Embed Size (px)
Citation preview
University of Groningen
Biodegradable plates and screws in oral and maxillofacial surgeryBuijs, Gerrit Jacob
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2011
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Buijs, G. J. (2011). Biodegradable plates and screws in oral and maxillofacial surgery. s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 06-01-2022
BIODEGRADABLE PLATES
AND SCREWS IN ORAL
AND MAXILLOFACIAL
SURGERY
Thesis
Jappe Buijs
The research presented in this thesis was performed at the Department of Oral and
Maxillofacial Surgery, University Medical Centre Groningen, The Netherlands.
This research was financially supported by:
Board of the UMCG, www.umcg.nl
Straumann, www.straumann.com
Camlog, www.pro-cam.nl
Nobel Biocare, www.nobelbiocare.com
BioComp, www.biocomp.euInion Ltd., www.inion.com
ConMed Linvatec Biomaterials Ltd., www.conmed.com
KLS Martin, www.klsmartin.com
Synthes, www.synthes.com
Dental Union, www.dentalunion.nl
Henry Schein, www.henryschein.nl NVGPT, www.nvgpt.nl
Fred Ribôt tandtechniek, www.fredribot-tandtechniek.nl
Examvision, www.examvision.nl
© Gerrit Jacob Buijs, 2011All rights reserved.
No parts of this publication may be transmitted, in any form or by any means,
without permission of the author.
Bookdesign: Sgaar Groningen
Printed by: Drukkerij van der Eems Heerenveen
ISBN: 978-90-367-4966-4
RIJKSUNIVERSITEIT GRONINGEN
BIODEGRADABLE PLATES
AND SCREWS IN ORAL
AND MAXILLOFACIAL
SURGERY
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. E. Sterken,
in het openbaar te verdedigen op
woensdag 14 september 2011
om 16.15 uur
door
Gerrit Jacob Buijs
geboren op 18 november 1980
te Purmerend
Promotores: Prof. dr. R.R.M. Bos
Prof. dr. B. Stegenga
Prof. dr. G.J. Verkerke
Copromotor: Dr. J. Jansma
Beoordelingscommissie: Prof. dr. dr. K.L. Gerlach
Prof. dr. J. de Lange
Prof. dr. D.B. Tuinzing
Paranimfen: N.B. van Bakelen
H.J.W.E. de Lange

CONTENTS
Chapter 1 09General introduction
Chapter 2 17Efficacy and Safety of Biodegradable Osteofixation Devices in Oral and Maxillofacial Surgery: a Systematic ReviewG.J. Buijs, B. Stegenga, R.R.M. Bos
Published in: J Dent Res. 2006 Nov;85(11):980-9.
Chapter 3.1 35Torsion Strength of Biodegradable and Titanium Screw Systems: a Comparison
G.J. Buijs, E.B. van der Houwen, B. Stegenga, R.R.M. Bos, G.J. Verkerke
Published in: J Oral Maxillofac Surg. 2007 Nov;65(11):2142-7.
Chapter 3.2.1 47Mechanical Strength and Stiffness of Biodegradable and Titanium Osteofixation SystemsG.J. Buijs, E.B. van der Houwen, B. Stegenga, R.R.M. Bos, G.J. Verkerke
Published in: J Oral Maxillofac Surg. 2007 Nov;65(11):2148-58.
Chapter 3.2.2 65Mechanical Strength and Stiffness of the Biodegradable SonicWeld Rx Osteofixation SystemG.J. Buijs, E.B. van der Houwen, B. Stegenga, R.R.M. Bos, G.J. Verkerke
Published in: J Oral Maxillofac Surg. 2009 Apr;67(4):782-7.
Chapter 4 79Biodegradable and Titanium Fixation Systems in Oral and Maxillofacial Surgery: a Randomized Controlled TrialG.J. Buijs, N.B. van Bakelen, J. Jansma, J.G.A.M. de Visscher, Th.J.M. Hoppenreijs,
J.E. Bergsma, B. Stegenga, R.R.M. Bos
Submitted
Chapter 5 93General discussion and future perspectives
Chapter 6 99Reference List
Chapter 7 115Summary
Chapter 8 121Dutch summary
Dankwoord 127
CHAPTER 1
GENERAL
INTRODUCTION

10 11
CH
AP
TE
R 1
GENERAL INTRODUCTION
Field of interest
Traumatic injuries in the maxillofacial region and dentofacial anomalies may have
considerable physical and psychological impact on patients. Therefore, major efforts
should be carried out to anatomically and aesthetically restore form and function of the
maxillofacial hard and soft tissues in such cases (6). The maxillofacial skeleton consists
of 3 parts: the cranium, the mid-face, and the mandible. The mandible articulates with
the base of the skull at the left and right temporomandibular joint and at the level of
the dental occlusion, and is powered by forceful masticatory muscles. This biomechani-
cal system allows people to perform important functions, such as chewing, swallowing,
laughing, and speaking. Physically, the mandible is a heavily loaded bony structure and,
consequently, its cortex is thick and compact. By contrast, the mid-face consists of thin-
walled cavities, strengthened by bony buttresses absorbing forces exerted through the
muscles of the maxillofacial skeleton (7).
The diagnosis and treatment of facial fractures and dentofacial anomalies play a
prominent role within oral and maxillofacial surgery. Through population growth,
increase of traffic, industrialization, violence and sport, the field of traumatology has
considerably increased. Today, of the fractures, approximately 55% are caused by traffic
accidents, 20% by accidental falls, and 17% by assaults (8). The wearing of helmets and
seatbelts and the general introduction of airbags in automobiles were major steps for-
ward in the prevention of trauma. In general, good clinical results are currently achieved
in both maxillofacial traumatology and dentofacial orthopedics primarily because of
advanced diagnostic radiographic methods as well as refined surgical techniques and
fixation materials.
Diagnostic radiographic methods
Diagnostic radiographic methods are essential (1) to determine the exact extent of sus-
pected maxillofacial fractures, and (2) for the diagnosis and treatment planning of oste-
otomies. Three-dimensional (3D) visualization of the bony skeleton and the dentition can
be obtained by Computed Tomography (CT) and is the golden standard for fractures.
The images are very precise and the surgeon can determine preoperatively where the
plates and screws should be placed to acquire immobilization of the bone fragments. A
disadvantage of CT examination is the relatively high radiation exposure. Recently, Cone
Beam Computed Tomography (CBCT) has been developed, which is faster and produces
less radiation (9). Conventional images, such as a panoramic radiograph and a fronto-
suboccipito radiograph, are the standard recordings to assess mandibular fractures. In
case of (para)median fractures, axial radiograph may provide additional information. A
panoramic radiograph and a lateral cephalogram are the standard radiographs for oste-
otomies of the mandible and maxilla.
Requirements for adequate bone healing
Essential aspects for bone healing of fractures and osteotomies are sufficient vasculariza-
tion, anatomical reduction, and immobilization of bone segments (7;10). The treatment
of nearly all maxillofacial fractures and osteotomies is currently performed by an open
surgical approach to have a better control of the (re)positioning of bone fragments (6;11).
Immobilization is obtained using fixation plates and screws. Various compressive, tensile,
and torsion forces need to be counteracted by the plates and screws at the fracture
crevice and the osteotomy site. After most of the mandibular fractures, the bone takes
over compressive forces, whereas the osteosynthesis devices counteract the lost tensile
forces. This is called load sharing between the bone and the plates and screws. In case
of bony defects, comminuted fractures and bi-lateral sagittal split osteotomies, a plate
is fully loaded for bending forces and is called load bearing. Load sharing allows plate
and screw dimensions that are much smaller than those necessary for load bearing. The
next sections comprise a review of the development of different fixation systems used
for immobilization.
Refined surgical techniques and development of fixation material
Closed fracture management – In the first half of the past century maxillofacial trau-
mata were predominantly treated in a closed (i.e. non-surgical) manner. Immobilization
of bone segments was achieved with InterMaxillary Fixation (IMF) in most cases. Stain-
less steel ligatures were tied up along the dental arches so that the correct dental oc-
clusion could be achieved, whereas in more difficult cases the upper or the lower jaw
could additionally serve as a template. Sophisticated external frame fixation devices were
applied to achieve immobilization in severe multi-fragment situations (12). An external
frame was usually secured with plaster of Paris, bandages or plastic head caps (13). Figure
1. Man with fixation ‘apparatus’ fixed with plaster of Paris. These devices were generally
uncomfortable, patient-unfriendly and had a rather gruesome appearance (6;13). They
immobilize the temporomandibular joints resulting in cartilage degeneration. Moreover,
the requirements for optimal bone healing could not be acquired. For example, fractures
and osteotomies above the Le Fort I level were difficult to immobilize with these external
devices (6). The transfer pins from the bone segments to the external fixtures facilitate
an easy entry of bacteria to the healing bone. Treatment without an open intervention
impedes surgeons to anatomically re-position the bone segments.
Open fracture management – In the second half of the past cen-
tury there was a shift from closed to open surgical treatment. Besides
the improved anaesthetic techniques and infection control, especially
the development of the so-called training- or function-stable fixation
materials, was responsible for this shift. Training-stable means ‘moving
without loading’ whereas function-stable means ‘moving and loading’.
CH
AP
TE
R 1
Figure 1. Man with fixation ‘apparatus’ fixed with plaster of Paris
12 13
Starting with wire osteosynthesis, surgeons made bur holes through both bone
fragments after careful stripping of the periostium. Subsequently, a wire was tied up
through the bur holes and the ends were twisted along each other (14). Due to the
open fracture management, there was a better control of repositioning the dislocated
fragments (6). The fragments could better be stabilized with wire osteosynthesis
compared to external fixation devices. Nonetheless, wire osteosynthesis were not able to op-
timally stabilize bone fragments in order to acquire training- of even function-stable fixation.
The first fixation systems that obtained sufficient stability to immediately restore the
functions of the maxillofacial skeleton were developed in 1957 by the “Arbeitsgemein-
schaft für Osteosynthese fragen” (AO), a Swiss study group. This study group used the
ideas of the fixation of fractures of the long bones published by Danis in 1947 (15). The
emergence of these plates and screws heralded, in the 60s of last century, the era of
training- and function-stable osteosynthesis system. With these systems fracture frag-
ments could anatomically be stabilized and held in position, and could be directly and
functionally loaded. With these plates and screws, it was possible to obtain a certain
stress on the fracture segments against each other. Because of this stress, the fracture
crevice obtained a resistance to friction and mobility. This so-called compression system
was later ingeniously built into the screw holes of the plates, where the screw heads, with
eccentric screw placement, could build up the required axial interfragmental compression
between the bone fragments. These plates are called dynamic compression plates, or
DCP plates (16-18). During the healing period, stability of the fracture is maintained for
approximately 6 to 8 weeks. The acquired compression does not lead to bone necrosis,
whereas the remodelling of the bone compensates for the instability that might arise
from the gradual decrease of the compression. When using this type of fixation, the for-
mation of callus, estimated as a sign of lack of stability could be prevented.
Initially, plates for application in the lower jaw with bicortical screws were developed to
achieve the desired stability analogous to the fixation of fractures in long bones (19-21).
Given the choice for bicortical anchoring of the screws and in order to avoid damage to
the roots of the teeth and nerve structures, the only safe place for these systems was
the lower border of the mandible. In terms of mechanical stress, this was the most de-
manding and the least favourable position to compensate dislocating forces. Often, these
plates were applied via an extra-oral approach and required a disadvantageous large skin
incision and wide stripping of the periostium to insert and apply the voluminous plates.
An advantage of these relatively large and bulky plates was that they were strong enough
to bridge bony defects, bone grafts, and comminute fractures used for reconstructions.
Late in the 70s, a mini-plate system for the mandible was introduced by Champy et. al.
(22;23). These small plates have much smaller dimensions than the AO-plates that were
used for the fixation of fractures of the facial skeleton. The system was derived from
the ‘midface’ fixation system launched by Michelet in 1973 (24). The size of the mini-
plates was adapted to a mechanically more favourable location for fixation of mandibular
fractures (Figure 1).
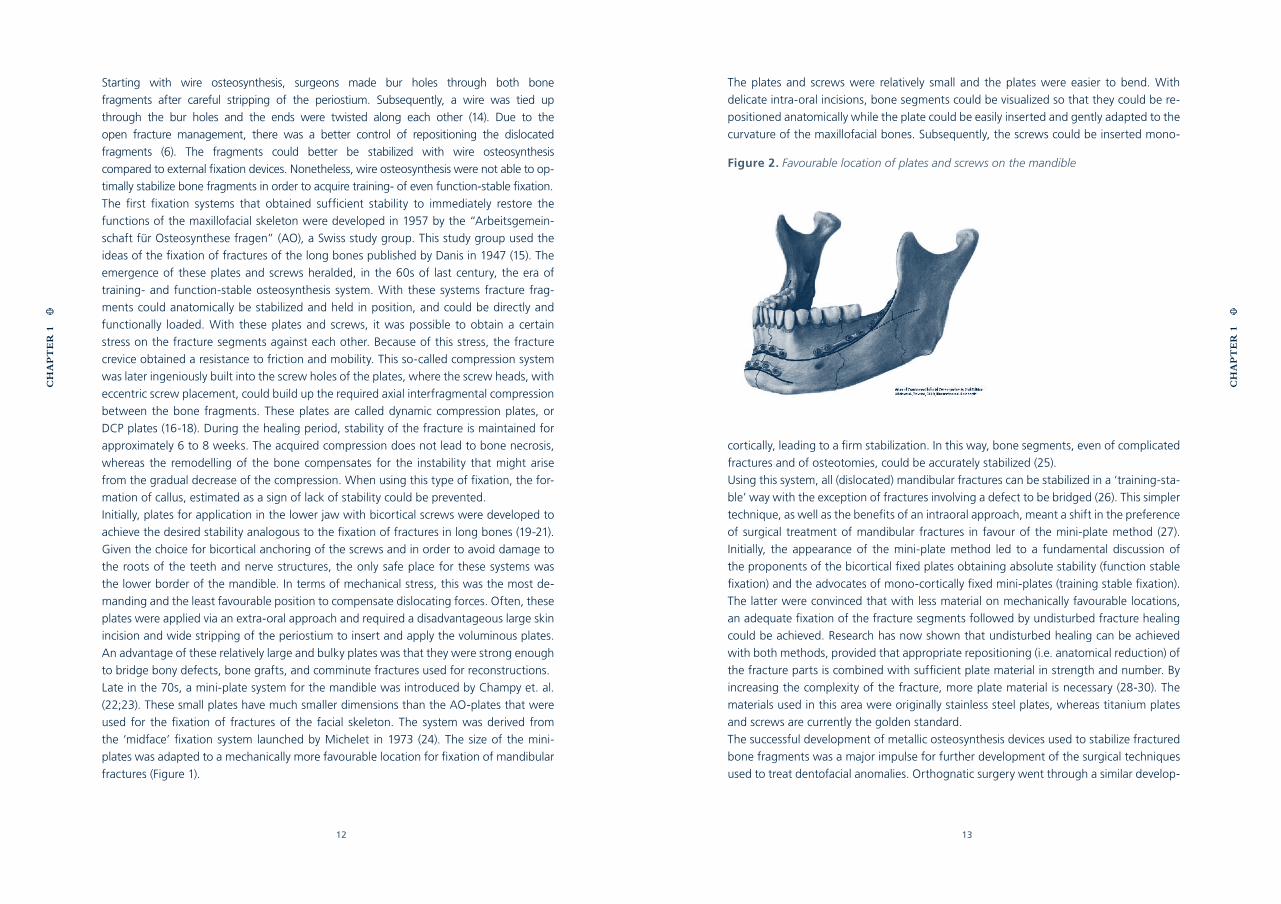
The plates and screws were relatively small and the plates were easier to bend. With
delicate intra-oral incisions, bone segments could be visualized so that they could be re-
positioned anatomically while the plate could be easily inserted and gently adapted to the
curvature of the maxillofacial bones. Subsequently, the screws could be inserted mono-
cortically, leading to a firm stabilization. In this way, bone segments, even of complicated
fractures and of osteotomies, could be accurately stabilized (25).
Using this system, all (dislocated) mandibular fractures can be stabilized in a ‘training-sta-
ble’ way with the exception of fractures involving a defect to be bridged (26). This simpler
technique, as well as the benefits of an intraoral approach, meant a shift in the preference
of surgical treatment of mandibular fractures in favour of the mini-plate method (27).
Initially, the appearance of the mini-plate method led to a fundamental discussion of
the proponents of the bicortical fixed plates obtaining absolute stability (function stable
fixation) and the advocates of mono-cortically fixed mini-plates (training stable fixation).
The latter were convinced that with less material on mechanically favourable locations,
an adequate fixation of the fracture segments followed by undisturbed fracture healing
could be achieved. Research has now shown that undisturbed healing can be achieved
with both methods, provided that appropriate repositioning (i.e. anatomical reduction) of
the fracture parts is combined with sufficient plate material in strength and number. By
increasing the complexity of the fracture, more plate material is necessary (28-30). The
materials used in this area were originally stainless steel plates, whereas titanium plates
and screws are currently the golden standard.
The successful development of metallic osteosynthesis devices used to stabilize fractured
bone fragments was a major impulse for further development of the surgical techniques
used to treat dentofacial anomalies. Orthognatic surgery went through a similar develop-
Figure 2. Favourable location of plates and screws on the mandible
CH
AP
TE
R 1
CH
AP
TE
R 1
14 15
ment for its fixation materials as did cranio-maxillofacial traumatology starting with wire
osteosynthesis in combination with IMF to only plate and/or screw fixation and postop-
erative guiding elastics. With orthognatic surgery osteotomized jaws are put into new po-
sitions thus changing facial anatomy and dental occlusion. In a way this can be considered
as non-anatomical reposition and fixation of facial fractures, often leaving gaps that are
bridged with osteosynthesis plates. The mechanical properties of the fixation materials
used for this type of surgery are therefore of utmost importance and can probably not be
compared with fracture treatment on a one-to-one ratio.
Characteristics of titanium devices
Titanium plates and screws are made of pure titanium or titanium alloys. The biocompat-
ibility (31) and the strength of titanium has been thoroughly investigated in many scien-
tific studies. Conventional titanium fixation devices have several disadvantages, which
can be summarized as follows:
1. in some patients, particularly those with thin soft tissues, the edges of the inserted
(large) plates and screws can be felt. Dehiscence can also occur in situations where the
overlying mucosa or skin is very thin. In extreme climates, plates and screws can lead to
sensitivity to high or low temperatures;
2. migration and displacement represents the limitation of the use of titanium plates and
screws in the growing bones of children or infants;
3. exact bending of the plates is an essential requirement for successful repositioning of the bone
fragments. This pre-shaping is time consuming, especially when using voluminous plates;
4. titanium plates and screws interfere with imaging techniques, such as computed to-
mography and magnetic resonance imaging. The interference with radio-therapeutic
treatment techniques is also disadvantageous. The plates and screws can block the radio-
therapeutic beam resulting in an inadequate treatment;
5. the most significant disadvantage is probably the continued presence of plates and
screws in the human body after the material has fulfilled its function. Despite its bio-
compatibility, titanium still is a foreign body for the human organism. This generates
controversies among experts as to whether implant removal is necessary or not. There is
consensus that a follow-up implant removal operation is sometimes indicated (5 - 40%)
(32-34), particularly in young patients with growing bone. Implant removal implies an ad-
ditional surgical procedure with all its associated disadvantages of time, costs, infection
risk, discomfort, and anaesthesia.
Characteristics of biodegradable devices
Since about 4 decades, there is a continuous drive to explore the feasibility of
biodegradable devices for the fixation of fractures and osteotomies. The introduction
of biodegradable implants can be helpful in eliminating and reducing the disadvantages
of titanium plates and screws. Research has revealed that biodegradable materials have
limitations as well:
1. most biodegradable plates or meshes must be heated before they can be shaped. The
screw holes must be drilled and tapped. This is disadvantageous for difficult and time-
consuming craniofacial operations where many plates and screws must be used;
2. low mechanical stability still represents an important issue of the biodegradable sys-
tems, particularly when used in load bearing areas such as the mandible;
3. the manufacturers of the biodegradable fixation devices have increased the dimen-
sions due to the low mechanical strength and stiffness of the polymer based fixation
devices. The enlarged dimensions could result in difficult wound closure and an increased
risk to develop dehiscence;
4. to our best knowledge, there is no definitive evidence that demonstrates that biode-
gradable (co)polymers can be fully degraded and resorbed by the human body. However,
the possible advantage of disappearing fixation devices still seems to be an appealing
alternative to fix bone segments in specific situations.
AIMS OF THIS THESIS
The performance of the currently used titanium fixation systems has been thoroughly
evaluated. Titanium systems have been proven to be adequate fixation devices except
for the disadvantageous aspects mentioned above. Biodegradable fixation devices seem
to be an attractive alternative as these systems can reduce or even erase the negative
aspects of titanium systems. During the search for the ideal fixation system, the local ana-
tomical circumstances, the forces exerted through the maxillofacial skeleton, as well as
the advantages and disadvantages of titanium and biodegradable fixation devices should
be taken into account.
The general aim of this research project was to establish the effectiveness and safety of
biodegradable plates and screws to fix bone segments in the maxillofacial skeleton as a
potential alternative to metallic ones.
More specifically, the aims of this research project were:
- to review the currently available scientific evidence for the applicability of biodegrad
able plates and screws for the fixation of bone segments in the maxillofacial skeleton
(chapter 2);
- to establish the torsion strength of titanium and biodegradable fixation screws
(chapter 3.1);
- to establish the tensile strength and stiffness, bending stiffness, and torsion stiffness
of titanium and biodegradable fixation systems (chapter 3.2.1 and 3.2.2)
- to establish the short term effectiveness and safety (chapter 4) of biodegradable
plates and screws used for fixation of fractures and osteotomies in the maxillofacial
skeleton compared to conventional titanium plates and screws.
CH
AP
TE
R 1
CH
AP
TE
R 1
CHAPTER 2
EFFICACY AND SAFETY
OF BIODEGRADABLE
OSTEOFIXATION DEVICES IN
ORAL AND MAXILLOFACIAL
SURGERY: A SYSTEMATIC
REVIEW
G.J. BUIJS
B. STEGENGA
R.R.M. BOS
Published in: J Dent Res. 2006 Nov;85(11):980-9.
18 19
CH
AP
TE
R 2
Abstract:
Background - The use of osteofixation devices should be evidence-based in order to se-
cure uncomplicated bone healing. Numerous studies describe and claim the advantages
of biodegradable over titanium devices as a bone fixation method.
Objective - To systematically review the available literature to determine the clinical ef-
ficacy and safety of biodegradable devices compared with titanium devices in oral and
maxillofacial surgery. In addition, related general aspects of bone surgery are discussed.
Methods & materials - A highly sensitive search in the databases of MEDLINE (1966-
2005), EMBASE (1989-2005) and CENTRAL (1800-2005) was conducted to identify eligi-
ble studies. Eligible studies were independently evaluated by two assessors using a quality
assessment scale.
Results - The study selection procedure revealed four methodologically ‘acceptable’ arti-
cles. Owing to the different outcome measures used in the studies, it was impossible to
perform a meta-analysis. Therefore, the major effects regarding the stability and morbid-
ity of fracture fixation using titanium and biodegradable fixation systems were qualita-
tively described.
Conclusion & discussion - Any firm conclusions regarding the fixation of traumatically
fractured bone segments cannot be drawn due to the lack of controlled clinical trials. Re-
garding the fixation of bone segments in orthognathic surgery, only a few controlled clin-
ical studies are available. There does not appear to be a significant short-term difference
between titanium and biodegradable fixation systems regarding stability and morbidity.
However, definite conclusions, especially with respect to the long-term performance of
biodegradable fixation devices used in maxillofacial surgery, cannot be drawn.
Abbreviations used in this paper are: CENTRAL, Cochrane Central Register of Control-
led Trials; MeSH, Medical Subject Heading; VAS, Visual Analogue Scale; and W, weight.
Key words: Biodegradable, osteofixation, treatment, stability, morbidity, systematic
review.
INTRODUCTION
Background
Maxillofacial traumatology and orthognathic surgery are major fields of oral and
maxillofacial surgery. Internal rigid fixation systems are used for fixation and stabilization
of osteotomized or fractured bone segments (35;36). Plates and screws are generally
made of titanium and are currently regarded as the golden standard (4;37;38).
Titanium fixation systems can be used safely and effectively (35;39). The intrinsic
mechanical properties ensure that the device dimensions are kept within acceptable limits.
The handling characteristics of titanium systems are simple and efficient (40). However,
titanium devices also have disadvantages. These systems interfere with radiotherapy
(37;41;42) and imaging techniques. Besides, titanium implants have been associated
with complications such as growth restriction and brain damage (43;44), infection, and
possible mutagenic effects (45).
A second intervention to remove the implants implies additional surgical discomfort, risks,
and associated socio-economical costs (43;46-48). A plate removal percentage of 11.1%
in Le Fort I osteotomies due to infection and plate exposure has been reported (49). In a
retrospective study of 279 patients with isolated mandibular fractures, a plate removal
percentage of 11.5% has been reported (50). In another study (32-34), 23 oral and
maxillofacial surgeons were interviewed regarding removal of mini-plates. The authors
concluded that the plate removal percentage varies between 5% and 40%.
Biodegradable osteofixation systems have the possibility to degrade, thus preventing the
need for a second intervention (51;52). Another advantage of biodegradable devices is
their radiolucency, implying good compatibility with radiotherapy and imaging techniques
(42;53;54). Besides, osteoporosis can be prevented due to the gradual transfer of
functional forces to the healing bone during the disintegration process of biodegradable
devices (55;56).
Since the introduction of biodegradable devices in 1966 (57), the development of their
mechanical properties and degradation characteristics has been extensive (58). Numerous
in vitro, animal, and clinical studies have been published about positive (59-65) as well as
negative results (66-69). Despite the supposed advantages of biodegradable osteofixation
devices, these systems did not replace the titanium systems and are currently applied in
only limited numbers (43;70). The mechanical properties are less favourable and ultimate
resorption has not been proven (71). Another significant factor of the limited use is
the resistance by surgeons to modify their conventional, well experienced, treatment
techniques (72). The major drawback for general use of biodegradable devices is the lack
of clinical evidence.
CH
AP
TE
R 2
20 21
Objectives
The use of biodegradable osteofixation devices should be evidence-based in order to
secure uncomplicated bone healing (73). Numerous studies describe and claim the
advantages of biodegradable over titanium devices as a bone fixation method (60;74). In
the present study, the currently available literature regarding the clinical efficacy and safety
of biodegradable osteofixation devices compared with titanium osteofixation devices in
oral and maxillofacial surgery was systematically reviewed. The research question was
phrased as follows: “is there a difference in stability and morbidity regarding the fixation
of bone segments with biodegradable or titanium fixation devices in orthognathic and
trauma surgery?” The available literature regarding current relevant aspects of bone
surgery will also be discussed.
GENERAL ASPECTS OF BONE SURGERY
Various in vitro and in vivo studies must be performed before innovative interventions
can be used safely and effectively in the clinic (75). Studies that have been important
for understanding the behaviour and characteristics of biodegradable and titanium
osteofixation systems are reviewed in the subsequent sections.
Mechanism of bone healing
Fractured bone or locally damaged bone causes disruption of many blood vessels.
This disruption results in local haemorrhage followed by the formation of a blood clot.
Osteocytes at both sides of the fracture die due to deprivation of blood perfusion.
Restoration of the fracture area starts with the clearance of the blot clot, death cells
and bone matrix under the influence of revascularization. Periosteum, endosteum and
surrounding tissues respond by cell proliferation. The tissue that arises between both
fracture ends, and serves as a temporary bridging, is called callus. Its composition varies
with site and circumstances (76;77). Cartilage is formed in parts of the callus that are not
sufficiently saturated with blood. Subsequently, cartilage is transformed into bone by
enchondral bone formation. If sufficient blood saturation occurs, a direct network of bars
of plexiform bone is formed by endesmale bone formation. As a strong bony callus arises,
it can be subjected to normal tension- and compression forces (78).
Resorption and formation of bone is a dynamic and continuously changing process, which
has an equilibrium defined by internal factors (mainly hormones) and external factors
(mainly mechanical forces). Inadequate immobilization during the healing process causes
disruption of the revascularization process. This results in the formation of a fibrous callus
followed by an incomplete healing of the fracture. Too rigid fixation, on the other hand,
may also cause problems. Lack of normal functional stimuli in the final stages of bone
healing will inhibit the formation of new bone, while the resorption of bone still proceeds
(79;80). This could result in local osteoporosis (76;77;81).
Mechanical aspects
Various muscles of the maxillofacial skeleton exert a wide variety of forces in different direc-
tions. This implies that it is difficult to estimate the required mechanical properties of a fixation
system. Decisions regarding the required plates and screws are rarely evidence-based (82).
The primary mechanical strength and stiffness of biodegradable osteofixation devices are
less favourable compared to their conventional titanium counterparts. This is inherent to
the use of biodegradable polymers. However, the question is whether their mechanical
properties are sufficient for resisting the local deforming forces (83).
The main objective in orthognathic and trauma surgery is fast, anatomical and painless
functional reunion of bone segments (84). Revascularization plays an essential role
in this process (78;85). Titanium plates and screws are intrinsically small, strong, and
biocompatible (37). As a result, the main objectives regarding fixation management can be
met. The rigidity of titanium fixation systems might also be disadvantageous. The system
probably inhibits the transfer of functional forces to healing (or healed) bone, which may
result in osteoporosis as was mentioned in the previous section (55;56;81). By contrast,
the strength and stiffness of biodegradable fixation systems decrease with time because
of the disintegration of the polymer chains, in this way ensuring progressive loading
during the subsequent stages of bone healing. To compensate for the less favourable
primary mechanical strength and stiffness of biodegradable devices, manufacturers
increase their dimensions. This may interfere with tensionless wound closing, making
the wound area more prone to infection. Enlarged dimensions restrict easy application
in small areas which are difficult to access (e.g. paediatric surgery) (40). These factors
imply that the field of application of biodegradable devices, in particular regarding bone
fixation in the maxillofacial area, is restricted (43), whereas titanium systems may be
applied almost anywhere.
Despite the disadvantages of the enlarged dimensions of biodegradable systems as
mentioned above, several patient series have been published regarding the successful use
of biodegradable fixation systems applied in different (e.g. heavy load bearing) situations
(e.g. mandibular fractures and bilateral sagittal split osteotomies). The treatment of 1883
patients, in whom craniomaxillofacial deformities were fixed with the biodegradable
LactoSorb fixation system, was evaluated in a recent study (60). Regarding to the rapidly
growing cranial vault, the authors noted, that fewer potential complications occurred
using the biodegradable system compared with the titanium plates and screws. The
BioSorb FX biodegradable fixation system has been found to be an appealing alternative
for titanium fixation systems regarding orthognathic, trauma and cancer surgery,
corrective cranioplasty, and fixation of bone grafts in another recent study (86).
Considering the biomechanical aspects, selecting plates and screws is not always that
straightforward. The surgeon should consider the (1) local deforming forces and (2) which
system (biodegradable or titanium) could optimally resist the deforming forces (87), and
in what configuration (number of screws in both fracture ends).
CH
AP
TE
R 2
CH
AP
TE
R 2
22 23
Biocompatibility and resorption aspects
Biocompatibility refers to how a material elicits a host response in a specific situation. Tissue
responses to implanted material are numerous and complex. The term biocompatibility
also describes aspects of interactions between implanted material and the host (88;89).
The process of removal of a material by cellular activity and/or dissolution in a biological
environment, is called resorption (90). Degradation is the disintegration of material into
smaller parts. Biocompatibility, resorption and degradation are closely interrelated.
The biocompatibility of biodegradable internal fixation devices is strongly influenced by
the degradation and resorption behaviour of the polymers used (75;91). These systems
are made of different polymers (e.g. poly(L-lactide), poly(D-lactide), poly-glycolide,
polydioxanone, trimethylene carbonate). These materials degrade and resorb in two
phases (92). During the first phase, water molecules hydrolyze the long polymer chains
into shorter fragments. The molecular weight and the polymer strength decrease during
this process. The second phase consists of a physiologic response of the body in which
macrophages phagocyte and metabolize the short fragments which subsequently enter
the citric acid cycle (93-95). Water and carbon dioxide remain and are subsequently
excreted from the body, mainly through respiration. The mass of the biomaterial rapidly
disappears during phase two (57;96). In addition, enzymes are supposed to play a
considerable role in the degradation (97;98).
Degradation and resorption processes of biodegradable polymers frequently elicit adverse
tissue responses. This represents an inherent biologic tissue response (75) as occurs with
every implanted material (67). Regarding orthopedic surgery, the general incidence of
adverse tissue responses using fixation devices made of poly-glycolide varies from 2.0 to
46.7% (75). The incidence of adverse tissue responses is generally lower for plates and
screws made of poly-lactide (75). The time between implantation and appearance of
adverse tissue responses varies from 10-12 weeks (48;67;99) to 4-5 years (66;100;101) for
respectively poly-glycolide and poly-lactide.
The clinical characteristics of the adverse tissue responses vary from a local swelling without
signs of inflammation (66) to a suddenly emerging painful, erythematous, fluctuating
papule which reveals a sinus discharge of liquid remnants of disintegrated implant materials
(75). Radiographs obtained at the time of manifestation show osteolytic changes around
the implanted material in 50% of the patients (68;102). The histopathologic picture has
been characterized by an abundant polymeric debris, being surrounded by mononuclear
phagocytes and multinucleated foreign-body giant cells (67;68;103;104).
The possible risk factors for developing adverse tissue responses seem to be associated with
the extent of vascularization, which inherently depends on the site of implantation. Moreover,
the implant design appears to affect the response rate. Cylindrical pins and rods show a
lower incidence of adverse tissue responses than screws. Foreign-body response rates seem
to be independent of patients’ age and gender as well as the implanted polymer volume.
The long-term ultimate biocompatibility and resorption of biodegradable plates and screws
have frequently been investigated, yet remain to be established (75;105). Researchers
have reported varying in vivo results. A recent histologic study (106) reported complete
resorption of Resorb® X and LactoSorb screws after 12 and 14 months, respectively,
found by the use of a fluorescence microscope. However, bone re-modelling was not
completed after 26 months. The degradation process of biodegradable implants has also
been investigated through MRI (107). The authors concluded that no complete resorption
had occurred after 34 months.
Based on these findings, large-scale, long-term controlled clinical trials can be
recommended to verify the ultimate biocompatibility and resorption characteristics of
biodegradable implants and to establish evidence-based treatment methods.
Characteristics of “ideal” osteofixation devices
Considering the aspects mentioned in the previous sections, an ideal osteofixation
device should (82;92): (1) be fabricated and designed with appropriate initial strength to
meet the bio-mechanical demands, (2) not cause tissue responses necessitating device
removal, (3) be easy to use and handle, (4) be cost-effective, and (5) be compatible with
radiotherapy and imaging techniques. Regarding biodegradable osteofixation devices,
the following aspects should additionally be incorporated: (6) degrade in a predictable
fashion and allow for safe progressive loading during each stage of bone healing and (7)
disappear completely.
CONTROLLED CLINICAL STUDIES – A SYSTEMATIC REVIEW
METHODS
Literature search
To identify studies on the efficacy and safety of biodegradable osteofixation devices, a
highly sensitive search was carried out in the databases of MEDLINE (1966-2005) and
EMBASE (1989-2005). The search was supplemented with a systematic search in the
‘Cochrane Central Register of Controlled Trials’ (CENTRAL) (1800-2005). Free text words
and the applied thesaurus (MeSH) regarding the search strategy are summarized in Table
I. Several experts in the field of biodegradable osteofixation devices were contacted to
ensure eligible studies were not overlooked. Moreover, leading oral and maxillofacial
journals were screened for missing articles. To complete the search, reference lists in the
obtained literature were checked for additional relevant articles. No language and time
restrictions have been included in the search strategy.
The search strategy was focused on three aspects: (1) terms to search the ‘health’ condition
of interest (i.e. fracture and osteotomies of the maxillofacial skeleton); (2) terms to search for
the intervention(s) evaluated (i.e. biodegradable and titanium osteofixation device(s)); and
(3) terms to search for the types of study design to be included (i.e. clinical controlled trials)
(108). Free text words and MeSH terms were formulated precisely, resulting in a scrupulous
primary exclusion of ‘non clinical trials’ as well as studies which are rarely topic related.
CH
AP
TE
R 2
CH
AP
TE
R 2
24 25
Study selection
The relevance of studies was evaluated by a first selection based on title and abstract. Since
the research question focuses on the efficacy and safety of biodegradable osteofixation
devices in comparison with titanium devices, only controlled clinical trials (CCT) were
considered for inclusion in the systematic analysis.
