Embed Size (px)
Citation preview
FM 8-10-4
CHAPTER 5
UNIT-LEVEL HEALTH SERVICE SUPPORT
Section I. TYPE UNITS SUPPORTED
5-1. Mission and Functions
a. The mission and functions of unit-level(Echelon I) HSS elements are—
Prevention of disease and illnessthrough applied PVNTMED programs.
Acquisition and immediate treat-ment of the sick, injured, and wounded.
Clinical stabilization of the criticallyinjured or wounded.
Provision for routine medical care(sick call) and the immediate RTD of soldiers "fit tofight.‘‘
b. Echelon I HSS is reinforced by EchelonII and III HSS; each providing increased support tothe patient. During lulls in operations, unit-levelmedical personnel conduct tactical and technicalproficiency training. When required, they provideinstructions to nonmedical personnel in self-aid/buddy aid (first aid), CLS procedures, patientevacuation, field sanitation, and personal hygiene.
c. Unit level HSS within the division isprovided by organic medical elements assigned tocombat battalions, selected CS battalions, divisionheadquarters, CAB headquarters, and theDIVARTY headquarters. Their purpose is toprovide direct HSS to subordinate elements of theorganization. This support is provided by medicalplatoons or sections in the followingorganizations/units:
Armored Battalion—MedicalPlatoon, HHC.
Mechanized Infantry Bat-talion—Medical Platoon, HHC.
