so that it contains concrete recommendations and delineates clearly the role of the consultant and the role of the consulting team in the plan
DL, DPC, GD, RM/FS
GR/FE
Present concise and relevant data to supervisors and use supervision appropriately
DPC GR/FE
Be aware of the stressors the consulting team faces and be clear about the team’s projected discharge date for the patient as recommendations are being made
DPC, GD GR/FE
Advise and guide consultees about the role of the medical disease and medications in the patient’s presenting symptoms
DPC, GD GR/FE
Work effectively as a member of a multidisciplinary staff to maximize the care of complex medically ill patients
DPC GR/FE
Provide appropriate direction to consultees regarding management of dangerous or psychotic patients who must be treated on general hospital units
DPC, GD, RM/FS
GR/FE
Engage in effective interactions with a variety of consultees, including determination of consultation questions, and reporting of findings and recommendations
DPC, GD, RM/FS
GR/FE
Maintain verbal contact with the resident of the DPC GR/FE
30
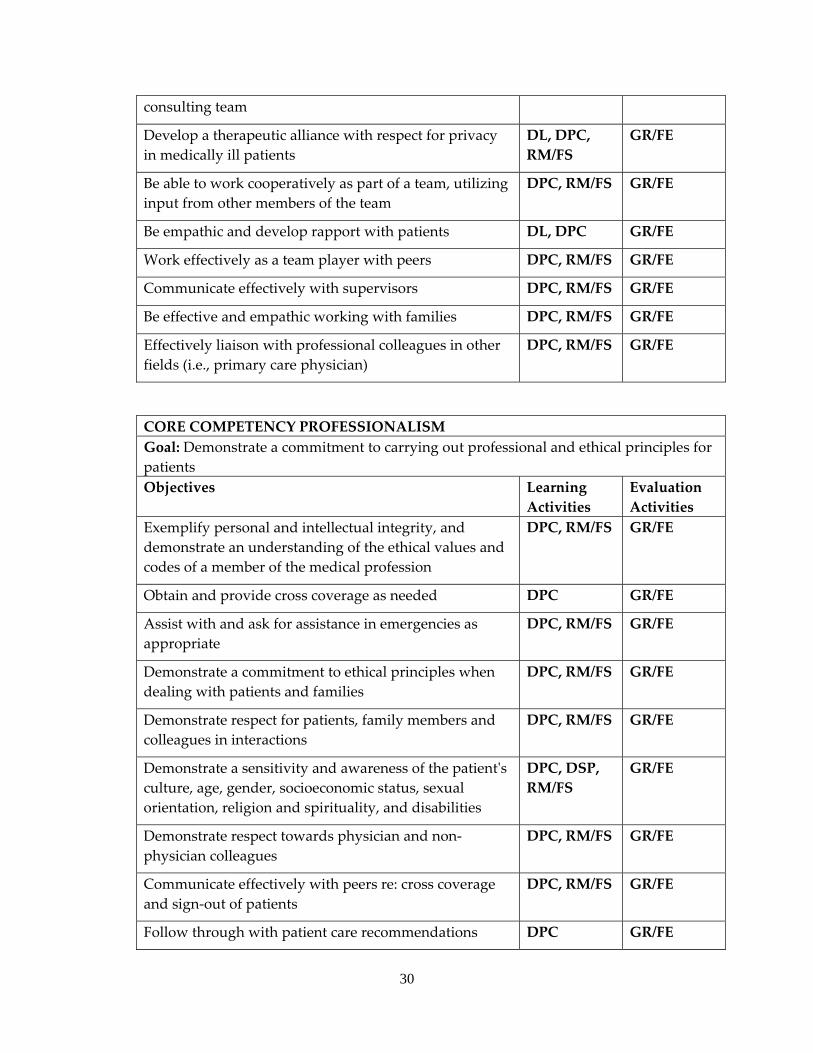
consulting team
Develop a therapeutic alliance with respect for privacy in medically ill patients
DL, DPC, RM/FS
GR/FE
Be able to work cooperatively as part of a team, utilizing input from other members of the team
DPC, RM/FS GR/FE
Be empathic and develop rapport with patients DL, DPC GR/FE
Work effectively as a team player with peers DPC, RM/FS GR/FE
Communicate effectively with supervisors DPC, RM/FS GR/FE
Be effective and empathic working with families DPC, RM/FS GR/FE
Effectively liaison with professional colleagues in other fields (i.e., primary care physician)
DPC, RM/FS GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Obtain and provide cross coverage as needed DPC GR/FE
Assist with and ask for assistance in emergencies as appropriate
DPC, RM/FS GR/FE
Demonstrate a commitment to ethical principles when dealing with patients and families
DPC, RM/FS GR/FE
Demonstrate respect for patients, family members and colleagues in interactions
DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE
Demonstrate respect towards physician and non‐physician colleagues
DPC, RM/FS GR/FE
Communicate effectively with peers re: cross coverage and sign‐out of patients
DPC, RM/FS GR/FE
Follow through with patient care recommendations DPC GR/FE
31
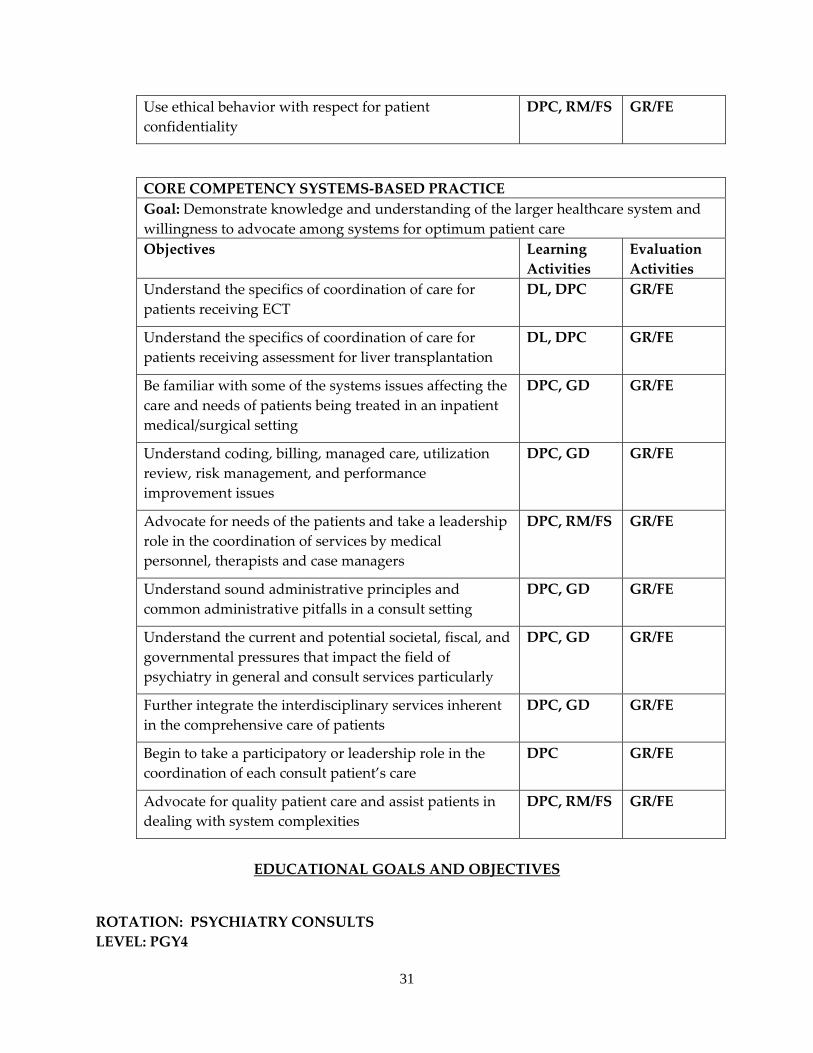
Use ethical behavior with respect for patient confidentiality
DPC, RM/FS GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Understand the specifics of coordination of care for patients receiving ECT
DL, DPC GR/FE
Understand the specifics of coordination of care for patients receiving assessment for liver transplantation
DL, DPC GR/FE
Be familiar with some of the systems issues affecting the care and needs of patients being treated in an inpatient medical/surgical setting
DPC, GD GR/FE
Understand coding, billing, managed care, utilization review, risk management, and performance improvement issues
DPC, GD GR/FE
Advocate for needs of the patients and take a leadership role in the coordination of services by medical personnel, therapists and case managers
DPC, RM/FS GR/FE
Understand sound administrative principles and common administrative pitfalls in a consult setting
DPC, GD GR/FE
Understand the current and potential societal, fiscal, and governmental pressures that impact the field of psychiatry in general and consult services particularly
DPC, GD GR/FE
Further integrate the interdisciplinary services inherent in the comprehensive care of patients
DPC, GD GR/FE
Begin to take a participatory or leadership role in the coordination of each consult patient’s care
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: PSYCHIATRY CONSULTS LEVEL: PGY4
32
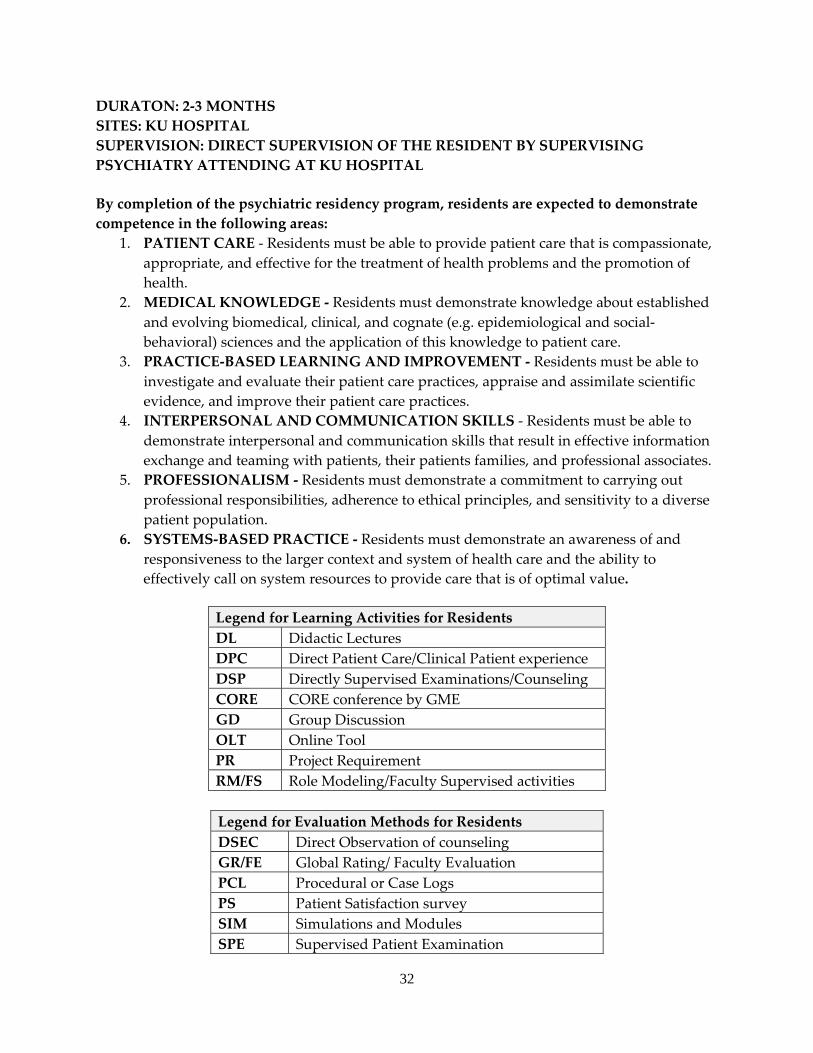
DURATON: 2‐3 MONTHS SITES: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KU HOSPITAL
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination
33
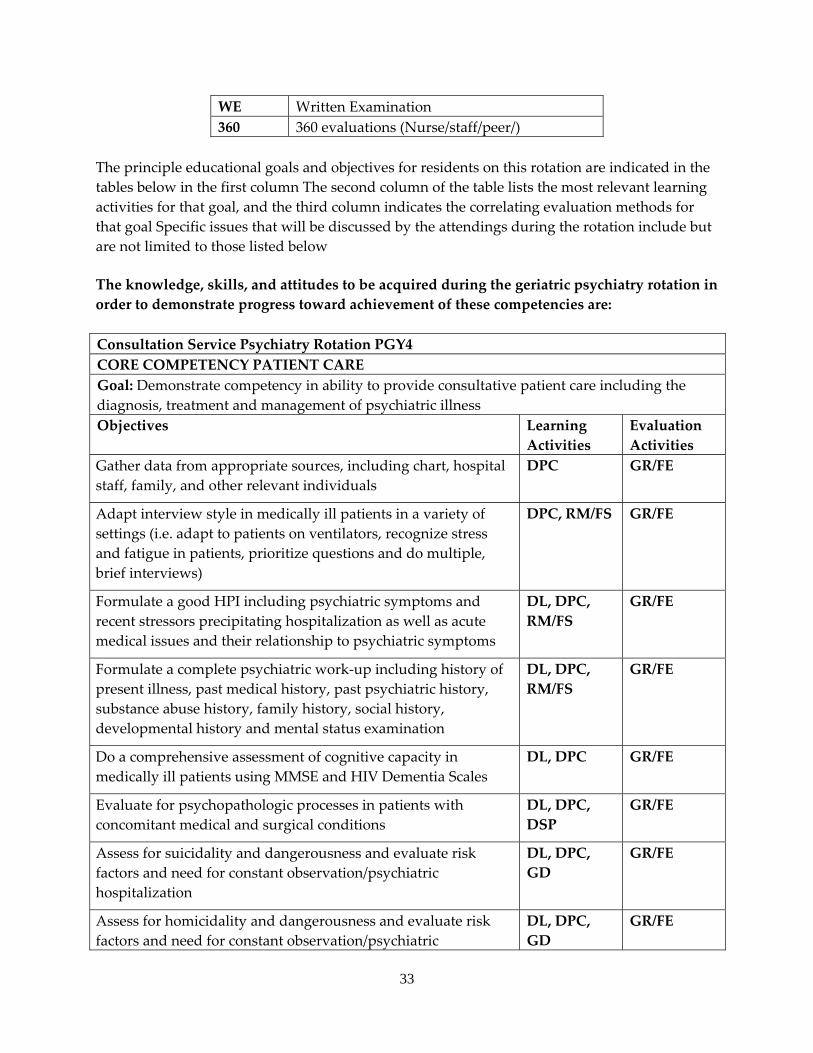
WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the rotation include but are not limited to those listed below
The knowledge, skills, and attitudes to be acquired during the geriatric psychiatry rotation in order to demonstrate progress toward achievement of these competencies are: Consultation Service Psychiatry Rotation PGY4 CORE COMPETENCY PATIENT CARE Goal: Demonstrate competency in ability to provide consultative patient care including the diagnosis, treatment and management of psychiatric illnessObjectives Learning
Activities Evaluation Activities
Gather data from appropriate sources, including chart, hospital staff, family, and other relevant individuals
DPC GR/FE
Adapt interview style in medically ill patients in a variety of settings (i.e. adapt to patients on ventilators, recognize stress and fatigue in patients, prioritize questions and do multiple, brief interviews)
DPC, RM/FS GR/FE
Formulate a good HPI including psychiatric symptoms and recent stressors precipitating hospitalization as well as acute medical issues and their relationship to psychiatric symptoms
DL, DPC, RM/FS
GR/FE
Formulate a complete psychiatric work‐up including history of present illness, past medical history, past psychiatric history, substance abuse history, family history, social history, developmental history and mental status examination
DL, DPC, RM/FS
GR/FE
Do a comprehensive assessment of cognitive capacity in medically ill patients using MMSE and HIV Dementia Scales
DL, DPC GR/FE
Evaluate for psychopathologic processes in patients with concomitant medical and surgical conditions
DL, DPC, DSP
GR/FE
Assess for suicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric hospitalization
DL, DPC, GD
GR/FE
Assess for homicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric
DL, DPC, GD
GR/FE
34
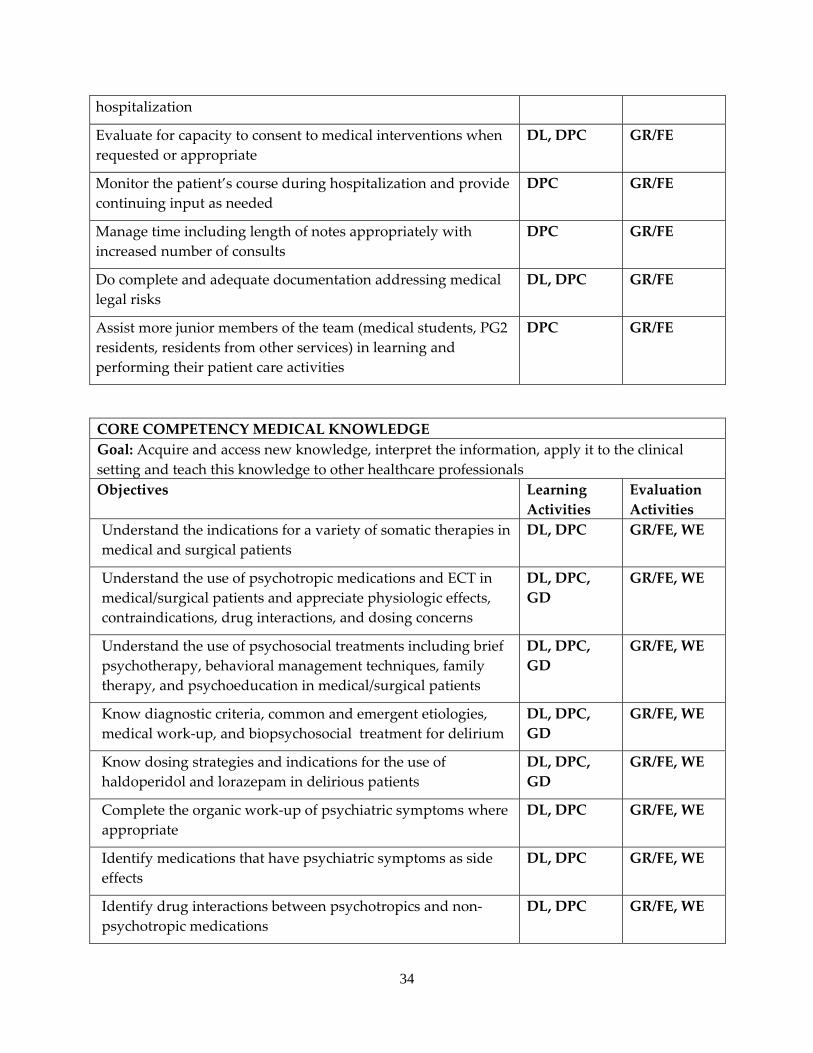
hospitalization
Evaluate for capacity to consent to medical interventions when requested or appropriate
DL, DPC GR/FE
Monitor the patient’s course during hospitalization and provide continuing input as needed
DPC GR/FE
Manage time including length of notes appropriately with increased number of consults
DPC GR/FE
Do complete and adequate documentation addressing medical legal risks
DL, DPC GR/FE
Assist more junior members of the team (medical students, PG2 residents, residents from other services) in learning and performing their patient care activities
DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionalsObjectives Learning
Activities Evaluation Activities
Understand the indications for a variety of somatic therapies in medical and surgical patients
DL, DPC GR/FE, WE
Understand the use of psychotropic medications and ECT in medical/surgical patients and appreciate physiologic effects, contraindications, drug interactions, and dosing concerns
DL, DPC, GD
GR/FE, WE
Understand the use of psychosocial treatments including brief psychotherapy, behavioral management techniques, family therapy, and psychoeducation in medical/surgical patients
DL, DPC, GD
GR/FE, WE
Know diagnostic criteria, common and emergent etiologies, medical work‐up, and biopsychosocial treatment for delirium
DL, DPC, GD
GR/FE, WE
Know dosing strategies and indications for the use of haldoperidol and lorazepam in delirious patients
DL, DPC, GD
GR/FE, WE
Complete the organic work‐up of psychiatric symptoms where appropriate
DL, DPC GR/FE, WE
Identify medications that have psychiatric symptoms as side effects
DL, DPC GR/FE, WE
Identify drug interactions between psychotropics and non‐psychotropic medications
DL, DPC GR/FE, WE
35
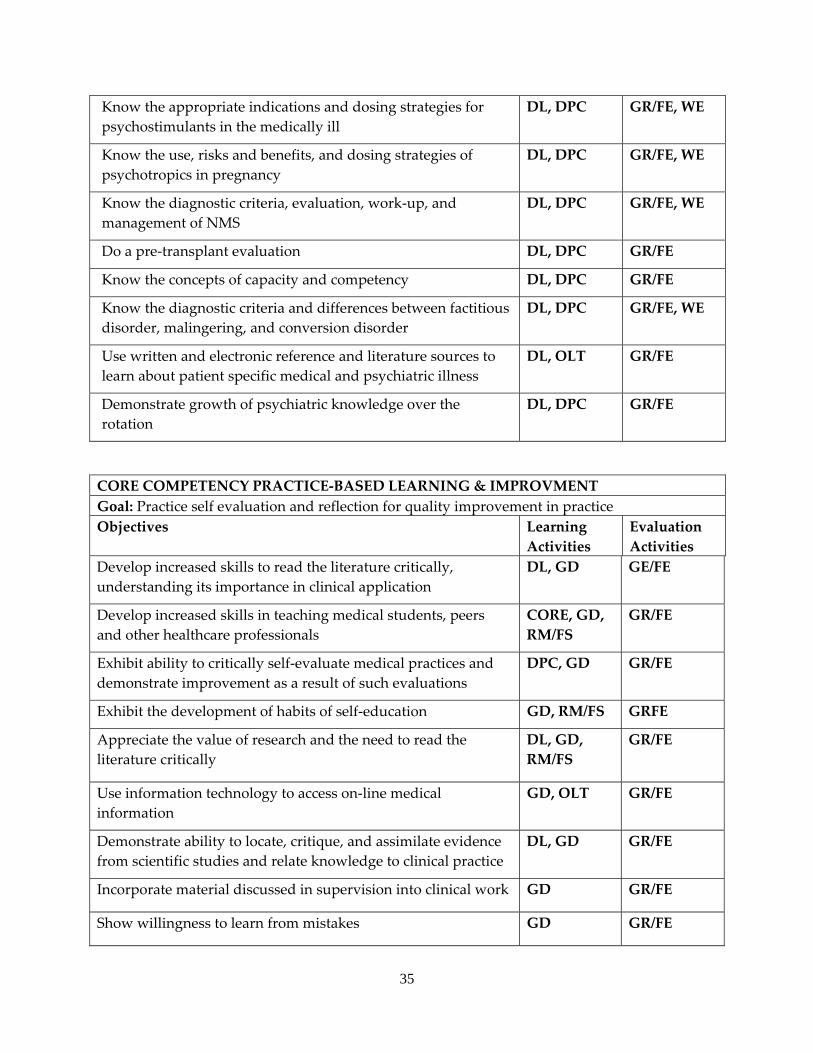
Know the appropriate indications and dosing strategies for psychostimulants in the medically ill
DL, DPC GR/FE, WE
Know the use, risks and benefits, and dosing strategies of psychotropics in pregnancy
DL, DPC GR/FE, WE
Know the diagnostic criteria, evaluation, work‐up, and management of NMS
DL, DPC GR/FE, WE
Do a pre‐transplant evaluation DL, DPC GR/FE
Know the concepts of capacity and competency DL, DPC GR/FE
Know the diagnostic criteria and differences between factitious disorder, malingering, and conversion disorder
DL, DPC GR/FE, WE
Use written and electronic reference and literature sources to learn about patient specific medical and psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Develop increased skills to read the literature critically, understanding its importance in clinical application
DL, GD GE/FE
Develop increased skills in teaching medical students, peers and other healthcare professionals
CORE, GD, RM/FS
GR/FE
Exhibit ability to critically self‐evaluate medical practices and demonstrate improvement as a result of such evaluations
DPC, GD GR/FE
Exhibit the development of habits of self‐education GD, RM/FS GRFE
Appreciate the value of research and the need to read the literature critically
DL, GD, RM/FS
GR/FE
Use information technology to access on‐line medical information
GD, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, GD GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
36
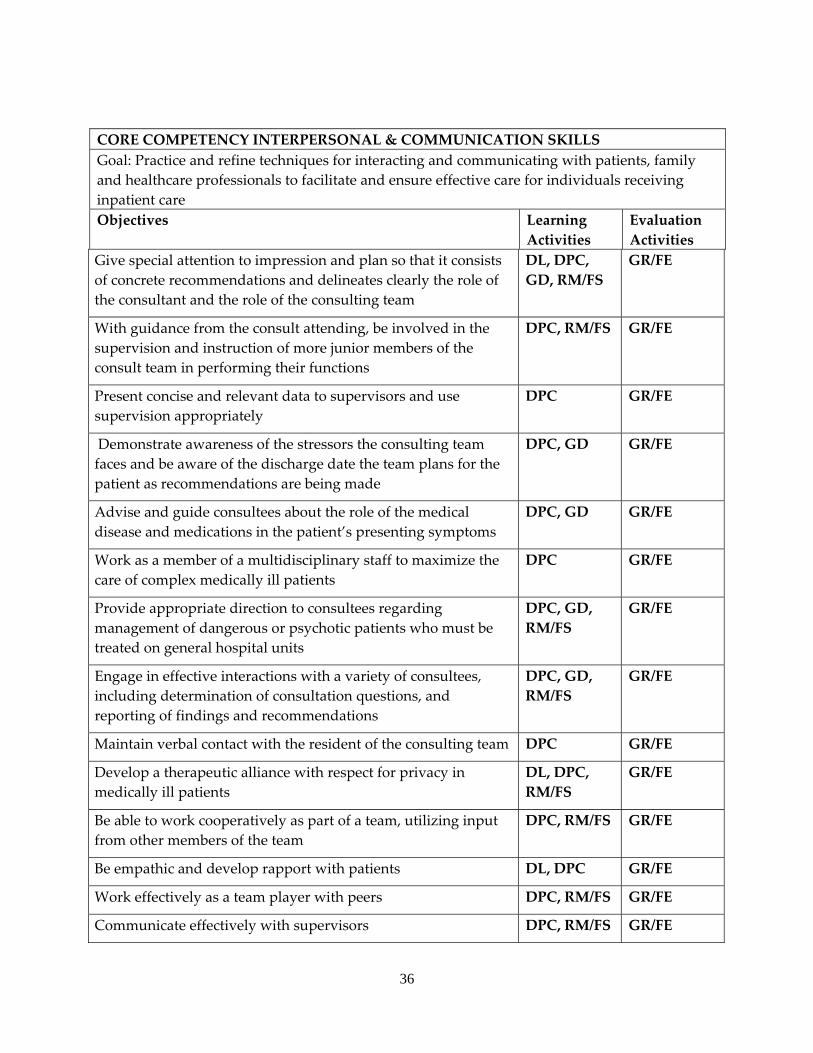
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Give special attention to impression and plan so that it consists of concrete recommendations and delineates clearly the role of the consultant and the role of the consulting team
DL, DPC, GD, RM/FS
GR/FE
With guidance from the consult attending, be involved in the supervision and instruction of more junior members of the consult team in performing their functions
DPC, RM/FS GR/FE
Present concise and relevant data to supervisors and use supervision appropriately
DPC GR/FE
Demonstrate awareness of the stressors the consulting team faces and be aware of the discharge date the team plans for the patient as recommendations are being made
DPC, GD GR/FE
Advise and guide consultees about the role of the medical disease and medications in the patient’s presenting symptoms
DPC, GD GR/FE
Work as a member of a multidisciplinary staff to maximize the care of complex medically ill patients
DPC GR/FE
Provide appropriate direction to consultees regarding management of dangerous or psychotic patients who must be treated on general hospital units
DPC, GD, RM/FS
GR/FE
Engage in effective interactions with a variety of consultees, including determination of consultation questions, and reporting of findings and recommendations
DPC, GD, RM/FS
GR/FE
Maintain verbal contact with the resident of the consulting team DPC GR/FE
Develop a therapeutic alliance with respect for privacy in medically ill patients
DL, DPC, RM/FS
GR/FE
Be able to work cooperatively as part of a team, utilizing input from other members of the team
DPC, RM/FS GR/FE
Be empathic and develop rapport with patients DL, DPC GR/FE
Work effectively as a team player with peers DPC, RM/FS GR/FE
Communicate effectively with supervisors DPC, RM/FS GR/FE
37
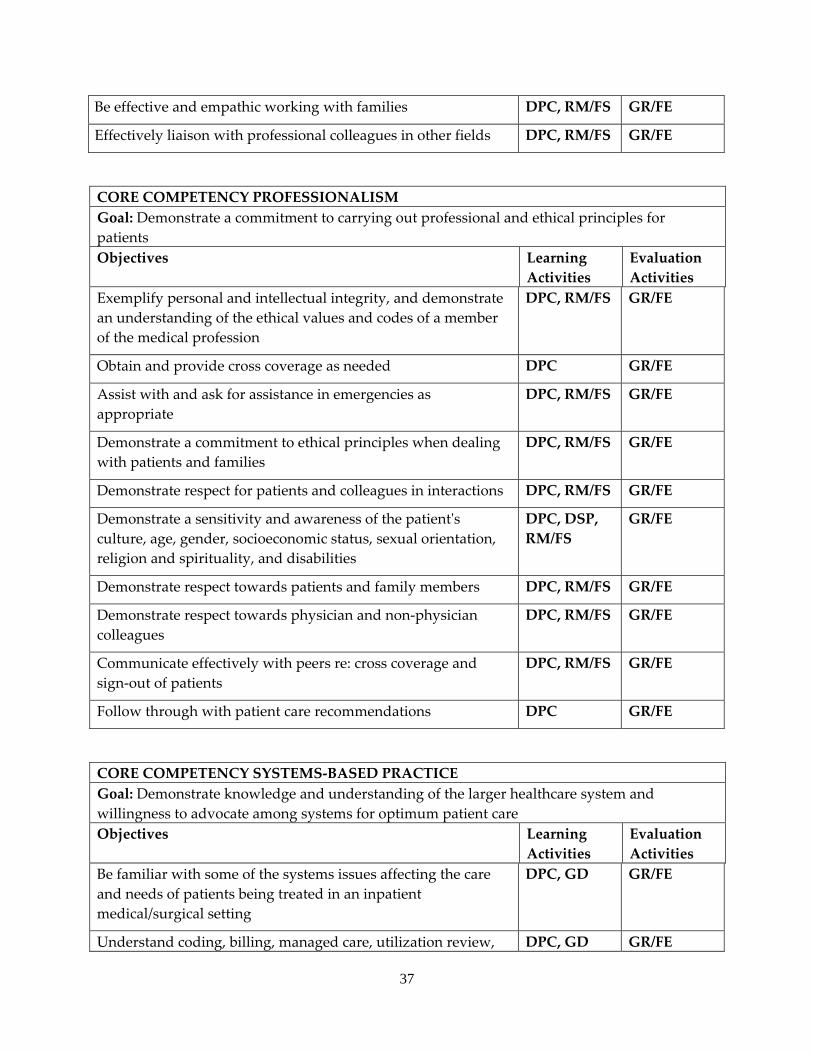
Be effective and empathic working with families DPC, RM/FS GR/FE
Effectively liaison with professional colleagues in other fields DPC, RM/FS GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Obtain and provide cross coverage as needed DPC GR/FE
Assist with and ask for assistance in emergencies as appropriate
DPC, RM/FS GR/FE
Demonstrate a commitment to ethical principles when dealing with patients and families
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE
Demonstrate respect towards patients and family members DPC, RM/FS GR/FE
Demonstrate respect towards physician and non‐physician colleagues
DPC, RM/FS GR/FE
Communicate effectively with peers re: cross coverage and sign‐out of patients
DPC, RM/FS GR/FE
Follow through with patient care recommendations DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Be familiar with some of the systems issues affecting the care and needs of patients being treated in an inpatient medical/surgical setting
DPC, GD GR/FE
Understand coding, billing, managed care, utilization review, DPC, GD GR/FE
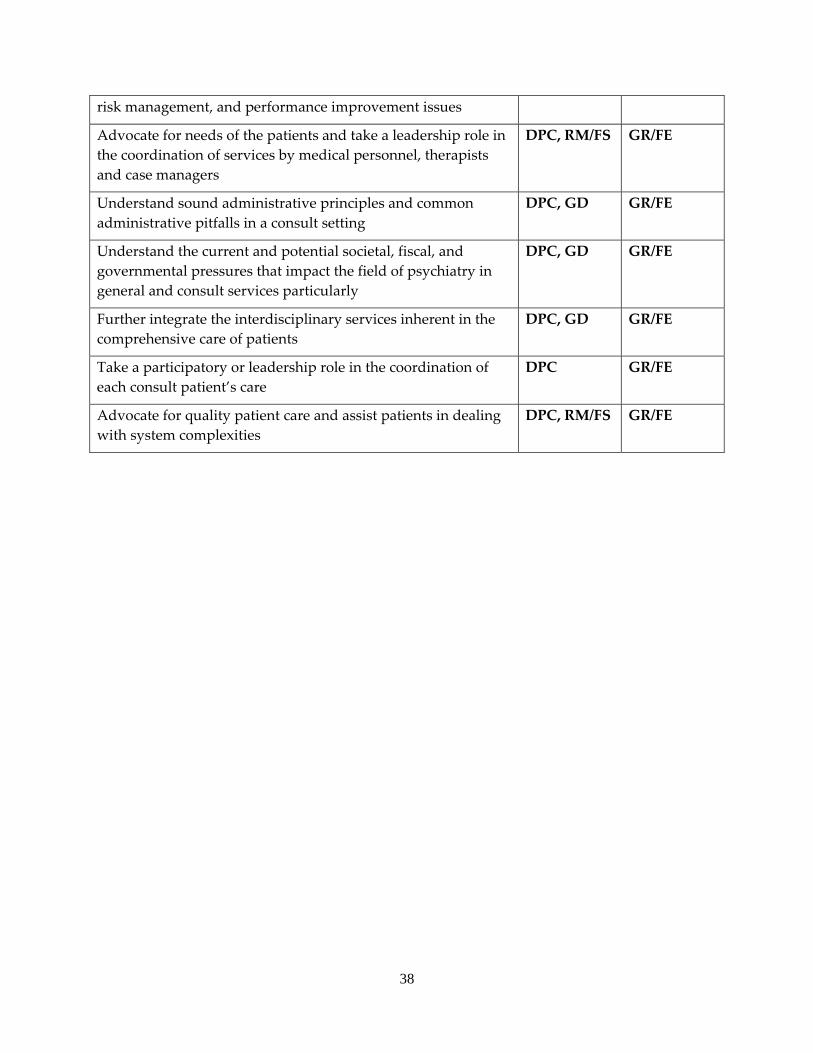
38
risk management, and performance improvement issues
Advocate for needs of the patients and take a leadership role in the coordination of services by medical personnel, therapists and case managers
DPC, RM/FS GR/FE
Understand sound administrative principles and common administrative pitfalls in a consult setting
DPC, GD GR/FE
Understand the current and potential societal, fiscal, and governmental pressures that impact the field of psychiatry in general and consult services particularly
DPC, GD GR/FE
Further integrate the interdisciplinary services inherent in the comprehensive care of patients
DPC, GD GR/FE
Take a participatory or leadership role in the coordination of each consult patient’s care
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
39
a. PSYCHIATRIC EMERGENCY LIAISON SERVICE (PLS) b. Required 1‐2 month rotation occurring in the PGY4 year. c. Psychiatric Emergency Services are provided 24‐hours a day, 7 days per week by a
psychiatric nurse and a qualified mental health professional. Monday to Friday resident coverage is as follows: 8:00 a.m.‐12:00 p.m. by the resident assigned to the Psychiatry Consult Service; 12:00 p.m.‐10:00 p.m. by the resident assigned to the Psychiatric Emergency Liaison Service and 10:00 p.m.‐8:00 a.m. by the first call psychiatry resident. Saturday and Sunday resident coverage is provided by the first call psychiatry resident. Coverage at other times (assigned resident sick, on vacation) is provided by the consult resident (for emergency calls). An algorithm exists for emergency coverage when the consult resident is unavailable. Senior residents (PGY3 and PGY4 year) provide pager/phone‐available back‐up ʺsecond callʺ after hours and on weekends. PLS faculty consists of one full‐time psychiatrist. Additionally, the emergency medicine attending staffing the Emergency Department gives added supervision 24‐hours a day. An attending psychiatrist is assigned as backup at all times for phone consultation. Residents are mandated to call their back‐up on all patients seen during their first year of residency on all patients seen and to check out on‐call cases, and thereafter if they have any questions. The Emergency Department staff physician is available at all times to check out cases seen by the psychiatry residents in the Psychiatric Emergency Liaison Service.
d. Residents are required to attend the weekly didactic series and Psychiatry Grand Rounds, which include topics related to emergency psychiatry. Once a week, the Psychiatric Emergency Liaison Service staff, resident and faculty meet for an hour to receive in‐service training or discuss clinical or administrative issues, details regarding auxiliary services, and to aid communication with and education about community resources and legal/personnel issues. While assigned to the Psychiatry Emergency Liaison Service rotation, residents are exposed to a broad and varied clinical population, gaining skills that are both specific to the emergency room and emergency psychiatric setting and valuable for psychiatry in general.
e. Approximately three‐fourths of the patient population falls between the ages of 15 and 45 with ages ranging from 4 years to 97 years. The female/male ratio is approximately 1:0.84. Approximately 50% of the population is Caucasian, 30% is African‐American with the remainder comprising other ethnic backgrounds such as Hispanic, Native American, and Asian. Approximately 40% of the patient population presents with substance abuse diagnoses, 30% present with Psychosis NOS; 20% present with bipolar disorder or major depression, and 10% present with schizophrenia. The police bring approximately 20% of the patients evaluated in the Psychiatric Emergency Liaison Service. The Psychiatric Emergency Liaison Service rotation teaches effective management of psychiatric emergencies. Skills that are gained include the ability to do focused interviewing under pressure, proficiency in diagnosis of common psychiatric and medical problems, the value and application of crisis intervention techniques including the evaluation and management of
40
suicidal or homicidal patients, the fundamentals of legal aspects of psychiatric practice as they apply to the emergency setting, the insight to recognize and flexibility to change decisions, and the ability to work under pressure and receive cooperation from emergency department staff, other clinicians and community agency personnel.
f. On the average, 190‐220 patients are seen for psychiatric emergency services per month, 6‐8 patients per day.
g. In addition to daily supervision, the residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision during the PGY3 and PGY4 years.
h. The resident assigned to the Psychiatric Emergency Liaison Service is very involved with public sector and community mental health services, as well as working closely with police and other emergency room supervisory staff providing a well‐rounded experience for the assigned resident. Optional elective experiences are available to psychiatry residents.
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: PSYCHIATRY LIAISON SERVICE (PLS) LEVEL: PGY4 DURATON: 1‐3 MONTHS SITE: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING ED ATTENDING AT KU HOSPITAL
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
41
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the emergency psychiatry rotation include but are not limited to those listed below.
The knowledge, skills, and attitudes to be acquired during the geriatric psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Emergency Psychiatry Rotation PGY4 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout the continuum of patient care for individuals receiving emergency psychiatric care including the diagnosis, treatment and management of acute psychiatric illness Objectives Learning
Activities Evaluation Activities
42
Assess and begin to manage crisis situations with appropriate supervision as needed
DL, DPC GR/FE
Efficiently and appropriately acquire clinical information in a variety of ways including:
• Gathering information on referrals by phone • Reviewing medical and psychiatric records • Interviewing the patient and acquiring a
complete mental status exam • Interviewing collateral sources including
family, friends, police, etc • Calling collateral sources of information such
as family, caregivers, current or previous providers, or recent pertinent contacts
DL, DPC, DSP
GR/FE
Effectively manage the violent or agitated patient in PLS through the judicious use of verbal de‐escalation, psychotropic medications, and physical restraints
DL, DPC GR/FE
Identify, assess, and manage patients with suicidal, homicidal and/or assaultive ideation or behavior
DL, DPC GR/FE
Identify, assess, and manage patients with psychosis in the ER setting
DL, DPC GR/FE
Integrate biopsychosocial constructs into formulation of cases
DL, DPC GR/FE
Demonstrate knowledge and ability to provide psychoeducation, community referrals, supportive crisis counseling in addition to pharmacotherapy
DL, DPC, DSP
GR/FE
Appropriately and succinctly document decisions with written justification for professional judgments
DPC GR/FE
Assess patients medically through history and physical exam and recognize and manage uncomplicated medical needs
DL, DPC GR/FE
Utilize appropriate medical and psychiatric screening tools including appropriate laboratory measures
DL, DPC GR/FE
Evaluate the cognitive capacity of medically ill patients and comment on the patient’s ability to make decisions
DL, DPC, DSP
GR/FE
Develop initial treatment plans including safety and DPC GR/FE
43
biopsychosocial aspects
Demonstrate proficiency in recognizing and managing patients requiring detoxification from drugs
DL, DPC GR/FE
Recognize complicating medical factors in the patient with substance dependence
DL, DPC GR/FE
Demonstrate understanding of informed consent by documentation of risk/benefit discussion of treatment options with patients and patients choice regarding treatment options
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionalsObjectives Learning
Activities Evaluation Activities
Formulate a comprehensive differential diagnosis including medical causes for psychiatric presentations
DL, DPC, GD
GR/FE
Know the indications and pharmacological properties of psychotropic medications used in emergency settings
DL, DPC, DSP
GR/FE, WE
Know the presentation and treatments of pharmacological emergencies including, anticholinergic toxicity, neuroleptic malignant syndrome (NMS), serotonin syndrome, and extrapyramidal side effect (EPS) reactions
DL, DPC, DSP
GR/FE, WE
Know the major interaction effects among psychotropic and non‐psychotropic medications and how to avoid/manage them
DL, DPC GR/FE, WE
Know the appropriate methods of detoxification from licit and illicit psychotropic medications
DL, DPC GR/FE, WE
Use written and electronic references and literature sources to further understanding of psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation
DL, DPC GR/FE, WE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice
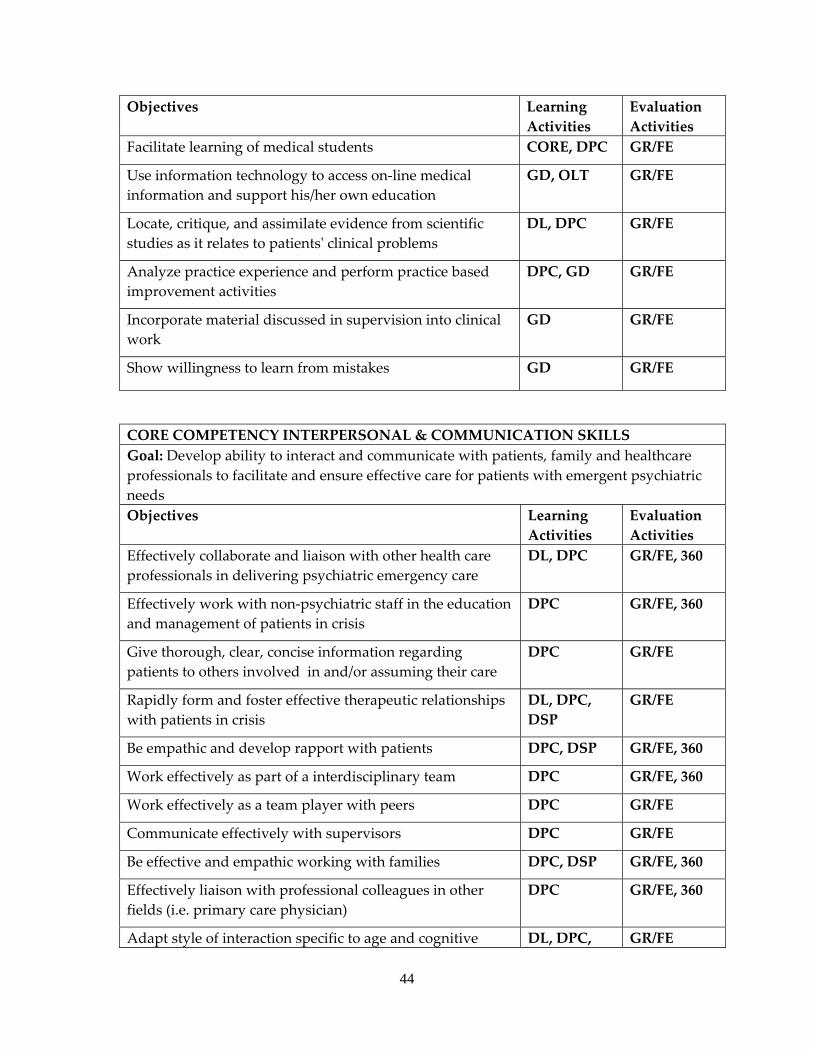
44
Objectives Learning Activities
Evaluation Activities
Facilitate learning of medical students CORE, DPC GR/FE
Use information technology to access on‐line medical information and support his/her own education
GD, OLT GR/FE
Locate, critique, and assimilate evidence from scientific studies as it relates to patientsʹ clinical problems
DL, DPC GR/FE
Analyze practice experience and perform practice based improvement activities
DPC, GD GR/FE
Incorporate material discussed in supervision into clinical work
GD GR/FE
Show willingness to learn from mistakes GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for patients with emergent psychiatric needs Objectives Learning
Activities Evaluation Activities
Effectively collaborate and liaison with other health care professionals in delivering psychiatric emergency care
DL, DPC GR/FE, 360
Effectively work with non‐psychiatric staff in the education and management of patients in crisis
DPC GR/FE, 360
Give thorough, clear, concise information regarding patients to others involved in and/or assuming their care
DPC GR/FE
Rapidly form and foster effective therapeutic relationships with patients in crisis
DL, DPC, DSP
GR/FE
Be empathic and develop rapport with patients DPC, DSP GR/FE, 360
Work effectively as part of a interdisciplinary team DPC GR/FE, 360
Work effectively as a team player with peers DPC GR/FE
Communicate effectively with supervisors DPC GR/FE
Be effective and empathic working with families DPC, DSP GR/FE, 360
Effectively liaison with professional colleagues in other fields (i.e. primary care physician)
DPC GR/FE, 360
Adapt style of interaction specific to age and cognitive DL, DPC, GR/FE
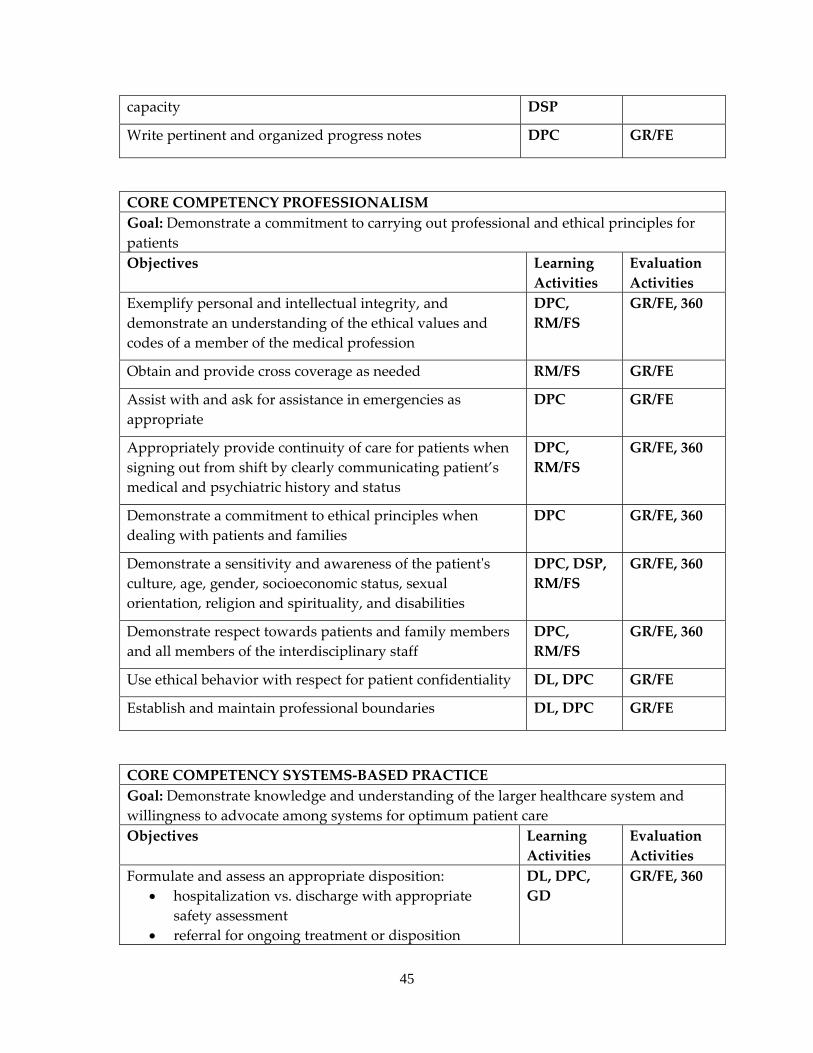
45
capacity DSP
Write pertinent and organized progress notes DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS
GR/FE, 360
Obtain and provide cross coverage as needed RM/FS GR/FE
Assist with and ask for assistance in emergencies as appropriate
DPC GR/FE
Appropriately provide continuity of care for patients when signing out from shift by clearly communicating patient’s medical and psychiatric history and status
DPC, RM/FS
GR/FE, 360
Demonstrate a commitment to ethical principles when dealing with patients and families
DPC GR/FE, 360
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE, 360
Demonstrate respect towards patients and family members and all members of the interdisciplinary staff
DPC, RM/FS
GR/FE, 360
Use ethical behavior with respect for patient confidentiality DL, DPC GR/FE
Establish and maintain professional boundaries DL, DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Formulate and assess an appropriate disposition: • hospitalization vs. discharge with appropriate
safety assessment • referral for ongoing treatment or disposition
DL, DPC, GD
GR/FE, 360
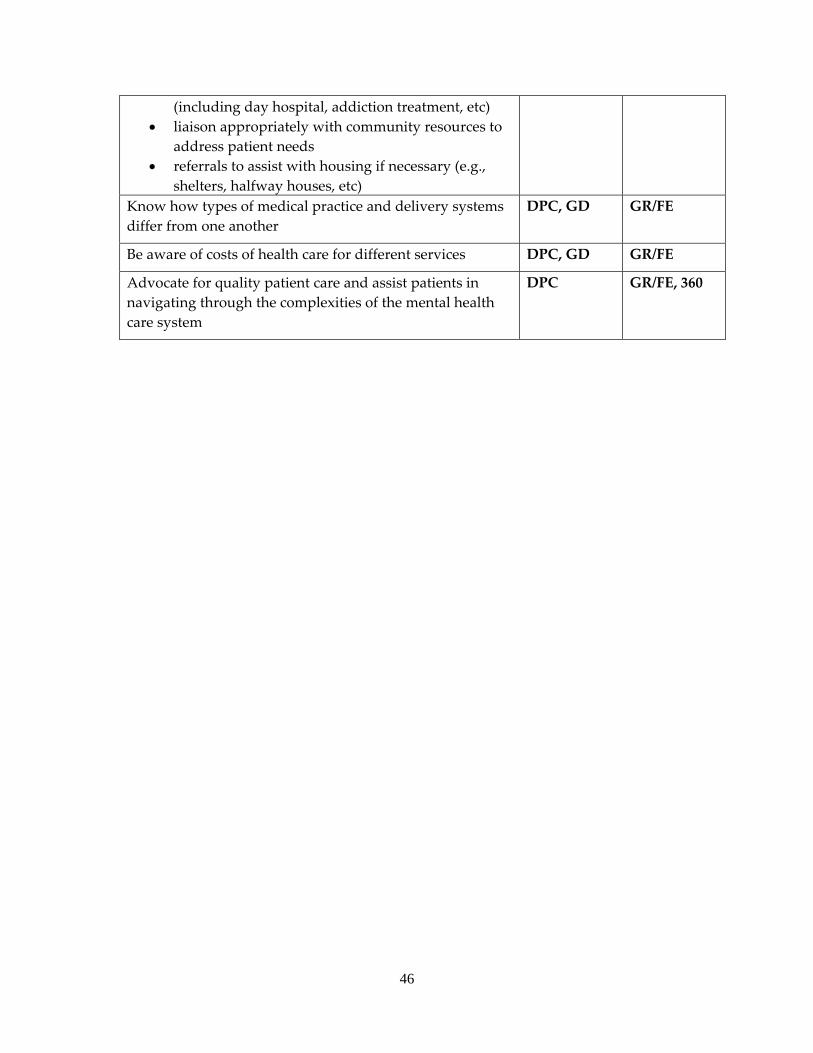
46
(including day hospital, addiction treatment, etc) • liaison appropriately with community resources to
address patient needs • referrals to assist with housing if necessary (e.g.,
shelters, halfway houses, etc) Know how types of medical practice and delivery systems differ from one another
DPC, GD GR/FE
Be aware of costs of health care for different services DPC, GD GR/FE
Advocate for quality patient care and assist patients in navigating through the complexities of the mental health care system
DPC GR/FE, 360
47
a. METHADONE CLINIC b. A 1‐2 month required rotation usually occurring in the PGY4 year. c. Faculty consists of one full‐time psychiatrist with extensive experience in addiction
treatment, who is the medical director, two masters level and one certified substance abuse counselors, one advanced practice nurse and one bachelors level nurse.
d. During the rotation at the clinic, the psychiatry resident will receive supervision in the evaluation and management of opioid dependent patients, management of comorbid disorders and receive training regarding regulatory requirements for opioid replacement, including buprenorphine. The resident learns the stages of stabilization, relapse, and recovery. Faculty is always available for consultation.
e. The clinical population consists of about 250 individuals enrolled in opioid replacement treatment, with an average patient age of slightly less than 42 years. There is a 2:1 male to female ratio. The ethnic distribution is approximately 85% Caucasian, 10% African‐American, 3% Hispanic and 2% not specified. Treatment modalities include individual therapy, psychoeducational groups, relapse prevention, cognitive‐behavioral treatment, introduction to 12‐step programs, and continuing care. The majority of patients have comorbid psychiatric disorders including major depression, anxiety, bipolar affective disorder, antisocial personality and borderline personality disorders. Abused opioids include heroin and narcotic analgesics; most patients also have a history of polysubstance abuse.
f. The caseload consists of 2‐3 acute evaluations weekly and 8‐10 individual therapy patients.
g. The resident will work with a multidisciplinary treatment team available for assistance and training. Supervision will be provided for one hour, twice weekly during the intensive training phase; and one hour weekly during the extension phase. The resident will work with a multidisciplinary treatment team available for assistance and training. Additional supervision may be provided on an individual basis. In addition to daily supervision, the residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision.
PAIN MANAGEMENT SERVICE
a. A 1‐2 month required half‐time rotation combined with the Methadone Clinic rotation. This rotation most frequently occurs in the PGY4 year.
b. Faculty consists of 2 full‐time Internist/Psychiatrists with added qualifications in pain management. Residents also interact frequently with the hospital‐based pain management team.
c. Residents learn the assessment of pain and associated psychiatric symptoms in the patient with chronic pain.
d. The patient population is a widely diverse population of patients with chronic low back and abdominal pain, headache, neurogenic, and post‐traumatic pain
48
syndromes. They are a selection of patients referred from both physicians at the University of Kansas Medical Center and community physicians. Some patients have histories of substance use disorders and psychiatric disorders.
e. Residents participate in two clinic sessions per week, for a total of 4 to 10 patient contacts weekly, four of those being new patient evaluations.. In addition, they make hospital rounds with the KU Hospital Pain Management Team, and see a variety of patients with acute pain. They see from 4 to 6 patients weekly in that venue.
f. The psychiatry resident is constantly supervised by the faculty attending. Supervision of the resident by the faculty attending during their rotations consists of one full‐day and one half‐day clinic, weekly supervision sessions, and pain consult rounds lasting 8‐10 hours weekly. In addition to daily supervision, residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision.
a. NEUROLOGY SERVICE b. Required 1‐2 month rotation occurring in either the PGY1 or PGY2 year. c. At this institution there are 21 clinical full‐time clinical faculty. Three faculty provide
the majority of hospital based supervision, Gary Gronseth, MD, Collen Lechtenberg, MD, and Yunxia Wang, MD. The rest of the faculty cover for the hospitalist service and share weekend supervision and teaching responsibilities. Usually there are two or more residents on the Ward service; which may include Neurology residents, Pediatric Neurology fellows, PGY1 Neurosurgical resident, and Psychiatry residents. The consult service is usually one Neurology resident and one rotating resident from Internal Medicine
d. Residents spend approximately five to seven hours per week in Neurology case conferences, seminars, didactic lecturers, and Journal Club activity. The monthly rotation consists of two weeks on the KU ward service and two weeks on consults. Every day, one‐half day is spent with the Neurology attending on teaching rounds, and one‐half day is spent with the neurology resident on the wards or consults.
e. The Neurology patient population is 45%male and 55% female. 80% percent are Caucasian, 10% African‐American, and 10% other ethnic categories. The age range is 18‐90+ years of age with average ages between 60 and 70 years. The most frequent diagnoses are stroke (ischemic and hemorrhagic), Multiple Sclerosis, epilepsy, acute and chronic neuropathies, dementia, movement disorders, ALS and neurological problems secondary to medical illnesses.
f. The psychiatry residents’ caseload varies between 4‐6 patients daily, on the neurology ward service and 3‐7 patients daily on the neurology consult service. The average daily ward census is 16 patients and there are usually five to ten new consultation requests each day.
g. All residents have a minimum of 4 hours of daily supervision by faculty, which are given in a small group setting. Other supervision includes senior and junior neurology residents teaching and reviewing the neuro‐exam.
