Embed Size (px)
Citation preview

University of Groningen
Effect of clinical pathway implementation and patients' characteristics on outcomes ofcoronary artery bypass graft surgeryEl-Baz, Noha
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish tocite from it. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2009
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):El-Baz, N. E-S. H. (2009). Effect of clinical pathway implementation and patients' characteristics onoutcomes of coronary artery bypass graft surgery s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 07-11-2017

Noha El-Sayed Hussein El-Baz
CHAPTER 1 INTRODUCTION

Introduction
10

Chapter 1
11
CHAPTER 1 INTRODUCTION
General introduction, aims and outline
Coronary artery bypass graft (CABG) surgery is one of the most frequentlyperformed cardiac surgical procedures with unquestionable benefits, aimed atrelieving anginal symptoms and improving health related quality of life(HRQoL). In the past decades, there has been a great development in themethods of delivering care to CABG patients, one of which was the introductionof a clinical pathway. A clinical pathway (CP) is a method of delivering care thatwas developed in the 1980’s in the United States and since then it has beenwidely used in other parts of the world. Recently, the use of CP as a method ofdelivering care was initiated and introduced at the University Medical CenterGroningen (UMCG) in the Netherlands, where the Thoracic Surgerydepartment, UMCG, implemented a clinical pathway for patients undergoingCABG.This study was undertaken to investigate the effect of CABG pathway on thepatients’ outcomes. The outcomes investigated were length of stay (LOS),readmission and complications and outcomes that were rarely examined whenevaluating the effects of CABG pathways, such as health-related quality of life(HRQoL) and psychological distress (PD), i.e. anxiety and depression.Existing studies evaluating the effect of clinical pathways on outcomes ofpatients were mainly of poor methodological quality1. These studies alsoconcentrated on evaluating organization related outcomes, e.g. LOS and costs,and few articles investigated the effect of CPs on patients’ related outcomes, likecomplications, HRQoL, and psychological distress1. Therefore, the aim of ourstudy was to investigate the effect of implementing the CABG pathway plan onpatient related outcomes compared to patients in a conventional care plan. Thesignificance of the current study lies in the fact that it is a controlled study andwe investigated patients’ outcomes that were mainly rarely addressed bystudies evaluating the effect of pathways, e.g. HRQoL and psychologicaldistress. Furthermore, this study also reports on the role played by theEuroSCORE on predicting outcomes other than mortality, e.g. functional status,LOS, and postoperative complications. Moreover, we are presenting the effect ofother patients’ characteristics that can affect the desired outcomes of CABGsurgery as Type-D personality, and psychological distress (anxiety anddepression), and lastly the effect of positive affectivity on cardiac related healthcomplaints after CABG.In this chapter, we also present an overview of the epidemiology andpathophysiology of coronary artery disease (CAD) in order to present an outlineof the disease process and the development of anginal symptoms which in turn

Introduction
12
affect patients’ functional abilities. In addition, this introductory chapterpresents the significance of HRQoL measurements in patients undergoingcritical procedures, i.e. CABG, and reviews the process of development andevaluation of clinical pathways. Finally, at the end of this introductory chapterwe present a conceptual model that we developed based on the conceptual modelof Wilson and Cleary in 19952, which provided the basis for the researchquestions and the aims formulated.
1.1 Coronary artery disease
1.1.1 Epidemiological dataCoronary artery disease (CAD) is a leading cause of mortality and morbidity inthe developed world. It involves the narrowing or total occlusion of the arteriesthat provide oxygenated blood and nutrients to the cells of the heart as a resultof plaque forming on the lining of the arteries by the atherosclerotic process3. Inthe Netherlands, according to the Dutch Heart Foundation, the incidence ofcardiac infarction in 2004 in men was 32.000 and in women 36.000.Furthermore, it was found that the prevalence of ischemic heart diseases in bothmen and women 55 years was 277.300 in 2004, while mortality due to ischemicheart disease constituted 32,5% among the other diseases causing mortality in20034.The concept of ‘burden of disease’ combines mortality and morbidity into a singleindicator denoted as the Disability Adjusted Life Years (DALYs). According tothe Atlas of heart disease and stroke5. The disability-adjusted life years lost, canbe thought of as healthy years lost to a disease, and they indicate the totalburden of disease as opposed to simply the resulting deaths. By comparing thedata from the Netherlands with Egypt regarding DALYs, we may conclude thatthe burden of CAD in Egypt is three times higher compared to the Netherlands6.
1.1.2 PathophysiologyCAD is a chronic process that begins early in life, particularly duringadolescence, and slowly progresses throughout life7. The main cause of CAD isthe development of atherosclerosis. The word Atherosclerosis originates from theGreek words athera meaning gruel or paste or porridge and sclerosis meaninghardness. Risk factors of CAD include: older age, male gender, family history ofpremature coronary artery diseases, cigarette smoking, diabetes mellitus,hypertension, hyperlipidemia, inactive lifestyle, obesity and as well as stressedpersonality behavior8. These risk factors accelerate a complex and chronicinflammatory process that manifests as fibrous atherosclerotic plaque7,9.Recently, psychological distress presented in depression and anxiety10,11 were

Chapter 1
13
also proven to be risk factors for the development of CAD, and poorprognosis12,13.
1.2 Types of CADCoronary artery diseases can be classified into angina pectoris, myocardialinfarction (MI) and acute coronary syndrome (ACS).
1.2.1 Angina pectorisThe word angina comes from the Latin word meaning ‘to choke’14. Anginapectoris, however, is the term used to describe chest pain or discomfort thatresults from CAD. The patient may describe the sensation as pressure, fullness,squeezing, heaviness or pain15.
Angina can be classified into16:1. Angina pectoris: which is an uncomfortable sensation in the chest andneighboring anatomic structures produced by myocardial ischemia. Anginapectoris is caused by temporary, reversible myocardial ischemia induced by animbalance between myocardial oxygen demand and myocardial oxygen supply,which occurs as a result of atherosclerotic narrowing, arterial inflammation, andobstruction resulting from intense focal spasm of the coronary arteries. Othercauses of unstable angina are fever, tachycardia and thyrotoxicosis leading toincreased oxygen demand.2. Stable angina which is a chronic pattern of transient angina pectoris,precipitated by physical activity or emotional upset, relieved by rest within afew minutes. Episodes are associated with temporary depression of ST segment,but it does not result in permanent myocardial damage.3. Variant angina or angina inversa is a typical angina discomfort, usually atrest, that occurs in cycles and develops because of coronary artery spasm ratherthan an increase of myocardial oxygen demands. It is usually associated with STsegment elevation.4. Unstable angina is a pattern of increased frequency and duration of anginaepisodes produced by less exertion or at rest, there is also a high risk ofprogression to myocardial infarction if untreated16.
The severity of anginal symptoms can be classified either by New York HeartAssociation Functional Classification17 or Canadian Cardiovascular SocietyFunctional Classification18.The New York Heart Association (NYHA) Functional Classification placespatients in one of four categories based on how much they are limited duringphysical activity; the limitations/symptoms are in regards to normal breathing