Infantry Battalion—MedicalPlatoon, HHC.
Division Artillery-Medical Section,Headquarters and Headquarters Battery (HHB).
Combat Aviation Brigade (CAB)–Medical Section, HHC.
Field Artillery Battalion (DirectSupport), DIVARTY–Medical Section,Headquarters and Headquarters and ServiceBattery (HHS).
Attack Helicopter Battalion, CAB–Medical Section, Headquarters and ServiceCompany.
Reconnaissance Squadron (RECONSQDN), CAB–Medical Section, Headquarters andHeadquarters Troop.
Infantry Division (Light)–MedicalSection, HHC.
d. The organic medical platoons andsections above are modular in design, and operatefrom mobile treatment shelters. They have organicvehicles which provide maximum deployability andmission responsiveness.
5-2. Area Support
Unit level HSS is provided on an area support basisto all organizations and units of the division withoutorganic HSS by medical companies of the FSB,MSB, or DISCOM medical battalion. Thesecompanies are located in the BSA and DSA.
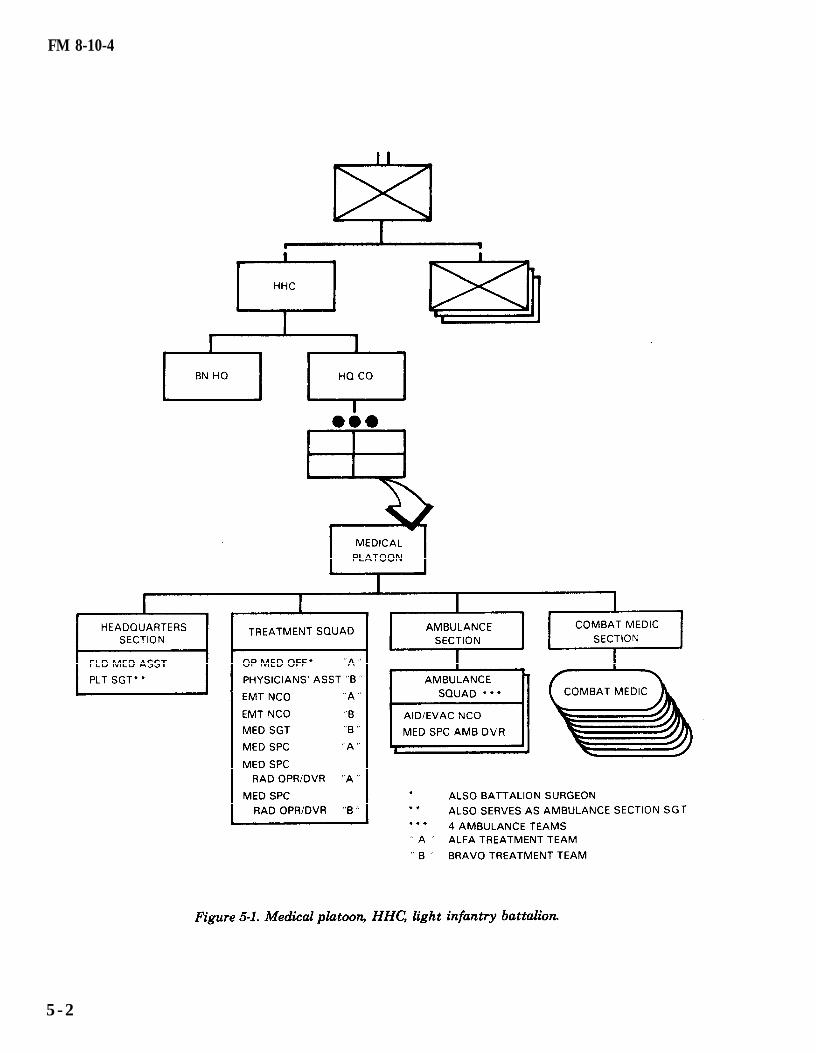
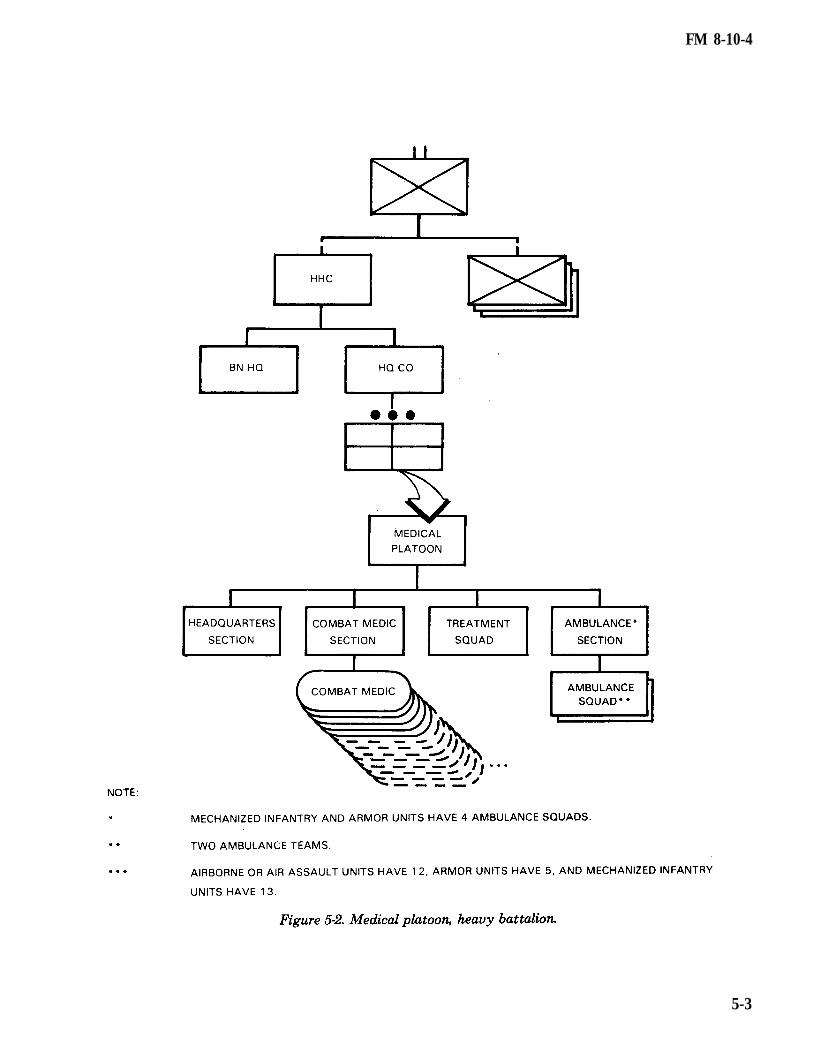
Section II. MEDICAL PLATOON5-3. Assignment headquarters section, a treatment squad (two
treatment teams), an ambulance section, and aA medical platoon is organic to each combat combat medic section. The medical platoon isbattalion HHC. The platoon is organized with a organized as shown in Figures 5-1 and 5-2.
