Embed Size (px)
DESCRIPTION
Citation preview

1
IN THE NAME OF GOD
CARDIOGENIC PULMONARY
EDEMA

2
Cardiogenic pulmonary edema

3
CPECPE due to:• increased capillary hydrostatic
pressure secondary to elevated pulmonary venous pressure

4
following major pathophysiologic mechanisms:
• Imbalance of Starling forces - Ie, increased pulmonary capillary pressure, decreased plasma oncotic pressure, increased negative interstitial pressure
• Damage to the alveolar-capillary barrier• Lymphatic obstruction• Idiopathic (unknown) mechanism

5
Mechanism of CPE
• alveolar-capillary membrane• Increase of net flux of fluid from the
vasculature into the interstitial space• Net flow of fluid across a membrane is
determined by applying the following equation:
Q = K(Pcap - Pis) - l(Pcap - Pis)•

6

7
Lymphatics
• 10-20 mL/h• acute rise in pulmonary arterial capillary
pressure (ie, to >18 mm Hg)• chronically elevated LA pressure, the rate
of lymphatic removal can be as high as 200 mL/h

8
Stages
Stage 1• elevated LA pressure→ distention and
opening of small pulmonary vessels• blood gas exchange does not deteriorate

9
Stage 2
• fluid and colloid shift into the lung interstitium from the pulmonary capillaries→but an initial increase in lymphatic outflow efficiently removes the fluid
• may overpower the drainage capacity of the lymphatics

10
Stage 2
• mild hypoxemia• Tachypnea→stimulation of
juxtapulmonary capillary (J-type)

11
Stage 3
• alveolar flooding• abnormalities in gas exchange• vital capacity and other respiratory
volumes are substantially reduced• hypoxemia becomes more severe

12
Cardiac disorders manifesting as CPE
• Atrial outflow obstruction• LV systolic dysfunction• LV diastolic dysfunction• Dysrhythmias• LV hypertrophy and cardiomyopathies• LV volume overload• Myocardial infarction• LV outflow obstruction

13
Presentation
• History
• Physical Examination

14
History
Symptoms• Sudden (acute)• Long-term (chronic)

15
Sudden (acute)
• Extreme shortness of breath or difficulty breathing (dyspnea) that worsens when lying down
• A feeling of suffocating or drowning• Wheezing or gasping for breath• Anxiety, restlessness or a sense of apprehension• A cough that produces frothy sputum that may
be tinged with blood

16
Sudden (acute)
• Excessive sweating• Pale skin• Chest pain, if pulmonary edema is caused
by heart disease• A rapid, irregular heartbeat (palpitations)

17
Long-term (chronic)
• Having more shortness of breath than normal when you're physically active
• Difficulty breathing with exertion, often when you're lying flat as opposed to sitting up
• Wheezing• Awakening at night with a breathless feeling
that may be relieved by sitting up• Rapid weight gain

18
Long-term (chronic)
• Swelling in your legs and ankles• Loss of appetite• Fatigue• Ortner sign?

19
Physical Examination
• Tachypnea • Tachycardia• sitting upright→air hunger• Confuse• agitate • anxious • diaphoretic

20
• Hypertension • Hypotension indicates severe LV systolic
dysfunction and the possibility of cardiogenic shock
• Cool extremities may indicate low cardiac output and poor perfusion.

21

22
Auscultation
• fine, crepitant rales• rhonchi or wheezes may also be present• Cardiovascular findings→S3,accentuation
of the pulmonic component of S2, jugular venous distention
• Auscultation of murmurs→acute valvular disorders

23
Auscultation
• Aortic stenosis→ harsh crescendo-decrescendo systolic murmur, which is heard best at the upper sternal border and radiating to the carotid arteries
• acute aortic regurgitation→short, soft diastolic murmur
• Acute mitral regurgitation produces a loud systolic murmur heard best at the apex or lower sternal border

24
• Mitral stenosis typically produces a loud S1, opening snap, and diastolic rumble at the cardiac apex
• skin pallor or mottling→peripheral vasoconstriction, low cardiac output

25
Severe CPE→mental status→hypoxia or hypercapnia
hypercapnia with respiratory acidosis may be seen in patients with severe CPE or underlying chronic obstructive pulmonary disease (COPD).