Introduction
14
and varying degrees in shortness of breath and or angina pain. NYHA ClassSymptoms are classified into: Class (I) No symptoms and no limitation inordinary physical activity; Class (II) Mild symptoms (mild shortness of breathand/or angina) and slight limitation during ordinary activity; Class (III) Markedlimitation in activity due to symptoms, even during less-than-ordinary activity,e.g. walking short distances (20-100 m), and comfortable only at rest; Class (IV)Severe limitations: experiences symptoms even while at rest; mostly bedboundpatients.Furthermore, the Canadian Cardiovascular Society Angina Grading Scale is alsocommonly used for the classification of severity of angina and it is classified asfollows: Class (I) – Angina only during strenuous or prolonged physical activity;Class (II) – Slight limitation, with angina only during vigorous physical activity;Class (III) – Symptoms with everyday living activities, i.e. moderate limitation;and Class (IV) – Inability to perform any activity without angina or angina atrest, i.e. severe limitation.
1.2.2 Myocardial infarctionMyocardial infarction (MI) is the rapid development of myocardial necrosiscaused by a critical imbalance between oxygen supply and demand of themyocardium. This usually results from plaque rupture with thrombus formationin a coronary vessel, resulting in an acute reduction of blood supply to a portionof the myocardium19.The size of the infarction is determined by factors such as extent, severity andduration of ischemia, the size of the vessel affected and amount of collateralcirculation, the status of intrinsic fibrinolytic system, vascular tone, andmetabolic demands of the myocardium at time of event.MI mostly results in damage of the left ventricle, leading to compromise of leftventricular function. MI can also occur in the right ventricle or both ventricles.When all the tissues of the layers of the myocardium are necrotic it is calledtransmural infarction. As a result the pumping effect of the heart is affectedwhich compromises cardiac output20.Signs and symptoms of MI: the onset of symptoms in MI is usually gradual,lasting several minutes, and rarely instantaneous. Chest pain is the mostcommon symptom of acute myocardial infarction and is often described as asensation of tightness, pressure, or squeezing. Pain radiates most often to theleft arm, but may also radiate to the lower jaw, neck, right arm, back, andepigastrium, where it may mimic heartburn. Levine's sign, in which the patientlocalizes his chest pain by clenching his fist over the sternum, has classicallybeen thought to be predictive of cardiac chest pain, although a prospectiveobservational study showed that it had a poor positive predictive value21.

Chapter 1
15
Shortness of breath (dyspnea) occurs when the damage to the heart limits theoutput of the left ventricle, causing left ventricular failure and consequentpulmonary edema. Other symptoms include diaphoresis (an excessive form ofsweating), weakness, light-headedness, nausea, vomiting, and palpitations.These symptoms are likely induced by a massive surge of catecholamine fromthe sympathetic nervous system which occurs in response to pain and thehemodynamic abnormalities that result from cardiac dysfunction. Loss ofconsciousness (due to inadequate cerebral perfusion and cardiogenic shock) andeven sudden death (frequently due to the development of ventricular fibrillation)can occur in myocardial infarctions. Complications that may arise include:recurrent MI, cardiogenic shock, ventricular septal wall rupture, left ventricularwall rupture, pericarditis, thromboembolism, dysrhythmias, and conductiondisturbances caused by affection of sinoatrial (SA) and atrioventricular (AV)nodes.
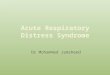
1.2.3 Acute coronary syndromeThe terminology acute coronary syndrome (Figure 1.) is used to describe clinicalsymptoms compatible with acute myocardial ischemia and includes unstableangina and acute MI. Unstable angina refers to unexpected chest pain ordiscomfort that occurs at rest. Patients with MI are either those with STsegment elevation MI or non-ST segment elevation MI22.
Figure 1. Clinical classification of acute coronary syndromes23
N QMI = non-Q - wave myocardial infarction; NSTEMI = non-ST elevation myocardial infarction;Q wave MI = Q wave myocardial infarction; ST = ST segment of ECG tracing

Introduction
16
1.3 Treatment of CADThe aim of therapy in patients with angina is to restore the balance betweenoxygen supply and oxygen demand. This can be achieved by modification of riskfactors, pharmacological therapy or invasive therapy.Pharmacological therapy includes nitroglycerin, morphine, beta blockers,calcium antagonists and anti-platelets therapy24. In case of MI, the medicaltherapy includes: thrombolytic therapy, oxygen therapy, nitroglycerine andmorphine sulfate. Invasive treatment includes percutaneous coronaryintervention (PCI) or (CABG).Cardiac rehabilitation: one of the important aspects of treating MI is cardiacrehabilitation. The rehabilitation program begins by preparing patients fordischarge following the initial treatment through education about the programwhich includes exercise, smoking cessation, lipid management, weight control,psychological intervention, blood pressure control and return to work. Familymembers are also included in the program, so they can learn about heartdiseases and help achieve the goals of the program.
1.3.1 Non invasive treatmentNon invasive treatment of CAD is aimed at controlling symptoms and slowing orstopping the progression of disease. The method of treatment is based on manyfactors determined by symptoms, a physical exam and diagnostic testing. Inmany cases, if the blockage is less than 70 percent, medications may be the firstline of treatment. Treatment includes modification of risk factors andmedication. Risk factors of CAD are either modifiable e.g. smoking, stress,obesity, high blood cholesterol, high blood pressure, physical inactivity, diabetesmellitus, alcohol and high fat diet or non modifiable, e.g. increased age, male sexand heredity factors (including race)15,19.The medications used to treat CAD include: anticoagulants, which help indecreasing the clotting (coagulating) ability of the blood, help to prevent harmfulclots from forming in the blood vessels and may prevent the clots from becominglarger and causing more serious problems. Antiplatelet agents most commonlyprescribed is Aspirin which keeps blood clots from forming by preventing bloodplatelets from sticking together in patients who have had a heart attack,unstable angina, ischemic strokes, or transient ischemic attacks. Angiotensin IIReceptor Blockers (or Inhibitors) prevent this angiotensin from having anyeffects on the heart and blood vessels, and prevent rise in blood pressure.Moreover, Beta Blockers which act to decrease the heart rate and cardiacoutput, subsequently lowering the blood pressure and making the heart beat ata slower rate and with reduced force, Calcium Channel Blockers interrupt themovement of calcium into the cells of the heart and blood vessels, which