The review was focused on studies concerning the treatment of fractures and the
performance of osteotomies of the maxillofacial skeleton (i.e. Le Fort I, Le Fort II, and Le
Fort III fractures and osteotomies, cranial fractures, malar fractures, mandibular fractures,
and sagittal split osteotomies of the mandible). Studies involving children were also
considered for inclusion. Disagreement about whether or not a study should be included
was resolved by a consensus discussion. Full-text documents were retrieved of all relevant
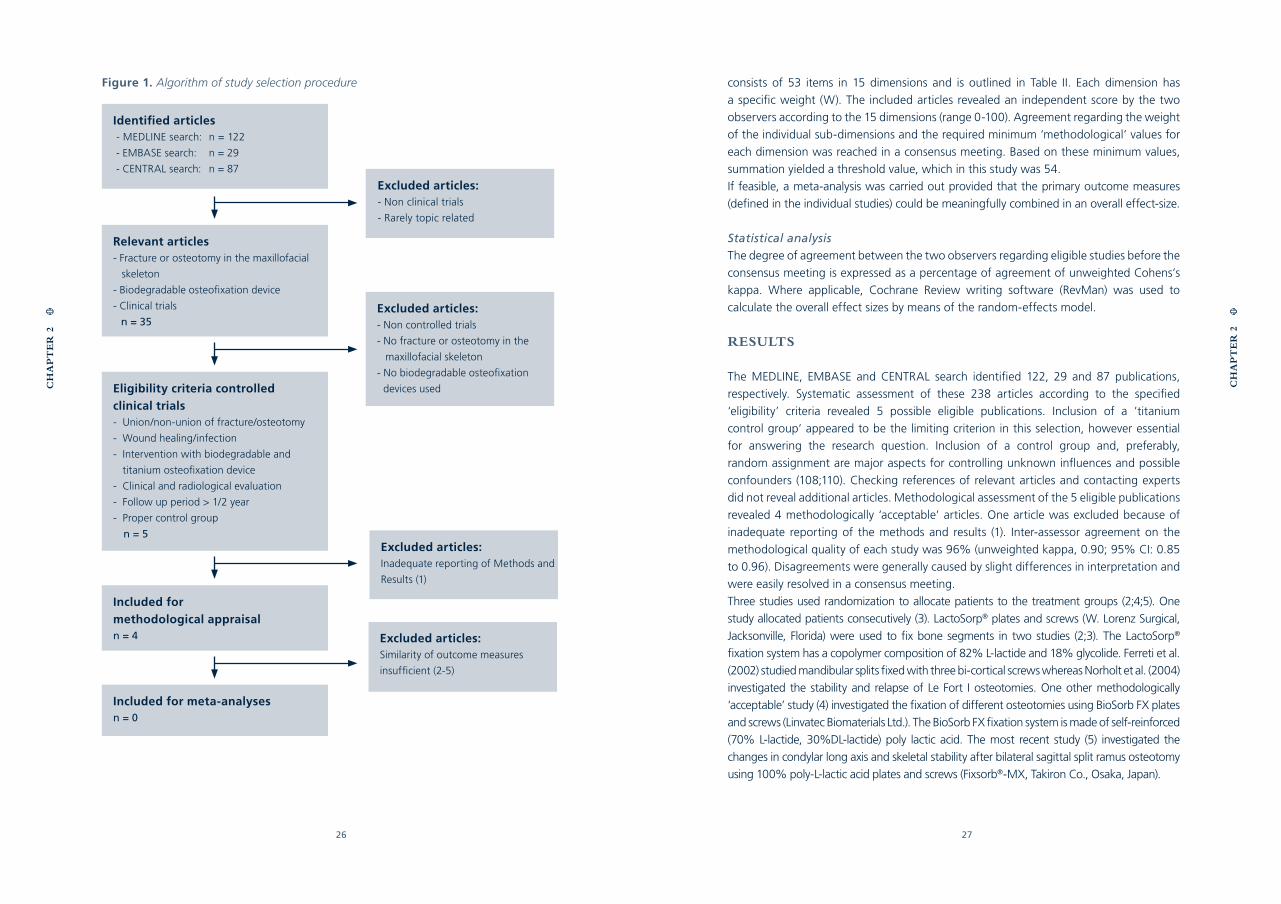
articles. The study selection procedure is outlined in figure 1.
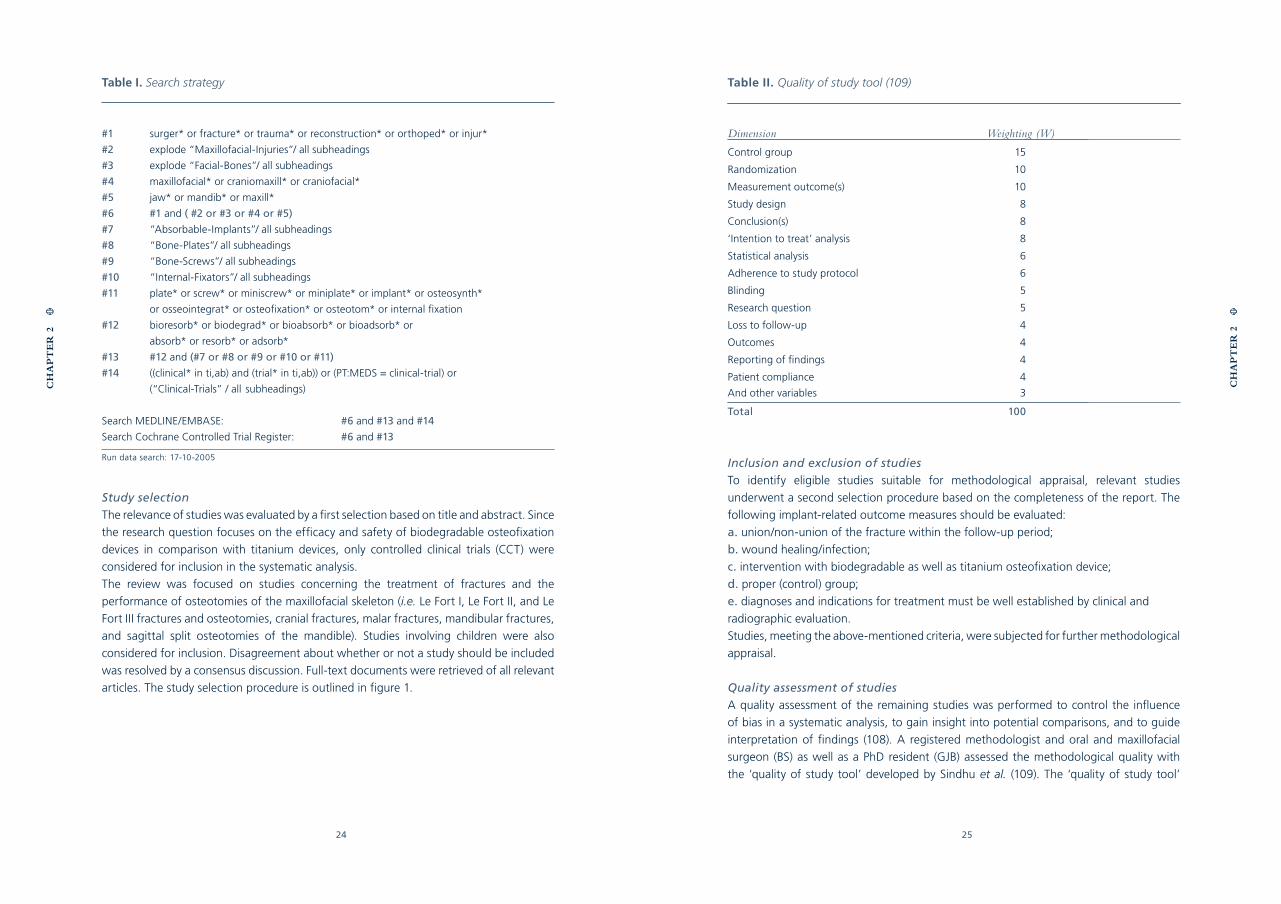
Table I. Search strategy
#1 surger* or fracture* or trauma* or reconstruction* or orthoped* or injur*
#2 explode “Maxillofacial-Injuries”/ all subheadings
#3 explode “Facial-Bones”/ all subheadings
#4 maxillofacial* or craniomaxill* or craniofacial*
#5 jaw* or mandib* or maxill*
#6 #1 and ( #2 or #3 or #4 or #5)
#7 “Absorbable-Implants”/ all subheadings
#8 “Bone-Plates”/ all subheadings
#9 “Bone-Screws”/ all subheadings
#10 “Internal-Fixators”/ all subheadings
#11 plate* or screw* or miniscrew* or miniplate* or implant* or osteosynth*
or osseointegrat* or osteofixation* or osteotom* or internal fixation
#12 bioresorb* or biodegrad* or bioabsorb* or bioadsorb* or
absorb* or resorb* or adsorb*
#13 #12 and (#7 or #8 or #9 or #10 or #11)
#14 ((clinical* in ti,ab) and (trial* in ti,ab)) or (PT:MEDS = clinical-trial) or
(“Clinical-Trials” / all subheadings)
Search MEDLINE/EMBASE: #6 and #13 and #14
Search Cochrane Controlled Trial Register: #6 and #13
Run data search: 17-10-2005 Inclusion and exclusion of studies
To identify eligible studies suitable for methodological appraisal, relevant studies
underwent a second selection procedure based on the completeness of the report. The
following implant-related outcome measures should be evaluated:
a. union/non-union of the fracture within the follow-up period;
b. wound healing/infection;
c. intervention with biodegradable as well as titanium osteofixation device;
d. proper (control) group;
e. diagnoses and indications for treatment must be well established by clinical and
radiographic evaluation.
Studies, meeting the above-mentioned criteria, were subjected for further methodological
appraisal.
Quality assessment of studies
A quality assessment of the remaining studies was performed to control the influence
of bias in a systematic analysis, to gain insight into potential comparisons, and to guide
interpretation of findings (108). A registered methodologist and oral and maxillofacial
surgeon (BS) as well as a PhD resident (GJB) assessed the methodological quality with
the ‘quality of study tool’ developed by Sindhu et al. (109). The ‘quality of study tool’
CH
AP
TE
R 2
CH
AP
TE
R 2
Table II. Quality of study tool (109)
Dimension Weighting (W)
Control group
Randomization
Measurement outcome(s)
Study design
Conclusion(s)
‘Intention to treat’ analysis
Statistical analysis
Adherence to study protocol
Blinding
Research question
Loss to follow-up
Outcomes
Reporting of findings
Patient compliance
And other variables
Total
15
10
10
8
8
8
6
6
5
5
4
4
4
4
3
100
26 27
consists of 53 items in 15 dimensions and is outlined in Table II. Each dimension has
a specific weight (W). The included articles revealed an independent score by the two
observers according to the 15 dimensions (range 0-100). Agreement regarding the weight
of the individual sub-dimensions and the required minimum ‘methodological’ values for
each dimension was reached in a consensus meeting. Based on these minimum values,
summation yielded a threshold value, which in this study was 54.
If feasible, a meta-analysis was carried out provided that the primary outcome measures
(defined in the individual studies) could be meaningfully combined in an overall effect-size.
Statistical analysis
The degree of agreement between the two observers regarding eligible studies before the
consensus meeting is expressed as a percentage of agreement of unweighted Cohens’s
kappa. Where applicable, Cochrane Review writing software (RevMan) was used to
calculate the overall effect sizes by means of the random-effects model.
RESULTS
The MEDLINE, EMBASE and CENTRAL search identified 122, 29 and 87 publications,
respectively. Systematic assessment of these 238 articles according to the specified
‘eligibility’ criteria revealed 5 possible eligible publications. Inclusion of a ’titanium
control group‘ appeared to be the limiting criterion in this selection, however essential
for answering the research question. Inclusion of a control group and, preferably,
random assignment are major aspects for controlling unknown influences and possible
confounders (108;110). Checking references of relevant articles and contacting experts
did not reveal additional articles. Methodological assessment of the 5 eligible publications
revealed 4 methodologically ‘acceptable’ articles. One article was excluded because of
inadequate reporting of the methods and results (1). Inter-assessor agreement on the
methodological quality of each study was 96% (unweighted kappa, 0.90; 95% CI: 0.85
to 0.96). Disagreements were generally caused by slight differences in interpretation and
were easily resolved in a consensus meeting.
Three studies used randomization to allocate patients to the treatment groups (2;4;5). One
study allocated patients consecutively (3). LactoSorp® plates and screws (W. Lorenz Surgical,
Jacksonville, Florida) were used to fix bone segments in two studies (2;3). The LactoSorp®
fixation system has a copolymer composition of 82% L-lactide and 18% glycolide. Ferreti et al.
(2002) studied mandibular splits fixed with three bi-cortical screws whereas Norholt et al. (2004)
investigated the stability and relapse of Le Fort I osteotomies. One other methodologically
‘acceptable’ study (4) investigated the fixation of different osteotomies using BioSorb FX plates
and screws (Linvatec Biomaterials Ltd.). The BioSorb FX fixation system is made of self-reinforced
(70% L-lactide, 30%DL-lactide) poly lactic acid. The most recent study (5) investigated the
changes in condylar long axis and skeletal stability after bilateral sagittal split ramus osteotomy
using 100% poly-L-lactic acid plates and screws (Fixsorb®-MX, Takiron Co., Osaka, Japan).
Identified articles - MEDLINE search: n = 122
- EMBASE search: n = 29
- CENTRAL search: n = 87
Relevant articles- Fracture or osteotomy in the maxillofacial
skeleton
- Biodegradable osteofixation device
- Clinical trials
n = 35
Eligibility criteria controlled clinical trials- Union/non-union of fracture/osteotomy
- Wound healing/infection
- Intervention with biodegradable and
titanium osteofixation device
- Clinical and radiological evaluation
- Follow up period > 1/2 year
- Proper control group
n = 5
Included for methodological appraisaln = 4
Excluded articles:- Non clinical trials
- Rarely topic related
Excluded articles:- Non controlled trials
- No fracture or osteotomy in the
maxillofacial skeleton
- No biodegradable osteofixation
devices used
Excluded articles:Inadequate reporting of Methods and
Results (1)
Excluded articles:Similarity of outcome measures
insufficient (2-5)
Included for meta-analysesn = 0
Figure 1. Algorithm of study selection procedure
CH
AP
TE
R 2
CH
AP
TE
R 2
28 29
Because of the different effect-sizes used in the methodologically ‘acceptable’ studies, it was
impossible to perform a meta-analysis. Therefore, the major effects regarding the stability
and morbidity of fracture fixation are qualitatively described in the subsequent sections.
Stability
Stability of fixed bone segments is an important outcome measure since the aim of
fixation systems is to establish a functional, anatomical and pain-free reunion of bone
segments. In the four included articles, the stability of the osteotomized segments was
assessed with different methods.
Cephalometric analysis was used in three of the four included studies to accurately assess
the skeletal stability (2;3;5). Regarding bilateral sagittal osteotomies (5), the outcome
measures SNA, SNB and ANB did not significantly differ for the titanium and PLLA
group. The interincisor angle, occlusal plane angle, mandibular length, overbite, overjet,
and convexity were also similar in both groups. The location of the pogonion neither
showed a significant difference. In the second study (2), Le Fort I osteotomies fixed with
biodegradable plates and screws revealed a significant difference in vertical dimension of
the upper jaw (mean difference 0.6 mm) after 6 weeks post-operatively. The osteotomies
fixed with titanium plates and screws did not present a significant difference. The authors
(2) concluded that the statistical significant difference of the vertical dimension in the
biodegradable group (LactoSorp®) was not clinically relevant. Ferretti et al. (3) evaluated
the relapse (skeletal stability) of bilateral sagittal osteotomies. The mean transposition of
the mandible fixed with three bi-cortical screws was 4.7 (sd = 1.3) and 5.5 (sd = 1.7)
millimetres for respectively the titanium and biodegradable group. The mean relapse was
0.25 (sd = 1.25) and 0.83 (sd = 1.25) millimetres, respectively (not statistically significant).
The clinical mobility of the bone segments was evaluated in two included studies
(2;4). The first study (2) reported a slight mobility during the first 6 weeks (6 in the
biodegradable group and 3 in the titanium group) whereas one case presented mobility in
the biodegradable group 1 year post-operatively. The second study (4) reported that the
clinical stability improved gradually over time. No difference in this respect was revealed
between titanium and biodegradable fixation. In all patients, the mobility was very mild
and present in the maxilla. The mobile maxillae became stable and firm in the sixth week,
and no further mobility could be detected during the follow-up period.
Morbidity
The morbidity of osteofixation devices is evaluated in all of the included studies (2-5).
Ueki et al. (5) evaluated different aspects regarding morbidity: pain on chewing (using a
visual analogue scale), maximum mouth opening range (measuring the distance between the
edges of the upper and lower incisors) and temporomandibular disorder (TMD) symptoms
mainly based on sound (click and crepitus) on movement. Pain on post-operative chewing
revealed lower VAS scores compared to pre-operative chewing in both groups. The VAS
scores between both groups were nearly similar. Maximum mouth opening range did not
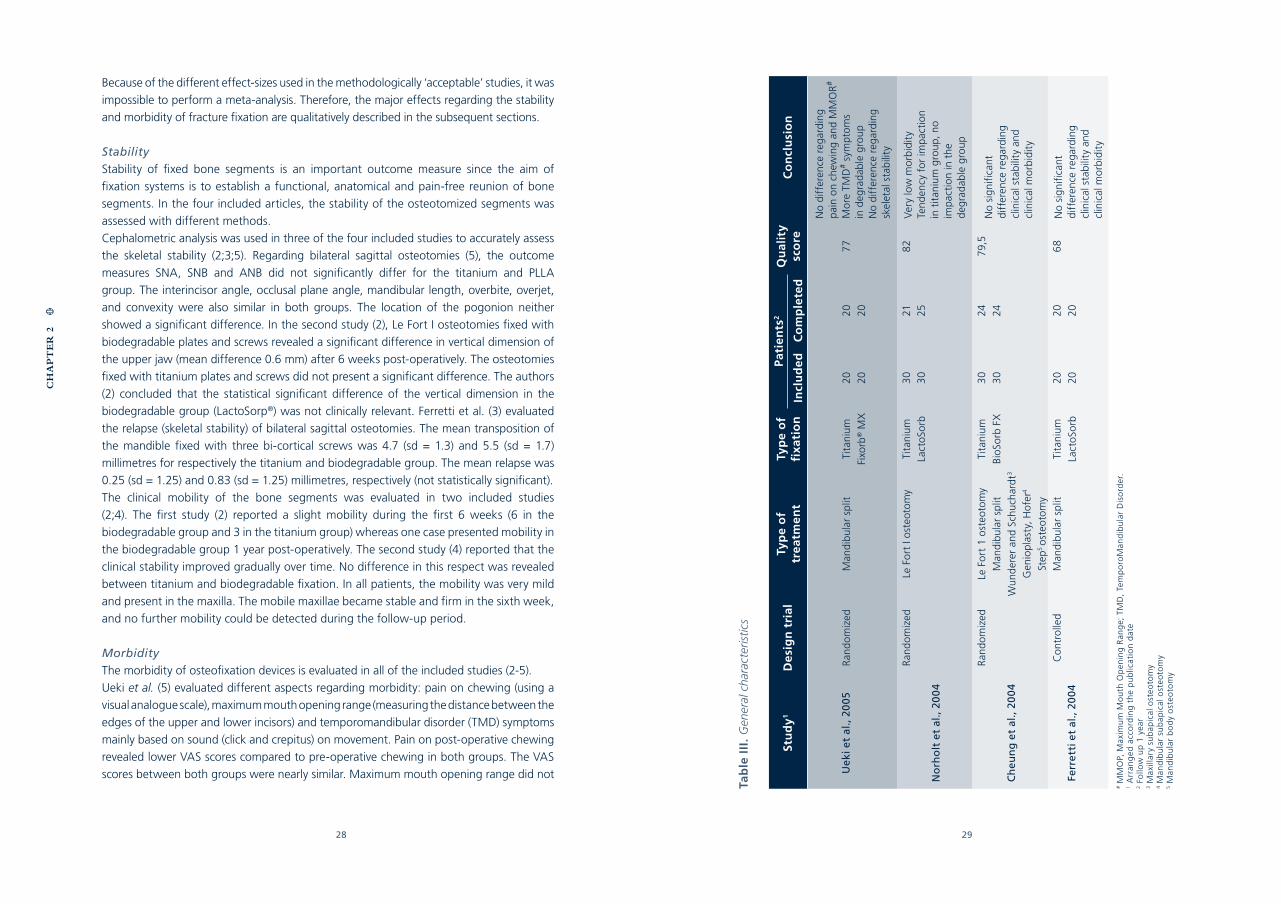
Tab
le I
II.
Gen
eral
cha
ract
eris
tics
Stu
dy1
De
sig
n t
rial
Typ
e o
ftr
eatm
ent
Typ
e o
ffi
xati
on
Pati
ents
2Q
ual
ity
sco
reC
on
clu
sio
nIn
clu
de
dC
om
ple
ted
No
diff
eren
ce r
egar
ding
p
ain
on
chew
ing
and
MM
OR
#
Mo
re T
MD
# sym
pto
ms
in d
egra
dab
le g
roup
No
diff
eren
ce r
egar
ding
sk
elet
al s
tab
ility
Uek
i et
al.,
2005
Ran
do
miz
edM
andi
bula
r sp
litTi
tani
um20
2077
Fixo
rb® M
X20
20
Ran
do
miz
edLe
Fo
rt I
ost
eoto
my
Tita
nium
30
218
2V
ery
low
mo
rbid
ity
Tend
ency
fo
r im
pac
tio
nin
tit
aniu
m g
roup
, no
imp
acti
on
in t
he
deg
rada
ble
gro
up
Lact
oSo
rb3
025
No
rho
lt e
t al
., 20
04
Ran
do
miz
edLe
Fo
rt 1
ost
eoto
my
Tita
nium
30
2479
,5N
o si
gnifi
cant
diff
eren
ce r
egar
ding
clin
ical
sta
bili
ty a
ndcl
inic
al m
orb
idit
y
Man
dibu
lar
split
Bio
Sorb
FX
30
24C
heu
ng
et
al.,
200
4W
und
erer
and
Sch
ucha
rdt3
Gen
iop
last
y, H
ofer
4
Step
5 o
steo
tom
y
Ferr
etti
et
al.,
200
4C
ont
rolle
dM
andi
bula
r sp
litTi
tani
um20
206
8N
o si
gnifi
cant
diff
eren
ce r
egar
ding
clin
ical
sta
bili
ty a
ndcl
inic
al m
orb
idit
y
Lact
oSo
rb20
20
# M
MO
P, M
axim
um
Mo
uth
Op
enin
g R
ang
e; T
MD
, Te
mp
oro
Man
dib
ula
r D
iso
rder
.1 A
rran
ged
acc
ord
ing
th
e p
ub
licat
ion
dat
e2 F
ollo
w u
p 1
yea
r3 M
axill
ary
sub
apic
al o
steo
tom
y4 M
and
ibu
lar
sub
apic
al o
steo
tom
y5 M
and
ibu
lar
bo
dy
ost
eoto
my
CH
AP
TE
R 2
30 31
reveal a significant difference. The number of symptomatic joints in the titanium group was
significantly less compared to the PLLA group. General clinical aspects (infection, wound
dehiscence, plate exposure and palpability of plates and screws) are objectively assessed in
two included studies (2;4). The inflammatory responses gradually decreased with time. The
first study (2) reported wound dehiscence in 1 patient in the biodegradable group whereas
the second study (4) revealed wound dehiscence in 3 patients in the titanium group (10%)
and in 2 patients in the biodegradable group (6.7%). No complications occurred as result
of the dehiscence. The palpability of biodegradable plates and screws decreased with
time in both studies, while the palpability of titanium plates and screws increased. In the
study of Cheung et al. (4), plate exposure affected 1.02% and 1.21% of the patients in the
titanium group and biodegradable group respectively whereas Norholt et al. (2) discussed
one patient in the biodegradable group with plate exposure (4.2%). One included study
(4) reported the removal of 3 titanium (1.53%) and 6 (3.36%) biodegradable plates (as
a percentage of all plates and screws used). Ferreti et al. (3) reported briefly the clinical
appearance of the surgical ‘sites’. They appeared to be abnormal with respect to the
evaluation criteria (swelling, discharge, pain, or discoloration of the mucosa and skin)
during the post-operative 12 months. The general characteristics, results and conclusions
of the included studies are summarized in Table III.
GENERAL DISCUSSION
Mechanical aspects
Regarding the mechanical aspects, the selection of an adequate fixation system remains
difficult due to varying local situations (fracture line(s), anatomy, patients and muscle
activity). To guide decisions regarding the required fixation system in different clinical
situations, a comparison of the initial mechanical strength and stiffness of biodegradable
and titanium systems could be valuable. Moreover, the surgeon is predominantly
interested in the device (functional unit) characteristics of a fixation system rather than
in the material characteristics. The variability of biodegradable osteofixation systems (i.e.
co-polymer composition and geometry) makes a well-funded selection difficult (82).
Besides the initial mechanical characteristics of osteofixation systems, the torsion strength
and stiffness of the screws are important. The screws fix the osteofixation plate against
the bone segments and prevent sliding of the bone segments and the fixation system
relative to each other. This ensures adequate stabilization of the bone segments. Screws
also generate inter-fragmentary compression to stabilize mandibular splits, which will
enhance fracture healing. The torsion strength and stiffness of the biodegradable screws
are less favourable (111) compared to titanium screws, which have been reported as a
disadvantage by several authors (111;112). Moreover, biodegradable polymeric screws
relax when a force is continuously applied (111). These aspects may result in decreased
fracture stability and possible compromised fracture healing.
Biocompatibility and resorption aspects
Long-term ultimate biocompatibility, as is the goal of any implanted material, is difficult to
establish. Despite considerable clinical experience of fracture fixation using biodegradable
materials, long term clinical studies are scarce. Moreover, studies reporting the long-term
complications (66;67;101) probably represent one end of a continuous spectrum of biological
responses. The majority of the cases pass sub-clinically and remain unnoticed despite the
elicitation of a (small) biological host response as is the case with every implanted material (67).
The degradation and resorption characteristics as well as the possibility to develop
adverse tissue responses, depend largely on the nature of the implanted materials. Poly-
lactide is a major component of the biodegradable fixation devices and the time to elicit
a considerable host response is 4 to 5 years (66;100;101;113). Therefore, studies reporting
the biocompatibility and degradation characteristics regarding this material should
last for at least 5 years (114). However, few laboratory animals live long enough and,
consequently, long-term biocompatibility experiments are difficult to design.
The development of adverse tissue responses seems to originate from several different
physiologic and chemical processes. Crystalline remnants and a decrease of pH (115) during
degradation are probably responsible for the adverse effects of biodegradable polymers,
although the local tissue tolerance and the local clearing capacity seem to be important
aspects as well (67;100;116;117). The rate of crystalline remnants and decrease of pH
are partly determined by the molecular structure of the biomaterial (118). Amorphous
polymers degrade faster than crystalline polymers, resulting in a rapid decrease of the
pH. Crystalline polymers may remain in situ for decades (92). A high blood flow rate is
an essential prerequisite for successful implantation of biodegradable fixation materials,
since adequate blood flow secures sufficient removal of degradation products preventing
a decrease in pH (114). PDLLA implants enriched with calcium phosphates have been
investigated in rats to prevent a local decrease in pH (119). The control group received
pure PDLLA implants. The PDLLA implants enriched with calcium phosphates showed
an increased tissue response after 72 weeks. The authors concluded that the ‘enriched’
implants are not suitable for clinical use.
Clinical aspects
The major objective of this systematic review was to evaluate the clinical efficacy and safety
of biodegradable osteofixation devices in comparison with titanium osteofixation devices
used in oral and maxillofacial surgery. Unfortunately, we cannot draw any firm conclusions
regarding the fixation of traumatically fractured bone segments, owing to the lack of
controlled clinical trials. Studies using two randomized treatment groups are difficult to
design and not (yet) available. Regarding the fixation of bone segments in orthognathic
surgery, only a few controlled clinical studies (2-4) are available. There does not appear
to be a significant difference in outcome between titanium and biodegradable fixation
systems. Definite conclusions regarding the long-term performance of biodegradable
fixation devices used in maxillofacial surgery cannot be drawn.
CH
AP
TE
R 2
CH
AP
TE
R 2
32 33
The methodologically ‘acceptable’ studies contain much heterogeneity. The studies
individually defined the outcome measures for stability and morbidity. Moreover, the
treatment modalities performed in these studies were different (Le Fort I, sagittal split
osteotomies and various osteotomies). The biodegradable fixation system (LactoSorb)
used, was similar in only 2 studies (2;3). Because of the heterogeneity, pooling of outcome
measures was not meaningful.
A primary way to establish whether a fixation system has functioned successfully is to
assess the extent of clinical mobility. However, objective mobility measurements in the
maxillofacial skeleton are difficult to perform. One study reports the stability according
to a nominal scale: none-, slight- and gross mobility (2) while another study reports the
mobility according to a binary scale: immobility versus mobility (4). One methodologically
‘acceptable’ study did not even report the extent of mobility (3). In our opinion, it is
essential to report the extent of mobility when investigating the clinical efficacy and
safety of biodegradable osteofixation systems. Therefore, we advise the use of a binary
scale. The aim of an osteofixation device is to achieve functional, pain-free re-union within
a reasonable period of time (6 weeks) (120). Compromised healing or slight mobility
after 6 weeks should be defined as non -union. The most recent study (5) applied post-
operative inter-maxillary fixation (IMF) for 2 weeks to prevent adverse alterations of the
post-operative occlusion. The authors did not know whether the PLLA plates were strong
enough to stabilize the bone segments. Today, IMF is not the state of art and thus, in our
opinion, improper to apply when comparing the skeletal stability of bilateral sagittal split
osteotomies fixed with titanium or PLLA plates.
One of the major drawbacks of the reviewed literature is the lack of sufficient follow-up.
Three of the included studies (2;3;5) followed their patients only 1 year post-operatively.
Another included recent study (4) followed a few of their patients for 2 years (6 out of the
titanium group and 7 out of the biodegradable group) and 24 patients in both groups were
evaluated for 1 year. In our opinion, the follow up periods are too short to draw definite
conclusions as to whether these biodegradable implants could serve as a safe and reliable
fixation method on the long term. Many authors (60;70;86) have reported patient series
with longer follow up periods. As mentioned earlier, since these patient series lack a control
group, an adequate comparison with titanium fixation devices has not been made in these
studies. Future clinical trials should, from a biocompatibility and resorption point of view,
evaluate patients for at least 5 years as mentioned in the previous section (4.2).
The onset of infections seems to differ for fixation of fractures with titanium or
biodegradable devices. One included study (4) reported that the infections in the
biodegradable group were diagnosed after 6 weeks, 3 months, and 6 months, while
those in the titanium group were diagnosed after 2 weeks, 6 weeks, and 3 months.
Another included study (2) reported that 1 infection in the titanium group was diagnosed
after 1 week, whereas 2 infections in the biodegradable group were diagnosed after 6
months. These clinical findings suggest that the onset of infections tend to occur later in
the biodegradable groups. The authors could not explain this tendency, although one (2)
suggested that it could be caused by the ongoing degradation of the plates and screws.
The known causes of infection are loosened screws and wound dehiscence (4). In one of
the included trials, the authors (4) report the infection percentages in terms of individual
plates (1.53% in the titanium group and 1.82% in the biodegradable group) and in terms
of individual patients (10% in each group). In the discussion, the authors advocate that
it is more reasonable to use the plate and screw as the unit for calculation, because an
infection will occur if any single component fails. However, in our opinion it is more
reasonable to use the individual patient infection-percentages to calculate the percentage
of infection. After all, infection percentages in terms of individual patients will gain more
insight in the extent of actual re-operating procedures. Moreover, cost-effectiveness
analyses are more meaningful using infection percentages in terms of individual patients.
However, cost-effectiveness analysis regarding the use of biodegradable fracture fixation
devices were not reported in any of the included trials (2-5).
SUMMARIZING AND CONCLUDING REMARKS
The implications for the clinical applicability of biodegradable osteofixation systems
on the long-term remain inconclusive. There is evidence available from randomized
controlled trials to support the conclusion that there is no significant difference between
biodegradable and titanium osteofixation devices with regard to short-term clinical
outcome, complication rate and infections in the area of orthognathic surgery. Re-
operation rates do not significantly differ in the biodegradable and titanium group. A
sufficient follow up (of at least 5 years) is necessary in order to draw decisive conclusions
regarding the use of biodegradable implants in oral and maxillofacial surgery. Until
then, we can conclude that decisions with respect to plate and screw size, number of
plates and screws, and biodegradable or titanium must be made on individually relevant
aspects. Relevant factors include the nature of the injury, technical considerations, and
the experience of the surgeon.
Since this systematic review has some implications for future research, there is an urgent
need for sufficiently powered, high quality and appropriately reported randomized
controlled trials with respect to biodegradable osteofixation devices versus non-
degradable osteofixation devices for well-defined maxillofacial fractures and osteotomies.
Future studies should include a cost-effectiveness analysis in which hospital admission
costs, surgical costs (material), and the costs associated with sick leave of the patients
should be analyzed.
Acknowledgments
The authors thank Ms. S van der Werf from the Groningen University medical library for
her assistance in the elaboration of the search strategy. The authors also thank Ms. S.
Shaw for correcting the American English language.
CH
AP
TE
R 2
CH
AP
TE
R 2
CHAPTER 3.1
TORSION STRENGTH OF
BIODEGRADABLE AND
TITANIUM SCREW SYSTEMS:
A COMPARISON
G.J. BUIJS
E.B. VAN DER HOUWEN
B. STEGENGA
R.R.M. BOS
G.J. VERKERKE
Published in: J Oral Maxillofac Surg. 2007 Nov;65(11):2142-7.
36
CH
AP
TE
R 3
.1
CH
AP
TE
R 3
.1
37
Abstract:
Objectives- To determine: (1) the differences in maximum torque between 7 biodegradable
and 2 titanium screw systems, and (2) the differences of maximum torque between ‘hand
tight’ and break of the biodegradable and the titanium osteofixation screw systems.
Materials & Methods- Four oral and maxillofacial surgeons inserted 8 specimens of all 9
screw systems in polymethylmethacrylate (PMMA) plates. The surgeons were instructed to
insert the screws as they would do in the clinic (‘hand tight’). The data were recorded by a
torque measurement meter. A PhD resident inserted 8 specimens of the same set of 9 screw
systems until fracture occurred. The maximum applied torque was recorded likewise.
Results- (1) the mean maximum torque of the 2 titanium screw systems was significantly
higher than that of the 7 biodegradable screw systems, and (2) the mean maximum
torque for ‘hand tight’ was significantly lower than for break regarding 2 biodegradable,
and both titanium screw systems.
Conclusion & discussion- Based on the results, we conclude that the 1.5- and 2.0
mm titanium screw systems still present the highest torque strength compared to the
biodegradable screw systems. When there is an intention to use biodegradable screws,
we recommend the use of 2.0 mm BioSorb FX, 2.0 mm LactoSorb or the larger 2.5 mm
Inion CPS screws.
Keywords: screw; osteofixation; biodegradable; titanium; torsion strength; properties.
INTRODUCTION
Background
Fast, anatomical and pain-free re-union of bone fragments are the essential goals in
orthognathic and trauma surgery (84). Adequate reposition, stabilization and fixation of
fractured or osteotomized bone segments are essential preconditions (7;121). Plates and
screws are generally used for the internal stabilization and fixation of the bone segments
(35;36). Screws are used to fix osteofixation plates or to position bone segments (e.g. sag-
ittal split osteotomies) (3). During insertion, the screws occasionally break (4). Fracture of
a screw occurs when the applied torque is higher than the maximum allowable torque of
the screw. Removal of broken screws and re-application of screws is expensive and time-
consuming. Besides, additional operations may result in complications and subsequent
compromised bone healing.
It is generally acknowledged that biodegradable screws have different torsion character-
istics than titanium screws. Some clinical studies reported a higher number of broken bio-
degradable screws compared to titanium screws (2;4). Several authors have reported this
experience as a considerable disadvantage (40;111;112). The maximum torque strength
differs for the various screws mainly because of the use of different materials for manu-
facturing (biodegradable) screws, and different geometry of those screws.