49
h. The Neurology ward rotation provides good exposure to common neurological problems. On the consult service the psychiatry resident is exposed to the neurological manifestations of systemic illnesses, many which have psychiatric comorbidities such as metabolic encephalopathy, behavioral disorders, traumatic brain injury, movement disorders secondary to psychotropic meds and non‐epileptic seizures. They have the opportunity to interact closely with Neurology residents.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: METHADONE‐PAIN LEVEL: PGY4 DURATON: 1‐2 MONTHS (1/2 TIME METHADONE CLINIC, 1/2 TIME PAIN CLINIC) SITE: KU SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KU HOSPITAL By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
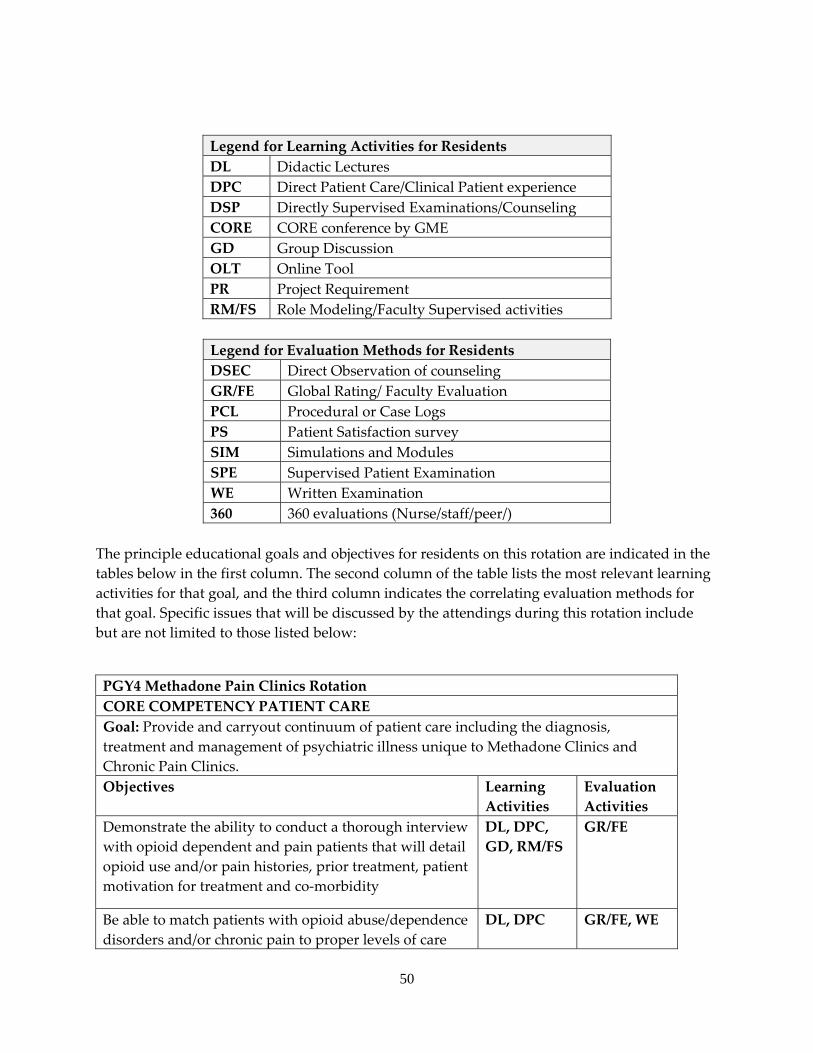
50
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during this rotation include but are not limited to those listed below:
PGY4 Methadone Pain Clinics Rotation CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to Methadone Clinics and Chronic Pain Clinics. Objectives Learning
Activities Evaluation Activities
Demonstrate the ability to conduct a thorough interview with opioid dependent and pain patients that will detail opioid use and/or pain histories, prior treatment, patient motivation for treatment and co‐morbidity
DL, DPC, GD, RM/FS
GR/FE
Be able to match patients with opioid abuse/dependence disorders and/or chronic pain to proper levels of care
DL, DPC GR/FE, WE
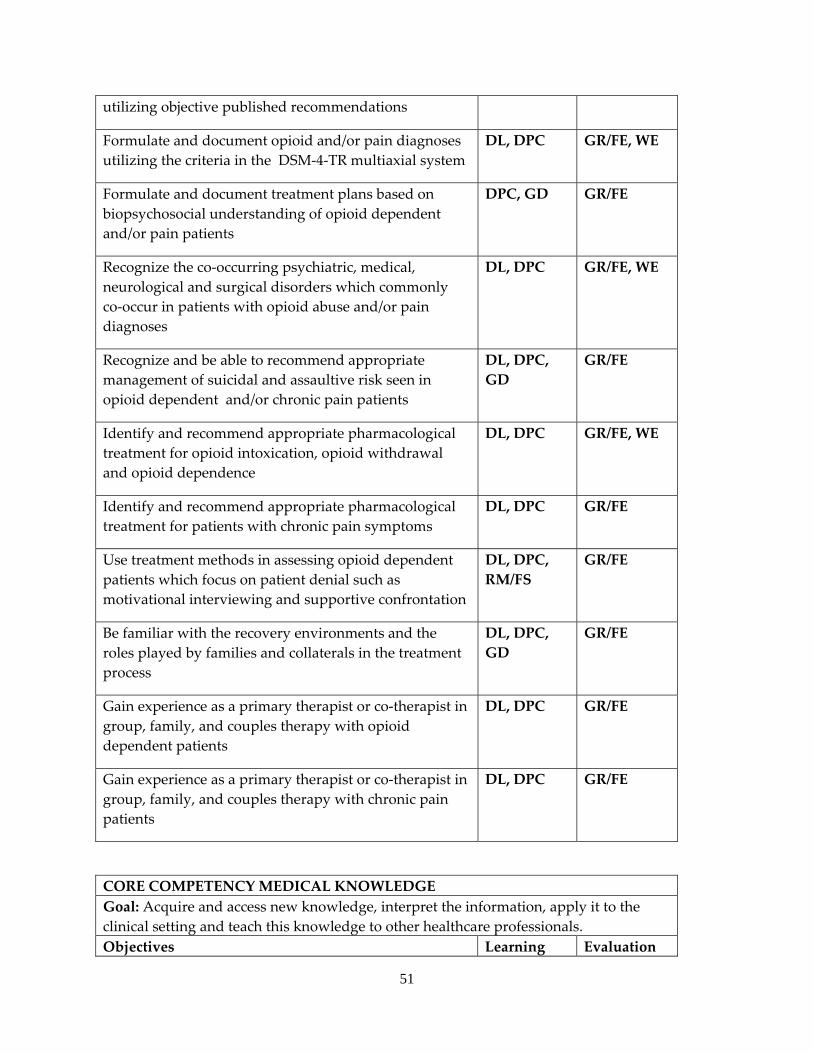
51
utilizing objective published recommendations
Formulate and document opioid and/or pain diagnoses utilizing the criteria in the DSM‐4‐TR multiaxial system
DL, DPC GR/FE, WE
Formulate and document treatment plans based on biopsychosocial understanding of opioid dependent and/or pain patients
DPC, GD GR/FE
Recognize the co‐occurring psychiatric, medical, neurological and surgical disorders which commonly co‐occur in patients with opioid abuse and/or pain diagnoses
DL, DPC GR/FE, WE
Recognize and be able to recommend appropriate management of suicidal and assaultive risk seen in opioid dependent and/or chronic pain patients
DL, DPC, GD
GR/FE
Identify and recommend appropriate pharmacological treatment for opioid intoxication, opioid withdrawal and opioid dependence
DL, DPC GR/FE, WE
Identify and recommend appropriate pharmacological treatment for patients with chronic pain symptoms
DL, DPC GR/FE
Use treatment methods in assessing opioid dependent patients which focus on patient denial such as motivational interviewing and supportive confrontation
DL, DPC, RM/FS
GR/FE
Be familiar with the recovery environments and the roles played by families and collaterals in the treatment process
DL, DPC, GD
GR/FE
Gain experience as a primary therapist or co‐therapist in group, family, and couples therapy with opioid dependent patients
DL, DPC GR/FE
Gain experience as a primary therapist or co‐therapist in group, family, and couples therapy with chronic pain patients
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionals. Objectives Learning Evaluation
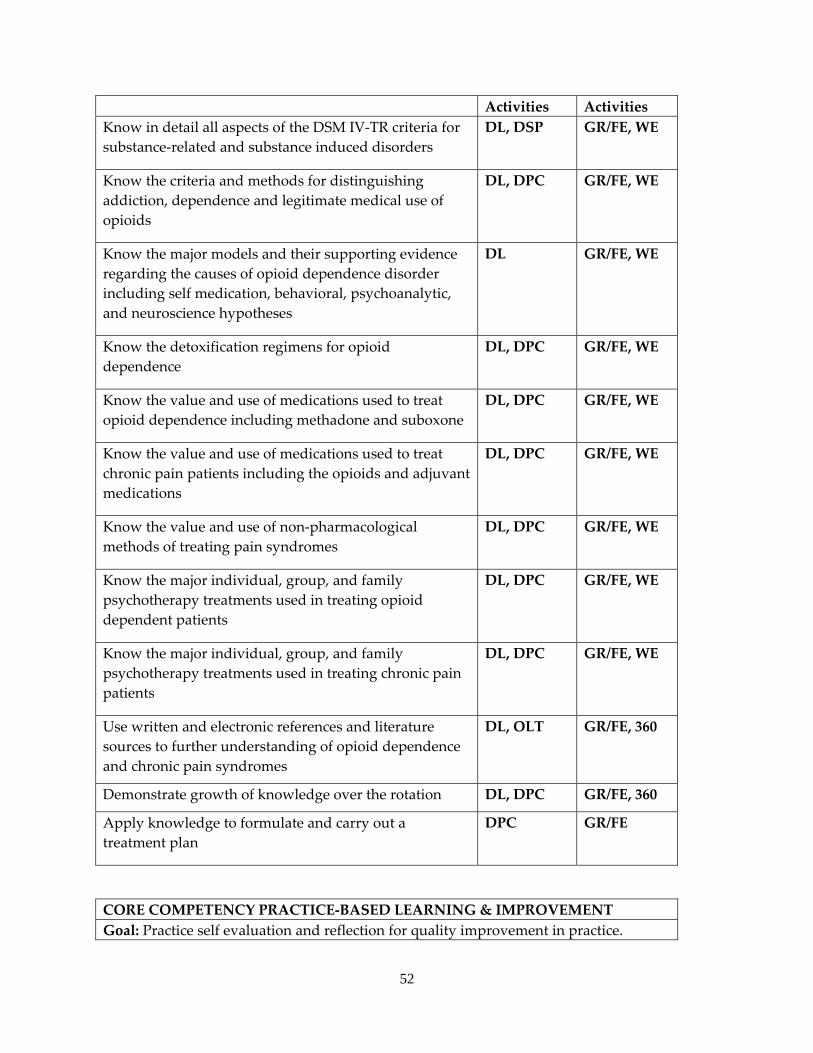
52
Activities Activities Know in detail all aspects of the DSM IV‐TR criteria for substance‐related and substance induced disorders
DL, DSP GR/FE, WE
Know the criteria and methods for distinguishing addiction, dependence and legitimate medical use of opioids
DL, DPC GR/FE, WE
Know the major models and their supporting evidence regarding the causes of opioid dependence disorder including self medication, behavioral, psychoanalytic, and neuroscience hypotheses
DL GR/FE, WE
Know the detoxification regimens for opioid dependence
DL, DPC GR/FE, WE
Know the value and use of medications used to treat opioid dependence including methadone and suboxone
DL, DPC GR/FE, WE
Know the value and use of medications used to treat chronic pain patients including the opioids and adjuvant medications
DL, DPC GR/FE, WE
Know the value and use of non‐pharmacological methods of treating pain syndromes
DL, DPC GR/FE, WE
Know the major individual, group, and family psychotherapy treatments used in treating opioid dependent patients
DL, DPC GR/FE, WE
Know the major individual, group, and family psychotherapy treatments used in treating chronic pain patients
DL, DPC GR/FE, WE
Use written and electronic references and literature sources to further understanding of opioid dependence and chronic pain syndromes
DL, OLT GR/FE, 360
Demonstrate growth of knowledge over the rotation DL, DPC GR/FE, 360
Apply knowledge to formulate and carry out a treatment plan
DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Practice self evaluation and reflection for quality improvement in practice.
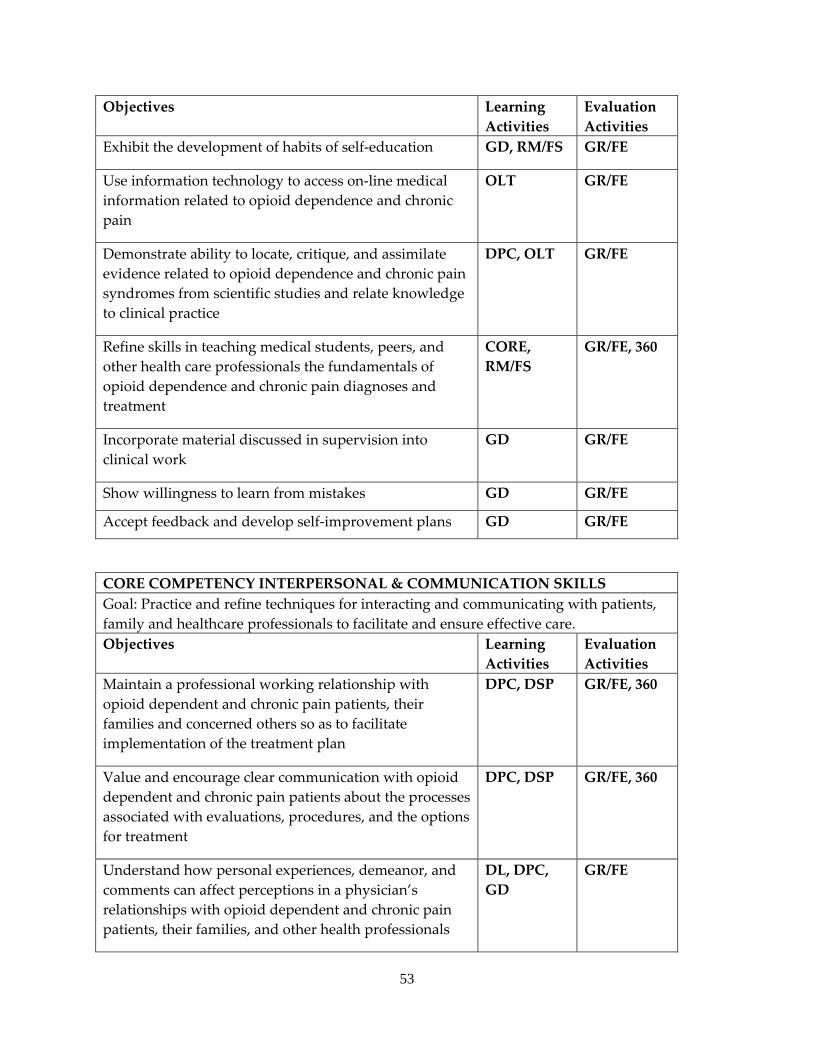
53
Objectives Learning Activities
Evaluation Activities
Exhibit the development of habits of self‐education GD, RM/FS GR/FE
Use information technology to access on‐line medical information related to opioid dependence and chronic pain
OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence related to opioid dependence and chronic pain syndromes from scientific studies and relate knowledge to clinical practice
DPC, OLT GR/FE
Refine skills in teaching medical students, peers, and other health care professionals the fundamentals of opioid dependence and chronic pain diagnoses and treatment
CORE, RM/FS
GR/FE, 360
Incorporate material discussed in supervision into clinical work
GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self‐improvement plans GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care. Objectives Learning
Activities Evaluation Activities
Maintain a professional working relationship with opioid dependent and chronic pain patients, their families and concerned others so as to facilitate implementation of the treatment plan
DPC, DSP GR/FE, 360
Value and encourage clear communication with opioid dependent and chronic pain patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE, 360
Understand how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with opioid dependent and chronic pain patients, their families, and other health professionals
DL, DPC, GD
GR/FE
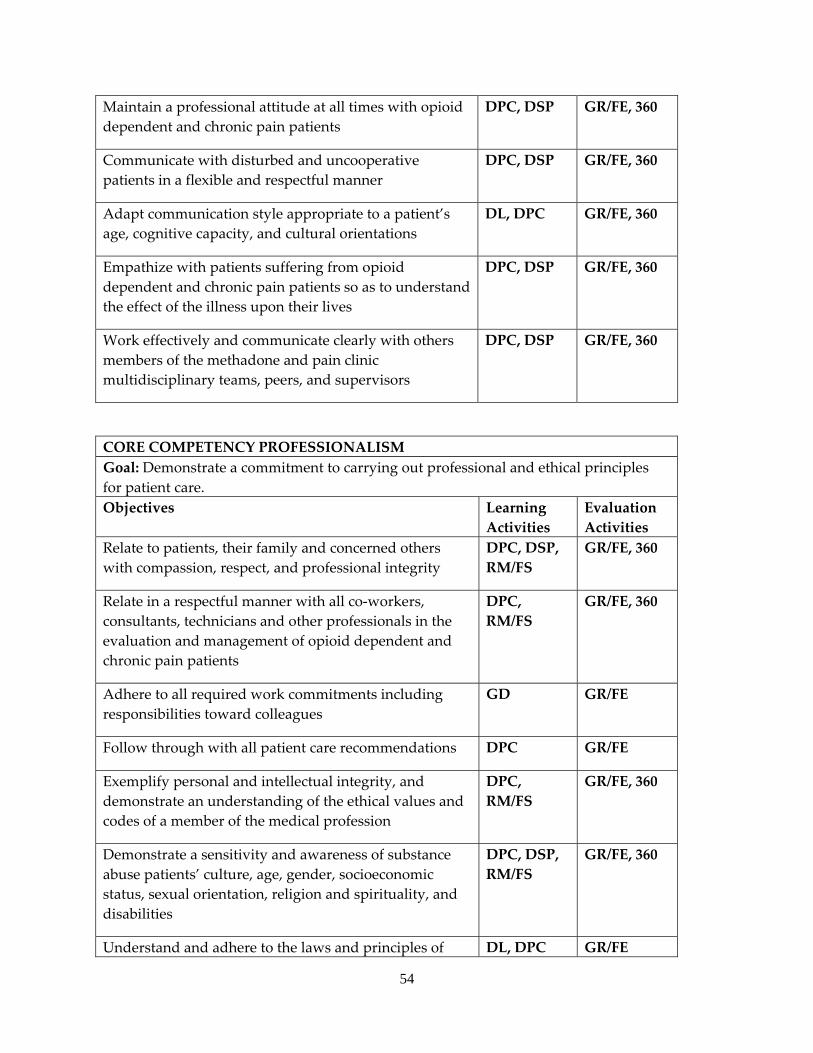
54
Maintain a professional attitude at all times with opioid dependent and chronic pain patients
DPC, DSP GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC, DSP GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from opioid dependent and chronic pain patients so as to understand the effect of the illness upon their lives
DPC, DSP GR/FE, 360
Work effectively and communicate clearly with others members of the methadone and pain clinic multidisciplinary teams, peers, and supervisors
DPC, DSP GR/FE, 360
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patient care. Objectives Learning
Activities Evaluation Activities
Relate to patients, their family and concerned others with compassion, respect, and professional integrity
DPC, DSP, RM/FS
GR/FE, 360
Relate in a respectful manner with all co‐workers, consultants, technicians and other professionals in the evaluation and management of opioid dependent and chronic pain patients
DPC, RM/FS
GR/FE, 360
Adhere to all required work commitments including responsibilities toward colleagues
GD GR/FE
Follow through with all patient care recommendations DPC GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS
GR/FE, 360
Demonstrate a sensitivity and awareness of substance abuse patients’ culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE, 360
Understand and adhere to the laws and principles of DL, DPC GR/FE
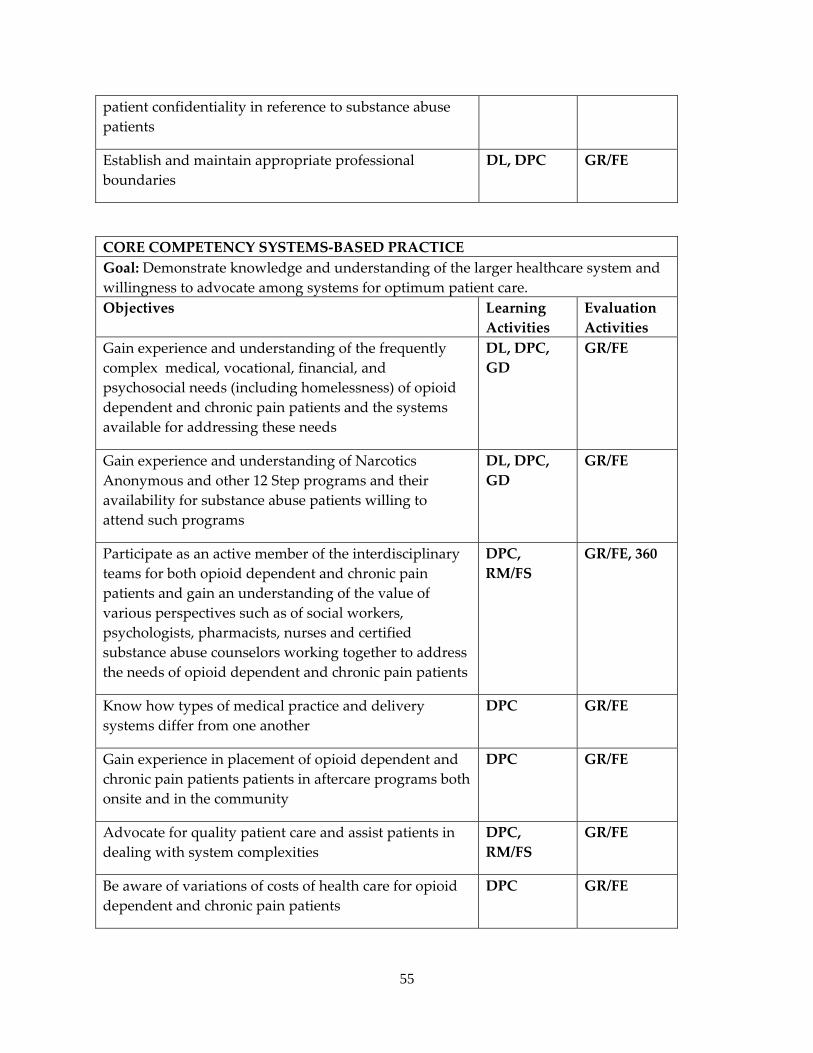
55
patient confidentiality in reference to substance abuse patients
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care.Objectives Learning
Activities Evaluation Activities
Gain experience and understanding of the frequently complex medical, vocational, financial, and psychosocial needs (including homelessness) of opioid dependent and chronic pain patients and the systems available for addressing these needs
DL, DPC, GD
GR/FE
Gain experience and understanding of Narcotics Anonymous and other 12 Step programs and their availability for substance abuse patients willing to attend such programs
DL, DPC, GD
GR/FE
Participate as an active member of the interdisciplinary teams for both opioid dependent and chronic pain patients and gain an understanding of the value of various perspectives such as of social workers, psychologists, pharmacists, nurses and certified substance abuse counselors working together to address the needs of opioid dependent and chronic pain patients
DPC, RM/FS
GR/FE, 360
Know how types of medical practice and delivery systems differ from one another
DPC GR/FE
Gain experience in placement of opioid dependent and chronic pain patients patients in aftercare programs both onsite and in the community
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS
GR/FE
Be aware of variations of costs of health care for opioid dependent and chronic pain patients
DPC GR/FE
56
INTERNAL MEDICINE SERVICE
a. A required 2 month rotation during the PGY1 year as part of the 4 month primary care medicine block.
b. A different full time faculty internist and senior supervising internal medicine resident is assigned to the service every 4 weeks.
c. Residents attend 12 hours of case conferences and didactic presentations weekly (six days per week); attend daily morning conference; and meet daily with attending staff for consultation regarding patient management.
d. The patients at KU Hospital represent a wide range of ages from young adult to geriatric and both genders are equally represented. While there are plenty of patients with “common” diagnoses such as pneumonia, cellulitis, COPD, etc., admitted to the general medicine services from the ED or the general medicine clinics, there are also significant numbers of patients with less common diagnoses admitted to both internal medicine and subspecialty services.
e. An average case load consists of a maximum of 6‐8 patients per intern. f. Residents receive daily close supervision by the attending staff physician and
continuous supervision by a senior internal medicine resident. Consultation is available at all times.
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: INTERNAL MEDICINE LEVEL: PGY1 DURATON: 4 MONTHS SITE: KU HOSPITAL SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING INTERNAL MEDICINE ATTENDING AT KU HOSPITAL
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
57
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the internal medicine rotation include but are not limited to those listed below:
The knowledge, skills, and attitudes to be acquired during the internal medicine rotation in order to demonstrate progress toward achievement of these competencies are:
PGY1 Internal Medicine Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving
58
inpatient medical care including the diagnosis, treatment and management of medical illness. Objectives Learning
Activities Evaluation Activities
Obtain accurate clinical history DL, DPC, RM/FS
GR/FE
Identify and review relevant existing patient data DPC GR/FE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, RM/FS
GR/FE
Demonstrate appropriate physical exam skills DPC, RM/FS GR/FE
Order appropriate diagnostic tests DL, DPC GR/FE
Prioritize problems and treatment plans appropriately DPC GR/FE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DPC, RM/FS GR/FE
Effectively use consultation services DPC, RM/FS GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting. Objectives Learning
Activities Evaluation Activities
Demonstrate understanding of clinical problems and their pathophysiology
DL, DPC, GD
GR/FE
Develop appropriate differential diagnoses DPC, GD GR/FE
Evaluate scientific basis of diagnostic tests used DL, DPC, OLT
GR/FE
Read service specific literature DL GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DPC, GD
GR/FE, WE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC GR/FE
Know the indications and restrictions regarding the use of behavioral restraints on the medical ward
DL, DPC, GD
GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting for the optimum care
DPC, GD, RM/FS
GR/FE
59
of medical patients (e.g., nurses, social workers, nurse case managers, police)
Use written and electronic reference and literature sources to learn about patients’ medical illness
DL, OLT GR/FE
Demonstrate growth of medical knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice. Objectives Learning
Activities Evaluation Activities
Apply lessons learned from medical errors into practice GD, RM/FS GR/FE
Identify areas for improvement and apply it to practice DPC, GD GR/FE
Show interest in learning from complex care issues DPC GR/FE
Develop fundamental skills in teaching medical students, peers, and other heal care professionals
CORE, GD, RM/FS
GR/FE
Use information technology to access on‐line medical information
GD, OLT GR/FE
Learn to locate, critique, and assimilate evidence from scientific studies and related knowledge to clinical practice
DL GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for medically ill patients. Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families, and concerned others so as to facilitate the treatment plan in inpatient settings
DPC GR/FE
Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, DPC, RM/FS
GR/FE
Maintain a professional attitude at all times with patients DPC, RM/FS GR/FE Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE
Write pertinent and organized progress notes and timely DPC GR/FE
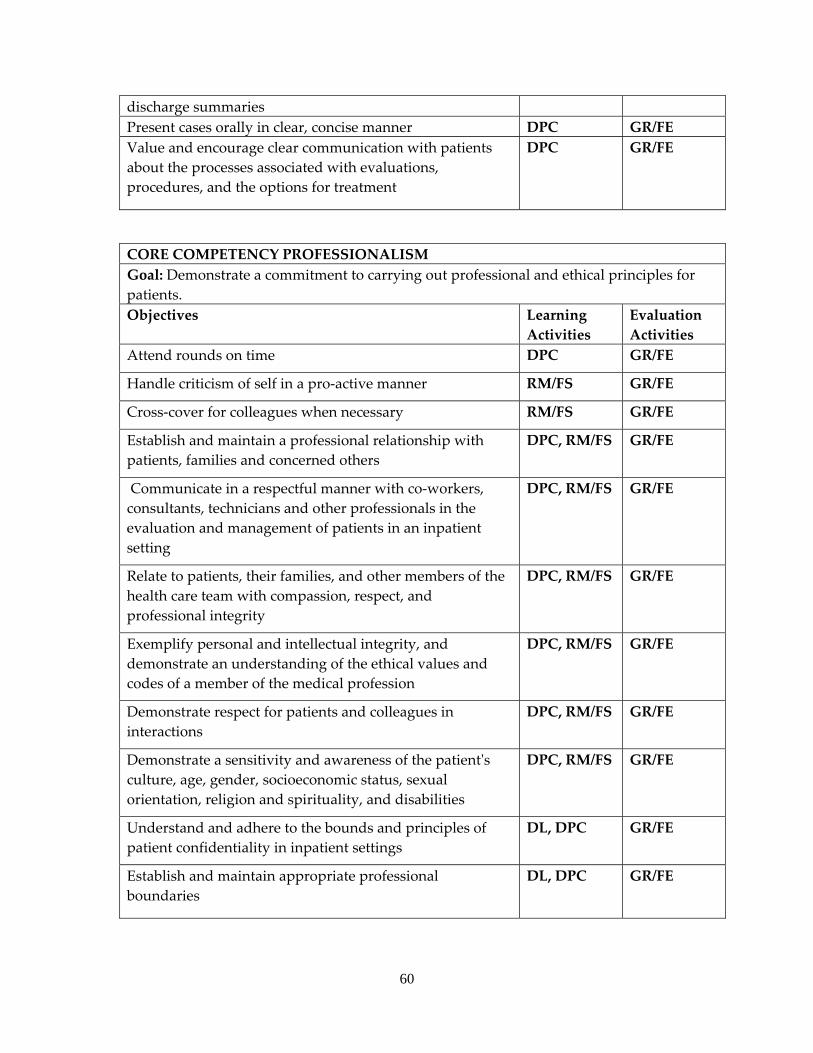
60
discharge summaries Present cases orally in clear, concise manner DPC GR/FE Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients. Objectives Learning
Activities Evaluation Activities
Attend rounds on time DPC GR/FE
Handle criticism of self in a pro‐active manner RM/FS GR/FE
Cross‐cover for colleagues when necessary RM/FS GR/FE
Establish and maintain a professional relationship with patients, families and concerned others
DPC, RM/FS GR/FE
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions
DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS GR/FE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
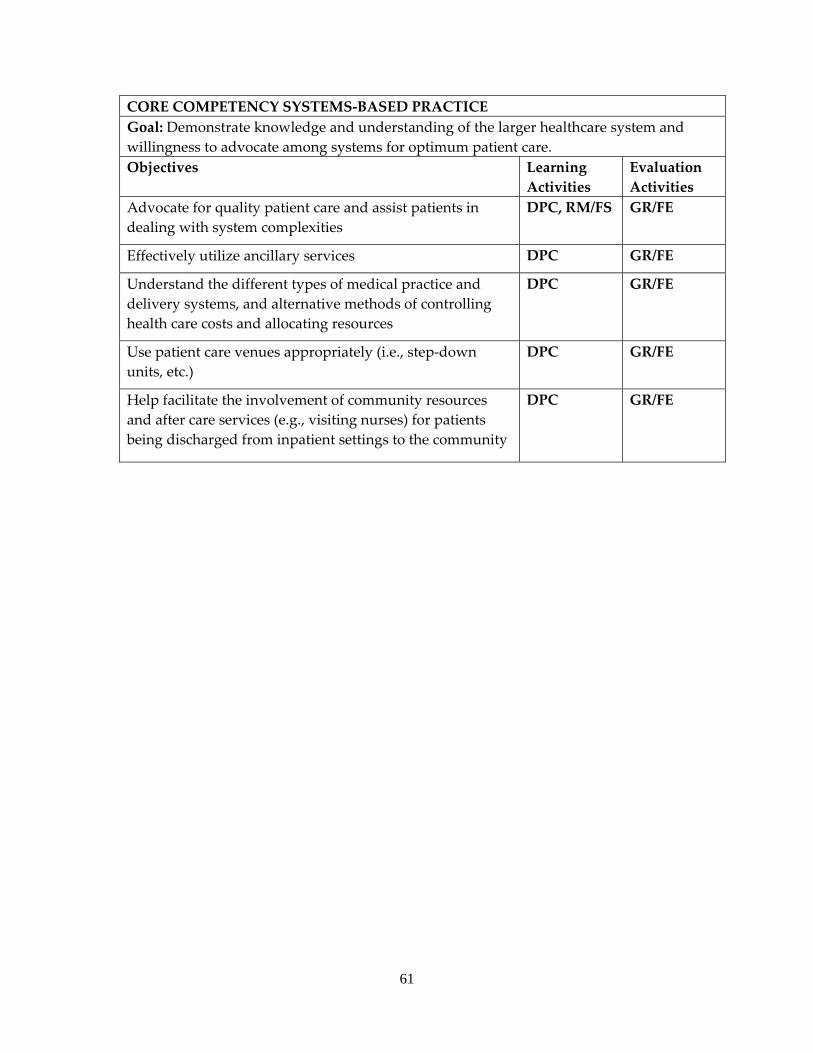
61
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care. Objectives Learning
Activities Evaluation Activities
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
Effectively utilize ancillary services DPC GR/FE
Understand the different types of medical practice and delivery systems, and alternative methods of controlling health care costs and allocating resources
DPC GR/FE
Use patient care venues appropriately (i.e., step‐down units, etc.)
DPC GR/FE
Help facilitate the involvement of community resources and after care services (e.g., visiting nurses) for patients being discharged from inpatient settings to the community
DPC GR/FE
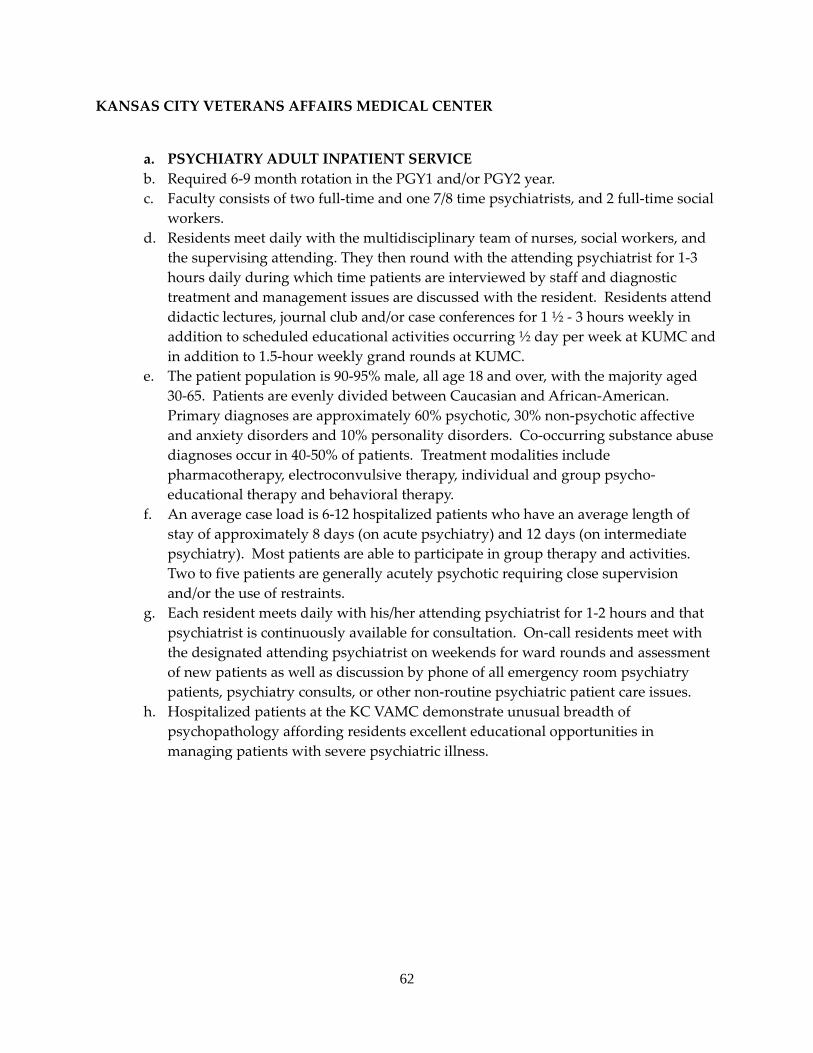
62
KANSAS CITY VETERANS AFFAIRS MEDICAL CENTER
a. PSYCHIATRY ADULT INPATIENT SERVICE b. Required 6‐9 month rotation in the PGY1 and/or PGY2 year. c. Faculty consists of two full‐time and one 7/8 time psychiatrists, and 2 full‐time social
workers. d. Residents meet daily with the multidisciplinary team of nurses, social workers, and
the supervising attending. They then round with the attending psychiatrist for 1‐3 hours daily during which time patients are interviewed by staff and diagnostic treatment and management issues are discussed with the resident. Residents attend didactic lectures, journal club and/or case conferences for 1 ½ ‐ 3 hours weekly in addition to scheduled educational activities occurring ½ day per week at KUMC and in addition to 1.5‐hour weekly grand rounds at KUMC.
e. The patient population is 90‐95% male, all age 18 and over, with the majority aged 30‐65. Patients are evenly divided between Caucasian and African‐American. Primary diagnoses are approximately 60% psychotic, 30% non‐psychotic affective and anxiety disorders and 10% personality disorders. Co‐occurring substance abuse diagnoses occur in 40‐50% of patients. Treatment modalities include pharmacotherapy, electroconvulsive therapy, individual and group psycho‐educational therapy and behavioral therapy.
f. An average case load is 6‐12 hospitalized patients who have an average length of stay of approximately 8 days (on acute psychiatry) and 12 days (on intermediate psychiatry). Most patients are able to participate in group therapy and activities. Two to five patients are generally acutely psychotic requiring close supervision and/or the use of restraints.
g. Each resident meets daily with his/her attending psychiatrist for 1‐2 hours and that psychiatrist is continuously available for consultation. On‐call residents meet with the designated attending psychiatrist on weekends for ward rounds and assessment of new patients as well as discussion by phone of all emergency room psychiatry patients, psychiatry consults, or other non‐routine psychiatric patient care issues.
h. Hospitalized patients at the KC VAMC demonstrate unusual breadth of psychopathology affording residents excellent educational opportunities in managing patients with severe psychiatric illness.
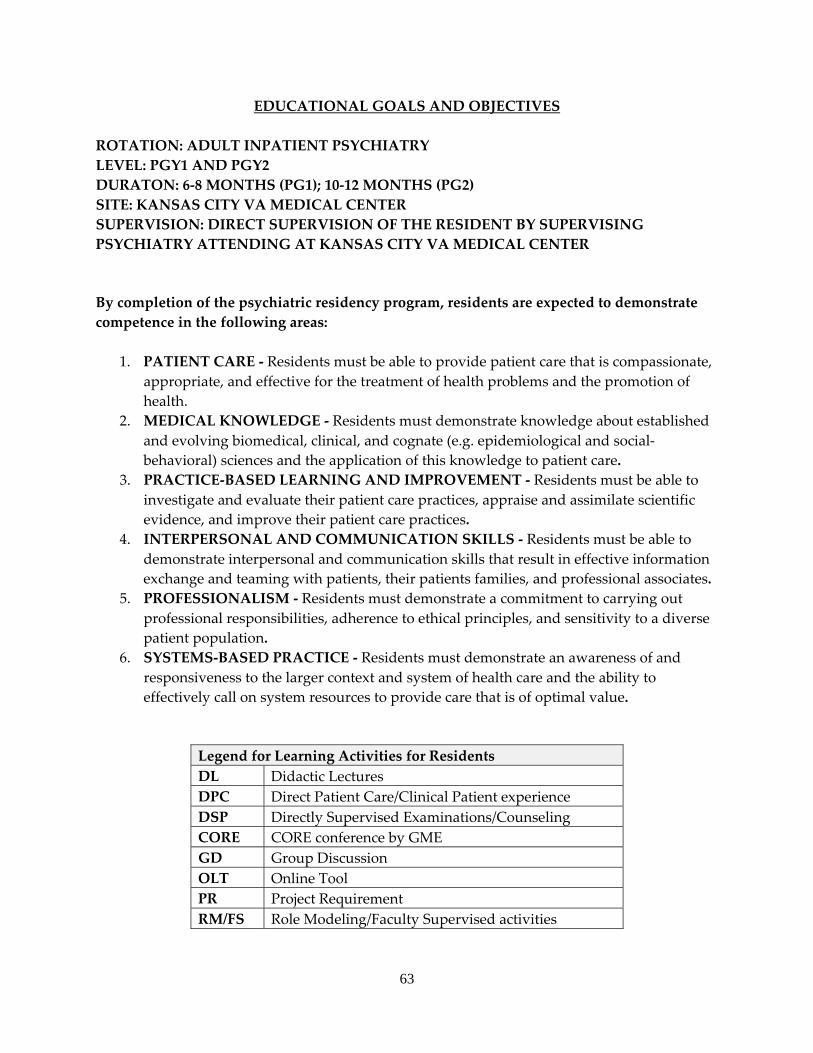
63
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: ADULT INPATIENT PSYCHIATRY LEVEL: PGY1 AND PGY2 DURATON: 6‐8 MONTHS (PG1); 10‐12 MONTHS (PG2) SITE: KANSAS CITY VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KANSAS CITY VA MEDICAL CENTER
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
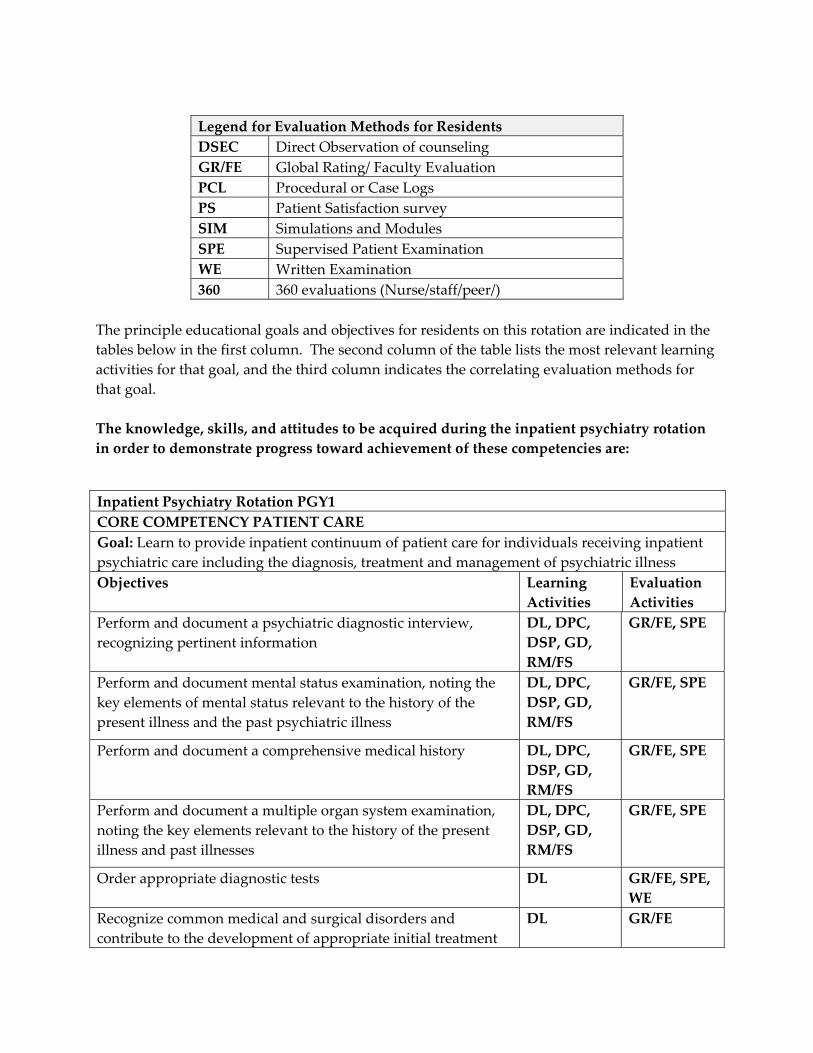
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. The knowledge, skills, and attitudes to be acquired during the inpatient psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Inpatient Psychiatry Rotation PGY1 CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illness Objectives Learning
Activities Evaluation Activities
Perform and document a psychiatric diagnostic interview, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Order appropriate diagnostic tests DL GR/FE, SPE, WE
Recognize common medical and surgical disorders and contribute to the development of appropriate initial treatment
DL GR/FE
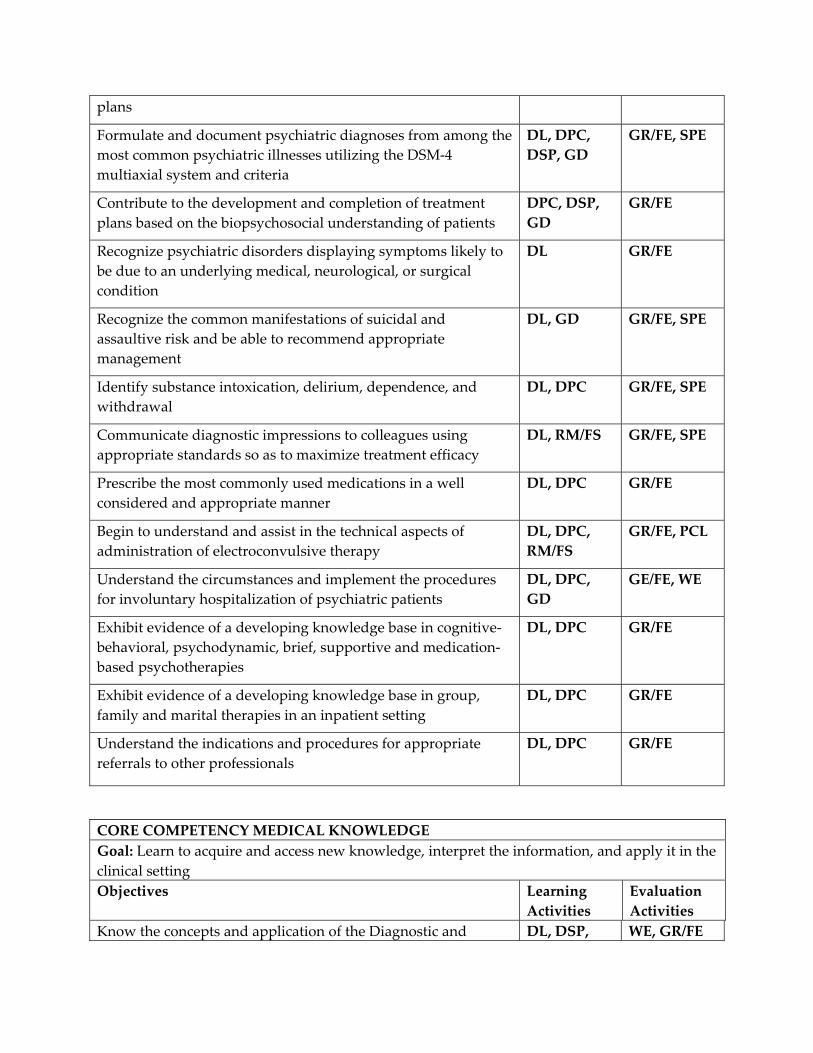
plans
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DL, DPC, DSP, GD
GR/FE, SPE
Contribute to the development and completion of treatment plans based on the biopsychosocial understanding of patients
DPC, DSP, GD
GR/FE
Recognize psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL GR/FE
Recognize the common manifestations of suicidal and assaultive risk and be able to recommend appropriate management
DL, GD GR/FE, SPE
Identify substance intoxication, delirium, dependence, and withdrawal
DL, DPC GR/FE, SPE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe the most commonly used medications in a well considered and appropriate manner
DL, DPC GR/FE
Begin to understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GE/FE, WE
Exhibit evidence of a developing knowledge base in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Exhibit evidence of a developing knowledge base in group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and DL, DSP, WE, GR/FE
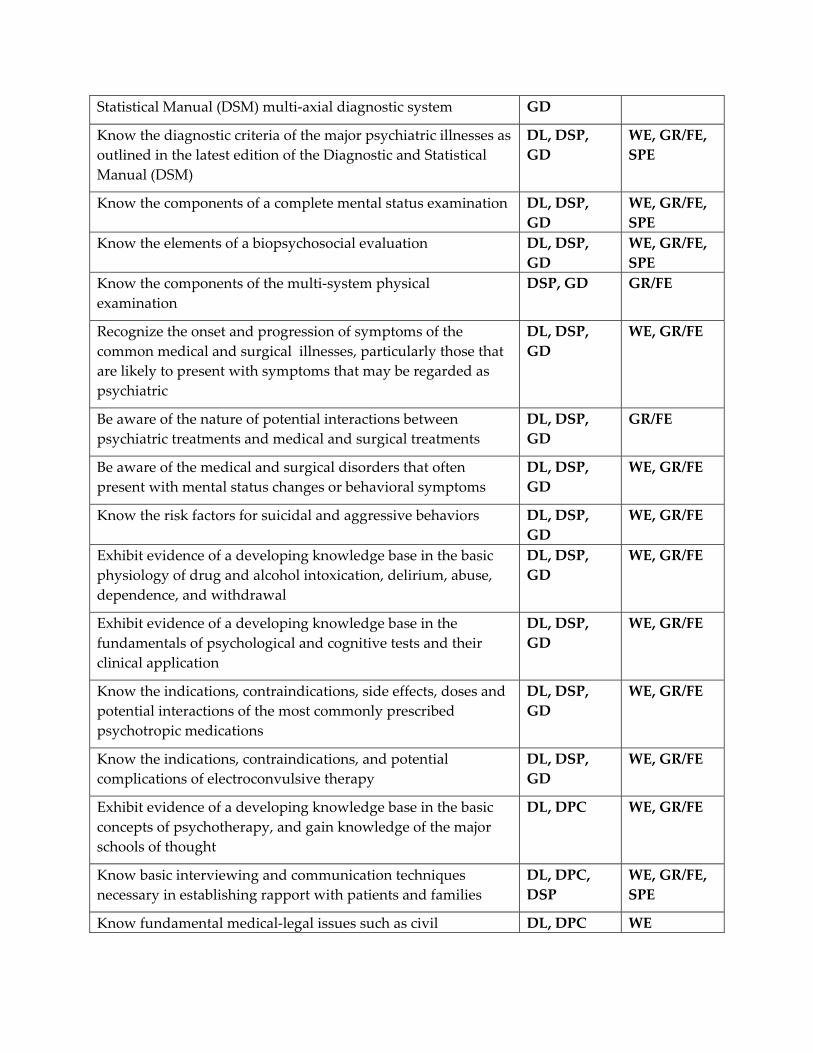
Statistical Manual (DSM) multi‐axial diagnostic system GD
Know the diagnostic criteria of the major psychiatric illnesses as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Recognize the onset and progression of symptoms of the common medical and surgical illnesses, particularly those that are likely to present with symptoms that may be regarded as psychiatric
DL, DSP, GD
WE, GR/FE
Be aware of the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Be aware of the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of the most commonly prescribed psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil DL, DPC WE
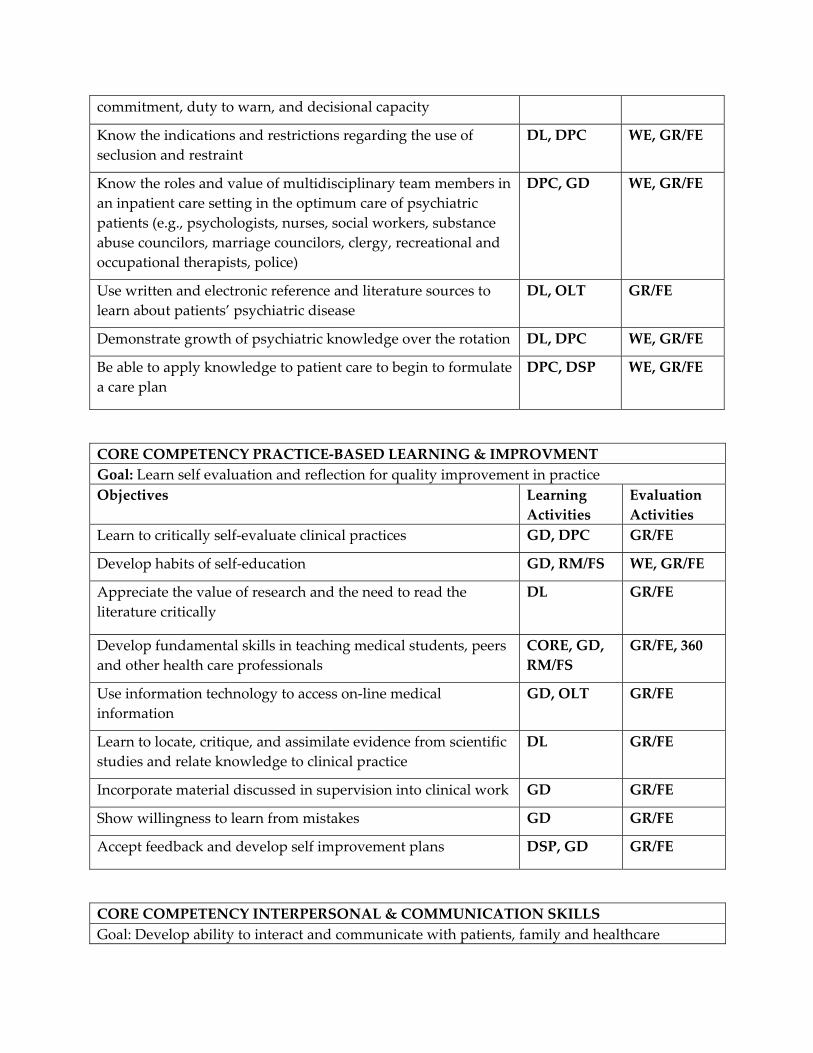
commitment, duty to warn, and decisional capacity
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and occupational therapists, police)
DPC, GD WE, GR/FE
Use written and electronic reference and literature sources to learn about patients’ psychiatric disease
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
Be able to apply knowledge to patient care to begin to formulate a care plan
DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Learn to critically self‐evaluate clinical practices GD, DPC GR/FE
Develop habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Develop fundamental skills in teaching medical students, peers and other health care professionals
CORE, GD, RM/FS
GR/FE, 360
Use information technology to access on‐line medical information
GD, OLT GR/FE
Learn to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare
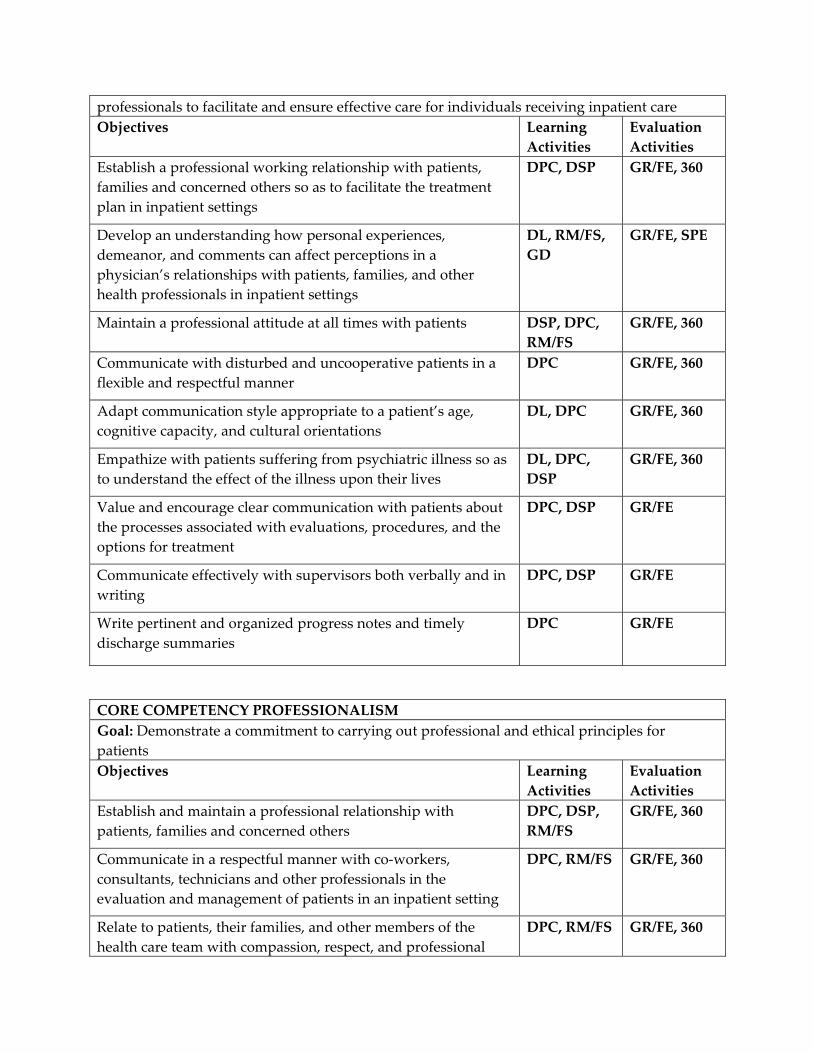
professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, RM/FS, GD
GR/FE, SPE
Maintain a professional attitude at all times with patients DSP, DPC, RM/FS
GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors both verbally and in writing
DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional
DPC, RM/FS GR/FE, 360
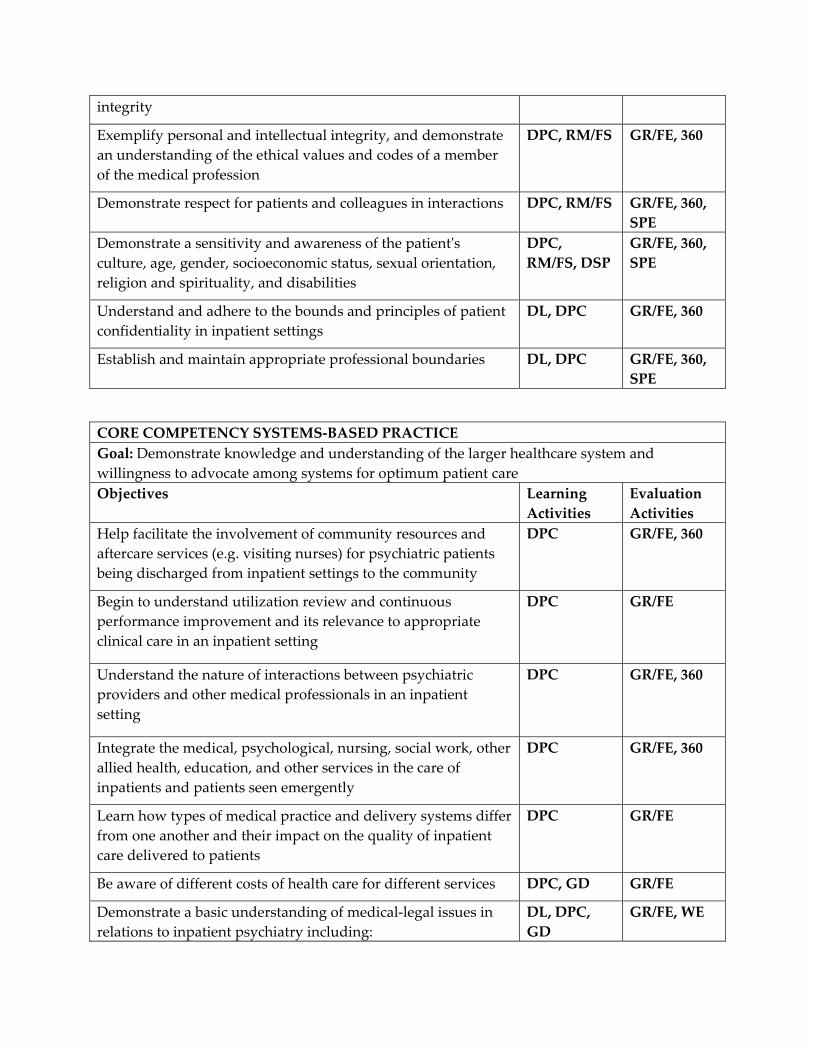
integrity
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/FE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC GR/FE, 360
Begin to understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Learn how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate a basic understanding of medical‐legal issues in relations to inpatient psychiatry including:
DL, DPC, GD
GR/FE, WE
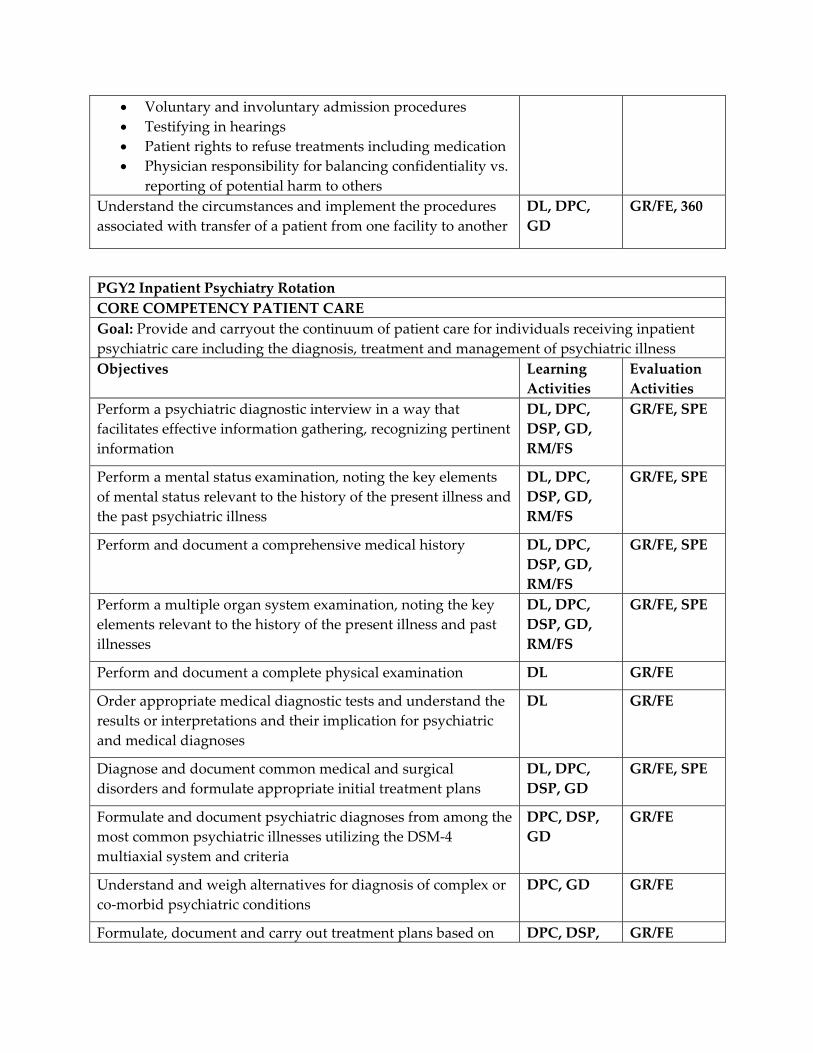
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360
PGY2 Inpatient Psychiatry Rotation CORE COMPETENCY PATIENT CARE Goal: Provide and carryout the continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illness Objectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview in a way that facilitates effective information gathering, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a complete physical examination DL GR/FE
Order appropriate medical diagnostic tests and understand the results or interpretations and their implication for psychiatric and medical diagnoses
DL GR/FE
Diagnose and document common medical and surgical disorders and formulate appropriate initial treatment plans
DL, DPC, DSP, GD
GR/FE, SPE
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DPC, DSP, GD
GR/FE
Understand and weigh alternatives for diagnosis of complex or co‐morbid psychiatric conditions
DPC, GD GR/FE
Formulate, document and carry out treatment plans based on DPC, DSP, GR/FE
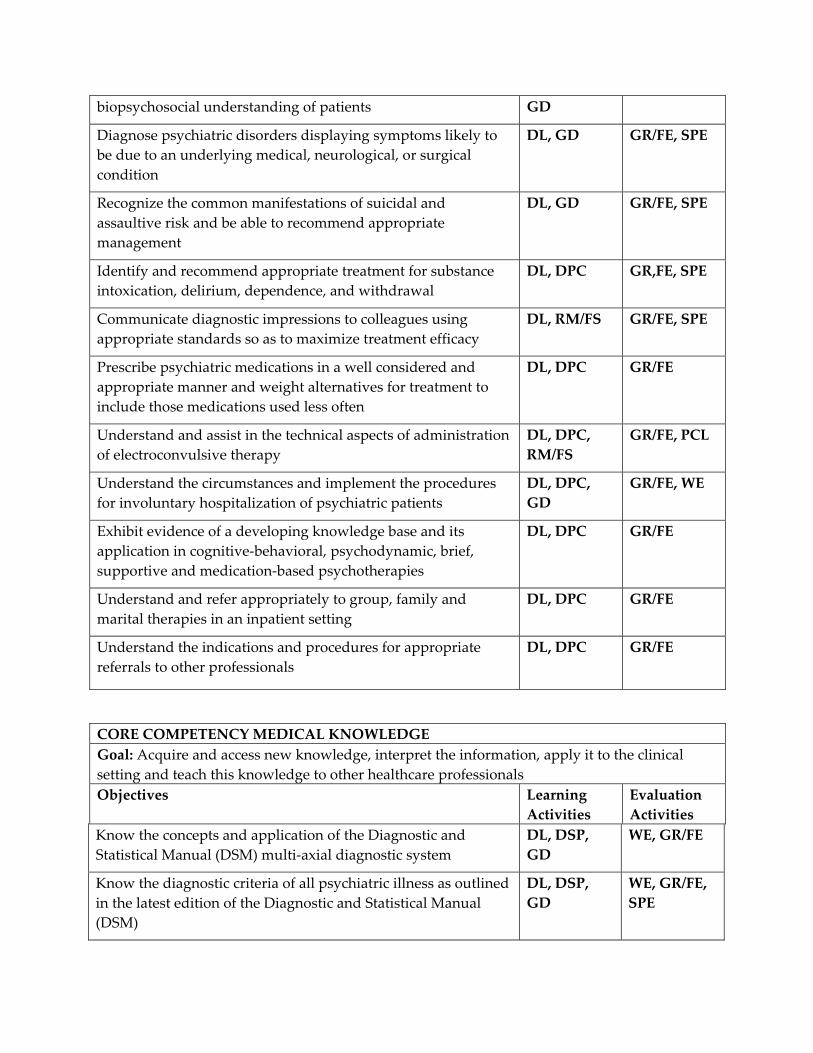
biopsychosocial understanding of patients GD
Diagnose psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL, GD GR/FE, SPE
Recognize the common manifestations of suicidal and assaultive risk and be able to recommend appropriate management
DL, GD GR/FE, SPE
Identify and recommend appropriate treatment for substance intoxication, delirium, dependence, and withdrawal
DL, DPC GR,FE, SPE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe psychiatric medications in a well considered and appropriate manner and weight alternatives for treatment to include those medications used less often
DL, DPC GR/FE
Understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GR/FE, WE
Exhibit evidence of a developing knowledge base and its application in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Understand and refer appropriately to group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionals Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and Statistical Manual (DSM) multi‐axial diagnostic system