Chapter 1
17
decreases the heart’s pumping strength and relaxes blood vessels, thus loweringthe blood pressure and chest pain related to reduced blood supply. Diuretics helpthe body to rid itself of excess fluids and sodium through urination, whichrelieves the heart's workload, decrease blood pressure and edema. Vasodilatorsrelax blood vessels and increase the supply of blood and oxygen to the heart,while reducing its workload leading to relief of chest pain. Digitalis increasesthe force of the heart's contractions, which can be beneficial in case of heartfailure and for irregular heart beats. Finally, statins are also prescribed tolower blood cholesterol level15,19,25.
1.3.2 Invasive treatment of CAD
1.3.2.1 Types of Invasive treatmentTreatment generally aims to reduce cardiac workload, improve coronary arteryblood flow, and, over the long term, slow down and reverse the atheroscleroticprocess. Coronary blood flow can be improved by PCI or CABG, our mainconcern in this study is CABG surgery.
Coronary artery bypass graft surgeryThe indications of CABG are listed in Table 1. according to the guidelinesestablished by the 2004 American College of Cardiology (ACC) and AmericanHeart Association (AHA).In CABG, native vessels or conduits are ‘harvested’ during the initial phase ofsurgery to reroute or bypass blood flow past diseases areas of coronary arteries.The first saphenous vein aortocoronary bypass graft was performed in 1964.Since then, the use of CABG has become an acceptable treatment for CAD.Selection of the graft or conduit depends on the diameter similar to coronaryarteries, absence of disease or wall abnormalities, and adequate length. Thecommonly used grafts are saphenous vein grafts, internal mammary arterygrafts, radial artery, and right gastroepiploic artery. After one year, about 85%of the venous bypass grafts are patent, but after ten years, as many as 97% ofthe internal mammary artery grafts are patent. Arteries show hypertrophy toaccommodate the increased blood flow, where veins do not.CABG has proved to be effective in relieving angina and improving exercisetolerance, and it prolongs life in patients with left main CAD and three vesselsdisease with poor left ventricular function. To decrease mortality associatedwith bypass surgery, it is necessary to consider several factors: urgency ofoperation, age, previous heart surgery, sex, left ventricular ejection fraction,percentage of stenosis of the left main coronary artery, and the number of major

Introduction
18

Chapter 1
19

Introduction
20
coronary arteries with greater than 70% stenosis.
Complications of CABGCABG is typically performed during cardiopulmonary bypass with the heartstopped; a heart lung machine pumps the blood, removes carbon dioxide (CO2)and oxygenates the blood. The main risks of the procedure include stroke andMI. For patients with a normal-sized heart, no history of MI, good ventricularfunction, and no additional risk factors, risk is < 5% for peri-operative MI, 2 to3% for stroke, and 1% for mortality; risk increases with age and presence ofunderlying disease. Operative mortality rate is 3 to 5 times higher for a secondbypass than for the first; thus, timing of the first bypass should be optimal.After cardiopulmonary bypass, about 25 to 30% of patients develop cognitivedysfunction, possibly caused by micro-emboli originating in the bypass machine.Dysfunction ranges from mild to severe and may persist for weeks to years. Tominimize this risk, some centers use a beating heart technique (i.e., nocardiopulmonary bypass), in which a device mechanically stabilizes the part ofthe heart upon which the surgeon is working.
Prognosis of CABGCAD may progress despite bypass surgery. Postoperatively, the rate of proximalobstruction of bypassed vessels increases. Vein grafts become obstructed early ifthrombi form and later (several years) if atherosclerosis causes slowdegeneration of the intima and media. Aspirin prolongs vein graft patency.Continued smoking has a profound adverse effect on patency.
1.4 The role of nursing care in CABG surgeryThe nursing care of patients is not limited to the postoperative period, butnurses are responsible for patients’ care during preoperative and postoperativephases. The main focus during preoperative phase involves: history recording,physical examination, diagnostic procedures, preoperative teaching, includingoperative procedure, intensive care unit (ICU), invasive lines and recoveryperiod. Postoperative care mainly includes transporting the patients to ICU,where they will recover from anesthesia and may remain for up to 24 hours aftersurgery.This phase involves monitoring of vital signs, cardiac output, connection tomechanical ventilator, measuring end-tidal CO2, SpO2, peripheral pulses andperfusion signs, output of chest tubes and body temperature to preventhypothermia. Once the patient is hemodynamically stable, urine output ismeasured and assessed, clinical data are obtained, chest radiograph, 12 leadECG, routine blood work, assessment of neurological status and pacemaker

Chapter 1
21
function. Furthermore, the patient is closely monitored for systematicinflammatory responses, severity and control of pain and prevention ofcomplications.The achievement of optimum patient outcomes following CABG surgery is theaim of health care providers involved in patient care, especially critical carenurses. In the past decades there has been a great focus on the use of managedcare, due to increased costs and demand for high quality care. This presented aunique challenge for critical care nurses to integrate theoretical knowledge,assessment skills, and problem solving ability to provide optimal, high qualitynursing care15,27.
1.5 Outcomes of coronary artery bypass graft surgeryCABG is an established treatment procedure with clear benefits, includingsymptom relief, prolonged survival and improved health related quality of life.Studies evaluating the effect of CABG primarily concentrated on mortalityrates, occurrence of complications and length of stay in the health care facility.In the past decades there has been a great interest in the effect of both CABGthe factors affecting HRQoL before and after the operation. Several studies wereconducted to examine whether patient related factors28-36, such as: (i) age, (ii)sex, (iii) educational level, (iv) type of work, (v) marital status and (vi) socialsupport, or clinical variables such as: (vii) severity of illness, (viii) leftventricular ejection fraction (LVEF), (ix) multiple vessels diseases 28,30,33,35,37 andrecently the role of (x) psychological distress (anxiety and depression)31, and (xi)type of personality38-40 affect the HRQoL of patients after CABG.
1.5.1 HRQoL in relation to critical illnessOver the last decades quality of life (QoL) has become an increasingly importantconcept in evaluating healthcare outcomes in several fields of critical care,including open heart surgery, which is considered a major surgery and the firstfew months after surgery are considered a critical and crucial period.Nevertheless, some clinicians disregard HRQoL measures as they perceive themas “soft” or “not as scientific” as physiological measures41. However, health carepersonnel working in any critical or intensive care setting recognizes that apatient’s physical status at discharge is only a preliminary measure of success oftherapeutic outcomes. Short term outcomes include changes in clinical statusand improvement or relief of symptoms, while long term outcomes take intoconsideration the impact of hospitalization, undergoing a critical procedure (e.g.open heart surgery), and the nature of care the patient receives followingsurgery in ICU or intermediate care units on his HRQoL after discharge.