The manufacturers do not specify the torque for inserting the screws. The torque to be
applied for adequate tightening the screws can be defined as ‘hand tight’. The maximally
applied torque is, to some extent, controlled by the construction of the screwdriver han-
dles (diameter, hand posture, geometry, and texture). But with most handles, the maxi-
mum torque that can be applied exceeds the torque strength of the screws, so fracture of
the screws might occur. An estimate of a safe torque for screws of different diameter and
length is difficult, especially for biodegradable screws (82). Moreover, many surgeons are
not that experienced in using polymeric screws. To guide decisions regarding the selec-
tion and application of different osteofixation screws, clarification of the differences in
torque strength of biodegradable as well as titanium osteofixation screw systems could
be valuable (122).
Objectives
The objectives of this study were to determine: (1) the differences in maximum torque
between 7 biodegradable and 2 titanium screw systems, and (2) the differences in maxi-
mum torque between ‘hand tight’ and break of the biodegradable as well as the titanium
screw systems.
MATERIALS AND METHODS
Seven (5 x 2.0-mm, 1 x 2.1-mm, and 1 x 2.5-mm) commercially available biodegradable
as well as two (1.5- and 2.0-mm) commercially available titanium screw systems were
38
CH
AP
TE
R 3
.1
CH
AP
TE
R 3
.1
39
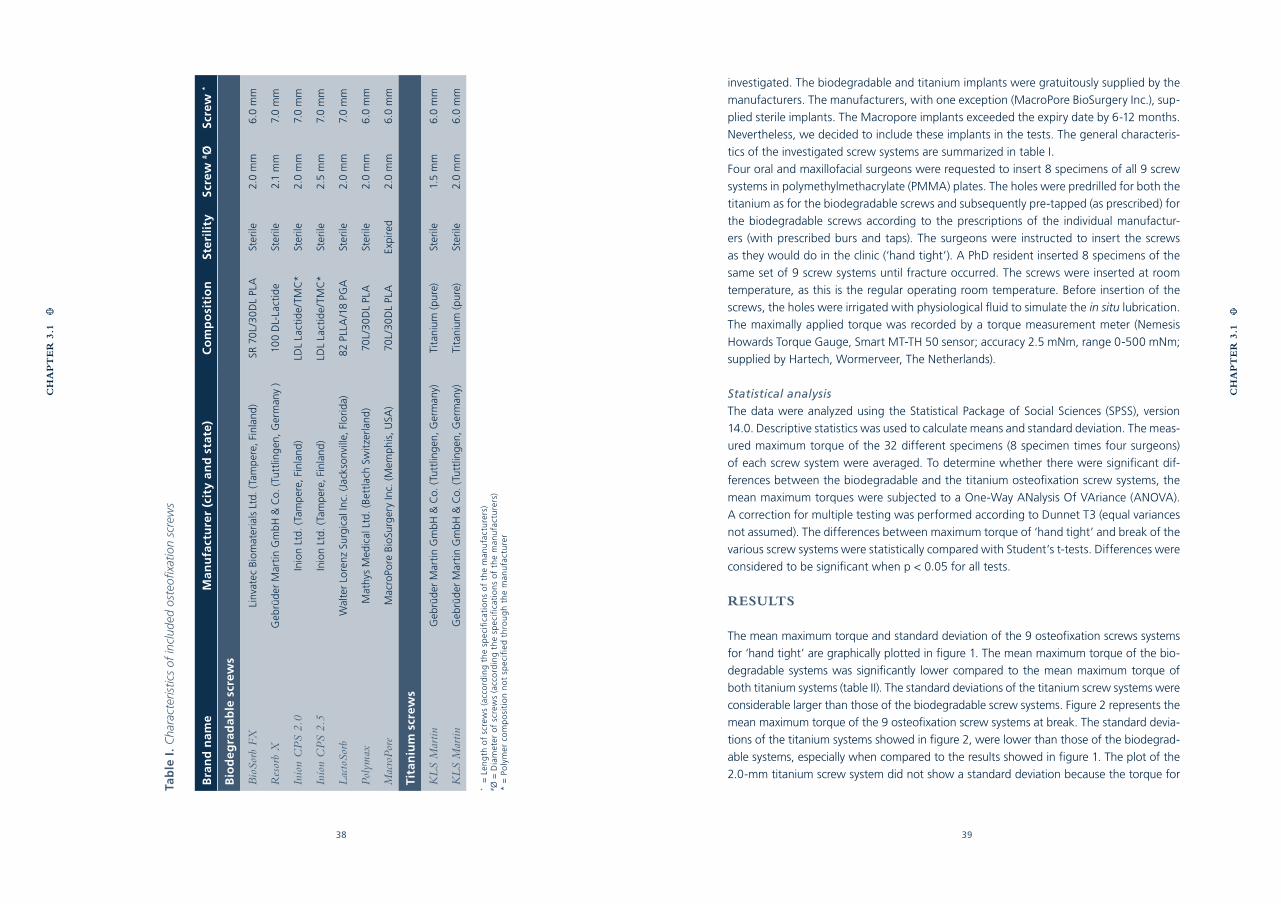
investigated. The biodegradable and titanium implants were gratuitously supplied by the
manufacturers. The manufacturers, with one exception (MacroPore BioSurgery Inc.), sup-
plied sterile implants. The Macropore implants exceeded the expiry date by 6-12 months.
Nevertheless, we decided to include these implants in the tests. The general characteris-
tics of the investigated screw systems are summarized in table I.
Four oral and maxillofacial surgeons were requested to insert 8 specimens of all 9 screw
systems in polymethylmethacrylate (PMMA) plates. The holes were predrilled for both the
titanium as for the biodegradable screws and subsequently pre-tapped (as prescribed) for
the biodegradable screws according to the prescriptions of the individual manufactur-
ers (with prescribed burs and taps). The surgeons were instructed to insert the screws
as they would do in the clinic (‘hand tight’). A PhD resident inserted 8 specimens of the
same set of 9 screw systems until fracture occurred. The screws were inserted at room
temperature, as this is the regular operating room temperature. Before insertion of the
screws, the holes were irrigated with physiological fluid to simulate the in situ lubrication.
The maximally applied torque was recorded by a torque measurement meter (Nemesis
Howards Torque Gauge, Smart MT-TH 50 sensor; accuracy 2.5 mNm, range 0-500 mNm;
supplied by Hartech, Wormerveer, The Netherlands).
Statistical analysis
The data were analyzed using the Statistical Package of Social Sciences (SPSS), version
14.0. Descriptive statistics was used to calculate means and standard deviation. The meas-
ured maximum torque of the 32 different specimens (8 specimen times four surgeons)
of each screw system were averaged. To determine whether there were significant dif-
ferences between the biodegradable and the titanium osteofixation screw systems, the
mean maximum torques were subjected to a One-Way ANalysis Of VAriance (ANOVA).
A correction for multiple testing was performed according to Dunnet T3 (equal variances
not assumed). The differences between maximum torque of ‘hand tight’ and break of the
various screw systems were statistically compared with Student’s t-tests. Differences were
considered to be significant when p < 0.05 for all tests.
RESULTS
The mean maximum torque and standard deviation of the 9 osteofixation screws systems
for ‘hand tight’ are graphically plotted in figure 1. The mean maximum torque of the bio-
degradable systems was significantly lower compared to the mean maximum torque of
both titanium systems (table II). The standard deviations of the titanium screw systems were
considerable larger than those of the biodegradable screw systems. Figure 2 represents the
mean maximum torque of the 9 osteofixation screw systems at break. The standard devia-
tions of the titanium systems showed in figure 2, were lower than those of the biodegrad-
able systems, especially when compared to the results showed in figure 1. The plot of the
2.0-mm titanium screw system did not show a standard deviation because the torque for
Tab
le I
. C
hara
cter
istic
s of
incl
uded
ost
eofix
atio
n sc
rew
s
Bra
nd
nam
eM
anu
fact
ure
r (c
ity
and
sta
te)
Co
mp
osi
tio
nSt
eril
ity
Scre
w #
ØSc
rew
*
Bio
de
gra
dab
le s
crew
s
Bio
Sorb
FX
Linv
atec
Bio
mat
eria
ls L
td. (
Tam
per
e, F
inla
nd)
SR 7
0L/
30
DL
PLA
Ster
ile2.
0 m
m6
.0 m
m
Res
orb
XG
ebrü
der
Mar
tin
Gm
bH
& C
o. (
Tutt
ling
en, G
erm
any
)10
0 D
L-La
ctid
eSt
erile
2.1
mm
7.0
mm
Inio
n C
PS
2.0
Inio
n Lt
d. (
Tam
per
e, F
inla
nd)
LDL
Lact
ide/
TMC
*St
erile
2.0
mm
7.0
mm
Inio
n C
PS
2.5
Inio
n Lt
d. (
Tam
per
e, F
inla
nd)
LDL
Lact
ide/
TMC
*St
erile
2.5
mm
7.0
mm
Lac
toSo
rbW
alte
r Lo
renz
Sur
gica
l Inc
. (Ja
ckso
nvill
e, F
lori
da)
82
PLLA
/18
PGA
Ster
ile2.
0 m
m7.
0 m
m
Pol
ymax
Mat
hys
Med
ical
Ltd
. (B
ettl
ach
Swit
zerl
and
)70
L/3
0D
L PL
ASt
erile
2.0
mm
6.0
mm
Mac
roP
ore
Mac
roPo
re B
ioSu
rger
y In
c. (M
emp
his,
USA
)70
L/3
0D
L PL
AEx
pire
d2.
0 m
m6
.0 m
m
Tit
aniu
m s
crew
s
KL
S M
artin
Geb
rüd
er M
arti
n G
mb
H &
Co.
(Tu
ttlin
gen
, Ger
man
y)Ti
tani
um (
pure
)St
erile
1.5
mm
6.0
mm
KL
S M
artin
Geb
rüd
er M
arti
n G
mb
H &
Co.
(Tu
ttlin
gen
, Ger
man
y)Ti
tani
um (
pure
)St
erile
2.0
mm
6.0
mm
*
= L
eng
th o
f sc
rew
s (a
cco
rdin
g t
he
spec
ifica
tio
ns
of
the
man
ufa
ctu
rers
)#Ø
= D
iam
eter
of
scre
ws
(acc
ord
ing
th
e sp
ecifi
cati
on
s o
f th
e m
anu
fact
ure
rs)
* =
Po
lym
er c
om
po
siti
on
no
t sp
ecifi
ed t
hro
ug
h t
he
man
ufa
ctu
rer
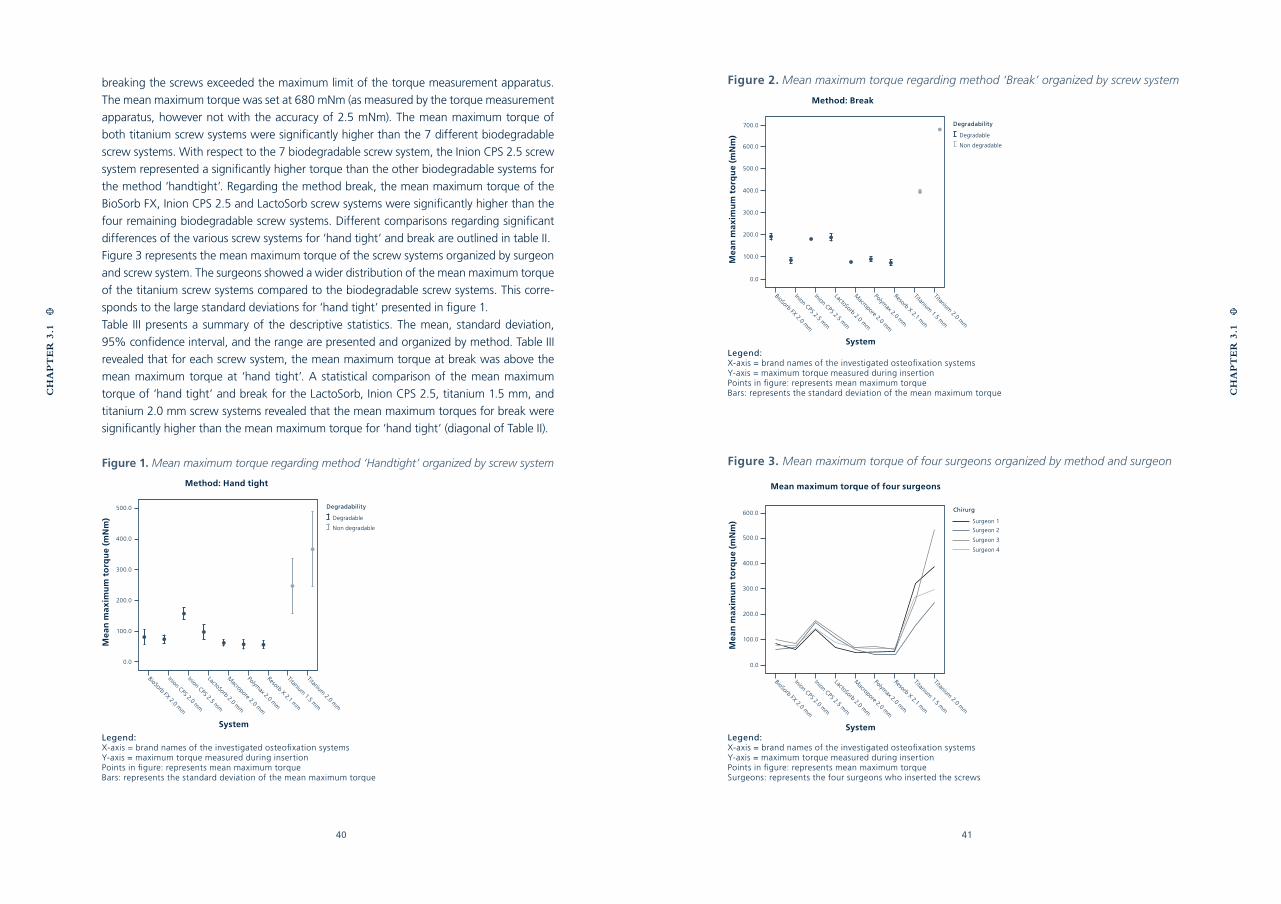
40
CH
AP
TE
R 3
.1
CH
AP
TE
R 3
.1
41
Figure 2. Mean maximum torque regarding method ‘Break’ organized by screw system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = maximum torque measured during insertionPoints in figure: represents mean maximum torqueBars: represents the standard deviation of the mean maximum torque
Figure 3. Mean maximum torque of four surgeons organized by method and surgeon
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = maximum torque measured during insertionPoints in figure: represents mean maximum torque Surgeons: represents the four surgeons who inserted the screws
breaking the screws exceeded the maximum limit of the torque measurement apparatus.
The mean maximum torque was set at 680 mNm (as measured by the torque measurement
apparatus, however not with the accuracy of 2.5 mNm). The mean maximum torque of
both titanium screw systems were significantly higher than the 7 different biodegradable
screw systems. With respect to the 7 biodegradable screw system, the Inion CPS 2.5 screw
system represented a significantly higher torque than the other biodegradable systems for
the method ‘handtight’. Regarding the method break, the mean maximum torque of the
BioSorb FX, Inion CPS 2.5 and LactoSorb screw systems were significantly higher than the
four remaining biodegradable screw systems. Different comparisons regarding significant
differences of the various screw systems for ‘hand tight’ and break are outlined in table II.
Figure 3 represents the mean maximum torque of the screw systems organized by surgeon
and screw system. The surgeons showed a wider distribution of the mean maximum torque
of the titanium screw systems compared to the biodegradable screw systems. This corre-
sponds to the large standard deviations for ‘hand tight’ presented in figure 1.
Table III presents a summary of the descriptive statistics. The mean, standard deviation,
95% confidence interval, and the range are presented and organized by method. Table III
revealed that for each screw system, the mean maximum torque at break was above the
mean maximum torque at ‘hand tight’. A statistical comparison of the mean maximum
torque of ‘hand tight’ and break for the LactoSorb, Inion CPS 2.5, titanium 1.5 mm, and
titanium 2.0 mm screw systems revealed that the mean maximum torques for break were
significantly higher than the mean maximum torque for ‘hand tight’ (diagonal of Table II).
Figure 1. Mean maximum torque regarding method ‘Handtight’ organized by screw system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = maximum torque measured during insertionPoints in figure: represents mean maximum torque Bars: represents the standard deviation of the mean maximum torque
Degradability
Degradable
Non degradable
Method: Hand tight
System
BioSorb FX 2.0 mm
500.0
400.0
300.0
200.0
100.0
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.1 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.0 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n m
axi
mu
m t
orq
ue
(mN
m)
Degradability
Degradable
Non degradable
Method: Break
System
BioSorb FX 2.0 mm
700.0
600.0
500.0
400.0
300.0
200.0
100.0
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.1 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.5 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n m
axi
mu
m t
orq
ue
(mN
m)
Chirurg
Surgeon 1
Surgeon 2
Surgeon 3
Surgeon 4
System
BioSorb FX 2.0 mm
600.0
500.0
400.0
300.0
200.0
100.0
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.1 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.0 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n m
axi
mu
m t
orq
ue
(mN
m)
Mean maximum torque of four surgeons
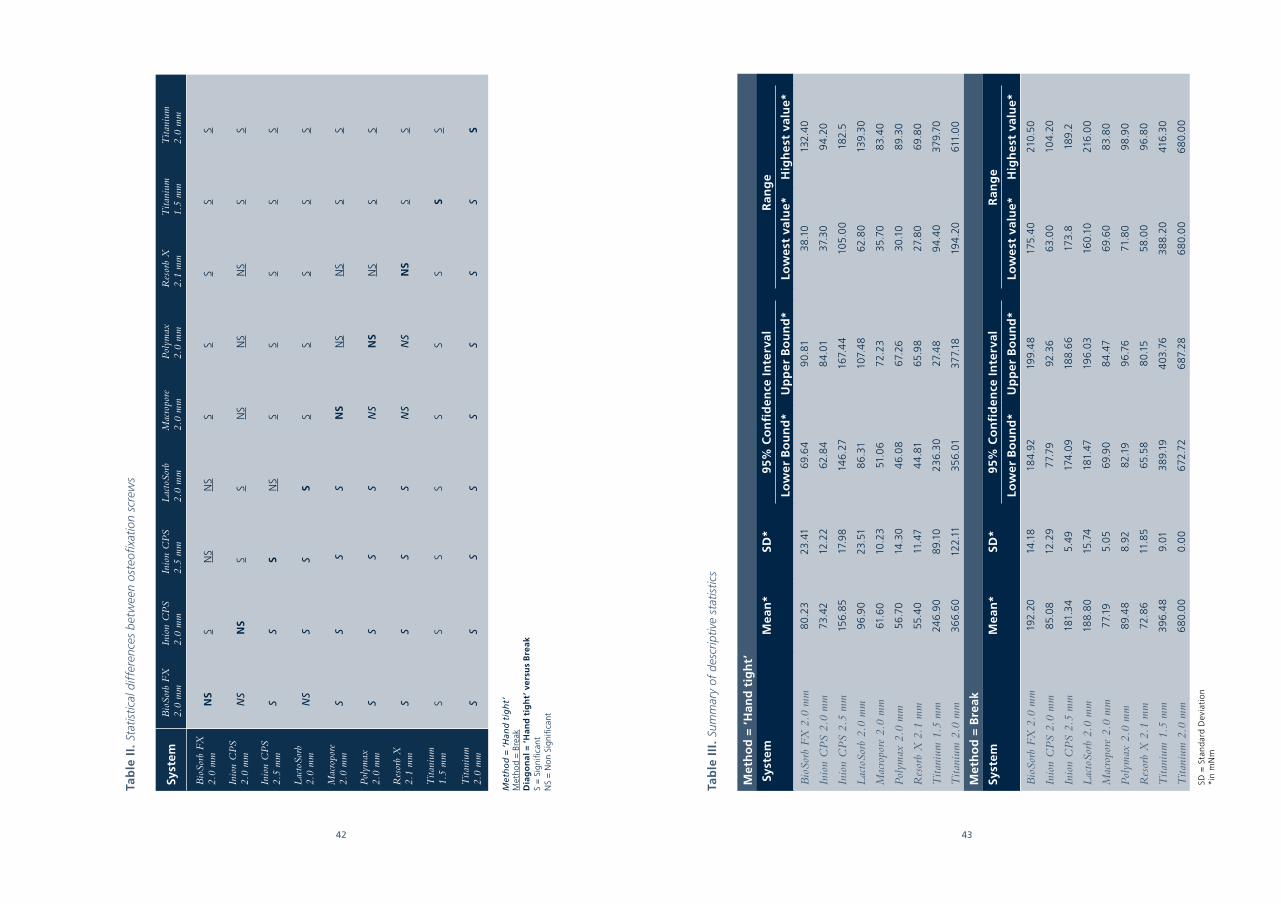
42 43
Tab
le I
I. S
tatis
tical
dif
fere
nces
bet
wee
n os
teofi
xatio
n sc
rew
s
Syst
emB
ioSo
rb F
X
2.0
mm
Inio
n C
PS
2.0
mm
Inio
n C
PS
2.5
mm
Lac
toSo
rb
2.0
mm
Mac
ropo
re
2.0
mm
Pol
ymax
2.
0 m
mR
esor
b X
2.1
mm
Tita
nium
1.
5 m
mT
itani
um
2.0
mm
Bio
Sorb
FX
2.
0 m
mN
SS
NS
NS
SS
SS
S
Inio
n C
PS
2.0
mm
NS
NS
SS
NS
NS
NS
SS
Inio
n C
PS
2.5
mm
SS
SN
SS
SS
SS
Lac
toSo
rb
2.0
mm
NS
SS
SS
SS
SS
Mac
ropo
re
2.0
mm
SS
SS
NS
NS
NS
SS
Pol
ymax
2.0
mm
SS
SS
NS
NS
NS
SS
Res
orb
X2.
1 m
mS
S S
SN
SN
SN
SS
S
Tita
nium
1.5
mm
SS
SS
SS
SS
S
Tita
nium
2.0
mm
SS
SS
SS
SS
S
Met
ho
d =
‘H
and
tig
ht’
Met
ho
d =
Bre
akD
iag
on
al =
‘H
and
tig
ht’
ver
sus
Bre
akS
= S
ign
ifica
ntN
S =
No
n Si
gn
ifica
nt
Tab
le I
II.
Sum
mar
y of
des
crip
tive
stat
istic
s
Met
ho
d =
‘H
and
tig
ht’
Sys
tem
Mea
n*
SD*
95%
Co
nfi
den
ce I
nte
rval
Ran
ge
Low
er B
ou
nd
*U
pp
er B
ou
nd
*Lo
we
st v
alu
e*H
igh
est
val
ue*
Bio
Sorb
FX
2.0
mm
80.
2323
.41
69.6
49
0.81
38
.10
132.
40
Inio
n C
PS
2.0
mm
73.4
212
.22
62.8
48
4.0
137
.30
94
.20
Inio
n C
PS
2.5
mm
156
.85
17.9
814
6.2
716
7.4
410
5.0
018
2.5
Lac
toSo
rb 2
.0 m
m9
6.9
023
.51
86
.31
107.
48
62.8
013
9.3
0
Mac
ropo
re 2
.0 m
m61
.60
10.2
351
.06
72.2
335
.70
83.
40
Pol
ymax
2.0
mm
56
.70
14.3
04
6.0
867
.26
30.
108
9.3
0
Res
orb
X 2
.1 m
m55
.40
11.4
74
4.8
165
.98
27.8
069
.80
Tita
nium
1.5
mm
246
.90
89.
1023
6.3
027
.48
94
.40
379.
70
Tita
nium
2.0
mm
36
6.6
012
2.11
356
.01
377.
1819
4.2
061
1.0
0
Met
ho
d =
Bre
ak
Syst
emM
ean
*SD
*95
% C
on
fid
ence
In
terv
alR
ang
e
Low
er B
ou
nd
*U
pp
er B
ou
nd
*Lo
we
st v
alu
e*H
igh
est
val
ue*
Bio
Sorb
FX
2.0
mm
192.
2014
.18
184
.92
199.
48
175.
40
210.
50
Inio
n C
PS
2.0
mm
85.0
812
.29
77.7
992
.36
63.0
010
4.2
0
Inio
n C
PS
2.5
mm
181.
34
5.49
174
.09
188
.66
173.
818
9.2
Lac
toSo
rb 2
.0 m
m18
8.8
015
.74
181.
4719
6.0
316
0.10
216
.00
Mac
ropo
re 2
.0 m
m77
.19
5.0
569
.90
84
.47
69.6
08
3.8
0
Pol
ymax
2.0
mm
89.
48
8.9
28
2.19
96
.76
71.8
09
8.9
0
Res
orb
X 2
.1 m
m72
.86
11.8
565
.58
80.
155
8.0
09
6.8
0
Tita
nium
1.5
mm
396
.48
9.01
38
9.19
403
.76
38
8.2
041
6.3
0
Tita
nium
2.0
mm
68
0.0
00.
00
672.
726
87.2
86
80.
00
68
0.0
0
SD =
Sta
nd
ard
Dev
iati
on
*in
mN
m
44
CH
AP
TE
R 3
.1
CH
AP
TE
R 3
.1
45
DISCUSSION
The differences in maximum torque found for the studied systems can be explained
by the different screw diameters (1.5-, 2.0-, 2.1- and 2.5 mm), different (co-polymer)
compositions, different geometry (pitch and shaft) of the screws, different tools used
to insert the screws, different ages of the screws, and different methods to sterilize
the screws. As expected, the use of titanium for manufacturing osteofixation screws
revealed a high maximum torque strength whereas the use of polymers revealed a sig-
nificantly lower torque strength. A surprising finding was the significant mean maximum
torque difference of the BioSorb FX, Inion CPS 2.5 and LactoSorb screw systems com-
pared to the remaining four biodegradable screw systems for the method break. The
self-reinforced polymers of the BioSorb FX screw system, the larger dimensions of the
2.5 mm Inion CPS screws, and the ponderous geometry of the LactoSorb screws are
probably responsible for the high maximum torque. The large standard deviations of
the 2 titanium screw systems presented in figure 1 are probably caused by the higher
maximum torque. After all, when surgeons apply higher torque forces, this inevitably
implies loss of accuracy.
The comparison of the maximum torque of ‘hand tight’ and break for the individual
screw systems revealed statistically significant differences for 4 (LactoSorb, Inion CPS
2.5, titanium 1.5 mm, and titanium 2.0 mm) of the 9 osteofixation screw systems (diago-
nal Table II). In the case of individual biodegradable screws (Inion CPS 2.0 mm, Inion CPS
2.5 mm, Macropore 2.0 mm, and Resorb X 2.1 mm), the lowest torque at break was not
always above the highest torque of ‘hand tight’. Besides, the 95% confidence intervals
of the maximum torque with respect to break and ‘hand tight’ of biodegradable screws
did overlap (Table III). These two aspects indicate that the torsion characteristics of bio-
degradable screws are not always that repeatable.
For analyzing the results, the data of the four surgeons have been combined in order to
reduce the influence of outliers and to determine statistical significant differences. The
results of the independent surgeons are graphically presented in figure 3. Note the large
differences in mean maximum torque regarding the 2 titanium systems compared to the
7 biodegradable systems. Statistical analysis yielded no significant differences between
most surgeons except for two surgeons. This is largely due to the statistical influence of
the large differences in mean maximum torque for titanium screws. Despite the signifi-
cant difference between the two surgeons, the data were combined. After all, combin-
ing the results of the four surgeons should be allowed because the insertion torque of
screws of maxillofacial surgeons should be approximately equal.
Investigating 7 different biodegradable screws theoretically implies 7 learning curves, as
is the case with every new technique (64;123;124). These learning curves could influence
the results and consequent statistically significant differences. To find out whether the
learning curves affected the results, the screw 1- and 2- data have been deleted for every
surgeon and system. The raw data were then analyzed (6 instead of 8 screws) again.
Eliminating the first 2 screws did not reveal different statistically (significant) results be-
tween the osteofixation screw systems.
Statistically significant differences do not necessarily imply differences to be clinically rel-
evant. With respect to the investigated osteosynthesis screws in this study, it is ques-
tionable whether the statistically significant differences are clinically relevant. The large
significant differences between titanium screws and biodegradable screws in mean maxi-
mum torque are clinically relevant, although the field of application may be different. In
contrast, the statistically significant differences between some of the 7 biodegradable
devices regarding the method ‘hand tight’ are not clinically relevant, because they are
considered to be too small. Moreover, it has been reported that biodegradable devices
physically relax under constant force (a process called creep). In this case, the applied
torque is ‘counteracted’ by the reorganizing polymer chains (111). Titanium screws do not
undergo this material relaxation. The significant differences between some of the 7 bio-
degradable devices for the method break are of clinical importance, because biodegrad-
able screws can fracture easily during insertion. The significant differences of maximum
torque for ‘hand tight’ and break of 2 biodegradable (Inion CPS 2.5, and LactoSorb) as
well as both titanium screw systems presented in the current study are clinically relevant.
After all, screws will break easily during insertion, when the differences between ‘hand
tight’ and break are small.
The objectives of this investigation were to determine: (1) the differences in mean maxi-
mum torque between 7 biodegradable and 2 titanium screw systems, and (2) the differ-
ences of mean maximum torque between ‘hand tight’ and break of the biodegradable
as well as the titanium osteofixation screw systems. This study has presented that: (1) the
mean maximum torque of titanium screw systems was significantly higher than of the
biodegradable screw systems, and (2) the mean maximum torque of all 9 screw systems
at break was (significantly) higher than at ‘hand tight’. Based on the results and discus-
sion points mentioned above, we can conclude that the 1.5- and 2.0 mm titanium screw
systems still present the highest torque strength compared to the biodegradable screw
systems. When there is an intention to use biodegradable screws, we would recommend
the use of 2.0 mm BioSorb FX, 2.0 mm LactoSorb or the larger 2.5 mm Inion CPS screws.
Acknowledgements
We would like to thank, prof. dr. G.M. Raghoebar, dr. F.K.L. Spijkervet and dr. J. Jansma
for inserting the osteofixation screws. The authors also would like to thank dr. H. Groen
and dr. M.M. Span for their statistical assistance. The gratuitously supply of biodegrad-
able screws through the manufacturers (Linvatec Biomaterials Ltd., KLS Martin, Inion Ltd.,
Walter Lorenz Surgical Inc., Synthes, and Macropore Inc.) was gratefully appreciated.
CHAPTER 3.2.1
MECHANICAL STRENGTH
AND STIFFNESS OF
BIODEGRADABLE AND
TITANIUM OSTEOFIXATION
SYSTEMS
G.J. BUIJS
E.B. VAN DER HOUWEN
B. STEGENGA
R.R.M. BOS
G.J. VERKERKE
Published in: J Oral Maxillofac Surg. 2007 Nov;65(11):2148-58.
48 49
CH
AP
TE
R 3
.2.1
Abstract:
Objective - The objective of this study was to present relevant mechanical data in order
to simplify the selection of an osteofixation system for situations requiring immobilization
in oral and maxillofacial surgery.
Materials & Methods - 7 biodegradable and 2 titanium osteofixation systems were in-
vestigated. The plates and screws were fixed to 2 polymethylmethacrylate (PMMA) blocks
to simulate bone segments. The plates and screws were subjected to tensile, side bend-
ing, and torsion tests. During tensile tests, the strength of the osteofixation system was
monitored. The stiffness was calculated for the tensile, side bending, and torsion tests.
Results - The two titanium systems (1.5 mm and 2.0 mm) presented significantly higher
tensile strength and stiffness compared to the 7 biodegradable systems (2.0 mm, 2.1 mm,
and 2.5 mm). The 2.0 mm titanium system revealed significantly higher side bending and
torsion stiffness than the other 7 systems.
Conclusion & discussion - Based on the results of the current study, it can be concluded
that the titanium osteofixation systems were (significantly) stronger and stiffer than the
biodegradable systems. The BioSorb FX, LactoSorb, and Inion CPS 2.5 mm systems have
high mechanical device strength and stiffness compared to the investigated biodegrad-
able osteofixation systems. With the cross-sectional surface taken into account, the Bio-
Sorb FX system (with its subtle design), proves to be the far more superior system. The
Resorb X and MacroPore systems present to be, at least from a mechanical point of view,
the least strong and stiff systems in the test.
Key words: osteofixation system; biodegradable; titanium; mechanical; strength; stiff-
ness; properties.
INTRODUCTION
Background
Sufficient revascularization, anatomical reduction, and proper immobilization of bone
segments are essential aspects of the healing of fractures and osteotomies (7;10). Im-
mobilization of bone fragments is currently obtained by the use of osteofixation plates
and screws (125;126). The plates and screws are applied subperiostally in order to secure
sufficient revascularization (7). These fixation devices must withstand the local deforming
forces that are exerted through the maxillofacial muscles.
Currently, titanium fixation systems are successfully used to realize adequate immobiliza-
tion (39). These systems, however, have several disadvantages: (1) the need for a second
intervention to remove the devices, if indicated (46-48), (2) interference with imaging or
radio-therapeutic techniques (37;41;127), (3) possible growth disturbance or mutagenic
effects (37;41;43-45), (4) brain damage (44;128), (5) and thermal sensitivity (129).
Biodegradable ‘dissolving’ fixation systems could reduce the problems associated with
titanium systems (74). However, these systems are mechanically weaker than titanium
systems due to the use of biodegradable polymers. Moreover, adverse reactions to the
degradation products have been reported (66;67;100;114). Despite these disadvantages,
there is a continuous drive to explore fixation devices which will ‘dissolve’ when bone
healing has been occurred (4). In order to investigate whether biodegradable systems
are proper alternatives for titanium systems, they have been the subject of research for
decades (58). Nevertheless, the mechanical properties of biodegradable systems have
hardly been objectively compared in the scientific literature. In addition, many biodegrad-
able fixation systems with a great variety in dimensions and co-polymer compositions
are commercially available. As a result, the mechanical characteristics differ substantially,
which consequently hampers surgeons to select an adequate fixation system for a specif-
ic situation (82). Determining the different mechanical properties of titanium and biode-
gradable osteofixation systems could support the procedure of finding the right fixation
system for the right situation (122).
Objectives
The objective of this study was to present relevant mechanical data in order to simplify
the selection of an osteofixation system for situations requiring immobilization in oral and
maxillofacial surgery.
MATERIALS AND METHODS
The specimens to be investigated were 7 commercially available biodegradable (5 x 2.0
mm, 1 x 2.1 mm, and 1 x 2.5 mm) and 2 commonly used commercially available titanium
(1.5 mm and 2.0 mm) osteofixation systems. The general characteristics of the included
plates and screws are summarized in table I.