DL, DSP, GD
WE, GR/FE
Know the diagnostic criteria of all psychiatric illness as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
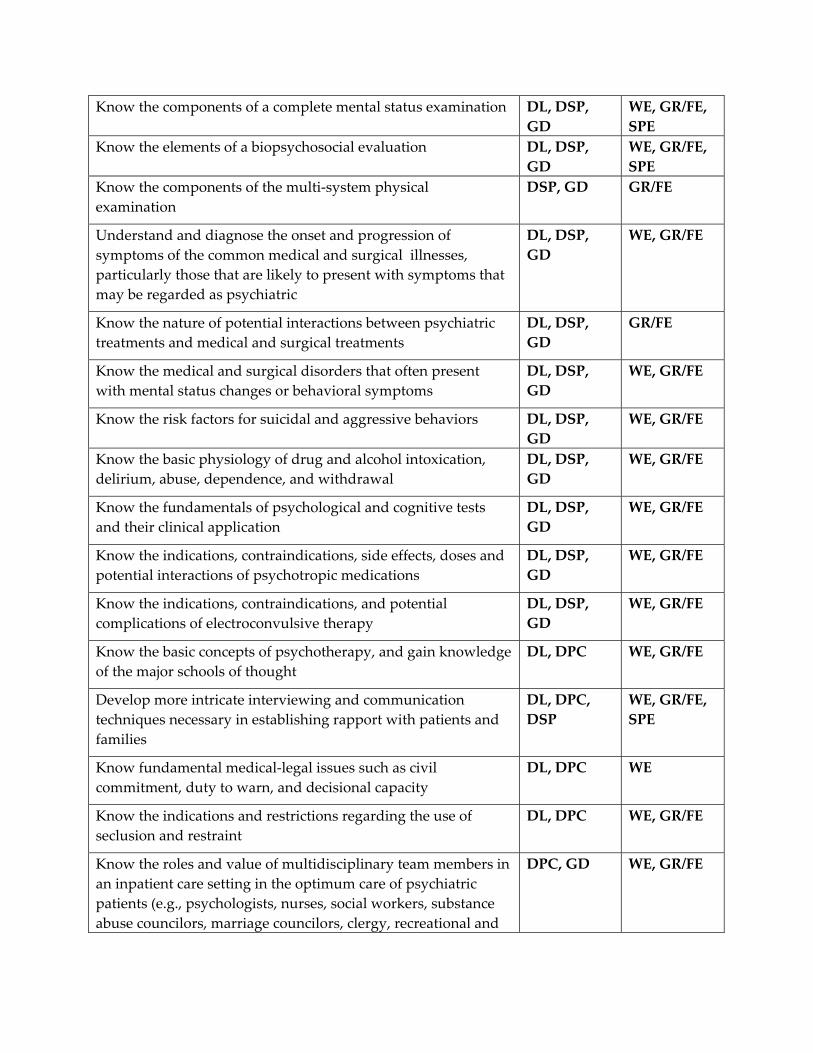
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Understand and diagnose the onset and progression of symptoms of the common medical and surgical illnesses, particularly those that are likely to present with symptoms that may be regarded as psychiatric
DL, DSP, GD
WE, GR/FE
Know the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Know the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Know the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Know the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Develop more intricate interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil commitment, duty to warn, and decisional capacity
DL, DPC WE
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and
DPC, GD WE, GR/FE
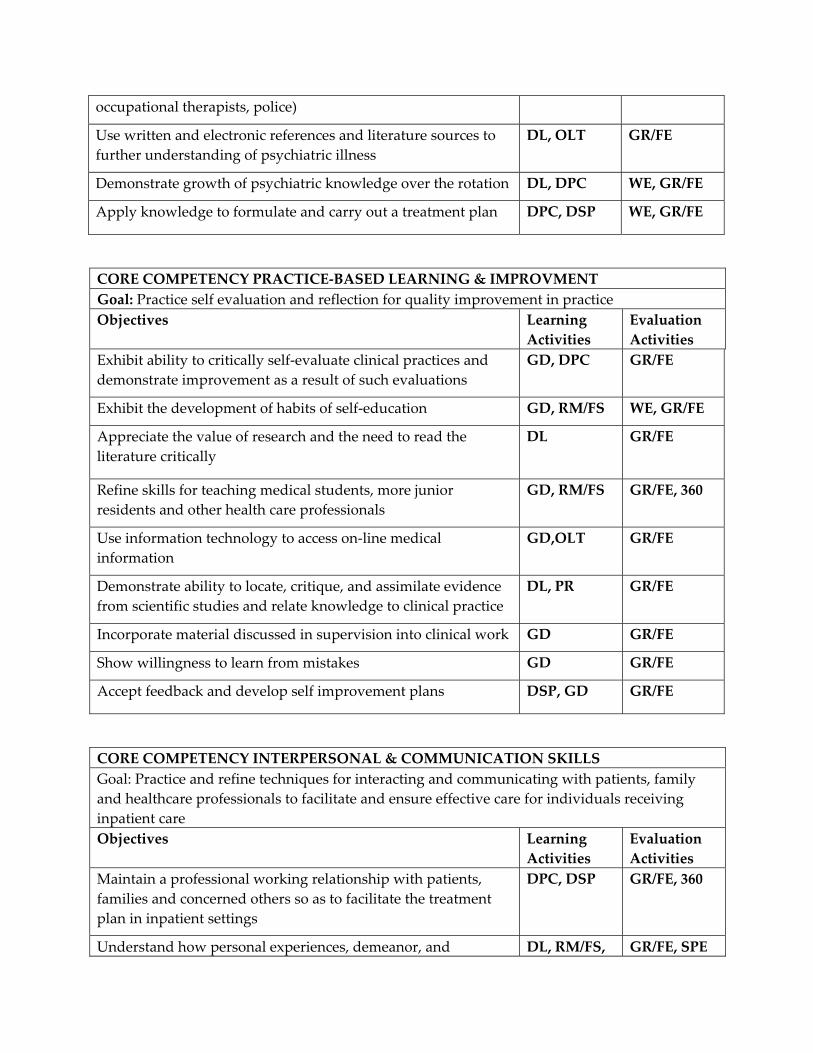
occupational therapists, police)
Use written and electronic references and literature sources to further understanding of psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
Apply knowledge to formulate and carry out a treatment plan DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Exhibit ability to critically self‐evaluate clinical practices and demonstrate improvement as a result of such evaluations
GD, DPC GR/FE
Exhibit the development of habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Refine skills for teaching medical students, more junior residents and other health care professionals
GD, RM/FS GR/FE, 360
Use information technology to access on‐line medical information
GD,OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, PR GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Maintain a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
Understand how personal experiences, demeanor, and DL, RM/FS, GR/FE, SPE
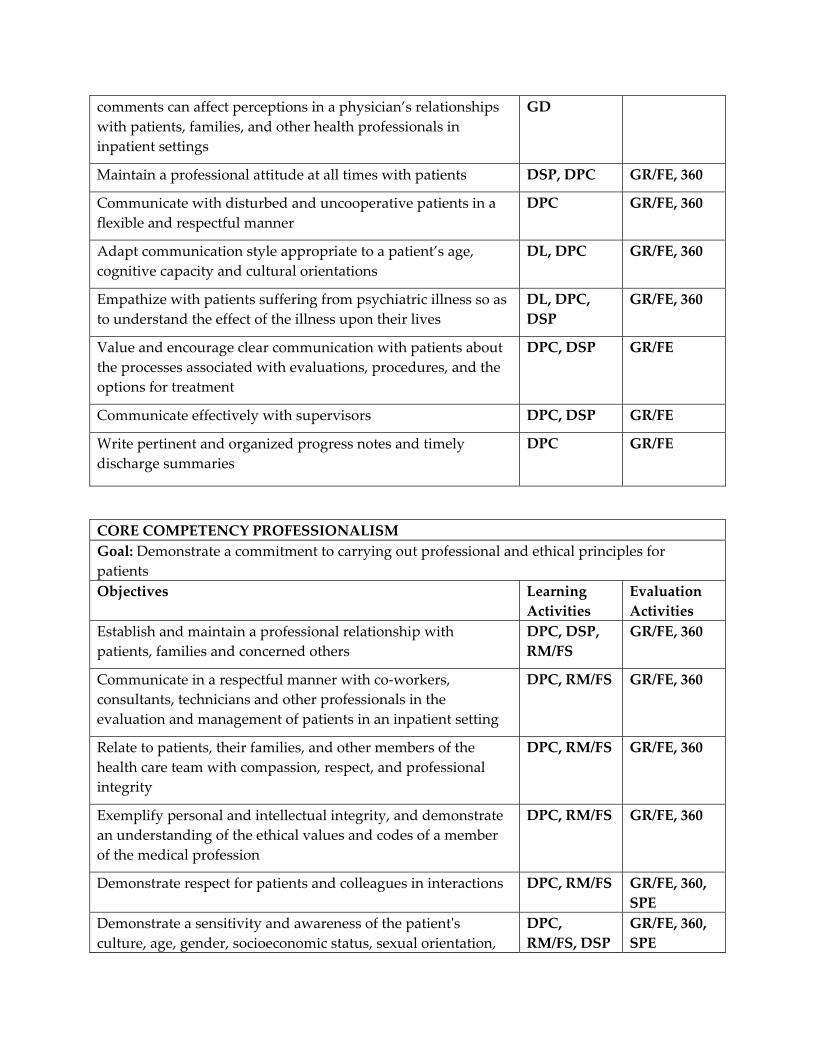
comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
GD
Maintain a professional attitude at all times with patients DSP, DPC GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation,
DPC, RM/FS, DSP
GR/FE, 360, SPE
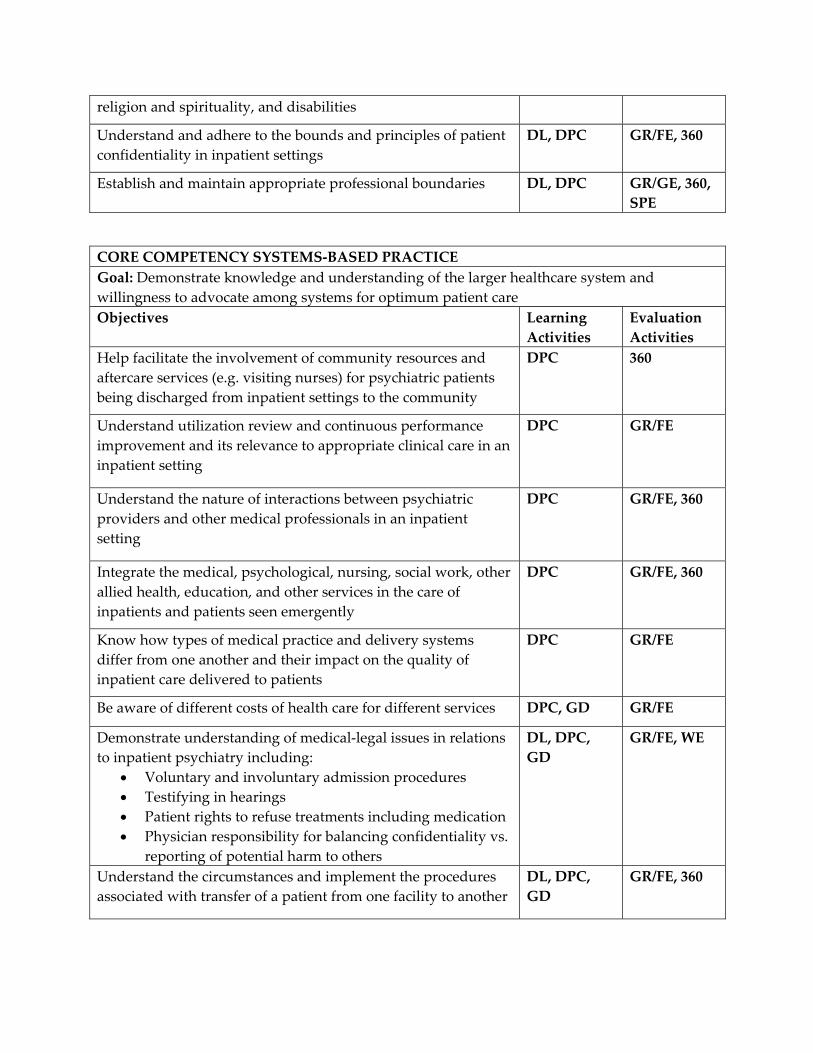
religion and spirituality, and disabilities
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/GE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC 360
Understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Know how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate understanding of medical‐legal issues in relations to inpatient psychiatry including:
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others
DL, DPC, GD
GR/FE, WE
Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360

a. PSYCHIATRY INTENSIVE SUBSTANCE ABUSE TREATMENT PROGRAM b. Required 1 month rotation occurring in the PGY1 or PGY2 year. c. The faculty consists of one full‐time addiction psychiatrist, a full time social worker,
nurse, physicians’ assistant and three substance abuse counselors. d. Residents are expected to evaluate a selected number of new patients, follow them
through their time on the unit, work closely with the treatment team, attend and lead selected group activities, and provide ongoing routine medical care of patients as needed. Residents meet daily with their supervising psychiatrist and members of the multidisciplinary staff to discuss new patients and to establish and monitor treatment plans for each patient. An attending psychiatrist is always available for consultation. Residents also participate in evaluating patients referred to the substance abuse service by other services and are supervised in this by faculty.
e. The demographics of the patient population is 90% male, all age 18 and over, with the majority aged 30‐65. Patients are evenly divided between Caucasian and African‐American. Primary diagnoses are approximately 70% polysubstance abuse (with the majority of patients using cocaine, methamphetamine, alcohol, marihuana, and/or PCP in various combinations) and 30% evenly divided between alcohol or stimulants as the primary or sole drug of abuse). Co‐occurring substance abuse diagnoses occur in 40‐50% of patients with 15% of those patients psychotic, 30% with a non‐psychotic affective and/or anxiety disorder and 15% personality disorders. Treatment modalities include pharmacotherapy, individual and group psycho‐educational therapy and behavioral therapy.
f. An average resident case load is 5‐10 patients on the inpatient service and 2‐5 patient evaluations and follow‐up per week on the substance abuse consult service. Average length on the inpatient service is approximately 21 days.
g. Residents receive ongoing supervision by their attending through individual case review and rounds on a daily basis. Multidisciplinary substance abuse staff supervise individually and through multidisciplinary treatment planning meetings. In addition, residents are required to have two hours of individual supervision per week with their assigned psychiatry supervisor.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: SUBSTANCE ABUSE LEVEL: PGY1 or PGY2 DURATON: 1 MONTH SITES: KCVA SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING ADDICTION PSYCHIATRY ATTENDING AT KANSAS CITY VAMC By completion of the psychiatric residency program, residents are expected to demonstrate
competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
The knowledge, skills, and attitudes to be acquired during the substance abuse rotation in order to demonstrate progress toward achievement of these competencies are:
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination
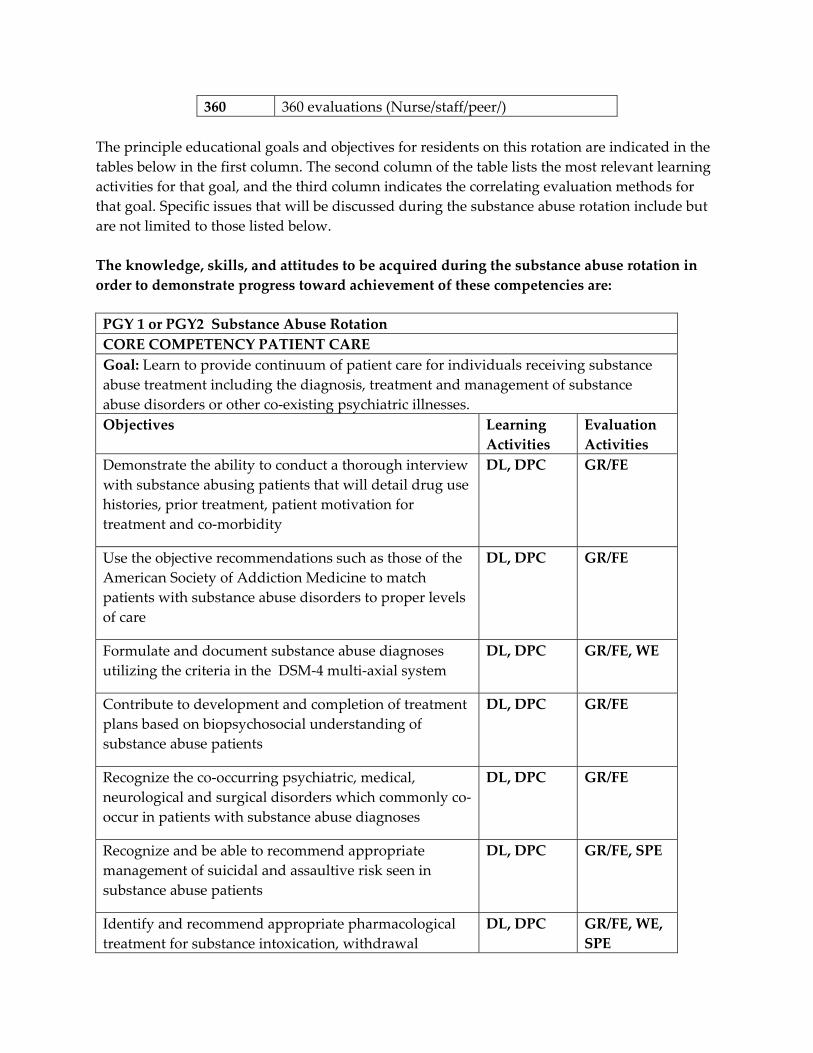
360 360 evaluations (Nurse/staff/peer/) The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed during the substance abuse rotation include but are not limited to those listed below. The knowledge, skills, and attitudes to be acquired during the substance abuse rotation in order to demonstrate progress toward achievement of these competencies are:
PGY 1 or PGY2 Substance Abuse Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide continuum of patient care for individuals receiving substance abuse treatment including the diagnosis, treatment and management of substance abuse disorders or other co‐existing psychiatric illnesses.Objectives Learning
Activities Evaluation Activities
Demonstrate the ability to conduct a thorough interview with substance abusing patients that will detail drug use histories, prior treatment, patient motivation for treatment and co‐morbidity
DL, DPC GR/FE
Use the objective recommendations such as those of the American Society of Addiction Medicine to match patients with substance abuse disorders to proper levels of care
DL, DPC GR/FE
Formulate and document substance abuse diagnoses utilizing the criteria in the DSM‐4 multi‐axial system
DL, DPC GR/FE, WE
Contribute to development and completion of treatment plans based on biopsychosocial understanding of substance abuse patients
DL, DPC GR/FE
Recognize the co‐occurring psychiatric, medical, neurological and surgical disorders which commonly co‐occur in patients with substance abuse diagnoses
DL, DPC GR/FE
Recognize and be able to recommend appropriate management of suicidal and assaultive risk seen in substance abuse patients
DL, DPC GR/FE, SPE
Identify and recommend appropriate pharmacological treatment for substance intoxication, withdrawal
DL, DPC GR/FE, WE, SPE
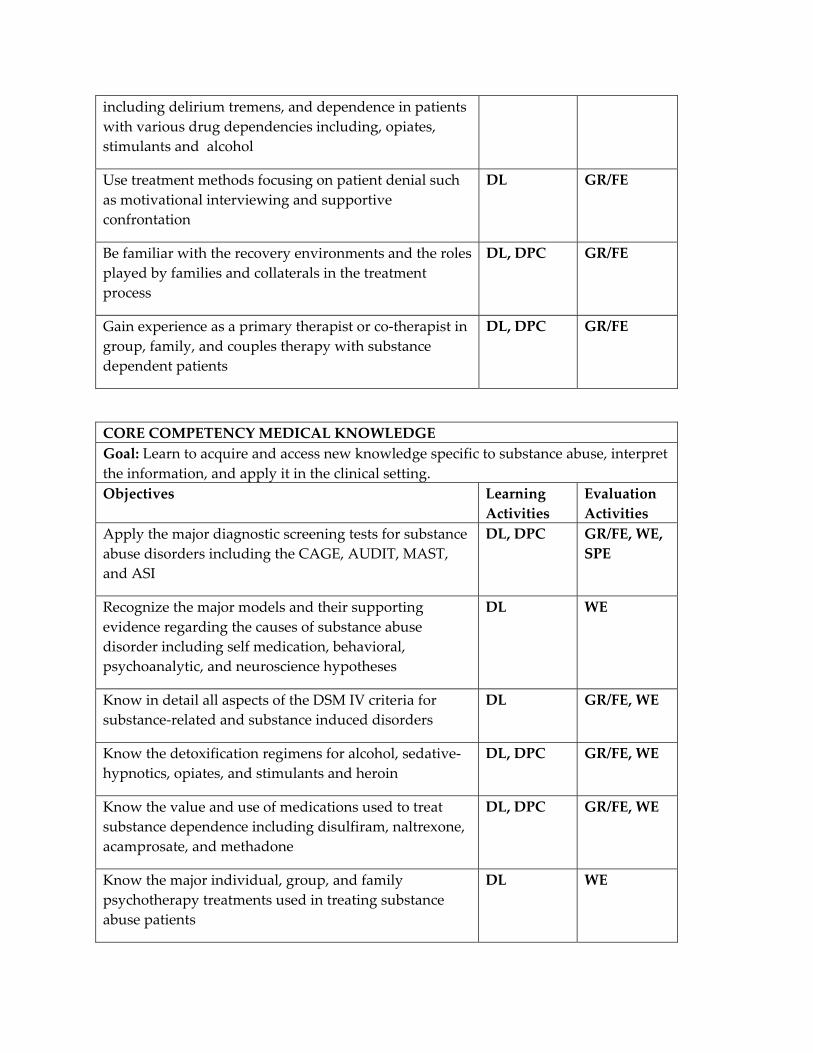
including delirium tremens, and dependence in patients with various drug dependencies including, opiates, stimulants and alcohol
Use treatment methods focusing on patient denial such as motivational interviewing and supportive confrontation
DL GR/FE
Be familiar with the recovery environments and the roles played by families and collaterals in the treatment process
DL, DPC GR/FE
Gain experience as a primary therapist or co‐therapist in group, family, and couples therapy with substance dependent patients
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge specific to substance abuse, interpret the information, and apply it in the clinical setting.Objectives Learning
Activities Evaluation Activities
Apply the major diagnostic screening tests for substance abuse disorders including the CAGE, AUDIT, MAST, and ASI
DL, DPC GR/FE, WE, SPE
Recognize the major models and their supporting evidence regarding the causes of substance abuse disorder including self medication, behavioral, psychoanalytic, and neuroscience hypotheses
DL WE
Know in detail all aspects of the DSM IV criteria for substance‐related and substance induced disorders
DL GR/FE, WE
Know the detoxification regimens for alcohol, sedative‐hypnotics, opiates, and stimulants and heroin
DL, DPC GR/FE, WE
Know the value and use of medications used to treat substance dependence including disulfiram, naltrexone, acamprosate, and methadone
DL, DPC GR/FE, WE
Know the major individual, group, and family psychotherapy treatments used in treating substance abuse patients
DL WE
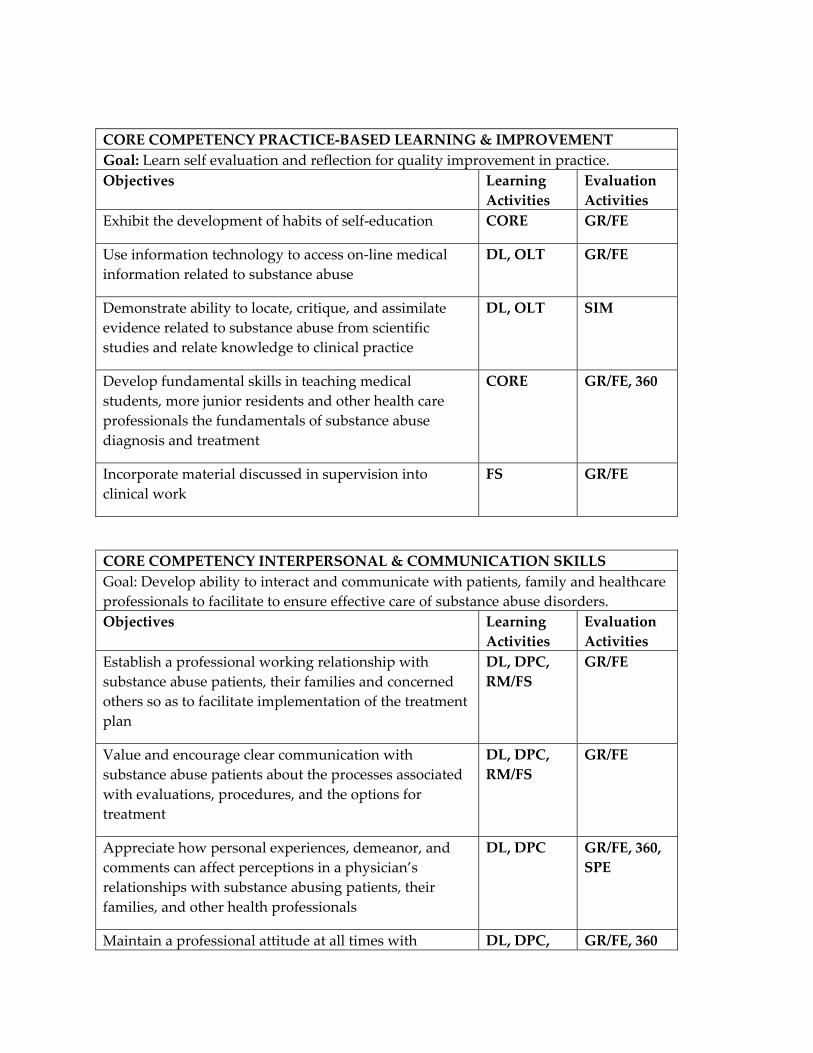
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Learn self evaluation and reflection for quality improvement in practice. Objectives Learning
Activities Evaluation Activities
Exhibit the development of habits of self‐education CORE GR/FE
Use information technology to access on‐line medical information related to substance abuse
DL, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence related to substance abuse from scientific studies and relate knowledge to clinical practice
DL, OLT SIM
Develop fundamental skills in teaching medical students, more junior residents and other health care professionals the fundamentals of substance abuse diagnosis and treatment
CORE GR/FE, 360
Incorporate material discussed in supervision into clinical work
FS GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate to ensure effective care of substance abuse disorders. Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with substance abuse patients, their families and concerned others so as to facilitate implementation of the treatment plan
DL, DPC, RM/FS
GR/FE
Value and encourage clear communication with substance abuse patients about the processes associated with evaluations, procedures, and the options for treatment
DL, DPC, RM/FS
GR/FE
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with substance abusing patients, their families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times with DL, DPC, GR/FE, 360
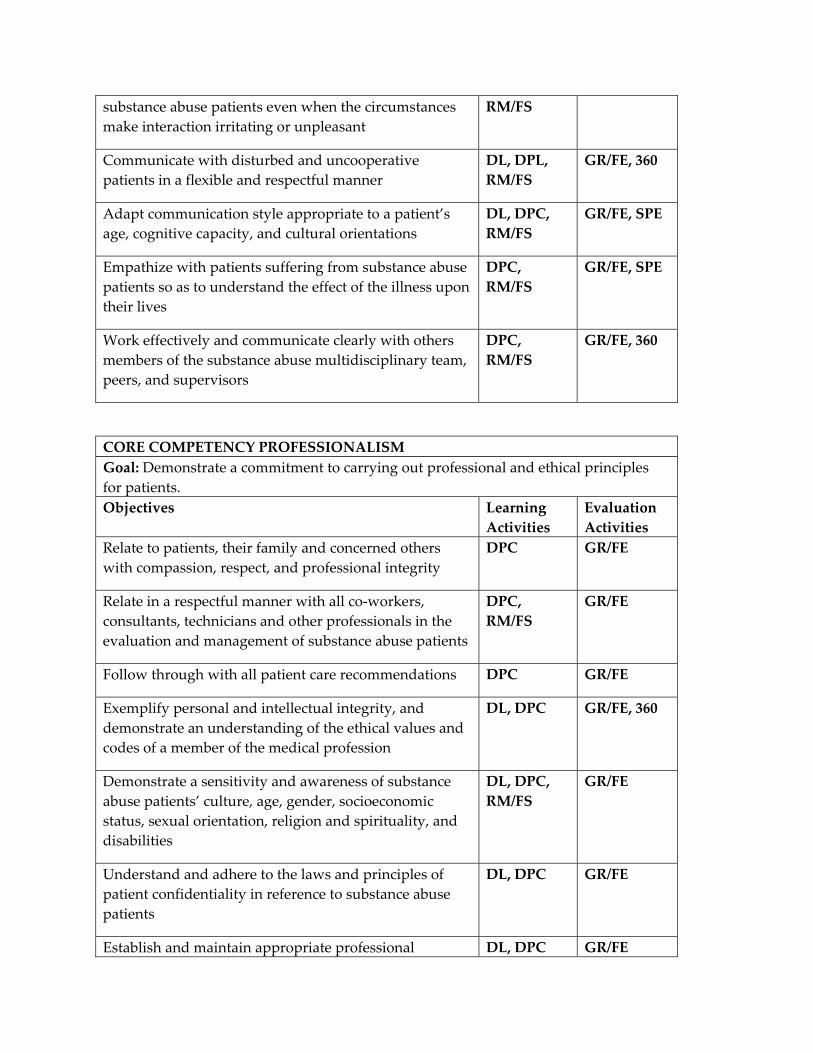
substance abuse patients even when the circumstances make interaction irritating or unpleasant
RM/FS
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DL, DPL, RM/FS
GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Empathize with patients suffering from substance abuse patients so as to understand the effect of the illness upon their lives
DPC, RM/FS
GR/FE, SPE
Work effectively and communicate clearly with others members of the substance abuse multidisciplinary team, peers, and supervisors
DPC, RM/FS
GR/FE, 360
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients. Objectives Learning
Activities Evaluation Activities
Relate to patients, their family and concerned others with compassion, respect, and professional integrity
DPC GR/FE
Relate in a respectful manner with all co‐workers, consultants, technicians and other professionals in the evaluation and management of substance abuse patients
DPC, RM/FS
GR/FE
Follow through with all patient care recommendations DPC GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DL, DPC GR/FE, 360
Demonstrate a sensitivity and awareness of substance abuse patients’ culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DL, DPC, RM/FS
GR/FE
Understand and adhere to the laws and principles of patient confidentiality in reference to substance abuse patients
DL, DPC GR/FE
Establish and maintain appropriate professional DL, DPC GR/FE
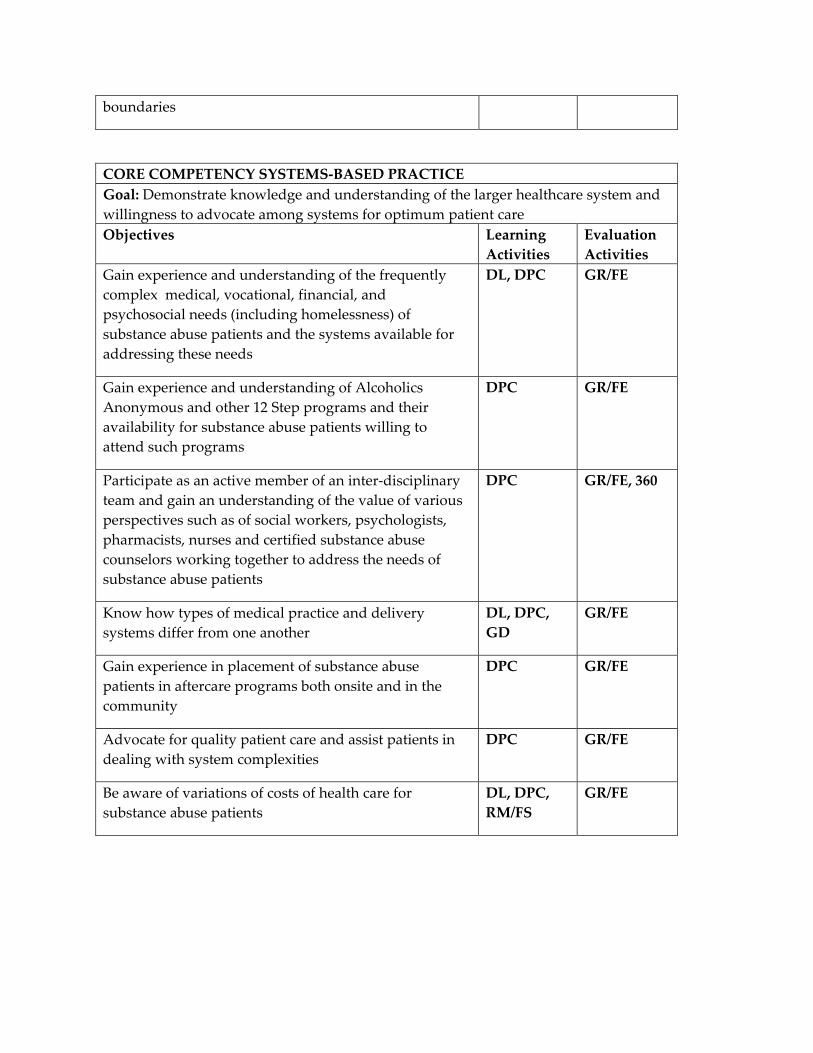
boundaries
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Gain experience and understanding of the frequently complex medical, vocational, financial, and psychosocial needs (including homelessness) of substance abuse patients and the systems available for addressing these needs
DL, DPC GR/FE
Gain experience and understanding of Alcoholics Anonymous and other 12 Step programs and their availability for substance abuse patients willing to attend such programs
DPC GR/FE
Participate as an active member of an inter‐disciplinary team and gain an understanding of the value of various perspectives such as of social workers, psychologists, pharmacists, nurses and certified substance abuse counselors working together to address the needs of substance abuse patients
DPC GR/FE, 360
Know how types of medical practice and delivery systems differ from one another
DL, DPC, GD
GR/FE
Gain experience in placement of substance abuse patients in aftercare programs both onsite and in the community
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC GR/FE
Be aware of variations of costs of health care for substance abuse patients
DL, DPC, RM/FS
GR/FE
a. PSYCHIATRY ADULT OUTPATIENT SERVICE b. Required continuous half‐time 6 month rotation occurring in the PGY3 year. c. Faculty consists of two full‐time psychiatrists, one 7/8 time, three 1/2 time and one
3/8 time psychiatrist, 2.5 psychiatric social workers and two psychologists. d. Residents spend 1.5 hours a week in formal didactic or interviewing skill conferences
and attend ½ day of didactic programming at KUMC during this rotation in addition to attendance at grand rounds 2 hours weekly. In addition, residents regularly discuss with faculty treatment planning for new patients and continuing management of outpatient case load.
e. Patient diagnoses cover the spectrum of adult psychiatric disorders with the greatest concentration in affective disorders, schizophrenia and personality disorders. Co‐occurring substance abuse is commonly associated with these diagnoses. The patient population is 90% male with age ranges from 18‐85 with the majority age 30‐65. Residents spend approximately 40% of their time learning management of new acute cases, 50% following an established case load of patients treated with psychotherapy and/or pharmacotherapy, and 10% in emergency evaluations and crisis management. Optional experience in group therapy of post‐traumatic stress disorders, impulse disorders and chronic pain is available.
f. Residents evaluate approximately 3‐7 new patients per week and follow approximately 25 established patients per week.
g. An attending psychiatrist is always available for consultation and review of patients. In addition, residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision.
h. Outpatient psychiatry at the Kansas City VA‐MC represents an excellent multidisciplinary setting demonstrating efficacy of collaborative care for outpatients and family members. Faculty members have special interests in psychopharmacology, substance abuse, cognitive psychotherapy and PTSD. Residents are also exposed to a clinic where services are organized so that effective and efficient care is provided to a large number of patients.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: SUBSTANCE ABUSE LEVEL: PGY1 or PGY2 DURATON: 1 MONTH SITES: KCVA SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING ADDICTION PSYCHIATRY ATTENDING AT KANSAS CITY VAMC By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
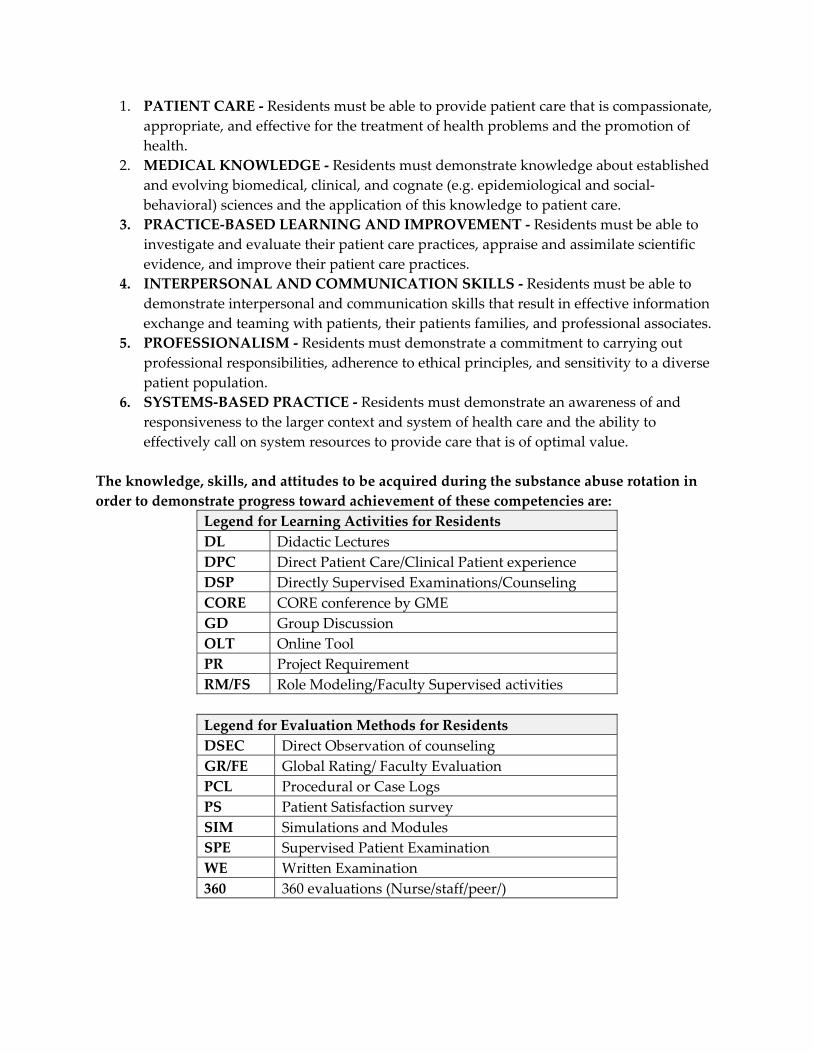
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
The knowledge, skills, and attitudes to be acquired during the substance abuse rotation in order to demonstrate progress toward achievement of these competencies are:
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
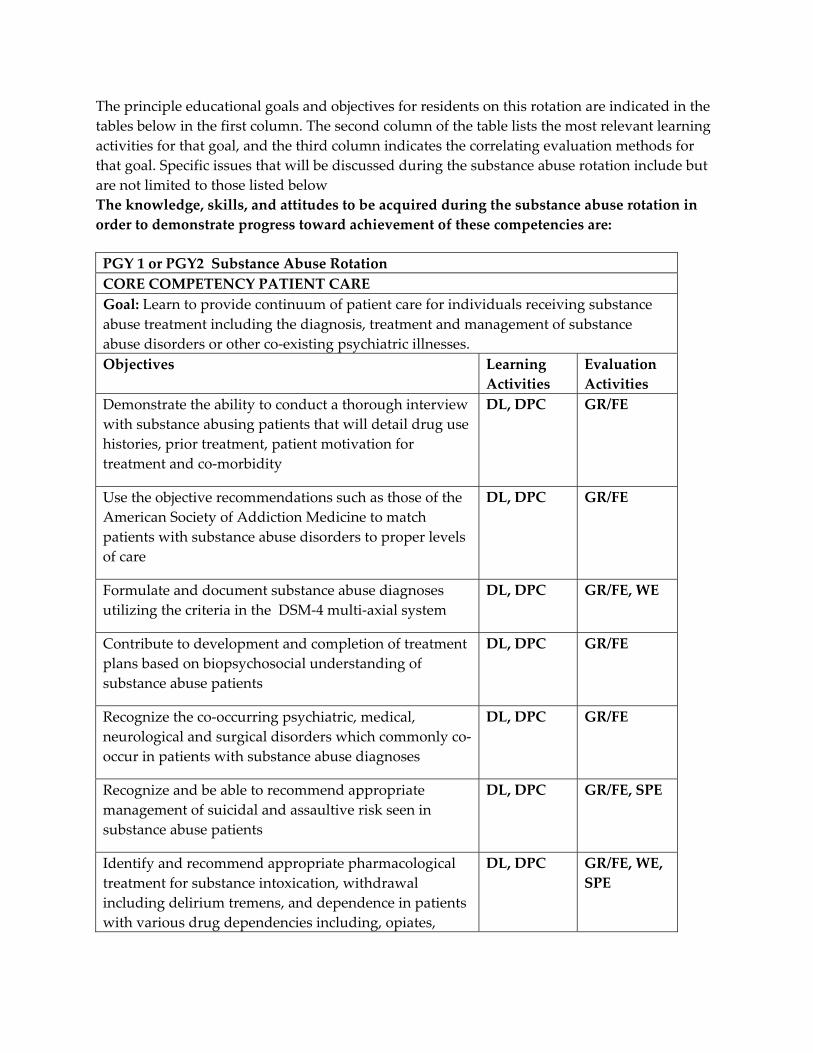
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed during the substance abuse rotation include but are not limited to those listed below The knowledge, skills, and attitudes to be acquired during the substance abuse rotation in order to demonstrate progress toward achievement of these competencies are:
PGY 1 or PGY2 Substance Abuse Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide continuum of patient care for individuals receiving substance abuse treatment including the diagnosis, treatment and management of substance abuse disorders or other co‐existing psychiatric illnesses.Objectives Learning
Activities Evaluation Activities
Demonstrate the ability to conduct a thorough interview with substance abusing patients that will detail drug use histories, prior treatment, patient motivation for treatment and co‐morbidity
DL, DPC GR/FE
Use the objective recommendations such as those of the American Society of Addiction Medicine to match patients with substance abuse disorders to proper levels of care
DL, DPC GR/FE
Formulate and document substance abuse diagnoses utilizing the criteria in the DSM‐4 multi‐axial system
DL, DPC GR/FE, WE
Contribute to development and completion of treatment plans based on biopsychosocial understanding of substance abuse patients
DL, DPC GR/FE
Recognize the co‐occurring psychiatric, medical, neurological and surgical disorders which commonly co‐occur in patients with substance abuse diagnoses
DL, DPC GR/FE
Recognize and be able to recommend appropriate management of suicidal and assaultive risk seen in substance abuse patients
DL, DPC GR/FE, SPE
Identify and recommend appropriate pharmacological treatment for substance intoxication, withdrawal including delirium tremens, and dependence in patients with various drug dependencies including, opiates,
DL, DPC GR/FE, WE, SPE
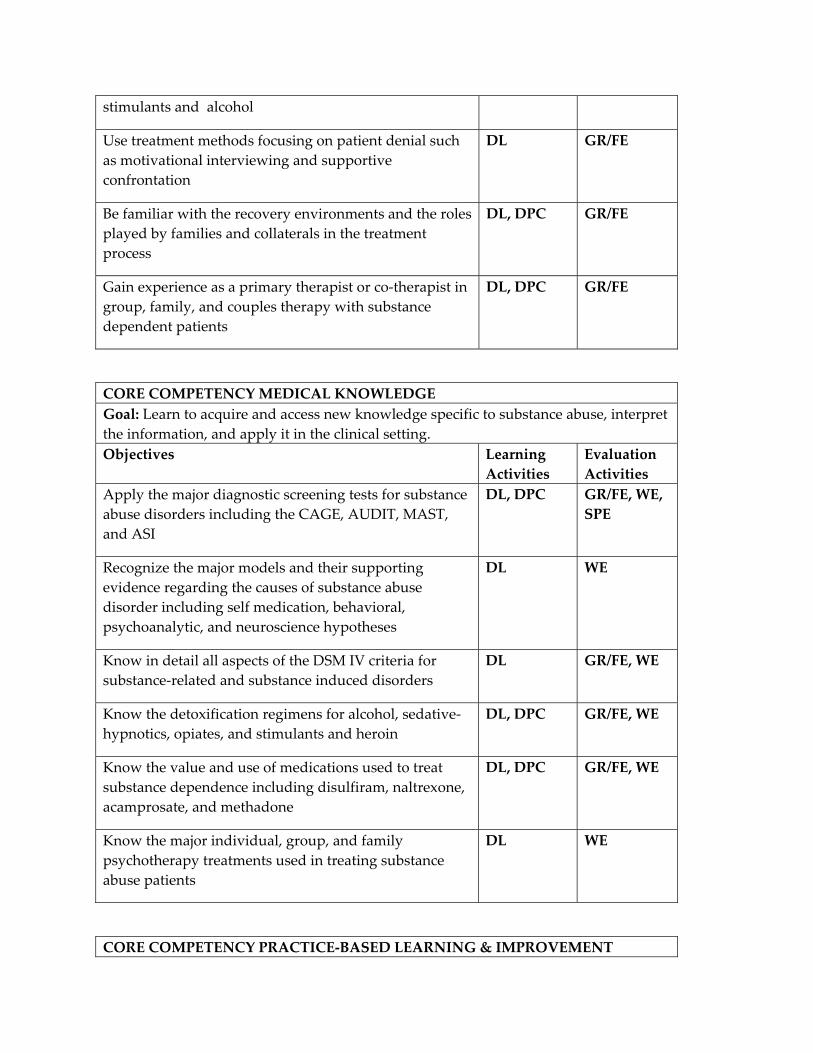
stimulants and alcohol
Use treatment methods focusing on patient denial such as motivational interviewing and supportive confrontation
DL GR/FE
Be familiar with the recovery environments and the roles played by families and collaterals in the treatment process
DL, DPC GR/FE
Gain experience as a primary therapist or co‐therapist in group, family, and couples therapy with substance dependent patients
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge specific to substance abuse, interpret the information, and apply it in the clinical setting.Objectives Learning
Activities Evaluation Activities
Apply the major diagnostic screening tests for substance abuse disorders including the CAGE, AUDIT, MAST, and ASI
DL, DPC GR/FE, WE, SPE
Recognize the major models and their supporting evidence regarding the causes of substance abuse disorder including self medication, behavioral, psychoanalytic, and neuroscience hypotheses
DL WE
Know in detail all aspects of the DSM IV criteria for substance‐related and substance induced disorders
DL GR/FE, WE
Know the detoxification regimens for alcohol, sedative‐hypnotics, opiates, and stimulants and heroin
DL, DPC GR/FE, WE
Know the value and use of medications used to treat substance dependence including disulfiram, naltrexone, acamprosate, and methadone
DL, DPC GR/FE, WE
Know the major individual, group, and family psychotherapy treatments used in treating substance abuse patients
DL WE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT
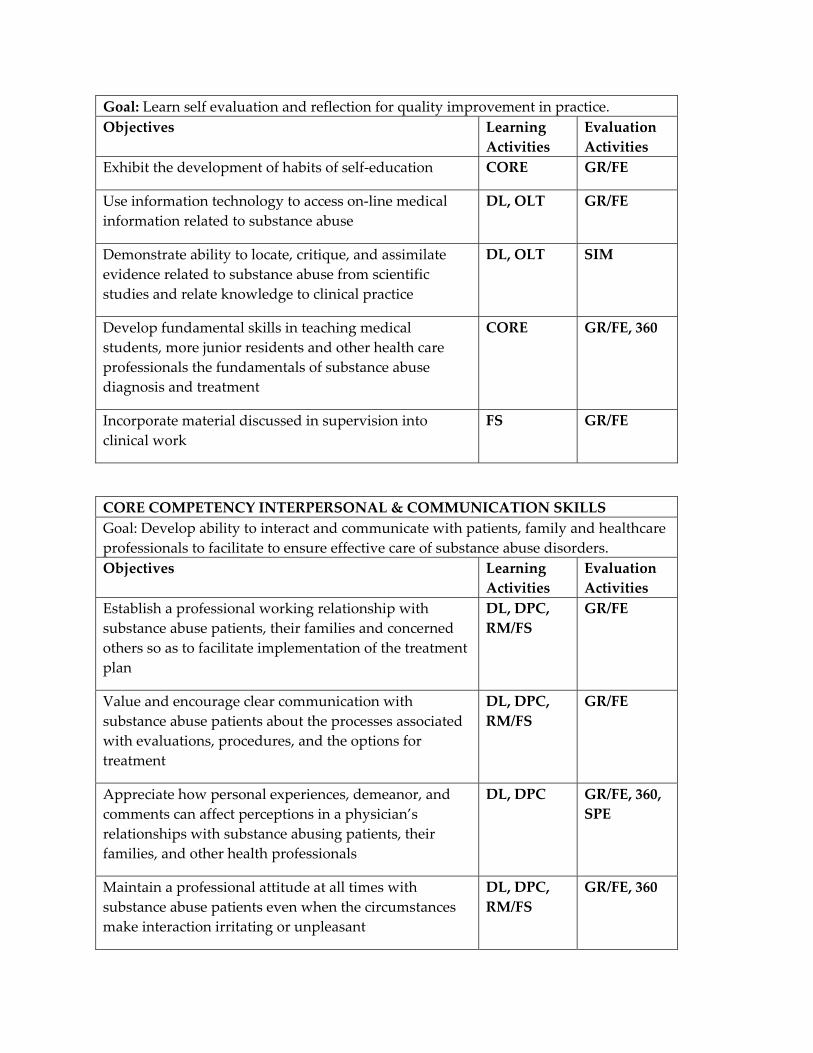
Goal: Learn self evaluation and reflection for quality improvement in practice. Objectives Learning
Activities Evaluation Activities
Exhibit the development of habits of self‐education CORE GR/FE
Use information technology to access on‐line medical information related to substance abuse
DL, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence related to substance abuse from scientific studies and relate knowledge to clinical practice
DL, OLT SIM
Develop fundamental skills in teaching medical students, more junior residents and other health care professionals the fundamentals of substance abuse diagnosis and treatment
CORE GR/FE, 360
Incorporate material discussed in supervision into clinical work
FS GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate to ensure effective care of substance abuse disorders. Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with substance abuse patients, their families and concerned others so as to facilitate implementation of the treatment plan
DL, DPC, RM/FS
GR/FE
Value and encourage clear communication with substance abuse patients about the processes associated with evaluations, procedures, and the options for treatment
DL, DPC, RM/FS
GR/FE
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with substance abusing patients, their families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times with substance abuse patients even when the circumstances make interaction irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360
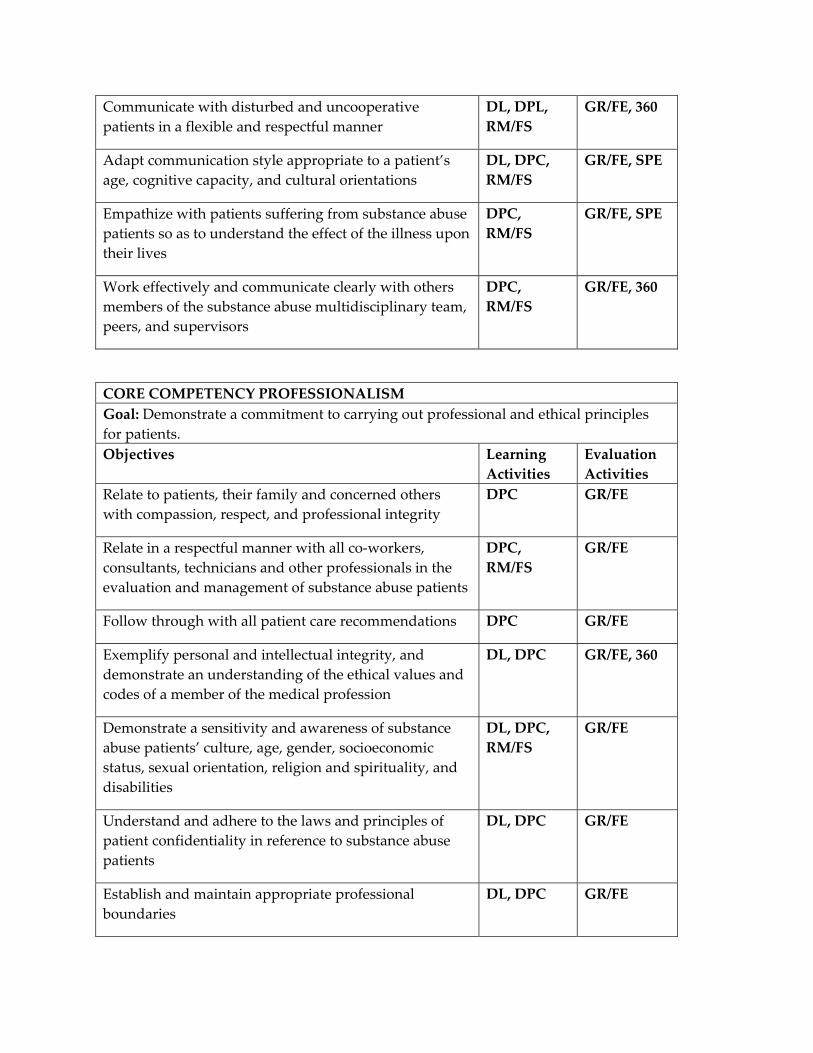
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DL, DPL, RM/FS
GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Empathize with patients suffering from substance abuse patients so as to understand the effect of the illness upon their lives
DPC, RM/FS
GR/FE, SPE
Work effectively and communicate clearly with others members of the substance abuse multidisciplinary team, peers, and supervisors
DPC, RM/FS
GR/FE, 360
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients. Objectives Learning
Activities Evaluation Activities
Relate to patients, their family and concerned others with compassion, respect, and professional integrity
DPC GR/FE
Relate in a respectful manner with all co‐workers, consultants, technicians and other professionals in the evaluation and management of substance abuse patients
DPC, RM/FS
GR/FE
Follow through with all patient care recommendations DPC GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DL, DPC GR/FE, 360
Demonstrate a sensitivity and awareness of substance abuse patients’ culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DL, DPC, RM/FS
GR/FE
Understand and adhere to the laws and principles of patient confidentiality in reference to substance abuse patients
DL, DPC GR/FE
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
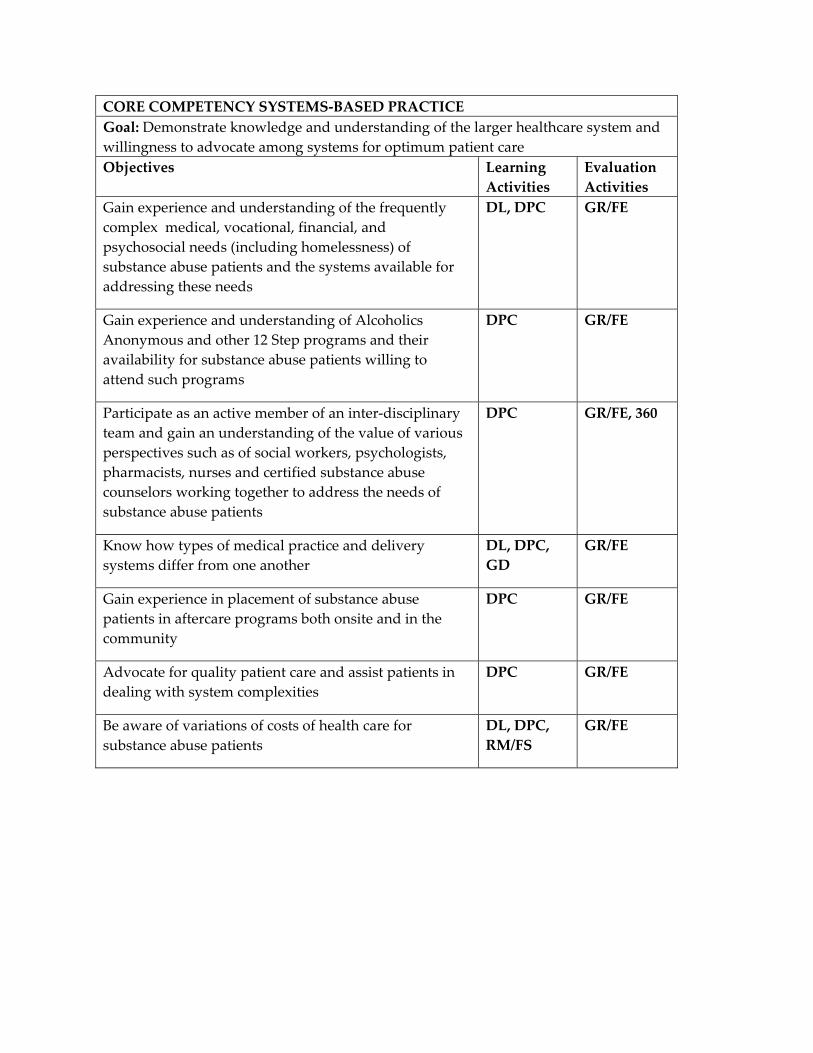
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Gain experience and understanding of the frequently complex medical, vocational, financial, and psychosocial needs (including homelessness) of substance abuse patients and the systems available for addressing these needs
DL, DPC GR/FE
Gain experience and understanding of Alcoholics Anonymous and other 12 Step programs and their availability for substance abuse patients willing to attend such programs
DPC GR/FE
Participate as an active member of an inter‐disciplinary team and gain an understanding of the value of various perspectives such as of social workers, psychologists, pharmacists, nurses and certified substance abuse counselors working together to address the needs of substance abuse patients
DPC GR/FE, 360
Know how types of medical practice and delivery systems differ from one another
DL, DPC, GD
GR/FE
Gain experience in placement of substance abuse patients in aftercare programs both onsite and in the community
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC GR/FE
Be aware of variations of costs of health care for substance abuse patients
DL, DPC, RM/FS
GR/FE
a. PSYCHIATRY CONSULT SERVICE/CHIEF RESIDENT b. A 6 month rotation occurring during the PGY4 year. The resident in this position is
peer‐elected to serve as KCVA Chief Resident. The resident spends 50% of this rotation assigned to the consult service and 50% overseeing junior residents when they are assigned to inpatient services.