Introduction
22
There is a need for longer period of assessment to evaluate the meaningfuleffects of the treatment received. In order to assure that clinical protocols haveresulted in the required outcomes, symptoms relief and return to normalfunctioning. More importantly, a patient’s perception of his health is unique andthe main factor in explaining and predicting outcomes. Thus, HRQoL measuresshould be advocated in critical care research42. Currently, there has been a greatinterest in the effect of critical care and treatment on HRQoL. Several studieshave attempted to address this issue and came up with the conclusion thatHRQoL measurement is an important aspect of patient care, evaluation andfollow-up43-49.
1.5.2 CABG, HRQoL and related factorsSeveral studies28,29,31-35,50,51 investigated the effect of CABG surgery on HRQoLand also factors affecting HRQoL after CABG. Their findings were mainly thatCABG improved HRQoL in the majority of patients and there were severalfactors that affected this outcome.These factors can be classified into patients related characteristics, e.g. age,female gender, marital status, type of work, personality trait, smoking habits,high alcohol intake and high socioeconomic deprivation28-35,52, and biological andmedical factors, such as diabetes mellitus, a body mass index of >35kg/m2,chronic obstructive pulmonary disease, peripheral vascular disease, NYHA classat baseline, gastrointestinal problems, congestive heart failure, decreased forcedexpiratory pressure, LVEF, elevated serum creatinine53, and health status atbaseline54, sleep problems, hypertension, infection55, history of psychiatricdiseases, postoperative events, like hospital readmission, and not following arehabilitation program after CABG. Furthermore, mood disturbances andpsychological aspects, like depression and anxiety, were also found to play amajor role in affecting patients HRQoL undergoing CABG56-58,59. It was reportedthat a higher score of depression at baseline has been shown to predictdeterioration in mental HRQoL60.Risk stratification models for cardiac surgery, like the Parsonnet score61,62 andCleveland Clinic score63, were developed over the last few decades mainly topredict operative mortality. Currently, the European System of Cardiac-Operative Risk Evaluation score (EuroSCORE) is a widely used operative risk-prediction tool, that has been shown to be a valuable measure for prediction ofoperative mortality related to adult cardiac surgery64,65. Higher levels ofEuroSCORE were associated with increased in-hospital and thirty-daymortality, longer stay in the ICU and more frequent readmission. However, veryfew studies attempted to investigate whether risk stratification models,specifically EuroSCORE, can predict postoperative HRQoL66-68.

Chapter 1
23
1.6 The clinical pathway experienceThe following section presents the history of CPs development and the use of CPin the UMCG, in addition to the process of designing, implementing andevaluating a CPs.
1.6.1 Early phases of CP developmentIn the early 1980’s critical pathways were developed in The New EnglandMedical center in Boston, Massachusetts in the United States of America. CPsare also referred to as clinical pathway, integrated care pathway, care map, andmultidisciplinary action plan. CPs have been developed in health care asmultidisciplinary care plans that outline the sequence and timing of actions,necessary for achieving expected patient outcomes and organizational goals,regarding quality, costs, patient satisfaction and efficiency.The concept of CPs refers to specific guidelines for care that describe patienttreatment goals and define a sequence and timing of intervention for meetingthose goals efficiently. They can also be defined as care plans that detailessential steps in patient care with a view to describing the expected progress ofthe patient69. The use of CPs has become very popular in the past decades in alot of diseases and surgical procedures. CABG pathway as designed containedthe following components: assessment, consultations, rehabilitation, tests,treatments, activities, diet and nutrition, elimination, medications, educationand counseling of patients and their families, and preparation for discharge.The efficacy of CPs designed for patients undergoing CABG were mainlydescribed in studies without randomized clinical trial design or did not use(matched) control groups70,71. Studies that compared CP with standard care onlyevaluated the success of the pathway on decreasing length of stay and costs72,73,but recently studies have shifted to evaluate the effects of CPs on otheroutcomes like readmission, complications, patients’ satisfaction, and quality oflife74-76. In a recent review article we recommended that more (randomized)controlled studies should be conducted in which patients are randomly assignedto the condition of either a pathway or conventional care, and that standardizedtools should be used to measure important outcomes, like HRQoL, cardiacrelated complaints, anxiety and depression.
1.6.2 Clinical pathways in the UMCGThe department of Thoracic Surgery in the UMCG decided in the spring of 2004to implement a CP for patients undergoing CABG surgery. Collaboration wasstarted between the former Care Sciences Department at the Medical Facultyand the department of Thoracic Surgery to evaluate the effect of the clinicalpathway on patient outcomes, including: physical and mental functioning

Introduction
24
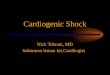
(overall HRQoL), quality of care, LOS, hospital waiting time till surgery,psychological stress, use of health services, patient expectation of care and staffjob satisfaction. The process of developing, implementing and evaluating theclinical pathway is presented in Figure 2.
The Steering CommitteeThe formulation of the CP was overseen by a Steering Committee (stuurgroep)that planned the designing, and implementation of the CP. The SteeringCommittee consisted of: the head of the Thoracic Surgery Department, thenursing care manager of the Thoracic Center, the head of Anesthesiology andthe coordinator of Thoracic Anesthesia.The Committee provided support to determine what is needed to initiate thepathway, determine the needed resources, and direct all disciplines involved inthe pathway. The Committee conducted a review of literature to evaluateexisting LOS in the UMCG and also determined the best practice available.Next, the committee facilitated the setting of the actual team that developed thepathway and assisted the team in overcoming any difficulties. The project teamincluded the head nurse of Thoracic Surgery, acute care nurse practitioner, staffnurse, physiotherapist, social worker and dietician. The Committee alsodetermined that 8 days-CP was suitable for the patient population at theUMCG.Furthermore, the latest patient care evidence based guidelines were revised. Allthe current protocols were also revised and updated, and new protocolsregarding sternal wound infection control, nutrition and pain control wereadded.
Development of the pathwayThe pathway team, which included all disciplines involved in patient care,determines the type and sequence of care that will be provided to the patient, inaddition to the daily goals that must be achieved in order to reach the clinicaloutcomes expected by the time of discharge. The pathway comprised of 8 daystemplate and comprised of the following elements: general assessment,circulation, respiration, intake and output balance, pain relief, neurological,nutrition/metabolism, physiotherapy, activity/movement, and patientinformation/education.
Education of the staffThe development and implementation of CP require changes and modificationsin clinical practice, and patient care in the Thoracic Surgery unit. Thus, the staff

Chapter 1
25
members of different disciplines involved in patient care received educationalsessions about the components of the pathway before the implementation.
Patient interactive educational sessionsDuring the pre-operative period, patients who were visiting the out-patientclinic were invited to join interactive education sessions. Patients were alsoinformed about what to expect during the immediate preoperative, postoperativeperiods till discharge (in the pathway), and were invited to express their feelingsof anxiety and their concerns about surgery and recovery. Furthermore, patientswere provided with booklets with information regarding surgery and expectedoutcomes.
Tracking of variances (Appendix II.)Variances occur when the patient does not follow the plan and sequence outlinedin the CP. Variances can be classified into patient or family, care provider orclinician, hospital or system, or community. Patient variances occur when apatient develops a complication or is unable to reach a goal set in the pathwayplan. Care provider variance is when a staff member or clinician does not carryout the task that is crucial for a patient to be discharged on the preset time.Hospital or system variance is due to inefficiencies such as not scheduling a teston time. Finally, community variances occur when discharge is postponed,because the patient needs further care that can not be arranged after discharge.Tracking and analyzing variances facilitates the patient’s progress along the CP.When the CP fails to meet 70% of the patients needs, the pathway should bereevaluated. Variance data are collected every few months and analyzed forrepeating trends or patterns. It is recommended that the pathway be evaluatedevery six months. Tracking of variances was performed by a nursing director atthe UMCG and a full variance analyses report was presented to the ThoracicSurgery Department
Outcome evaluationThe efficacy of the pathway is determined by measuring patient outcomes.Outcomes measured include: LOS (meeting discharge date), readmission rate,morbidity, mortality and patient satisfaction. In this study we also measureHRQoL, health complaints, anxiety and depression.