5-1
FM 8-10-4
5 - 2
FM 8-10-4
5-3

FM 8-10-4
5-4. Battalion Surgeon
The battalion surgeon/medical platoon leader is themedical advisor to the battalion commander and hisstaff. He is the supervising physician (operationalmedicine officer) of the medical platoon treatmentsquad. This officer is responsible for all medicaltreatment provided by the platoon. His responsi-bilities include—
Planning and directing unit-level HSS forthe battalion.
Advising the battalion commander andhis staff on the status of the health of the command.
Supervising the administration, disci-pline, maintenance of equipment, supply functions,organizational training, and employment ofassigned or attached personnel.
Examining, diagnosing, treating, andprescribing courses of treatment for patients toinclude ATM.
Coordinating the establishment andtraining of patient decontamination teams.
Training CLS.
Supervising the battalion preventivepsychiatry program to include training troopleaders in the preventive aspects of stress onsoldiers.
Planning and conducting medical civicaction programs (MEDCAP), when directed.
5-5. Platoon Headquarters
a. The headquarters section, under thedirection of the battalion surgeon, provides for thecommand, control, communications, and logisticsfor the platoon. The platoon headquarters is mannedby the field medical assistant and the platoonsergeant. It is normally collocated with thetreatment squad to form the BAS. The commandpost includes the plans and operations functionsperformed by the field medical assistant. Theplatoon has access to the battalion wirecommunication network for communications withall major elements of the battalion and with
5-4
supporting units. Wireless communications for thissection consists of a tactical FM radio mounted inthe platoon headquarters vehicle. The medicalplatoon employs an FM radio network for HSSoperations (Figure 5-3). The headquarters sectionserves as the net control station for the platoon.
b. The field medical assistant, an MSCofficer, is the operations/readiness officer for theplatoon. He is the principal assistant to thebattalion surgeon for operations, administration,and logistics. The field medical assistantcoordinates HSS operations with the battalion S3and S4, and coordinates patient evacuation with thesupporting medical company. This officer serves asthe medical platoon leader in the absence of anassigned physician.
c. The platoon sergeant assists insupervising the operations of the platoon. He alsoserves as the ambulance section sergeant. This NCOprepares reports; requests general supplies as wellas medical supplies; advises on supply economyprocedures; and maintains authorized stockagelevels of expendable supplies. He supervises theactivities and functions of the ambulance section toinclude operator maintenance of ambulances andequipment; operations security (OPSEC); and EMT.
d. The PA is a warrant officer. He performsgeneral technical health care and administrativeduties. The PA is ATM qualified and works underthe clinical supervision of the medical officer. Heperforms the following duties:
FM 8-10-4
Establishes and operates a BAS orBAS minus (1 treatment team).
Treats, within his ability, sick orinjured patients. He refers those patients requiringtreatment beyond his capability to the supervisingphysician.
Provides initial resuscitation towounded personnel.
Conducts training for battalionpersonnel in first aid procedures (self-aid/buddy aid),CLS, field sanitation, evacuation of the sick andwounded, and the medical aspects of injuryprevention.
Assists in the conduct of thebattalion preventive psychiatry program, to includetraining troop leaders in the preventive aspects ofstress on soldiers.
Trains medical personnel in emer-gency medical procedures. See Appendix A for atraining procedures guide.