c. Faculty consists of 4 full‐time staff psychiatrists assigned to the consult service for varying periods of time. The resident will also have direction from the Chief of Mental Health.
d. The resident sees psychiatric consultations from all services, evaluates the patients and then presents his/her findings to the psychiatry attending and the two decide on a final assessment and recommendations to the requesting team. The Chief Resident oversees the junior residents and medical students assigned to inpatient services.
e. For the consult service, the clinical population is 90% male mainly between 25‐80 years of age, 50% African‐American and 50% Caucasian with a wide variety of psychiatric and medical diagnoses. 25‐40 new consult patients are evaluated per month. For inpatient services, patient diagnoses cover the spectrum of adult psychiatric disorders with the greatest concentration in affective disorders, schizophrenia and personality disorders. Co‐occurring substance abuse is commonly associated with these diagnoses. The patient population is 90% male with age ranges from 18‐85 with the majority age 30‐65.
f. The resident sees 25‐40 new consult patients for evaluation each month. As a part of the Chief Resident responsibilities, the resident oversees the residents assigned to the inpatient psychiatry service. An average case load would be 6‐12 hospitalized patients.
g. For the consult service, supervision occurs daily with the staff psychiatrist regarding specific patients and topics related to consultation and liaison psychiatry. For inpatient services, the Chief Resident meets daily with the staff psychiatrist on a one‐to‐one basis and in addition, interacts with the staff psychiatrist at daily interdisciplinary and weekly multidisciplinary treatment reviews, and at daily ward rounds.
h. This rotation gives the Chief Resident an opportunity to function as a supervising resident, while being supervised by an attending psychiatrist, allowing them to gain experience in this capacity.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: PSYCHIATRY CONSULTS/CHIEF RESIDENT LEVEL: PGY4 DURATON: 6 MONTHS SITES: KANSAS CITY VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT KANSAS CITY VA MEDICAL CENTER
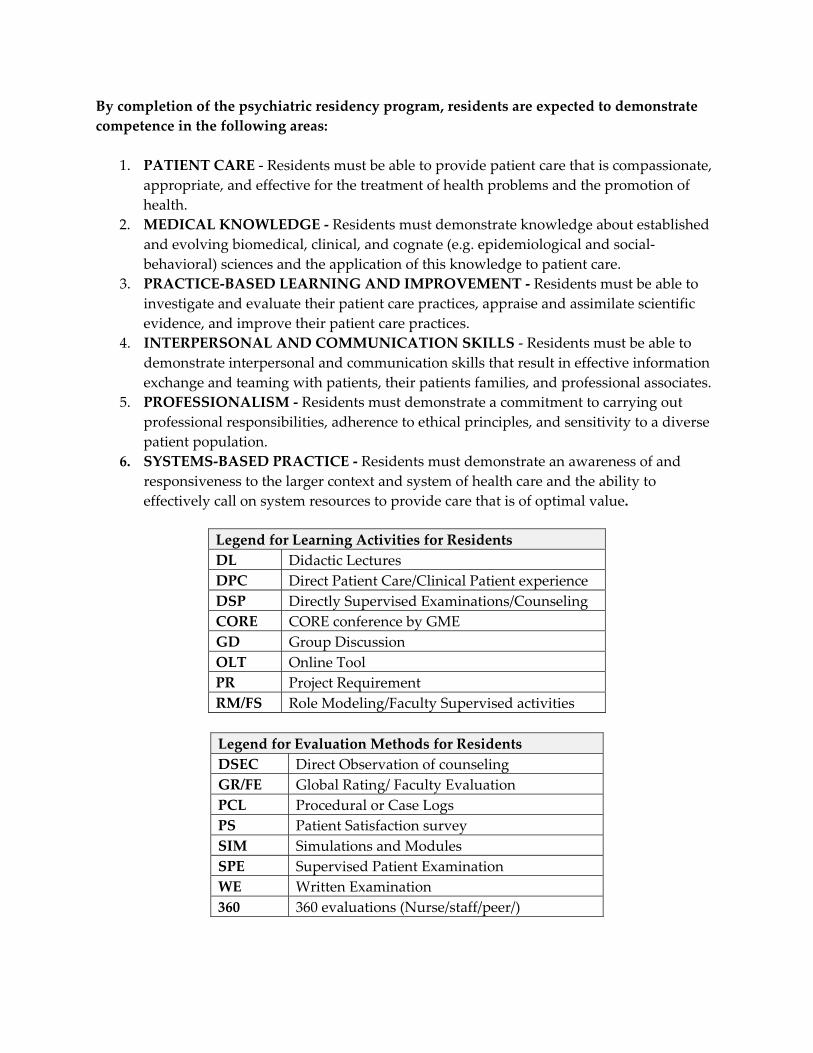
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
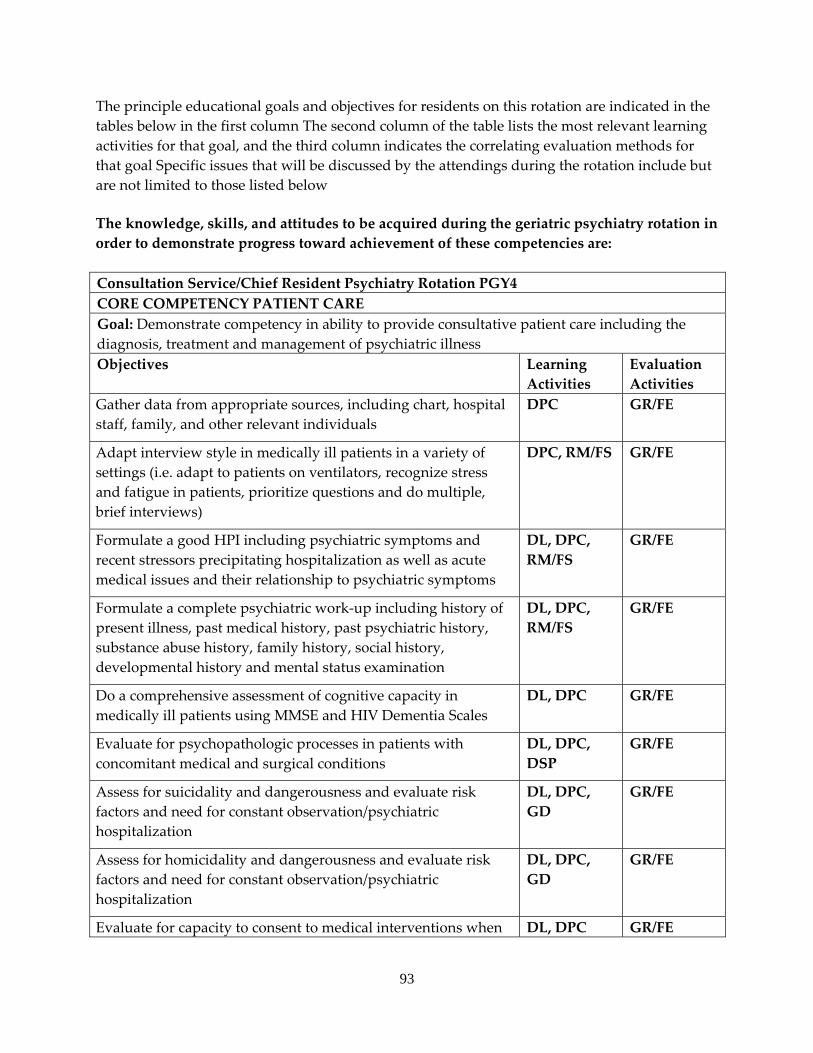
93
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the rotation include but are not limited to those listed below
The knowledge, skills, and attitudes to be acquired during the geriatric psychiatry rotation in order to demonstrate progress toward achievement of these competencies are: Consultation Service/Chief Resident Psychiatry Rotation PGY4 CORE COMPETENCY PATIENT CARE Goal: Demonstrate competency in ability to provide consultative patient care including the diagnosis, treatment and management of psychiatric illnessObjectives Learning
Activities Evaluation Activities
Gather data from appropriate sources, including chart, hospital staff, family, and other relevant individuals
DPC GR/FE
Adapt interview style in medically ill patients in a variety of settings (i.e. adapt to patients on ventilators, recognize stress and fatigue in patients, prioritize questions and do multiple, brief interviews)
DPC, RM/FS GR/FE
Formulate a good HPI including psychiatric symptoms and recent stressors precipitating hospitalization as well as acute medical issues and their relationship to psychiatric symptoms
DL, DPC, RM/FS
GR/FE
Formulate a complete psychiatric work‐up including history of present illness, past medical history, past psychiatric history, substance abuse history, family history, social history, developmental history and mental status examination
DL, DPC, RM/FS
GR/FE
Do a comprehensive assessment of cognitive capacity in medically ill patients using MMSE and HIV Dementia Scales
DL, DPC GR/FE
Evaluate for psychopathologic processes in patients with concomitant medical and surgical conditions
DL, DPC, DSP
GR/FE
Assess for suicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric hospitalization
DL, DPC, GD
GR/FE
Assess for homicidality and dangerousness and evaluate risk factors and need for constant observation/psychiatric hospitalization
DL, DPC, GD
GR/FE
Evaluate for capacity to consent to medical interventions when DL, DPC GR/FE
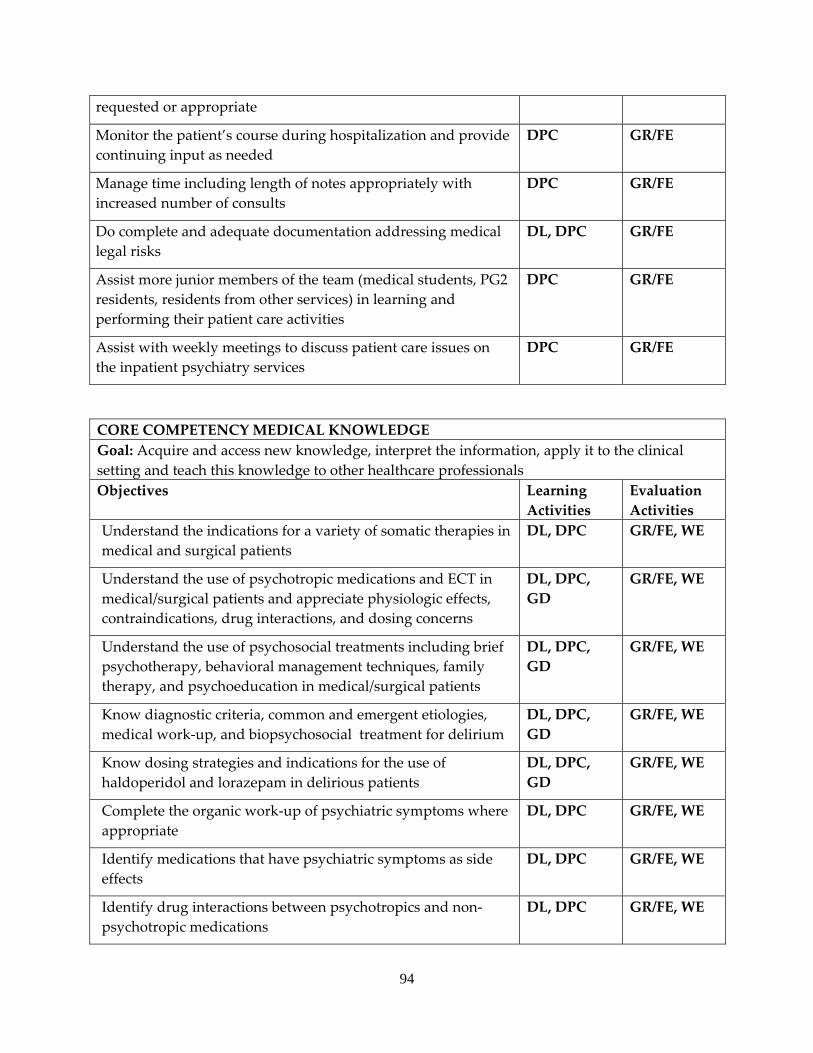
94
requested or appropriate
Monitor the patient’s course during hospitalization and provide continuing input as needed
DPC GR/FE
Manage time including length of notes appropriately with increased number of consults
DPC GR/FE
Do complete and adequate documentation addressing medical legal risks
DL, DPC GR/FE
Assist more junior members of the team (medical students, PG2 residents, residents from other services) in learning and performing their patient care activities
DPC GR/FE
Assist with weekly meetings to discuss patient care issues on the inpatient psychiatry services
DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionalsObjectives Learning
Activities Evaluation Activities
Understand the indications for a variety of somatic therapies in medical and surgical patients
DL, DPC GR/FE, WE
Understand the use of psychotropic medications and ECT in medical/surgical patients and appreciate physiologic effects, contraindications, drug interactions, and dosing concerns
DL, DPC, GD
GR/FE, WE
Understand the use of psychosocial treatments including brief psychotherapy, behavioral management techniques, family therapy, and psychoeducation in medical/surgical patients
DL, DPC, GD
GR/FE, WE
Know diagnostic criteria, common and emergent etiologies, medical work‐up, and biopsychosocial treatment for delirium
DL, DPC, GD
GR/FE, WE
Know dosing strategies and indications for the use of haldoperidol and lorazepam in delirious patients
DL, DPC, GD
GR/FE, WE
Complete the organic work‐up of psychiatric symptoms where appropriate
DL, DPC GR/FE, WE
Identify medications that have psychiatric symptoms as side effects
DL, DPC GR/FE, WE
Identify drug interactions between psychotropics and non‐psychotropic medications
DL, DPC GR/FE, WE
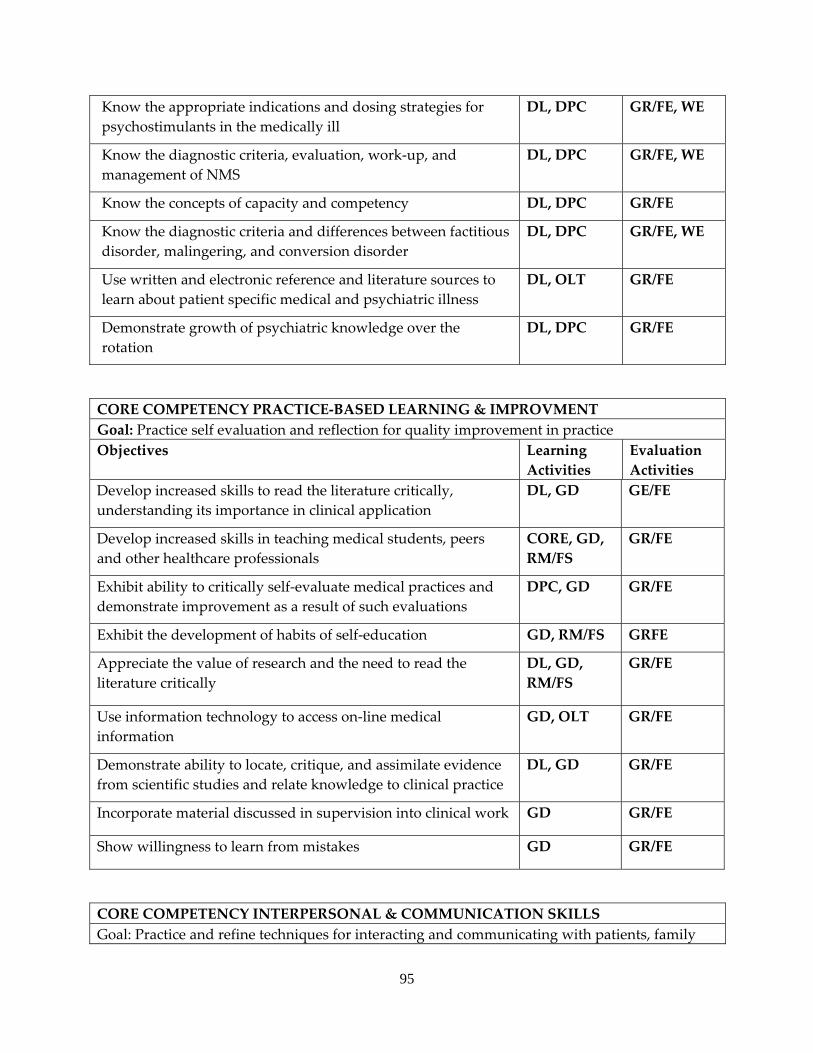
95
Know the appropriate indications and dosing strategies for psychostimulants in the medically ill
DL, DPC GR/FE, WE
Know the diagnostic criteria, evaluation, work‐up, and management of NMS
DL, DPC GR/FE, WE
Know the concepts of capacity and competency DL, DPC GR/FE
Know the diagnostic criteria and differences between factitious disorder, malingering, and conversion disorder
DL, DPC GR/FE, WE
Use written and electronic reference and literature sources to learn about patient specific medical and psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Develop increased skills to read the literature critically, understanding its importance in clinical application
DL, GD GE/FE
Develop increased skills in teaching medical students, peers and other healthcare professionals
CORE, GD, RM/FS
GR/FE
Exhibit ability to critically self‐evaluate medical practices and demonstrate improvement as a result of such evaluations
DPC, GD GR/FE
Exhibit the development of habits of self‐education GD, RM/FS GRFE
Appreciate the value of research and the need to read the literature critically
DL, GD, RM/FS
GR/FE
Use information technology to access on‐line medical information
GD, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, GD GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family
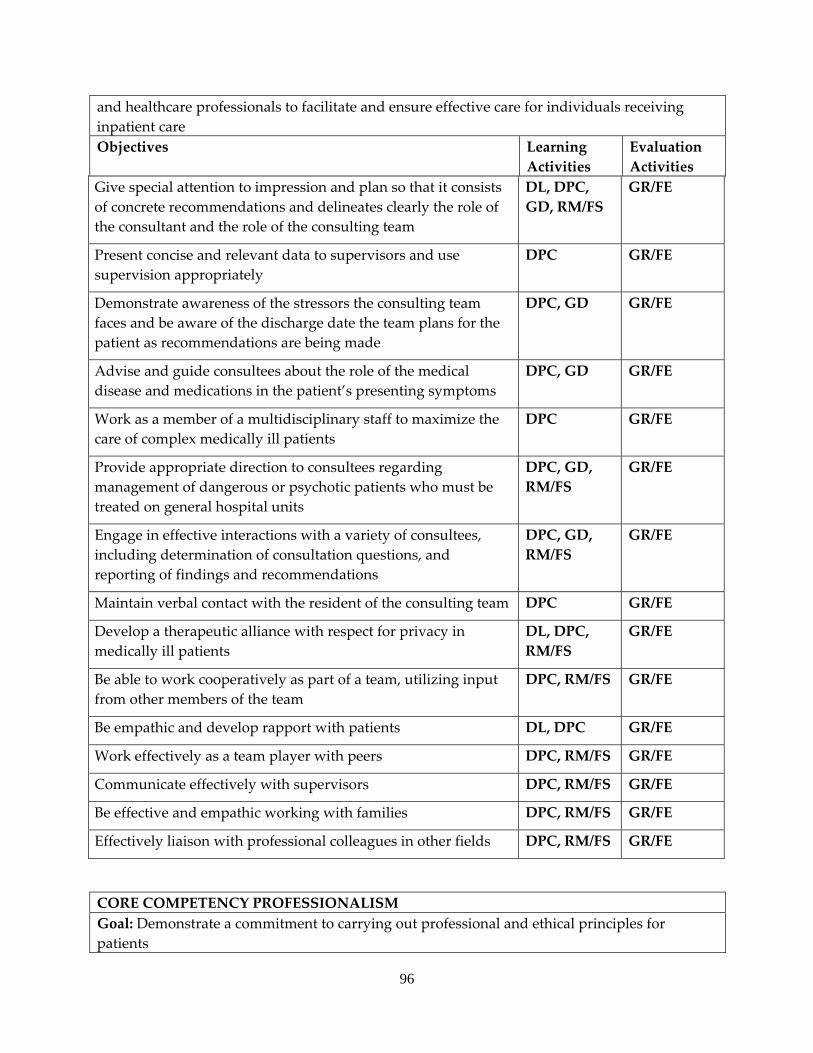
96
and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Give special attention to impression and plan so that it consists of concrete recommendations and delineates clearly the role of the consultant and the role of the consulting team
DL, DPC, GD, RM/FS
GR/FE
Present concise and relevant data to supervisors and use supervision appropriately
DPC GR/FE
Demonstrate awareness of the stressors the consulting team faces and be aware of the discharge date the team plans for the patient as recommendations are being made
DPC, GD GR/FE
Advise and guide consultees about the role of the medical disease and medications in the patient’s presenting symptoms
DPC, GD GR/FE
Work as a member of a multidisciplinary staff to maximize the care of complex medically ill patients
DPC GR/FE
Provide appropriate direction to consultees regarding management of dangerous or psychotic patients who must be treated on general hospital units
DPC, GD, RM/FS
GR/FE
Engage in effective interactions with a variety of consultees, including determination of consultation questions, and reporting of findings and recommendations
DPC, GD, RM/FS
GR/FE
Maintain verbal contact with the resident of the consulting team DPC GR/FE
Develop a therapeutic alliance with respect for privacy in medically ill patients
DL, DPC, RM/FS
GR/FE
Be able to work cooperatively as part of a team, utilizing input from other members of the team
DPC, RM/FS GR/FE
Be empathic and develop rapport with patients DL, DPC GR/FE
Work effectively as a team player with peers DPC, RM/FS GR/FE
Communicate effectively with supervisors DPC, RM/FS GR/FE
Be effective and empathic working with families DPC, RM/FS GR/FE
Effectively liaison with professional colleagues in other fields DPC, RM/FS GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients
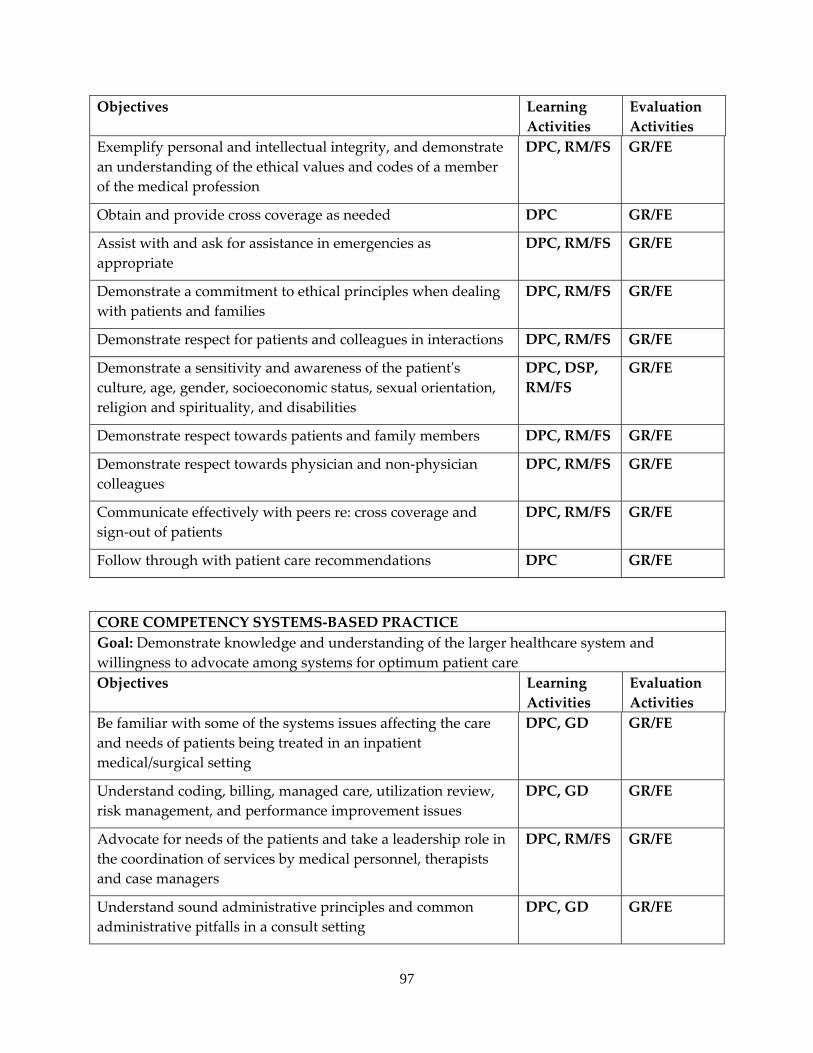
97
Objectives Learning Activities
Evaluation Activities
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Obtain and provide cross coverage as needed DPC GR/FE
Assist with and ask for assistance in emergencies as appropriate
DPC, RM/FS GR/FE
Demonstrate a commitment to ethical principles when dealing with patients and families
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE
Demonstrate respect towards patients and family members DPC, RM/FS GR/FE
Demonstrate respect towards physician and non‐physician colleagues
DPC, RM/FS GR/FE
Communicate effectively with peers re: cross coverage and sign‐out of patients
DPC, RM/FS GR/FE
Follow through with patient care recommendations DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Be familiar with some of the systems issues affecting the care and needs of patients being treated in an inpatient medical/surgical setting
DPC, GD GR/FE
Understand coding, billing, managed care, utilization review, risk management, and performance improvement issues
DPC, GD GR/FE
Advocate for needs of the patients and take a leadership role in the coordination of services by medical personnel, therapists and case managers
DPC, RM/FS GR/FE
Understand sound administrative principles and common administrative pitfalls in a consult setting
DPC, GD GR/FE
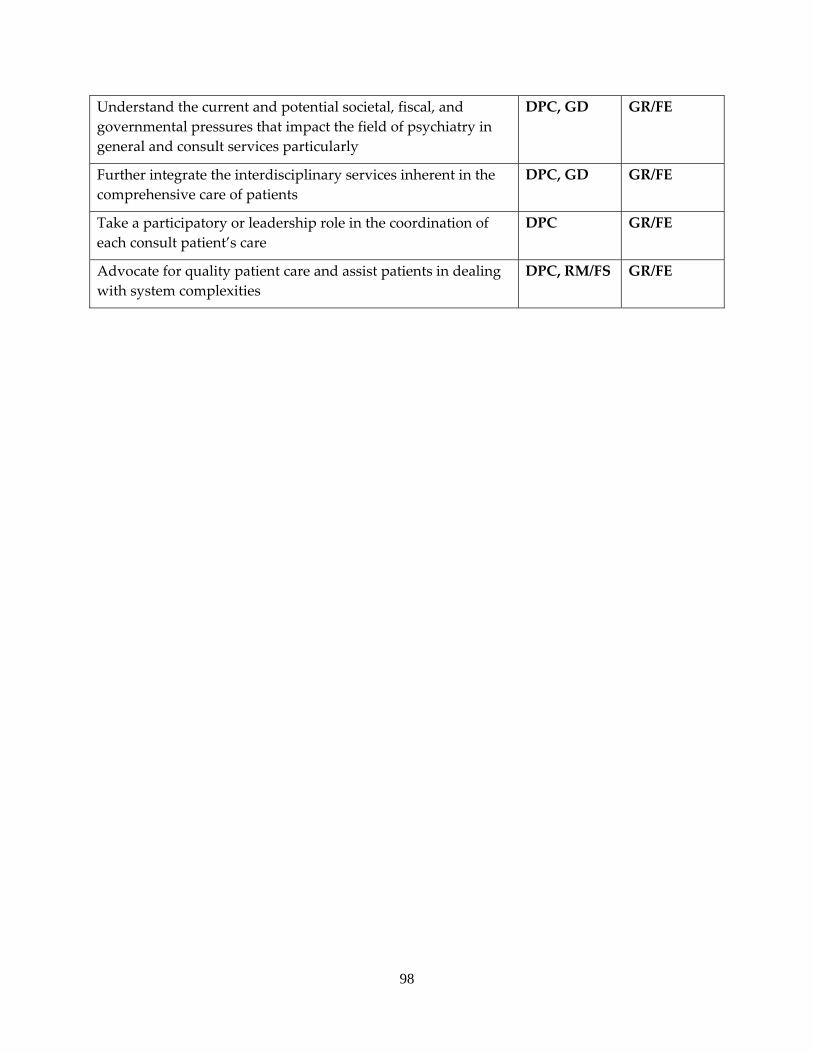
98
Understand the current and potential societal, fiscal, and governmental pressures that impact the field of psychiatry in general and consult services particularly
DPC, GD GR/FE
Further integrate the interdisciplinary services inherent in the comprehensive care of patients
DPC, GD GR/FE
Take a participatory or leadership role in the coordination of each consult patient’s care
DPC GR/FE
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
99
a. INTERNAL MEDICINE SERVICE b. A required 2 month rotation during the PGY1 year as part of the 4 month primary
care medicine block. c. A different full time faculty internist and senior supervising internal medicine
resident is assigned to the service every 4 weeks. d. Residents attend 12 hours of case conferences and didactic presentations weekly (six
days per week); attend daily morning conference; and meet daily with attending staff for consultation regarding patient management.
e. Patients come from rural, urban, and inner city areas and the population is male‐prevalent at this site. However, there is an increasing broad range of ages and more females as younger veterans enter the VA patient panel. This tertiary referral center manages the entire range of medical diagnoses. Residents care for inpatients with more common constellations of medical illness, such as diabetes, CAD, COPD and HTN.
f. An average case load consists of 5‐8 patients per intern. g. Residents receive daily close supervision by the attending staff physician and
continuous supervision by a senior internal medicine resident. Consultation is available at all times.
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: INTERNAL MEDICINE LEVEL: PGY1 DURATON: 4 MONTHS SITE: KANSAS CITY VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING INTERNAL MEDICINE ATTENDING AT KANSAS CITY VA MEDICAL CENTER
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
13. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
14. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
15. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
16. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
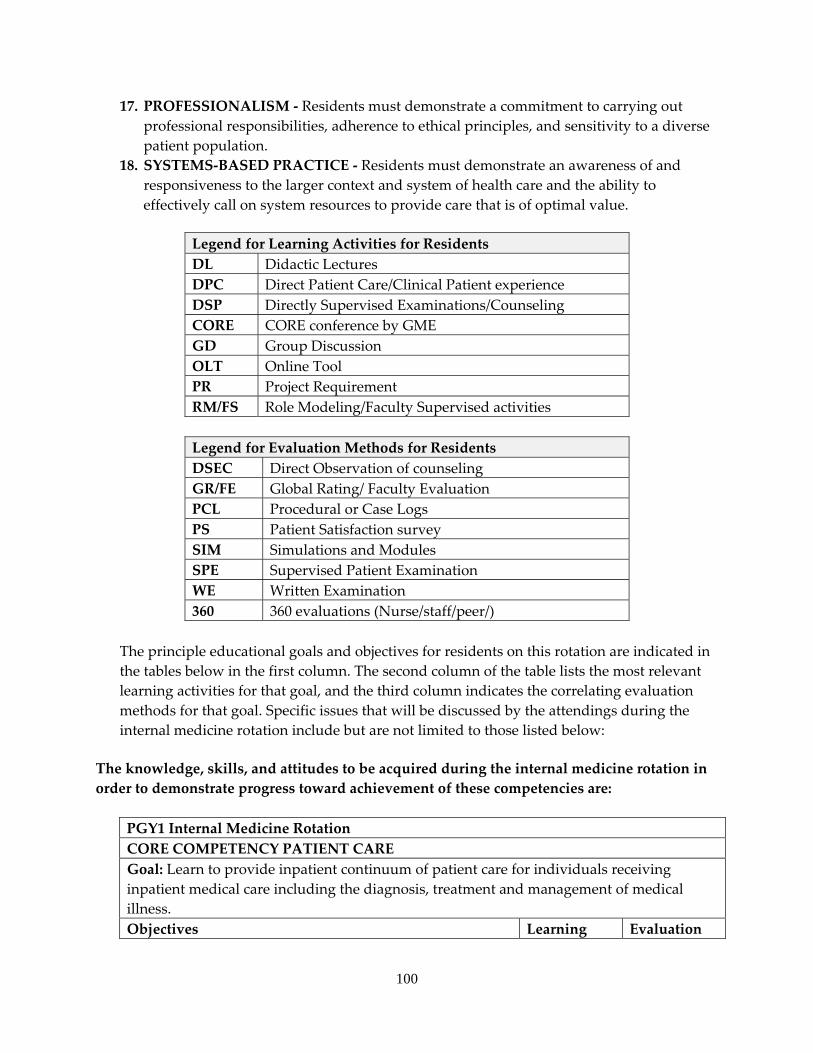
100
17. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
18. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the internal medicine rotation include but are not limited to those listed below:
The knowledge, skills, and attitudes to be acquired during the internal medicine rotation in order to demonstrate progress toward achievement of these competencies are:
PGY1 Internal Medicine Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving inpatient medical care including the diagnosis, treatment and management of medical illness. Objectives Learning Evaluation
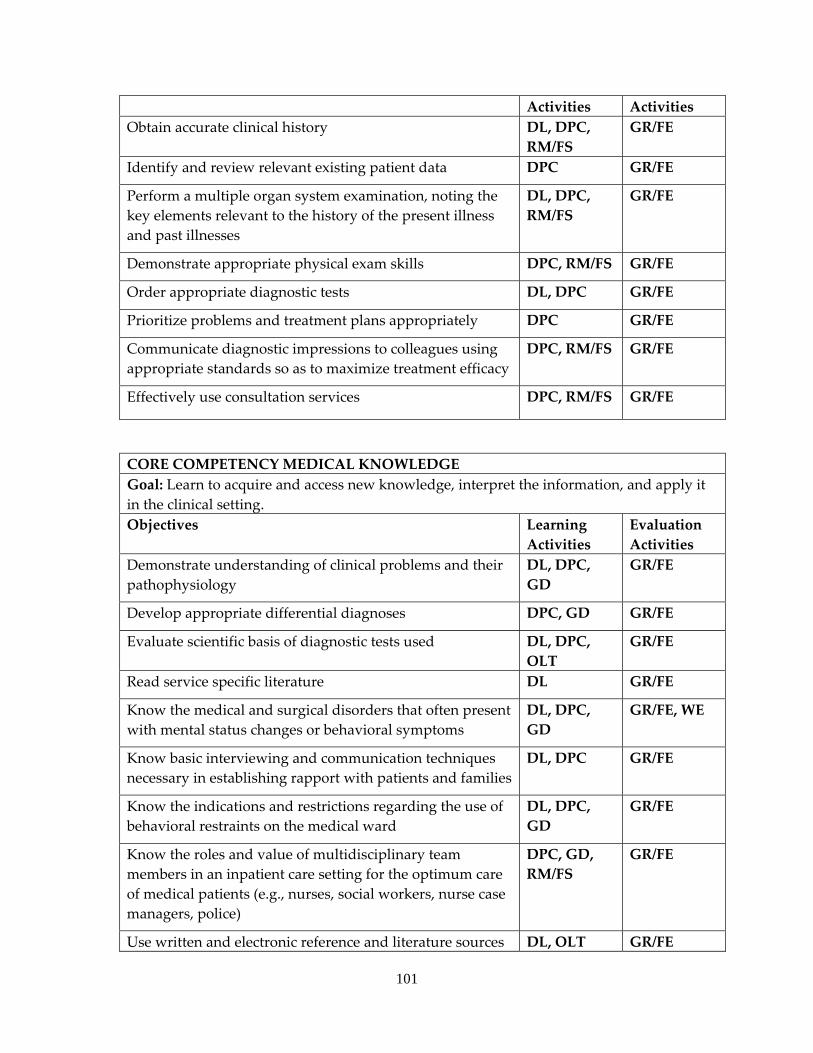
101
Activities Activities Obtain accurate clinical history DL, DPC,
RM/FS GR/FE
Identify and review relevant existing patient data DPC GR/FE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, RM/FS
GR/FE
Demonstrate appropriate physical exam skills DPC, RM/FS GR/FE
Order appropriate diagnostic tests DL, DPC GR/FE
Prioritize problems and treatment plans appropriately DPC GR/FE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DPC, RM/FS GR/FE
Effectively use consultation services DPC, RM/FS GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting. Objectives Learning
Activities Evaluation Activities
Demonstrate understanding of clinical problems and their pathophysiology
DL, DPC, GD
GR/FE
Develop appropriate differential diagnoses DPC, GD GR/FE
Evaluate scientific basis of diagnostic tests used DL, DPC, OLT
GR/FE
Read service specific literature DL GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DPC, GD
GR/FE, WE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC GR/FE
Know the indications and restrictions regarding the use of behavioral restraints on the medical ward
DL, DPC, GD
GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting for the optimum care of medical patients (e.g., nurses, social workers, nurse case managers, police)
DPC, GD, RM/FS
GR/FE
Use written and electronic reference and literature sources DL, OLT GR/FE
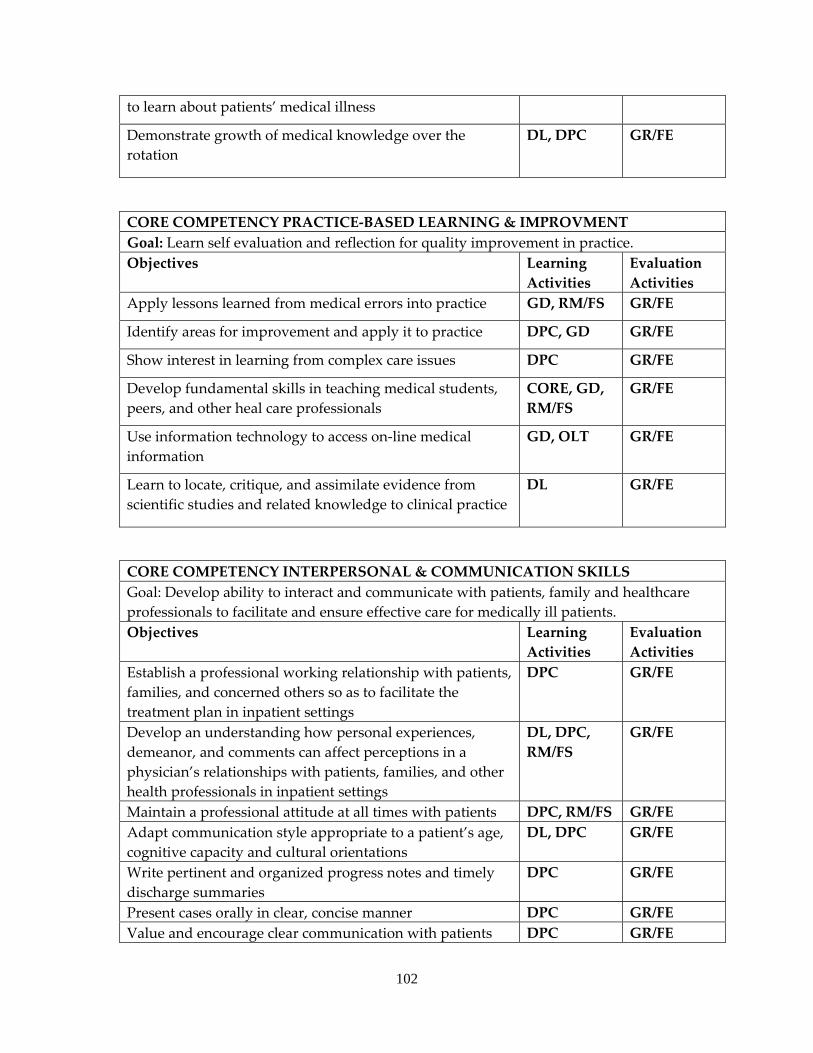
102
to learn about patients’ medical illness
Demonstrate growth of medical knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice. Objectives Learning
Activities Evaluation Activities
Apply lessons learned from medical errors into practice GD, RM/FS GR/FE
Identify areas for improvement and apply it to practice DPC, GD GR/FE
Show interest in learning from complex care issues DPC GR/FE
Develop fundamental skills in teaching medical students, peers, and other heal care professionals
CORE, GD, RM/FS
GR/FE
Use information technology to access on‐line medical information
GD, OLT GR/FE
Learn to locate, critique, and assimilate evidence from scientific studies and related knowledge to clinical practice
DL GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for medically ill patients. Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families, and concerned others so as to facilitate the treatment plan in inpatient settings
DPC GR/FE
Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, DPC, RM/FS
GR/FE
Maintain a professional attitude at all times with patients DPC, RM/FS GR/FE Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
Present cases orally in clear, concise manner DPC GR/FE Value and encourage clear communication with patients DPC GR/FE
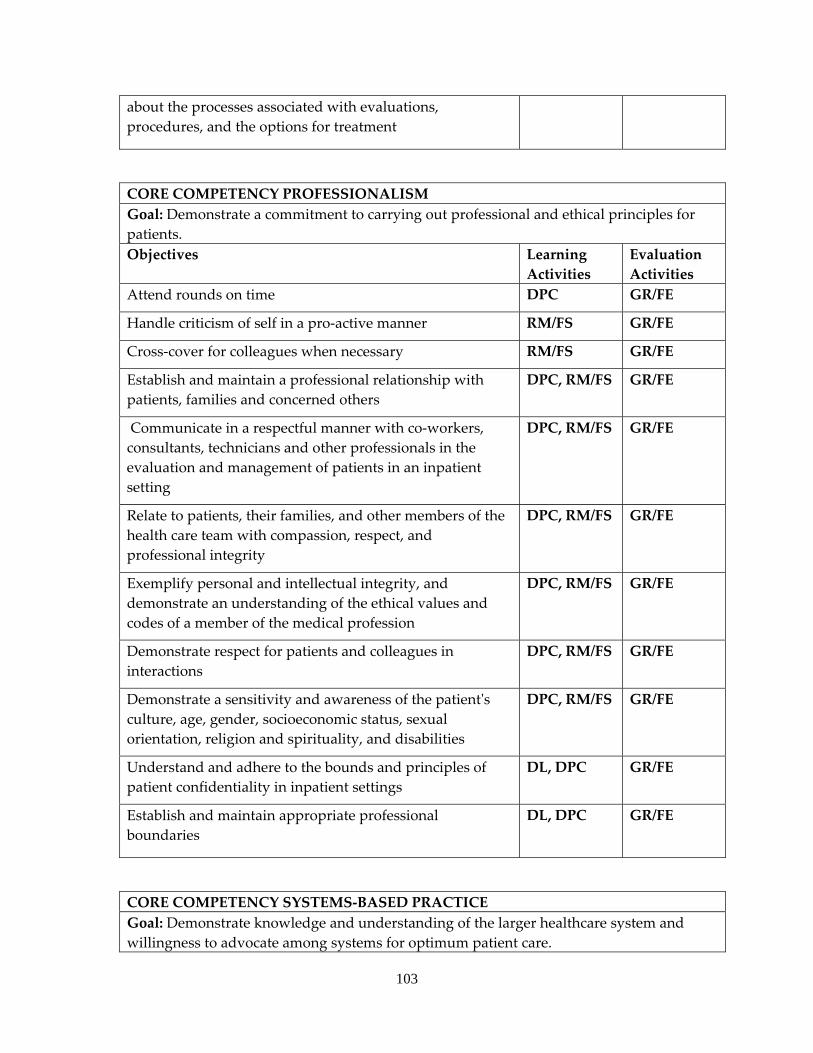
103
about the processes associated with evaluations, procedures, and the options for treatment
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients. Objectives Learning
Activities Evaluation Activities
Attend rounds on time DPC GR/FE
Handle criticism of self in a pro‐active manner RM/FS GR/FE
Cross‐cover for colleagues when necessary RM/FS GR/FE
Establish and maintain a professional relationship with patients, families and concerned others
DPC, RM/FS GR/FE
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions
DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS GR/FE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care.
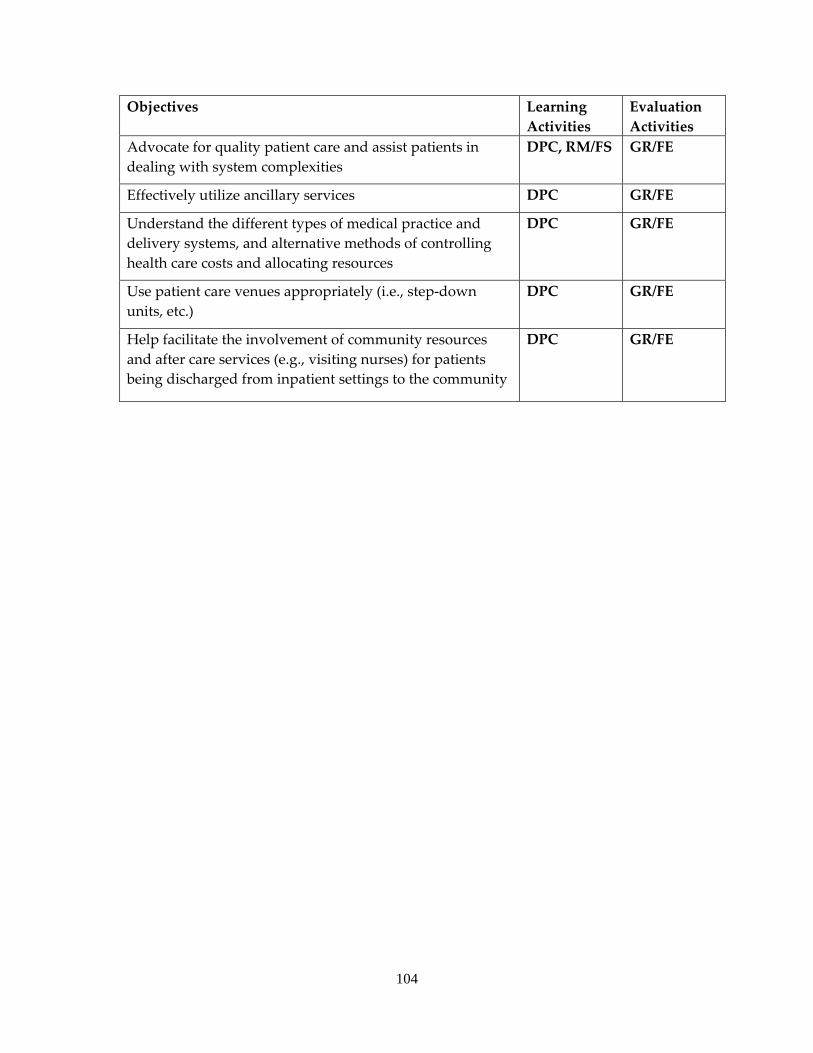
104
Objectives Learning Activities
Evaluation Activities
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
Effectively utilize ancillary services DPC GR/FE
Understand the different types of medical practice and delivery systems, and alternative methods of controlling health care costs and allocating resources
DPC GR/FE
Use patient care venues appropriately (i.e., step‐down units, etc.)