Introduction
26
Figure 2. The process of designing, implementing and evaluating the clinicalpathway
1.7 The conceptual modelThe central concepts of this study are introduced in a conceptual model (Figure3.) based on a model developed by Wilson and Cleary, 199577, and themodifications of Spertus et al,. 200278, and Rumsfeld, 200241. The Wilson andCleary model has been used in several publications investigating the factorsaffecting HRQoL33,79-83.Wilson and Cleary proposed a valuable framework for classifying predictors ofHRQoL. They distinguished physiological/biological factors, symptoms(including emotional and cognitive variables), individual patient characteristics,such as gender or age51,54 and environmental characteristics, such as provision ofservices, e.g. cardiac rehabilitation84.The biological/physiological or medical characteristics that have been constantlyrelated to poor HRQoL outcomes after CABG include the New York HeartAssociation (NYHA) classification of dyspnoea, current smoking, poor leftventricular ejection fraction, presence of a chronic disease, such as diabetes, orpulmonary disease as chronic obstructive pulmonary disease (COPD), operativerelated variables, such as complications arising from the surgery that may wellalso affect HRQoL after surgery28,30,50,51,54,85,86. In our model we also added theEuroSCORE as variable affecting HRQoL. Recently, there has been an interestin whether there is an association between the EuroSCORE and HRQoL66,68,87,88
(Figure 3).

Chapter 1
27
Furthermore, the model includes symptoms of depression and anxiety that havean effect on mental HRQoL and worse outcomes after CABG. It is of note that inpatients scheduled for CABG the prevalence of depressive symptoms is high89.Preoperative anxiety and depression has been known to predict the incidence ofadverse symptoms or psychopathology following surgery13,90-94. A study by Höferand colleagues31 found that depression has the main indirect effect on HRQoL inCAD patients. Thus, we included in our model psychological factors (anxiety anddepression) in addition to positive and negative affectivity95-99.Moreover, We included patients’ characteristics that have been linked to poorHRQoL outcomes after coronary procedure, such as age and gender. Youngerpatients30,100 have reported more physical improvement in HRQoL compared toolder patients30,50. The findings regarding the influence of gender, reported thatwomen benefit less from CABG in relation to HRQoL30,80,101,102. Othersocioeconomic data, such as marital status or having a partner85,103 working ornot33, have been associated with poor HRQoL. We also took into account the typeof personality (Type-D personality), which has been found to affect HRQoL aftercardiac related intervention39,104-106.In relation to environmental influence on HRQoL outcomes used cardiacrehabilitation (CR) program attendance is one of the factors affecting HRQol84,107. In our model, we further added the effect of method of care provided, i.e.care in a CP plan to determine it’s effect on HRQoL and psychological distress.Other outcomes we included were the effects of these variables on cardiacrelated complaints after CABG, which we measured using the healthcomplaints scales (HCS)108. Thus, it is theorized here that physiological,psychological, and environmental variables influence symptom status, which inturn affects functional health and general health perceptions, which influencesoverall HRQoL. Furthermore, we are addressing the issue of the discrepancybetween the expected effect of surgery, which is an improvement in cardiacfunction and which is the main focus of clinicians, versus patient focus, which ismainly concerned with the interpretation of this improvement into a meaningfulchange in his functional status and HRQoL. In light of this proposed model weformulated our research questions.

Introduction
28

Chapter 1
29
1.8 Research questionsFinally, we present the research questions of this thesis, which were developedbased on the presented conceptual model.
1. Are the outcomes of CPs really evidence-based given the methodological andstatistical conclusion validity?
2. What is the difference between the CP group and the conventional care groupin relation to LOS, complications, readmission, HRQoL and psychologicaldistress? Does a CP contribute towards an improved HRQoL six months afterCABGas compared to a conventional care trajectory?
3. Does physical and mental HRQoL assessed with self-reported SF-36 differacross classes of the EuroSCORE before and six months after CABG? Is theEuroSCORE a predictor of physical and mental domains of HRQoL six monthsafter CABG?
4. What are the predictors of deterioration HRQoL six months following CABG?Do anxiety and depression mediate the effect of type D personality ondeterioration in HRQoL using structural equation modeling?
5. What is the impact of positive affectivity on cardiac-related health complaintsin CABG surgery patients?
1.9 Outline of the thesisFollowing this introductory chapter, Chapter 2 is a systematic reviewaddressing the question whether the outcomes of CPs are evidence-based andprovides a critical appraisal of the evaluation studies that examined the effectsof clinical pathways. Chapter 3 presents the effect of implementing a CABGpathway on patients’ outcomes in comparison with conventional care. Itaddresses short term outcomes like: LOS, hospital delay, readmission andcomplications, and long term outcomes, like HRQoL and psychological distress.The focus is mainly the question regarding whether pathway patients gainedmore in their HRQoL compared to patients who received conventional care.Chapter 4 reports on the use of EuroSCORE as a predictor of health relatedphysical functioning six months after CABG and highlights the associationbetween EuroSCORE and physical functioning before and after CABG, inaddition to the association between EuroSCORE and LOS, and number ofcomplications.

Introduction
30
Chapter 5 is addressing the important topic of factors associated withdeterioration in health after CABG. In this chapter we present the results of aregression model and a structural equation model that highlights the role playedby PD, i.e. anxiety and depression and Type D personality in deterioration ofpatients HRQoL six months after CABG. Whilst Chapter 6 is mainly presentingthe results of investigating the impact of positive affectivity and age on cardiacrelated health complaints measured by health complaints scales in CABGsurgery. Chapter 7 summarizes the main results of the thesis, generalconclusion concerning the main objectives of the thesis are formulated anddiscussed, and finally, implications for future research and clinical practicediscussed and formulated.