CH
AP
TE
R 3
.2.1
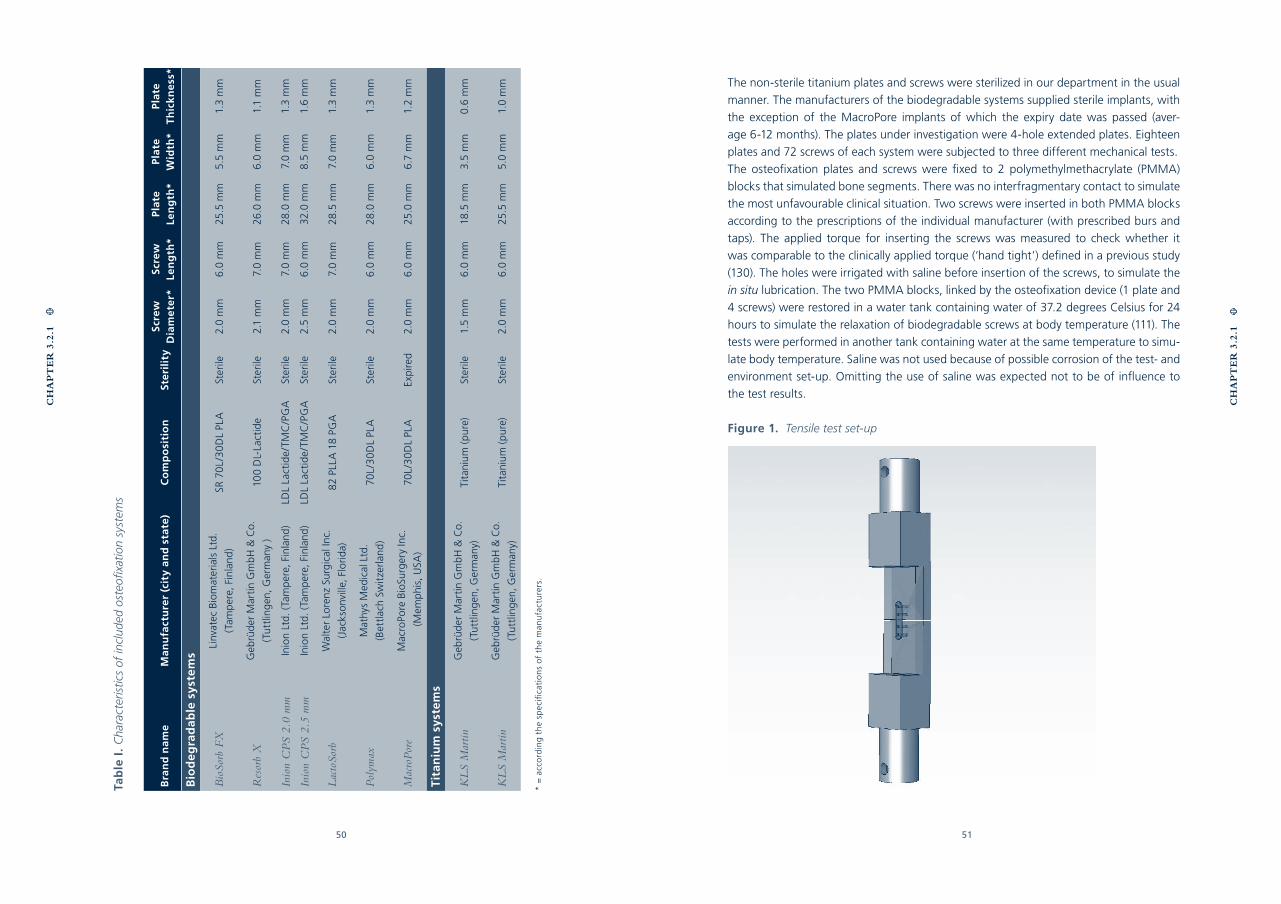
50 51
Tab
le I
. C
hara
cter
istic
s of
incl
uded
ost
eofix
atio
n sy
stem
s
Bra
nd
na
me
Ma
nu
fact
ure
r (c
ity
an
d s
tate
)C
om
po
siti
on
Ste
rili
tyS
crew
D
iam
ete
r*S
crew
Le
ng
th*
Plat
eLe
ng
th*
Plat
eW
idth
*Pl
ate
Th
ick
ne
ss*
Bio
de
gra
dab
le s
yste
ms
Bio
Sorb
FX
Linv
atec
Bio
mat
eria
ls L
td.
(Tam
per
e, F
inla
nd)
SR 7
0L/
30
DL
PLA
Ster
ile2.
0 m
m6
.0 m
m25
.5 m
m5.
5 m
m1.
3 m
m
Res
orb
XG
ebrü
der
Mar
tin
Gm
bH
& C
o.
(Tu
ttlin
gen
, Ger
man
y )
100
DL-
Lact
ide
Ster
ile2.
1 m
m7.
0 m
m26
.0 m
m6
.0 m
m1.
1 m
m
Inio
n C
PS
2.0
mm
Inio
n Lt
d. (
Tam
per
e, F
inla
nd)
LDL
Lact
ide/
TMC
/PG
ASt
erile
2.0
mm
7.0
mm
28.0
mm
7.0
mm
1.3
mm
Inio
n C
PS
2.5
mm
Inio
n Lt
d. (
Tam
per
e, F
inla
nd)
LDL
Lact
ide/
TMC
/PG
ASt
erile
2.5
mm
6.0
mm
32.0
mm
8.5
mm
1.6
mm
Lac
toSo
rbW
alte
r Lo
renz
Sur
gica
l Inc
.
(Jac
kso
nvill
e, F
lori
da)
82
PLLA
18
PGA
Ster
ile2.
0 m
m7.
0 m
m28
.5 m
m7.
0 m
m1.
3 m
m
Pol
ymax
Mat
hys
Med
ical
Ltd
.
(Bet
tlac
h Sw
itze
rlan
d)
70L/
30
DL
PLA
Ster
ile2.
0 m
m6
.0 m
m28
.0 m
m6
.0 m
m1.
3 m
m
Mac
roP
ore
Mac
roPo
re B
ioSu
rger
y In
c.
(Mem
phi
s, U
SA)
70L/
30
DL
PLA
Exp
ired
2.0
mm
6.0
mm
25.0
mm
6.7
mm
1.2
mm
Tit
aniu
m s
yste
ms
KL
S M
artin
Geb
rüd
er M
arti
n G
mb
H &
Co.
(Tu
ttlin
gen
, Ger
man
y)Ti
tani
um (
pure
)St
erile
1.5
mm
6.0
mm
18.5
mm
3.5
mm
0.6
mm
KL
S M
artin
Geb
rüd
er M
arti
n G
mb
H &
Co.
(Tu
ttlin
gen
, Ger
man
y)Ti
tani
um (
pure
)St
erile
2.0
mm
6.0
mm
25.5
mm
5.0
mm
1.0
mm
* =
acc
ord
ing
th
e sp
ecifi
cati
on
s o
f th
e m
anu
fact
ure
rs.
The non-sterile titanium plates and screws were sterilized in our department in the usual
manner. The manufacturers of the biodegradable systems supplied sterile implants, with
the exception of the MacroPore implants of which the expiry date was passed (aver-
age 6-12 months). The plates under investigation were 4-hole extended plates. Eighteen
plates and 72 screws of each system were subjected to three different mechanical tests.
The osteofixation plates and screws were fixed to 2 polymethylmethacrylate (PMMA)
blocks that simulated bone segments. There was no interfragmentary contact to simulate
the most unfavourable clinical situation. Two screws were inserted in both PMMA blocks
according to the prescriptions of the individual manufacturer (with prescribed burs and
taps). The applied torque for inserting the screws was measured to check whether it
was comparable to the clinically applied torque (‘hand tight’) defined in a previous study
(130). The holes were irrigated with saline before insertion of the screws, to simulate the
in situ lubrication. The two PMMA blocks, linked by the osteofixation device (1 plate and
4 screws) were restored in a water tank containing water of 37.2 degrees Celsius for 24
hours to simulate the relaxation of biodegradable screws at body temperature (111). The
tests were performed in another tank containing water at the same temperature to simu-
late body temperature. Saline was not used because of possible corrosion of the test- and
environment set-up. Omitting the use of saline was expected not to be of influence to
the test results.
Figure 1. Tensile test set-up
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
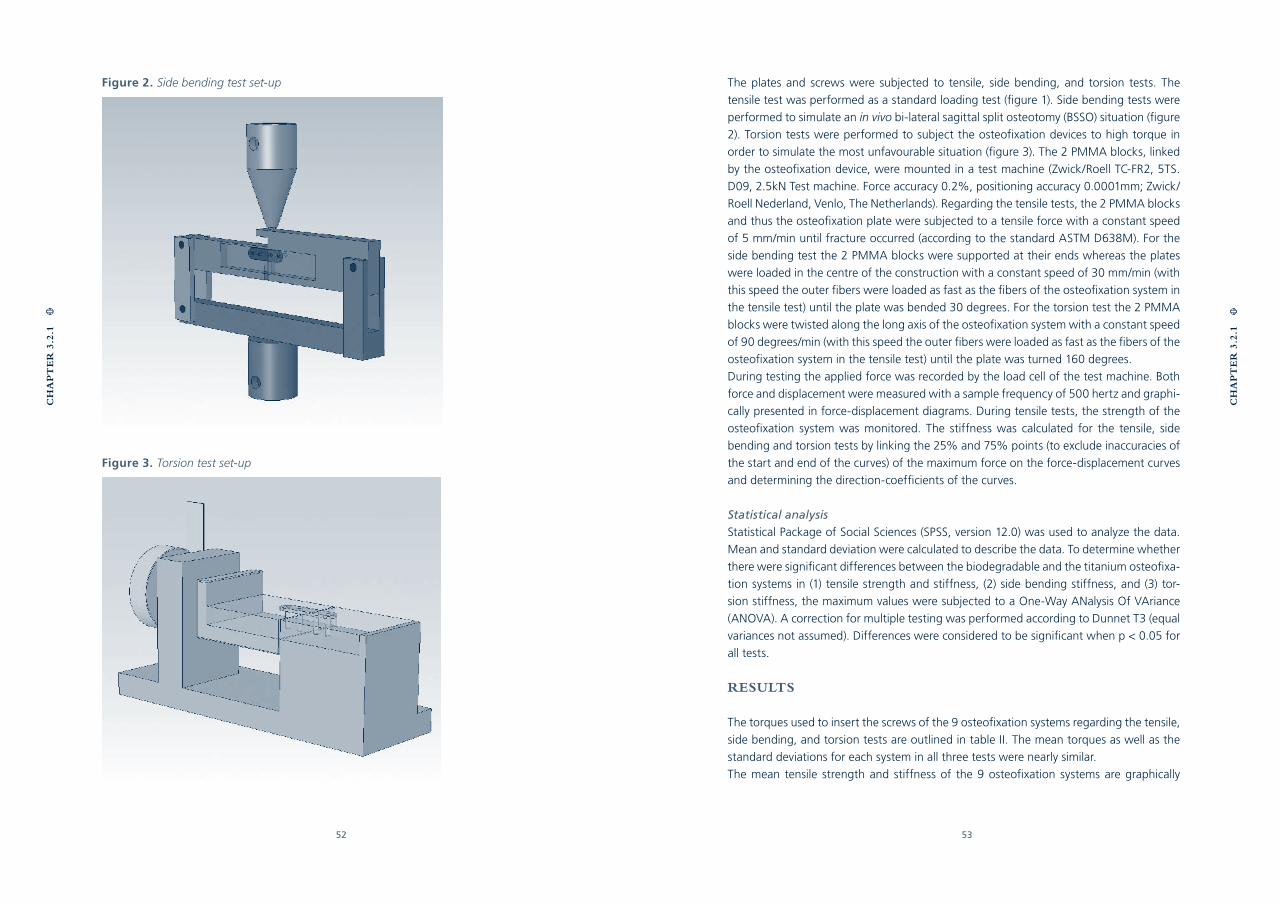
52 53
The plates and screws were subjected to tensile, side bending, and torsion tests. The
tensile test was performed as a standard loading test (figure 1). Side bending tests were
performed to simulate an in vivo bi-lateral sagittal split osteotomy (BSSO) situation (figure
2). Torsion tests were performed to subject the osteofixation devices to high torque in
order to simulate the most unfavourable situation (figure 3). The 2 PMMA blocks, linked
by the osteofixation device, were mounted in a test machine (Zwick/Roell TC-FR2, 5TS.
D09, 2.5kN Test machine. Force accuracy 0.2%, positioning accuracy 0.0001mm; Zwick/
Roell Nederland, Venlo, The Netherlands). Regarding the tensile tests, the 2 PMMA blocks
and thus the osteofixation plate were subjected to a tensile force with a constant speed
of 5 mm/min until fracture occurred (according to the standard ASTM D638M). For the
side bending test the 2 PMMA blocks were supported at their ends whereas the plates
were loaded in the centre of the construction with a constant speed of 30 mm/min (with
this speed the outer fibers were loaded as fast as the fibers of the osteofixation system in
the tensile test) until the plate was bended 30 degrees. For the torsion test the 2 PMMA
blocks were twisted along the long axis of the osteofixation system with a constant speed
of 90 degrees/min (with this speed the outer fibers were loaded as fast as the fibers of the
osteofixation system in the tensile test) until the plate was turned 160 degrees.
During testing the applied force was recorded by the load cell of the test machine. Both
force and displacement were measured with a sample frequency of 500 hertz and graphi-
cally presented in force-displacement diagrams. During tensile tests, the strength of the
osteofixation system was monitored. The stiffness was calculated for the tensile, side
bending and torsion tests by linking the 25% and 75% points (to exclude inaccuracies of
the start and end of the curves) of the maximum force on the force-displacement curves
and determining the direction-coefficients of the curves.
Statistical analysis
Statistical Package of Social Sciences (SPSS, version 12.0) was used to analyze the data.
Mean and standard deviation were calculated to describe the data. To determine whether
there were significant differences between the biodegradable and the titanium osteofixa-
tion systems in (1) tensile strength and stiffness, (2) side bending stiffness, and (3) tor-
sion stiffness, the maximum values were subjected to a One-Way ANalysis Of VAriance
(ANOVA). A correction for multiple testing was performed according to Dunnet T3 (equal
variances not assumed). Differences were considered to be significant when p < 0.05 for
all tests.
RESULTS
The torques used to insert the screws of the 9 osteofixation systems regarding the tensile,
side bending, and torsion tests are outlined in table II. The mean torques as well as the
standard deviations for each system in all three tests were nearly similar.
The mean tensile strength and stiffness of the 9 osteofixation systems are graphically
Figure 2. Side bending test set-up
Figure 3. Torsion test set-up
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
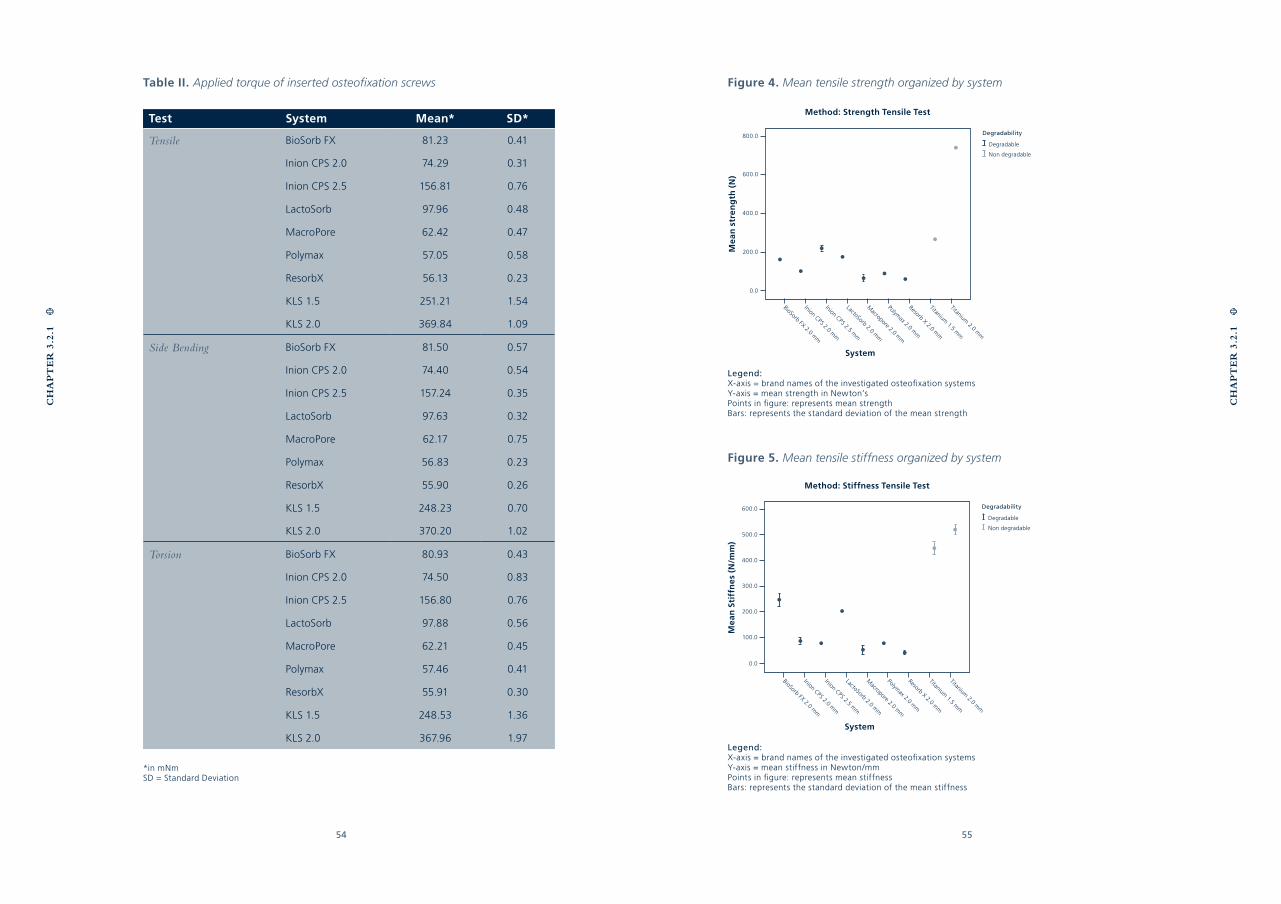
54 55
Table II. Applied torque of inserted osteofixation screws
Test System Mean* SD*
Tensile BioSorb FX 81.23 0.41
Inion CPS 2.0 74.29 0.31
Inion CPS 2.5 156.81 0.76
LactoSorb 97.96 0.48
MacroPore 62.42 0.47
Polymax 57.05 0.58
ResorbX 56.13 0.23
KLS 1.5 251.21 1.54
KLS 2.0 369.84 1.09
Side Bending BioSorb FX 81.50 0.57
Inion CPS 2.0 74.40 0.54
Inion CPS 2.5 157.24 0.35
LactoSorb 97.63 0.32
MacroPore 62.17 0.75
Polymax 56.83 0.23
ResorbX 55.90 0.26
KLS 1.5 248.23 0.70
KLS 2.0 370.20 1.02
Torsion BioSorb FX 80.93 0.43
Inion CPS 2.0 74.50 0.83
Inion CPS 2.5 156.80 0.76
LactoSorb 97.88 0.56
MacroPore 62.21 0.45
Polymax 57.46 0.41
ResorbX 55.91 0.30
KLS 1.5 248.53 1.36
KLS 2.0 367.96 1.97
*in mNm SD = Standard Deviation
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
Figure 5. Mean tensile stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mmPoints in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness
Figure 4. Mean tensile strength organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean strength in Newton’sPoints in figure: represents mean strengthBars: represents the standard deviation of the mean strength
Degradability
Degradable
Non degradable
Method: Strength Tensile Test
System
BioSorb FX 2.0 mm
800.0
600.0
400.0
200.0
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.0 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.0 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n s
tren
gth
(N
)
Degradability
Degradable
Non degradable
Method: Stiffness Tensile Test
System
BioSorb FX 2.0 mm
600.0
500.0
400.0
300.0
200.0
100.0
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.0 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.0 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n S
tiff
ne
s (N
/mm
)
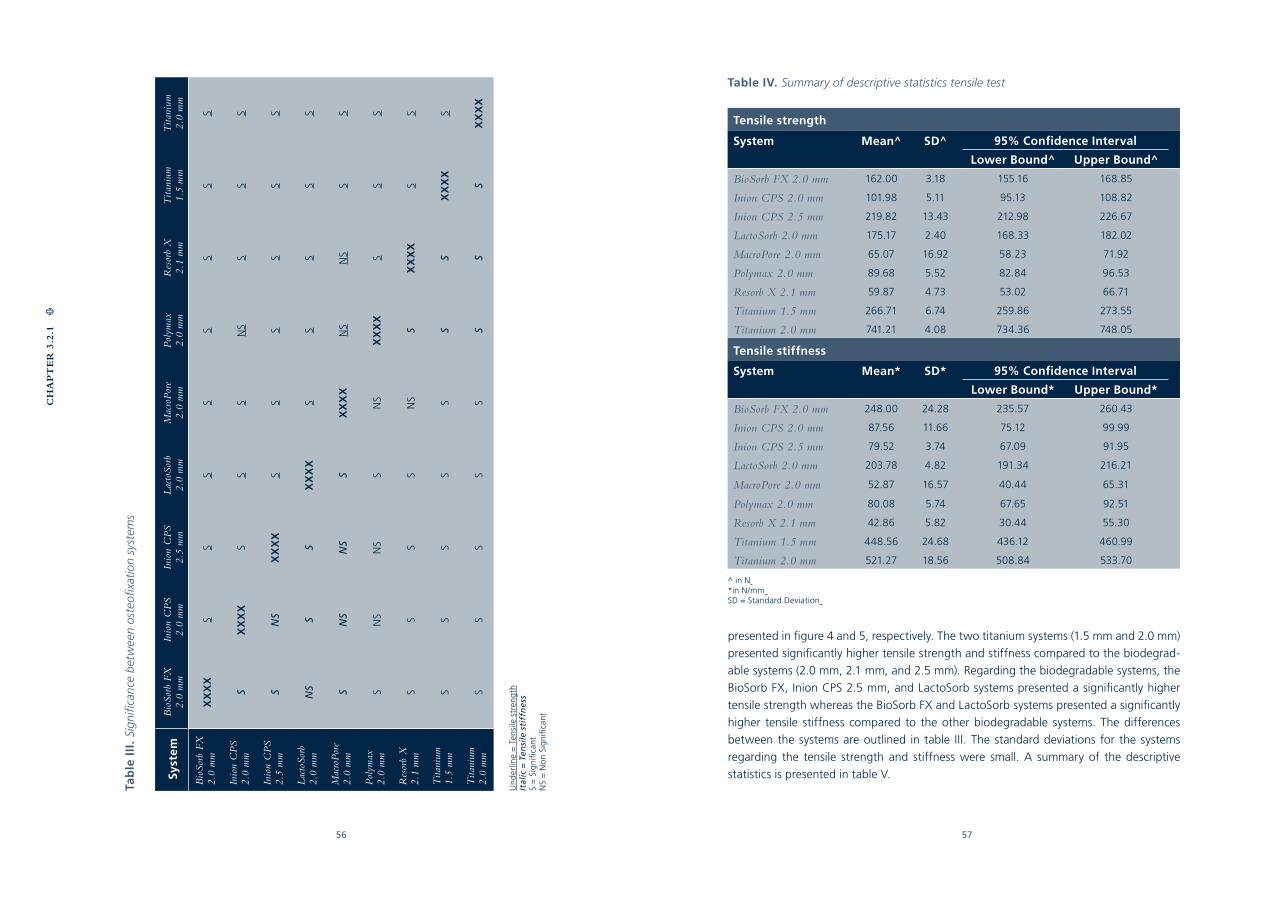
56 57
Tab
le I
II.
Sign
ifica
nce
bet
wee
n os
teofi
xatio
n sy
stem
s
Syst
emB
ioSo
rb F
X
2.0
mm
Inio
n C
PS
2.0
mm
Inio
n C
PS
2.5
mm
Lac
toSo
rb
2.0
mm
Mac
roP
ore
2.0
mm
Pol
ymax
2.
0 m
mR
esor
b X
2.
1 m
mT
itani
um
1.5
mm
Tita
nium
2.
0 m
m
Bio
Sorb
FX
2.
0 m
mX
XX
XS
SS
SS
SS
S
Inio
n C
PS
2.0
mm
SX
XX
XS
SS
NS
SS
S
Inio
n C
PS
2.5
mm
SN
SX
XX
XS
SS
SS
S
Lac
toSo
rb
2.0
mm
NS
SS
XX
XX
SS
SS
S
Mac
roP
ore
2.0
mm
SN
SN
SS
XX
XX
NS
NS
SS
Pol
ymax
2.
0 m
mS
NS
NS
SN
SX
XX
XS
SS
Res
orb
X
2.1
mm
SS
SS
NS
SX
XX
XS
S
Tita
nium
1.
5 m
mS
SS
SS
SS
XX
XX
S
Tita
nium
2.0
mm
SS
SS
SS
SS
XX
XX
Un
der
line
= T
ensi
le s
tren
gth
Ital
ic =
Ten
sile
sti
ffn
ess
S =
Sig
nifi
cant
NS
= N
on
Sig
nifi
cant
CH
AP
TE
R 3
.2.1
Table IV. Summary of descriptive statistics tensile test
Tensile strength
System Mean^ SD^ 95% Confidence Interval
Lower Bound^ Upper Bound^
BioSorb FX 2.0 mm 162.00 3.18 155.16 168.85
Inion CPS 2.0 mm 101.98 5.11 95.13 108.82
Inion CPS 2.5 mm 219.82 13.43 212.98 226.67
LactoSorb 2.0 mm 175.17 2.40 168.33 182.02
MacroPore 2.0 mm 65.07 16.92 58.23 71.92
Polymax 2.0 mm 89.68 5.52 82.84 96.53
Resorb X 2.1 mm 59.87 4.73 53.02 66.71
Titanium 1.5 mm 266.71 6.74 259.86 273.55
Titanium 2.0 mm 741.21 4.08 734.36 748.05
Tensile stiffness
System Mean* SD* 95% Confidence Interval
Lower Bound* Upper Bound*
BioSorb FX 2.0 mm 248.00 24.28 235.57 260.43
Inion CPS 2.0 mm 87.56 11.66 75.12 99.99
Inion CPS 2.5 mm 79.52 3.74 67.09 91.95
LactoSorb 2.0 mm 203.78 4.82 191.34 216.21
MacroPore 2.0 mm 52.87 16.57 40.44 65.31
Polymax 2.0 mm 80.08 5.74 67.65 92.51
Resorb X 2.1 mm 42.86 5.82 30.44 55.30
Titanium 1.5 mm 448.56 24.68 436.12 460.99
Titanium 2.0 mm 521.27 18.56 508.84 533.70
^ in N *in N/mm SD = Standard Deviation
presented in figure 4 and 5, respectively. The two titanium systems (1.5 mm and 2.0 mm)
presented significantly higher tensile strength and stiffness compared to the biodegrad-
able systems (2.0 mm, 2.1 mm, and 2.5 mm). Regarding the biodegradable systems, the
BioSorb FX, Inion CPS 2.5 mm, and LactoSorb systems presented a significantly higher
tensile strength whereas the BioSorb FX and LactoSorb systems presented a significantly
higher tensile stiffness compared to the other biodegradable systems. The differences
between the systems are outlined in table III. The standard deviations for the systems
regarding the tensile strength and stiffness were small. A summary of the descriptive
statistics is presented in table V.
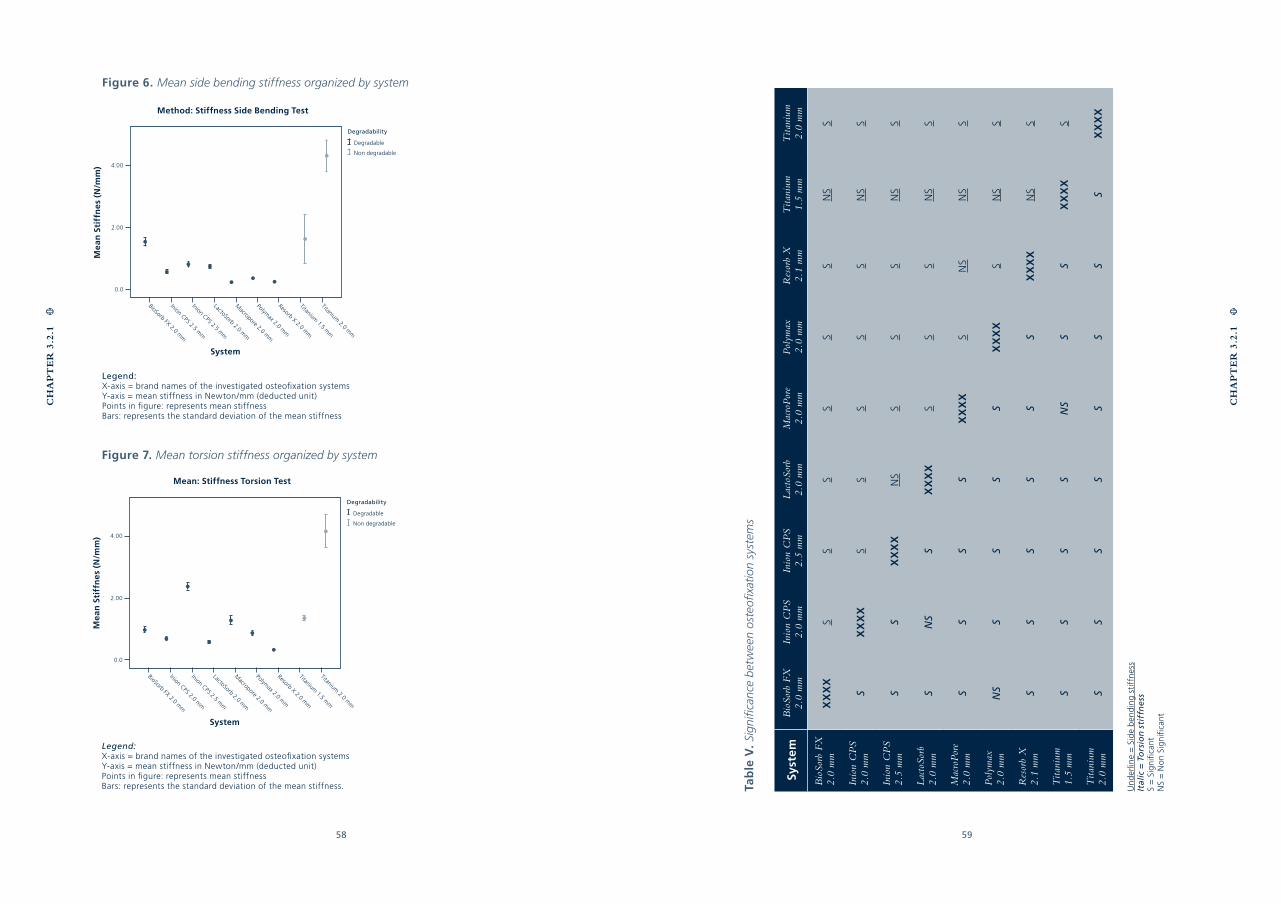
58 59
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
Figure 6. Mean side bending stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mm (deducted unit)Points in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness
Figure 7. Mean torsion stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mm (deducted unit)Points in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness. Ta
ble
V.
Sign
ifica
nce
bet
wee
n os
teofi
xatio
n sy
stem
s
Syst
emB
ioSo
rb F
X
2.0
mm
Inio
n C
PS
2.0
mm
Inio
n C
PS
2.5
mm
Lac
toSo
rb
2.0
mm
Mac
roP
ore
2.0
mm
Pol
ymax
2.
0 m
mR
esor
b X
2.
1 m
mT
itani
um
1.5
mm
Tita
nium
2.
0 m
m
Bio
Sorb
FX
2.
0 m
mX
XX
XS
SS
SS
SN
SS
Inio
n C
PS
2.0
mm
SX
XX
XS
SS
SS
NS
S
Inio
n C
PS
2.5
mm
SS
XX
XX
NS
SS
SN
SS
Lac
toSo
rb
2.0
mm
SN
SS
XX
XX
SS
SN
SS
Mac
roP
ore
2.0
mm
SS
SS
XX
XX
SN
SN
SS
Pol
ymax
2.
0 m
mN
SS
SS
SX
XX
XS
NS
S
Res
orb
X
2.1
mm
SS
SS
SS
XX
XX
NS
S
Tita
nium
1.
5 m
mS
SS
SN
SS
SX
XX
XS
Tita
nium
2.
0 m
mS
SS
SS
SS
SX
XX
X
Un
der
line
= S
ide
ben
din
g st
iffn
ess
Ital
ic =
To
rsio
n s
tiff
ne
ssS
= S
ign
ifica
ntN
S =
No
n Si
gn
ifica
nt
Degradability
Degradable
Non degradable
Method: Stiffness Side Bending Test
System
BioSorb FX 2.0 mm
4.00
2.00
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.0 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.5 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n S
tiff
ne
s (N
/mm
)
System
Degradability
Degradable
Non degradable
Mean: Stiffness Torsion Test
BioSorb FX 2.0 mm
4.00
2.00
0.0
Macropore 2.0 m
m
Polymax 2.0 m
m
Resorb X 2.0 mm
Titanium 1.5 m
m
Titanium 2.0 m
m
Inion CPS 2.0 mm
Inion CPS 2.5 mm
LactoSorb 2.0 mm
Mea
n S
tiff
ne
s (N
/mm
)
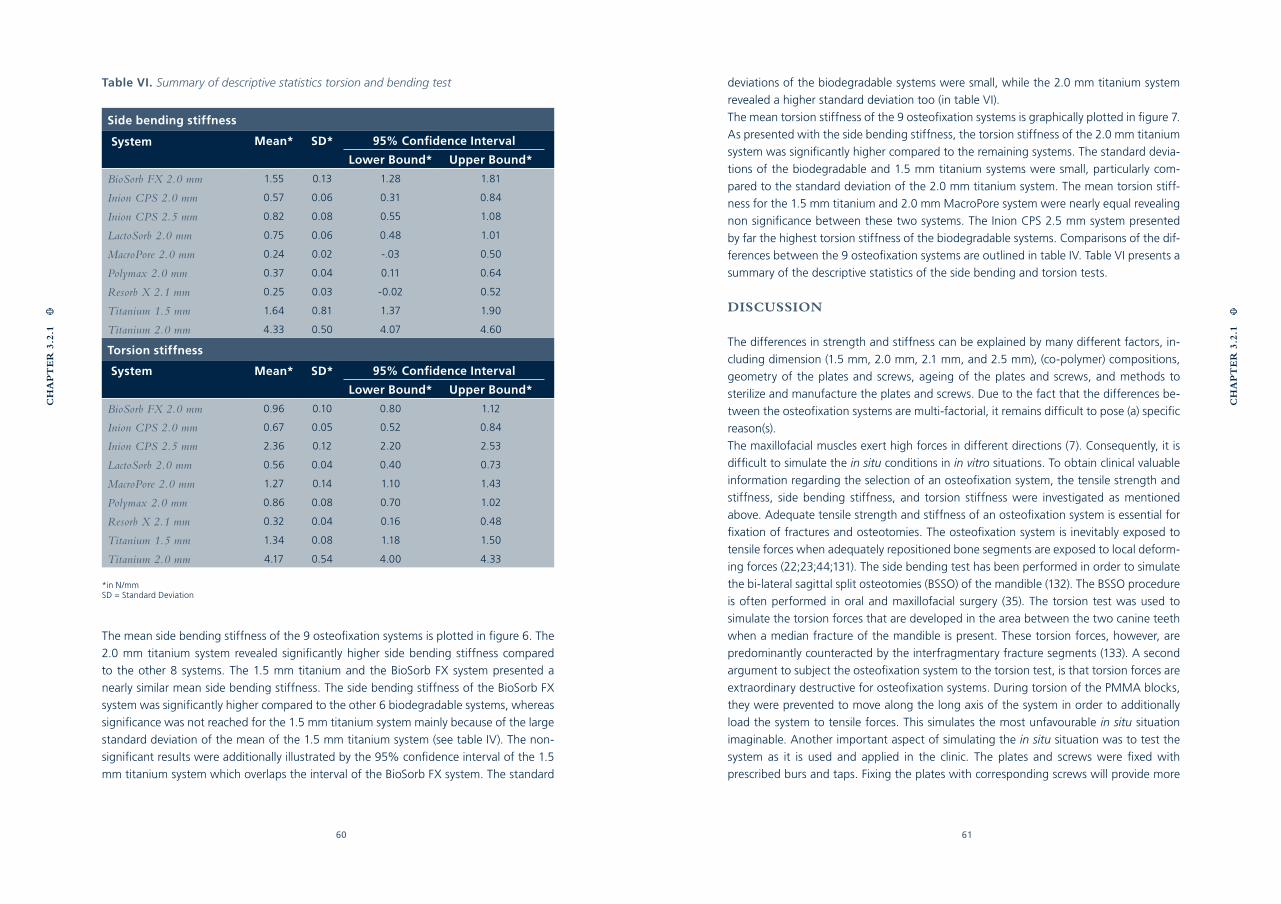
60 61
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
Table VI. Summary of descriptive statistics torsion and bending test
Side bending stiffness
System Mean* SD* 95% Confidence Interval
Lower Bound* Upper Bound*
BioSorb FX 2.0 mm 1.55 0.13 1.28 1.81
Inion CPS 2.0 mm 0.57 0.06 0.31 0.84
Inion CPS 2.5 mm 0.82 0.08 0.55 1.08
LactoSorb 2.0 mm 0.75 0.06 0.48 1.01
MacroPore 2.0 mm 0.24 0.02 -.03 0.50
Polymax 2.0 mm 0.37 0.04 0.11 0.64
Resorb X 2.1 mm 0.25 0.03 -0.02 0.52
Titanium 1.5 mm 1.64 0.81 1.37 1.90
Titanium 2.0 mm 4.33 0.50 4.07 4.60
Torsion stiffness
System Mean* SD* 95% Confidence Interval
Lower Bound* Upper Bound*
BioSorb FX 2.0 mm 0.96 0.10 0.80 1.12
Inion CPS 2.0 mm 0.67 0.05 0.52 0.84
Inion CPS 2.5 mm 2.36 0.12 2.20 2.53
LactoSorb 2.0 mm 0.56 0.04 0.40 0.73
MacroPore 2.0 mm 1.27 0.14 1.10 1.43
Polymax 2.0 mm 0.86 0.08 0.70 1.02
Resorb X 2.1 mm 0.32 0.04 0.16 0.48
Titanium 1.5 mm 1.34 0.08 1.18 1.50
Titanium 2.0 mm 4.17 0.54 4.00 4.33
*in N/mmSD = Standard Deviation
The mean side bending stiffness of the 9 osteofixation systems is plotted in figure 6. The
2.0 mm titanium system revealed significantly higher side bending stiffness compared
to the other 8 systems. The 1.5 mm titanium and the BioSorb FX system presented a
nearly similar mean side bending stiffness. The side bending stiffness of the BioSorb FX
system was significantly higher compared to the other 6 biodegradable systems, whereas
significance was not reached for the 1.5 mm titanium system mainly because of the large
standard deviation of the mean of the 1.5 mm titanium system (see table IV). The non-
significant results were additionally illustrated by the 95% confidence interval of the 1.5
mm titanium system which overlaps the interval of the BioSorb FX system. The standard
deviations of the biodegradable systems were small, while the 2.0 mm titanium system
revealed a higher standard deviation too (in table VI).