DPC GR/FE
Help facilitate the involvement of community resources and after care services (e.g., visiting nurses) for patients being discharged from inpatient settings to the community
DPC GR/FE
105
DWIGHT D. EISENHOWER VETERANS ADMINISTRATION MEDICAL CENTER
a. NEUROLOGY SERVICE b. Faculty consists of one full‐time neurologist and two part‐time neurologists. c. Residents spend approximately 5‐7 hours per week in Neurology case conferences,
seminars, didactic lecturers, and Journal Club activity. In addition to supervision on the inpatient service, residents spend three half‐days per week in the General Neurology and Movement Disorder clinic, one half day in resident consult clinic. Residents also see Neurology consults under supervision. All residents attend the Psychiatry Core Didactic Series at KUMC one half‐day per week, as well as weekly Grand Rounds at KUMC.
d. The Neurology section patient population is 99% male and 1% female. Ninety‐one percent are Caucasian, 8% African‐American, and 1% other ethnic categories. The age range is 18‐90+ years of age with average ages between 60 and 70 years. The most frequent diagnoses are headache, cerebral artery occlusion, generalized convulsive epilepsy, senile dementia of the Alzheimer’s Type, transient ischemic attack, Parkinson’s Disease, and essential and other specified forms of tremor.
e. The patient caseload in Neurology is 6 outpatients in the General Neurology Clinic, 2 patients in the Movement Disorder Clinic and 1‐ 2 patient in the Neurology consult clinic. They may carry 1‐2 inpatients on a rare occasion.
f. All residents have a minimum of one hour of supervision by faculty daily, as well as case supervision during their outpatient experience.
g. The Neurology rotation provides good exposure to common neurological problems. The Movement Disorder Clinic gives experience to specific neurological diseases. The residents are also exposed to basic EEG interpretations and EMG nerve conduction studies. They have the opportunity to interact closely with Neurology residents and internal medicine residents.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: NEUROLOGY LEVEL: PGY1 or PGY2 DURATON: 1‐2 MONTHS SITE: DWIGHT D. EISENHOWER VA MEDICAL DENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING NEUROLOGY ATTENDING AT DWIGHT D. EISENHOWER VA MEDICAL CENTER By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
106
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the neurology rotation include but are not limited to those listed below:
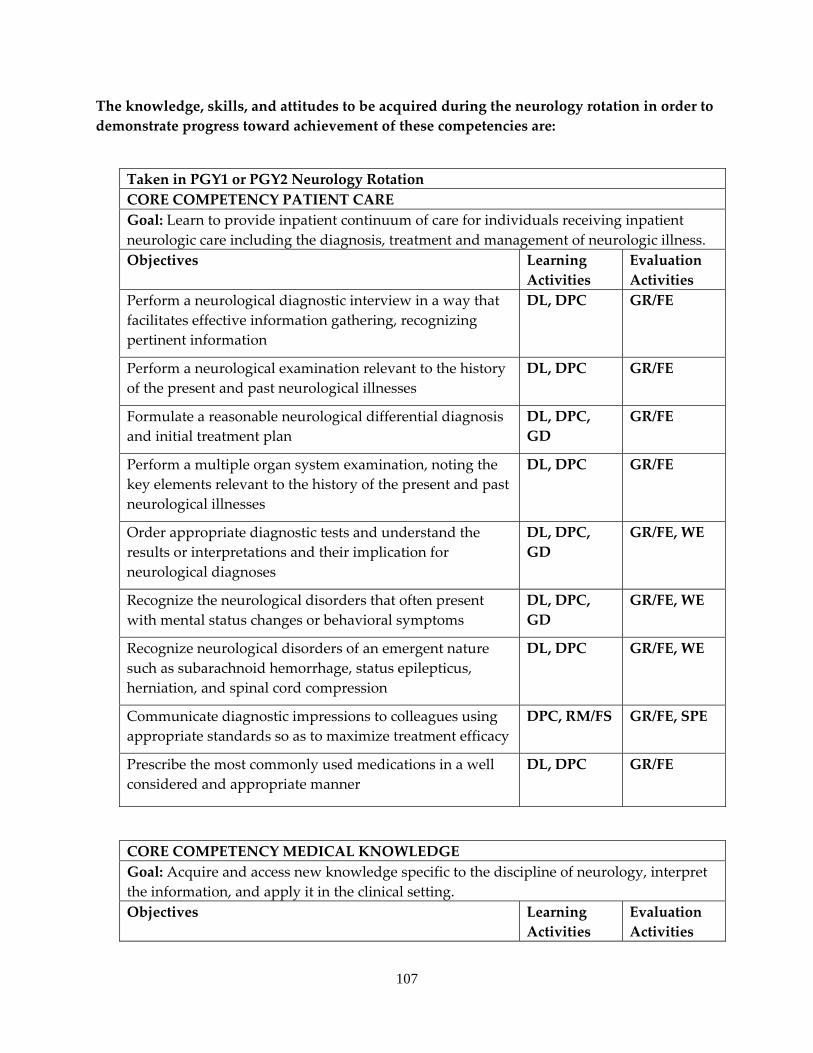
107
The knowledge, skills, and attitudes to be acquired during the neurology rotation in order to demonstrate progress toward achievement of these competencies are:
Taken in PGY1 or PGY2 Neurology Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of care for individuals receiving inpatient neurologic care including the diagnosis, treatment and management of neurologic illness.Objectives Learning
Activities Evaluation Activities
Perform a neurological diagnostic interview in a way that facilitates effective information gathering, recognizing pertinent information
DL, DPC GR/FE
Perform a neurological examination relevant to the history of the present and past neurological illnesses
DL, DPC GR/FE
Formulate a reasonable neurological differential diagnosis and initial treatment plan
DL, DPC, GD
GR/FE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present and past neurological illnesses
DL, DPC GR/FE
Order appropriate diagnostic tests and understand the results or interpretations and their implication for neurological diagnoses
DL, DPC, GD
GR/FE, WE
Recognize the neurological disorders that often present with mental status changes or behavioral symptoms
DL, DPC, GD
GR/FE, WE
Recognize neurological disorders of an emergent nature such as subarachnoid hemorrhage, status epilepticus, herniation, and spinal cord compression
DL, DPC GR/FE, WE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DPC, RM/FS GR/FE, SPE
Prescribe the most commonly used medications in a well considered and appropriate manner
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge specific to the discipline of neurology, interpret the information, and apply it in the clinical setting.Objectives Learning
Activities Evaluation Activities
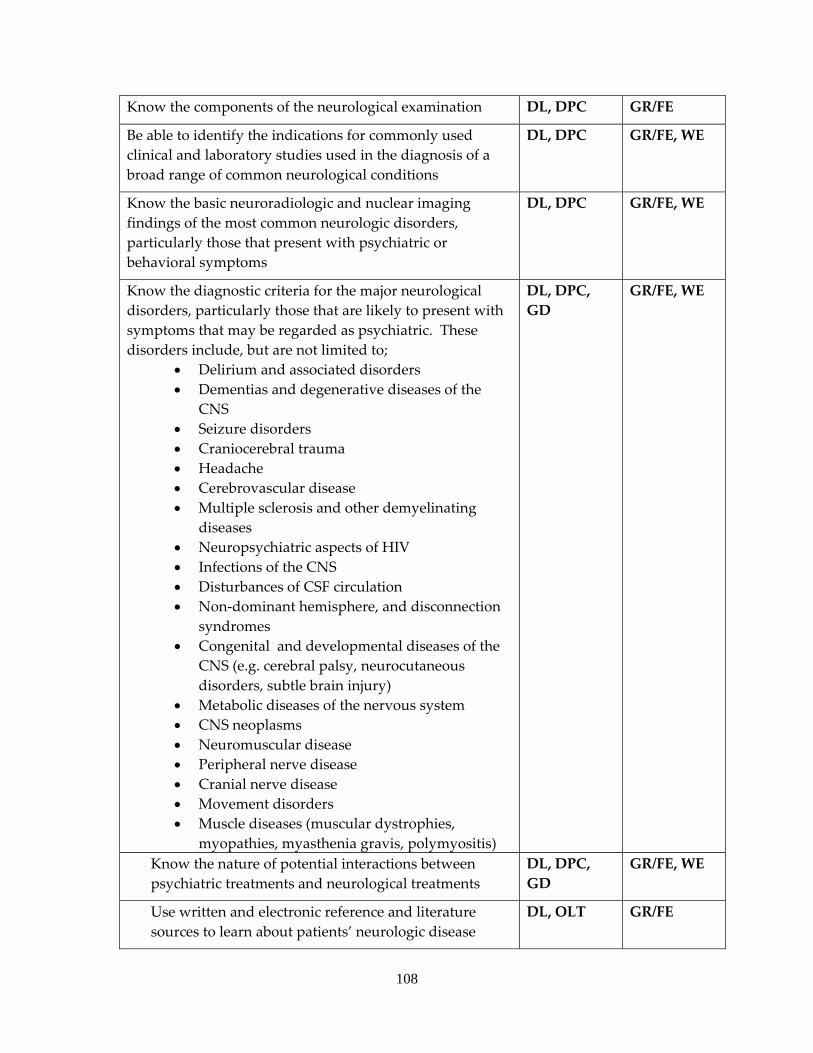
108
Know the components of the neurological examination DL, DPC GR/FE
Be able to identify the indications for commonly used clinical and laboratory studies used in the diagnosis of a broad range of common neurological conditions
DL, DPC GR/FE, WE
Know the basic neuroradiologic and nuclear imaging findings of the most common neurologic disorders, particularly those that present with psychiatric or behavioral symptoms
DL, DPC GR/FE, WE
Know the diagnostic criteria for the major neurological disorders, particularly those that are likely to present with symptoms that may be regarded as psychiatric. These disorders include, but are not limited to;
• Delirium and associated disorders • Dementias and degenerative diseases of the
CNS • Seizure disorders • Craniocerebral trauma • Headache • Cerebrovascular disease • Multiple sclerosis and other demyelinating
diseases • Neuropsychiatric aspects of HIV • Infections of the CNS • Disturbances of CSF circulation • Non‐dominant hemisphere, and disconnection
syndromes • Congenital and developmental diseases of the
CNS (e.g. cerebral palsy, neurocutaneous disorders, subtle brain injury)
• Metabolic diseases of the nervous system • CNS neoplasms • Neuromuscular disease • Peripheral nerve disease • Cranial nerve disease • Movement disorders • Muscle diseases (muscular dystrophies,
myopathies, myasthenia gravis, polymyositis)
DL, DPC, GD
GR/FE, WE
Know the nature of potential interactions between psychiatric treatments and neurological treatments
DL, DPC, GD
GR/FE, WE
Use written and electronic reference and literature sources to learn about patients’ neurologic disease
DL, OLT GR/FE

109
Demonstrate growth of neurologic knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Learn to critically self‐evaluate neurological practices and demonstrate improvement as a result of such evaluations
DPC, GD GR/FE
Develop habits of self‐education GD, RM/FS GR/FE, WE
Appreciate the value of research and the need to read the literature critically
DL, PR GR/FE
Develop fundamental skills in teaching medical students, peers and other health care professionals
CORE, GD, RM/FS
GR/FE
Use information technology to access on‐line medical information
GD, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies regarding neurological disorders and relate knowledge to clinical practice
DL, DPC GR/FE
Show willingness to learn from mistakes GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan
DPC, DSP GR/FE
Maintain a professional attitude at all times with patients DSP, DPC, RM/FS
GR/FE
Communicate with neurological disordered and/or uncooperative patients in a flexible and respectful manner
DPC GR/FE
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE
Empathize with patients suffering from neurological illness DL, DPC, GR/FE
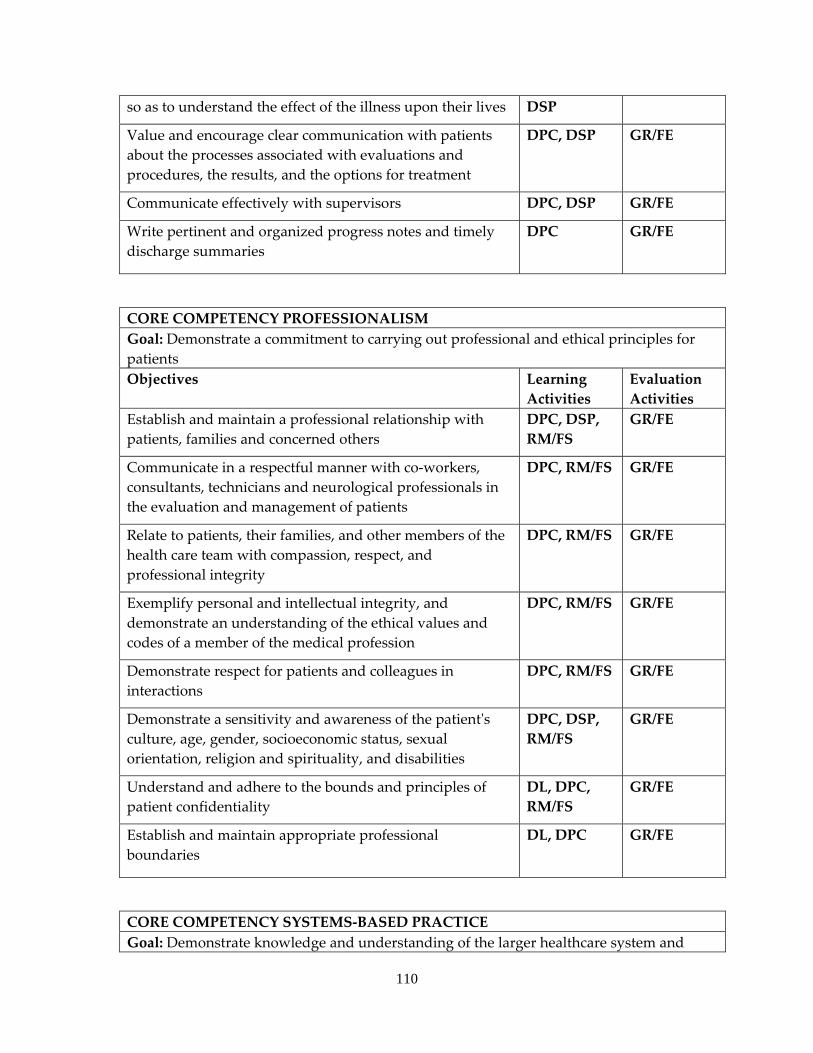
110
so as to understand the effect of the illness upon their lives DSP
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE
Communicate in a respectful manner with co‐workers, consultants, technicians and neurological professionals in the evaluation and management of patients
DPC, RM/FS GR/FE
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions
DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE
Understand and adhere to the bounds and principles of patient confidentiality
DL, DPC, RM/FS
GR/FE
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and
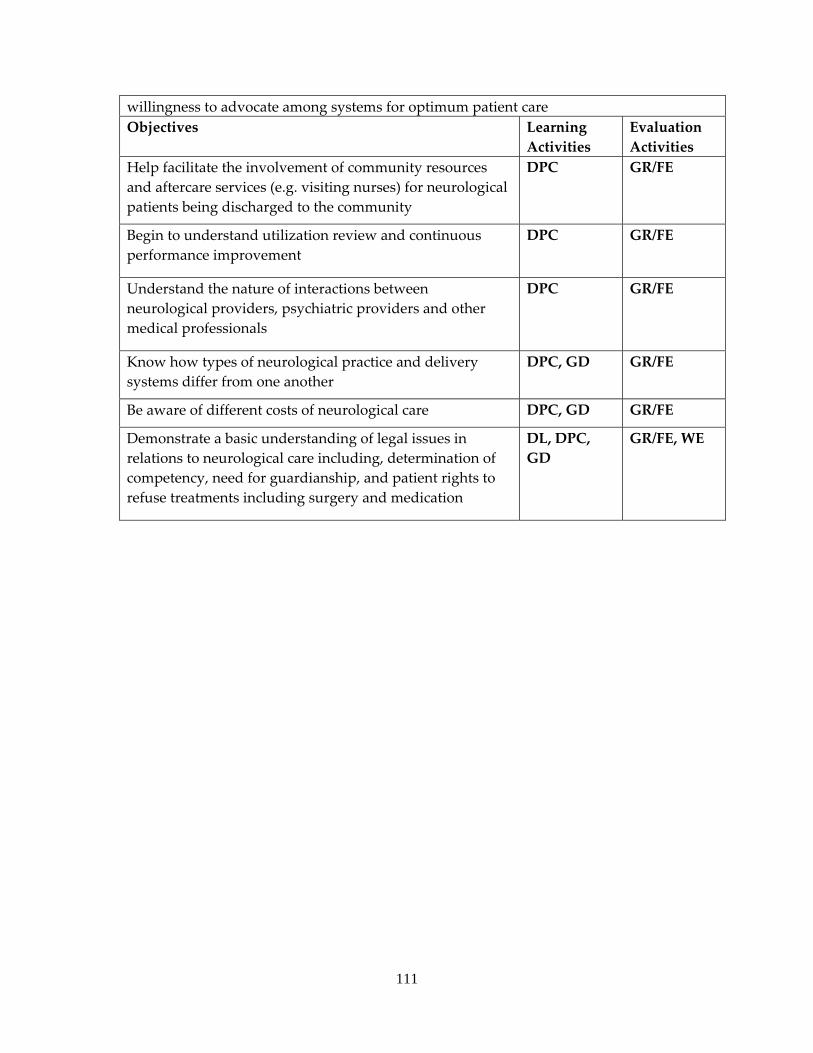
111
willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for neurological patients being discharged to the community
DPC GR/FE
Begin to understand utilization review and continuous performance improvement
DPC GR/FE
Understand the nature of interactions between neurological providers, psychiatric providers and other medical professionals
DPC GR/FE
Know how types of neurological practice and delivery systems differ from one another
DPC, GD GR/FE
Be aware of different costs of neurological care DPC, GD GR/FE
Demonstrate a basic understanding of legal issues in relations to neurological care including, determination of competency, need for guardianship, and patient rights to refuse treatments including surgery and medication
DL, DPC, GD
GR/FE, WE
112
a. PSYCHIATRY ADULT OUTPATIENT SERVICE b. Required continuous half‐time 6 month rotation occurring in the PGY3 year. c. Faculty consists of two full‐time time psychiatrists d. Residents spend 1.5 hours a week in formal didactic or interviewing skill conferences
and attend ½ day of didactic programming at KUMC during this rotation and attend grand rounds 2 hours weekly. In addition, residents regularly discuss with faculty treatment planning for new patients and continuing management of outpatient case load.
e. Patient diagnoses cover the spectrum of adult psychiatric disorders with the greatest concentration in affective disorders, schizophrenia and personality disorders. Co‐occurring substance abuse is commonly associated with these diagnoses. The patient population is 90% male with age ranges from 18‐85 with the majority age 35‐70. Residents spend approximately 35% of their time evaluating new cases, 55% following an established case load of patients treated with psychotherapy and/or pharmacotherapy, and 10% in emergency evaluations and crisis management.
f. Residents evaluate approximately 5‐7 new patients per week and follow approximately 20‐25 established patients per week.
g. An attending psychiatrist is always available for consultation and review of patients. In addition, residents receive two hours of individual supervision, one hour of which is devoted exclusively to psychotherapy supervision.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: OUTPATIENT ADULT PSYCHIATRY LEVEL: PGY3 DURATION: 6 MONTHS, HALF‐TIME (PGY3) SITE: DWIGHT D. EISENHOWER VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT DWIGHT D. EISENHOWER VA MEDICAL CENTER By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
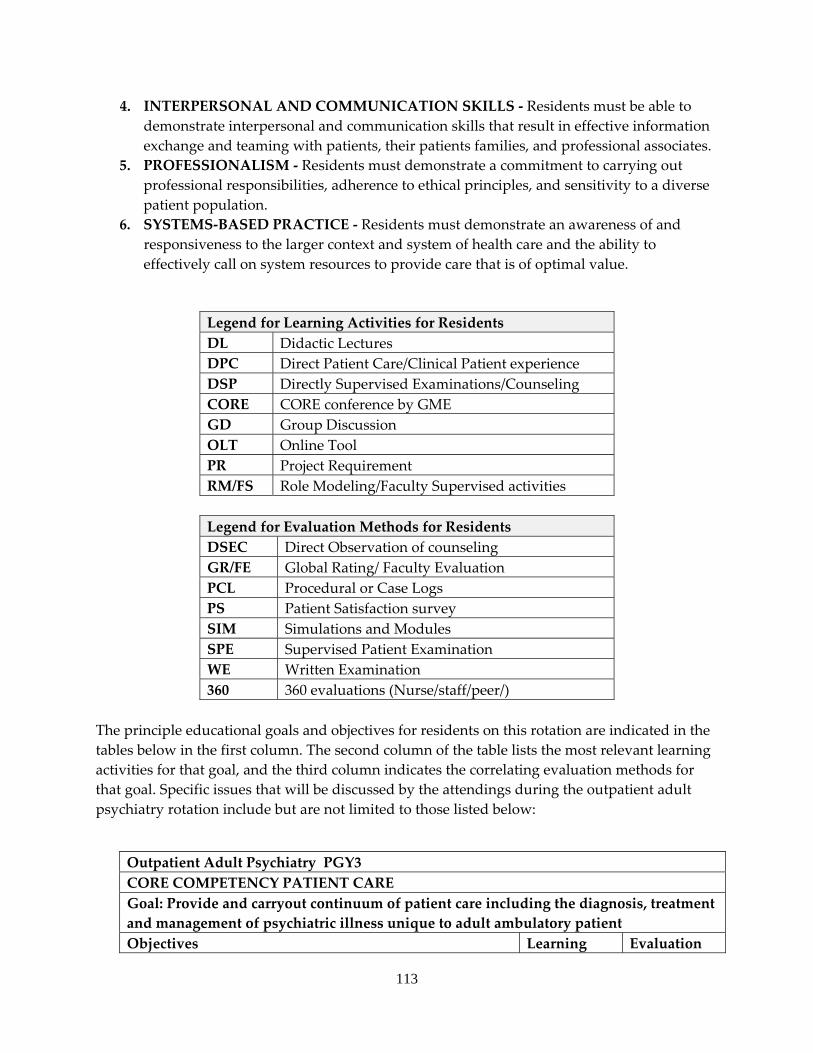
113
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the outpatient adult psychiatry rotation include but are not limited to those listed below:
Outpatient Adult Psychiatry PGY3 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to adult ambulatory patient Objectives Learning Evaluation
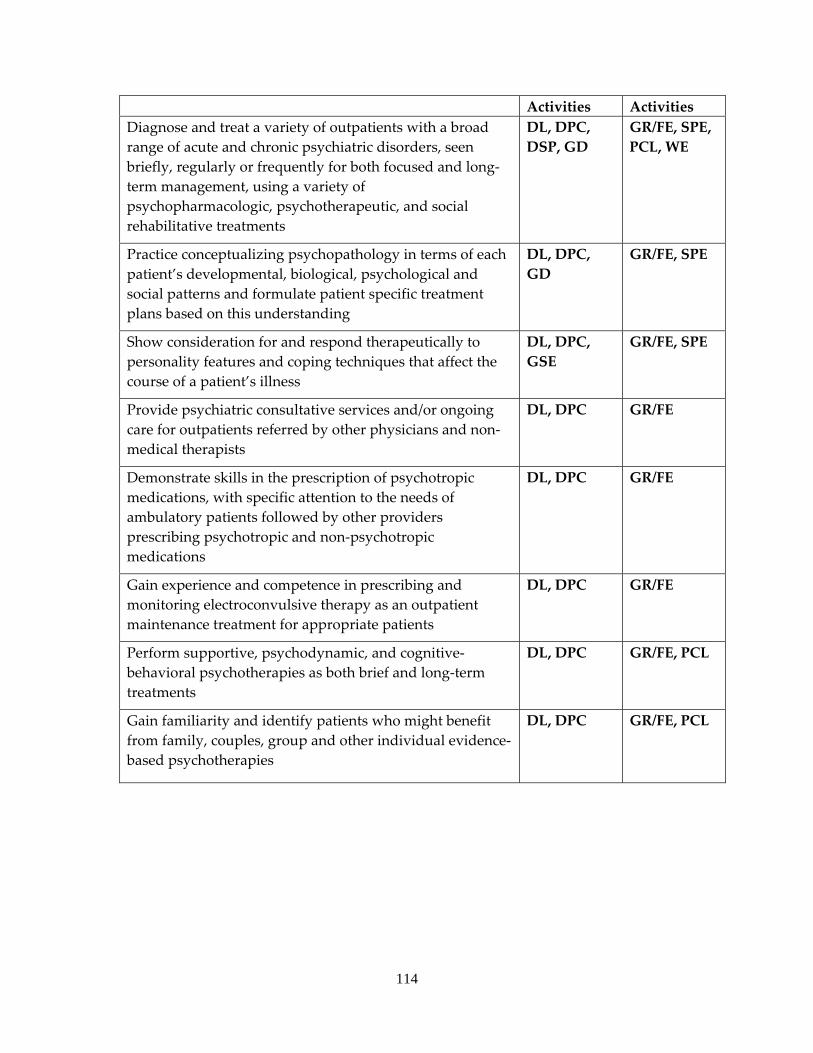
114
Activities Activities Diagnose and treat a variety of outpatients with a broad range of acute and chronic psychiatric disorders, seen briefly, regularly or frequently for both focused and long‐term management, using a variety of psychopharmacologic, psychotherapeutic, and social rehabilitative treatments
DL, DPC, DSP, GD
GR/FE, SPE, PCL, WE
Practice conceptualizing psychopathology in terms of each patient’s developmental, biological, psychological and social patterns and formulate patient specific treatment plans based on this understanding
DL, DPC, GD
GR/FE, SPE
Show consideration for and respond therapeutically to personality features and coping techniques that affect the course of a patient’s illness
DL, DPC, GSE
GR/FE, SPE
Provide psychiatric consultative services and/or ongoing care for outpatients referred by other physicians and non‐medical therapists
DL, DPC GR/FE
Demonstrate skills in the prescription of psychotropic medications, with specific attention to the needs of ambulatory patients followed by other providers prescribing psychotropic and non‐psychotropic medications
DL, DPC GR/FE
Gain experience and competence in prescribing and monitoring electroconvulsive therapy as an outpatient maintenance treatment for appropriate patients
DL, DPC GR/FE
Perform supportive, psychodynamic, and cognitive‐behavioral psychotherapies as both brief and long‐term treatments
DL, DPC GR/FE, PCL
Gain familiarity and identify patients who might benefit from family, couples, group and other individual evidence‐based psychotherapies
DL, DPC GR/FE, PCL
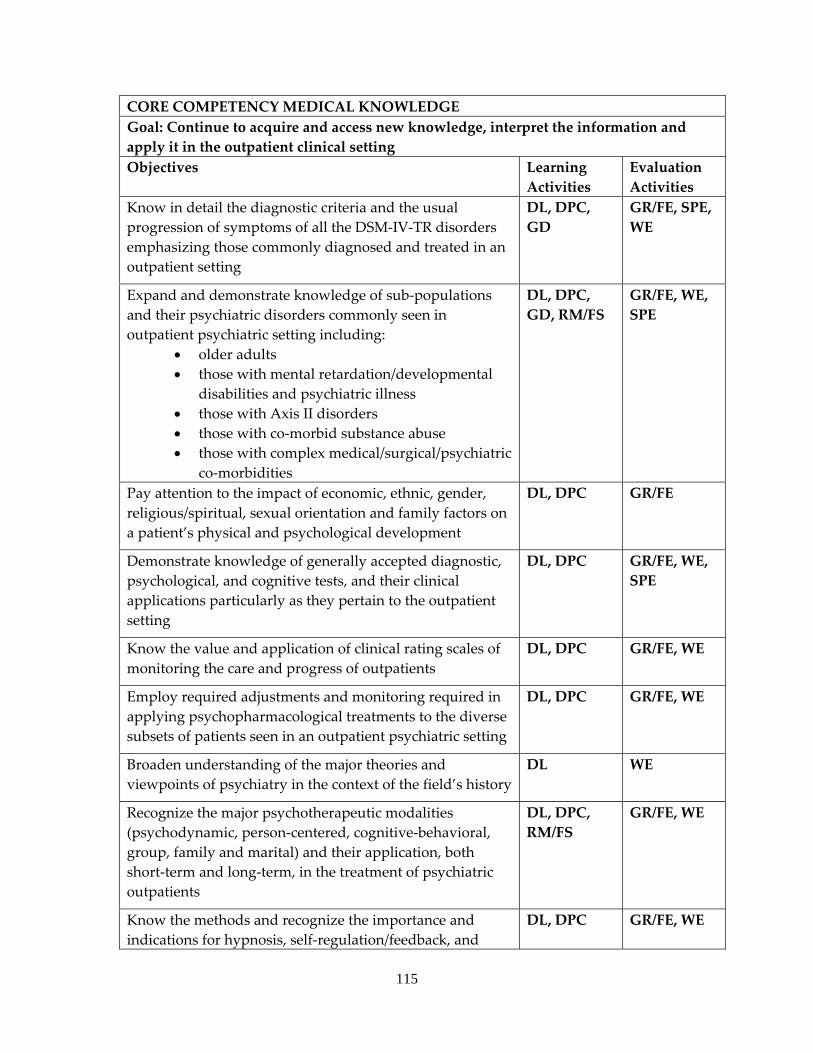
115
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Continue to acquire and access new knowledge, interpret the information and apply it in the outpatient clinical setting Objectives Learning
Activities Evaluation Activities
Know in detail the diagnostic criteria and the usual progression of symptoms of all the DSM‐IV‐TR disorders emphasizing those commonly diagnosed and treated in an outpatient setting
DL, DPC, GD
GR/FE, SPE, WE
Expand and demonstrate knowledge of sub‐populations and their psychiatric disorders commonly seen in outpatient psychiatric setting including:
• older adults • those with mental retardation/developmental
disabilities and psychiatric illness • those with Axis II disorders • those with co‐morbid substance abuse • those with complex medical/surgical/psychiatric
co‐morbidities
DL, DPC, GD, RM/FS
GR/FE, WE, SPE
Pay attention to the impact of economic, ethnic, gender, religious/spiritual, sexual orientation and family factors on a patient’s physical and psychological development
DL, DPC GR/FE
Demonstrate knowledge of generally accepted diagnostic, psychological, and cognitive tests, and their clinical applications particularly as they pertain to the outpatient setting
DL, DPC GR/FE, WE, SPE
Know the value and application of clinical rating scales of monitoring the care and progress of outpatients
DL, DPC GR/FE, WE
Employ required adjustments and monitoring required in applying psychopharmacological treatments to the diverse subsets of patients seen in an outpatient psychiatric setting
DL, DPC GR/FE, WE
Broaden understanding of the major theories and viewpoints of psychiatry in the context of the field’s history
DL WE
Recognize the major psychotherapeutic modalities (psychodynamic, person‐centered, cognitive‐behavioral, group, family and marital) and their application, both short‐term and long‐term, in the treatment of psychiatric outpatients
DL, DPC, RM/FS
GR/FE, WE
Know the methods and recognize the importance and indications for hypnosis, self‐regulation/feedback, and
DL, DPC GR/FE, WE
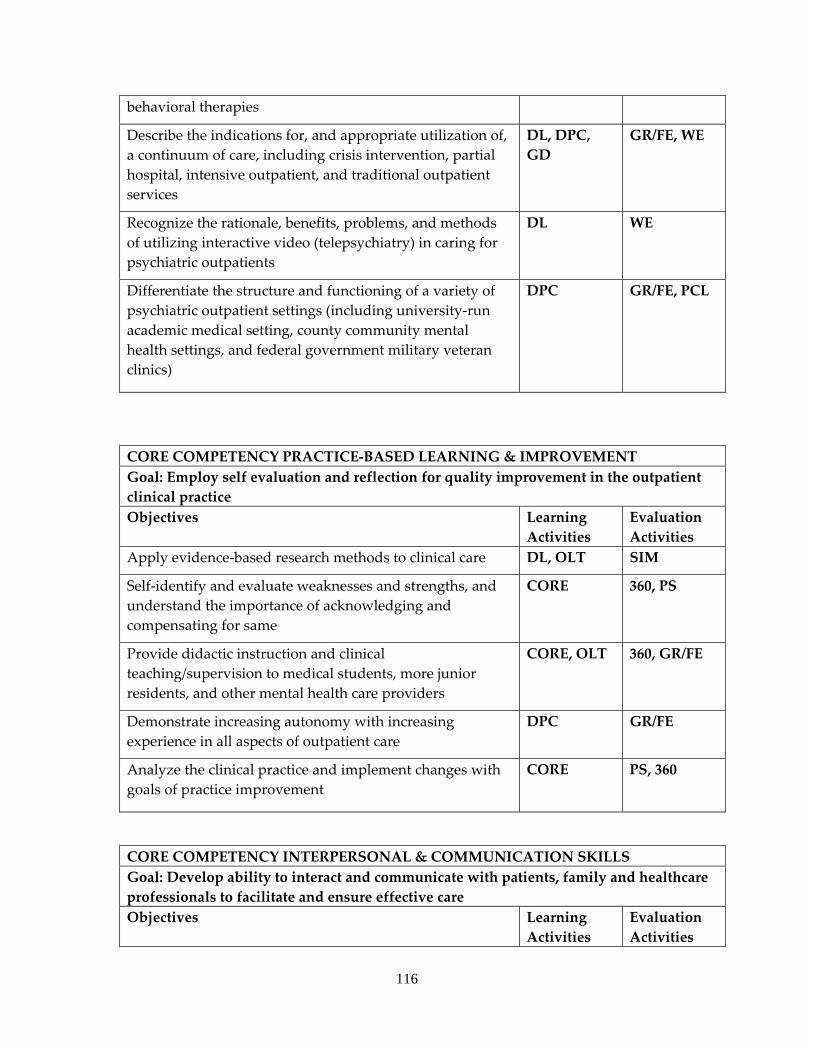
116
behavioral therapies
Describe the indications for, and appropriate utilization of, a continuum of care, including crisis intervention, partial hospital, intensive outpatient, and traditional outpatient services
DL, DPC, GD
GR/FE, WE
Recognize the rationale, benefits, problems, and methods of utilizing interactive video (telepsychiatry) in caring for psychiatric outpatients
DL WE
Differentiate the structure and functioning of a variety of psychiatric outpatient settings (including university‐run academic medical setting, county community mental health settings, and federal government military veteran clinics)
DPC GR/FE, PCL
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Employ self evaluation and reflection for quality improvement in the outpatient clinical practice Objectives Learning
Activities Evaluation Activities
Apply evidence‐based research methods to clinical care DL, OLT SIM
Self‐identify and evaluate weaknesses and strengths, and understand the importance of acknowledging and compensating for same
CORE 360, PS
Provide didactic instruction and clinical teaching/supervision to medical students, more junior residents, and other mental health care providers
CORE, OLT 360, GR/FE
Demonstrate increasing autonomy with increasing experience in all aspects of outpatient care
DPC GR/FE
Analyze the clinical practice and implement changes with goals of practice improvement
CORE PS, 360
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care Objectives Learning
Activities Evaluation Activities
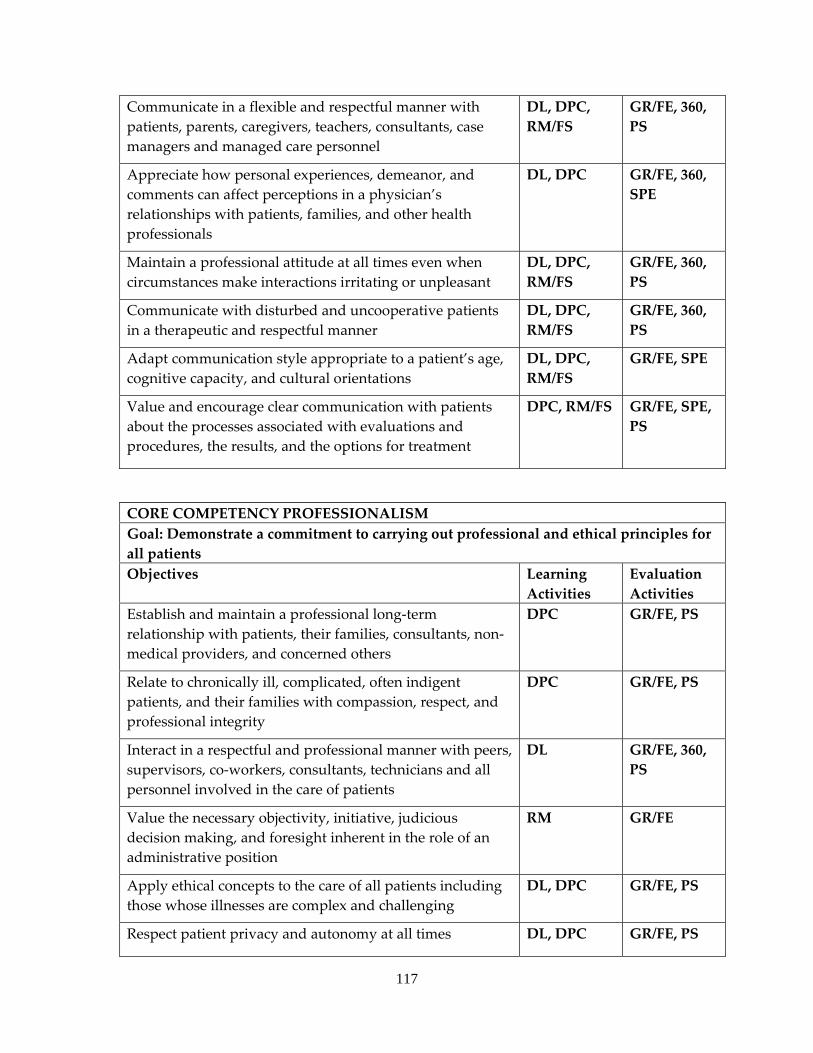
117
Communicate in a flexible and respectful manner with patients, parents, caregivers, teachers, consultants, case managers and managed care personnel
DL, DPC, RM/FS
GR/FE, 360, PS
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times even when circumstances make interactions irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360, PS
Communicate with disturbed and uncooperative patients in a therapeutic and respectful manner
DL, DPC, RM/FS
GR/FE, 360, PS
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, RM/FS GR/FE, SPE, PS
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for all patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional long‐term relationship with patients, their families, consultants, non‐medical providers, and concerned others
DPC GR/FE, PS
Relate to chronically ill, complicated, often indigent patients, and their families with compassion, respect, and professional integrity
DPC GR/FE, PS
Interact in a respectful and professional manner with peers, supervisors, co‐workers, consultants, technicians and all personnel involved in the care of patients
DL GR/FE, 360, PS
Value the necessary objectivity, initiative, judicious decision making, and foresight inherent in the role of an administrative position
RM GR/FE
Apply ethical concepts to the care of all patients including those whose illnesses are complex and challenging
DL, DPC GR/FE, PS
Respect patient privacy and autonomy at all times DL, DPC GR/FE, PS
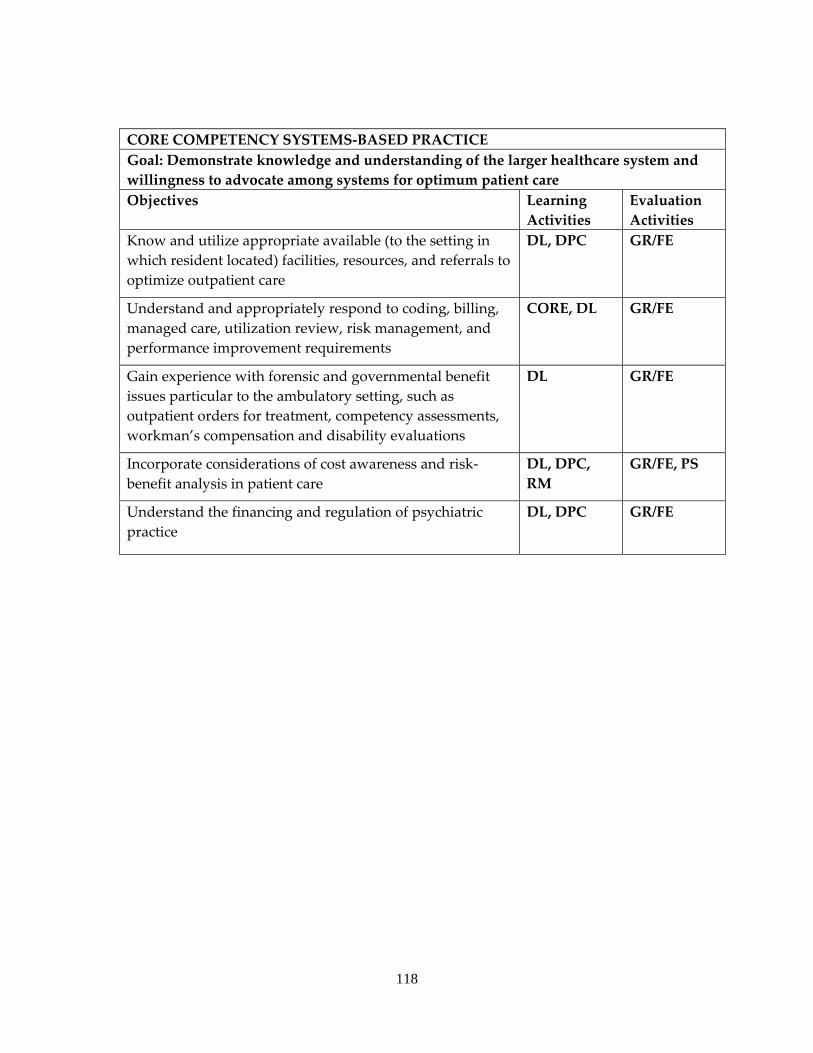
118
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Know and utilize appropriate available (to the setting in which resident located) facilities, resources, and referrals to optimize outpatient care
DL, DPC GR/FE
Understand and appropriately respond to coding, billing, managed care, utilization review, risk management, and performance improvement requirements
CORE, DL GR/FE
Gain experience with forensic and governmental benefit issues particular to the ambulatory setting, such as outpatient orders for treatment, competency assessments, workman’s compensation and disability evaluations
DL GR/FE
Incorporate considerations of cost awareness and risk‐benefit analysis in patient care
DL, DPC, RM
GR/FE, PS
Understand the financing and regulation of psychiatric practice
DL, DPC GR/FE
119
COLMERY O’NEILL VETERANS AFFAIRS MEDICAL CENTER
a. ACUTE INPATIENT PSYCHIATRY SERVICE b. A required 1 month rotation for PGY1 (or occasionally PGY2 or PGY4) residents. c. Faculty consists of 3 psychiatrists. d. Residents meet daily with the multidisciplinary team of nurses, social workers, and
the supervising attending. They then round with the attending psychiatrist for 1‐3 hours daily during which time patients are interviewed by staff and diagnostic treatment and management issues are discussed with the resident. Residents attend didactic lectures, journal club and/or case conferences for 1 ½ ‐ 3 hours weekly in addition to scheduled educational activities occurring ½ day per week at KUMC and in addition to 1.5‐hour weekly grand rounds through videolink with KUMC. Each resident also reviews and discusses their assigned Kaplan and Sadock’s book chapter with a supervising psychiatrist.
e. The patient population is 90‐95% male, all age 18 and over with a wide range of ages. About 20% of the patients are Active Duty soldiers and the rest are Veterans. Patients are quite diverse in their racial/ethnic and cultural backgrounds. Primary diagnoses are approximately 60% psychotic, 30% non‐psychotic affective and anxiety disorders and 10% personality disorders. Co‐occurring substance abuse diagnoses occur in 40‐50% of patients. Treatment modalities include pharmacotherapy, electroconvulsive therapy, individual and group psycho‐educational therapy and behavioral therapy.
f. An average case load is 4‐10 hospitalized patients who have an average length of stay of approximately 9 days. Most patients are able to participate in group therapy and activities. Two to five patients are generally acutely psychotic requiring close supervision and/or the use of restraints.
g. Each resident meets daily with his/her attending psychiatrist for 1‐3 hours and that psychiatrist is continuously available for consultation. Due to the driving requirements no on‐call time is required. Hospitalized patients at the VA Eastern Kansas VA Health Care System demonstrate unusual breadth of psychopathology affording residents excellent educational opportunities in managing patients with severe psychiatric illness.
120
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: INTERNAL MEDICINE LEVEL: PGY1 DURATON: 4 MONTHS SITE: COLMERY O’NEILL VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING INTERNAL MEDICINE ATTENDING AT COLMERY O’NEILL VA MEDICAL CENTER
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
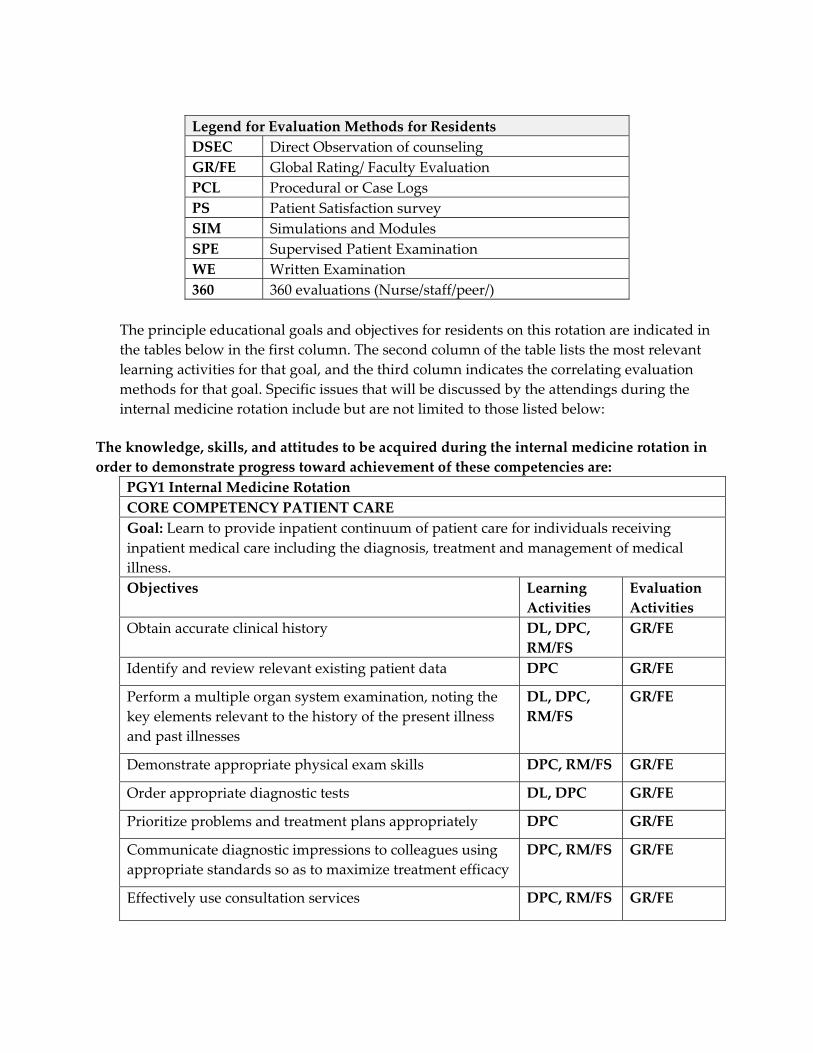
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the internal medicine rotation include but are not limited to those listed below:
The knowledge, skills, and attitudes to be acquired during the internal medicine rotation in order to demonstrate progress toward achievement of these competencies are:
PGY1 Internal Medicine Rotation CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving inpatient medical care including the diagnosis, treatment and management of medical illness. Objectives Learning
Activities Evaluation Activities
Obtain accurate clinical history DL, DPC, RM/FS
GR/FE
Identify and review relevant existing patient data DPC GR/FE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, RM/FS
GR/FE
Demonstrate appropriate physical exam skills DPC, RM/FS GR/FE
Order appropriate diagnostic tests DL, DPC GR/FE
Prioritize problems and treatment plans appropriately DPC GR/FE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DPC, RM/FS GR/FE
Effectively use consultation services DPC, RM/FS GR/FE
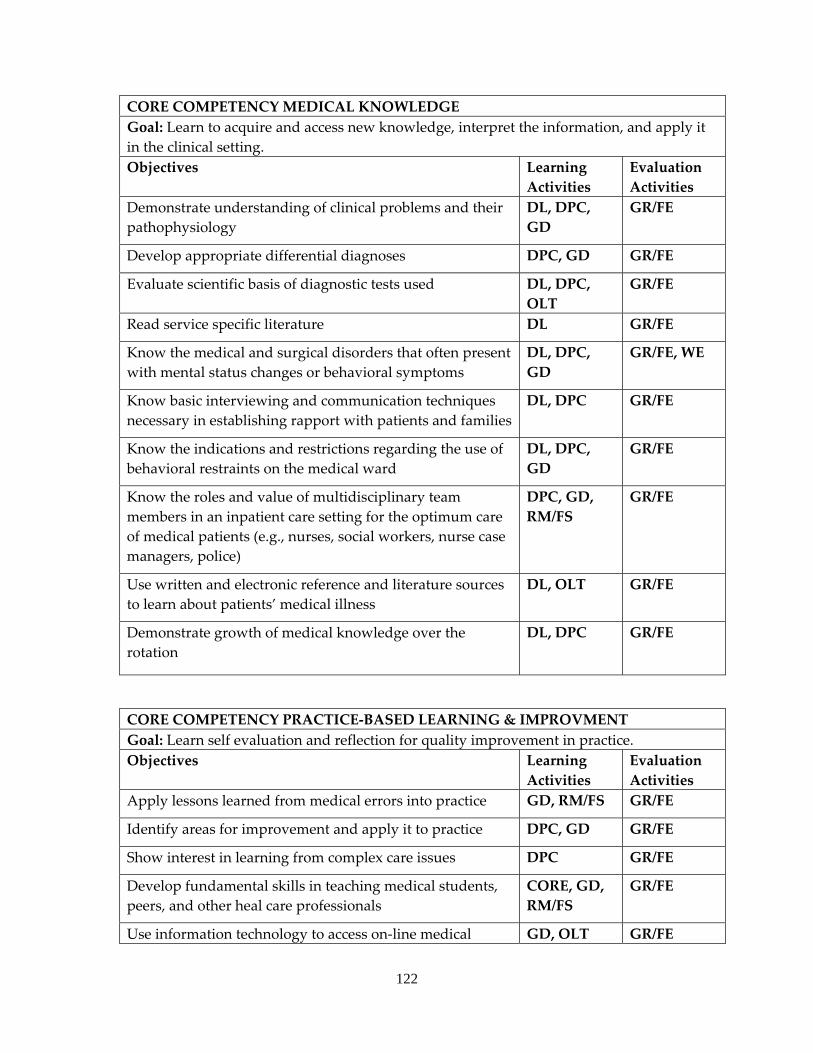
122
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting. Objectives Learning
Activities Evaluation Activities
Demonstrate understanding of clinical problems and their pathophysiology
DL, DPC, GD
GR/FE
Develop appropriate differential diagnoses DPC, GD GR/FE
Evaluate scientific basis of diagnostic tests used DL, DPC, OLT
GR/FE
Read service specific literature DL GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DPC, GD
GR/FE, WE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC GR/FE
Know the indications and restrictions regarding the use of behavioral restraints on the medical ward
DL, DPC, GD
GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting for the optimum care of medical patients (e.g., nurses, social workers, nurse case managers, police)
DPC, GD, RM/FS
GR/FE
Use written and electronic reference and literature sources to learn about patients’ medical illness
DL, OLT GR/FE
Demonstrate growth of medical knowledge over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice. Objectives Learning
Activities Evaluation Activities
Apply lessons learned from medical errors into practice GD, RM/FS GR/FE
Identify areas for improvement and apply it to practice DPC, GD GR/FE
Show interest in learning from complex care issues DPC GR/FE
Develop fundamental skills in teaching medical students, peers, and other heal care professionals
CORE, GD, RM/FS
GR/FE
Use information technology to access on‐line medical GD, OLT GR/FE
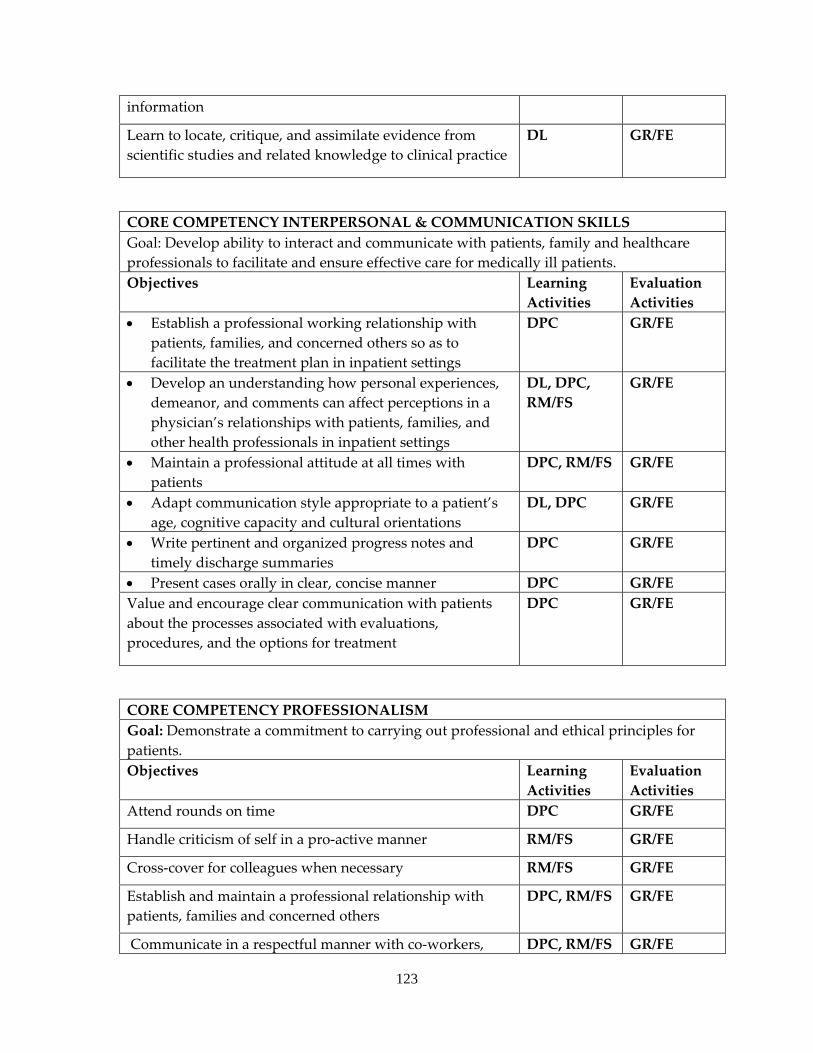
123
information
Learn to locate, critique, and assimilate evidence from scientific studies and related knowledge to clinical practice
DL GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for medically ill patients. Objectives Learning
Activities Evaluation Activities
• Establish a professional working relationship with patients, families, and concerned others so as to facilitate the treatment plan in inpatient settings
DPC GR/FE
• Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, DPC, RM/FS
GR/FE
• Maintain a professional attitude at all times with patients
DPC, RM/FS GR/FE
• Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE
• Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
• Present cases orally in clear, concise manner DPC GR/FE Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients. Objectives Learning
Activities Evaluation Activities
Attend rounds on time DPC GR/FE
Handle criticism of self in a pro‐active manner RM/FS GR/FE
Cross‐cover for colleagues when necessary RM/FS GR/FE
Establish and maintain a professional relationship with patients, families and concerned others
DPC, RM/FS GR/FE
Communicate in a respectful manner with co‐workers, DPC, RM/FS GR/FE
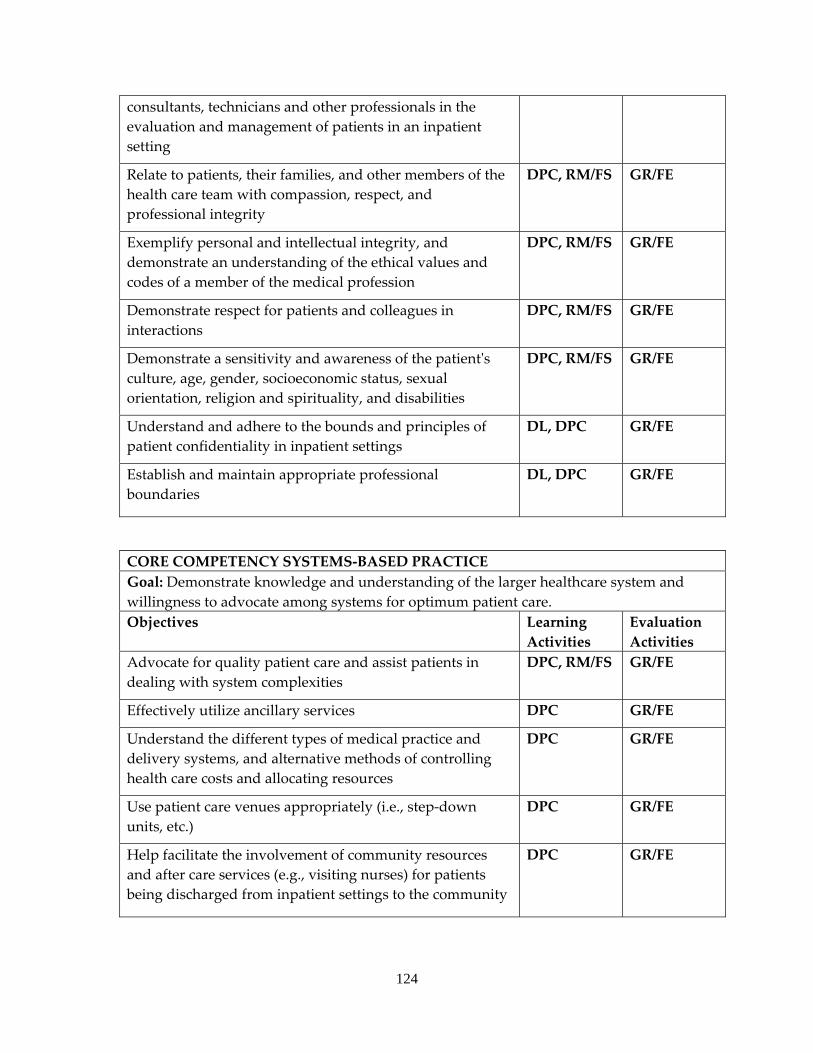
124
consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE
Demonstrate respect for patients and colleagues in interactions
DPC, RM/FS GR/FE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS GR/FE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE
Establish and maintain appropriate professional boundaries
DL, DPC GR/FE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care.Objectives Learning
Activities Evaluation Activities
Advocate for quality patient care and assist patients in dealing with system complexities
DPC, RM/FS GR/FE
Effectively utilize ancillary services DPC GR/FE
Understand the different types of medical practice and delivery systems, and alternative methods of controlling health care costs and allocating resources
DPC GR/FE
Use patient care venues appropriately (i.e., step‐down units, etc.)