Chapter 1
31
1.10 Reference List1. El Baz N, Middel B, van Dijk J, Oosterhof A, Boonstra P, Reijneveld S. Are theoutcomes of clinical pathways evidence-based? A critical appraisal of clinical pathwayevaluation research. Journal of Evaluation in Clinical Practice 2007; 13:920-929.2. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. Aconceptual model of patient outcomes. Jama 1995; 273(1):59-65.3.Hirani SP, Patterson DLH, Newman SP. What Do Coronary Artery Disease PatientsThink about Their Treatments? An Assessment of Patients' Treatment Representations.J Health Psychol 2008; 13(3):311-322.4. Hart - en vaatziekten in Nederland 2005. cijfers over risicofactoren, ziekte,behandeling, en sterfte. 1-21. 2005. Nederlands Hartstichting.5. McKay J, Mensah GA. The Atlas of Heart Disease and Stroke. 2004. Geneva, WorldHealth Organization.6. Hart - en vaatziekten in Nederland 2005. cijfers over risicofactoren, ziekte,behandeling, en sterfte. 1-21. 2005. Nederlands Hartstichting.7. American Heart Association. Heart Disease and Stroke Statistics. 2006.8. Jenkins CD. Behavioral Risk Factors in Coronary Artery Disease. Annual Review ofMedicine 1978; 29(1):543-562.9. Nanda N, Bobby Z, Hamide A, Koner B, Sridhar M. Association between oxidativestress and coronary lipid risk factors in hypothyroid women is independent of body massindex. Metabolism 2007; 56(10):1350-1355.10. Nicholson A. Psychological distress as a predictor of CHD events in men: the effect ofpersistence and components of risk. Psychosom Med 2005; 67(4):522-530.11. Vural M. Association between depression and anxiety symptoms and majoratherosclerosis risk factors in patients with chest pain. The Tohoku journal ofexperimental medicine 2007; 212(2):169-175.12. Kop WJ. Acute and chronic psychological risk factors for coronary syndromes:moderating effects of coronary artery disease severity. Journal of PsychosomaticResearch 1997; 43(2):167-181.13. Shibeshi WA. Anxiety worsens prognosis in patients with coronary artery disease.Journal of the American College of Cardiology 2007; 49(20):2021-2027.14. Miklaucich M. Limitations on life: women's lived experiences of angina. Journal ofAdvanced Nursing 1998; 28(6):1207-1215.15. Morton PG, Fontaine D, Hudak CM, Gallo BM. Critical Care Nursing: A HolisticApproach. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2005.16. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS et al.ACC/AHA guideline update for the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction--2002: summary article: a report of theAmerican College of Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee on the Management of Patients With Unstable Angina).Circulation 2002; 106(14):1893-1900.17. Criteria Committee, New York Heart Association. Diseases of the heart and bloodvessels. Nomenclature and criteria for diagnosis. 6th ed. Boston: Little, Brown and co;1964.

Introduction
32
18. Campeau L. Letter: Grading of angina pectoris. Circulation 1976; 54(3):522-523.19. Willerson JT, Wellens HJ, Cohn JN, Holmes DR. Cardiovascular Medicine. 3rd ed.London: Springer; 2007.20. Cunningham S. Pathophysiology of myocardial ischemia and infarction.In Woods,S.L., Froelicher, E.S., Motzer, S.U.: Cardiac Nursing. 4th ed. Philadelphia: LippincottWilliams & Wilkins.; 2000. 495-505.21. Marcus GM. The utility of gestures in patients with chest discomfort. The Americanjournal of medicine 2007; 120(1):83-89.22. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS et al.ACC/AHA guideline update for the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction--2002: summary article: a report of theAmerican College of Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee on the Management of Patients With Unstable Angina).Circulation 2002; 106(14):1893-1900.23. Alpert JS. Myocardial infarction redefined--a consensus document of The JointEuropean Society of Cardiology/American College of Cardiology Committee for theredefinition of myocardial infarction. Journal of the American College of Cardiology2000; 36(3):959-969.24. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, Hochman JS et al.ACC/AHA guideline update for the management of patients with unstable angina andnon-ST-segment elevation myocardial infarction--2002: summary article: a report of theAmerican College of Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee on the Management of Patients With Unstable Angina).Circulation 2002; 106(14):1893-1900.25. Pathophysiology of heart disease ; A collaborative project of medical students andfaculty. 4th ed. Philadelphia: Lippincott Williams &Wilkins; 2007.26. Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ et al.ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report ofthe American College of Cardiology/American Heart Association Task Force on PracticeGuidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass GraftSurgery). Circulation 2004; 110(14):e340-e437.27. Margereson C, Riley J. Cardiothoracic Surgical Nursing: Current Trends in AdultCare. Blackwell Publishing; 2003.28. Al-Ruzzeh S. Predictors of poor mid-term health related quality of life after primaryisolated coronary artery bypass grafting surgery. Heart 2005; 91(12):1557-1562.29. Hawkes AL, Mortensen OS. Up to one third of individual cardiac patients have adecline in quality of life post-intervention. Scandinavian Cardiovascular Journal 2006;40(4):214-218.30. Herlitz J, Brandrup-Wognsen G, Caidahl K, Haglid M, Karlson BW, Hartford M etal. Improvement and factors associated with improvement in quality of life during 10years after coronary artery bypass grafting. Coronary Artery Disease 2003; 14(7):509-517.31. Hofer S, Doering S, Rumpold G, Oldridge N, Benzer W. Determinants of health-related quality of life in patients with coronary artery disease. European Journal ofCardiovascular Prevention & Rehabilitation 2006; 13(3):398-406.

Chapter 1
33
32. Jarvinen O, Saarinen T, Julkunen J, Laurikka J, Huhtala H, Tarkka MR. Improvedhealth-related quality of life after coronary artery bypass grafting is unrelated to use ofcardiopulmonary bypass. World Journal of Surgery 2004; 28(10):1030-1035.33. Le Grande MR, Elliott PC, Murphy BM, Worcester MU, Higgins RO, Ernest CS et al.Health related quality of life trajectories and predictors following coronary artery bypasssurgery. Health and Quality of Life Outcomes 2006; 4.34. Lindsay GM, Hanlon P, Smith LN, Wheatley DJ. Assessment of changes in generalhealth status using the short-form 36 questionnaire 1 year following coronary arterybypass grafting. European journal of cardio-thoracic surgery 2000; 18(5):557-564.35. Muller-Nordhorn J, Kulig M, Binting S, Voller H, Gohlke H, Linde K et al. Change inquality of life in the year following cardiac rehabilitation. Quality of Life Research 2004;13(2):399-410.36. Panagopoulou E, Montgomery A, Benos A. Quality of life after coronary arterybypass grafting: evaluating the influence of preoperative physical and psychosocialfunctioning. Journal of Psychosomatic Research 2006; 60(6):639-644.37. Welke KF, Stevens JP, Schults WC, Nelson EC, Beggs VL, Nugent WC. Patientcharacteristics can predict improvement in functional health after elective coronaryartery bypass grafting. Ann Thorac Surg 2003; 75(6):1849-1855.38. Denollet J. DS14: Standard Assessment of Negative Affectivity, Social Inhibition,and Type D Personality. Psychosom Med 2005; 67(1):89-97.39. Pedersen SS, Denollet J. Type D personality, cardiac events, and impaired quality oflife: a review. European journal of cardiovascular prevention and rehabilitation 2003;10(4):241-248.40. Pedersen SS, Theuns DAMJ, Muskens-Heemskerk A, Erdman RAM, Jordaens L.Type-D personality but not implantable cardioverter-defibrillator indication isassociated with impaired health-related quality of life 3 months post-implantation.Europace 2007; 9(8):675-680.41. Rumsfeld JS. Health status and clinical practice: when will they meet? Circulation2002; 106(1):5-7.42. Jordan-Marsh M. The SF-36 quality-of-life instrument: updates and strategies forcritical care research. Crit Care Nurse 2002; 22(6):35-43.43. Kanaskie ML, Tringali CA. Promoting quality of life for geriatric oncology patients inacute care and critical care settings. Crit Care Nurs Q 2008; 31(1):2-11.44. Eastwood JA, Doering L, Roper J, Hays RD. Uncertainty and health-related qualityof life 1 year after coronary angiography. American Journal of Critical Care 2008;17(3):232-242.45. Orwelius L. Prevalence of sleep disturbances and long-term reduced health-relatedquality of life after critical care: a prospective multicenter cohort study. Critical care2008; 12(4):R97.46. Weinert CR. Health-related quality of life after acute lung injury. American journalof respiratory and critical care medicine 1997; 156(4 Pt 1):1120-1128.47. Fildissis G. Quality of life outcome of critical care survivors eighteen months afterdischarge from intensive care. Croatian medical journal 2007; 48(6):814-821.