The mean torsion stiffness of the 9 osteofixation systems is graphically plotted in figure 7.
As presented with the side bending stiffness, the torsion stiffness of the 2.0 mm titanium
system was significantly higher compared to the remaining systems. The standard devia-
tions of the biodegradable and 1.5 mm titanium systems were small, particularly com-
pared to the standard deviation of the 2.0 mm titanium system. The mean torsion stiff-
ness for the 1.5 mm titanium and 2.0 mm MacroPore system were nearly equal revealing
non significance between these two systems. The Inion CPS 2.5 mm system presented
by far the highest torsion stiffness of the biodegradable systems. Comparisons of the dif-
ferences between the 9 osteofixation systems are outlined in table IV. Table VI presents a
summary of the descriptive statistics of the side bending and torsion tests.
DISCUSSION
The differences in strength and stiffness can be explained by many different factors, in-
cluding dimension (1.5 mm, 2.0 mm, 2.1 mm, and 2.5 mm), (co-polymer) compositions,
geometry of the plates and screws, ageing of the plates and screws, and methods to
sterilize and manufacture the plates and screws. Due to the fact that the differences be-
tween the osteofixation systems are multi-factorial, it remains difficult to pose (a) specific
reason(s).
The maxillofacial muscles exert high forces in different directions (7). Consequently, it is
difficult to simulate the in situ conditions in in vitro situations. To obtain clinical valuable
information regarding the selection of an osteofixation system, the tensile strength and
stiffness, side bending stiffness, and torsion stiffness were investigated as mentioned
above. Adequate tensile strength and stiffness of an osteofixation system is essential for
fixation of fractures and osteotomies. The osteofixation system is inevitably exposed to
tensile forces when adequately repositioned bone segments are exposed to local deform-
ing forces (22;23;44;131). The side bending test has been performed in order to simulate
the bi-lateral sagittal split osteotomies (BSSO) of the mandible (132). The BSSO procedure
is often performed in oral and maxillofacial surgery (35). The torsion test was used to
simulate the torsion forces that are developed in the area between the two canine teeth
when a median fracture of the mandible is present. These torsion forces, however, are
predominantly counteracted by the interfragmentary fracture segments (133). A second
argument to subject the osteofixation system to the torsion test, is that torsion forces are
extraordinary destructive for osteofixation systems. During torsion of the PMMA blocks,
they were prevented to move along the long axis of the system in order to additionally
load the system to tensile forces. This simulates the most unfavourable in situ situation
imaginable. Another important aspect of simulating the in situ situation was to test the
system as it is used and applied in the clinic. The plates and screws were fixed with
prescribed burs and taps. Fixing the plates with corresponding screws will provide more
62 63
CH
AP
TE
R 3
.2.1
CH
AP
TE
R 3
.2.1
the biodegradable systems, whereas the differences between the biodegradable systems
also revealed significance in most cases with regard to tensile strength as well as stiffness.
Moreover, it showed that the side bending stiffness of the titanium 2.0 mm was signifi-
cantly higher than the 8 remaining systems. The BioSorb FX revealed high side bending
stiffness too in comparison to the other biodegradable systems, with both Resorb X and
MacroPore at the lower side. Finally, this study has shown that the torsion stiffness of the
titanium 2.0 mm system was high compared to the other systems. Based on the results
of the current study, it can be concluded the BioSorb FX, Inion CPS 2.5 and LactoSorb
systems represent the highest strength and stiffness’s amongst the investigated biode-
gradable osteofixation systems. With the cross-sectional surface taken into account, the
BioSorb FX system (with its subtle design), proves to be the far more strong and stiff sys-
tem. The Resorb X and MacroPore systems are, at least from a mechanical point of view,
the least strong and stiff systems in the test.
Acknowledgements
The gratuitously supply of titanium as well as biodegradable plates and screws through
the manufacturers (Linvatec Biomaterials Ltd., Gebrüder Martin GmbH & Co., Inion Ltd.,
Walter Lorenz Surgical Inc., Mathys Medical Ltd., and MacroPore BioSurgery Inc.) was
gratefully appreciated. The authors also would like to thank dr. H. Groen for his statistical
assistance. Mr. J. de Jonge is acknowledged for the fabrication of the test set-ups.
clinical relevant information rather than fix the plates with metal screws (122). In this way,
information on the entire system’s (device) mechanical characteristics was obtained.
The stiffness was calculated in all three tests (tensile, side bending, and torsion), while the
strength is reported in just one case (tensile test). The stiffness of an osteofixation system
is a more clinically applicable characteristic (134). Contrary to the stiffness, the maximum
strength will ‘only’ become relevant when the bone segments are separated more than a
few millimeters which inherently results in compromised bone healing. Enlargement of the
healing period is the result, and loosening of the screws and plates, or infection is possible
(134). The stiffness was calculated from the raw data as described in the materials and meth-
ods section. Determining the 25% Fmax and 75% Fmax point as well as the corresponding
displacement implies loss of accuracy due to the limited sample frequency (500 Hz.). This
results in higher relative standard deviations when comparing the tensile strength.
The small standard deviations regarding the tensile strength (predominantly the titanium
systems), elucidate that the method of testing and the test hardware were properly de-
signed regarding reproducibility. The high standard deviations concerning the stiffness of
the titanium systems, however, in both the torsion (titanium 2.0 mm) and side bending
(titanium 1.5 en 2.0 mm) tests, did not support that obviously the assumption of proper
method and hardware design. The explanation for these phenomena could be the meas-
urement imprecision mentioned above or the variety in mechanical properties of the
specimens of each system.
Conspicuous are the torsion and side bending stiffness of the 1.5 mm titanium system
and 4 (BioSorb FX, Inion CPS 2.0, Inion CPS 2.5, and LactoSorb) of the biodegradable
systems which were nearly in the same range of stiffness. This is most probably a result
of the smaller dimensions of the 1.5 mm titanium system. Table IV reveals significant dif-
ferences between the side bending stiffness of the biodegradable systems (caused by the
small standard deviations) while the differences between the 1.5 mm titanium and the
biodegradable systems were non significant.
Titanium osteofixation systems were (significantly) stronger and stiffer than biodegrad-
able systems. Despite the favourable mechanical properties of these systems compared
to the biodegradable systems, the question arises whether the biodegradable systems
pose adequate resistance to the local deforming forces in order to achieve adequate
bone healing in patients (83). After all, the disappearance of a fixation system when
bone union of the bone segments has been obtained, is still very appealing. The question
mentioned above, can only be answered through well-designed randomized clinical trials
which compare biodegradable and titanium osteofixation systems. The present study,
however, provides well-funded information to help surgeons to select a mechanically po-
tent bone fixation system for restoring, fixing, and stabilizing bone segments in specific
situations in the maxillofacial area. The objective of this study was to present relevant
mechanical data in order to simplify the selection of an osteofixation system for situations
requiring immobilization in oral and maxillofacial surgery. This study has presented that
the tensile strength and stiffness of both titanium systems were significantly higher than
CHAPTER 3.2.2
MECHANICAL STRENGTH
AND STIFFNESS OF THE
BIODEGRADABLE SONICWELD
RX OSTEOFIXATION
SYSTEM
G.J. BUIJS
E.B. VAN DER HOUWEN
B. STEGENGA
R.R.M. BOS
G.J. VERKERKE
Published in: J Oral Maxillofac Surg. 2009 Apr;67(4):782-7.
66 67
Abstract:
Objective - To determine the mechanical strength and stiffness of the new 2.1 mm biode-
gradable ultra-sound activated SonicWeld Rx (Gebrüder Martin GmbH & Co., Tuttlingen,
Germany) osteofixation system in comparison with the conventional 2.1 mm biodegrada-
ble Resorb X (Gebrüder Martin GmbH & Co., Tuttlingen, Germany) osteofixation system.
Materials & Methods - The plates and screws were fixed to 2 polymethylmethacrylate
(PMMA) blocks to simulate bone segments and were subjected to tensile, side bending,
and torsion tests. During testing, force and displacement were recorded and graphically
presented in force-displacement diagrams. For the tensile tests, the strength of the oste-
ofixation system was measured. The stiffness was calculated for the tensile, side bending,
and torsion tests.
Results - The tensile strength and stiffness as well as the side bending stiffness of the
SonicWeld Rx system presented up to 11.5 times higher mean values than the conven-
tional Resorb X system. The torsion stiffness of both systems presents similar mean values
and standard deviations.
Conclusion & discussion - The SonicWeld Rx system is an improvement in the search
for a mechanically strong and stiff as well as a biodegradable osteofixation system. Future
research should be done in order to find out whether the promising in vitro results can be
transferred to the in situ clinical situation.
Key words: plate; screw; biodegradable; titanium; mechanical; strength; stiffness; prop-
erties; SonicWeld Rx.
Abbreviations: PMMA, PolyMethylMethAcrylate; SPSS, Statistical Package of Social Sci-
ences; BSSO, Bi-lateral Sagittal Split Osteotomy;
INTRODUCTION
Background
Biodegradable plates and screws are used increasingly in today’s oral and maxillofacial
practice. These biodegradable plates and screws have several advantages over conventional
titanium plates and screws. There is (1) no need for a second intervention to remove
the devices (46-48), (2) no interference with imaging or radio-therapeutic techniques
(37;41;127), (3) no possible growth disturbance or mutagenic effects (37;41;43-45), (4) no
potential brain damage (44;128), (5) and no thermal sensitivity (129). However, the use
of biodegradable plates and screws also has introduced several disadvantages. First, the
boreholes need to be tapped before the screws can be inserted which is time-consuming.
A second disadvantage could be that the biodegradable plates and screws represent
inferior mechanical strength and stiffness compared with conventional titanium plates and
screws (135). In order to resolve these disadvantages, a new biodegradable osteofixation
system, SonicWeld Rx, has been developed. In contrast to conventional biodegradable
osteofixation systems, tapping of the cortical bone layer is not necessary before inserting
the SonicWeld Rx biodegradable pins. A biodegradable pin is simply placed onto an ultra-
sound activated sonic electrode, called a sonotrode, and inserted into the borehole. As
a result of the added ultra-sound energy, the thermoplastic biodegradable pin will melt,
resulting in a flow of biodegradable polymers into the cortical bone layer and the cavities
of the cancellous bone. There is no cellular reaction due to thermal stress during insertion
(136). At the same time the biodegradable plate and pinhead fuse. Theoretically, the
fusion of plate and pinhead will result into superior mechanical device characteristics
in comparison with conventional biodegradable osteofixation systems. This has been
claimed as a second advantage.
The mechanical strength and stiffness of 7 biodegradable as well as 2 titanium
osteofixation systems have recently been investigated (135). One of these investigated
biodegradable systems is the Resorb X biodegradable osteofixation system. The
SonicWeld Rx and the Resorb X biodegradable osteofixation systems are made of the
same co-polymer compositions and have the same device dimensions. These systems are
supplied by the same manufacturer (Gebrüder Martin GmbH & Co. (Tuttlingen, Germany
)). The question arises to what extent the biodegradable ultra-sound activated SonicWeld
Rx osteofixation system presents superior mechanical strength and stiffness as compared
with the conventional biodegradable Resorb X osteofixation system.
Objectives
The objective of this study was to determine the mechanical strength and stiffness of the
biodegradable ultra-sound activated SonicWeld Rx osteofixation system in comparison
with the conventional biodegradable Resorb X osteofixation system.
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2
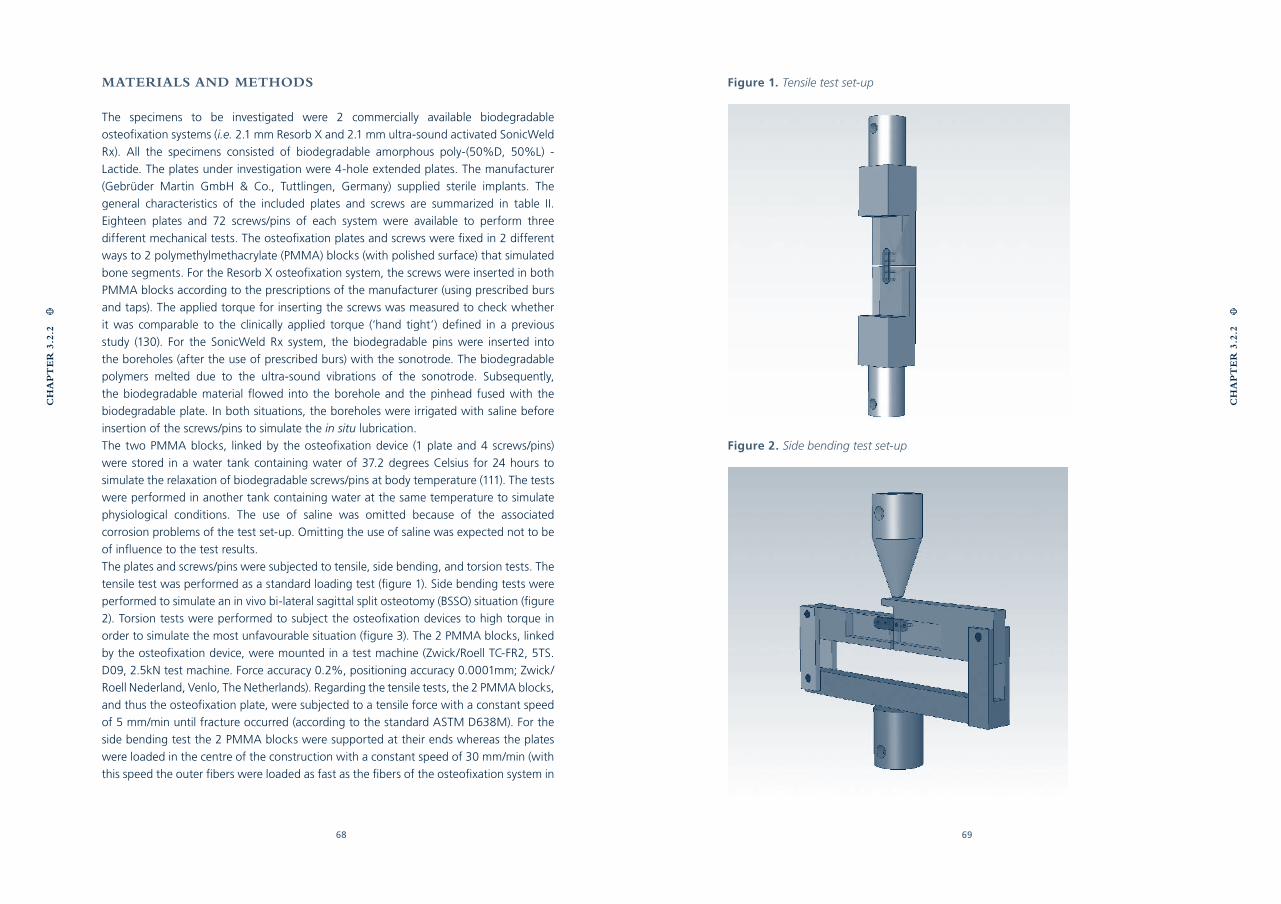
68 69
MATERIALS AND METHODS
The specimens to be investigated were 2 commercially available biodegradable
osteofixation systems (i.e. 2.1 mm Resorb X and 2.1 mm ultra-sound activated SonicWeld
Rx). All the specimens consisted of biodegradable amorphous poly-(50%D, 50%L) -
Lactide. The plates under investigation were 4-hole extended plates. The manufacturer
(Gebrüder Martin GmbH & Co., Tuttlingen, Germany) supplied sterile implants. The
general characteristics of the included plates and screws are summarized in table II.
Eighteen plates and 72 screws/pins of each system were available to perform three
different mechanical tests. The osteofixation plates and screws were fixed in 2 different
ways to 2 polymethylmethacrylate (PMMA) blocks (with polished surface) that simulated
bone segments. For the Resorb X osteofixation system, the screws were inserted in both
PMMA blocks according to the prescriptions of the manufacturer (using prescribed burs
and taps). The applied torque for inserting the screws was measured to check whether
it was comparable to the clinically applied torque (‘hand tight’) defined in a previous
study (130). For the SonicWeld Rx system, the biodegradable pins were inserted into
the boreholes (after the use of prescribed burs) with the sonotrode. The biodegradable
polymers melted due to the ultra-sound vibrations of the sonotrode. Subsequently,
the biodegradable material flowed into the borehole and the pinhead fused with the
biodegradable plate. In both situations, the boreholes were irrigated with saline before
insertion of the screws/pins to simulate the in situ lubrication.
The two PMMA blocks, linked by the osteofixation device (1 plate and 4 screws/pins)
were stored in a water tank containing water of 37.2 degrees Celsius for 24 hours to
simulate the relaxation of biodegradable screws/pins at body temperature (111). The tests
were performed in another tank containing water at the same temperature to simulate
physiological conditions. The use of saline was omitted because of the associated
corrosion problems of the test set-up. Omitting the use of saline was expected not to be
of influence to the test results.
The plates and screws/pins were subjected to tensile, side bending, and torsion tests. The
tensile test was performed as a standard loading test (figure 1). Side bending tests were
performed to simulate an in vivo bi-lateral sagittal split osteotomy (BSSO) situation (figure
2). Torsion tests were performed to subject the osteofixation devices to high torque in
order to simulate the most unfavourable situation (figure 3). The 2 PMMA blocks, linked
by the osteofixation device, were mounted in a test machine (Zwick/Roell TC-FR2, 5TS.
D09, 2.5kN test machine. Force accuracy 0.2%, positioning accuracy 0.0001mm; Zwick/
Roell Nederland, Venlo, The Netherlands). Regarding the tensile tests, the 2 PMMA blocks,
and thus the osteofixation plate, were subjected to a tensile force with a constant speed
of 5 mm/min until fracture occurred (according to the standard ASTM D638M). For the
side bending test the 2 PMMA blocks were supported at their ends whereas the plates
were loaded in the centre of the construction with a constant speed of 30 mm/min (with
this speed the outer fibers were loaded as fast as the fibers of the osteofixation system in
Figure 1. Tensile test set-up
Figure 2. Side bending test set-up
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2
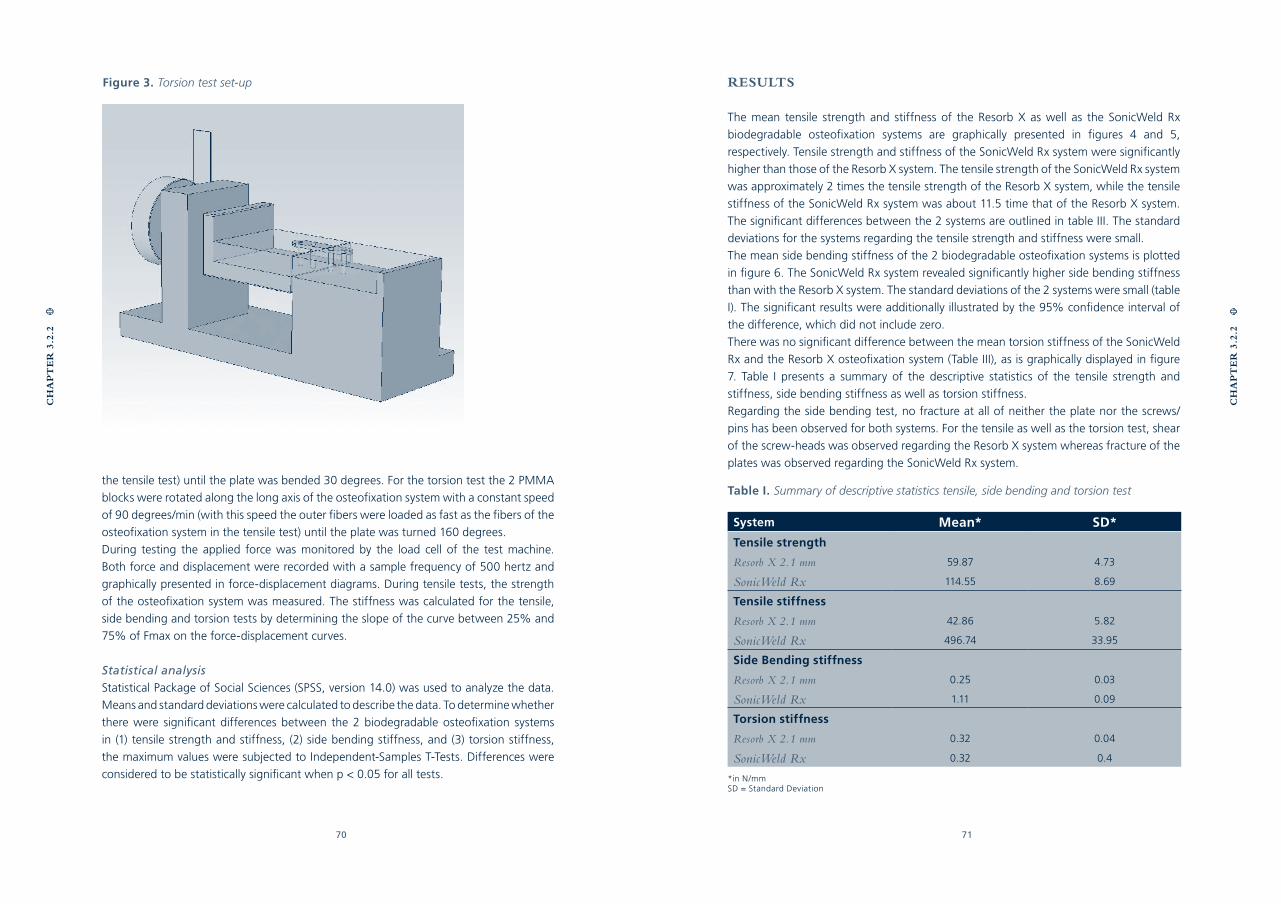
70 71
the tensile test) until the plate was bended 30 degrees. For the torsion test the 2 PMMA
blocks were rotated along the long axis of the osteofixation system with a constant speed
of 90 degrees/min (with this speed the outer fibers were loaded as fast as the fibers of the
osteofixation system in the tensile test) until the plate was turned 160 degrees.
During testing the applied force was monitored by the load cell of the test machine.
Both force and displacement were recorded with a sample frequency of 500 hertz and
graphically presented in force-displacement diagrams. During tensile tests, the strength
of the osteofixation system was measured. The stiffness was calculated for the tensile,
side bending and torsion tests by determining the slope of the curve between 25% and
75% of Fmax on the force-displacement curves.
Statistical analysis
Statistical Package of Social Sciences (SPSS, version 14.0) was used to analyze the data.
Means and standard deviations were calculated to describe the data. To determine whether
there were significant differences between the 2 biodegradable osteofixation systems
in (1) tensile strength and stiffness, (2) side bending stiffness, and (3) torsion stiffness,
the maximum values were subjected to Independent-Samples T-Tests. Differences were
considered to be statistically significant when p < 0.05 for all tests.
Figure 3. Torsion test set-up RESULTS
The mean tensile strength and stiffness of the Resorb X as well as the SonicWeld Rx
biodegradable osteofixation systems are graphically presented in figures 4 and 5,
respectively. Tensile strength and stiffness of the SonicWeld Rx system were significantly
higher than those of the Resorb X system. The tensile strength of the SonicWeld Rx system
was approximately 2 times the tensile strength of the Resorb X system, while the tensile
stiffness of the SonicWeld Rx system was about 11.5 time that of the Resorb X system.
The significant differences between the 2 systems are outlined in table III. The standard
deviations for the systems regarding the tensile strength and stiffness were small.
The mean side bending stiffness of the 2 biodegradable osteofixation systems is plotted
in figure 6. The SonicWeld Rx system revealed significantly higher side bending stiffness
than with the Resorb X system. The standard deviations of the 2 systems were small (table
I). The significant results were additionally illustrated by the 95% confidence interval of
the difference, which did not include zero.
There was no significant difference between the mean torsion stiffness of the SonicWeld
Rx and the Resorb X osteofixation system (Table III), as is graphically displayed in figure
7. Table I presents a summary of the descriptive statistics of the tensile strength and
stiffness, side bending stiffness as well as torsion stiffness.
Regarding the side bending test, no fracture at all of neither the plate nor the screws/
pins has been observed for both systems. For the tensile as well as the torsion test, shear
of the screw-heads was observed regarding the Resorb X system whereas fracture of the
plates was observed regarding the SonicWeld Rx system.
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2
Table I. Summary of descriptive statistics tensile, side bending and torsion test
System Mean* SD*
Tensile strength
Resorb X 2.1 mm 59.87 4.73
SonicWeld Rx 114.55 8.69
Tensile stiffness
Resorb X 2.1 mm 42.86 5.82
SonicWeld Rx 496.74 33.95
Side Bending stiffness
Resorb X 2.1 mm 0.25 0.03
SonicWeld Rx 1.11 0.09
Torsion stiffness
Resorb X 2.1 mm 0.32 0.04
SonicWeld Rx 0.32 0.4
*in N/mmSD = Standard Deviation
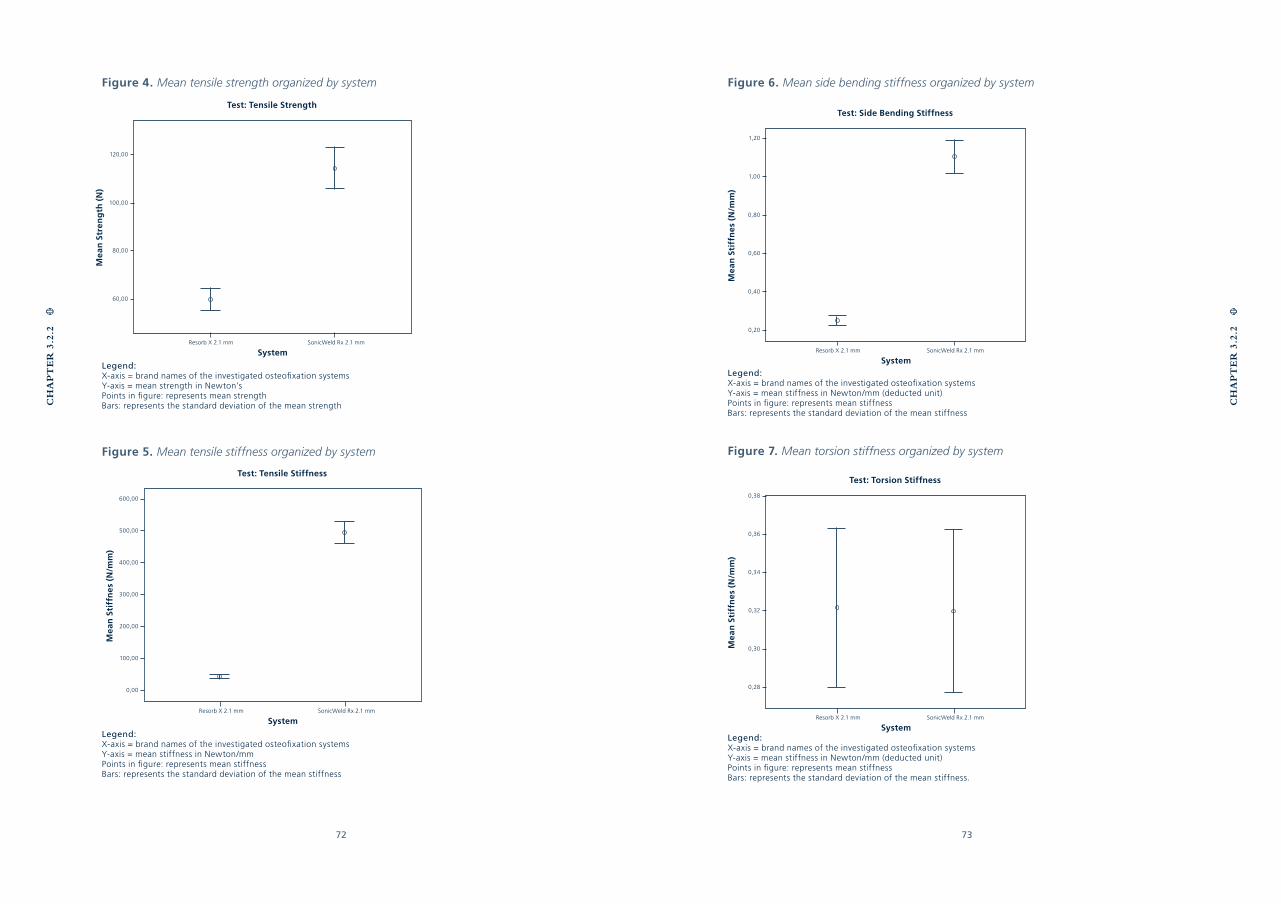
72 73
Figure 6. Mean side bending stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mm (deducted unit)Points in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness
Figure 7. Mean torsion stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mm (deducted unit)Points in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness.
Figure 4. Mean tensile strength organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean strength in Newton’sPoints in figure: represents mean strengthBars: represents the standard deviation of the mean strength
Figure 5. Mean tensile stiffness organized by system
Legend:X-axis = brand names of the investigated osteofixation systemsY-axis = mean stiffness in Newton/mmPoints in figure: represents mean stiffnessBars: represents the standard deviation of the mean stiffness
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2
System
120,00
100,00
80,00
60,00
Resorb X 2.1 mm SonicWeld Rx 2.1 mm
Mea
n S
tren
gth
(N
)Test: Tensile Strength
System
600,00
500,00
400,00
300,00
200,00
100,00
0,00
Resorb X 2.1 mm SonicWeld Rx 2.1 mm
Mea
n S
tiff
ne
s (N
/mm
)
Test: Tensile Stiffness
System
1,20
1,00
0,80
0,60
0,40
0,20
SonicWeld Rx 2.1 mm
Mea
n S
tiff
ne
s (N
/mm
)
Test: Side Bending Stiffness
Resorb X 2.1 mm
System
0,38
0,36
0,34
0,32
0,30
0,28
SonicWeld Rx 2.1 mm
Mea
n S
tiff
ne
s (N
/mm
)
Test: Torsion Stiffness
Resorb X 2.1 mm
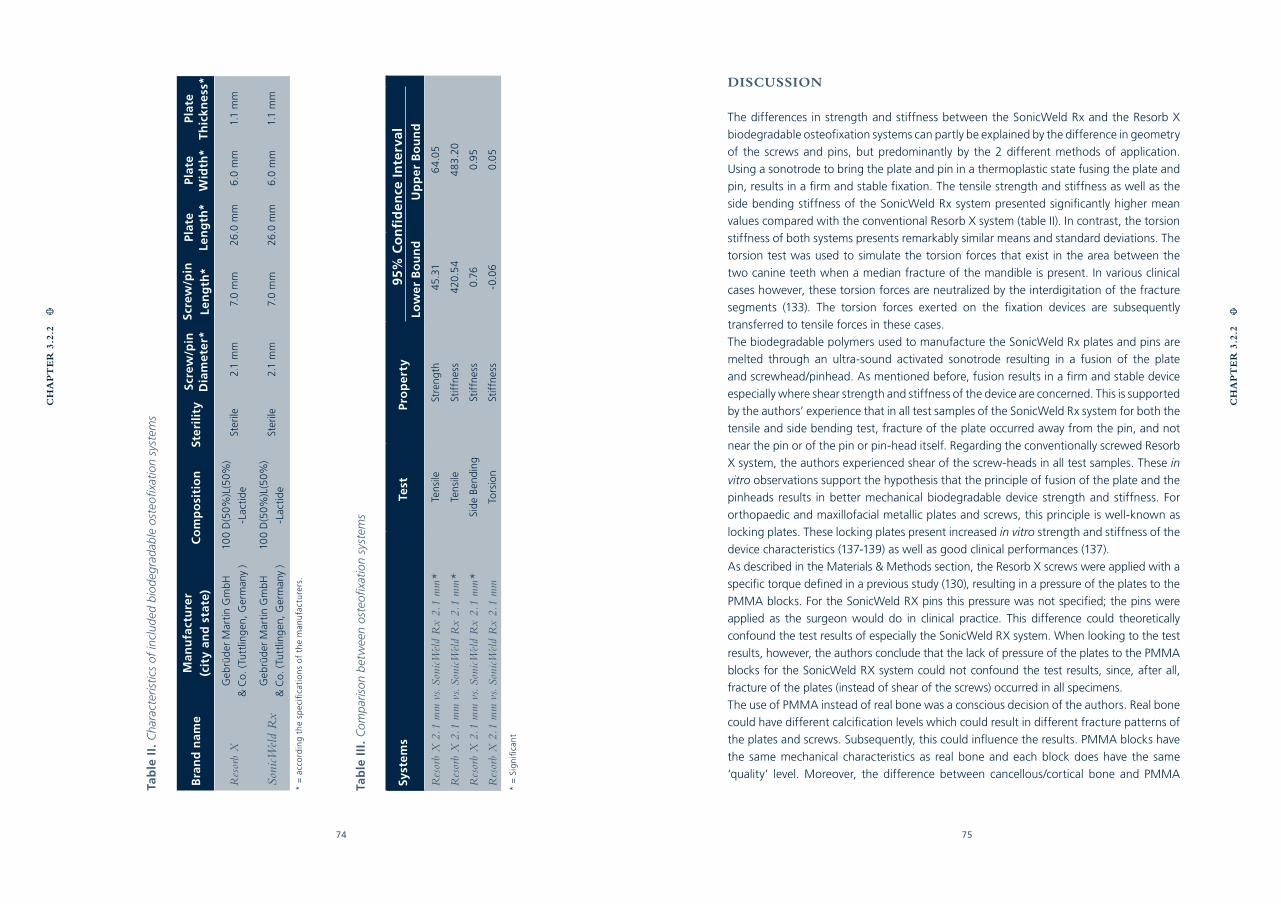
74 75
Tab
le I
II.
Com
par
ison
bet
wee
n os
teofi
xatio
n sy
stem
s
Syst
ems
Test
Pro
per
ty95
% C
on
fid
ence
In
terv
alLo
wer
Bo
un
dU
pp
er B
ou
nd
Res
orb
X 2
.1 m
m v
s. So
nicW
eld
Rx
2.1
mm
*Te
nsile
Stre
ngth
45.3
16
4.0
5
Res
orb
X 2
.1 m
m v
s. So
nicW
eld
Rx
2.1
mm
*Te
nsile
Stif
fnes
s42
0.5
44
83.
20
Res
orb
X 2
.1 m
m v
s. So
nicW
eld
Rx
2.1
mm
*Si
de
Ben
ding
Stif
fnes
s0.
760.
95
Res
orb
X 2
.1 m
m v
s. So
nicW
eld
Rx
2.1
mm
Tors
ion
Stif
fnes
s-0
.06
0.0
5
* =
Sig
nifi
can
t
Tab
le I
I. C
hara
cter
istic
s of
incl
uded
bio
degr
adab
le o
steo
fixat
ion
syst
ems
Bra
nd
nam
eM
anu
fact
ure
r (c
ity
and
sta
te)
Co
mp
osi
tio
nSt
eril
ity
Scre
w/p
inD
iam
eter
*Sc
rew
/pin
Len
gth
*Pl
ate
Len
gth
*Pl
ate
Wid
th*
Plat
eT
hic
kne
ss*
Res
orb
XG
ebrü
der
Mar
tin
Gm
bH
& C
o. (
Tutt
ling
en, G
erm
any
)
100
D(5
0%)L
(50%
)
-Lac
tid
eSt
erile
2.1
mm
7.0
mm
26.0
mm
6.0
mm
1.1
mm
Soni
cWel
d R
xG
ebrü
der
Mar
tin
Gm
bH
& C
o. (
Tutt
ling
en, G
erm
any
)
100
D(5
0%)L
(50%
)
-Lac
tid
eSt
erile
2.1
mm
7.0
mm
26.0
mm
6.0
mm
1.1
mm
* =
acc
ord
ing
th
e sp
ecifi
cati
on
s o
f th
e m
anu
fact
ure
rs.