DPC GR/FE
Help facilitate the involvement of community resources and after care services (e.g., visiting nurses) for patients being discharged from inpatient settings to the community
DPC GR/FE
125
GERIATRIC PSYCHIATRY SERVICE
a. A required 1 month rotation for PGY1 (or occasionally PGY2 or PGY4) residents. b. Faculty consists of one full‐time Geriatric Psychiatrist. c. Residents meet daily with the multidisciplinary team of nurses, social workers, and
the supervising attending. They then round with the attending geriatric psychiatrist for 1‐3 hours daily during which time patients are interviewed by staff and diagnostic treatment and management issues are discussed with the resident. Residents attend didactic lectures, journal club and/or case conferences for 1 ½ ‐ 3 hours weekly in addition to scheduled educational activities occurring ½ day per week at KUMC and in addition to 1.5‐hour weekly grand rounds via videolink with KUMC. Each resident also reviews and discusses their assigned Kaplan and Saddock’s book chapter with the supervising geriatric psychiatrist.
d. The patient population is 90‐95% male mostly age 60 and above. Patients are about 2/3 Caucasian and 1/3African‐American and other minorities. Primary diagnoses are approximately 40% psychotic, 30% non‐psychotic affective and anxiety disorders and 30% Dementia disorders. Co‐occurring substance abuse diagnoses occur in 40‐50% of patients. Treatment modalities include pharmacotherapy, electroconvulsive therapy, individual and group psycho‐educational therapy and behavioral therapy.
e. An average case load is 10‐12 hospitalized patients who have an average length of stay of approximately 55 days. Many patients are able to participate in group therapy and activities.
f. Each resident meets daily with his/her attending psychiatrist for 1‐3 hours and that psychiatrist is continuously available for consultation.
g. Hospitalized patients at the VA Eastern Kansas demonstrate unusual breadth of psychopathology affording residents excellent educational opportunities in managing patients with severe psychiatric illness.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: GERIATRIC PSYCHIATRY LEVEL: PGY1 or PGY2 DURATON: 1 MONTH SITE: TOPEKA VAMC GERIATRIC INPATIENT UNIT SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING GERIATRIC PSYCHIATRIST AT TOPEKA VAMC
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health
126
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the geriatric psychiatry rotation include but are not limited to those listed below:
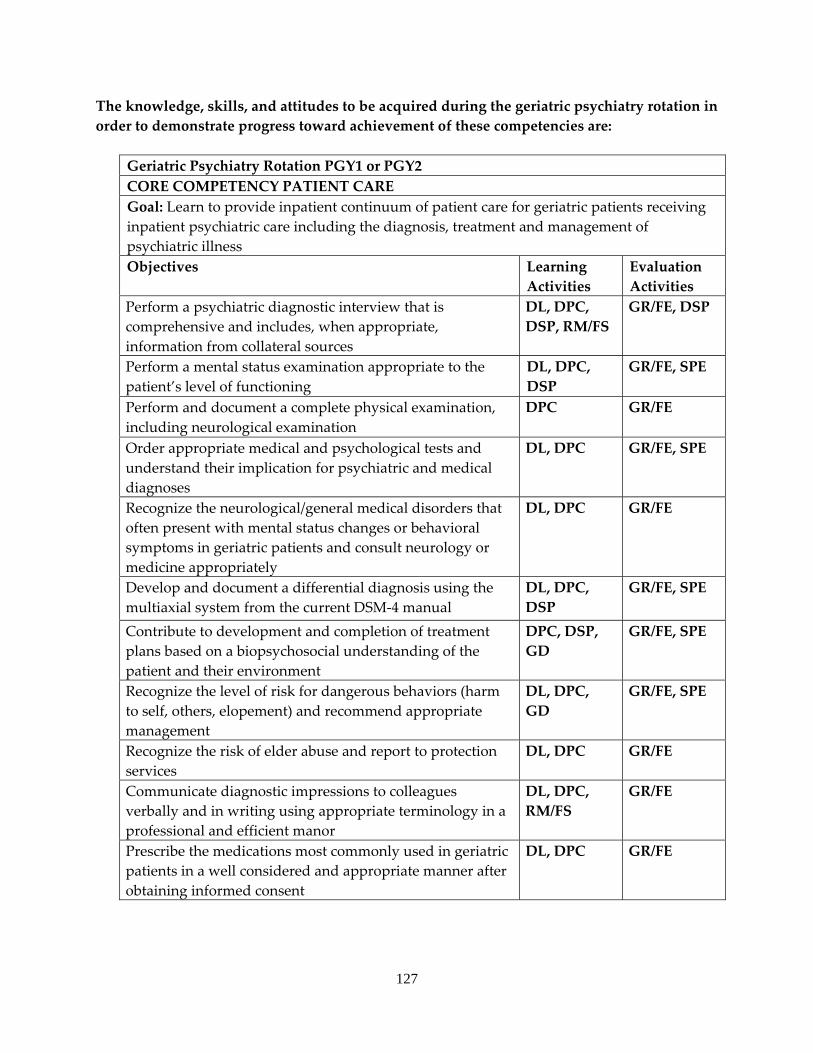
127
The knowledge, skills, and attitudes to be acquired during the geriatric psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Geriatric Psychiatry Rotation PGY1 or PGY2 CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for geriatric patients receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illness Objectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview that is comprehensive and includes, when appropriate, information from collateral sources
DL, DPC, DSP, RM/FS
GR/FE, DSP
Perform a mental status examination appropriate to the patient’s level of functioning
DL, DPC, DSP
GR/FE, SPE
Perform and document a complete physical examination, including neurological examination
DPC GR/FE
Order appropriate medical and psychological tests and understand their implication for psychiatric and medical diagnoses
DL, DPC GR/FE, SPE
Recognize the neurological/general medical disorders that often present with mental status changes or behavioral symptoms in geriatric patients and consult neurology or medicine appropriately
DL, DPC GR/FE
Develop and document a differential diagnosis using the multiaxial system from the current DSM‐4 manual
DL, DPC, DSP
GR/FE, SPE
Contribute to development and completion of treatment plans based on a biopsychosocial understanding of the patient and their environment
DPC, DSP, GD
GR/FE, SPE
Recognize the level of risk for dangerous behaviors (harm to self, others, elopement) and recommend appropriate management
DL, DPC, GD
GR/FE, SPE
Recognize the risk of elder abuse and report to protection services
DL, DPC GR/FE
Communicate diagnostic impressions to colleagues verbally and in writing using appropriate terminology in a professional and efficient manor
DL, DPC, RM/FS
GR/FE
Prescribe the medications most commonly used in geriatric patients in a well considered and appropriate manner after obtaining informed consent
DL, DPC GR/FE
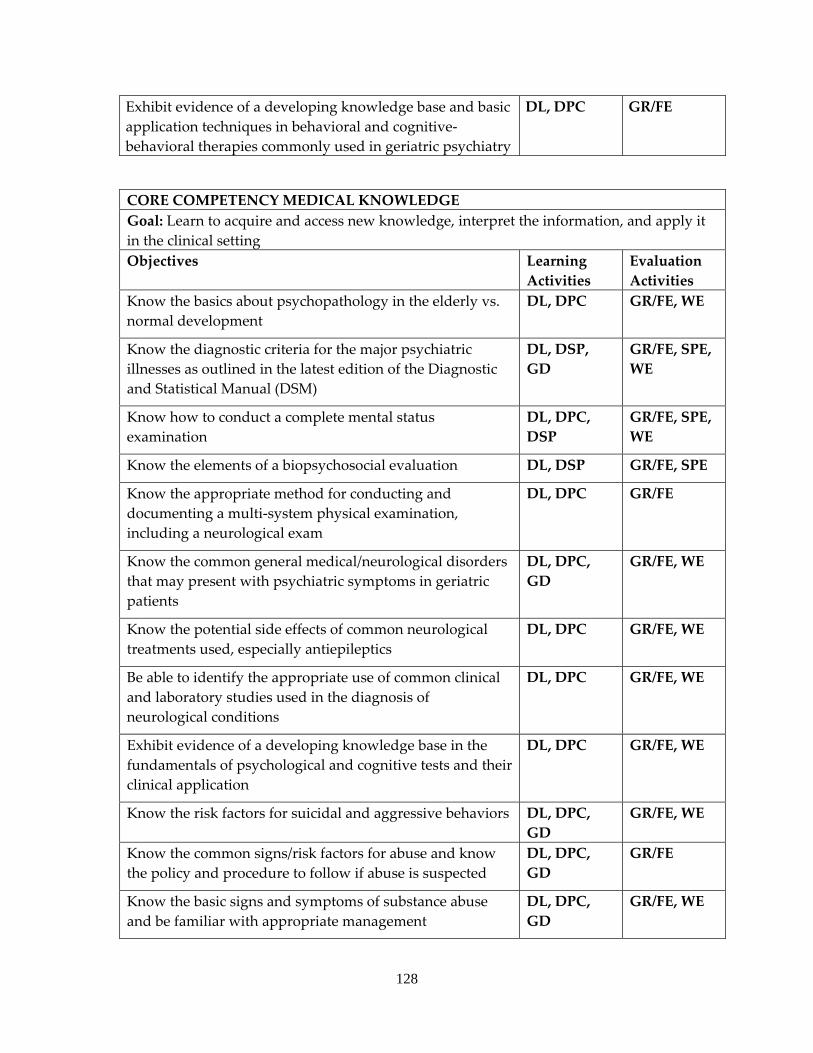
128
Exhibit evidence of a developing knowledge base and basic application techniques in behavioral and cognitive‐behavioral therapies commonly used in geriatric psychiatry
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting Objectives Learning
Activities Evaluation Activities
Know the basics about psychopathology in the elderly vs. normal development
DL, DPC GR/FE, WE
Know the diagnostic criteria for the major psychiatric illnesses as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
GR/FE, SPE, WE
Know how to conduct a complete mental status examination
DL, DPC, DSP
GR/FE, SPE, WE
Know the elements of a biopsychosocial evaluation DL, DSP GR/FE, SPE
Know the appropriate method for conducting and documenting a multi‐system physical examination, including a neurological exam
DL, DPC GR/FE
Know the common general medical/neurological disorders that may present with psychiatric symptoms in geriatric patients
DL, DPC, GD
GR/FE, WE
Know the potential side effects of common neurological treatments used, especially antiepileptics
DL, DPC GR/FE, WE
Be able to identify the appropriate use of common clinical and laboratory studies used in the diagnosis of neurological conditions
DL, DPC GR/FE, WE
Exhibit evidence of a developing knowledge base in the fundamentals of psychological and cognitive tests and their clinical application
DL, DPC GR/FE, WE
Know the risk factors for suicidal and aggressive behaviors DL, DPC, GD
GR/FE, WE
Know the common signs/risk factors for abuse and know the policy and procedure to follow if abuse is suspected
DL, DPC, GD
GR/FE
Know the basic signs and symptoms of substance abuse and be familiar with appropriate management
DL, DPC, GD
GR/FE, WE
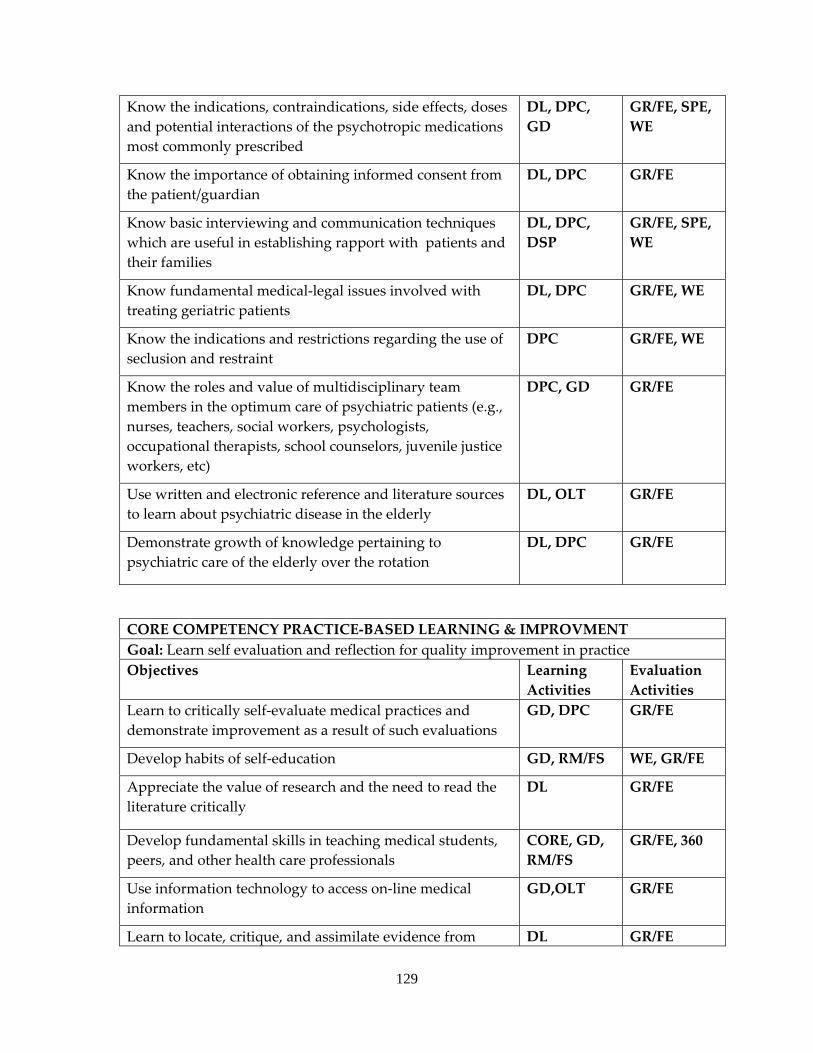
129
Know the indications, contraindications, side effects, doses and potential interactions of the psychotropic medications most commonly prescribed
DL, DPC, GD
GR/FE, SPE, WE
Know the importance of obtaining informed consent from the patient/guardian
DL, DPC GR/FE
Know basic interviewing and communication techniques which are useful in establishing rapport with patients and their families
DL, DPC, DSP
GR/FE, SPE, WE
Know fundamental medical‐legal issues involved with treating geriatric patients
DL, DPC GR/FE, WE
Know the indications and restrictions regarding the use of seclusion and restraint
DPC GR/FE, WE
Know the roles and value of multidisciplinary team members in the optimum care of psychiatric patients (e.g., nurses, teachers, social workers, psychologists, occupational therapists, school counselors, juvenile justice workers, etc)
DPC, GD GR/FE
Use written and electronic reference and literature sources to learn about psychiatric disease in the elderly
DL, OLT GR/FE
Demonstrate growth of knowledge pertaining to psychiatric care of the elderly over the rotation
DL, DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Learn to critically self‐evaluate medical practices and demonstrate improvement as a result of such evaluations
GD, DPC GR/FE
Develop habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Develop fundamental skills in teaching medical students, peers, and other health care professionals
CORE, GD, RM/FS
GR/FE, 360
Use information technology to access on‐line medical information
GD,OLT GR/FE
Learn to locate, critique, and assimilate evidence from DL GR/FE
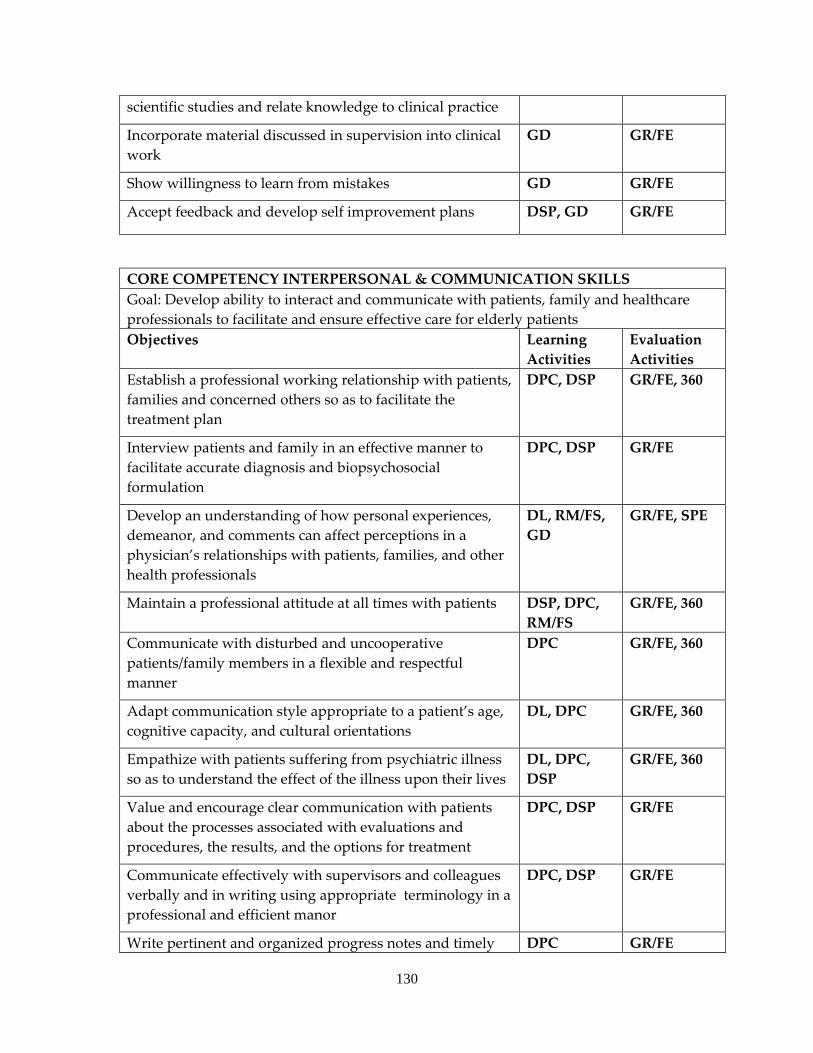
130
scientific studies and relate knowledge to clinical practice
Incorporate material discussed in supervision into clinical work
GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for elderly patients Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan
DPC, DSP GR/FE, 360
Interview patients and family in an effective manner to facilitate accurate diagnosis and biopsychosocial formulation
DPC, DSP GR/FE
Develop an understanding of how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, RM/FS, GD
GR/FE, SPE
Maintain a professional attitude at all times with patients DSP, DPC, RM/FS
GR/FE, 360
Communicate with disturbed and uncooperative patients/family members in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors and colleagues verbally and in writing using appropriate terminology in a professional and efficient manor
DPC, DSP GR/FE
Write pertinent and organized progress notes and timely DPC GR/FE
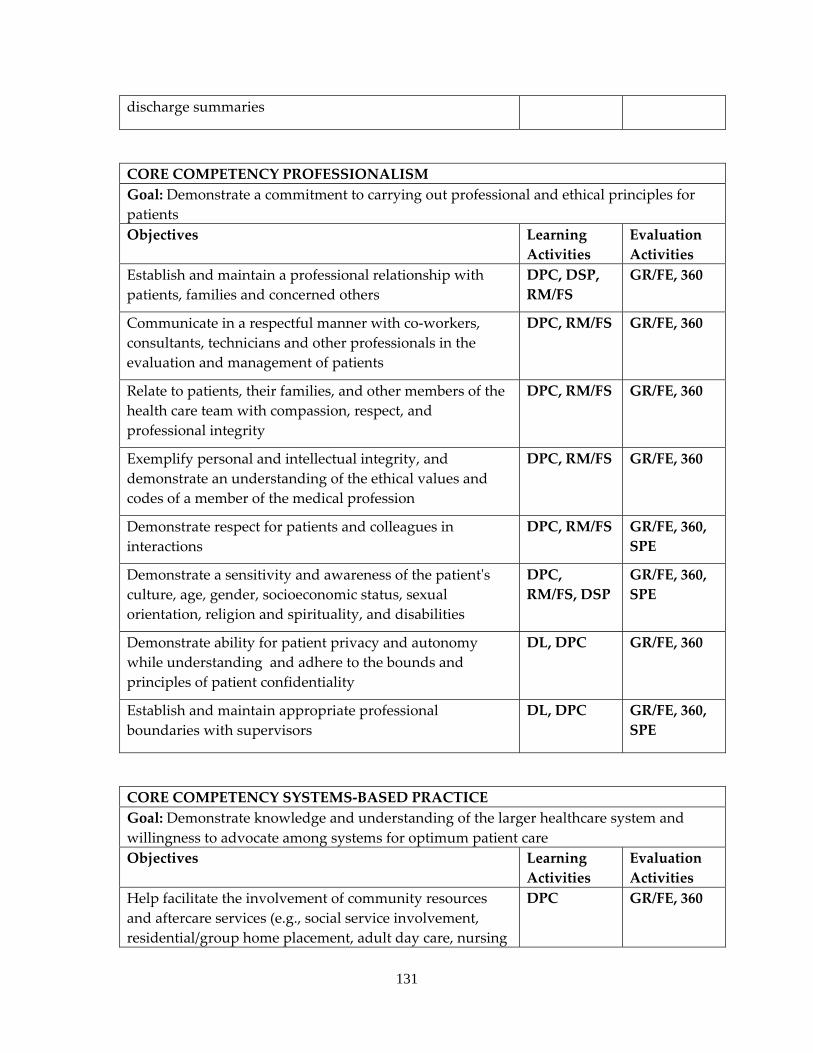
131
discharge summaries
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions
DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Demonstrate ability for patient privacy and autonomy while understanding and adhere to the bounds and principles of patient confidentiality
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries with supervisors
DL, DPC GR/FE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g., social service involvement, residential/group home placement, adult day care, nursing
DPC GR/FE, 360
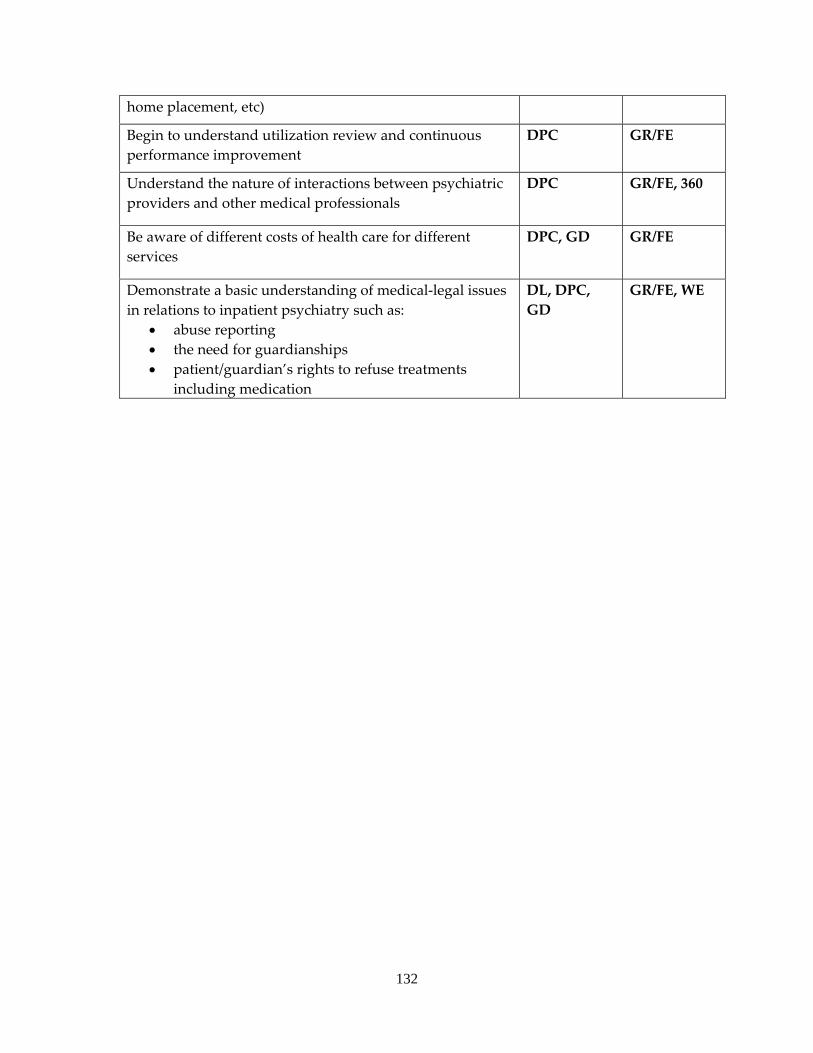
132
home placement, etc)
Begin to understand utilization review and continuous performance improvement
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals
DPC GR/FE, 360
Be aware of different costs of health care for different services
DPC, GD GR/FE
Demonstrate a basic understanding of medical‐legal issues in relations to inpatient psychiatry such as:
• abuse reporting • the need for guardianships • patient/guardian’s rights to refuse treatments
including medication
DL, DPC, GD
GR/FE, WE
133
a. INTERNAL MEDICINE SERVICE b. PGY1 residents have this rotation for 2 months to fulfill their internal medicine
requirements. c. The residents rotate for 1 month at a time with 2 of the 3 full‐time hospitalists,
trained in internal medicine. They may also rotate on the weekends with some of the 6 primary care physicians who work on the inpatient service. These physicians are either internal medicine or family practice trained. The residents will interact weekly if not daily with multiple specialists, including our cardiologist, pulmonologist, gastroenterologist, psychiatrists, neurologist, and infectious disease specialists.
d. Residents attend VA Journal Club, VA Ground Rounds, and KUMC Internal Medicine Grand Rounds once a week. They also attend lectures given by our attending 2 days per week. Attendance is strongly encouraged for these meetings. Optional programs include Tumor Board Conference weekly. Once a month Journal Club is replaced by Morbidity and Mortality conference, which the residents also attend. Residents round daily with attending staff for consultation regarding patient management and for every new patient admissions throughout the day. Attending physicians do patient‐based teaching throughout the day.
e. Patients come from rural, urban, and inner city areas of all socioeconomic status. This hospital manages the entire range of general medical diagnoses, with the exception of acute STEMI and acute dialysis needs. Residents care for inpatients on general medicine services and receive training in management of a variety of diseases with concentrations in pulmonary, cardiovascular, and infectious disease. They also care for patients in the open ICU and step‐down units. The patient population is mostly male, though there are some female inpatients. Most of the patients are age 40‐90, though again there are at times younger inpatients.
f. An average caseload consists of four patients, with a range of 2‐10 patients at any time.
g. Residents receive daily close supervision by the attending staff physician, who is available at all times.
h. As of 2011, there is no overnight call. The residents will work 2 weekends per month.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: ADULT INPATIENT PSYCHIATRY LEVEL: PGY1 AND PGY2 DURATON: 6‐8 MONTHS (PG1); 10‐12 MONTHS (PG2) SITE: COLMERY O’NEILL VA MEDICAL CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT COLMERY O’NEILL VA MEDICAL CENTER
134
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
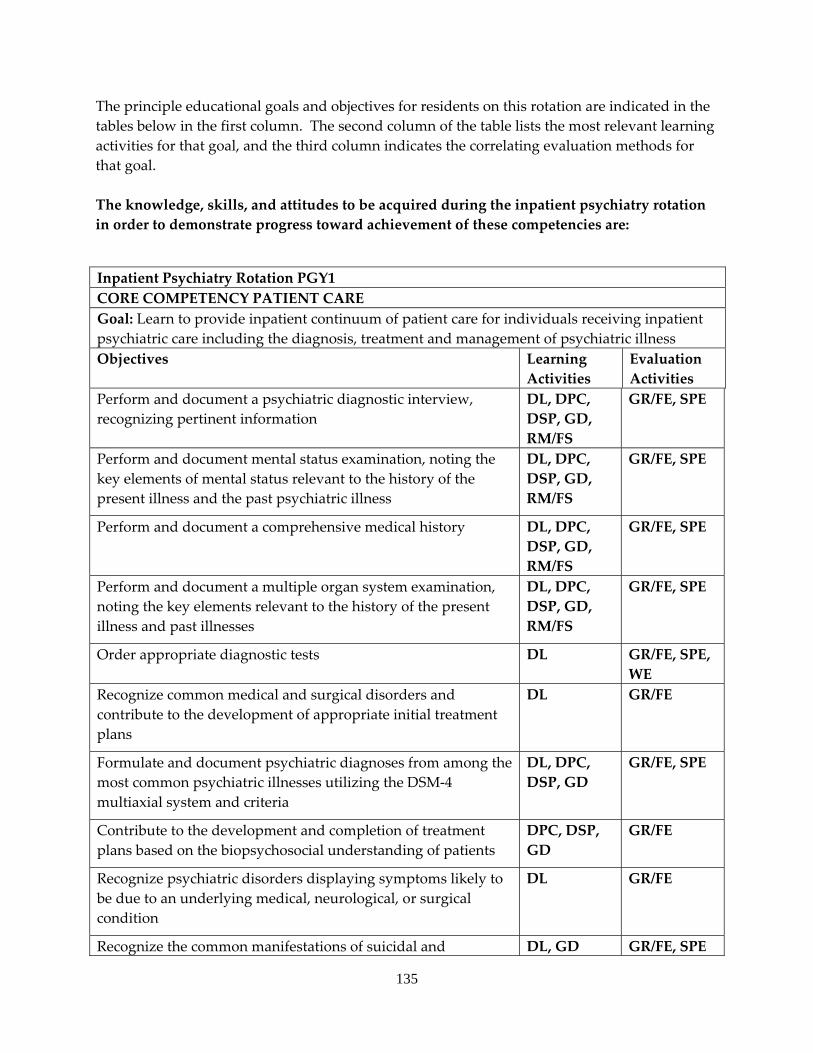
135
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. The knowledge, skills, and attitudes to be acquired during the inpatient psychiatry rotation in order to demonstrate progress toward achievement of these competencies are:
Inpatient Psychiatry Rotation PGY1 CORE COMPETENCY PATIENT CARE Goal: Learn to provide inpatient continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illness Objectives Learning
Activities Evaluation Activities
Perform and document a psychiatric diagnostic interview, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Order appropriate diagnostic tests DL GR/FE, SPE, WE
Recognize common medical and surgical disorders and contribute to the development of appropriate initial treatment plans
DL GR/FE
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DL, DPC, DSP, GD
GR/FE, SPE
Contribute to the development and completion of treatment plans based on the biopsychosocial understanding of patients
DPC, DSP, GD
GR/FE
Recognize psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL GR/FE
Recognize the common manifestations of suicidal and DL, GD GR/FE, SPE
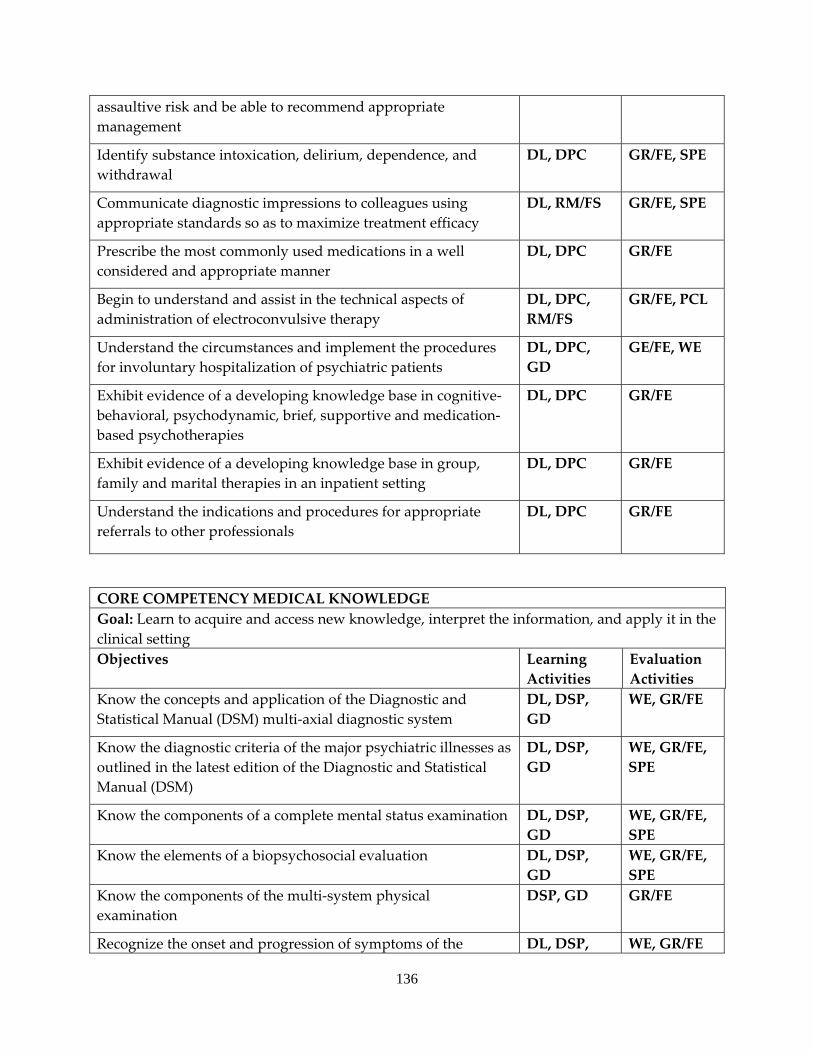
136
assaultive risk and be able to recommend appropriate management
Identify substance intoxication, delirium, dependence, and withdrawal
DL, DPC GR/FE, SPE
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe the most commonly used medications in a well considered and appropriate manner
DL, DPC GR/FE
Begin to understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GE/FE, WE
Exhibit evidence of a developing knowledge base in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Exhibit evidence of a developing knowledge base in group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Learn to acquire and access new knowledge, interpret the information, and apply it in the clinical setting Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and Statistical Manual (DSM) multi‐axial diagnostic system
DL, DSP, GD
WE, GR/FE
Know the diagnostic criteria of the major psychiatric illnesses as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Recognize the onset and progression of symptoms of the DL, DSP, WE, GR/FE
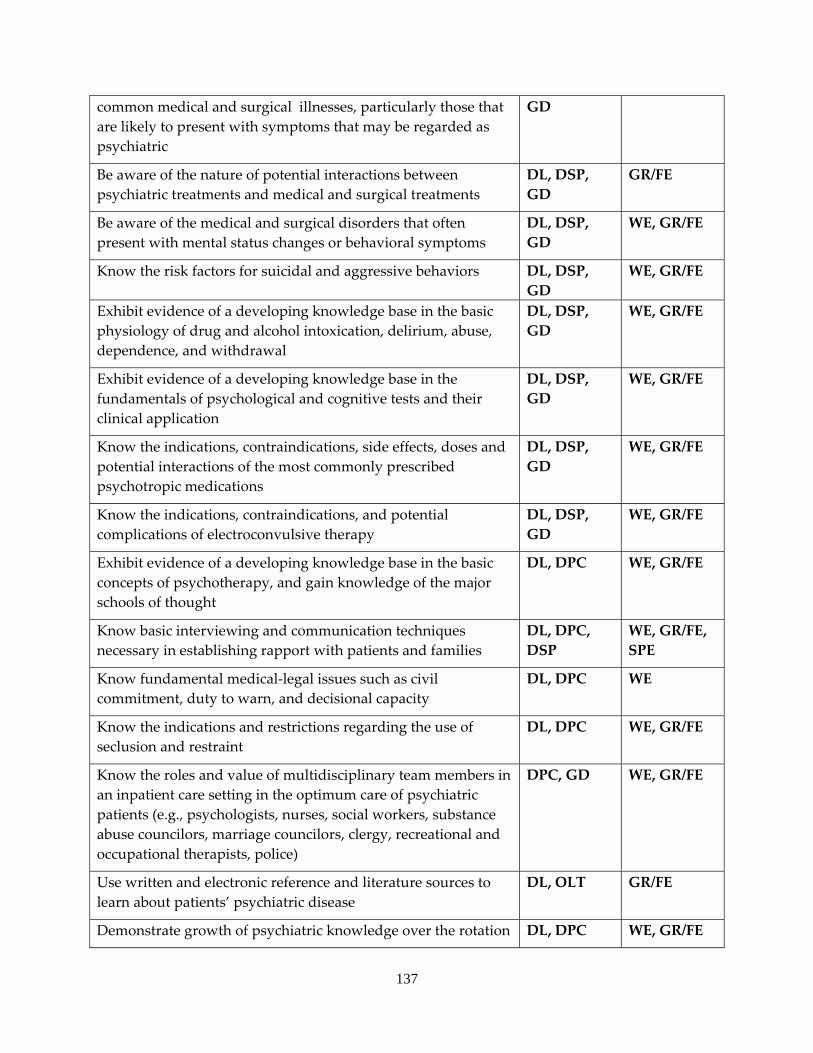
137
common medical and surgical illnesses, particularly those that are likely to present with symptoms that may be regarded as psychiatric
GD
Be aware of the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Be aware of the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of the most commonly prescribed psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Exhibit evidence of a developing knowledge base in the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Know basic interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil commitment, duty to warn, and decisional capacity
DL, DPC WE
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and occupational therapists, police)
DPC, GD WE, GR/FE
Use written and electronic reference and literature sources to learn about patients’ psychiatric disease
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
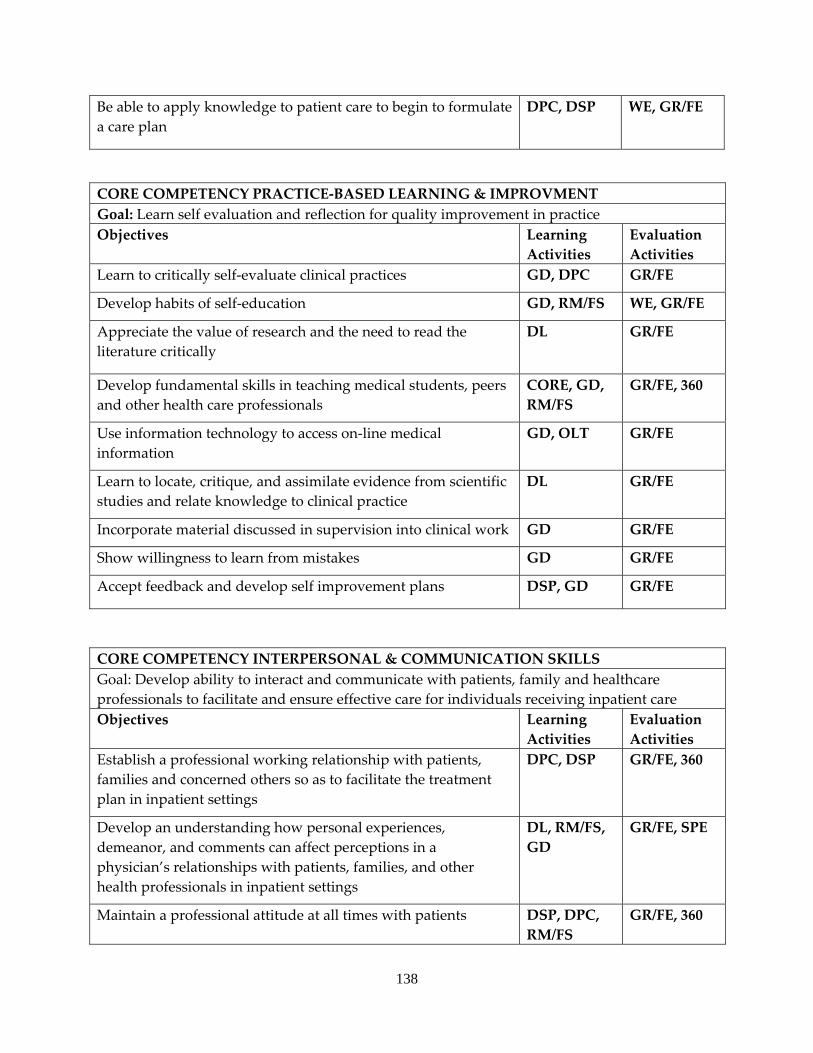
138
Be able to apply knowledge to patient care to begin to formulate a care plan
DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Learn self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Learn to critically self‐evaluate clinical practices GD, DPC GR/FE
Develop habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Develop fundamental skills in teaching medical students, peers and other health care professionals
CORE, GD, RM/FS
GR/FE, 360
Use information technology to access on‐line medical information
GD, OLT GR/FE
Learn to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
Develop an understanding how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, RM/FS, GD
GR/FE, SPE
Maintain a professional attitude at all times with patients DSP, DPC, RM/FS
GR/FE, 360
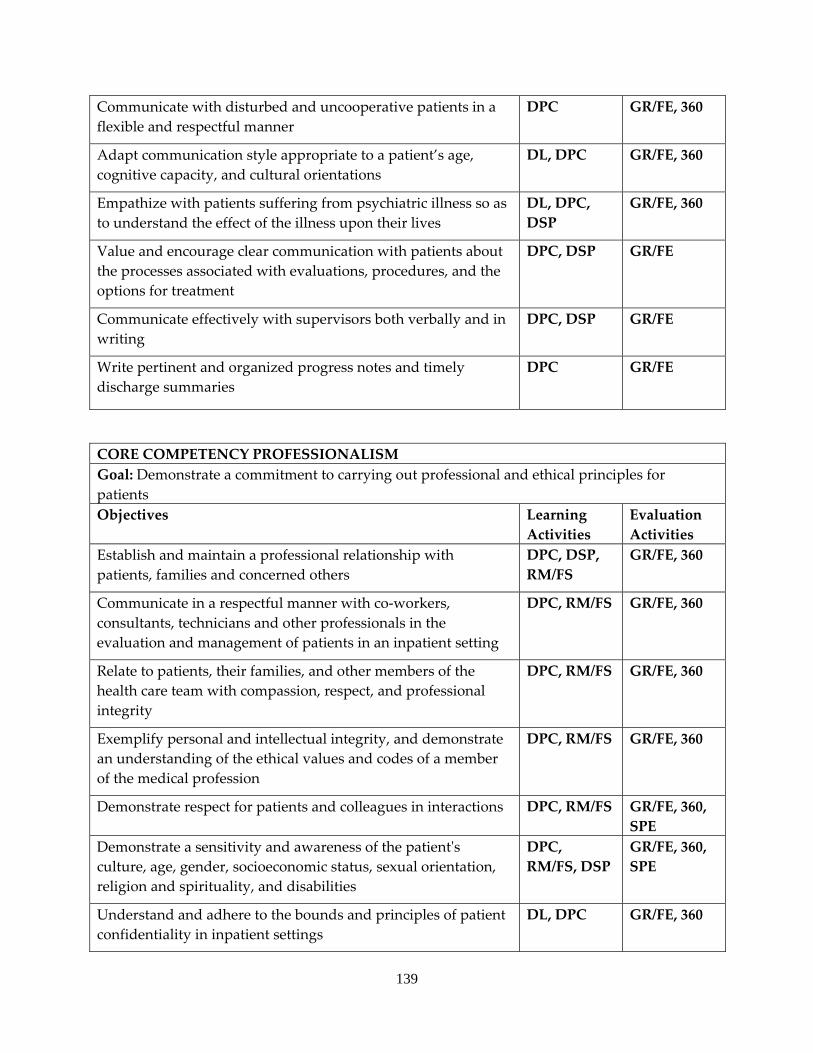
139
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors both verbally and in writing
DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
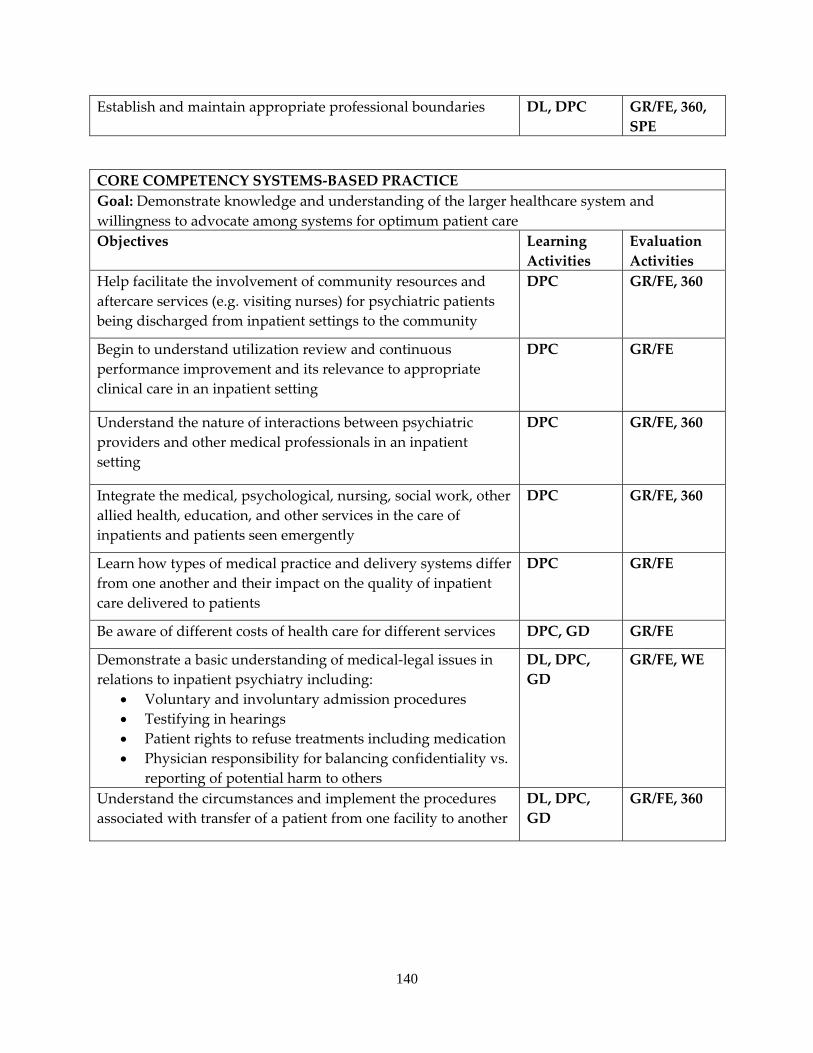
140
Establish and maintain appropriate professional boundaries DL, DPC GR/FE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient careObjectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC GR/FE, 360
Begin to understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Learn how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate a basic understanding of medical‐legal issues in relations to inpatient psychiatry including:
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others
DL, DPC, GD
GR/FE, WE
Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360
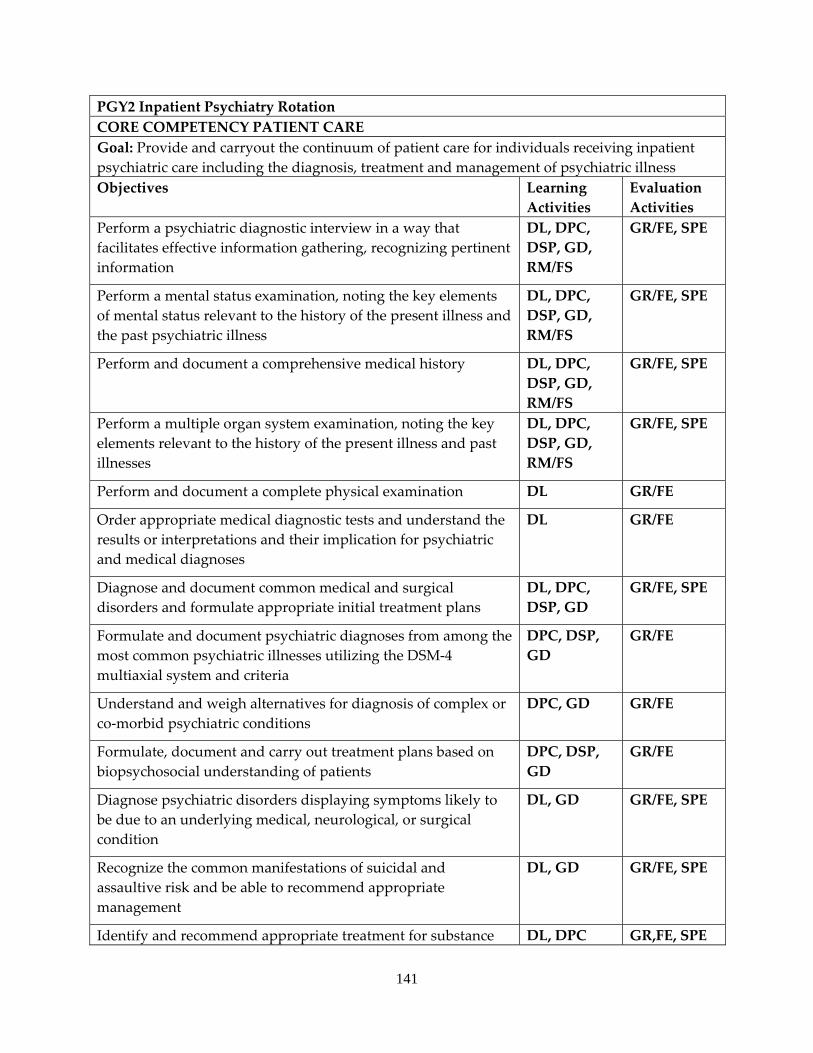
141
PGY2 Inpatient Psychiatry Rotation CORE COMPETENCY PATIENT CARE Goal: Provide and carryout the continuum of patient care for individuals receiving inpatient psychiatric care including the diagnosis, treatment and management of psychiatric illnessObjectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview in a way that facilitates effective information gathering, recognizing pertinent information
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a mental status examination, noting the key elements of mental status relevant to the history of the present illness and the past psychiatric illness
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a comprehensive medical history DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform a multiple organ system examination, noting the key elements relevant to the history of the present illness and past illnesses
DL, DPC, DSP, GD, RM/FS
GR/FE, SPE
Perform and document a complete physical examination DL GR/FE
Order appropriate medical diagnostic tests and understand the results or interpretations and their implication for psychiatric and medical diagnoses
DL GR/FE
Diagnose and document common medical and surgical disorders and formulate appropriate initial treatment plans
DL, DPC, DSP, GD
GR/FE, SPE
Formulate and document psychiatric diagnoses from among the most common psychiatric illnesses utilizing the DSM‐4 multiaxial system and criteria
DPC, DSP, GD
GR/FE
Understand and weigh alternatives for diagnosis of complex or co‐morbid psychiatric conditions
DPC, GD GR/FE
Formulate, document and carry out treatment plans based on biopsychosocial understanding of patients
DPC, DSP, GD
GR/FE
Diagnose psychiatric disorders displaying symptoms likely to be due to an underlying medical, neurological, or surgical condition
DL, GD GR/FE, SPE
Recognize the common manifestations of suicidal and assaultive risk and be able to recommend appropriate management
DL, GD GR/FE, SPE
Identify and recommend appropriate treatment for substance DL, DPC GR,FE, SPE
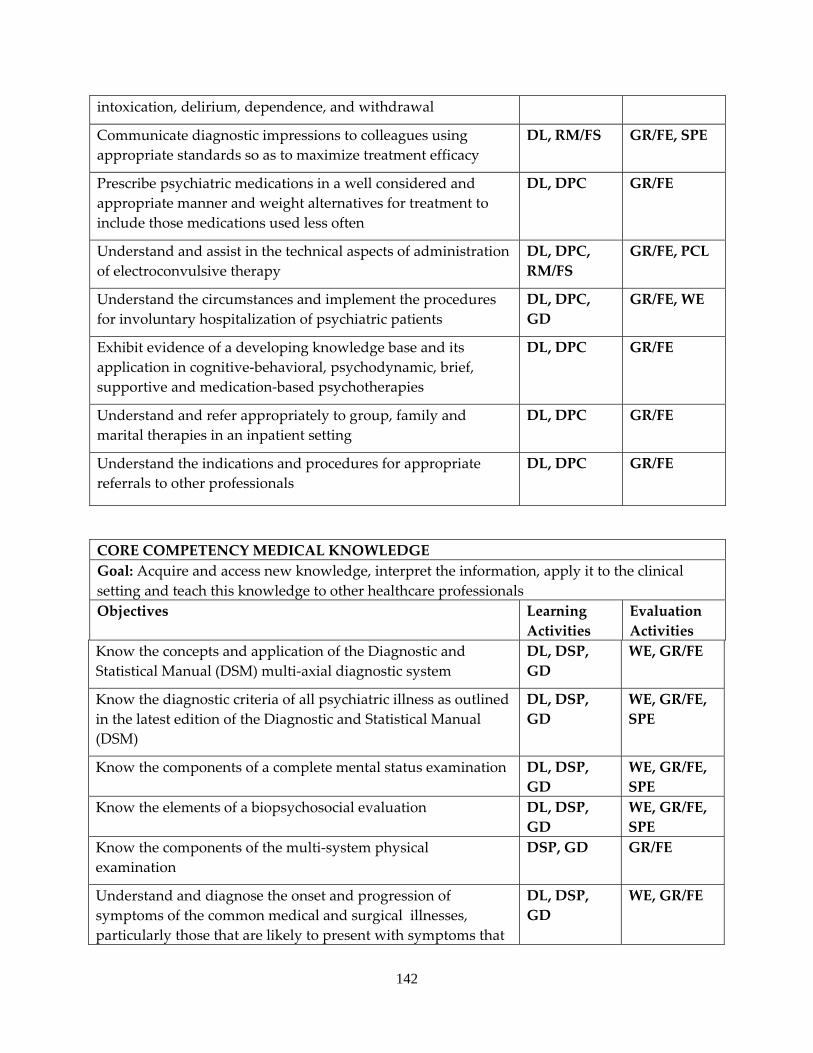
142
intoxication, delirium, dependence, and withdrawal
Communicate diagnostic impressions to colleagues using appropriate standards so as to maximize treatment efficacy
DL, RM/FS GR/FE, SPE
Prescribe psychiatric medications in a well considered and appropriate manner and weight alternatives for treatment to include those medications used less often
DL, DPC GR/FE
Understand and assist in the technical aspects of administration of electroconvulsive therapy
DL, DPC, RM/FS
GR/FE, PCL
Understand the circumstances and implement the procedures for involuntary hospitalization of psychiatric patients
DL, DPC, GD
GR/FE, WE
Exhibit evidence of a developing knowledge base and its application in cognitive‐behavioral, psychodynamic, brief, supportive and medication‐based psychotherapies
DL, DPC GR/FE
Understand and refer appropriately to group, family and marital therapies in an inpatient setting
DL, DPC GR/FE
Understand the indications and procedures for appropriate referrals to other professionals
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionals Objectives Learning
Activities Evaluation Activities
Know the concepts and application of the Diagnostic and Statistical Manual (DSM) multi‐axial diagnostic system
DL, DSP, GD
WE, GR/FE
Know the diagnostic criteria of all psychiatric illness as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL, DSP, GD
WE, GR/FE, SPE
Know the components of a complete mental status examination DL, DSP, GD
WE, GR/FE, SPE
Know the elements of a biopsychosocial evaluation DL, DSP, GD
WE, GR/FE, SPE
Know the components of the multi‐system physical examination
DSP, GD GR/FE
Understand and diagnose the onset and progression of symptoms of the common medical and surgical illnesses, particularly those that are likely to present with symptoms that
DL, DSP, GD
WE, GR/FE
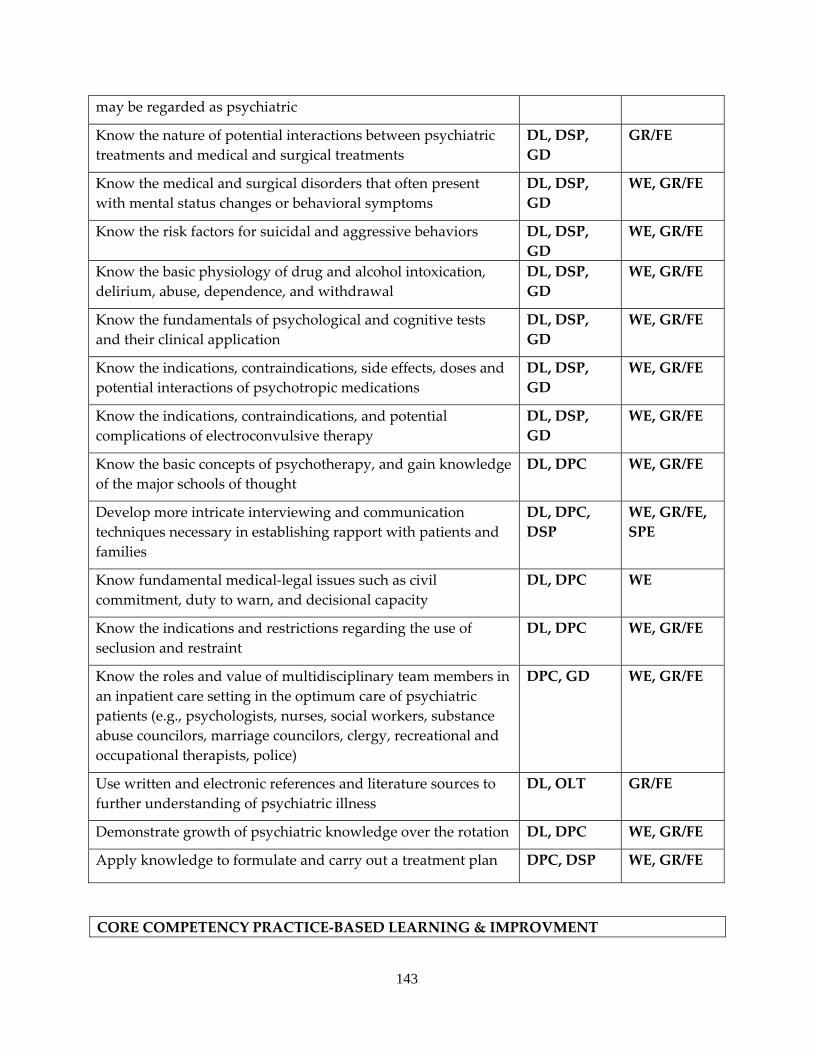
143
may be regarded as psychiatric
Know the nature of potential interactions between psychiatric treatments and medical and surgical treatments
DL, DSP, GD
GR/FE
Know the medical and surgical disorders that often present with mental status changes or behavioral symptoms
DL, DSP, GD
WE, GR/FE
Know the risk factors for suicidal and aggressive behaviors DL, DSP, GD
WE, GR/FE
Know the basic physiology of drug and alcohol intoxication, delirium, abuse, dependence, and withdrawal
DL, DSP, GD
WE, GR/FE
Know the fundamentals of psychological and cognitive tests and their clinical application
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, side effects, doses and potential interactions of psychotropic medications
DL, DSP, GD
WE, GR/FE
Know the indications, contraindications, and potential complications of electroconvulsive therapy
DL, DSP, GD
WE, GR/FE
Know the basic concepts of psychotherapy, and gain knowledge of the major schools of thought
DL, DPC WE, GR/FE
Develop more intricate interviewing and communication techniques necessary in establishing rapport with patients and families
DL, DPC, DSP
WE, GR/FE, SPE
Know fundamental medical‐legal issues such as civil commitment, duty to warn, and decisional capacity
DL, DPC WE
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC WE, GR/FE
Know the roles and value of multidisciplinary team members in an inpatient care setting in the optimum care of psychiatric patients (e.g., psychologists, nurses, social workers, substance abuse councilors, marriage councilors, clergy, recreational and occupational therapists, police)
DPC, GD WE, GR/FE
Use written and electronic references and literature sources to further understanding of psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation DL, DPC WE, GR/FE
Apply knowledge to formulate and carry out a treatment plan DPC, DSP WE, GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT
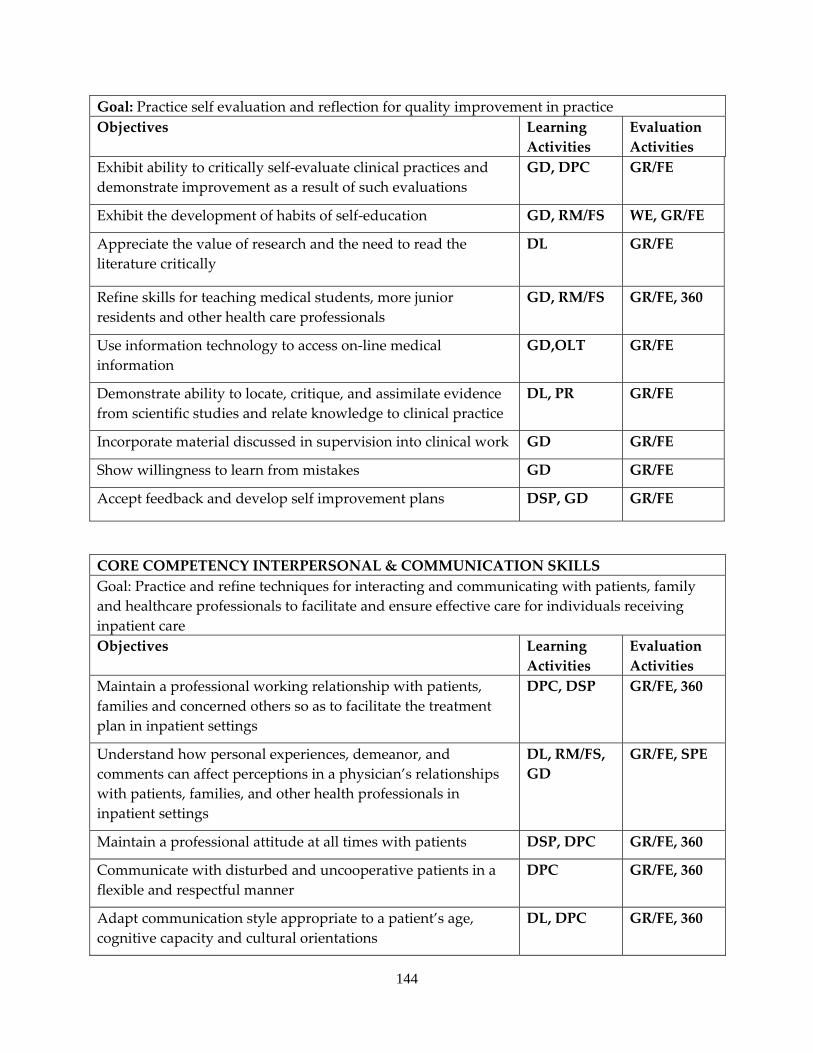
144
Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Exhibit ability to critically self‐evaluate clinical practices and demonstrate improvement as a result of such evaluations
GD, DPC GR/FE
Exhibit the development of habits of self‐education GD, RM/FS WE, GR/FE
Appreciate the value of research and the need to read the literature critically
DL GR/FE
Refine skills for teaching medical students, more junior residents and other health care professionals
GD, RM/FS GR/FE, 360
Use information technology to access on‐line medical information
GD,OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, PR GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Practice and refine techniques for interacting and communicating with patients, family and healthcare professionals to facilitate and ensure effective care for individuals receiving inpatient care Objectives Learning
Activities Evaluation Activities
Maintain a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan in inpatient settings
DPC, DSP GR/FE, 360
Understand how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals in inpatient settings
DL, RM/FS, GD
GR/FE, SPE
Maintain a professional attitude at all times with patients DSP, DPC GR/FE, 360
Communicate with disturbed and uncooperative patients in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity and cultural orientations
DL, DPC GR/FE, 360
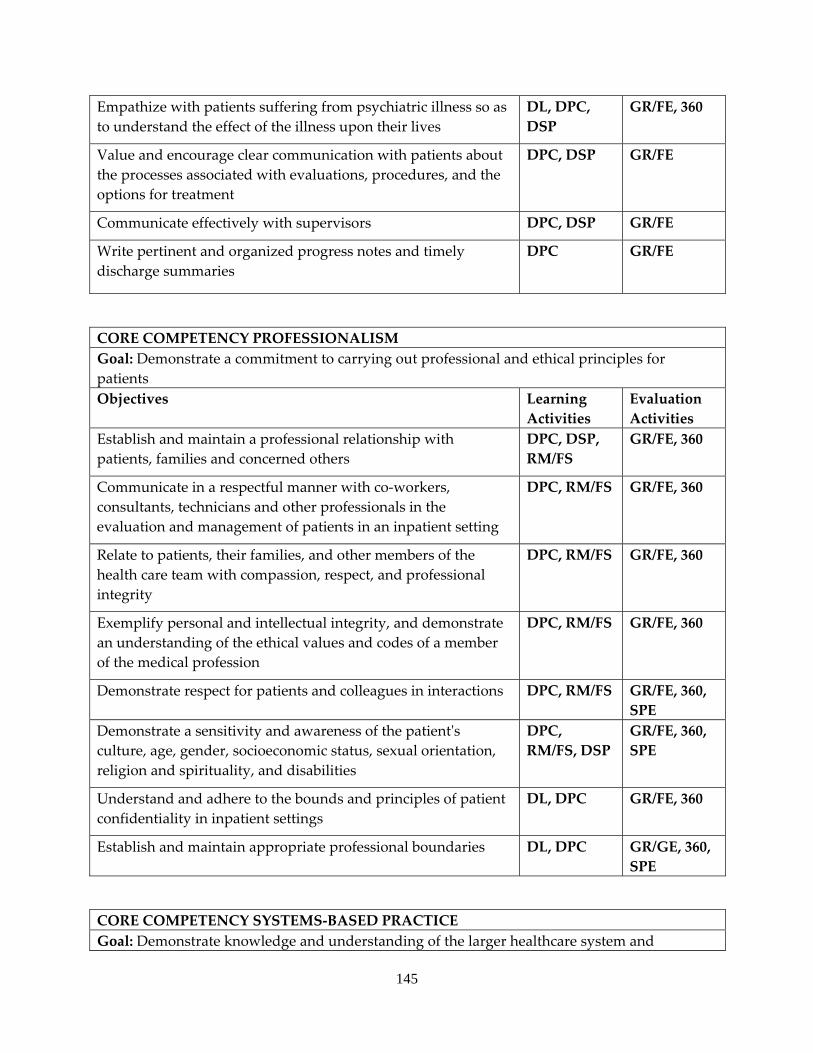
145
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations, procedures, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors DPC, DSP GR/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients in an inpatient setting
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Understand and adhere to the bounds and principles of patient confidentiality in inpatient settings
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/GE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and
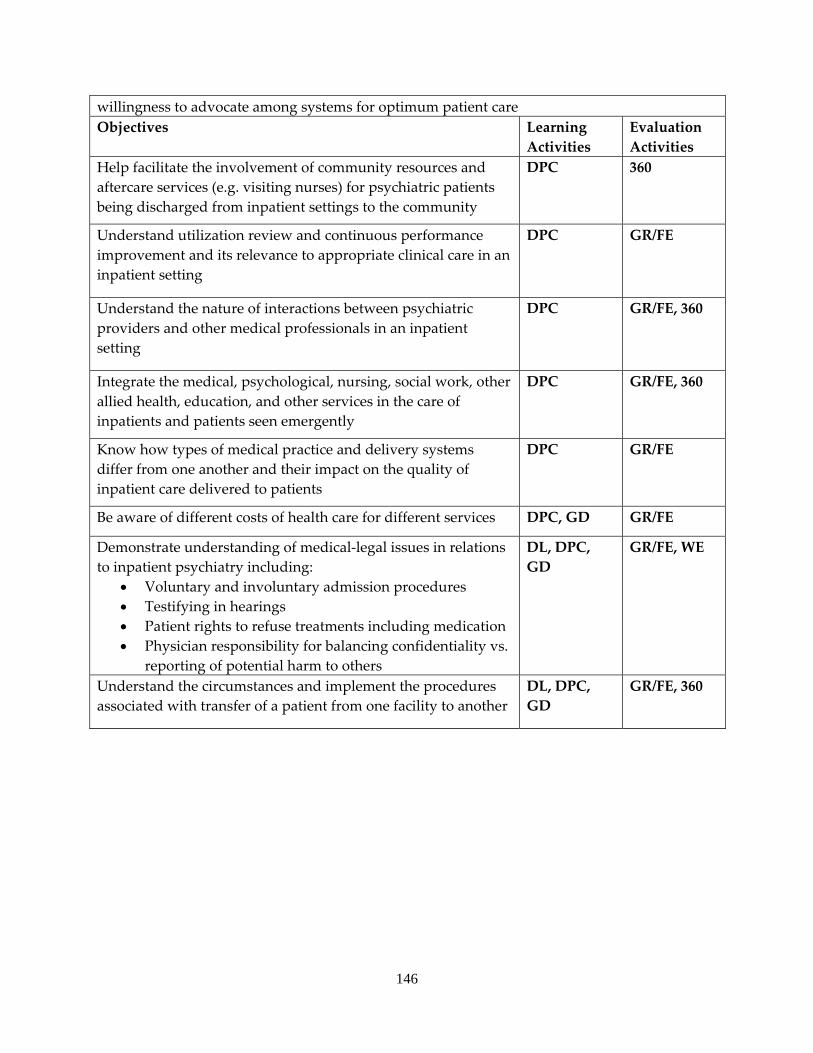
146
willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g. visiting nurses) for psychiatric patients being discharged from inpatient settings to the community
DPC 360
Understand utilization review and continuous performance improvement and its relevance to appropriate clinical care in an inpatient setting
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals in an inpatient setting
DPC GR/FE, 360
Integrate the medical, psychological, nursing, social work, other allied health, education, and other services in the care of inpatients and patients seen emergently
DPC GR/FE, 360
Know how types of medical practice and delivery systems differ from one another and their impact on the quality of inpatient care delivered to patients
DPC GR/FE
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate understanding of medical‐legal issues in relations to inpatient psychiatry including:
• Voluntary and involuntary admission procedures • Testifying in hearings • Patient rights to refuse treatments including medication • Physician responsibility for balancing confidentiality vs.