Introduction
34
48. Grady KL, Meyer P, Mattea A, Dressler D, Ormaza S, White-Williams C et al.Predictors of quality of life at 1 month after implantation of a left ventricular assistdevice. American Journal of Critical Care 2002; 11(4):345-352.49. Thomas SA, Friedmann SA, Kao CW, Inguito P, Metcalf M, Kelley FJ et al. Qualityof life and psychological status of patients with implantable cardioverter defibrillators.American Journal of Critical Care 2006; 15(4):389-398.50. Rumsfeld JS, Ho PM, Magid DJ, McCarthy M, Shroyer ALW, MaWhinney S et al.Predictors of health-related quality of life after coronary artery bypass surgery. Annalsof Thoracic Surgery 2004; 77(5):1508-1513.51. Simchen E, Galai N, Braun D, Zitser-Gurevich Y, Shabtai E, Naveh I.Sociodemographic and clinical factors associated with low quality of life one year aftercoronary bypass operations: The Israeli Coronary Artery Bypass Study (ISCAB). Journalof Thoracic and Cardiovascular Surgery 2001; 121(5):909-919.52. Panagopoulou E, Montgomery A, Benos A. Quality of life after coronary arterybypass grafting: evaluating the influence of preoperative physical and psychosocialfunctioning. Journal of Psychosomatic Research 2006; 60(6):639-644.53. Rumsfeld JS, Ho PM, Magid DJ, McCarthy M, Shroyer ALW, MaWhinney S et al.Predictors of health-related quality of life after coronary artery bypass surgery. Annalsof Thoracic Surgery 2004; 77(5):1508-1513.54. Welke KF, Stevens JP, Schults WC, Nelson EC, Beggs VL, Nugent WC. Patientcharacteristics can predict improvement in functional health after elective coronaryartery bypass grafting. Annals of Thoracic Surgery 2003; 75(6):1849-1855.55. Al Ruzzeh S, Athanasiou T, Mangoush O, Wray J, Modine T, George S et al.Predictors of poor mid-term health related quality of life after primary isolated coronaryartery bypass grafting surgery. Heart 2005; 91(12):1557-1562.56. Chocron S, Etievent JP, Viel JF, Dussaucy A, Clement F, Alwan K et al. Prospectivestudy of quality of life before and after open heart operations. Ann Thorac Surg 1996;61(1):153-157.57. Hawkes AL, Mortensen OS. Up to one third of individual cardiac patients have adecline in quality of life post-intervention. Scandinavian Cardiovascular Journal 2006;40(4):214-218.58. Hofer S, Doering S, Rumpold G, Oldridge N, Benzer W. Determinants of health-related quality of life in patients with coronary artery disease. European Journal ofCardiovascular Prevention & Rehabilitation 2006; 13(3):398-406.59. Ruo B, Rumsfeld JS, Hlatky MA, Liu H, Browner WS, Whooley MA. Depressivesymptoms and health-related quality of life: the Heart and Soul Study. JAMA 2003;290(2):215-221.60. Le Grande MR, Elliott PC, Murphy BM, Worcester MU, Higgins RO, Ernest CS et al.Health related quality of life trajectories and predictors following coronary artery bypasssurgery. Health and Quality of Life Outcomes 2006; 4.61. Lawrence DR, Valencia O, Smith EEJ, Murday A, Treasure T. Parsonnet score is agood predictor of the duration of intensive care unit stay following cardiac surgery.Heart 2000; 83(4):429-432.

Chapter 1
35
62. Parsonnet V, Dean D, Bernstein AD. A Method of Uniform Stratification of Risk forEvaluating the Results of Surgery in Acquired Adult Heart-Disease. Circulation 1989;79(6):3-12.63. Kurki TS, Jarvinen O, Kataja MJ, Laurikka J, Tarkka M. Performance of threepreoperative risk indices; CABDEAL, EuroSCORE and Cleveland models in aprospective coronary bypass database. European journal of cardio-thoracic surgery 2002;21(3):406-410.64. Biancari F, Kangasniemi OP, Luukkonen J, Vuorisalo S, Satta J, Pokela R et al.EuroSCORE predicts immediate and late outcome after coronary artery bypass surgery.Annals of Thoracic Surgery 2006; 82(1):57-61.65. De Maria R, Mazzoni M, Parolini M, Gregori D, Bortone F, Arena V et al. Predictivevalue of EuroSCORE on long term outcome in cardiac surgery patients: a singleinstitution study. Heart 2005; 91(6):779-784.66. Colak Z. Health related quality of life following cardiac surgery--correlation withEuroSCORE. European journal of cardio-thoracic surgery 2008; 33(1):72-76.67. Loponen P, Luther M, Nissinen J, Wistbacka J, Biancari F, Laurikka J et al.EuroSCORE predicts health-related quality of life after coronary artery bypass grafting.Interactive cardiovascular and thoracic surgery 2008;icvts.68. Peric V, V. The relationship between EuroSCORE preoperative risk prediction andquality of life changes after coronary artery by-pass surgery. Interactive cardiovascularand thoracic surgery 2005; 4(6):622-626.69. Renholm M, Leino-Kilpi H, Suominen T. Critical pathways: a systematic review.Journal of Nursing Administration 2002; 32(4):196-202.70. Velasco FT, Ko W, Rosengart T, Altorki N, Lang S, Gold JP et al. Cost containmentin cardiac surgery: results with a critical pathway for coronary bypass surgery at theNew York hospital-Cornell Medical Center. Best practices and benchmarking inhealthcare 1996; 1(1):21-28.71. Zevola DR, Raffa M, Brown K, Hourihan EC, Maier B. Clinical pathways andcoronary artery bypass surgery. Crit Care Nurse 1996; 17(6):20-33.72. Anderson B. Critical pathways: application to selected patient outcomes followingcoronary artery bypass graft. Applied nursing research 1999; 12(4):168-174.73. Rumble SJ, Jernigan MH, Rudisill PT. Determining the effectiveness of criticalpathways for coronary artery bypass graft patients: retrospective comparison ofreadmission rates. Journal of Nursing Care Quality 1996; 11(2):34-40.74. Corcoran WE. Quality of life as an outcome-based evaluation of coronary arterybypass graft critical paths using the SF-36. Quality Management in Health Care 2000;8(2):72-81.75. Porter HB. Health Resources utilization and quality of life outcomes of low riskcoronary artery bypass graft patients : a comparison study. Canadian Journal ofCardiovascular Nursing 1998; 9(1):10-15.76. Walters J, Schwartz C, Monaghan H, Watts J, Shlafer G, Deeb G et al. Long-termoutcome following case management after coronary artery bypass surgery. Journal ofcardiac surgery 1998; 13:123-128.77. Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. Aconceptual model of patient outcomes. Jama 1995; 273(1):59-65.