DISCUSSION
The differences in strength and stiffness between the SonicWeld Rx and the Resorb X
biodegradable osteofixation systems can partly be explained by the difference in geometry
of the screws and pins, but predominantly by the 2 different methods of application.
Using a sonotrode to bring the plate and pin in a thermoplastic state fusing the plate and
pin, results in a firm and stable fixation. The tensile strength and stiffness as well as the
side bending stiffness of the SonicWeld Rx system presented significantly higher mean
values compared with the conventional Resorb X system (table II). In contrast, the torsion
stiffness of both systems presents remarkably similar means and standard deviations. The
torsion test was used to simulate the torsion forces that exist in the area between the
two canine teeth when a median fracture of the mandible is present. In various clinical
cases however, these torsion forces are neutralized by the interdigitation of the fracture
segments (133). The torsion forces exerted on the fixation devices are subsequently
transferred to tensile forces in these cases.
The biodegradable polymers used to manufacture the SonicWeld Rx plates and pins are
melted through an ultra-sound activated sonotrode resulting in a fusion of the plate
and screwhead/pinhead. As mentioned before, fusion results in a firm and stable device
especially where shear strength and stiffness of the device are concerned. This is supported
by the authors’ experience that in all test samples of the SonicWeld Rx system for both the
tensile and side bending test, fracture of the plate occurred away from the pin, and not
near the pin or of the pin or pin-head itself. Regarding the conventionally screwed Resorb
X system, the authors experienced shear of the screw-heads in all test samples. These in
vitro observations support the hypothesis that the principle of fusion of the plate and the
pinheads results in better mechanical biodegradable device strength and stiffness. For
orthopaedic and maxillofacial metallic plates and screws, this principle is well-known as
locking plates. These locking plates present increased in vitro strength and stiffness of the
device characteristics (137-139) as well as good clinical performances (137).
As described in the Materials & Methods section, the Resorb X screws were applied with a
specific torque defined in a previous study (130), resulting in a pressure of the plates to the
PMMA blocks. For the SonicWeld RX pins this pressure was not specified; the pins were
applied as the surgeon would do in clinical practice. This difference could theoretically
confound the test results of especially the SonicWeld RX system. When looking to the test
results, however, the authors conclude that the lack of pressure of the plates to the PMMA
blocks for the SonicWeld RX system could not confound the test results, since, after all,
fracture of the plates (instead of shear of the screws) occurred in all specimens.
The use of PMMA instead of real bone was a conscious decision of the authors. Real bone
could have different calcification levels which could result in different fracture patterns of
the plates and screws. Subsequently, this could influence the results. PMMA blocks have
the same mechanical characteristics as real bone and each block does have the same
‘quality’ level. Moreover, the difference between cancellous/cortical bone and PMMA
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2

76 77
was not a major concern. Theoretically, the flow of polymers of the ultra-sound activated
SonicWeld Rx pin into the cavities of the cancellous bone would enhance the pull out
strength of the screws. However, none of the screws were pulled out during testing.
Regarding the thermoplastic state of the biodegradable pin, we were concerned about the
fusion or sticking of the biodegradable pin to the PMMA blocks. This could theoretically
affect the test results. To prevent this, the boreholes were irrigated with saline before
insertion of the pins. To check whether fusion or sticking had occurred, we checked
whether the pin could be pulled out the PMMA blocks after the test. Despite not actually
measuring the pull out strength of the pins, the authors noted that high forces were not
required to do so.
The SonicWeld Rx system is obviously an improvement in the search for a mechanically
strong and stiff as well as a biodegradable osteofixation system. Moreover, usage of the
device is relatively easy and comfortable. The application of SonicWeld Rx plates and
pins is fast and easy. Nevertheless, the plates and screws are still bulky compared to the
conventional titanium plates and screws. The question, though, is whether the promising
in vitro results can be transferred to the in situ clinical situation. Future research about
biodegradable osteofixation devices should therefore include the SonicWeld Rx system
in randomized clinical trials in which a conventional titanium fixation device serves as the
´golden´ standard fixation device.
Acknowledgements
The gratuitously supply of the biodegradable plates and screws/pins through the
manufacturer (Gebrüder Martin GmbH & Co.) was gratefully appreciated. The authors
also would like to thank dr. H. Groen for his statistical assistance. Mr. J. de Jonge is
acknowledged for the fabrication of the test set-ups.
CH
AP
TE
R 3
.2.2
CH
AP
TE
R 3
.2.2
CHAPTER 4
BIODEGRADABLE AND
TITANIUM FIXATION SYSTEMS
IN ORAL AND MAXILLOFACIAL
SURGERY: A RANDOMIZED
CONTROLLED TRIAL
G.J. BUIJS
N.B. VAN BAKELEN
J. JANSMA
J.G.A.M. DE VISSCHER
TH.J.M. HOPPENREIJS
J.E. BERGSMA
B. STEGENGA
R.R.M. BOS
Submitted
80 81
CH
AP
TE
R 4
Abstract:
Background - Metallic plates and screws are used for immobilization of bone fragments
in trauma and orthognathic surgery. Some authors advocate the removal of metallic
plates and screws because of potential adverse reactions. A second operation to remove
osteosynthesis following bone healing is reported in 5 - 40% of the cases. This is highly
undesirable in terms of cost-effectiveness, patient comfort, healthcare quality and risk of
complications. Biodegradable fixation systems could reduce or even delete the problems
associated with metallic systems since removal is not necessary.
Aim - The aim of this study was to establish the effectiveness and safety of biodegrad-
able plates and screws as a potential alternative to metallic ones.
Materials & Methods - This multi-centre randomized controlled trial was conducted
from December 2006 to July 2009. Included were patients who underwent mandibular-
and Le Fort I osteotomies and those with fractures of the mandible, maxilla, and zygoma.
The patients were assigned to a titanium control-group (KLS Martin) or to a biodegrad-
able test-group (Inion CPS). The primary outcome measure was ‘bone healing 8 weeks
after surgery’.
Results - The Intention To Treat analysis (ITT) of 111 patients in the titanium group and
112 patients in the biodegradable group yielded a non-significant difference. In 25 pa-
tients (22%) who were included in the biodegradable group, the surgeon made the deci-
sion to switch to the titanium system per-operatively.
Conclusion & discussion - Despite the ‘non inferior’ primary outcome result, the ben-
efits of using biodegradable systems (less plate removal operations) should be demon-
strated during a follow-up of minimally 5 years, especially when the large number of pa-
tients for whom it was per-operatively decided to switch from the biodegradable system
to the conventional titanium system, are taken into account.
INTRODUCTION
Essential prerequisites for the bone healing of fractures and osteotomies include sufficient
vascularization, anatomical reduction, and immobilization of bone segments (7;10). Up to
the seventies, fractures and osteotomies were fixed with (stainless) steel wires supported
by InterMaxillary Fixation (IMF) to achieve bone healing and restore occlusion. The use of
IMF during the healing period of 6 weeks is very uncomfortable. Besides, it immobilizes the
temporomandibular joints resulting in cartilage degeneration (140). The last four decades,
immobilization of bone fragments can be obtained using metallic plates and screws without
applying IMF (125;126). This allows patients to load functionally their masticatory system
immediately following surgery. The currently available metal plating systems have the
advantage of combining excellent mechanical and handling properties. A disadvantage of
the use of metallic plates and screws is that they remain during life. This results in several
potential adverse effects such as: (1) sensitivity to hot and cold stimuli (129), (2) palpability
of the plates, (3) possible growth disturbance or mutagenic effects (37;41;43-45), and
(4) interference with imaging or radio-therapeutic irradiation techniques (37;41;127).
As a consequence, some authors remove the implants in a second operation following
bone healing. This has been reported in 5 - 40% of the cases (32-34). Because of this
apparent disadvantage, there is a continuous drive to explore the use of biodegradable
fixation systems (4). These systems could reduce or even delete the problems associated
with metallic systems (74). This would be highly desirable from the viewpoint of cost-
effectiveness, patient comfort, healthcare quality, and risk of complications due to plate
removal. However, adverse tissue reactions to degradation products have been reported
(66;67;100;114). Moreover, biodegradable systems are mechanically less favourable than
metallic systems, which can result in insufficient bone healing.
Many case reports and case series have been published reporting the clinical performance
of a variety of commercially available biodegradable systems used for different indications.
These studies show various outcome results (48;64;70;141-143). Only a few controlled trials
have been published on this subject (2-4;144), which have previously been summarized
and analyzed in a systematic review (122). The results were inconclusive, mainly because
of the lack of sufficiently powered and appropriately designed trials and heterogeneity
among the included studies. Given the lack of adequate evidence as well as the obvious
advantages of using biodegradable plates and screws for the patient, and society, there is
a need for well-designed randomized controlled trials of sufficient size.
The aim of this study was to establish the effectiveness and safety of biodegradable plates
and screws as an alternative to metallic ones. Therefore, we tested the null-hypothesis
that the performance of the Inion CPS biodegradable system is inferior to the titanium
system regarding bone healing following treatment of mandibular, maxillary (Le Fort I),
and zygomatic fractures as well as after bi-lateral sagittal split (BSO) and/or Le Fort I
osteotomies.
CH
AP
TE
R 4
82 83
MATERIALS & METHODS
Patients
This prospective study was conducted from December 2006 to July 2009. The source
population consisted of patients who were treated at the departments of Oral and
Maxillofacial Surgery (OMFS) of the:
1. University Medical Centre Groningen (UMCG)
2. Rijnstate Hospital Arnhem (RHA)
3. Amphia Hospital Breda (AHB)
4. Medical Centre Leeuwarden (MCL).
Patients meeting the inclusion criteria were eligible for this study (Figure 1). All patients
were informed regarding the treatment options prior to surgery and were required to
provide informed consent in order to participate in the study. The surgeons recruited the
participants and subsequently assigned them randomly to two treatment groups a day
before (in case of osteotomies) or immediately prior to (in case of fractures) the operation.
A statistician generated the randomization sequences using a computerized randomization
Inclusion criteria:
- patients scheduled for a Le Fort I fracture, and/or a solitary or multiple (maximum 2)
mandibular fracture(s), and/or a zygoma fracture;
- patients scheduled for a Le Fort I osteotomy, and/or a Bi-lateral Sagittal Split
Osteotomy (BSO);
- patients (also parents or responsible persons if necessary) who signed the informed
consent form.
Exclusion criteria:
- patients who were younger than 18 years old (trauma), or patients who were younger
than 14 years (osteotomies);
- patients presented with heavily comminuted fractures of the facial skeleton;
- patients who experienced compromised bone healing in the past;
- patients who were pregnant;
- patients who could/would not participate in a 1-year follow-up (reasons);
- patients who would not agree with an at random assignment to one of the treatment
groups, or one of the methods or treatment administered in the study;
- patients who were diagnosed with a psychiatric disorder (diagnosed by a psychiatrist);
- patients who experienced cleft lip and palate surgery in the past;
- patients where fracture reduction and fixation was delayed for more than 7 days (after
day of trauma);
- patients of whom the general health and/or medication could affect bone healing, as
determined by the oral and maxillofacial surgeon.
Figure 1. In- and exclusion criteria
program. The randomization sequences were linked to a central telephone, which was
available 24-hours a day to conceal the sequence until the interventions were assigned.
Stratification to hospital was executed in order to detect hospital effects. The study was
approved by the Medical Ethical Committee (MEC) of the UMCG, and approved for local
workability by the MEC’s of the other centres.
Interventions
The patients were assigned to a titanium control-group (KLS Martin, Gebrüder Martin
GmbH & Co. Tuttlingen, Germany) or to a biodegradable test-group (Inion CPS, Inion
Ltd. Tampere, Finland). Neither prior to nor after surgery, the patients were aware of the
system that had been used.
All plates and screws were applied according to the instructions of the manufactures (with
prescribed burs and taps). The screw holes were predrilled for both the titanium as for
the biodegradable screws, and subsequently pre-tapped for the biodegradable screws.
For fixation of mandibular osteotomies and fractures 2.5-mm biodegradable or 2.0-
mm titanium plates and screws were used, whereas 2.0-mm biodegradable or 1.5-mm
titanium plates and screws were used for fixation of zygoma fractures, Le Fort I fractures,
and Le Fort I osteotomies. Each participating OMF surgeon performed 2 ‘test-surgeries’
using the biodegradable system in order to acquire the slightly different application-skills,
i.e., pre-tapping the screws and pre-heating the plates, and to get used to the different
dimensions. These ‘test-surgeries’ were not included in the study.
Outcome measures
The primary outcome measure was ‘bone healing 8 weeks after surgery’, which was
defined as follows:
1. absence of clinical mobility of the bone segments assessed using bi-manual traction on
the distal and proximal bone segments;
2. absence of radiographic signs of disturbed bone healing assessed on an orthopanto-
mogram (OPT; all indications), a lateral cephalogram (osteotomies), an occipito-mental-
radiograph (zygoma fractures), and a fronto-suboccipital radiograph (mandible fracture).
The following secondary outcome measures were assessed:
1. clinical: occlusion, palpability of plate/screw, wound dehiscence, and signs of inflammation;
2. radiographic: position of the bone segments (position of teeth, path of the mandibular
canal, and contour of cortical structures);
3. patient-related (by self-evaluation): pain reported on a Visual Analogue Scale (VAS;
ranging 1-100) and mandibular function evaluated by the mandibular function impair-
ment questionnaire (MFIQ (145); ranging 17-85);
4. handling characteristics (plate adaptation, drilling/tapping, screw insertion, and wound
closure recorded on a scale of 1-10).
5. cost-effectiveness: direct (hospital, surgeon, and time related) and indirect (discontinu-
ing employment process) costs were reported on a questionnaire.
CH
AP
TE
R 4
CH
AP
TE
R 4
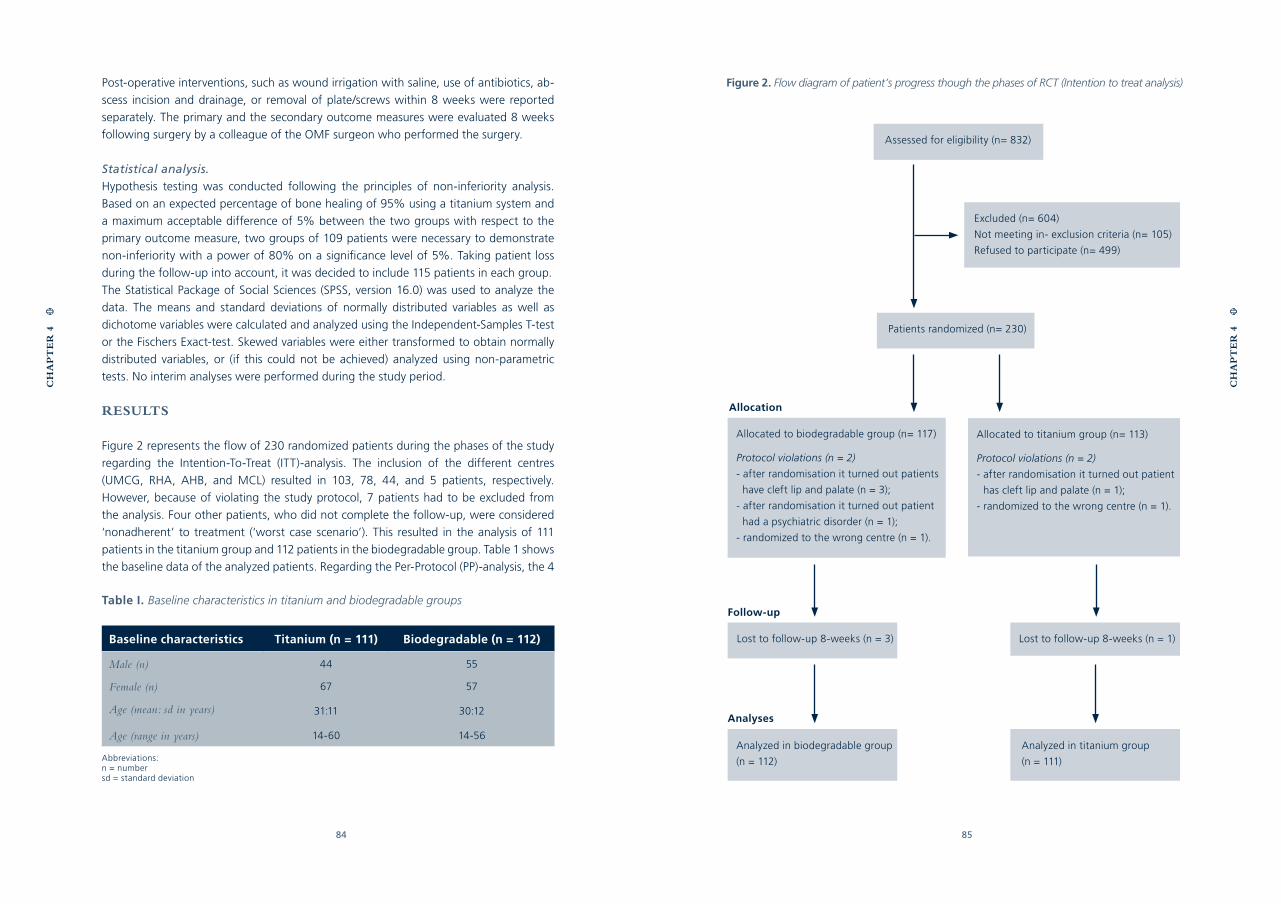
84 85
Post-operative interventions, such as wound irrigation with saline, use of antibiotics, ab-
scess incision and drainage, or removal of plate/screws within 8 weeks were reported
separately. The primary and the secondary outcome measures were evaluated 8 weeks
following surgery by a colleague of the OMF surgeon who performed the surgery.
Statistical analysis.
Hypothesis testing was conducted following the principles of non-inferiority analysis.
Based on an expected percentage of bone healing of 95% using a titanium system and
a maximum acceptable difference of 5% between the two groups with respect to the
primary outcome measure, two groups of 109 patients were necessary to demonstrate
non-inferiority with a power of 80% on a significance level of 5%. Taking patient loss
during the follow-up into account, it was decided to include 115 patients in each group.
The Statistical Package of Social Sciences (SPSS, version 16.0) was used to analyze the
data. The means and standard deviations of normally distributed variables as well as
dichotome variables were calculated and analyzed using the Independent-Samples T-test
or the Fischers Exact-test. Skewed variables were either transformed to obtain normally
distributed variables, or (if this could not be achieved) analyzed using non-parametric
tests. No interim analyses were performed during the study period.
RESULTS
Figure 2 represents the flow of 230 randomized patients during the phases of the study
regarding the Intention-To-Treat (ITT)-analysis. The inclusion of the different centres
(UMCG, RHA, AHB, and MCL) resulted in 103, 78, 44, and 5 patients, respectively.
However, because of violating the study protocol, 7 patients had to be excluded from
the analysis. Four other patients, who did not complete the follow-up, were considered
‘nonadherent’ to treatment (‘worst case scenario’). This resulted in the analysis of 111
patients in the titanium group and 112 patients in the biodegradable group. Table 1 shows
the baseline data of the analyzed patients. Regarding the Per-Protocol (PP)-analysis, the 4
Allocation
Analyzed in biodegradable group
(n = 112)
Analyzed in titanium group
(n = 111)
Allocated to biodegradable group (n= 117)
Protocol violations (n = 2)
- after randomisation it turned out patients
have cleft lip and palate (n = 3);
- after randomisation it turned out patient
had a psychiatric disorder (n = 1);
- randomized to the wrong centre (n = 1).
Excluded (n= 604)
Not meeting in- exclusion criteria (n= 105)
Refused to participate (n= 499)
Lost to follow-up 8-weeks (n = 3)
Patients randomized (n= 230)
Lost to follow-up 8-weeks (n = 1)
Allocated to titanium group (n= 113)
Protocol violations (n = 2)
- after randomisation it turned out patient
has cleft lip and palate (n = 1);
- randomized to the wrong centre (n = 1).
Assessed for eligibility (n= 832)
Follow-up
Analyses
Figure 2. Flow diagram of patient’s progress though the phases of RCT (Intention to treat analysis)
CH
AP
TE
R 4
CH
AP
TE
R 4
Table I. Baseline characteristics in titanium and biodegradable groups
Baseline characteristics Titanium (n = 111) Biodegradable (n = 112)
Male (n) 44 55
Female (n) 67 57
Age (mean: sd in years) 31:11 30:12
Age (range in years) 14-60 14-56
Abbreviations:n = numbersd = standard deviation
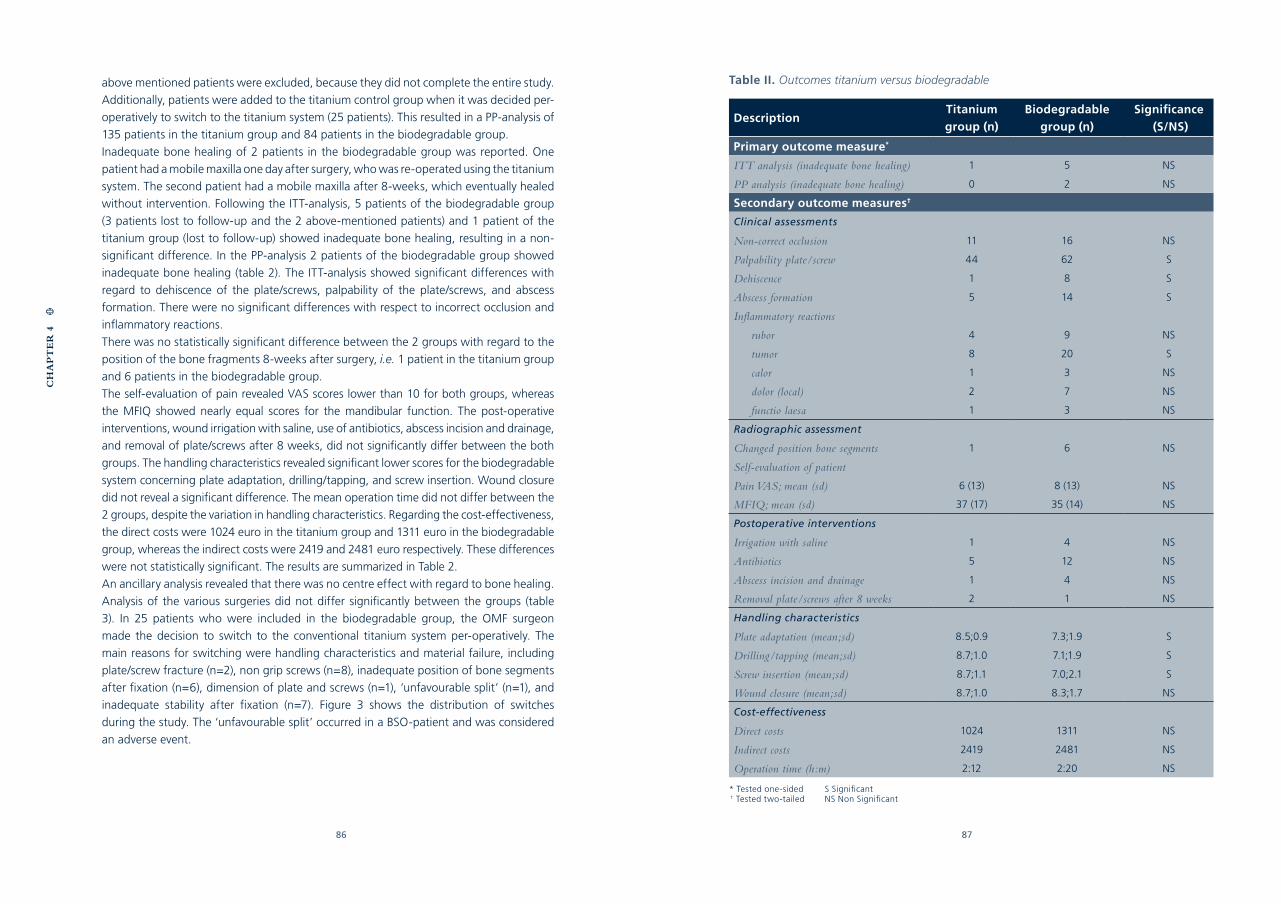
86 87
above mentioned patients were excluded, because they did not complete the entire study.
Additionally, patients were added to the titanium control group when it was decided per-
operatively to switch to the titanium system (25 patients). This resulted in a PP-analysis of
135 patients in the titanium group and 84 patients in the biodegradable group.
Inadequate bone healing of 2 patients in the biodegradable group was reported. One
patient had a mobile maxilla one day after surgery, who was re-operated using the titanium
system. The second patient had a mobile maxilla after 8-weeks, which eventually healed
without intervention. Following the ITT-analysis, 5 patients of the biodegradable group
(3 patients lost to follow-up and the 2 above-mentioned patients) and 1 patient of the
titanium group (lost to follow-up) showed inadequate bone healing, resulting in a non-
significant difference. In the PP-analysis 2 patients of the biodegradable group showed
inadequate bone healing (table 2). The ITT-analysis showed significant differences with
regard to dehiscence of the plate/screws, palpability of the plate/screws, and abscess
formation. There were no significant differences with respect to incorrect occlusion and
inflammatory reactions.
There was no statistically significant difference between the 2 groups with regard to the
position of the bone fragments 8-weeks after surgery, i.e. 1 patient in the titanium group
and 6 patients in the biodegradable group.
The self-evaluation of pain revealed VAS scores lower than 10 for both groups, whereas
the MFIQ showed nearly equal scores for the mandibular function. The post-operative
interventions, wound irrigation with saline, use of antibiotics, abscess incision and drainage,
and removal of plate/screws after 8 weeks, did not significantly differ between the both
groups. The handling characteristics revealed significant lower scores for the biodegradable
system concerning plate adaptation, drilling/tapping, and screw insertion. Wound closure
did not reveal a significant difference. The mean operation time did not differ between the
2 groups, despite the variation in handling characteristics. Regarding the cost-effectiveness,
the direct costs were 1024 euro in the titanium group and 1311 euro in the biodegradable
group, whereas the indirect costs were 2419 and 2481 euro respectively. These differences
were not statistically significant. The results are summarized in Table 2.
An ancillary analysis revealed that there was no centre effect with regard to bone healing.
Analysis of the various surgeries did not differ significantly between the groups (table
3). In 25 patients who were included in the biodegradable group, the OMF surgeon
made the decision to switch to the conventional titanium system per-operatively. The
main reasons for switching were handling characteristics and material failure, including
plate/screw fracture (n=2), non grip screws (n=8), inadequate position of bone segments
after fixation (n=6), dimension of plate and screws (n=1), ‘unfavourable split’ (n=1), and
inadequate stability after fixation (n=7). Figure 3 shows the distribution of switches
during the study. The ‘unfavourable split’ occurred in a BSO-patient and was considered
an adverse event.
CH
AP
TE
R 4
Table II. Outcomes titanium versus biodegradable
DescriptionTitanium group (n)
Biodegradable group (n)
Significance (S/NS)
Primary outcome measure*
ITT analysis (inadequate bone healing) 1 5 NS
PP analysis (inadequate bone healing) 0 2 NS
Secondary outcome measures†
Clinical assessments
Non-correct occlusion 11 16 NS
Palpability plate/screw 44 62 S
Dehiscence 1 8 S
Abscess formation 5 14 S
Inflammatory reactions
rubor 4 9 NS
tumor 8 20 S
calor 1 3 NS
dolor (local) 2 7 NS
functio laesa 1 3 NS
Radiographic assessment
Changed position bone segments 1 6 NS
Self-evaluation of patient
Pain VAS; mean (sd) 6 (13) 8 (13) NS
MFIQ; mean (sd) 37 (17) 35 (14) NS
Postoperative interventions
Irrigation with saline 1 4 NS
Antibiotics 5 12 NS
Abscess incision and drainage 1 4 NS
Removal plate/screws after 8 weeks 2 1 NS
Handling characteristics
Plate adaptation (mean;sd) 8.5;0.9 7.3;1.9 S
Drilling/tapping (mean;sd) 8.7;1.0 7.1;1.9 S
Screw insertion (mean;sd) 8.7;1.1 7.0;2.1 S
Wound closure (mean;sd) 8.7;1.0 8.3;1.7 NS
Cost-effectiveness
Direct costs 1024 1311 NS
Indirect costs 2419 2481 NS
Operation time (h:m) 2:12 2:20 NS
* Tested one-sided S Significant † Tested two-tailed NS Non Significant
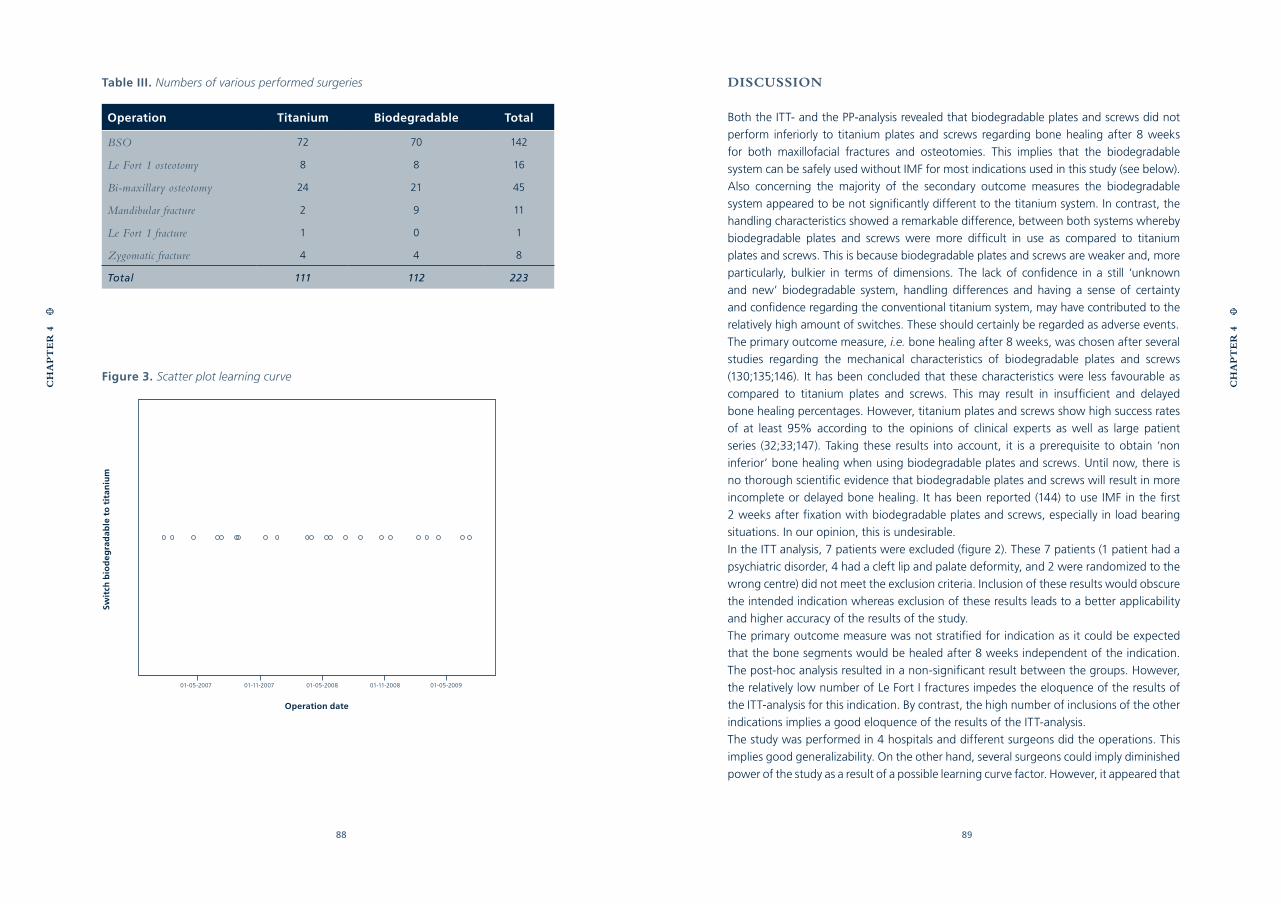
88 89
Table III. Numbers of various performed surgeries
Operation Titanium Biodegradable Total
BSO 72 70 142
Le Fort 1 osteotomy 8 8 16
Bi-maxillary osteotomy 24 21 45
Mandibular fracture 2 9 11
Le Fort 1 fracture 1 0 1
Zygomatic fracture 4 4 8
Total 111 112 223
DISCUSSION
Both the ITT- and the PP-analysis revealed that biodegradable plates and screws did not
perform inferiorly to titanium plates and screws regarding bone healing after 8 weeks
for both maxillofacial fractures and osteotomies. This implies that the biodegradable
system can be safely used without IMF for most indications used in this study (see below).
Also concerning the majority of the secondary outcome measures the biodegradable
system appeared to be not significantly different to the titanium system. In contrast, the
handling characteristics showed a remarkable difference, between both systems whereby
biodegradable plates and screws were more difficult in use as compared to titanium
plates and screws. This is because biodegradable plates and screws are weaker and, more
particularly, bulkier in terms of dimensions. The lack of confidence in a still ‘unknown
and new’ biodegradable system, handling differences and having a sense of certainty
and confidence regarding the conventional titanium system, may have contributed to the
relatively high amount of switches. These should certainly be regarded as adverse events.
The primary outcome measure, i.e. bone healing after 8 weeks, was chosen after several
studies regarding the mechanical characteristics of biodegradable plates and screws
(130;135;146). It has been concluded that these characteristics were less favourable as
compared to titanium plates and screws. This may result in insufficient and delayed
bone healing percentages. However, titanium plates and screws show high success rates
of at least 95% according to the opinions of clinical experts as well as large patient
series (32;33;147). Taking these results into account, it is a prerequisite to obtain ‘non
inferior’ bone healing when using biodegradable plates and screws. Until now, there is
no thorough scientific evidence that biodegradable plates and screws will result in more
incomplete or delayed bone healing. It has been reported (144) to use IMF in the first
2 weeks after fixation with biodegradable plates and screws, especially in load bearing
situations. In our opinion, this is undesirable.
In the ITT analysis, 7 patients were excluded (figure 2). These 7 patients (1 patient had a
psychiatric disorder, 4 had a cleft lip and palate deformity, and 2 were randomized to the
wrong centre) did not meet the exclusion criteria. Inclusion of these results would obscure
the intended indication whereas exclusion of these results leads to a better applicability
and higher accuracy of the results of the study.
The primary outcome measure was not stratified for indication as it could be expected
that the bone segments would be healed after 8 weeks independent of the indication.
The post-hoc analysis resulted in a non-significant result between the groups. However,
the relatively low number of Le Fort I fractures impedes the eloquence of the results of
the ITT-analysis for this indication. By contrast, the high number of inclusions of the other
indications implies a good eloquence of the results of the ITT-analysis.
The study was performed in 4 hospitals and different surgeons did the operations. This
implies good generalizability. On the other hand, several surgeons could imply diminished
power of the study as a result of a possible learning curve factor. However, it appeared that
CH
AP
TE
R 4
CH
AP
TE
R 4
Figure 3. Scatter plot learning curve
Operation date
Swit
ch b
iod
eg
rad
able
to
tit
aniu
m
01-05-2007 01-11-2007 01-05-2008 01-11-2008 01-05-2009

90 91
the switches of the biodegradable to the titanium system took place over the entire study
(figure 3). Moreover, the switches were made by all participating surgeons and centres. It
can therefore be expected that the performance of the Inion CPS biodegradable system
in other hospitals will not be inferior to the conventional titanium system.
In the materials and methods section it is stated that evaluation of outcome measures
was planned to be) performed by a colleague of the OMF surgeon who performed the
surgery. Despite the intended protocol, in too many cases it turned out to be practically
unfeasible to perform the evaluation of the outcome measures by a different OMF
surgeon than the OMF surgeon who performed the surgery. This phenomenon may have
introduced observer bias.
In summary, it is concluded that regarding bone healing after 8 weeks, the performance
of the Inion CPS biodegradable system is not inferior compared to the titanium system
regarding the treatment of mandibular-, and zygoma fractures as well as for BSO-,
and Le Fort I osteotomies. However, despite the ‘non inferior’ primary outcome result,
the benefits of using biodegradable systems (less plate removal operations) should be
demonstrated during a follow-up of minimally 5 years, especially when the large number
of patients for whom it was per-operatively decided to switch from the biodegradable
system to the conventional titanium system, are taken into account. The presented results
are part of a longer running follow-up study and the one year results will be published
in the near future.