reporting of potential harm to others
DL, DPC, GD
GR/FE, WE
Understand the circumstances and implement the procedures associated with transfer of a patient from one facility to another
DL, DPC, GD
GR/FE, 360
147
JOHNSON COUNTY MENTAL HEALTH CENTER (Community Mental Health Affiliate)
a. ADULT PSYCHIATRY OUTPATIENT SERVICE b. Required continuous half‐time 6 month rotation usually occurring in the PGY3 year. c. Supervising Faculty consists of three full‐time psychiatrists, all of whom are board
certified. One is the Medical Director of the Mental Health Center. The residents also work closely with nursing staff, an advanced registered nurse practitioner, therapists, and case management staff.
d. The residents spend 8‐9 hours a week at KUMC in formal didactics, grand rounds and interviewing skills conferences. At the mental health center, the residents divide their time between a general Outpatient Office and the Community Support Services Office (which serves only chronically ill patients classified with severe and persistent mental illness). All new patient evaluations (averaging 3 new patients per week) are thoroughly reviewed, supervised, and re‐evaluated by the mental health center psychiatrists with an emphasis on diagnosis and management. Supervisors are available for consultations; case loads are carefully monitored and controlled for both breadth and variety of experience. The staff psychiatrists review and countersign all resident documentation. The Medical Director and the other 2 supervising psychiatrists of the mental health center hold faculty appointments at KUMC. The Medical Director is responsible for ensuring that residents receive adequate supervision and quality of education while on site.
e. The mental health center served almost 11,000 clients in 2009. The clinical population is comprised of all age groups. Sixty‐nine percent of the clients are over the age of 18. Twenty‐three percent are 18‐29 years; thirty‐eight percent are ages 30‐54, six percent are ages 55‐64 and two percent are over the age of 65. The male: female ratio is 49:51. 11 percent are African American; 5 percent are Hispanic, 1.5 percent Asian, and 0.7 percent Native American. A further 0.8 percent represents other minorities, with the remainder being Caucasian. Two to three percent of the population receiving services is homeless and 2.8 percent are hearing impaired. 81 percent of the patients have an income of $25,000 or less per annum. Caseloads represent a variety of diagnoses, but there tends to be a heavy representation of major depression, schizophrenia, schizoaffective disorder, bipolar disorder, anxiety disorders and borderline personality disorder. Twenty‐two percent of the clients are dually diagnosed with substance abuse, and another three percent with mental retardation, in addition to severe mental illness.
f. An average caseload for each resident is 130 patients. g. All residents receive clinical supervision throughout the day on a case‐by‐case basis
from the mental health center medical director and/or staff psychiatrist to whom the clinic is assigned. In addition to the supervision of patient care, the residents receive individual supervision for one hour each per week (protected time) with an assigned psychiatrist mentor.
h. This rotation is done concurrently with a 0.5 FTE assignment to the adult outpatient clinic at KUMC. The experience at the mental health center helps to considerably
148
broaden the resident’s exposure to working with varied socio‐economic groups, including the indigent and homeless, with diverse ethnic groups, and with patients suffering from severe and persistent mental illness. The Mental health Center serves as a safety net for the Johnson County, and takes all comers. These, often very psychiatrically ill, clients are maintained as much as possible in the community, utilizing 24‐hour emergency services, case management services, respite care, and attendant care services. Special services for the aged, the deaf and hard of hearing, criminal offenders, and victims of sexual abuse are also important sub‐populations unique to the mental health center setting. There is also vital exchange between the residents and staff regarding the special issues related to long term outpatient commitment, leadership of an interdisciplinary teams, and consultation with community agencies, such as the jail.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: OUTPATIENT ADULT PSYCHIATRY LEVEL: PGY3 DURATION: 6 MONTHS‐ PART TIME (PGY3) SITE: JOHNSON COUNTY MENTAL HEALTH CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT JOHNSON COUNTY MENTAL HEALTH CENTER By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
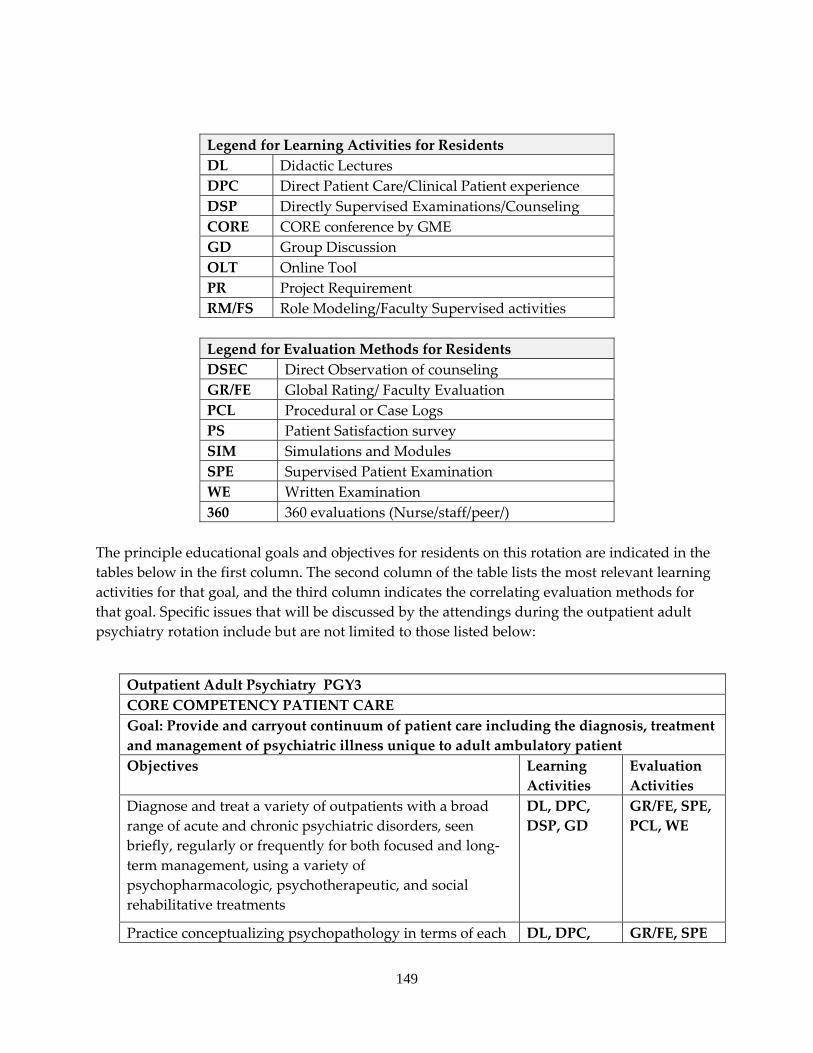
149
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the outpatient adult psychiatry rotation include but are not limited to those listed below:
Outpatient Adult Psychiatry PGY3 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to adult ambulatory patient Objectives Learning
Activities Evaluation Activities
Diagnose and treat a variety of outpatients with a broad range of acute and chronic psychiatric disorders, seen briefly, regularly or frequently for both focused and long‐term management, using a variety of psychopharmacologic, psychotherapeutic, and social rehabilitative treatments
DL, DPC, DSP, GD
GR/FE, SPE, PCL, WE
Practice conceptualizing psychopathology in terms of each DL, DPC, GR/FE, SPE
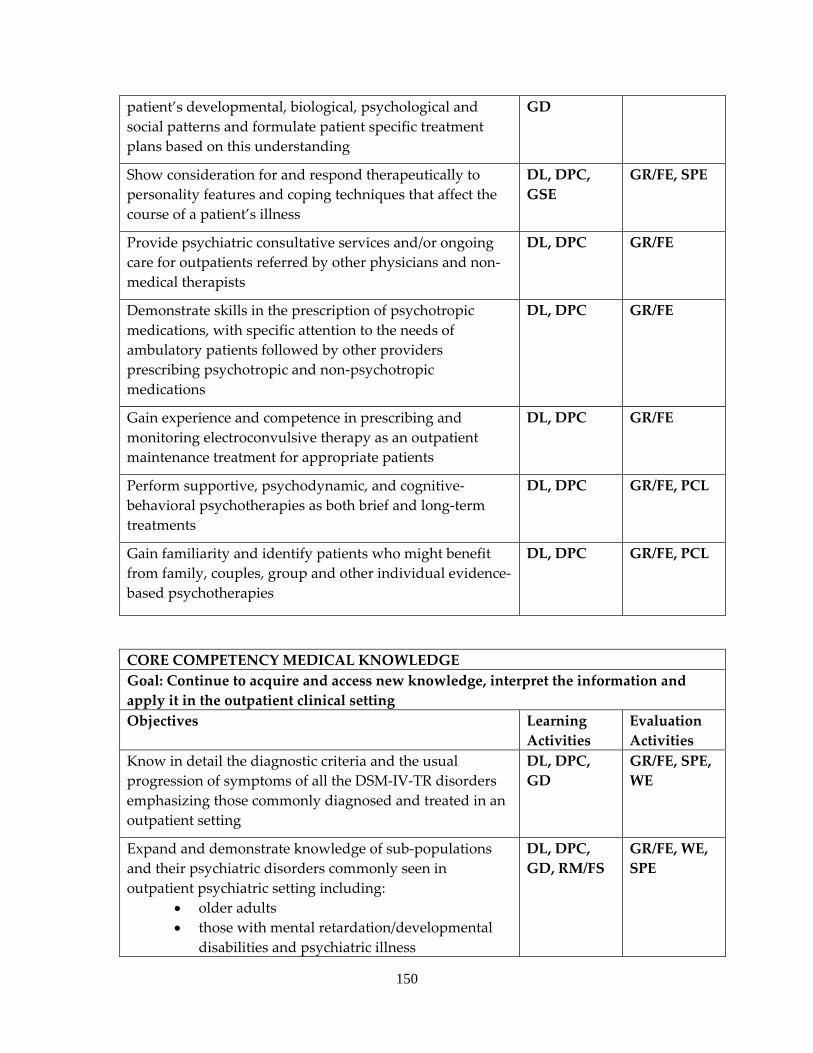
150
patient’s developmental, biological, psychological and social patterns and formulate patient specific treatment plans based on this understanding
GD
Show consideration for and respond therapeutically to personality features and coping techniques that affect the course of a patient’s illness
DL, DPC, GSE
GR/FE, SPE
Provide psychiatric consultative services and/or ongoing care for outpatients referred by other physicians and non‐medical therapists
DL, DPC GR/FE
Demonstrate skills in the prescription of psychotropic medications, with specific attention to the needs of ambulatory patients followed by other providers prescribing psychotropic and non‐psychotropic medications
DL, DPC GR/FE
Gain experience and competence in prescribing and monitoring electroconvulsive therapy as an outpatient maintenance treatment for appropriate patients
DL, DPC GR/FE
Perform supportive, psychodynamic, and cognitive‐behavioral psychotherapies as both brief and long‐term treatments
DL, DPC GR/FE, PCL
Gain familiarity and identify patients who might benefit from family, couples, group and other individual evidence‐based psychotherapies
DL, DPC GR/FE, PCL
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Continue to acquire and access new knowledge, interpret the information and apply it in the outpatient clinical setting Objectives Learning
Activities Evaluation Activities
Know in detail the diagnostic criteria and the usual progression of symptoms of all the DSM‐IV‐TR disorders emphasizing those commonly diagnosed and treated in an outpatient setting
DL, DPC, GD
GR/FE, SPE, WE
Expand and demonstrate knowledge of sub‐populations and their psychiatric disorders commonly seen in outpatient psychiatric setting including:
• older adults • those with mental retardation/developmental
disabilities and psychiatric illness
DL, DPC, GD, RM/FS
GR/FE, WE, SPE
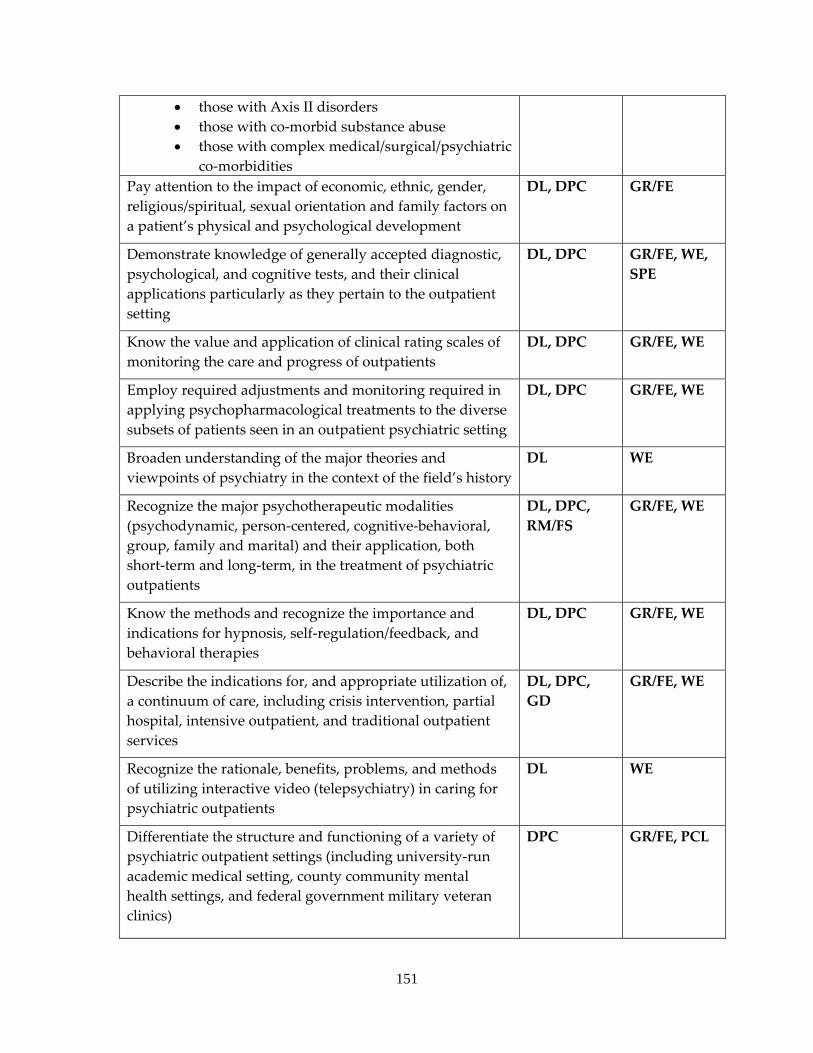
151
• those with Axis II disorders • those with co‐morbid substance abuse • those with complex medical/surgical/psychiatric
co‐morbidities Pay attention to the impact of economic, ethnic, gender, religious/spiritual, sexual orientation and family factors on a patient’s physical and psychological development
DL, DPC GR/FE
Demonstrate knowledge of generally accepted diagnostic, psychological, and cognitive tests, and their clinical applications particularly as they pertain to the outpatient setting
DL, DPC GR/FE, WE, SPE
Know the value and application of clinical rating scales of monitoring the care and progress of outpatients
DL, DPC GR/FE, WE
Employ required adjustments and monitoring required in applying psychopharmacological treatments to the diverse subsets of patients seen in an outpatient psychiatric setting
DL, DPC GR/FE, WE
Broaden understanding of the major theories and viewpoints of psychiatry in the context of the field’s history
DL WE
Recognize the major psychotherapeutic modalities (psychodynamic, person‐centered, cognitive‐behavioral, group, family and marital) and their application, both short‐term and long‐term, in the treatment of psychiatric outpatients
DL, DPC, RM/FS
GR/FE, WE
Know the methods and recognize the importance and indications for hypnosis, self‐regulation/feedback, and behavioral therapies
DL, DPC GR/FE, WE
Describe the indications for, and appropriate utilization of, a continuum of care, including crisis intervention, partial hospital, intensive outpatient, and traditional outpatient services
DL, DPC, GD
GR/FE, WE
Recognize the rationale, benefits, problems, and methods of utilizing interactive video (telepsychiatry) in caring for psychiatric outpatients
DL WE
Differentiate the structure and functioning of a variety of psychiatric outpatient settings (including university‐run academic medical setting, county community mental health settings, and federal government military veteran clinics)
DPC GR/FE, PCL
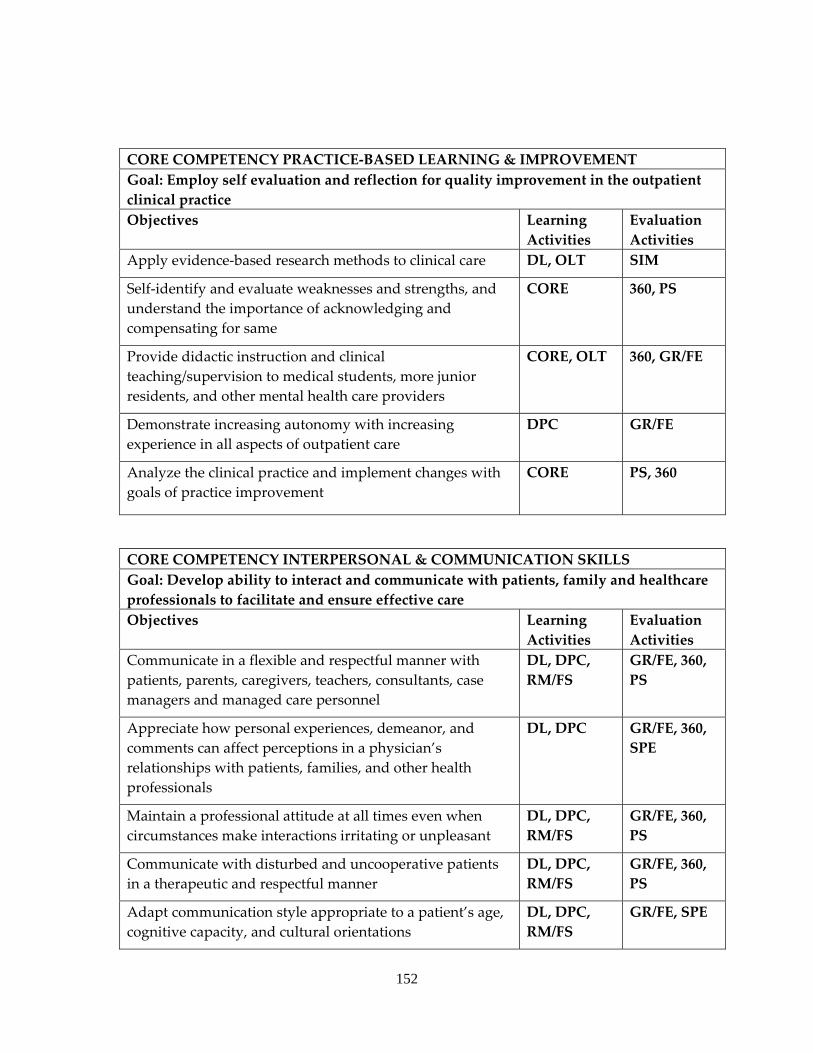
152
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Employ self evaluation and reflection for quality improvement in the outpatient clinical practice Objectives Learning
Activities Evaluation Activities
Apply evidence‐based research methods to clinical care DL, OLT SIM
Self‐identify and evaluate weaknesses and strengths, and understand the importance of acknowledging and compensating for same
CORE 360, PS
Provide didactic instruction and clinical teaching/supervision to medical students, more junior residents, and other mental health care providers
CORE, OLT 360, GR/FE
Demonstrate increasing autonomy with increasing experience in all aspects of outpatient care
DPC GR/FE
Analyze the clinical practice and implement changes with goals of practice improvement
CORE PS, 360
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care Objectives Learning
Activities Evaluation Activities
Communicate in a flexible and respectful manner with patients, parents, caregivers, teachers, consultants, case managers and managed care personnel
DL, DPC, RM/FS
GR/FE, 360, PS
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times even when circumstances make interactions irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360, PS
Communicate with disturbed and uncooperative patients in a therapeutic and respectful manner
DL, DPC, RM/FS
GR/FE, 360, PS
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
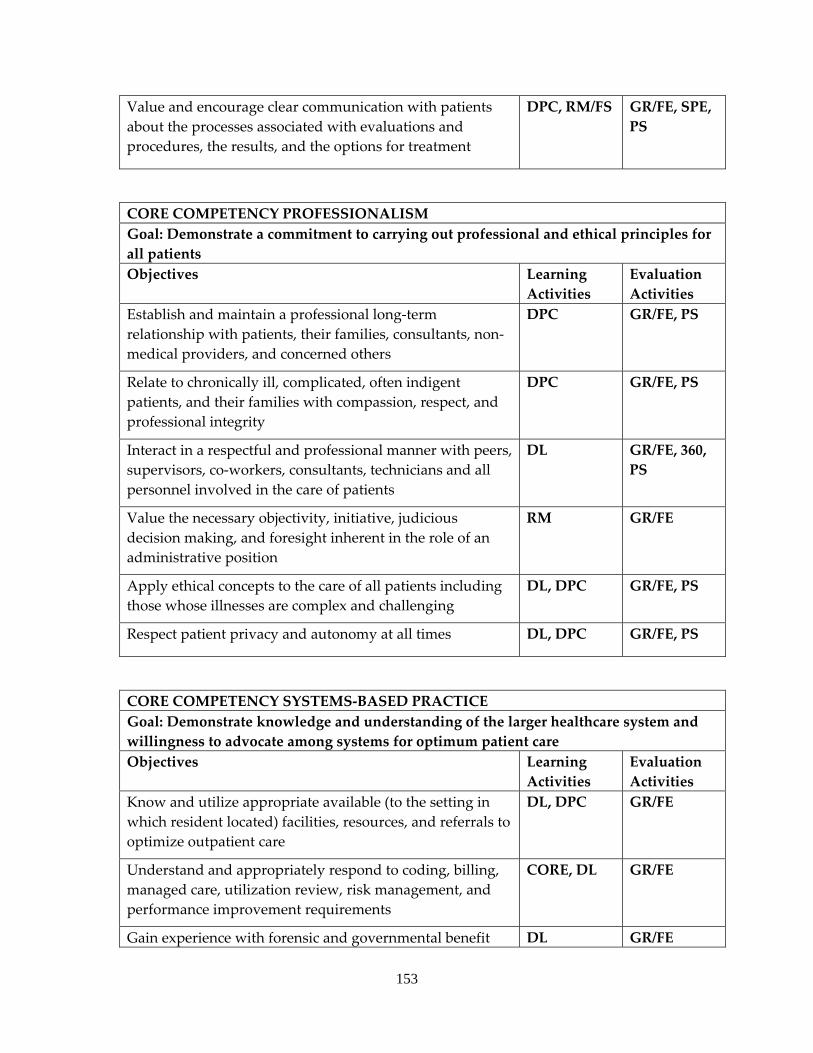
153
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, RM/FS GR/FE, SPE, PS
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for all patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional long‐term relationship with patients, their families, consultants, non‐medical providers, and concerned others
DPC GR/FE, PS
Relate to chronically ill, complicated, often indigent patients, and their families with compassion, respect, and professional integrity
DPC GR/FE, PS
Interact in a respectful and professional manner with peers, supervisors, co‐workers, consultants, technicians and all personnel involved in the care of patients
DL GR/FE, 360, PS
Value the necessary objectivity, initiative, judicious decision making, and foresight inherent in the role of an administrative position
RM GR/FE
Apply ethical concepts to the care of all patients including those whose illnesses are complex and challenging
DL, DPC GR/FE, PS
Respect patient privacy and autonomy at all times DL, DPC GR/FE, PS
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Know and utilize appropriate available (to the setting in which resident located) facilities, resources, and referrals to optimize outpatient care
DL, DPC GR/FE
Understand and appropriately respond to coding, billing, managed care, utilization review, risk management, and performance improvement requirements
CORE, DL GR/FE
Gain experience with forensic and governmental benefit DL GR/FE
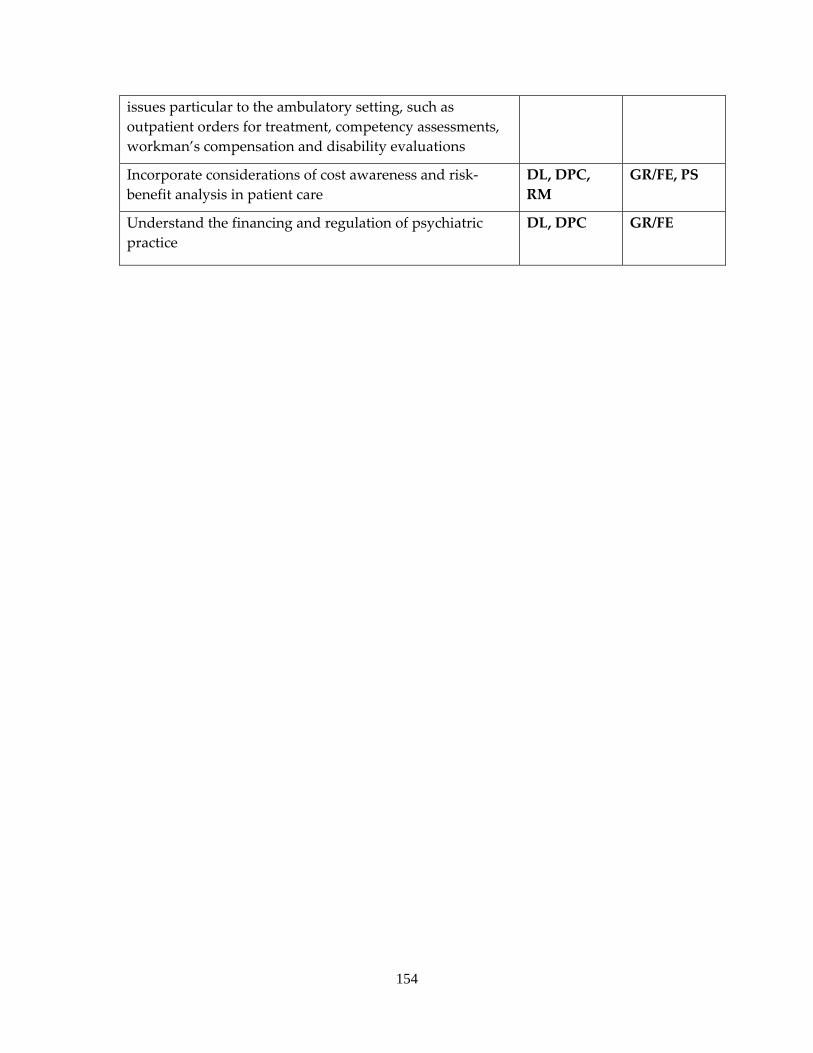
154
issues particular to the ambulatory setting, such as outpatient orders for treatment, competency assessments, workman’s compensation and disability evaluations
Incorporate considerations of cost awareness and risk‐benefit analysis in patient care
DL, DPC, RM
GR/FE, PS
Understand the financing and regulation of psychiatric practice
DL, DPC GR/FE
155
a. COMMUNITY PSYCHIATRY b. A required one month rotation usually occurring in the PGY3 or PGY4. Residents
may arrange for an additional elective experience in their PGY4 year. c. The primary faculty consists of the full‐time medical director of Johnson County or
Wyandot Mental Health Center, as well as part‐time psychiatrists, psychologists, and social workers employed by the mental health centers who may be assigned specific supervisory roles.
d. The residents learn the structure and functioning of community psychiatry through meetings with unit directors/supervisors, during which the composition and functioning of each unit is described. Each unitʹs connection with other mental health center units, and other community agencies and resources, are explored. They are involved in psychiatric evaluation, medication management, case management, and diversion from hospitalization of patients. They attend physician staff meetings, interdisciplinary review meetings and utilization review meetings. These experiences occur in conjunction with the Community Support Service, Outpatient, Family Focus, Deaf and Hard of Hearing, Adolescent and Sexual Abuse Treatment Units. They accompany mental health center staff as they work with clients in the community on problems ranging from emotional stress to budgeting money and securing housing. In addition, residents attend four hours of didactic lectures, weekly KUMC Journal Club and Psychiatry Grand Rounds, and receive two hours of individual supervision.
e. The mental health centers each serve over 5,000 clients a year. Thirteen to fourteen hundred of these are under age 18. Fifty‐two percent are female and forty‐eight percent are male. Eighty percent of those served have a family income of less than $20,000 per year. Ninety percent of the clients are Caucasian with the remaining 10% being African‐American, Hispanic and Asian. Special populations served include the hearing impaired, families in crisis, sexual abuse victims, the chronically and persistently mentally ill, and those on court referral. The patients seen suffer from a wide variety of psychiatric diagnoses.
f. Each resident is involved with approximately 30‐40 cases during the month rotation. g. Supervision of residents is coordinated by the Medical Director of the mental health
centers with teaching by various members of the interdisciplinary team.
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: COMMUNITY PSYCHIATRY LEVEL: PGY2 OR PGY4 DURATION: 1 MONTH SITE: JOHNSON COUNTY MENTAL HEALTH CENTER SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT JOHNSON COUNTY MENTAL HEALTH CENTER
156
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
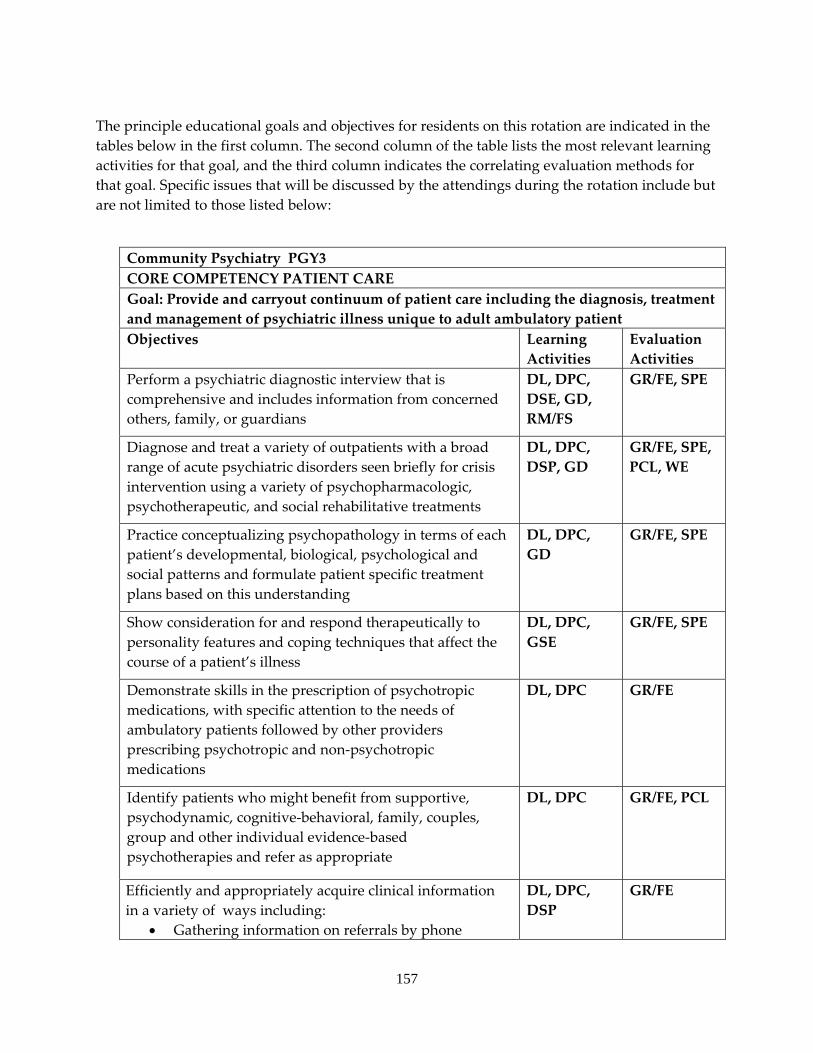
157
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the rotation include but are not limited to those listed below:
Community Psychiatry PGY3 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to adult ambulatory patient Objectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview that is comprehensive and includes information from concerned others, family, or guardians
DL, DPC, DSE, GD, RM/FS
GR/FE, SPE
Diagnose and treat a variety of outpatients with a broad range of acute psychiatric disorders seen briefly for crisis intervention using a variety of psychopharmacologic, psychotherapeutic, and social rehabilitative treatments
DL, DPC, DSP, GD
GR/FE, SPE, PCL, WE
Practice conceptualizing psychopathology in terms of each patient’s developmental, biological, psychological and social patterns and formulate patient specific treatment plans based on this understanding
DL, DPC, GD
GR/FE, SPE
Show consideration for and respond therapeutically to personality features and coping techniques that affect the course of a patient’s illness
DL, DPC, GSE
GR/FE, SPE
Demonstrate skills in the prescription of psychotropic medications, with specific attention to the needs of ambulatory patients followed by other providers prescribing psychotropic and non‐psychotropic medications
DL, DPC GR/FE
Identify patients who might benefit from supportive, psychodynamic, cognitive‐behavioral, family, couples, group and other individual evidence‐based psychotherapies and refer as appropriate
DL, DPC GR/FE, PCL
Efficiently and appropriately acquire clinical information in a variety of ways including:
• Gathering information on referrals by phone
DL, DPC, DSP
GR/FE
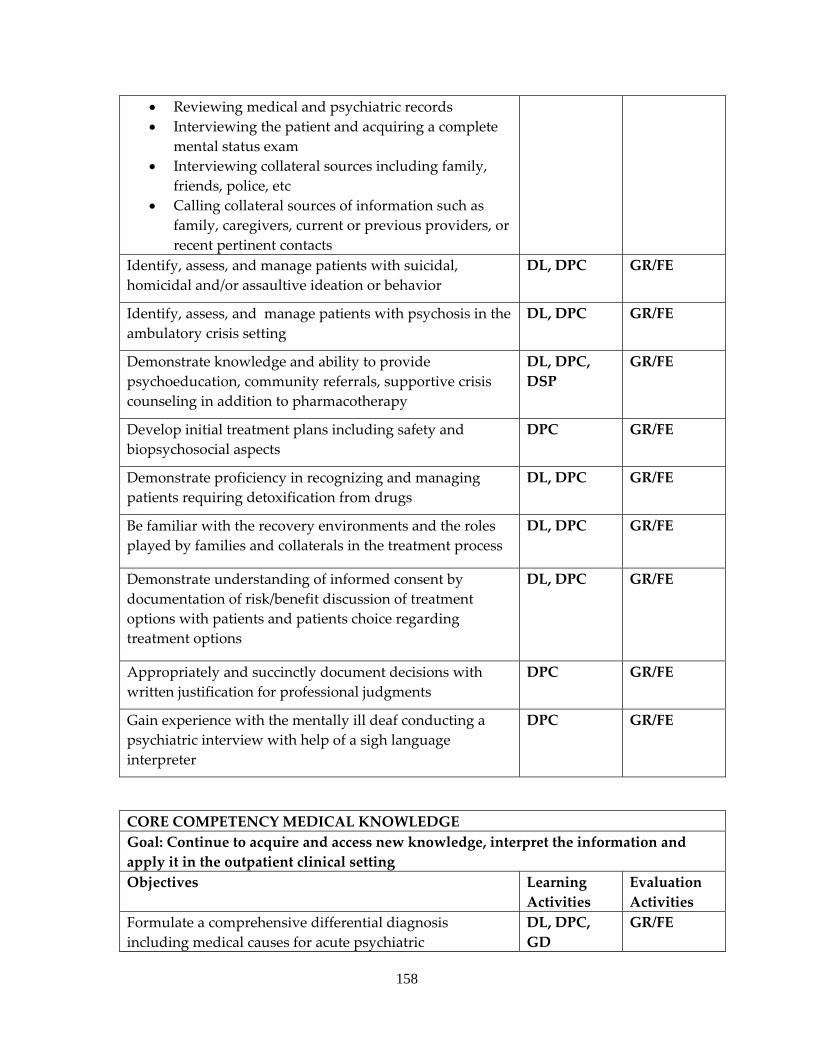
158
• Reviewing medical and psychiatric records • Interviewing the patient and acquiring a complete
mental status exam • Interviewing collateral sources including family,
friends, police, etc • Calling collateral sources of information such as
family, caregivers, current or previous providers, or recent pertinent contacts
Identify, assess, and manage patients with suicidal, homicidal and/or assaultive ideation or behavior
DL, DPC GR/FE
Identify, assess, and manage patients with psychosis in the ambulatory crisis setting
DL, DPC GR/FE
Demonstrate knowledge and ability to provide psychoeducation, community referrals, supportive crisis counseling in addition to pharmacotherapy
DL, DPC, DSP
GR/FE
Develop initial treatment plans including safety and biopsychosocial aspects
DPC GR/FE
Demonstrate proficiency in recognizing and managing patients requiring detoxification from drugs
DL, DPC GR/FE
Be familiar with the recovery environments and the roles played by families and collaterals in the treatment process
DL, DPC GR/FE
Demonstrate understanding of informed consent by documentation of risk/benefit discussion of treatment options with patients and patients choice regarding treatment options
DL, DPC GR/FE
Appropriately and succinctly document decisions with written justification for professional judgments
DPC GR/FE
Gain experience with the mentally ill deaf conducting a psychiatric interview with help of a sigh language interpreter
DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Continue to acquire and access new knowledge, interpret the information and apply it in the outpatient clinical setting Objectives Learning
Activities Evaluation Activities
Formulate a comprehensive differential diagnosis including medical causes for acute psychiatric
DL, DPC, GD
GR/FE
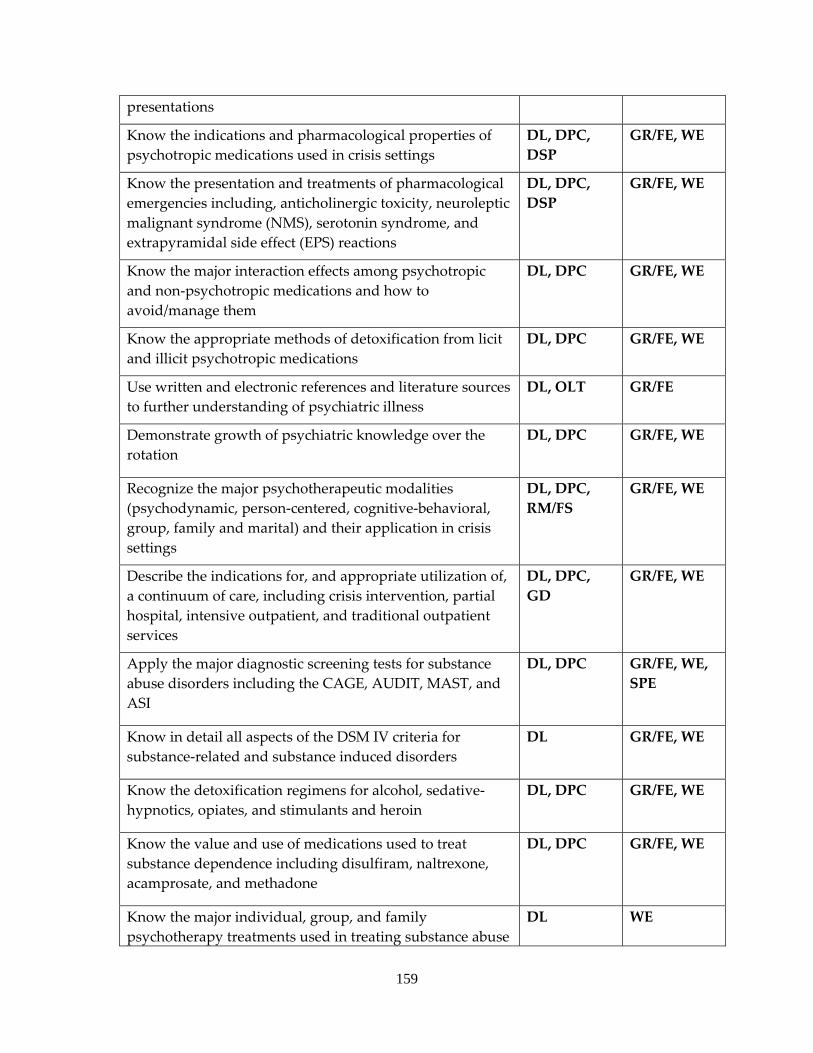
159
presentations
Know the indications and pharmacological properties of psychotropic medications used in crisis settings
DL, DPC, DSP
GR/FE, WE
Know the presentation and treatments of pharmacological emergencies including, anticholinergic toxicity, neuroleptic malignant syndrome (NMS), serotonin syndrome, and extrapyramidal side effect (EPS) reactions
DL, DPC, DSP
GR/FE, WE
Know the major interaction effects among psychotropic and non‐psychotropic medications and how to avoid/manage them
DL, DPC GR/FE, WE
Know the appropriate methods of detoxification from licit and illicit psychotropic medications
DL, DPC GR/FE, WE
Use written and electronic references and literature sources to further understanding of psychiatric illness
DL, OLT GR/FE
Demonstrate growth of psychiatric knowledge over the rotation
DL, DPC GR/FE, WE
Recognize the major psychotherapeutic modalities (psychodynamic, person‐centered, cognitive‐behavioral, group, family and marital) and their application in crisis settings
DL, DPC, RM/FS
GR/FE, WE
Describe the indications for, and appropriate utilization of, a continuum of care, including crisis intervention, partial hospital, intensive outpatient, and traditional outpatient services
DL, DPC, GD
GR/FE, WE
Apply the major diagnostic screening tests for substance abuse disorders including the CAGE, AUDIT, MAST, and ASI
DL, DPC GR/FE, WE, SPE
Know in detail all aspects of the DSM IV criteria for substance‐related and substance induced disorders
DL GR/FE, WE
Know the detoxification regimens for alcohol, sedative‐hypnotics, opiates, and stimulants and heroin
DL, DPC GR/FE, WE
Know the value and use of medications used to treat substance dependence including disulfiram, naltrexone, acamprosate, and methadone
DL, DPC GR/FE, WE
Know the major individual, group, and family psychotherapy treatments used in treating substance abuse
DL WE
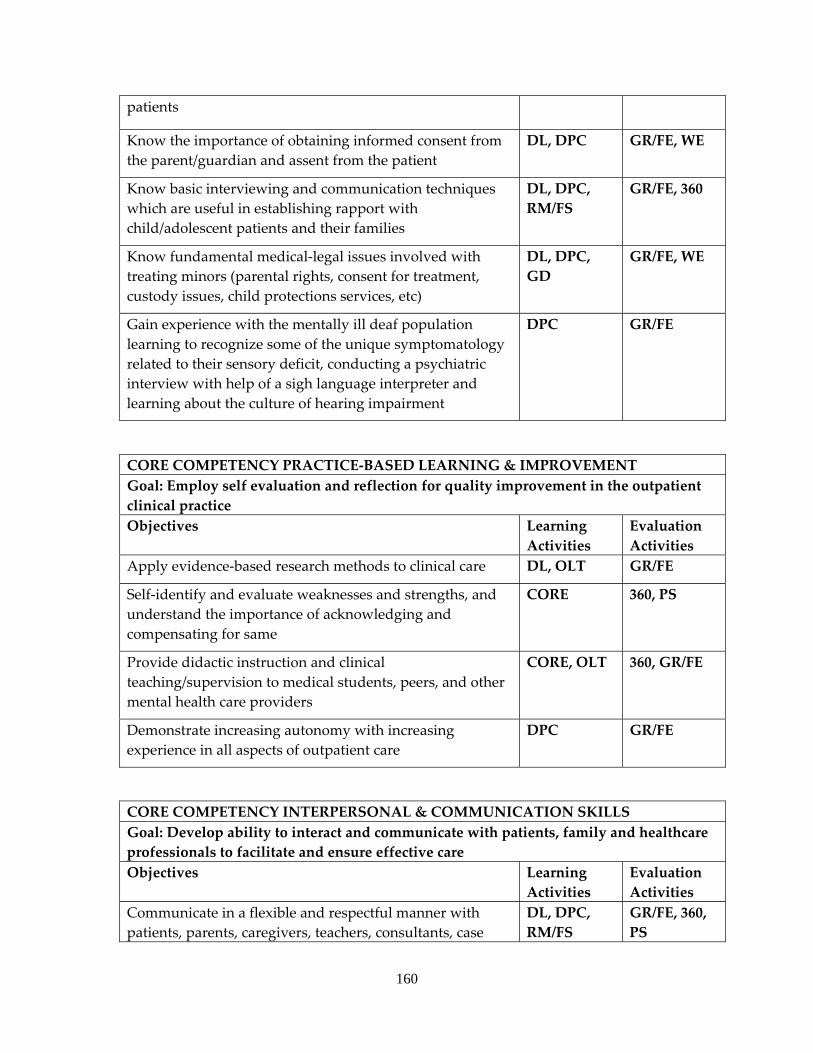
160
patients
Know the importance of obtaining informed consent from the parent/guardian and assent from the patient
DL, DPC GR/FE, WE
Know basic interviewing and communication techniques which are useful in establishing rapport with child/adolescent patients and their families
DL, DPC, RM/FS
GR/FE, 360
Know fundamental medical‐legal issues involved with treating minors (parental rights, consent for treatment, custody issues, child protections services, etc)
DL, DPC, GD
GR/FE, WE
Gain experience with the mentally ill deaf population learning to recognize some of the unique symptomatology related to their sensory deficit, conducting a psychiatric interview with help of a sigh language interpreter and learning about the culture of hearing impairment
DPC GR/FE
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Employ self evaluation and reflection for quality improvement in the outpatient clinical practice Objectives Learning
Activities Evaluation Activities
Apply evidence‐based research methods to clinical care DL, OLT GR/FE
Self‐identify and evaluate weaknesses and strengths, and understand the importance of acknowledging and compensating for same
CORE 360, PS
Provide didactic instruction and clinical teaching/supervision to medical students, peers, and other mental health care providers
CORE, OLT 360, GR/FE
Demonstrate increasing autonomy with increasing experience in all aspects of outpatient care
DPC GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care Objectives Learning
Activities Evaluation Activities
Communicate in a flexible and respectful manner with patients, parents, caregivers, teachers, consultants, case
DL, DPC, RM/FS
GR/FE, 360, PS
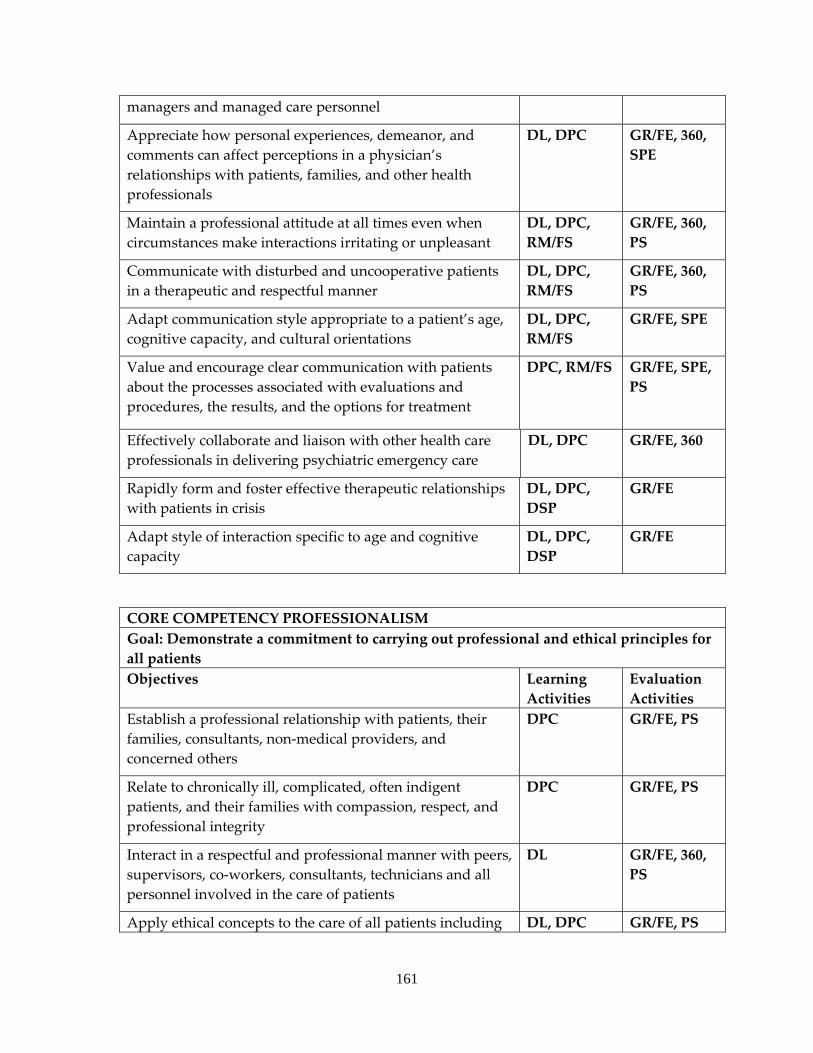
161
managers and managed care personnel
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times even when circumstances make interactions irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360, PS
Communicate with disturbed and uncooperative patients in a therapeutic and respectful manner
DL, DPC, RM/FS
GR/FE, 360, PS
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, RM/FS GR/FE, SPE, PS
Effectively collaborate and liaison with other health care professionals in delivering psychiatric emergency care
DL, DPC GR/FE, 360
Rapidly form and foster effective therapeutic relationships with patients in crisis
DL, DPC, DSP
GR/FE
Adapt style of interaction specific to age and cognitive capacity
DL, DPC, DSP
GR/FE
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for all patients Objectives Learning
Activities Evaluation Activities
Establish a professional relationship with patients, their families, consultants, non‐medical providers, and concerned others
DPC GR/FE, PS
Relate to chronically ill, complicated, often indigent patients, and their families with compassion, respect, and professional integrity
DPC GR/FE, PS
Interact in a respectful and professional manner with peers, supervisors, co‐workers, consultants, technicians and all personnel involved in the care of patients
DL GR/FE, 360, PS
Apply ethical concepts to the care of all patients including DL, DPC GR/FE, PS
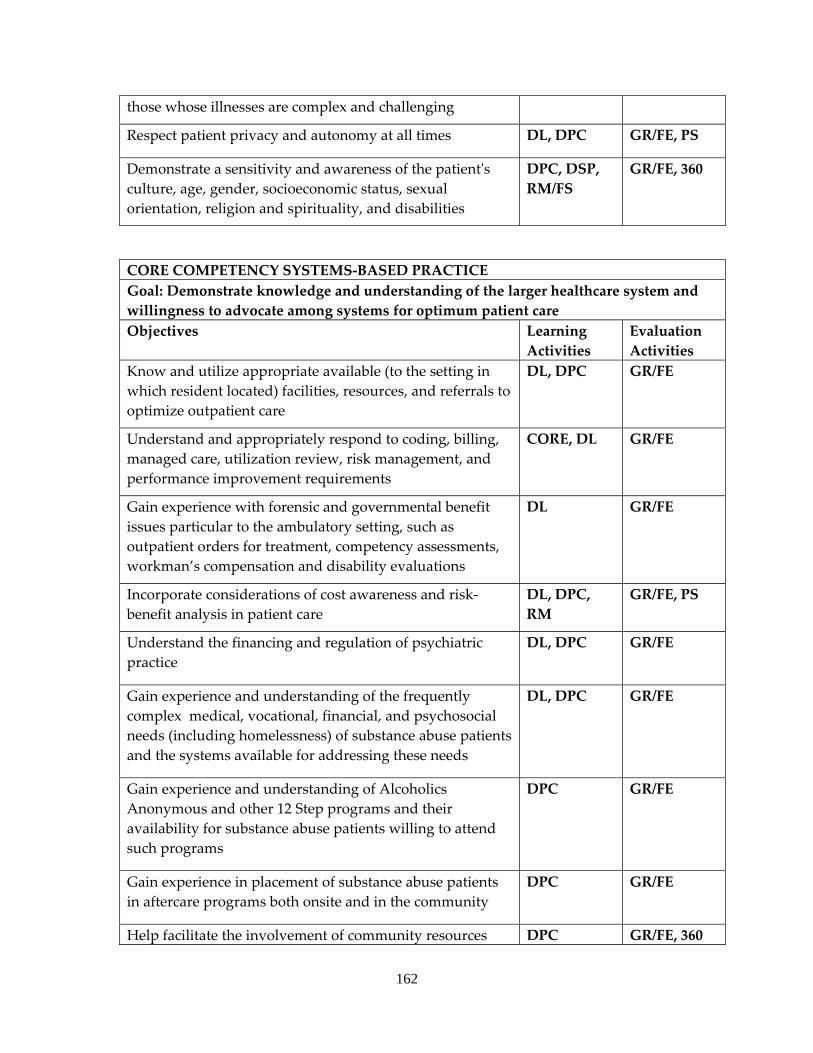
162
those whose illnesses are complex and challenging
Respect patient privacy and autonomy at all times DL, DPC GR/FE, PS
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, DSP, RM/FS
GR/FE, 360
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Know and utilize appropriate available (to the setting in which resident located) facilities, resources, and referrals to optimize outpatient care
DL, DPC GR/FE
Understand and appropriately respond to coding, billing, managed care, utilization review, risk management, and performance improvement requirements
CORE, DL GR/FE
Gain experience with forensic and governmental benefit issues particular to the ambulatory setting, such as outpatient orders for treatment, competency assessments, workman’s compensation and disability evaluations
DL GR/FE
Incorporate considerations of cost awareness and risk‐benefit analysis in patient care
DL, DPC, RM
GR/FE, PS
Understand the financing and regulation of psychiatric practice
DL, DPC GR/FE
Gain experience and understanding of the frequently complex medical, vocational, financial, and psychosocial needs (including homelessness) of substance abuse patients and the systems available for addressing these needs
DL, DPC GR/FE
Gain experience and understanding of Alcoholics Anonymous and other 12 Step programs and their availability for substance abuse patients willing to attend such programs
DPC GR/FE
Gain experience in placement of substance abuse patients in aftercare programs both onsite and in the community
DPC GR/FE
Help facilitate the involvement of community resources DPC GR/FE, 360
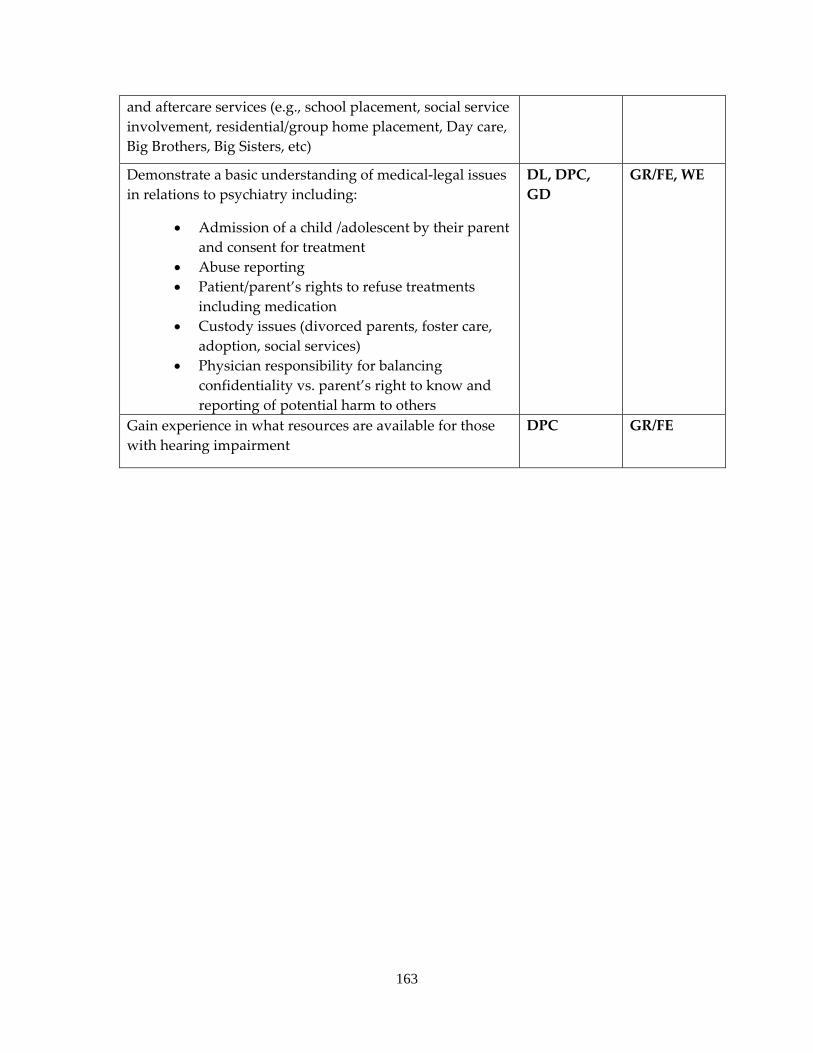
163
and aftercare services (e.g., school placement, social service involvement, residential/group home placement, Day care, Big Brothers, Big Sisters, etc)
Demonstrate a basic understanding of medical‐legal issues in relations to psychiatry including:
• Admission of a child /adolescent by their parent and consent for treatment
• Abuse reporting • Patient/parent’s rights to refuse treatments
including medication • Custody issues (divorced parents, foster care,
adoption, social services) • Physician responsibility for balancing
confidentiality vs. parent’s right to know and reporting of potential harm to others
DL, DPC, GD
GR/FE, WE
Gain experience in what resources are available for those with hearing impairment
DPC GR/FE
164
WYANDOT CENTER FOR COMMUNITY BEHAVIORAL HEALTHCARE (Community Mental Health Affiliate)
a. ADULT PSYCHIATRY OUTPATIENT SERVICE b. Required continuous half‐time 6 month rotation usually occurring in the PGY3 year. c. Faculty consists of two full‐time psychiatrists, who supervise residents assigned to
the general outpatient program at Wyandot Center. Both psychiatrists are board certified and hold a faculty appointment at KUMC, and are responsible for ensuring that residents receive adequate supervision and quality education while on site.