26
Diagnostic Considerations
Cardiogenic pulmonary edema (CPE) should be differentiated from pulmonary edema associated with injury to the alveolar-capillary membrane, caused by diverse etiologies.

27
DDx
• Acute Respiratory Distress Syndrome• Asthma• Cardiogenic Shock• Chronic Obstructive Pulmonary Disease• Emphysema• Goodpasture Syndrome• Myocardial Infarction

28
DDx
• Pneumothorax• High-altitude pulmonary edema• Neurogenic pulmonary edema• Pulmonary embolism• Respiratory failure

29
DDx
• Pneumocystis (carinii) jiroveci Pneumonia
• Pneumonia, Bacterial• Pneumonia, Viral

30
differentiate CPE from NCPE
• In CPE, a history of an acute cardiac event is usually present
• low-flow state• S3 gallop• jugular venous distention• crackles on auscultation

31
differentiate CPE from NCPE
Patients with NCPE have a warm periphery, a bounding pulse, and no S3 gallop or jugular venous distention
Definite differentiation is based on pulmonary capillary wedge pressure (PCWP) measurements. The PCWP is generally >18 mm Hg in CPE and < 18 mm Hg in NCPE, but superimposition of chronic pulmonary vascular disease can make this distinction difficult to assess.

32
Workup
Lab studies• Complete blood count• Serum electrolyte measurements• Blood urea nitrogen (BUN) and creatinine• Pulse oximetry• Arterial blood gas analysis

33
Electrocardiography
• LA enlargement• LV hypertrophy• acute tachydysrhythmia• bradydysrhythmia • acute myocardial ischemia or infarction

34
BNP
EFFECTS
1.Vasodilation
2. Diuresis
3. Natriuresis
4. Suppression of Renin Angiotensin Sys

35
BNP testing
• high negative predictive value; that is, in patients with BNP value of under 100 pg/mL, heart failure is unlikely
Values of 100-400 pg/mL may be related to various pulmonary conditions, such as cor pulmonale, COPD, and pulmonary embolism.

36
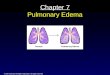
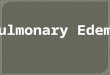
RadiographyChest radiography is helpful in distinguishing CPE from other
pulmonary causes of severe dyspnea.
Features that suggest CPE rather than NCPE and other lung pathologies include the following:
• Enlarged heart• Inverted blood flow• Kerley lines• Basilar edema (vs diffuse edema)• Absence of air bronchograms• Presence of pleural effusion (particularly bilateral and
symmetrical pleural effusions)

37

38

39

40

41

42
Echocardiographyimportant diagnostic tool in determining the etiology of
pulmonary edema
helpful in identifying a mechanical etiology for pulmonary edema, such as the following:
• Acute papillary muscle rupture• Acute ventricular septal defect• Cardiac tamponade• Contained LV rupture• Valvular vegetation with resulting acute severe
mitral, aortic regurgitation

43
Pulmonary Arterial Catheter
PCWP can be measured with a pulmonary arterial catheter (Swan-Ganz catheter)
This method helps in differentiating CPE from NCPE
A PCWP exceeding 18 mm Hg in a patient not known to have chronically elevated LA pressure indicates CPE.

44
Treatment
Following initial management, medical treatment of CPE focuses on 3 main goals
(1) reduction of pulmonary venous return (preload reduction)
(2) reduction of systemic vascular resistance (afterload reduction)
(3) inotropic support

45
Treatment
Patients with severe LV dysfunction or acute valvular disorders may present with hypotension. These patients may not tolerate medications to reduce their preload and afterload. Therefore, inotropic support is necessary in this subset of patients to maintain adequate blood pressure.

46
Ventilatory Support
• Noninvasive pressure-support ventilation
• Mechanical ventilation

47
Preload Reduction
• Nitroglycerin• Diuretics• Morphine sulfate• Nesiritide

48
Afterload Reduction
• ACE inhibitors• Angiotensin II receptor blockers• Nitroprusside• Phosphodiesterase inhibitors

49
Inotropic support
• Dobutamine• Dopamine• Norepinephrine• Phosphodiesterase inhibitors• Calcium sensitizers

50
SUMMARY
ABC
REDISTRIBUTE FLUID OUT OF LUNGS!
1ST Line: Nitrates
2 ND Line: ACE Inhibitors
3RD Line: Diuretics
NIPPV – use early !
Milrinone – preferred inotrope

51