ACKNOWLEDGEMENT
The authors thank the Stryker company for their support and the supply of the Inion CPS
product.
CH
AP
TE
R 4
CH
AP
TE
R 4
CHAPTER 5
GENERAL DISCUSSION
AND FUTURE PERSPECTIVES
94 95
GENERAL DISCUSSION
Titanium plates and screws are currently regarded as the gold standard for fixation of
bone fragments in the maxillofacial skeleton. As with any material, there are aspects that
are undesirable and should be improved to meet the ideal characteristics for fixation.
From the point of view of an ideal fixation system, there is a continuous drive to create a
fixation system that disappears from the human body without any residues as soon as it
has fulfilled its function, i.e. undisturbed healing of the bone segments. As stated in the
introduction of this thesis, biodegradable plates and screws could be a suitable material
as they dissolve in the human body.
The known pros and cons of both titanium and biodegradable plates and screws are
described in detail in the introduction. In this thesis, a systematic review was performed
to investigate the clinical efficacy and safety of biodegradable plates and screws.
Subsequently, in vitro studies were performed to establish the mechanical properties
of biodegradable plates and screws. Finally, a clinical trial was performed in order to
establish whether these plates and screws could be used safely and effectively to a large-
scale and fit into the current treatment protocols and guidelines in maxillofacial surgery.
Clinical, patient-related, surgeon-related, and cost aspects were taken into account.
Based on a systematic review of literature (122) regarding the clinical efficacy and safety of
titanium and biodegradable plates and screws, a definitive conclusion regarding the fixa-
tion of fractured bone segments and osteotomies with respect to their long-term perform-
ance in maxillofacial surgery could not be drawn. Lack of sufficiently powered, high quality
and appropriately reported (randomized) controlled clinical trials are the main reasons.
Moreover, the application of biodegradable plates and screws for mandibular fractures
and osteotomies without using IMF has not been thoroughly investigated.
The mechanical properties of biodegradable plates and screws appeared to have
less favourable strength and stiffness compared with titanium plates and screws
(130;135;146). These lower strength and stiffness values apply for the functional unit
characteristics, plate and screws together, as well as for the torsion characteristics of the
screws. Despite the inferior mechanical characteristics, the above-mentioned review (122)
presented uneventful clinical case series using biodegradable fixation devices. This raises
the question as to whether the effectiveness and safety of biodegradable plates and
screws will be at least non-inferior to the high success rates (more than 95%) of titanium
plates and screws in large patient series. Adequately powered randomized controlled
trials needed to be conducted to draw definitive conclusions regarding the effectiveness
and safety of biodegradable plates and screws for bone healing in maxillofacial surgery.
The manufacturers of biodegradable plates and screws increased the dimensions to
compensate for the inferior mechanical characteristics. The dimensions of the LactoSorb
CH
AP
TE
R 5
CH
AP
TE
R 5
system are relatively bulky compared with the subtle dimensions of the Inion CPS and
BioSorb FX biodegradable systems. It has been concluded that these bulky dimensions
are responsible for the relatively good mechanical properties of the LactoSorb system
(130;135). As the dimensions of biodegradable plates and screws are larger compared
to titanium devices, it was not desirable to include the relatively bulky plates and screws
of the LactoSorb system in the RCT. The manufacturers of the BioSorb FX system used
a special self-reinforment principle to enhance the mechanical characteristics in order to
keep the dimensions within acceptable limits.
The application of biodegradable plates and screws is commonly limited to upper- and
midface fractures and osteotomies. Most manufacturers discourage the use in the mandible
unless in conjunction with 6 weeks of IMF. The use of IMF would be a step back in history.
Inion Ltd. is the only exception and can be used to fixate fractures and osteotomies of the
mandible according to the manufacturer. IMF should additionally support the fixation only
in complex or comminuted cases. As the inclusion- and exclusion criteria of the RCT resulted
in exclusion of these cases, and the regular mandibular fractures and osteotomies could be
stabilized without using IMF, Inion CPS plates and screws were chosen to use in the RCT.
Little data were available for the Inion CPS plates and screws as the material was relatively
new onto the market. After contacting the manufacturer of the Inion CPS system, we
received the proof of an article of Nieminen et. al. published later in 2008 (148). The
authors investigated the tissue reactions and mechanical strength of the Inion CPS plates
and screws during the course of degradation. The materials were implanted to the mandible
and in the dorsal subcutis of 12 sheep. The animals were sacrificed at 6-156 weeks. In light
microscopy, the in vivo implant material began to fragment at 52 weeks and could not be
detected at 104 weeks. No significant foreign body reactions were seen in the mandibles.
The dorsal subcutis disclosed mild reactions which were not of clinical significance. These
findings suggest that Inion CPS plates can be used safely for fixation of the bony structures
in the maxillofacial skeleton. Definitive proof of full degradation and resorption is still
lacking, as it is for all biodegradable systems investigated in this thesis.
In order to accomplish the main aim of this thesis, ‘to establish the effectiveness and
safety of biodegradable plates and screws to fix bone segments in the maxillofacial
skeleton as a potential alternative to metallic ones’, the clinical aspects were investigated
in a randomized controlled clinical trial using the Inion CPS biodegradable fixation
system (Buijs et. al, submitted). The Intention To Treat analysis (ITT-analysis) and the Per
Protocol analysis (PP-analysis) yielded that Inion CPS biodegradable plates and screws
did not perform inferiorly to titanium plates and screws regarding bone healing after 8
weeks for maxillofacial fractures (except for Le Fort I fractures) as well as osteotomies.
This implies that the biodegradable system can be safely used without IMF, also for load
bearing situations like bilateral sagittal spit osteotomies and non-comminuted mandibular
fractures. Also regarding the secondary outcome measures, it can be concluded that
there are no important differences between the two investigated systems.
96 97
In contrast, the handling characteristics showed a remarkable difference, indicating
that biodegradable plates and screws performed significantly less compared to titanium
plates and screws. This is because biodegradable plates and screws are weaker and, more
particularly, bulkier in terms of dimensions. These large dimensions remain a problem,
especially in the small and subtle areas of the midface where thin bones are present. The
large dimensions as well as the inferior mechanical characteristics are the main reasons
for the high amount (22%) of peri-operative switches from biodegradable to titanium
plates and screws.
Besides the clinical aspects, the costs were also evaluated. It can be concluded that
there is no significant difference between the Inion CPS biodegradable and the titanium
plates and screws. The application of the biodegradable plates is slightly more expensive
compared to titanium ones. However, productivity losses of people are the main costs.
Following a post-operative period of 1 year, or perhaps even longer, one could draw
definitive conclusions regarding the cost-effectiveness of the biodegradable plates and
screws and whether the potential advantages of biodegradable plates and screws could
be ‘confirmed’. Patient’s potential productivity gains could resolve the negative aspects
of the per-operative switches of biodegradable plates and screws.
The skeletal stability of the bone segments is an important variable which is evaluated
in the RCT by assessing the dental occlusion and the positional change of the bone
segments. During the 8-weeks follow-up the main focus was on bone healing (primary
outcome measure). The skeletal stability will be evaluated after 1 year follow up. Skeletal
structures may change especially during the first postoperative year (relapse; postoperative
orthodontics). After 1 year the skeletal structures will be more reliable making complete
effect size measurement of the skeletal stability possible.
It is generally accepted that the strength and stiffness of different titanium plates and
screws are comparable. This is also applicable for biocompatibility as is investigated in
the study of Langford in 2002 (149). In this way, it can be concluded that the KLS Martin
titanium system, which is used in the RCT, has a good generalizability for other titanium
systems. Regarding the Inion CPS biodegradable system, the generalizability of the
mechanical aspects is limited to the BioSorb FX, and LactoSorb. These systems represent
comparable mechanical characteristics (135). The other biodegradable systems investigated
in the study, performed significantly inferior. With respect to the biocompatibility, the
generalizability of Inion CPS plates and screws is difficult as a result of the various co-
polymer compositions used to manufacture the different biodegradable plates and screws.
Although many studies report promising results, ultimate biocompatibility and complete
resorption has never been proven. It can be concluded that the results of the randomized
controlled trial can be extrapolated to at least 2 of the investigated biodegradable plate
and screw systems (BioSorb FX and LactoSorb).
Based on the results of the RCT performed in this thesis, it is concluded that biodegradable
CH
AP
TE
R 5
plates and screws do not perform inferior to titanium regarding a follow-up period of
8 weeks. The high percentage of switches is a threat to a widespread acceptation of
biodegradable plates and screws in the current treatment protocols and guidelines in
maxillofacial surgery. The follow-up period of 1 year will provide more clarity about
the potential differences in plate removal operations and thus the potential gain in
effectiveness in the treatment of fractures and osteotomies of the maxillofacial skeleton.
The 1 year follow up results will also provide more information about the skeletal stability,
biocompatibility, and resorption aspects of Inion CPS plates and screws. Further research
is performed and will be published in the near future.
FUTURE PERSPECTIVES
Despite the results of the RCT, some reservations remain regarding the use of biodegradable
plates and screws in maxillofacial surgery. There may be alternatives that can contribute
to finding the ideal fixation system. One such development is the welding technique
incorporated in the Sonicweld Rx system (Gebrüder Martin GmbH & Co., Tuttlingen,
Germany). A biodegradable pin is placed onto an ultra-sound activated sonic electrode,
called a sonotrode, and inserted into the borehole. As a result of the added ultra-sound
energy, the thermoplastic biodegradable pin will melt, resulting in a flow of biodegradable
polymers into the cortical bone layer and the cavities of the underlying cancellous bone. At
the same time the biodegradable plate and pinhead fuse. Due to the welding technique,
the handling characteristics as well as the mechanical properties are greatly enhanced
(146). These two aspects were the main reasons for the high amount of per-operative
switches reported in the randomized clinical trial. Despite these promising results (146), the
SonicWeld Rx system is considered not to be suitable for fixation of mandibular fractures
and osteotomies according to the manufacturer (KLS Martin). The present co-polymer
composition (50% L-lactide and 50% D-lactide) is not sufficient to fix mandibular fractures
and osteotomies in a stable manner. Different co-polymer(s) (compositions) with improved
mechanical characteristics could be used in conjunction with the welding technique to
achieve strong and easy to apply biodegradable plate and screw systems. Important
prerequisites, i.e. the biocompatibility and biodegradability of these polymers, should be
taken into account since they are important potential advantages of biodegradable plates
and screws. One should critically appraise the biocompatibility, biodegradability, and
finally the resorption of these polymers as up till now there is no evidence regarding the
complete resorption of biodegradable plate and screws to the electron microscopic level.
Future of research of biodegradable plates and screws will be determined to a large extent
by the above factors since the main rationale for using biodegradable plates and screws is
their disappearance after fulfilling their function (bone healing).
CH
AP
TE
R 5
CHAPTER 6
REFERENCE LIST
100 101
(1) Bohm H, Pistner H, Barth T, Reuther J, Muhling J. Bioresorbierbare Schrauben im Ver-
gleich zu Titanschrauben fur die Osteosynthese nach sagittaler Spaltung des Unterk-
iefers--Eine prospektive, randomisierte, kontrollierte klinische Studie. Biomed Tech
(Berl) 1998;43 Suppl:542-3.
(2) Norholt SE, Pedersen TK, Jensen J. Le Fort I miniplate osteosynthesis: a randomized,
prospective study comparing resorbable PLLA/PGA with titanium. Int J Oral Maxillofac
Surg 2004 April;33(3):245-52.
(3) Ferretti C, Reyneke JP. Mandibular, sagittal split osteotomies fixed with biodegradable
or titanium screws: a prospective, comparative study of postoperative stability. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2002 May;93(5):534-7.
(4) Cheung LK, Chow LK, Chiu WK. A randomized controlled trial of resorbable versus
titanium fixation for orthognathic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 2004 October;98(4):386-97.
(5) Ueki K, Marukawa K, Shimada M, Nakagawa K, Yamamoto E. Change in condylar
long axis and skeletal stability following sagittal split ramus osteotomy and intraoral
vertical ramus osteotomy for mandibular prognathia. J Oral Maxillofac Surg 2005
October;63(10):1494-9.
(6) Buchbinder D. Treatment of fractures of the edentulous mandible, 1943 to 1993: a
review of the literature. J Oral Maxillofac Surg 1993 November;51(11):1174-80.
(7) Haerle F, Champy M, Terry B. Atlas of Craniomaxillofacial Osteosynthesis. 2e edition.
2009. Thieme; Stuttgart, New York.
(8) Bataineh AB. Etiology and incidence of maxillofacial fractures in the north of Jordan.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998 July;86(1):31-5.
(9) Suomalainen A, Kiljunen T, Kaser Y, Peltola J, Kortesniemi M. Dosimetry and image qual-
ity of four dental cone beam computed tomography scanners compared with multislice
computed tomography scanners. Dentomaxillofac Radiol 2009 September;38(6):367-78.
(10) Bowers DG, Jr., Lynch JB. Management of facial fractures. South Med J 1977
August;70(8):910-8.
(11) Steinhauser EW. Historical development of orthognathic surgery. J Craniomaxillofac
Surg 1996 August;24(4):195-204.
(12) Stoelinga PJ. [110th volume of Dutch Journal of Dentistry 3. Developments in the treat-
ment of oral and craniomaxillofacial trauma during the last five decades]. Ned Tijdschr
Tandheelkd 2003 August;110(8):321-7.
(13) Schneider D. [The historical evolution of external cranio-maxillary fixation appliances
for treatment of midfacial fractures (author’s transl)]. Zahn Mund Kieferheilkd Zentralbl
1978;66(8):813-24.
(14) Merkx CA. [Fractures of the facial bones]. Ned Tijdschr Tandheelkd 1966
January;73(1):31-42.
(15) DANIS R. Treatment of fractures. Lancet 1947 October 4;2(6475):520.
(16) Perren SM, Russenberger M, Steinemann S, Muller ME, Allgower M. A dynamic com-
pression plate. Acta Orthop Scand Suppl 1969;125:31-41.
(17) Luhr HG. [Compression osteosynthesis in treatment of mandibular fractures--experimen-
tal principles and clinical experiences]. Dtsch Zahnarztl Z 1972 January;27(1):29-37.
(18) Luhr HG. [On the stable osteosynthesis in mandibular fractures]. Dtsch Zahnarztl Z
1968 July;23(7):754.
(19) Spiessl B. [Dynamic compression implant--principles, technic and results]. SSO Schweiz
Monatsschr Zahnheilkd 1976 September;86(9):964-74.
(20) Prein J, Eschmann A, Spiessl B. [Results of follow-up examinations in 81 patients
with functionally stable mandibular osteosynthesis]. Fortschr Kiefer Gesichtschir
1976;21:304-7.
(21) Spiessl B. [Functionally stable osteosynthesis in mandibular fractures--problems and
technic]. Fortschr Kiefer Gesichtschir 1975;19:68-72.
(22) Champy M, Lodde JP, Jaeger JH, Wilk A, Gerber JC. [Mandibular osteosynthesis ac-
cording to the Michelet technic. II. Presentation of new material. Results]. Rev Stomatol
Chir Maxillofac 1976 April;77(3):577-82.
(23) Champy M, Lodde JP, Jaeger JH, Wilk A. [Mandibular osteosynthesis according to
the Michelet technic. I. Biomechanical bases]. Rev Stomatol Chir Maxillofac 1976
April;77(3):569-76.

102 103
(24) Michelet FX, Deymes J, Dessus B. Osteosynthesis with miniaturized screwed plates in
maxillo-facial surgery. J Maxillofac Surg 1973 June;1(2):79-84.
(25) Bos RR, Jansma J, Vissink A. [Fractures of the midface]. Ned Tijdschr Tandheelkd 1997
November;104(11):440-3.
(26) Gerlach KL, Pape HD. [Principle and indication for mini-plate osteozynthesis]. Dtsch
Zahnarztl Z 1980 February;35(2):346-8.
(27) Cawood JI. Small plate osteosynthesis of mandibular fractures. Br J Oral Maxillofac
Surg 1985 April;23(2):77-91.
(28) Mommaerts MY, Engelke W. [Experiences with Champy/Lodde osteosynthesis plates in
mandibular fractures]. Dtsch Z Mund Kiefer Gesichtschir 1986 March;10(2):94-101.
(29) Spiessl B. [Perspectives of maxillary surgery in Switzerland]. Helv Chir Acta 1989
April;55(6):953-8.
(30) Ellis E, III, Moos KF, El Attar A. Ten years of mandibular fractures: an analysis of 2,137
cases. Oral Surg Oral Med Oral Pathol 1985 February;59(2):120-9.
(31) Adell R, Lekholm U, Rockler B, Branemark PI. A 15-year study of osseointegrated implants
in the treatment of the edentulous jaw. Int J Oral Surg 1981 December;10(6):387-416.
(32) Bhatt V, Langford RJ. Removal of miniplates in maxillofacial surgery: University Hospital
Birmingham experience. J Oral Maxillofac Surg 2003 May;61(5):553-6.
(33) Bhatt V, Chhabra P, Dover MS. Removal of miniplates in maxillofacial surgery: a follow-
up study. J Oral Maxillofac Surg 2005 June;63(6):756-60.
(34) Matthew IR, Frame JW. Policy of consultant oral and maxillofacial surgeons towards
removal of miniplate components after jaw fracture fixation: pilot study. Br J Oral Max-
illofac Surg 1999 April;37(2):110-2.
(35) Stoelinga PJ, Borstlap WA. The fixation of sagittal split osteotomies with miniplates:
the versatility of a technique. J Oral Maxillofac Surg 2003 December;61(12):1471-6.
(36) Ahn DK, Sims CD, Randolph MA, O’Connor D, Butler PE, Amarante MT, Yaremchuk
MJ. Craniofacial skeletal fixation using biodegradable plates and cyanoacrylate glue.
Plast Reconstr Surg 1997 May;99(6):1508-15.
(37) Goldstein JA. The use of bioresorbable material in craniofacial surgery. Clin Plast Surg
2001 October;28(4):653-9.
(38) Hasirci V, Lewandrowski KU, Bondre SP, Gresser JD, Trantolo DJ, Wise DL. High strength
bioresorbable bone plates: preparation, mechanical properties and in vitro analysis. Bi-
omed Mater Eng 2000;10(1):19-29.
(39) Matthews NS, Khambay BS, Ayoub AF, Koppel D, Wood G. Preliminary assessment
of skeletal stability after sagittal split mandibular advancement using a bioresorbable
fixation system. Br J Oral Maxillofac Surg 2003 June;41(3):179-84.
(40) Bos RR. Treatment of pediatric facial fractures: the case for metallic fixation. J Oral
Maxillofac Surg 2005 March;63(3):382-4.
(41) Peltoniemi HH, Ahovuo J, Tulamo RM, Tormala P, Waris T. Biodegradable and titanium
plating in experimental craniotomies: a radiographic follow-up study. J Craniofac Surg
1997 November;8(6):446-51.
(42) Rozema FR, Levendag PC, Bos RR, Boering G, Pennings AJ. Influence of resorbable
poly(L-lactide) bone plates and screws on the dose distributions of radiotherapy beams.
Int J Oral Maxillofac Surg 1990 December;19(6):374-6.
(43) Yerit KC, Hainich S, Turhani D, Klug C, Wittwer G, Ockher M, Ploder O, Undt G, Bau-
mann A, Ewers R. Stability of biodegradable implants in treatment of mandibular frac-
tures. Plast Reconstr Surg 2005 June;115(7):1863-70.
(44) Yaremchuk MJ, Posnick JC. Resolving controversies related to plate and screw fixation
in the growing craniofacial skeleton. J Craniofac Surg 1995 November;6(6):525-38.
(45) Penman HG, Ring PA. Osteosarcoma in association with total hip replacement. J Bone
Joint Surg Br 1984 November;66(5):632-4.
(46) Bostman O. Economic considerations on avoiding implant removals after fracture fixa-
tion by using absorbable devices. Scand J Soc Med 1994 March;22(1):41-5.
(47) Juutilainen T, Patiala H, Ruuskanen M, Rokkanen P. Comparison of costs in ankle frac-
tures treated with absorbable or metallic fixation devices. Arch Orthop Trauma Surg
1997;116(4):204-8.
(48) Rokkanen PU, Bostman O, Hirvensalo E, Makela EA, Partio EK, Patiala H, Vainionpaa SI,
Vihtonen K, Tormala P. Bioabsorbable fixation in orthopaedic surgery and traumatol-
ogy. Biomaterials 2000 December;21(24):2607-13.
104 105
(49) Schmidt BL, Perrott DH, Mahan D, Kearns G. The removal of plates and screws after Le
Fort I osteotomy. J Oral Maxillofac Surg 1998 February;56(2):184-8.
(50) Tuovinen V, Norholt SE, Sindet-Pedersen S, Jensen J. A retrospective analysis of 279
patients with isolated mandibular fractures treated with titanium miniplates. J Oral
Maxillofac Surg 1994 September;52(9):931-5.
(51) Kallela I, Laine P, Suuronen R, Lindqvist C, Iizuka T. Assessment of material- and tech-
nique-related complications following sagittal split osteotomies stabilized by biode-
gradable polylactide screws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005
January;99(1):4-10.
(52) Ylikontiola L, Sundqvuist K, Sandor GK, Tormala P, Ashammakhi N. Self-reinforced
bioresorbable poly-L/DL-lactide [SR-P(L/DL)LA] 70/30 miniplates and miniscrews are
reliable for fixation of anterior mandibular fractures: a pilot study. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 2004 March;97(3):312-7.
(53) Eppley BL, Sparks C, Herman E, Edwards M, McCarty M, Sadove AM. Effects of skel-
etal fixation on craniofacial imaging. J Craniofac Surg 1993 April;4(2):67-73.
(54) Disegi JA. Magnetic resonance imaging of AO/ASIF stainless steel and titanium im-
plants. Injury 1992;23 Suppl 2:S1-S4.
(55) Jainandunsing JS, van der Elst M, van der Werken CC. Bioresorbable fixation devices
for musculoskeletal injuries in adults. The Cochrane Database of Systematic Reviews:
Reviews 2005 Issue 2 John Wiley & Sons, Ltd Chichester, UK DOI: 10 1002/14651858
CD004 2005;(2).
(56) Laftman P, Nilsson OS, Brosjo O, Stromberg L. Stress shielding by rigid fixation studied
in osteotomized rabbit tibiae. Acta Orthop Scand 1989 December;60(6):718-22.
(57) Kulkarni RK, Pani KC, Neuman C, Leonard F. Polylactic acid for surgical implants. Arch
Surg 1966 November;93(5):839-43.
(58) Turvey TA, Bell RB, Tejera TJ, Proffit WR. The use of self-reinforced biodegrad-
able bone plates and screws in orthognathic surgery. J Oral Maxillofac Surg 2002
January;60(1):59-65.
(59) Ashammakhi N, Renier D, Arnaud E, Marchac D, Ninkovic M, Donaway D, Jones B, Serlo W,
Laurikainen K, Tormala P, Waris T. Successful use of biosorb osteofixation devices in 165 cra-
nial and maxillofacial cases: a multicenter report. J Craniofac Surg 2004 July;15(4):692-701.
(60) Eppley BL, Morales L, Wood R, Pensler J, Goldstein J, Havlik RJ, Habal M, Losken A,
Williams JK, Burstein F, Rozzelle AA, Sadove AM. Resorbable PLLA-PGA plate and
screw fixation in pediatric craniofacial surgery: clinical experience in 1883 patients.
Plast Reconstr Surg 2004 September 15;114(4):850-6.
(61) Eppley BL, Sadove AM. Resorbable coupling fixation in craniosynostosis surgery: ex-
perimental and clinical applications. J Craniofac Surg 1995 November;6(6):477-82.
(62) Kallela I, Laine P, Suuronen R, Ranta P, Iizuka T, Lindqvist C. Osteotomy site healing
following mandibular sagittal split osteotomy and rigid fixation with polylactide biode-
gradable screws. Int J Oral Maxillofac Surg 1999 June;28(3):166-70.
(63) Edwards RC, Kiely KD. Resorbable fixation of Le Fort I osteotomies. J Craniofac Surg
1998 May;9(3):210-4.
(64) Eppley BL, Prevel CD. Nonmetallic fixation in traumatic midfacial fractures. J Craniofac
Surg 1997 March;8(2):103-9.
(65) Voutilainen NH, Hess MW, Toivonen TS, Krogerus LA, Partio EK, Patiala HV. A long-
term clinical study on dislocated ankle fractures fixed with self-reinforced polylevolac-
tide (SR-PLLA) implants. J Long Term Eff Med Implants 2002;12(1):35-52.
(66) Bergsma EJ, Rozema FR, Bos RR, de Bruijn WC. Foreign body reactions to resorbable
poly(L-lactide) bone plates and screws used for the fixation of unstable zygomatic
fractures. J Oral Maxillofac Surg 1993 June;51(6):666-70.
(67) Bostman O, Hirvensalo E, Makinen J, Rokkanen P. Foreign-body reactions to fracture
fixation implants of biodegradable synthetic polymers. J Bone Joint Surg Br 1990
July;72(4):592-6.
(68) Bostman OM. Osteolytic changes accompanying degradation of absorbable fracture
fixation implants. J Bone Joint Surg Br 1991 July;73(4):679-82.
(69) Friden T, Rydholm U. Severe aseptic synovitis of the knee after biodegradable internal
fixation. A case report. Acta Orthop Scand 1992 February;63(1):94-7.
(70) Enislidis G, Lagogiannis G, Wittwer G, Glaser C, Ewers R. Fixation of zygomatic frac-
tures with a biodegradable copolymer osteosynthesis system: short- and long-term
results. Int J Oral Maxillofac Surg 2005 January;34(1):19-26.
106 107
(71) Cordewener FW, Schmitz JP. The future of biodegradable osteosyntheses. Tissue Eng
2000 August;6(4):413-24.
(72) Eppley BL. Bioabsorbable plates and screws: Current state of the art in facial fracture
repair. Discussion. J Craniomaxillofac Trauma 2000;6(1):28-9.
(73) Tiainen J, Soini Y, Tormala P, Waris T, Ashammakhi N. Self-reinforced polylactide/poly-
glycolide 80/20 screws take more than 1(1/2) years to resorb in rabbit cranial bone. J
Biomed Mater Res 2004 July 15;70B(1):49-55.
(74) Suuronen R, Kallela I, Lindqvist C. Bioabsorbable plates and screws: Current state of
the art in facial fracture repair. J Craniomaxillofac Trauma 2000;6(1):19-27.
(75) Bostman O, Pihlajamaki H. Clinical biocompatibility of biodegradable orthopaedic im-
plants for internal fixation: a review. Biomaterials 2000 December;21(24):2615-21.
(76) Frost HM. The biology of fracture healing. An overview for clinicians. Part II. Clin Or-
thop Relat Res 1989 November;(248):294-309.
(77) Frost HM. The biology of fracture healing. An overview for clinicians. Part I. Clin Or-
thop Relat Res 1989 November;(248):283-93.
(78) Junqueira JC, Carneiro J, Kelley RO. Botweefsel. In: Wisse E, Nie, enhuis P, nsel L, edi-
tors. Functionele histologie. 7 ed. Elsevier/ Bunge; 1996. p. 137-62.
(79) Kennady MC, Tucker MR, Lester GE, Buckley MJ. Stress shielding effect of rigid inter-
nal fixation plates on mandibular bone grafts. A photon absorption densitometry and
quantitative computerized tomographic evaluation. Int J Oral Maxillofac Surg 1989
October;18(5):307-10.
(80) Kennady MC, Tucker MR, Lester GE, Buckley MJ. Histomorphometric evaluation of
stress shielding in mandibular continuity defects treated with rigid fixation plates and
bone grafts. Int J Oral Maxillofac Surg 1989 June;18(3):170-4.
(81) Paavolainen P, Karaharju E, Slatis P, Ahonen J, Holmstrom T. Effect of rigid plate fixa-
tion on structure and mineral content of cortical bone. Clin Orthop Relat Res 1978
October;(136):287-93.
(82) Edwards TJ, David DJ. A comparative study of miniplates used in the treatment of man-
dibular fractures. Plast Reconstr Surg 1996 May;97(6):1150-7.
(83) Cox T, Kohn MW, Impelluso T. Computerized analysis of resorbable polymer plates and
screws for the rigid fixation of mandibular angle fractures. J Oral Maxillofac Surg 2003
April;61(4):481-7.
(84) Bozic KJ, Perez LE, Wilson DR, Fitzgibbons PG, Jupiter JB. Mechanical testing of bi-
oresorbable implants for use in metacarpal fracture fixation. J Hand Surg [Am ] 2001
July;26(4):755-61.
(85) Brons R, Boering G. Fractures of the mandibular body treated by stable internal fixa-
tion: a preliminary report. J Oral Surg 1970 June;28(6):407-15.
(86) Suuronen R, Kontio R, Ashammakhi N, Lindqvist C, Laine P. Bioabsorbable self-
reinforced plates and screws in craniomaxillofacial surgery. Biomed Mater Eng
2004;14(4):517-24.
(87) Rohner D, Tay A, Meng CS, Hutmacher DW, Hammer B. The sphenozygomatic suture
as a key site for osteosynthesis of the orbitozygomatic complex in panfacial fractures: a
biomechanical study in human cadavers based on clinical practice. Plast Reconstr Surg
2002 November;110(6):1463-71.
(88) Hunt JA, Vince DG, Williams DF. Image analysis in the evaluation of biomaterials. J
Biomed Eng 1993 January;15(1):39-45.
(89) Vince DG, Hunt JA, Williams DF. Quantitative assessment of the tissue response to
implanted biomaterials. Biomaterials 1991 October;12(8):731-6.
(90) Pinkhof H, van Everdingen JJE, Klazinga NS. Geneeskundig woordenboek. 10 ed. 1998.
(91) Vert M, Li S, Garreau H. New insights on the degradation of bioresorbable polymeric
devices based on lactic and glycolic acids. Clin Mater 1992;10(1-2):3-8.
(92) Pietrzak WS, Sarver DR, Verstynen ML. Bioabsorbable polymer science for the practic-
ing surgeon. J Craniofac Surg 1997 March;8(2):87-91.
(93) Vert M, Li SM, Garreau H. Attempts to map the structure and degradation character-
istics of aliphatic polyesters derived from lactic and glycolic acids. J Biomater Sci Polym
Ed 1994;6(7):639-49.
(94) Bostman O, Paivarinta U, Partio E, Vasenius J, Manninen M, Rokkanen P. Degradation
and tissue replacement of an absorbable polyglycolide screw in the fixation of rabbit
femoral osteotomies. J Bone Joint Surg Am 1992 August;74(7):1021-31.
108 109
(107) Pihlajamaki H, Kinnunen J, Bostman O. In vivo monitoring of the degradation process
of bioresorbable polymeric implants using magnetic resonance imaging. Biomaterials
1997 October;18(19):1311-5.
(108) Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions
4.2.4 [updated March 2005]. 2005.
(109) Sindhu F, Carpenter L, Seers K. Development of a tool to rate the quality assess-
ment of randomized controlled trials using a Delphi technique. J Adv Nurs 1997
June;25(6):1262-8.
(110) Bhanot S, Alex JC, Lowlicht RA, Ross DA, Sasaki CT. The efficacy of resorbable plates
in head and neck reconstruction. Laryngoscope 2002 May;112(5):890-8.
(111) Shetty V, Caputo AA, Kelso I. Torsion-axial force characteristics of SR-PLLA screws. J
Craniomaxillofac Surg 1997 February;25(1):19-23.
(112) Bahr W, Stricker A, Gutwald R, Wellens E. Biodegradable osteosynthesis material for
stabilization of midface fractures: experimental investigation in sheep. J Craniomaxil-
lofac Surg 1999 February;27(1):51-7.
(113) Suuronen R, Pohjonen T, Hietanen J, Lindqvist C. A 5-year in vitro and in vivo study of the
biodegradation of polylactide plates. J Oral Maxillofac Surg 1998 May;56(5):604-14.
(114) Bostman OM, Pihlajamaki HK. Adverse tissue reactions to bioabsorbable fixation de-
vices. Clin Orthop Relat Res 2000 February;(371):216-27.
(115) Taylor MS, Daniels AU, Andriano KP, Heller J. Six bioabsorbable polymers: in vitro acute
toxicity of accumulated degradation products. J Appl Biomater 1994;5(2):151-7.
(116) Pihlajamaki H, Bostman O, Hirvensalo E, Tormala P, Rokkanen P. Absorbable pins of
self-reinforced poly-L-lactic acid for fixation of fractures and osteotomies. J Bone Joint
Surg Br 1992 November;74(6):853-7.
(117) Matsusue Y, Hanafusa S, Yamamuro T, Shikinami Y, Ikada Y. Tissue reaction of bio-
absorbable ultra high strength poly (L-lactide) rod. A long-term study in rabbits. Clin
Orthop Relat Res 1995 August;(317):246-53.
(118) Vert M, Li S, Garreau H. New insights on the degradation of bioresorbable polymeric
devices based on lactic and glycolic acids. Clin Mater 1992;10(1-2):3-8.
(95) Brandt RB, Waters MG, Rispler MJ, Kline ES. D- and L-lactate catabolism to CO2 in rat
tissues. Proc Soc Exp Biol Med 1984 March;175(3):328-35.
(96) Williams DF. Mechanisms of biodegradation of implantable polymers. Clin Mater
1992;10(1-2):9-12.
(97) Williams DF, Mort E. Enzyme-accelerated hydrolysis of polyglycolic acid. J Bioeng 1977
August;1(3):231-8.
(98) Li S, Molina I, Martinez MB, Vert M. Hydrolytic and enzymatic degradations of physi-
cally crosslinked hydrogels prepared from PLA/PEO/PLA triblock copolymers. J Mater
Sci Mater Med 2002 January;13(1):81-6.
(99) Partio EK, Bostman O, Hirvensalo E, Vainionpaa S, Vihtonen K, Patiala H, Tormala P,
Rokkanen P. Self-reinforced absorbable screws in the fixation of displaced ankle frac-
tures: a prospective clinical study of 152 patients. J Orthop Trauma 1992;6(2):209-15.
(100) Bergsma JE, de Bruijn WC, Rozema FR, Bos RR, Boering G. Late degradation tissue re-
sponse to poly(L-lactide) bone plates and screws. Biomaterials 1995 January;16(1):25-
31.
(101) Bostman OM, Pihlajamaki HK. Late foreign-body reaction to an intraosseous bi-
oabsorbable polylactic acid screw. A case report. J Bone Joint Surg Am 1998
December;80(12):1791-4.
(102) Fraser RK, Cole WG. Osteolysis after biodegradable pin fixation of fractures in children.
J Bone Joint Surg Br 1992 November;74(6):929-30.
(103) Bostman OM. Intense granulomatous inflammatory lesions associated with absorbable
internal fixation devices made of polyglycolide in ankle fractures. Clin Orthop Relat Res
1992 May;(278):193-9.
(104) Hovis WD, Bucholz RW. Polyglycolide bioabsorbable screws in the treatment of ankle
fractures. Foot Ankle Int 1997 March;18(3):128-31.
(105) Ignatius AA, Claes LE. In vitro biocompatibility of bioresorbable polymers: poly(L, DL-
lactide) and poly(L-lactide-co-glycolide). Biomaterials 1996 April;17(8):831-9.
(106) Heidemann W, Fischer JH, Koebke J, Bussmann C, Gerlach KL. [In vivo study of degra-
dation of poly-(D,L-) lactide and poly-(L-lactide-co-glycolide) osteosynthesis material].
Mund Kiefer Gesichtschir 2003 September;7(5):283-8.
110 111
(130) Buijs GJ, van der Houwen EB, Stegenga B, Bos RR, Verkerke GJ. Torsion strength of biodegrada-
ble and titanium screws: a comparison. J Oral Maxillofac Surg 2007 November;65(11):2142-7.
(131) Ralph JP, Caputo AA. Analysis of stress patterns in the human mandible. J Dent Res
1975 July;54(4):814-21.
(132) Dolanmaz D, Uckan S, Isik K, Saglam H. Comparison of stability of absorbable and
titanium plate and screw fixation for sagittal split ramus osteotomy. Br J Oral Maxillofac
Surg 2004 April;42(2):127-32.
(133) Tams J, Rozema FR, Bos RR, Roodenburg JL, Nikkels PG, Vermey A. Poly(L-lactide) bone
plates and screws for internal fixation of mandibular swing osteotomies. Int J Oral
Maxillofac Surg 1996 February;25(1):20-4.
(134) Engroff SL, Blanchaert RH, Jr., von Fraunhofer JA. Mandibulotomy fixation: a labora-
tory analysis. J Oral Maxillofac Surg 2003 November;61(11):1297-301.