d. The community mental health center serves approximately 10,000 clients with a large volume seen directly by physicians per year. The clinical population is comprised of all age groups. Sixty One percent are over age 21. Fifteen percent are age 21‐30, fifteen percent age 31‐40, fifteen percent age 41‐50, eleven percent age 51‐60, three percent age 61‐70, and two percent age 71 and over. Forty nine per cent are Caucasian, Thirty‐three percent are African‐American, 10 percent are Hispanic, and one percent are Native American. Sixty one percent of the clients have a household income less than $5,000 per year, and eighty‐six percent of the clients have a household income less than $20,000 per year. Fifty percent of the patients are female, and fifty percent are male. Caseloads represent a variety of diagnoses, and an effort is made to ensure that residents have a broad educational experience. Mood disorders comprise 41%, childhood disorders 23%, schizophrenia 2%, anxiety disorders 11% and adjustment disorders 14%, and other diagnostic classes 9% of the Wyandot Center client population.
e. Each of the staff psychiatrists serves approximately 500 clients in the general outpatient program. An average caseload for a resident being supervised would be approximately 100 patients by the conclusion of the rotation. Primary psychiatric services include medication management, referral for psychotherapy when appropriate, referral for crisis case management when appropriate, and ongoing collaboration with psychotherapists and crisis case managers and nurses.
f. All residents receive one hour of individual supervision per week from the supervising psychiatrist at Wyandot Center in addition to supervision provided at KUMC.
g. This rotation is done concurrently with a 6 month, 0.5 FTE assignment to the adult outpatient clinic at KUMC. The experience at the mental health center broadens considerably the resident’s exposure to working with varied socio‐economic groups, including the indigent and homeless, with diverse ethnic groups, and with patients suffering from severe and persistent mental illness. These clients are maintained as much as possible in the community utilizing 24‐hour emergency services, case management services, and attendant care services. The rotation exposes the resident to important sub‐populations of the community and provides experience with the interface between community agencies and community and state hospital systems.
165
EDUCATIONAL GOALS AND OBJECTIVES ROTATION: OUTPATIENT ADULT PSYCHIATRY LEVEL: PGY3 DURATION: 6 MONTHS, HALF‐TIME (PGY3) SITE: WYANDOT CENTER FOR COMMUNITY BEHAVIORAL HEALTHCARE SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING PSYCHIATRY ATTENDING AT WYANDOT CENTER FOR COMMUNITY BEHAVIORAL HEALTHCARE By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
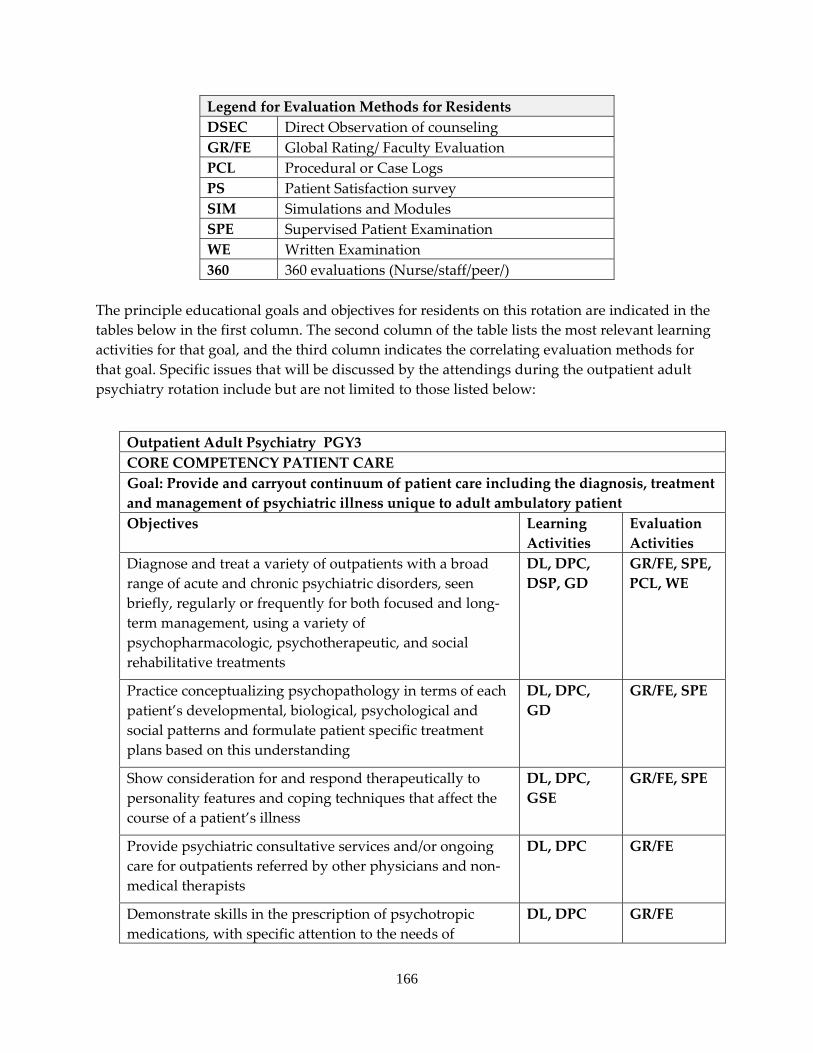
166
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column. The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal. Specific issues that will be discussed by the attendings during the outpatient adult psychiatry rotation include but are not limited to those listed below:
Outpatient Adult Psychiatry PGY3 CORE COMPETENCY PATIENT CARE Goal: Provide and carryout continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to adult ambulatory patient Objectives Learning
Activities Evaluation Activities
Diagnose and treat a variety of outpatients with a broad range of acute and chronic psychiatric disorders, seen briefly, regularly or frequently for both focused and long‐term management, using a variety of psychopharmacologic, psychotherapeutic, and social rehabilitative treatments
DL, DPC, DSP, GD
GR/FE, SPE, PCL, WE
Practice conceptualizing psychopathology in terms of each patient’s developmental, biological, psychological and social patterns and formulate patient specific treatment plans based on this understanding
DL, DPC, GD
GR/FE, SPE
Show consideration for and respond therapeutically to personality features and coping techniques that affect the course of a patient’s illness
DL, DPC, GSE
GR/FE, SPE
Provide psychiatric consultative services and/or ongoing care for outpatients referred by other physicians and non‐medical therapists
DL, DPC GR/FE
Demonstrate skills in the prescription of psychotropic medications, with specific attention to the needs of
DL, DPC GR/FE
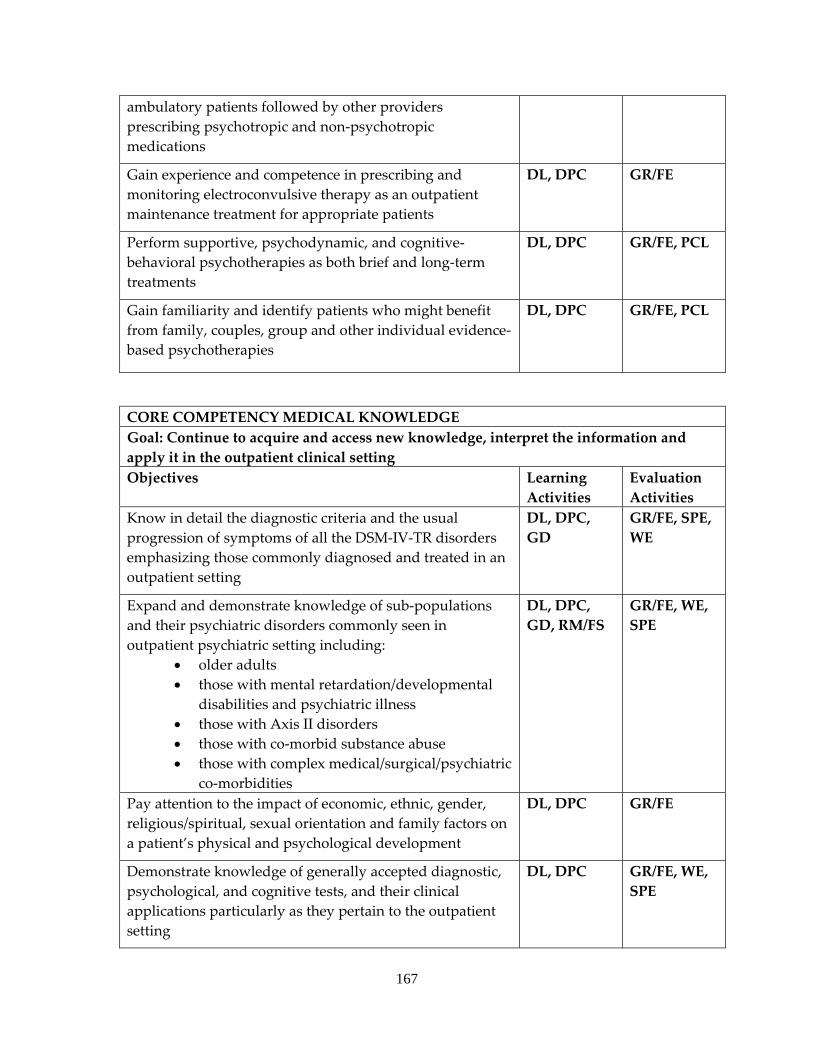
167
ambulatory patients followed by other providers prescribing psychotropic and non‐psychotropic medications
Gain experience and competence in prescribing and monitoring electroconvulsive therapy as an outpatient maintenance treatment for appropriate patients
DL, DPC GR/FE
Perform supportive, psychodynamic, and cognitive‐behavioral psychotherapies as both brief and long‐term treatments
DL, DPC GR/FE, PCL
Gain familiarity and identify patients who might benefit from family, couples, group and other individual evidence‐based psychotherapies
DL, DPC GR/FE, PCL
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Continue to acquire and access new knowledge, interpret the information and apply it in the outpatient clinical setting Objectives Learning
Activities Evaluation Activities
Know in detail the diagnostic criteria and the usual progression of symptoms of all the DSM‐IV‐TR disorders emphasizing those commonly diagnosed and treated in an outpatient setting
DL, DPC, GD
GR/FE, SPE, WE
Expand and demonstrate knowledge of sub‐populations and their psychiatric disorders commonly seen in outpatient psychiatric setting including:
• older adults • those with mental retardation/developmental
disabilities and psychiatric illness • those with Axis II disorders • those with co‐morbid substance abuse • those with complex medical/surgical/psychiatric
co‐morbidities
DL, DPC, GD, RM/FS
GR/FE, WE, SPE
Pay attention to the impact of economic, ethnic, gender, religious/spiritual, sexual orientation and family factors on a patient’s physical and psychological development
DL, DPC GR/FE
Demonstrate knowledge of generally accepted diagnostic, psychological, and cognitive tests, and their clinical applications particularly as they pertain to the outpatient setting
DL, DPC GR/FE, WE, SPE
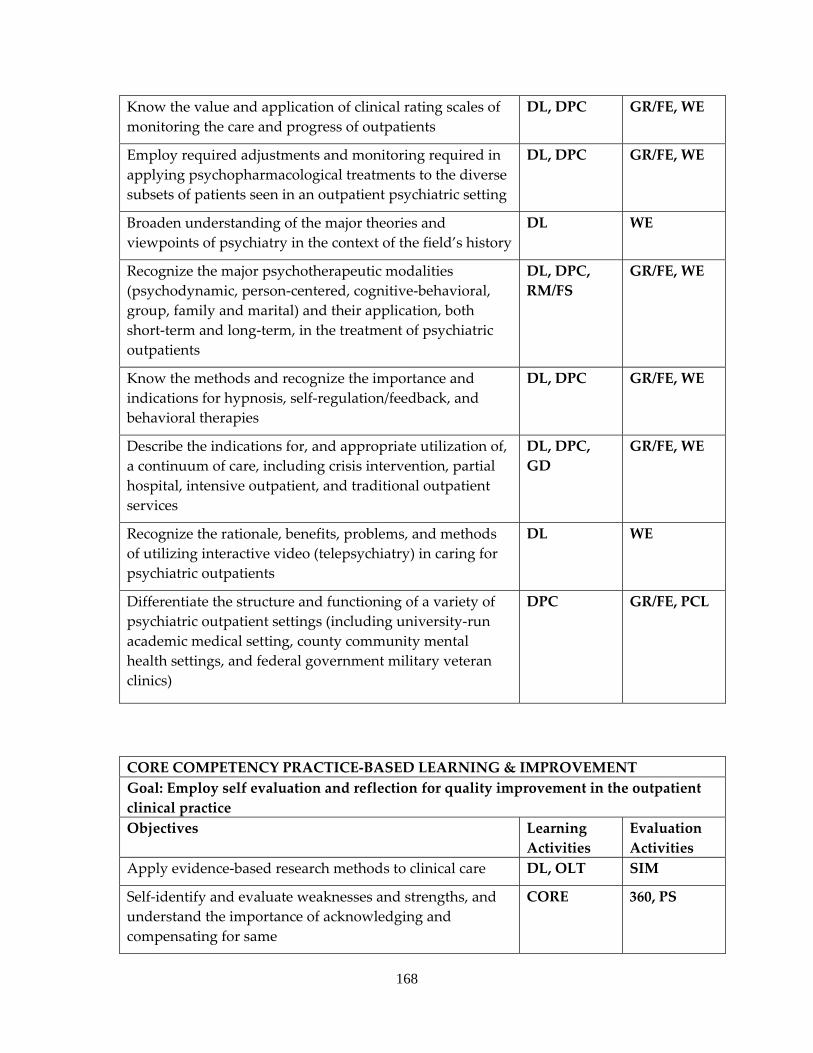
168
Know the value and application of clinical rating scales of monitoring the care and progress of outpatients
DL, DPC GR/FE, WE
Employ required adjustments and monitoring required in applying psychopharmacological treatments to the diverse subsets of patients seen in an outpatient psychiatric setting
DL, DPC GR/FE, WE
Broaden understanding of the major theories and viewpoints of psychiatry in the context of the field’s history
DL WE
Recognize the major psychotherapeutic modalities (psychodynamic, person‐centered, cognitive‐behavioral, group, family and marital) and their application, both short‐term and long‐term, in the treatment of psychiatric outpatients
DL, DPC, RM/FS
GR/FE, WE
Know the methods and recognize the importance and indications for hypnosis, self‐regulation/feedback, and behavioral therapies
DL, DPC GR/FE, WE
Describe the indications for, and appropriate utilization of, a continuum of care, including crisis intervention, partial hospital, intensive outpatient, and traditional outpatient services
DL, DPC, GD
GR/FE, WE
Recognize the rationale, benefits, problems, and methods of utilizing interactive video (telepsychiatry) in caring for psychiatric outpatients
DL WE
Differentiate the structure and functioning of a variety of psychiatric outpatient settings (including university‐run academic medical setting, county community mental health settings, and federal government military veteran clinics)
DPC GR/FE, PCL
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVEMENT Goal: Employ self evaluation and reflection for quality improvement in the outpatient clinical practice Objectives Learning
Activities Evaluation Activities
Apply evidence‐based research methods to clinical care DL, OLT SIM
Self‐identify and evaluate weaknesses and strengths, and understand the importance of acknowledging and compensating for same
CORE 360, PS
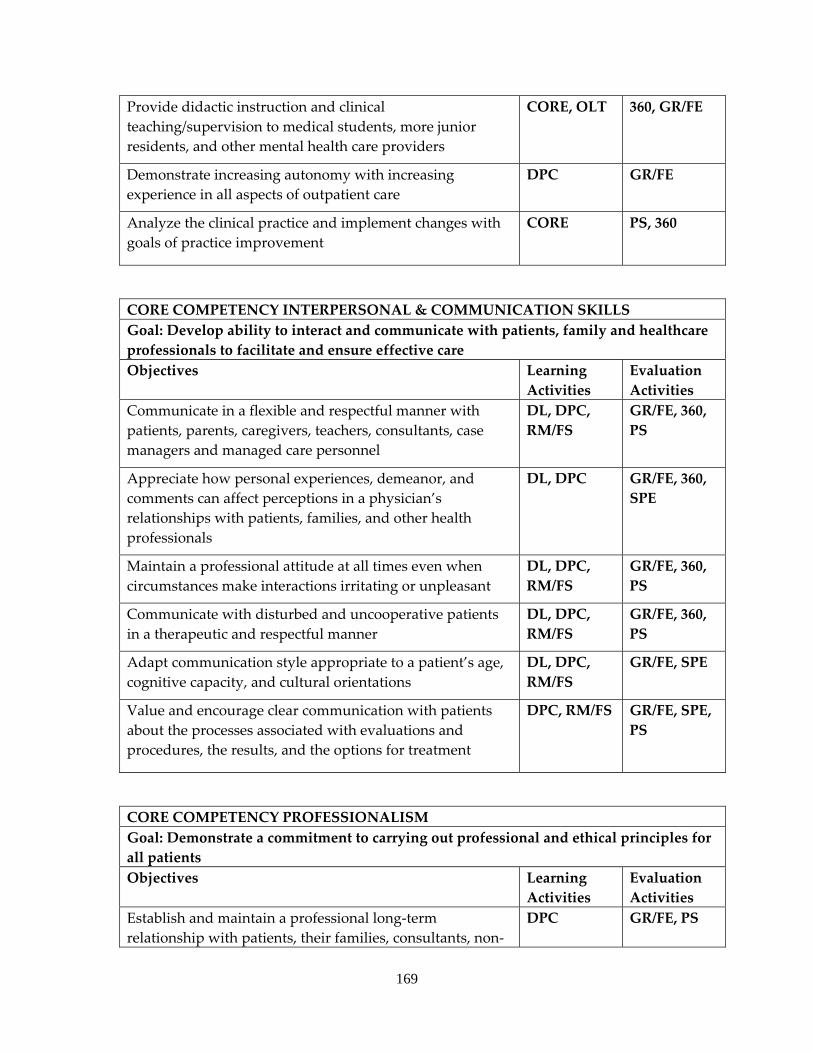
169
Provide didactic instruction and clinical teaching/supervision to medical students, more junior residents, and other mental health care providers
CORE, OLT 360, GR/FE
Demonstrate increasing autonomy with increasing experience in all aspects of outpatient care
DPC GR/FE
Analyze the clinical practice and implement changes with goals of practice improvement
CORE PS, 360
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate and ensure effective care Objectives Learning
Activities Evaluation Activities
Communicate in a flexible and respectful manner with patients, parents, caregivers, teachers, consultants, case managers and managed care personnel
DL, DPC, RM/FS
GR/FE, 360, PS
Appreciate how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, DPC GR/FE, 360, SPE
Maintain a professional attitude at all times even when circumstances make interactions irritating or unpleasant
DL, DPC, RM/FS
GR/FE, 360, PS
Communicate with disturbed and uncooperative patients in a therapeutic and respectful manner
DL, DPC, RM/FS
GR/FE, 360, PS
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC, RM/FS
GR/FE, SPE
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, RM/FS GR/FE, SPE, PS
CORE COMPETENCY PROFESSIONALISM Goal: Demonstrate a commitment to carrying out professional and ethical principles for all patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional long‐term relationship with patients, their families, consultants, non‐
DPC GR/FE, PS
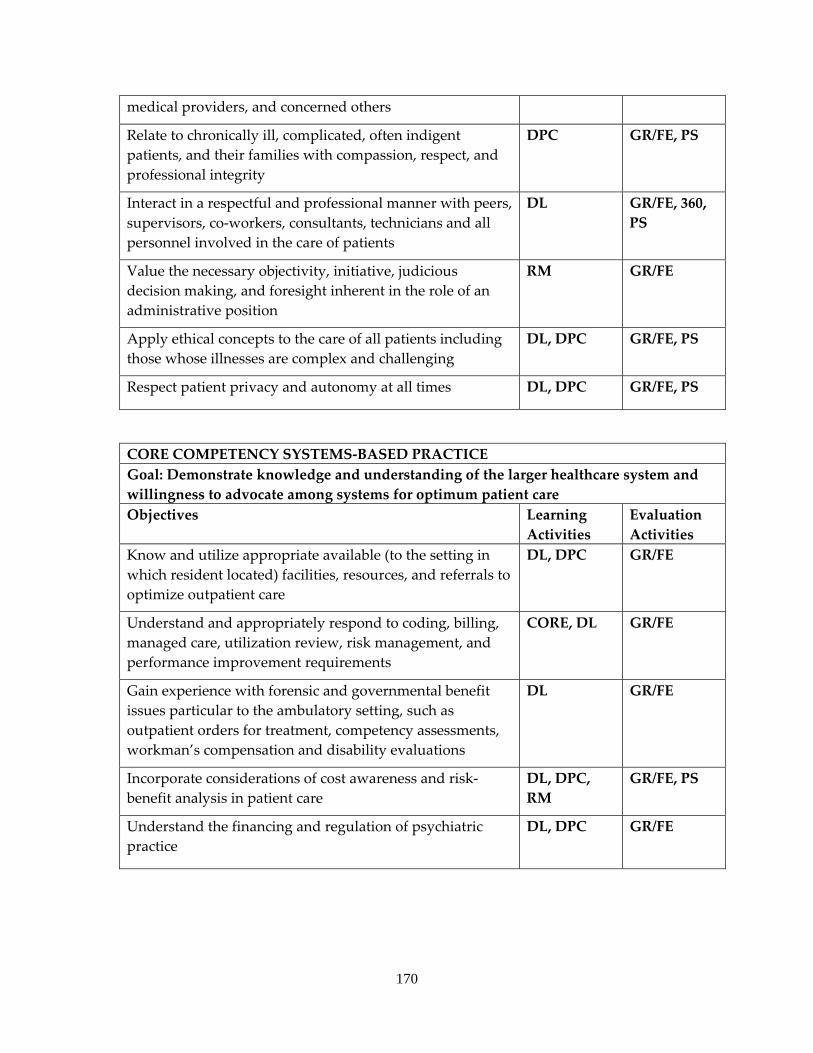
170
medical providers, and concerned others
Relate to chronically ill, complicated, often indigent patients, and their families with compassion, respect, and professional integrity
DPC GR/FE, PS
Interact in a respectful and professional manner with peers, supervisors, co‐workers, consultants, technicians and all personnel involved in the care of patients
DL GR/FE, 360, PS
Value the necessary objectivity, initiative, judicious decision making, and foresight inherent in the role of an administrative position
RM GR/FE
Apply ethical concepts to the care of all patients including those whose illnesses are complex and challenging
DL, DPC GR/FE, PS
Respect patient privacy and autonomy at all times DL, DPC GR/FE, PS
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Know and utilize appropriate available (to the setting in which resident located) facilities, resources, and referrals to optimize outpatient care
DL, DPC GR/FE
Understand and appropriately respond to coding, billing, managed care, utilization review, risk management, and performance improvement requirements
CORE, DL GR/FE
Gain experience with forensic and governmental benefit issues particular to the ambulatory setting, such as outpatient orders for treatment, competency assessments, workman’s compensation and disability evaluations
DL GR/FE
Incorporate considerations of cost awareness and risk‐benefit analysis in patient care
DL, DPC, RM
GR/FE, PS
Understand the financing and regulation of psychiatric practice
DL, DPC GR/FE
171
MARILLAC
a. Required 2‐3 month rotation occurring at Marillac in the PGY4 year. b. The faculty consists of one full‐time attending child and adolescent psychiatrist (with
backup from others when needed) and one psychologist both of whom attend team meetings and are available for teaching and consultation.
c. The main educational activity on this service is to provide clinical care to an inpatient population of child and adolescents under the close supervision of the faculty. During this rotation residents continue to attend approximately four hours per week of psychiatry didactics at KUMC and other required educational activities. In addition, residents have one hour per week of individual psychiatry supervision with the attending faculty and one hour per week of psychotherapy supervision.
d. The inpatient population is approximately 58% male, 42% female, 74% Caucasian, 3% Hispanic, 9% African American, 10% Multi‐Racial, and 4% other. The age ranges are mainly between 3 years to 17 years (63% teenagers) of age. The most commonly seen disorders are: ADHD, Learning Disability, PTSD, Acute Stress Reaction, Oppositional‐Defiant Disorder, Bipolar Disorder, Major Depression, Schizophrenia, Psychosis NOS, Substance Abuse/Dependence, Intermittent Explosive Disorder, Separation Anxiety disorder, Encopresis, Enuresis, Tourette’s Disorder, Mental Retardation, Autism, Anorexia nervosa, and Bulimia Nervosa. Treatment modalities include behavior modification, family therapy, group psychotherapy, individual psychotherapy (utilizing primarily cognitive, behavioral, interpersonal, and supportive approaches), school, art therapy, recreational therapy, medication, therapeutic structure, occupational therapy.
e. An average caseload consists of 6‐8 patients. Residents provide patient care from admit orders, to daily inpatient care, treatment team meetings, discharge orders and discharge summary. They participate in patient education, family therapy/meetings, conferring with primary physicians and outside mental health providers and coordinating aftercare. They have the opportunity to sit in on group therapies. Residents rotate weekend coverage (approximately every third weekend) with the child and adolescent psychiatry residents.
f. Individual supervision occurs daily on the inpatient service. Residents receive ongoing supervision through staffing and case reviews individually on a daily basis by the attending psychiatrist.
g. During this rotation the resident gains clinical experience in patient evaluation, diagnosis, and treatment with children of varying ages and with a wide range of diagnoses. Many of the patients are acute and seriously emotionally disturbed. Treatment modalities include pharmacologic therapy, individual and family therapy, and crisis intervention. There is also experience collaborating with a team of mental health and allied health professionals.
h. The resident is required to attend the unit quality improvement meetings and each resident is asked to work on a particular issue pertaining to improvement in patient care. Past examples include tracking the documentation of patient/parent education
172
when prescribing an SSRI and tracking the disposition of child psychiatry patients presenting to the emergency room.
EDUCATIONAL GOALS AND OBJECTIVES
ROTATION: CHILD AND ADOLESCENT PSYCHIATRY LEVEL: PGY4 DURATON: 2‐3 MONTHS SITES: MARILLAC SUPERVISION: DIRECT SUPERVISION OF THE RESIDENT BY SUPERVISING CHILD AND ADOLESCENT PSYCHIATRY ATTENDING AT MARILLAC
By completion of the psychiatric residency program, residents are expected to demonstrate competence in the following areas:
1. PATIENT CARE ‐ Residents must be able to provide patient care that is compassionate, appropriate, and effective for the treatment of health problems and the promotion of health.
2. MEDICAL KNOWLEDGE ‐ Residents must demonstrate knowledge about established and evolving biomedical, clinical, and cognate (e.g. epidemiological and social‐behavioral) sciences and the application of this knowledge to patient care.
3. PRACTICE‐BASED LEARNING AND IMPROVEMENT ‐ Residents must be able to investigate and evaluate their patient care practices, appraise and assimilate scientific evidence, and improve their patient care practices.
4. INTERPERSONAL AND COMMUNICATION SKILLS ‐ Residents must be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with patients, their patients families, and professional associates.
5. PROFESSIONALISM ‐ Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population.
6. SYSTEMS‐BASED PRACTICE ‐ Residents must demonstrate an awareness of and responsiveness to the larger context and system of health care and the ability to effectively call on system resources to provide care that is of optimal value.
Legend for Learning Activities for Residents DL Didactic Lectures DPC Direct Patient Care/Clinical Patient experience DSP Directly Supervised Examinations/Counseling CORE CORE conference by GME GD Group Discussion OLT Online Tool PR Project Requirement RM/FS Role Modeling/Faculty Supervised activities
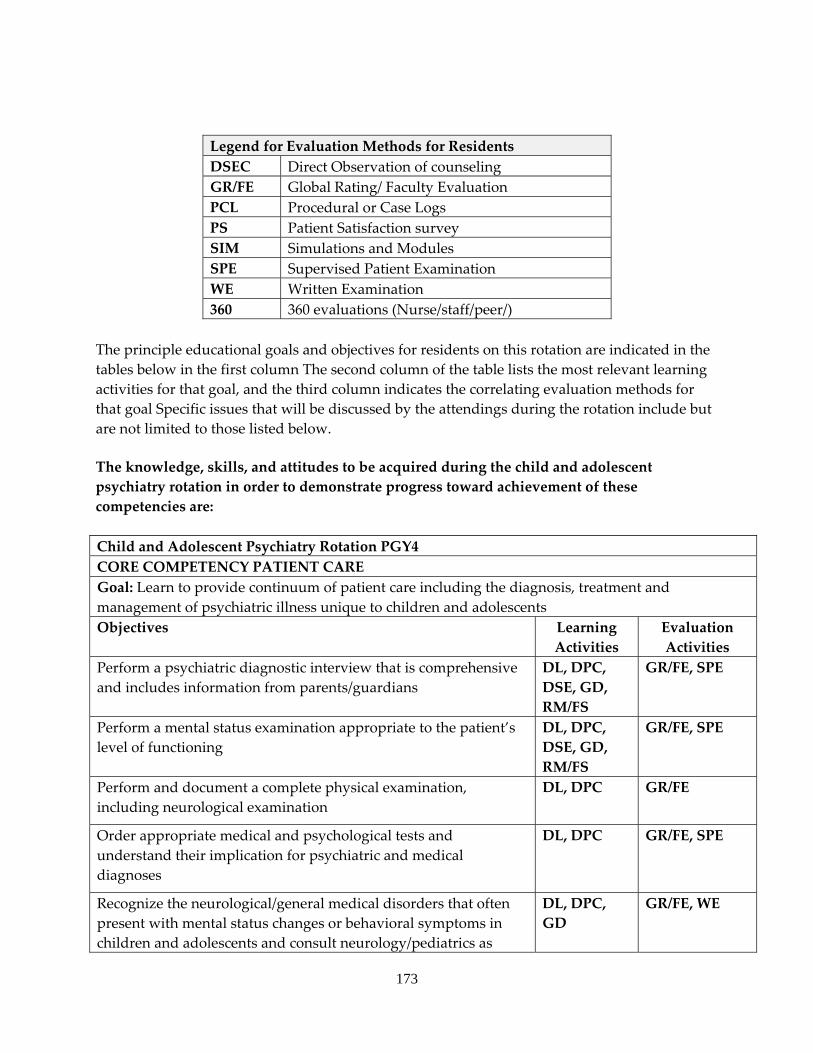
173
Legend for Evaluation Methods for Residents DSEC Direct Observation of counseling GR/FE Global Rating/ Faculty Evaluation PCL Procedural or Case Logs PS Patient Satisfaction survey SIM Simulations and Modules SPE Supervised Patient Examination WE Written Examination 360 360 evaluations (Nurse/staff/peer/)
The principle educational goals and objectives for residents on this rotation are indicated in the tables below in the first column The second column of the table lists the most relevant learning activities for that goal, and the third column indicates the correlating evaluation methods for that goal Specific issues that will be discussed by the attendings during the rotation include but are not limited to those listed below.
The knowledge, skills, and attitudes to be acquired during the child and adolescent psychiatry rotation in order to demonstrate progress toward achievement of these competencies are: Child and Adolescent Psychiatry Rotation PGY4 CORE COMPETENCY PATIENT CARE Goal: Learn to provide continuum of patient care including the diagnosis, treatment and management of psychiatric illness unique to children and adolescentsObjectives Learning
Activities Evaluation Activities
Perform a psychiatric diagnostic interview that is comprehensive and includes information from parents/guardians
DL, DPC, DSE, GD, RM/FS
GR/FE, SPE
Perform a mental status examination appropriate to the patient’s level of functioning
DL, DPC, DSE, GD, RM/FS
GR/FE, SPE
Perform and document a complete physical examination, including neurological examination
DL, DPC GR/FE
Order appropriate medical and psychological tests and understand their implication for psychiatric and medical diagnoses
DL, DPC GR/FE, SPE
Recognize the neurological/general medical disorders that often present with mental status changes or behavioral symptoms in children and adolescents and consult neurology/pediatrics as
DL, DPC, GD
GR/FE, WE
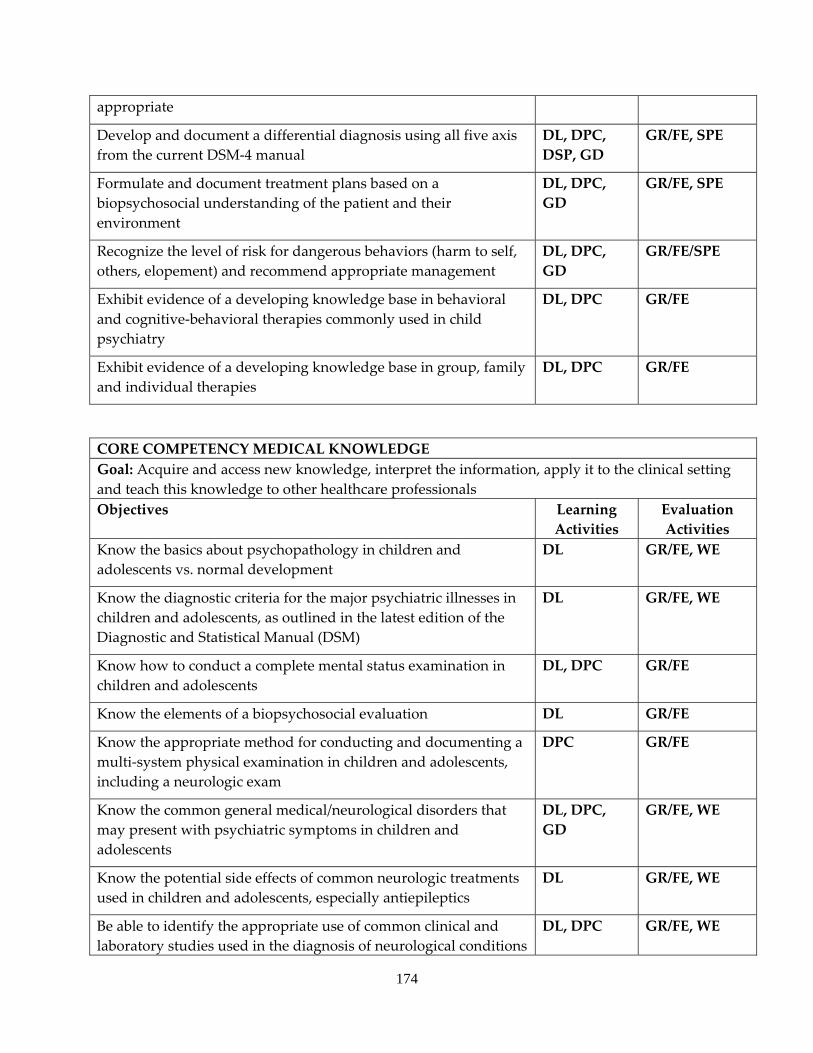
174
appropriate
Develop and document a differential diagnosis using all five axis from the current DSM‐4 manual
DL, DPC, DSP, GD
GR/FE, SPE
Formulate and document treatment plans based on a biopsychosocial understanding of the patient and their environment
DL, DPC, GD
GR/FE, SPE
Recognize the level of risk for dangerous behaviors (harm to self, others, elopement) and recommend appropriate management
DL, DPC, GD
GR/FE/SPE
Exhibit evidence of a developing knowledge base in behavioral and cognitive‐behavioral therapies commonly used in child psychiatry
DL, DPC GR/FE
Exhibit evidence of a developing knowledge base in group, family and individual therapies
DL, DPC GR/FE
CORE COMPETENCY MEDICAL KNOWLEDGE Goal: Acquire and access new knowledge, interpret the information, apply it to the clinical setting and teach this knowledge to other healthcare professionalsObjectives Learning
Activities Evaluation Activities
Know the basics about psychopathology in children and adolescents vs. normal development
DL GR/FE, WE
Know the diagnostic criteria for the major psychiatric illnesses in children and adolescents, as outlined in the latest edition of the Diagnostic and Statistical Manual (DSM)
DL GR/FE, WE
Know how to conduct a complete mental status examination in children and adolescents
DL, DPC GR/FE
Know the elements of a biopsychosocial evaluation DL GR/FE
Know the appropriate method for conducting and documenting a multi‐system physical examination in children and adolescents, including a neurologic exam
DPC GR/FE
Know the common general medical/neurological disorders that may present with psychiatric symptoms in children and adolescents
DL, DPC, GD
GR/FE, WE
Know the potential side effects of common neurologic treatments used in children and adolescents, especially antiepileptics
DL GR/FE, WE
Be able to identify the appropriate use of common clinical and laboratory studies used in the diagnosis of neurological conditions
DL, DPC GR/FE, WE
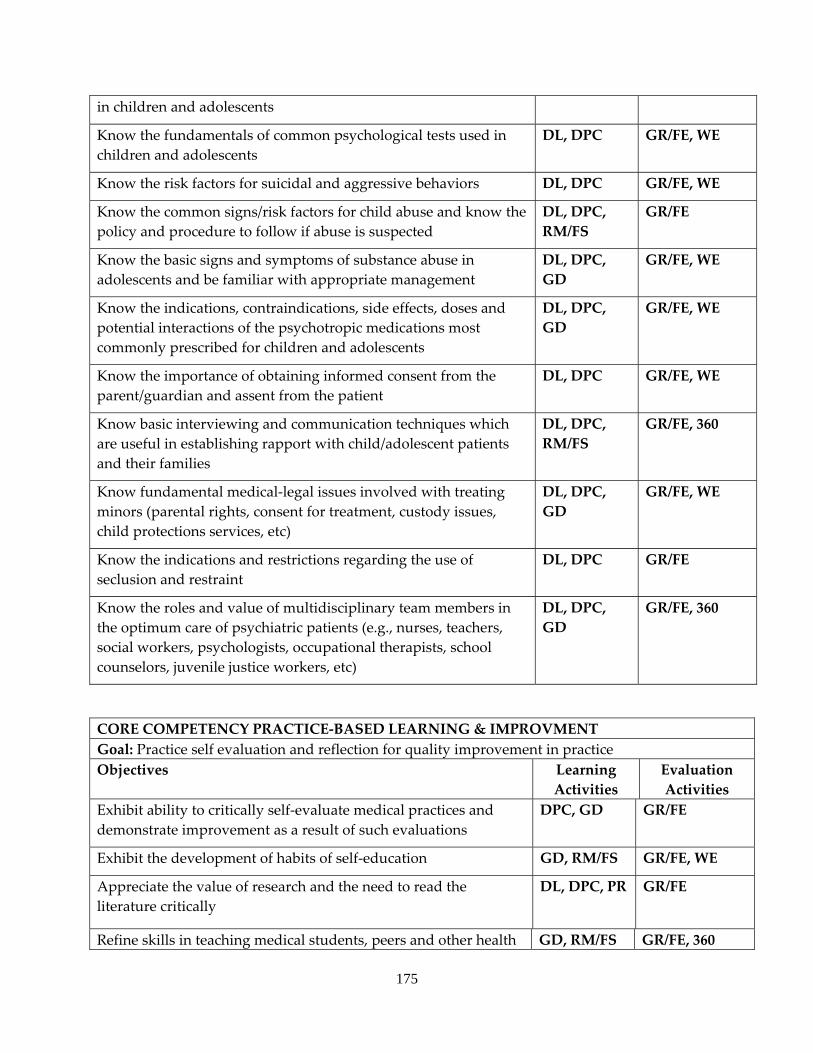
175
in children and adolescents
Know the fundamentals of common psychological tests used in children and adolescents
DL, DPC GR/FE, WE
Know the risk factors for suicidal and aggressive behaviors DL, DPC GR/FE, WE
Know the common signs/risk factors for child abuse and know the policy and procedure to follow if abuse is suspected
DL, DPC, RM/FS
GR/FE
Know the basic signs and symptoms of substance abuse in adolescents and be familiar with appropriate management
DL, DPC, GD
GR/FE, WE
Know the indications, contraindications, side effects, doses and potential interactions of the psychotropic medications most commonly prescribed for children and adolescents
DL, DPC, GD
GR/FE, WE
Know the importance of obtaining informed consent from the parent/guardian and assent from the patient
DL, DPC GR/FE, WE
Know basic interviewing and communication techniques which are useful in establishing rapport with child/adolescent patients and their families
DL, DPC, RM/FS
GR/FE, 360
Know fundamental medical‐legal issues involved with treating minors (parental rights, consent for treatment, custody issues, child protections services, etc)
DL, DPC, GD
GR/FE, WE
Know the indications and restrictions regarding the use of seclusion and restraint
DL, DPC GR/FE
Know the roles and value of multidisciplinary team members in the optimum care of psychiatric patients (e.g., nurses, teachers, social workers, psychologists, occupational therapists, school counselors, juvenile justice workers, etc)
DL, DPC, GD
GR/FE, 360
CORE COMPETENCY PRACTICE‐BASED LEARNING & IMPROVMENT Goal: Practice self evaluation and reflection for quality improvement in practice Objectives Learning
Activities Evaluation Activities
Exhibit ability to critically self‐evaluate medical practices and demonstrate improvement as a result of such evaluations
DPC, GD GR/FE
Exhibit the development of habits of self‐education GD, RM/FS GR/FE, WE
Appreciate the value of research and the need to read the literature critically
DL, DPC, PR GR/FE
Refine skills in teaching medical students, peers and other health GD, RM/FS GR/FE, 360
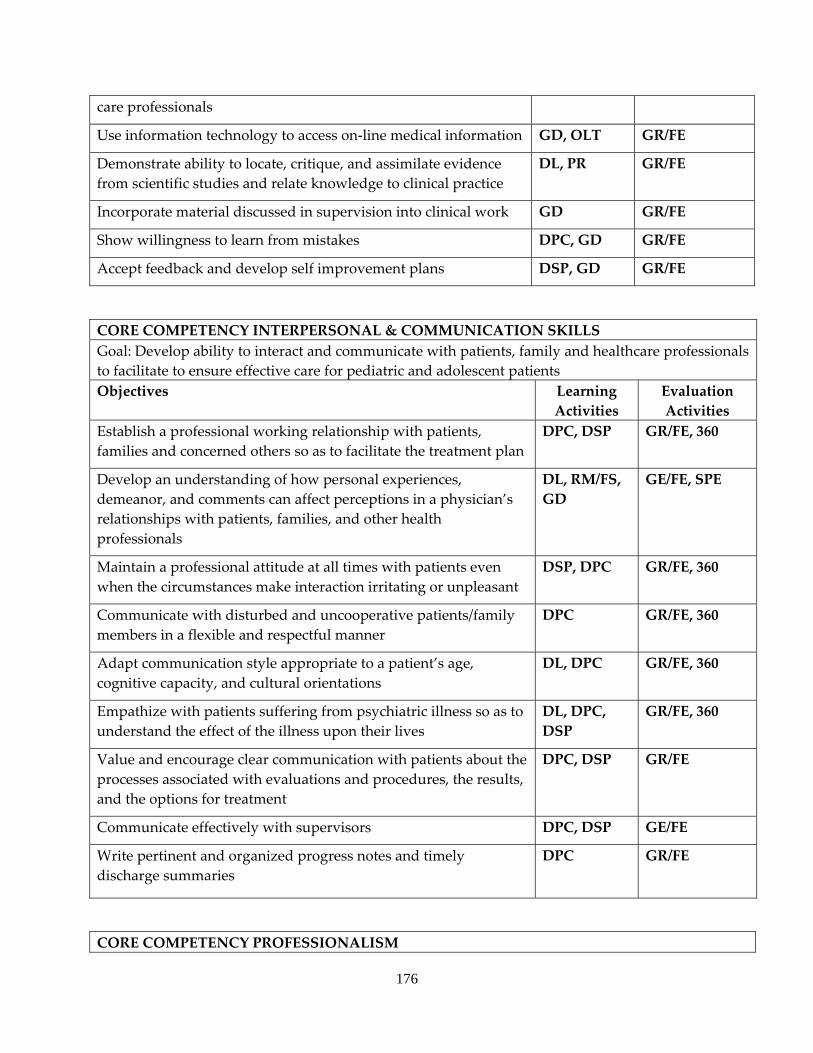
176
care professionals
Use information technology to access on‐line medical information GD, OLT GR/FE
Demonstrate ability to locate, critique, and assimilate evidence from scientific studies and relate knowledge to clinical practice
DL, PR GR/FE
Incorporate material discussed in supervision into clinical work GD GR/FE
Show willingness to learn from mistakes DPC, GD GR/FE
Accept feedback and develop self improvement plans DSP, GD GR/FE
CORE COMPETENCY INTERPERSONAL & COMMUNICATION SKILLS Goal: Develop ability to interact and communicate with patients, family and healthcare professionals to facilitate to ensure effective care for pediatric and adolescent patients Objectives Learning
Activities Evaluation Activities
Establish a professional working relationship with patients, families and concerned others so as to facilitate the treatment plan
DPC, DSP GR/FE, 360
Develop an understanding of how personal experiences, demeanor, and comments can affect perceptions in a physician’s relationships with patients, families, and other health professionals
DL, RM/FS, GD
GE/FE, SPE
Maintain a professional attitude at all times with patients even when the circumstances make interaction irritating or unpleasant
DSP, DPC GR/FE, 360
Communicate with disturbed and uncooperative patients/family members in a flexible and respectful manner
DPC GR/FE, 360
Adapt communication style appropriate to a patient’s age, cognitive capacity, and cultural orientations
DL, DPC GR/FE, 360
Empathize with patients suffering from psychiatric illness so as to understand the effect of the illness upon their lives
DL, DPC, DSP
GR/FE, 360
Value and encourage clear communication with patients about the processes associated with evaluations and procedures, the results, and the options for treatment
DPC, DSP GR/FE
Communicate effectively with supervisors DPC, DSP GE/FE
Write pertinent and organized progress notes and timely discharge summaries
DPC GR/FE
CORE COMPETENCY PROFESSIONALISM
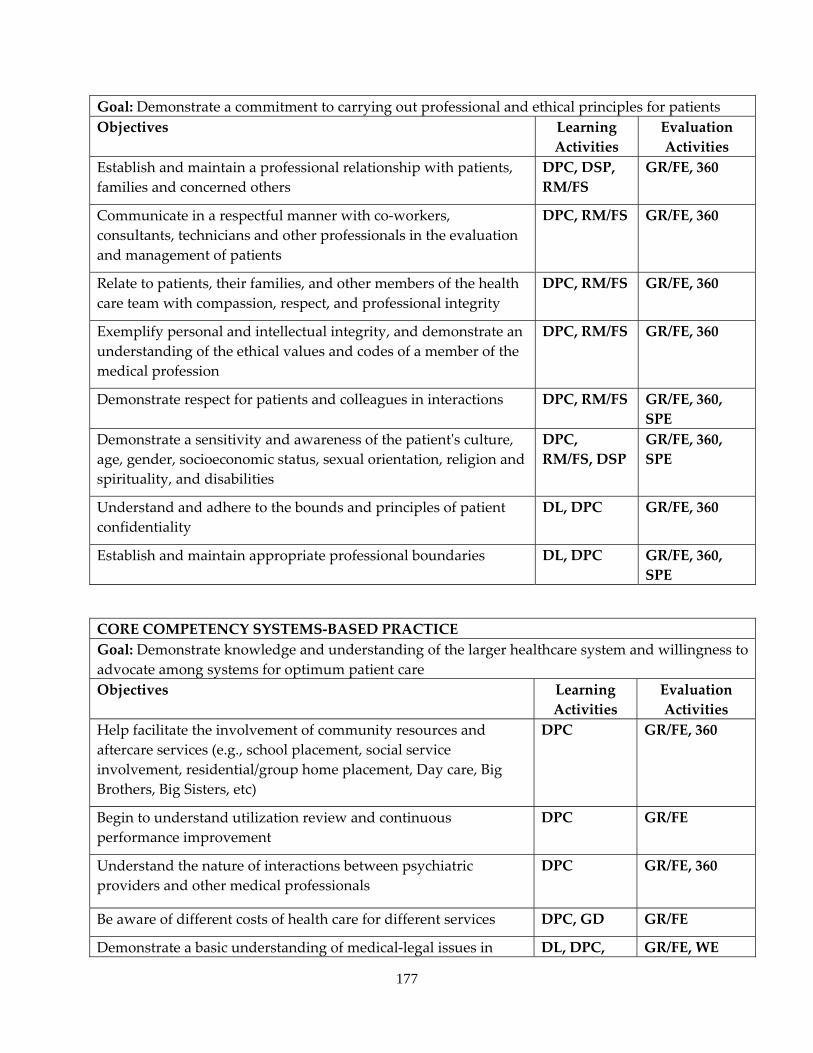
177
Goal: Demonstrate a commitment to carrying out professional and ethical principles for patients Objectives Learning
Activities Evaluation Activities
Establish and maintain a professional relationship with patients, families and concerned others
DPC, DSP, RM/FS
GR/FE, 360
Communicate in a respectful manner with co‐workers, consultants, technicians and other professionals in the evaluation and management of patients
DPC, RM/FS GR/FE, 360
Relate to patients, their families, and other members of the health care team with compassion, respect, and professional integrity
DPC, RM/FS GR/FE, 360
Exemplify personal and intellectual integrity, and demonstrate an understanding of the ethical values and codes of a member of the medical profession
DPC, RM/FS GR/FE, 360
Demonstrate respect for patients and colleagues in interactions DPC, RM/FS GR/FE, 360, SPE
Demonstrate a sensitivity and awareness of the patientʹs culture, age, gender, socioeconomic status, sexual orientation, religion and spirituality, and disabilities
DPC, RM/FS, DSP
GR/FE, 360, SPE
Understand and adhere to the bounds and principles of patient confidentiality
DL, DPC GR/FE, 360
Establish and maintain appropriate professional boundaries DL, DPC GR/FE, 360, SPE
CORE COMPETENCY SYSTEMS‐BASED PRACTICE Goal: Demonstrate knowledge and understanding of the larger healthcare system and willingness to advocate among systems for optimum patient care Objectives Learning
Activities Evaluation Activities
Help facilitate the involvement of community resources and aftercare services (e.g., school placement, social service involvement, residential/group home placement, Day care, Big Brothers, Big Sisters, etc)
DPC GR/FE, 360
Begin to understand utilization review and continuous performance improvement
DPC GR/FE
Understand the nature of interactions between psychiatric providers and other medical professionals
DPC GR/FE, 360
Be aware of different costs of health care for different services DPC, GD GR/FE
Demonstrate a basic understanding of medical‐legal issues in DL, DPC, GR/FE, WE
178
relations to inpatient psychiatry including:
• Admission of a child /adolescent by their parent and consent for treatment
• Abuse reporting • Patient/parent’s rights to refuse treatments including
medication • Custody issues (divorced parents, foster care,
adoption, social services) • Physician responsibility for balancing confidentiality
vs. parent’s right to know and reporting of potential harm to others
GD