Introduction
36
78. Spertus JA, Tooley J, Jones P, Poston C, Mahoney E, Deedwania P et al. Expandingthe outcomes in clinical trials of heart failure: the quality of life and economiccomponents of EPHESUS (EPlerenone's neuroHormonal Efficacy and SUrvival Study).Am Heart J 2002; 143(4):636-642.79. Mathisen L, Andersen MH, Veenstra M, Wahl AK, Hanestad BR, Fosse E. Quality oflife can both influence and be an outcome of general health perceptions after heartsurgery. Health and Quality of Life Outcomes 2007; 5.80. Penckofer S, Ferrans CE, Fink N, Barrett ML, Holm K. Quality of life in womenfollowing coronary artery bypass graft surgery. Nursing Science Quarterly 2005;18(2):176-183.81. Sousa KH, Kwok OM. Putting wilson and cleary to the test: Analysis of a HRQOLconceptual model using structural equation modeling. Quality of Life Research 2006;15(4):725-737.82. Valderas JM, Alonso J. Patient reported outcome measures: a model-basedclassification system for research and clinical practice. Quality of Life Research 2008;17(9):1125-1135.83. Ye LC, Liang ZA, Weaver TE. Predictors of health-related quality of life in patientswith obstructive sleep apnoea. Journal of Advanced Nursing 2008; 63(1):54-63.84. Simchen E, Naveh I, Zitser-Gurevich Y, Brown D, Galai N. Is participation in cardiacrehabilitation programs associated with better quality of life and return to work aftercoronary artery bypass operations? The Israeli CABG study. Israel Medical AssociationJournal 2001; 3(6):399-403.85. Allen JK, Young DR, Xu X. Predictors of long-term change in functional status aftercoronary artery bypass graft surgery in women. Progress in cardiovascular nursing1998; 13(2):4-10, 27.86. Falcoz PE, Chocron S, Stoica L, Kaili D, Puyraveau M, Mercier M et al. Open heartsurgery: One-year self-assessment of quality of life and functional outcome. Annals ofThoracic Surgery 2003; 76(5):1598-1604.87. El Baz N, Middel B, Van Dijk JP, Wesselman DC, Boonstra PW, Reijneveld SA.EuroSCORE predicts poor health-related physical functioning six month postcoronaryartery bypass graft surgery. Journal of cardiovascular surgery 2008; 49(5):663-672.88. Loponen P, Luther M, Nissinen J, Wistbacka J, Biancari F, Laurikka J et al.EuroSCORE predicts health-related quality of life after coronary artery bypass grafting.Interactive cardiovascular and thoracic surgery 2008;icvts.89. Cheok F, Schrader G, Banham D, Marker J, Hordacre AL. Identification, course, andtreatment of depression after admission for a cardiac condition: Rationale and patientcharacteristics for the Identifying Depression As a Comorbid Condition (IDACC) project.American Heart Journal 2003; 146(6):978-984.90. Duits AA, Boeke S, Taams MA, Passchier J, Erdman RAM. Prediction of quality oflife after coronary artery bypass graft surgery: A review and evaluation of multiple,recent studies. Psychosom Med 1997; 59(3):257-268.91. Jenkins CD, Stanton BA, Jono RT. Quantifying and predicting recovery after heartsurgery. Psychosom Med 1994; 56(3):203-212.92. Pignay-Demaria V, V. Depression and anxiety and outcomes of coronary arterybypass surgery. The Annals of Thoracic Surgery 2003; 75(1):314-321.

Chapter 1
37
93. Saur CD, Granger BB, Muhlbaier LH, Forman LM, McKenzie RJ, Taylor MC et al.Depressive symptoms and outcome of coronary artery bypass grafting. American Journalof Critical Care 2001; 10(1):4-10.94. Vingerhoets G. Perioperative anxiety and depression in open-heart surgery.Psychosomatics 1998; 39(1):30-37.95. Denollet J. Emotional Distress and Fatigue in Coronary Heart-Disease - the GlobalMood Scale (Gms). Psychological Medicine 1993; 23(1):111-121.96. Denollet J, De Vries J. Positive and negative affect within the realm of depression,stress and fatigue: The two-factor distress model of the Global Mood Scale (GMS).Journal of Affective Disorders 2006; 91(2-3):171-180.97. Prather AA, Marsland AL, Muldoon MF, Manuck SB. Positive affective style covarieswith stimulated IL-6 and IL-10 production in a middle-aged community sample. BrainBehavior and Immunity 2007; 21(8):1033-1037.98. Pressman SD, Cohen S. Does positive affect influence health? Psychological Bulletin2005; 131(6):925-971.99. Steptoe A, Wardle J, Marmot M. Positive affect and health-related neuroendocrine,cardiovascular, and inflammatory processes. Proceedings of the National Academy ofSciences of the United States of America 2005; 102(18):6508-6512.100. Gjeilo KH, Wahba A, Klepstad P, Lydersen S, Stenseth R. Health-related quality oflife three years after coronary surgery: a comparison with the general population.Scandinavian Cardiovascular Journal 2006; 40(1):29-36.101. Loponen P. Quality of life during 18 months after coronary artery bypass grafting.European journal of cardio-thoracic surgery 2007; 32(1):77-82.102. Vaccarino V, Lin ZQ, Kasl SV, Mattera JA, Roumanis SA, Abramson JL et al. SexDifferences in Health Status After Coronary Artery Bypass Surgery. Circulation 2003;108(21):2642-2647.103. Husak L. Social support as a predictor of participation in cardiac rehabilitationafter coronary artery bypass graft surgery. Journal of cardiopulmonary rehabilitation2004; 24(1):19-26.104. Denollet J. DS14: Standard Assessment of Negative Affectivity, Social Inhibition,and Type D Personality. Psychosom Med 2005; 67(1):89-97.105. Pedersen SS, Theuns DAMJ, Muskens-Heemskerk A, Erdman RAM, Jordaens L.Type-D personality but not implantable cardioverter-defibrillator indication isassociated with impaired health-related quality of life 3 months post-implantation.Europace 2007; 9(8):675-680.106. Pedersen SS, Daemen J. Type-D personality exerts a stable, adverse effect on vitalexhaustion in PCI patients treated with paclitaxel-eluting stents. Journal ofPsychosomatic Research 2007; 62(4):447-453.107. Smith KM, Naveh I, Zitser-Gurevich Y, Brown D, Galai N. Differences insustainability of exercise and health-related quality of life outcomes following home orhospital-based cardiac rehabilitation. European journal of cardiovascular prevention andrehabilitation 2004; 11(4):313-319.108. Denollet J. Health complaints and outcome assessment in coronary heart disease.Psychosom Med 1994; 56(5):463-474.

Introduction
38