(135) Buijs GJ, van der Houwen EB, Stegenga B, Bos RR, Verkerke GJ. Mechanical strength
and stiffness of biodegradable and titanium osteofixation systems. J Oral Maxillofac
Surg 2007 November;65(11):2148-58.
(136) Pilling E, Meissner H, Jung R, Koch R, Loukota R, Mai R, Reitemeier B, Richter G, Sta-
dlinger B, Stelnicki E, Eckelt U. An experimental study of the biomechanical stability of
ultrasound-activated pinned (SonicWeld Rx+Resorb-X) and screwed fixed (Resorb-X)
resorbable materials for osteosynthesis in the treatment of simulated craniosynostosis
in sheep. Br J Oral Maxillofac Surg 2007 September;45(6):451-6.
(137) Miller DL, Goswami T. A review of locking compression plate biomechanics and their
advantages as internal fixators in fracture healing. Clin Biomech (Bristol , Avon ) 2007
December;22(10):1049-62.
(138) Gutwald R, Alpert B, Schmelzeisen R. Principle and stability of locking plates. Keio J
Med 2003 March;52(1):21-4.
(139) Chritah A, Lazow SK, Berger JR. Transoral 2.0-mm locking miniplate fixation of man-
dibular fractures plus 1 week of maxillomandibular fixation: a prospective study. J Oral
Maxillofac Surg 2005 December;63(12):1737-41.
(140) Ellis E, III, Carlson DS. The effects of mandibular immobilization on the masticatory
system. A review. Clin Plast Surg 1989 January;16(1):133-46.
(119) Heidemann W, Jeschkeit S, Ruffieux K, Fischer JH, Wagner M, Kruger G, Wintermantel
E, Gerlach KL. Degradation of poly(D,L)lactide implants with or without addition of
calciumphosphates in vivo. Biomaterials 2001 September;22(17):2371-81.
(120) Juniper RP, Awty MD. The immobilization period for fractures of the mandibular body.
Oral Surg Oral Med Oral Pathol 1973 August;36(2):157-63.
(121) Louis PJ, Waite PD, Austin RB. Long-term skeletal stability after rigid fixation of Le Fort
I osteotomies with advancements. Int J Oral Maxillofac Surg 1993 April;22(2):82-6.
(122) Buijs GJ, Stegenga B, Bos RR. Efficacy and safety of biodegradable osteofixa-
tion devices in oral and maxillofacial surgery: a systematic review. J Dent Res 2006
November;85(11):980-9.
(123) Laine P, Kontio R, Lindqvist C, Suuronen R. Are there any complications with bioab-
sorbable fixation devices? A 10 year review in orthognathic surgery. Int J Oral Maxil-
lofac Surg 2004 April;33(3):240-4.
(124) Haers PE, Sailer HF. Biodegradable self-reinforced poly-L/DL-lactide plates and screws
in bimaxillary orthognathic surgery: short term skeletal stability and material related
failures. J Craniomaxillofac Surg 1998 December;26(6):363-72.
(125) Luhr HG. [The development of modern osteosynthesis]. Mund Kiefer Gesichtschir
2000 May;4 Suppl 1:S84-S90.
(126) Stoelinga PJ. [110th volume of Dutch Journal of Dentistry 3. Developments in the treat-
ment of oral and craniomaxillofacial trauma during the last five decades]. Ned Tijdschr
Tandheelkd 2003 August;110(8):321-7.
(127) Rozema FR, Levendag PC, Bos RR, Boering G, Pennings AJ. Influence of resorbable
poly(L-lactide) bone plates and screws on the dose distributions of radiotherapy beams.
Int J Oral Maxillofac Surg 1990 December;19(6):374-6.
(128) Ghali GE, Sinn DP, Tantipasawasin S. Management of nonsyndromic craniosynostosis.
Atlas Oral Maxillofac Surg Clin North Am 2002 March;10(1):1-41.
(129) Suuronen R, Laine P, Pohjonen T, Lindqvist C. Sagittal ramus osteotomies fixed with bio-
degradable screws: a preliminary report. J Oral Maxillofac Surg 1994 July;52(7):715-20.
112 113
(141) Wittwer G, Adeyemo WL, Voracek M, Turhani D, Ewers R, Watzinger F, Enislidis G. An
evaluation of the clinical application of three different biodegradable osteosynthesis
materials for the fixation of zygomatic fractures. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2005 December;100(6):656-60.
(142) Bayat M, Garajei A, Ghorbani K, Motamedi MH. Treatment of mandibular angle fractures
using a single bioresorbable miniplate. J Oral Maxillofac Surg 2010 July;68(7):1573-7.
(143) Cohen AJ, Dickerman RD, Schneider SJ. New method of pediatric cranioplasty for skull
defect utilizing polylactic acid absorbable plates and carbonated apatite bone cement.
J Craniofac Surg 2004 May;15(3):469-72.
(144) Ueki K, Nakagawa K, Marukawa K, Takazakura D, Shimada M, Takatsuka S, Yamamoto
E. Changes in condylar long axis and skeletal stability after bilateral sagittal split ramus
osteotomy with poly-L-lactic acid or titanium plate fixation. Int J Oral Maxillofac Surg
2005 September;34(6):627-34.
(145) Stegenga B, de Bont LG, de Leeuw R, Boering G. Assessment of mandibular function
impairment associated with temporomandibular joint osteoarthrosis and internal de-
rangement. J Orofac Pain 1993;7(2):183-95.
(146) Buijs GJ, van der Houwen EB, Stegenga B, Verkerke GJ, Bos RR. Mechanical strength
and stiffness of the biodegradable SonicWeld Rx osteofixation system. J Oral Maxil-
lofac Surg 2009 April;67(4):782-7.
(147) Iizuka T, Lindqvist C. Rigid internal fixation of mandibular fractures. An analysis of
270 fractures treated using the AO/ASIF method. Int J Oral Maxillofac Surg 1992
April;21(2):65-9.
(148) Nieminen T, Rantala I, Hiidenheimo I, Keranen J, Kainulainen H, Wuolijoki E, Kallela I.
Degradative and mechanical properties of a novel resorbable plating system during a
3-year follow-up in vivo and in vitro. J Mater Sci Mater Med 2008 March;19(3):1155-
63.
(149) Langford RJ, Frame JW. Surface analysis of titanium maxillofacial plates and screws
retrieved from patients. Int J Oral Maxillofac Surg 2002 October;31(5):511-8.
CHAPTER 7
SUMMARY
116 117
Maxillofacial traumatology and orthognathic surgery are major fields of oral and
maxillofacial surgery. Internal rigid fixation systems, i.e. plates and screws, are used
for fixation and stabilization of osteotomized or fractured bone segments. Plates and
screws are generally made of titanium and are currently regarded as the golden standard.
However, titanium devices also have disadvantages. They interfere with radiotherapy and
imaging techniques. Besides, titanium implants have been associated with complications
such as growth restriction and brain damage, infection, and possible mutagenic effects.
A second intervention to remove the implants implies additional surgical discomfort,
risks, and associated socio-economical costs. Biodegradable osteofixation systems have
the possibility to degrade, thus preventing the need for a second intervention. Another
advantage of biodegradable devices is their radiolucency, implying good compatibility with
radiotherapy and imaging techniques. Since the introduction of biodegradable devices in
1966, the development of their mechanical properties and degradation characteristics has
been extensive. Numerous in vitro, animal, and clinical studies have been published with
positive as well as negative results. Despite the supposed advantages of biodegradable
osteofixation devices, these systems did not replace the titanium systems and are
currently applied in only limited numbers. The mechanical properties are less favourable
and ultimate resorption has not been proven. Another significant factor of the limited use
is the resistance by surgeons to modify their conventional, well experienced, treatment
techniques. The major drawback for general use of biodegradable devices is the lack
of clinical evidence. The general aim of this thesis was to establish the effectiveness
and safety of biodegradable plates and screws to fix bone segments in the maxillofacial
skeleton as a potential alternative to metallic ones.
Chapter 2 comprises a systematic review of the available literature to determine the
clinical efficacy and safety of biodegradable devices compared with titanium devices in
oral and maxillofacial surgery. A highly sensitive search in the databases of MEDLINE
(1966-2005), EMBASE (1989-2005), and CENTRAL (1800-2005) was conducted to identify
eligible studies. The relevance of studies was evaluated by a first selection based on
title and abstract. Eligible studies were independently evaluated by two assessors using
a quality assessment scale. The procedure revealed four methodologically ‘acceptable’
articles. Owing to the different outcome measures used in the studies, it was impossible
to perform a meta-analysis. Therefore, the major effects regarding the stability and
morbidity of fracture fixation using titanium and biodegradable fixation systems were
qualitatively described. Firm conclusions regarding the fixation of traumatically fractured
bone segments cannot be drawn due to the lack of controlled clinical trials. Regarding
the fixation of bone segments in orthognathic surgery, only a few controlled clinical
studies are available. There does not appear to be a significant short-term difference
between titanium and biodegradable fixation systems regarding stability and morbidity.
However, definite conclusions, especially with respect to the long-term performance of
biodegradable fixation devices used in maxillofacial surgery, cannot be drawn.
CH
AP
TE
R 7
CH
AP
TE
R 7
Chapter 3 focuses on the mechanical characteristics of biodegradable versus titanium
plates and screws. In chapter 3.1 the differences in maximum torque of 7 commercially
available biodegradable and 2 commercially available titanium screw systems were
investigated. Besides, the differences of maximum torque between ‘hand tight’ and
break of the screws were investigated. Four oral and maxillofacial surgeons inserted 8
specimens of all 9 screw systems in polymethylmethacrylate (PMMA) plates. The surgeons
were instructed to insert the screws as they would have done in the clinic (‘hand tight’).
The data were recorded by a torque measurement meter. A PhD resident inserted 8
specimens of the same set of 9 screw systems until fracture occurred. The maximum
applied torque was recorded likewise. The mean maximum torque of the 2 titanium
screw systems was significantly higher than that of the 7 biodegradable screw systems.
Besides, the mean maximum torque for ‘hand tight’ was significantly lower than for break
regarding 2 biodegradable, and both titanium screw systems. Based on the results, we
conclude that the 1.5- and 2.0 mm titanium screw systems still present the highest torque
strength compared to the biodegradable screw systems. When there is an intention to use
biodegradable screws, with regard to there mechanical characteristics, we recommend
the use of 2.0 mm BioSorb FX, 2.0 mm LactoSorb or the 2.5 mm Inion CPS screws.
In chapter 3.2.1 and 3.2.2 relevant mechanical data is presented in order to simplify
the selection of an osteofixation system for situations requiring immobilization in oral
and maxillofacial surgery. Seven biodegradable and 2 titanium osteofixation systems
(chapter 3.2.1) and the SonicWeld Rx biodegradable osteofixation system (chapter 3.2.2) were investigated. The SonicWeld Rx system uses an ultra-sound activated sonic
electrode to insert the biodegradable pin into the borehole. As a result of the added
ultra-sound energy, the thermoplastic biodegradable pin will melt, resulting in a flow of
biodegradable polymers into the cortical bone layer and the cavities of the cancellous
bone. At the same time the biodegradable plate and pinhead fuse. The plates and screws
were fixed to 2 polymethylmethacrylate (PMMA) blocks to simulate bone segments.
The plates and screws were subjected to tensile, side bending, and torsion tests. During
tensile tests, the strength of the osteofixation system was monitored. The stiffness was
calculated for the tensile, side bending, and torsion tests. The results were that the two
titanium systems (1.5 mm and 2.0 mm) presented significantly higher tensile strength
and stiffness compared to the 7 biodegradable systems (2.0 mm, 2.1 mm, and 2.5 mm)
presented in chapter 3.2.1. The 2.0 mm titanium system revealed significantly higher
side bending and torsion stiffness than the other 7 systems. Regarding the SonicWeld
Rx biodegradable plates and screws (chapter 3.2.2), the tensile strength and stiffness
as well as the side bending stiffness of that system presented up to 11.5 times higher
mean values than the conventional biodegradable Resorb X system. The torsion stiffness
of both systems presents similar mean values and standard deviations. Based on the
results of the current study, it can be concluded that the titanium osteofixation systems
were (significantly) stronger and stiffer than the biodegradable systems. The BioSorb FX,
118 119
LactoSorb, and Inion CPS 2.5 mm systems have high mechanical device strength and
stiffness compared to the investigated biodegradable osteofixation systems. In addition,
the results presented in chapter 3.2.2 yielded that the SonicWeld Rx system is an
improvement in the search for a mechanically strong and stiff biodegradable osteofixation
system. Future research should be done in order to find out whether the promising in
vitro results can be transferred to the in situ clinical situation.
Chapter 4 comprises a randomized controlled trial regarding the effectiveness and safety
of biodegradable plates and screws as a potential alternative to metallic ones. The multi-
centre RCT was conducted from December 2006 to July 2009. Included were patients
who underwent mandibular- and Le Fort I osteotomies and those with fractures of the
mandible, maxilla, or zygoma. The patients were assigned to a titanium control-group (KLS
Martin) or to a biodegradable test-group (Inion CPS). The primary outcome measure was
‘bone healing 8 weeks after surgery’. The Intention To Treat analysis (ITT) of 111 patients in
the titanium group and 112 patients in the biodegradable group yielded a non-significant
difference. In 25 patients (22%) who were included in the biodegradable group, the
surgeon made the decision to switch to the titanium system per-operatively. Concerning
most of the secondary outcome measures, the biodegradable system appeared to be
non-inferior to the titanium system. In contrast, the handling characteristics showed a
remarkable difference between both systems whereby biodegradable plates and screws
were more difficult in use as compared to titanium plates and screws. Despite the ‘non
inferior’ primary outcome result, the benefits of using biodegradable systems (less plate
removal operations) should be demonstrated during a follow-up of minimally 5 years,
especially when the large number of patients for whom it was per-operatively decided
to switch from the biodegradable system to the conventional titanium system, are taken
into account.
The main research outcomes are discussed and general conclusions are drawn in
chapter 5. Based on the results of the RCT performed in this thesis, it is concluded that
biodegradable plates and screws do not perform inferior to titanium regarding a follow-
up period of 8 weeks. The high percentage of per-operative switches from biodegradable
to titanium is a threat to a widespread acceptation of biodegradable plates and screws
in the current treatment protocols and guidelines in maxillofacial surgery. The follow-up
period of 1 year is expected to provide more clarity about the potential differences in
plate removal operations and thus the potential gain in effectiveness in the treatment of
fractures and osteotomies of the maxillofacial skeleton. The 1 year follow up results will
also provide more information about the skeletal stability, biocompatibility, and resorption
aspects of Inion CPS plates and screws.
CH
AP
TE
R 7
CH
AP
TE
R 7
CHAPTER 8
DUTCH SUMMARY
122 123
Maxillofaciale traumatologie en orthognathische chirurgie zijn belangrijke deelgebieden
binnen de kaakchirurgie. Interne rigide fixatie systemen, dat wil zeggen platen en schroeven,
worden gebruikt voor fixatie en stabilisatie van kaakfracturen of kaakverplaatsingen. Platen
en schroeven zijn meestal gemaakt van titanium en worden op dit moment beschouwd als
de gouden standaard. Titanium platen en schroeven hebben ook nadelen. Ze interfereren
met radiotherapie en beeldvormende technieken. Verder zijn titanium platen en schroeven
in verband gebracht met complicaties zoals groeiachterstand en hersenbeschadiging,
infectie, en mogelijke mutagene effecten. Om deze nadelen weg te nemen worden de
platen en schroeven in 5-40% van de gevallen verwijderd. Dit impliceert extra chirurgisch
ongemak, risico’s en daarmee samenhangende sociaal-economische kosten. Biologisch
afbreekbare platen en schroeven hebben de mogelijkheid om in het lichaam af te
breken, waardoor de noodzaak van een tweede interventie zou worden voorkomen.
Een ander voordeel van biodegradeerbare platen en schroeven is hun radiolucentie,
wat een goede compatibiliteit met radiotherapie en beeldvormende technieken toelaat.
Sinds de introductie van biologisch afbreekbare platen en schroeven in 1966, heeft de
ontwikkeling van hun mechanische eigenschappen en degradatie karakteristieken een
uitgebreide ontwikkeling doorgemaakt. Vele in vitro-, dier- en klinische studies zijn
gepubliceerd met zowel positieve als negatieve resultaten. Ondanks de veronderstelde
voordelen van biodegradeerbare platen en schroeven, hebben deze de titanium platen en
schroeven (nog) niet vervangen. Biodegradeerbare platen en schroeven worden slechts
in beperkte aantallen gebruikt. De mechanische eigenschappen zijn minder gunstig en
de uiteindelijke (volledige) resorptie is niet bewezen. Een andere belangrijke factor van
het beperkte gebruik is de weerstand van chirurgen om hun traditionele, zeer ervaren
technieken en behandelwijze te wijzigen. Echter, het gebrek aan overtuigend klinisch
wetenschappelijk bewijs is wellicht het belangrijkste aspect voor het summiere gebruik
van biodegradeerbare platen en schroeven. Het doel van dit promotieonderzoek was om
de effectiviteit en veiligheid van biodegradeerbare platen en schroeven vast te stellen bij
het vastzetten van botsegmenten in het maxillofaciale skelet als een potentieel alternatief
voor metalen platen en schroeven.
Hoofdstuk 2 omvat een systematische review van de beschikbare literatuur om de
effectiviteit en veiligheid van biodegradeerbare platen en schroeven in vergelijking
met titanium platen en schroeven vast te stellen. Een uitgebreide zoekstrategie in de
databases van MEDLINE (1966-2005), EMBASE (1989-2005) en CENTRAL (1800-2005)
werd uitgevoerd om in aanmerking komende studies te identificeren. De relevantie van
de studies werd geëvalueerd door een eerste selectie op basis van titel en samenvatting.
In aanmerking komende studies werden onafhankelijk van elkaar beoordeeld door twee
beoordelaars met behulp van een schaal waarop de kwaliteit van de studie kan worden
getoetst. De procedure leverde vier methodologisch ‘aanvaardbare’ artikelen op. Vanwege
de verschillende uitkomstmaten die waren gebruikt in de studies, was het onmogelijk om
een meta-analyse uit te voeren. De belangrijkste effecten met betrekking tot de stabiliteit
CH
AP
TE
R 8
CH
AP
TE
R 8
en de veiligheid van fractuurfixatie werden dan ook kwalitatief beschreven. Definitieve
conclusies met betrekking tot de fixatie van gebroken botsegmenten konden niet worden
getrokken als gevolg van het ontbreken van gecontroleerde klinische studies. Met
betrekking tot de fixatie van botsegmenten bij orthognatische behandelingen, waren
slechts een paar gecontroleerde klinische studies beschikbaar. Er leek op de korte termijn
geen significant verschil te zijn tussen titanium en biodegradeerbare fixatie systemen met
betrekking tot de stabiliteit en veiligheid. Echter, definitieve conclusies met betrekking
tot de lange termijn prestaties van biodegradeerbare platen en schroeven konden niet
worden getrokken.
Hoofdstuk 3 richt zich op de mechanische eigenschappen van biodegradeerbare versus
titanium platen en schroeven. In hoofdstuk 3.1 werden de verschillen onderzocht in
het maximale draaimoment van 7 commercieel verkrijgbare biodegradeerbare en 2
commercieel verkrijgbare titanium schroeven. Bovendien werden de verschillen in
het maximale draaimoment tussen ‘handvast’ en het breken van de schroef (‘breuk’)
onderzocht. Vier kaakchirurgen draaiden 8 exemplaren van alle 9 verschillende schroeven
in polymethylmethacrylaat (PMMA) platen. De chirurgen kregen de opdracht het
aandraaien en plaatsen van de schroeven zo te doen als dat ze dat zouden doen in de
kliniek (‘handvast’). De gegevens werden geregistreerd door de draaimoment-meter. Een
promovendus schroefde eenzelfde set van 8 exemplaren van de 9 schroeven in de PMMA
platen totdat breuk optrad. Het maximale draaimoment werd opgenomen en genoteerd.
Het maximale draaimoment van de 2 verschillende titanium schroeven (1,5 mm en 2,0
mm) was significant hoger dan dat van de 7 biodegradeerbare schroeven (2,0 mm, 2,1
mm en 2,5 mm). Daarnaast kon worden vastgesteld dat het maximale draaimoment voor
‘handvast’ voor 2 biodegradeerbare alsook beide titanium schroeven, significant lager
was dan voor ‘breuk’. Op basis van de resultaten concluderen we dat de 1,5- en 2,0 mm
titanium schroeven het hoogste draaimoment vertonen. Wanneer er een voornemen is
om biologisch afbreekbare schroeven te gebruiken, raden wij het gebruik van 2,0 mm
BioSorb FX, 2,0 mm LactoSorb of de 2,5 mm Inion CPS schroeven aan.
In hoofdstuk 3.2.1 en 3.2.2 worden relevante mechanische eigenschappen
gepresenteerd met het oog op een goede selectie van platen en schroeven voor het
immobiliseren van botsegmenten in de kaakchirurgie. Zeven biologisch afbreekbare en
2 titanium plaat- en schroef systemen, werden onderzocht in hoofdstuk 3.2.1, terwijl
additioneel het SonicWeld Rx biologisch afbreekbaar plaat- en pin systeem in hoofdstuk 3.2.2 werd onderzocht. Het SonicWeld Rx systeem maakt gebruik van een ultra-geluid
geactiveerde sonische elektrode voor het plaatsen van de biologisch afbreekbare pin in
het boorgat. Als gevolg van de toegevoegde ultrasone energie, zal de thermoplastisch
biologisch afbreekbare pin smelten. Dit resulteert in een stroom van plastische
polymeren in de holten van het trabeculaire bot. Tegelijkertijd versmelten de biologisch
afbreekbare plaat en kop van de pin. De platen en schroeven werden vastgezet op 2
polymethylmethacrylaat (PMMA) blokken welke botsegmenten simuleren. De platen en
124 125
schroeven werden onderworpen aan trek-, zijdelings buigen-, en torsie- tests. Tijdens
trekproeven werd de sterkte gemeten. De stijfheid werd berekend voor de trek-, zijdelings
buigen- en torsie- testen. De resultaten waren dat de twee titanium systemen (1,5 mm
en 2,0 mm) significant hogere treksterktes en stijfheid presenteerden ten opzichte van de
7 biologisch afbreekbare systemen (2,0 mm, 2,1 mm en 2,5 mm). Het 2,0 mm titanium
systeem presenteerde significant hogere zijdelingse buig- en torsie- stijfheid dan de
andere 7-systemen (hoofdstuk 3.2.1). Met betrekking tot de SonicWeld Rx biologisch
afbreekbare platen en pinnen (hoofdstuk 3.2.2), presenteerde de treksterkte en stijfheid,
alsmede de zijdelingse buigstijfheid van dat systeem tot 11,5 maal hogere waarden dan
de conventionele biologisch afbreekbare Resorb X platen en schroeven. De torsiestijfheid
van beide systemen presenteerde vergelijkbare waarden. Gebaseerd op de resultaten
kon worden geconcludeerd dat de titanium platen en schroeven sterker en stijver zijn
dan de biologisch afbreekbare systemen. De BioSorb FX, LactoSorb, Inion CPS 2,5 mm-
platen en schroeven hebben een hoge mechanische sterkte en stijfheid in vergelijking
met de andere onderzochte biologisch afbreekbare platen en schroeven. Daarnaast lieten
de resultaten, gepresenteerd in hoofdstuk 3.2.2, zien dat de SonicWeld Rx platen en
pinnen een sterke verbetering betroffen in het zoeken naar een mechanisch sterk en stijf
biologisch afbreekbaar fixatie systeem. Toekomstig onderzoek moet worden uitgevoerd
om uit te vinden of de veelbelovende in vitro resultaten kunnen worden vertaald naar de
in situ klinische situatie.
Hoofdstuk 4 omvat een gerandomiseerde gecontroleerde studie met betrekking tot
de effectiviteit en veiligheid van biologisch afbreekbare platen en schroeven als een
potentieel alternatief voor metalen platen en schroeven. De multi-center RCT werd
uitgevoerd van december 2006 tot juli 2009. Patiënten bij wie een onderkaak- en
bovenkaak osteotomie werd uitgevoerd, en mensen met fracturen van de onderkaak,
bovenkaak, of het jukbeencomplex, werden geïncludeerd in de studie. De patiënten
werden toegewezen aan een titanium controlegroep (KLS Martin) of een biologisch
afbreekbare testgroep (Inion CPS). De primaire uitkomstmaat was ‘botgenezing 8 weken
na chirurgie’. De ‘intention to treat-analyse’ (ITT) van 111 patiënten in de titanium
groep en 112 patiënten in de biologisch afbreekbare groep leverde een niet-significant
verschil op. Bij 25 patiënten (22%) die werden geïncludeerd in de biologisch afbreekbare
studiegroep, nam de chirurg per-operatief de beslissing om over te schakelen naar het
titanium systeem. Met betrekking tot de meeste van de secundaire uitkomstmaten, bleek
dat het biologisch afbreekbare systeem niet inferieur was aan het titanium systeem. In
tegenstelling tot bovengenoemde, bleek dat de handelingeigenschappen een opvallend
verschil vertoonde tussen beide systemen. De biologisch afbreekbare platen en schroeven
waren moeilijker in het gebruik in vergelijking met titanium platen en schroeven. Ondanks
de ‘niet inferieure’ resultaten aangaande de primaire uitkomstmaat, moeten de voordelen
van het gebruik van biologisch afbreekbare systemen (minder plaat verwijdering) worden
bevestigd gedurende een follow-up van minimaal 5 jaar. Dit geldt voornamelijk wanneer
CH
AP
TE
R 8
men rekening houdt met het grote aantal patiënten voor wie per-operatief besloten
is om van de biologisch afbreekbare platen en schroeven over te schakelen naar de
conventionele titanium platen en schroeven.
De belangrijkste onderzoeksresultaten worden besproken en algemene conclusies
worden getrokken in hoofdstuk 5. Gebaseerd op de resultaten van de RCT uitgevoerd
in dit proefschrift wordt geconcludeerd dat biologisch afbreekbare platen en schroeven
niet inferieur zijn aan titanium platen en schroeven met betrekking tot de botheling 8
weken na chirurgie. Het hoge percentage van de per-operatieve switches van biologisch
afbreekbare platen en schroeven naar titanium platen en schroeven is echter wel een
bedreiging voor een brede acceptatie en invoering in protocollen en richtlijnen in de
kaakchirurgie. De follow-up periode van 1 jaar zal naar verwachting meer duidelijkheid
over de mogelijke verschillen in de plaat verwijdering geven. En dus ook in en de
eventuele winst in effectiviteit bij de behandeling van breuken en osteotomieën van het
maxillofaciale skelet. De 1-jaars follow-up resultaten zullen ook meer informatie moeten
geven over de skeletale stabiliteit, biocompatibiliteit en resorptie aspecten van Inion CPS
platen en schroeven.
CH
AP
TE
R 8
DANKWOORD
128 129
DA
NK
WO
OR
D
Eindelijk is het zover! Begonnen aan een promotietraject met als doel kaakchirurg te
worden. Enkele jaren later blijkt dat er voor mij bijzonder grote uitdagingen liggen binnen
de tandheelkunde. Er waren reeds drie artikelen gepubliceerd, en het vierde artikel was
geaccepteerd. Alhoewel de follow-up van het vijfde artikel 8 weken betrof, duurde de
daadwerkelijke afronding hiervan, nog vele weken langer. Na 7 jaren is het proefschrift
dan af. Tijd voor nieuwe hoofdstukken binnen de tandheelkunde, sociale activiteiten,
hobby’s, vrienden en familie. Maar eerst nog de afronding op de Broerstraat voordat dit
hoofdstuk gesloten kan worden.
Veel mensen hebben geholpen om dit proefschrift tot een goed einde te brengen.
Allereerst wil ik de patiënten bedanken die hebben gekozen om deel te nemen aan de
grootste en enige patiënten studie van dit proefschrift. Iedereen hartelijk dank hiervoor!
Geachte prof. dr. Bos, enthousiasmerende 1ste promotor, best Ruud, altijd druk, maar
toch ook altijd tijd! Je ongeëvenaarde aanstekelijke enthousiasme heeft ervoor gezorgd
dat ik je heb gevraagd begeleider te worden voor mijn scriptie. Dit heeft uiteindelijk de
basis gevormd voor dit proefschrift. Mede door al je contacten op het gebied van de
biodegradeerbare materialen alsook de bewaker van de grote lijnen heeft dit proefschrift
tot een goed einde kunnen komen. Naast het onderzoek was je ook ‘bewaker van een
ontspannen sfeer’ en had je altijd interesse in zaken buiten het onderzoek. Hartelijk dank
daarvoor!
Geachte prof. dr. Stegenga, scherpzinnige 2e promotor, beste Boudewijn, onze vele
onderzoeksbesprekingen waren altijd bijzonder leerzaam. Soms ging ik weg met het
gevoel dat er honderden beren op de weg waren bijgekomen en, soms ook met een
gevoel van ‘yes’ we hebben weer stappen in de goede richting gezet. Je hebt me geleerd
kritisch te zijn, oplossingsgericht te denken, en alles in hapklare brokken te verwerken.
De keren dat de brokken in m’n keel bleven hangen, kon ik altijd bij je terecht. Veel dank
voor dit alles, ik heb veel van je geleerd!
Geachte prof. dr. Verkerke, beste 3e promotor, beste Bart, dank voor de samenwerking
en de kritische commentaren ‘vanuit een andere invalshoek’ welke de 3 artikelen uit
hoofdstuk 3 voor een belangrijk deel hebben vormgegeven.
Geachte dr. Jansma, beste co-promotor, beste Johan, je hebt verreweg de meeste
patiënten met oplosbare platen en schroeven behandeld. Je hebt daarmee een belangrijke
bijdrage geleverd aan het tot stand komen van de RCT. Je praktische en klinische blik
hebben bovendien voor waardevolle op- en aanmerkingen gezorgd bij het schrijven van
het artikel van de RCT alsook de afronding van mijn proefschrift.
DA
NK
WO
OR
D
Geachte prof. de Bont, veel dank voor het feit dat ik mocht beginnen aan dit promotietraject
alsook de vrijheid die u mij heeft gegeven in het afronden hiervan.
Geachte leden van de promotie commissie, geachte prof. dr. de Lange en geachte prof.
dr. Tuinzing, ik ben u zeer erkentelijk voor de snelle en nauwgezette beoordeling van het
manuscript.
Dear member of the appraisal committee, dear prof. Gerlach, thanks for the fast and the
accurate appraisal of the manuscript.
Geachte drs. van der Houwen, beste Ward, samen hebben we vele uren achter de
computer en de trekbank doorgebracht om de mechanische testen te bedenken, te
testen en uit te voeren. Het was altijd gezellig en inspirerend. In het bijzonder je ‘net iets
andere’ kijk op dingen en zaken in de maatschappij heb ik altijd erg leuk gevonden! Voor
mij is het proefschrift nu afgerond; ik hoop dat je snel zult volgen!
Geachte dr. de Visscher, dr. Hoppenreijs, dr. Brouns, dr. Fennis, dr. Bergsma, dr. Gooris en
de secretariaten van bovengenoemde heren, beste Jan, Theo, John, Jeroen, Eelco en Peter.
Veel dank voor het uitvoeren van de operaties bij de patiënten en het invullen en opsturen
van de formulieren. Al jullie inspanningen hebben geleid tot de grootste gerandomiseerde
klinische studie naar osteotomieen en fracturen in het aangezicht van dit moment.
Drs. N.B. van Bakelen, beste Nico, we leerden elkaar kennen op het introductiekamp
van Panacea, jij ging geneeskunde doen en ik tandheelkunde. Gelukkig zijn we elkaar
niet uit het oog verloren. We werden vrienden, huisgenoten en uiteindelijk ook collega
promovendus. Ik ben zeer blij met de manier waarop jij ‘mijn’ promotieonderzoek hebt
opgepakt. De manier waarop jij dat hebt vormgegeven vind ik bewonderenswaardig.
Je nauwgezette manier van werken en je ongeëvenaarde inzet kenmerken je als collega
en goede vriend en zullen je helpen ‘jouw’ proefschrift tot een goed einde te brengen.
Bedankt dat je mijn paranimf wilt zijn.
Drs. H.J.W.E. de Lange, beste Henk-Jan, onze passie voor de tandheelkunde heeft ons
niet alleen vele levendige discussies opgeleverd, maar ook een bijzondere vriendschap. De
gesprekken en discussies doorspekt met humor en metaforen zijn altijd erg aanstekelijk.
Je onophoudelijke interesse in mijn onderzoek en in mijn persoon heb ik altijd als zeer
waardevol ervaren. Ik hoop daar nog lang van te mogen genieten. Bedankt dat je mijn
paranimf wilt zijn.
Geacht secretariaat, beste Karin, Lisa en Nienke, dank voor jullie plezierige koffiemomenten
en gezelligheid. Als er taart was wisten jullie mij gelukkig als een van de eerste te
vinden!
130 131
Medewerkers en kaakchirurgen in opleiding van de afdelingen Kaakchirurgie in het
UMCG, het Amphia ziekenhuis Breda, het Medisch Centrum Leeuwarden en het Rijnstate
Ziekenhuis Arnhem en ieder ander niet met naam en toenaam genoemd die heeft
geholpen de RCT in hoofdstuk 4 tot een goed einde te brengen, hartelijk dank hiervoor.
Alle mede-onderzoekers van de afdeling Kaakchirurgie op de derde verdieping. Hartelijk
dank voor de belangstelling en interesse de afgelopen jaren.
Lieve vrienden; Jeroen en Anke, Klaske en Pieter, Wietse en Annemarie, Marieke, Alies,
Maurits, Leony, Christiaan, Marco, Stephan, Eric en Derk Jan, dank voor jullie warme
belangstelling voor mijn onderzoek en de gezelligheid en biertjes in de kroeg en daarbuiten
welke voor de nodige afleiding hebben gezorgd.
Broertjes, lieve Janne, lieve Jauke, de afgelopen tijd hebben we weinig tijd gehad om
samen leuke dingen te doen. Toch hebben jullie altijd belangstelling getoond en tijdens
de familie aangelegenheden hebben we veel gelachen. Nu de drukke periode wat
verminderd is, kunnen we dit weer meer gaan oppakken.
Lieve pap en mam, jullie hebben me altijd gesteund in wat voor opzicht dan ook. Nooit
hebben jullie me gestuurd in dingen; jullie hebben me altijd vrijgelaten om mij mijn eigen
keuzes te laten maken. Maar, jullie gaven wel jullie visie en ideeën op de keuzes die ik
maakte en de manier waarop ik tegen dingen aankeek. Nooit heb ik daarbij het gevoel
gehad daarbij belemmerd te worden, maar juist heeft mij dat het gevoel gegeven van
‘altijd bij jullie terecht kunnen’. Jullie zijn er altijd voor me!
Lieve Kirs, jij bent degene die het proces van promoveren van dichtbij hebt meegemaakt.
Regelmatig kwam ik met stukken naar je toe met de vraag of je naar het Engels wilde
kijken. Gelukkig wilde je altijd tijd vrijmaken om me hierbij te helpen. Gelukkig hielp je me
ook bij het zien dat promoveren en werken als tandarts niet de enige bezigheden zijn die
optimale aandacht verdienen. Ironisch genoeg ben je nu zelf ook een promotieonderzoek
begonnen en ga je ook drukke tijden tegemoet. Je hebt me geholpen me te ontspannen
op de momenten dat dit nodig was. Met het afronden van dit proefschrift zal ik daar
ongetwijfeld meer tijd voor krijgen. En, zal ik zorgen dat jij ook aan je ontspanning komt.
Elke dag geniet ik van jouw aanwezigheid, je grappen en je mooie verschijning. Ik hoop
dat we samen nog veel mogen reizen en genieten van elkaar. I love you!
DA
NK
WO
OR
D
DA
NK
WO
OR
D
132
CURRICULUM VITAE
Jappe Buijs was born on November 18th 1980 in Purmerend, the Netherlands. After
finishing secondary school in 1999 at the ‘Baudartius College’ in Zutphen, he studied
Dentistry at the University of Groningen. During his study, in cooperation with other
faculty students, he founded the ‘dental faculty association Archigenes’ and took place in
the first board. He obtained his qualification as a dentist in 2004. Subsequently he started
his PhD research project. In January 1st 2008 he became partner in the private practice
‘de Boer Tandartsen’ in Groningen. Jappe is living together with Kirsten Slagter, dentist,
PhD-resident.