5-6. Treatment Squad
The treatment squad is the basic medical treatmentelement of the BAS. It provides routine medicalcare, triage, ATM, and tailgate medicine. Thissquad is staffed with an operational medicine officer(primary care physician/battalion surgeon), a PA,two EMT NCOs, and four medical specialists (referto Figure 5-1). The squad’s physician, PA, and EMTsergeants are all trained in ATM procedures,commensurate with their occupational positions/specialties.
5-7. Battalion Aid Station/Treatment SquadOperation
Battalion aid station is the generic term used indesignating the unit-level medical treatmentfacility.
a. The treatment squad can split into twotreatment teams and operate as two separate aidstations (BAS minus), normally not to exceed 24hours. In continuous operations, when operating for
longer periods, personnel efficiency and unitcapability will tend to deteriorate. Each teamemploys treatment vehicle(s) with two medicalequipment sets (MES); one trauma set and onegeneral sick call set. See Appendix D for an exampleof the treatment squad in the split team mode.
b. For communications, each treatmentteam uses a FM tactical radio and is deployed in themedical platoon’s operations net. However, undercertain tactical conditions the battalion S4 mayrequire BAS elements to use the S4 net.
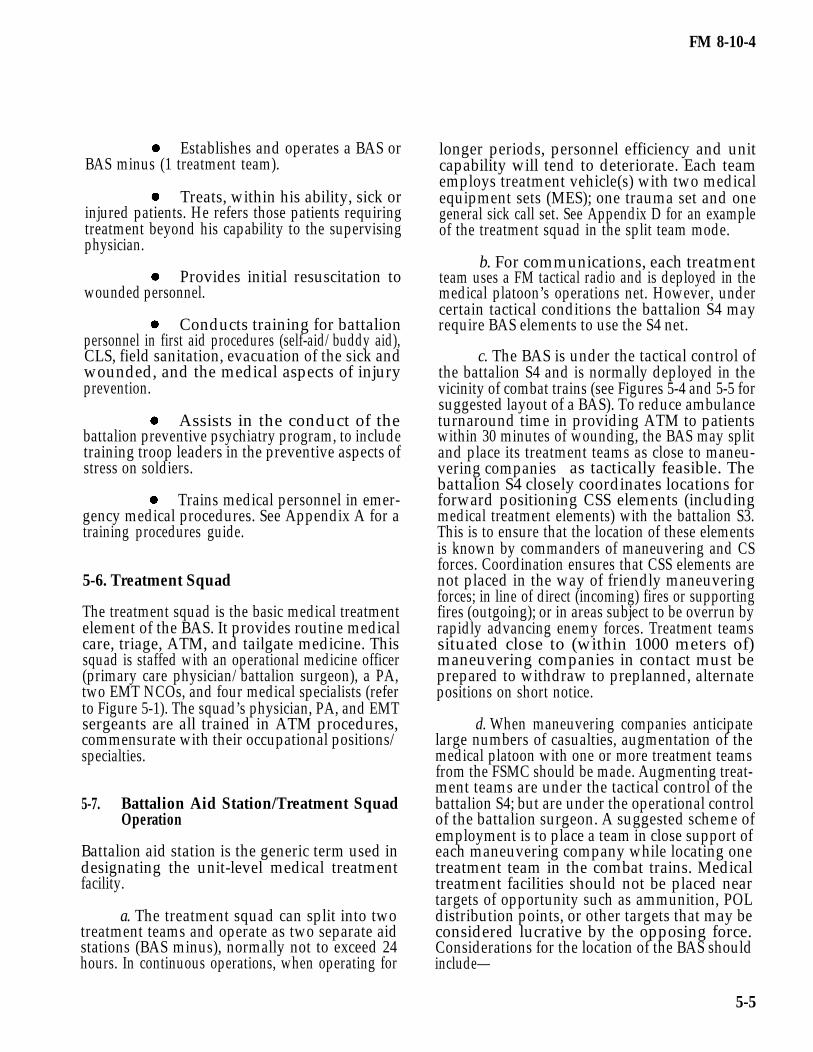
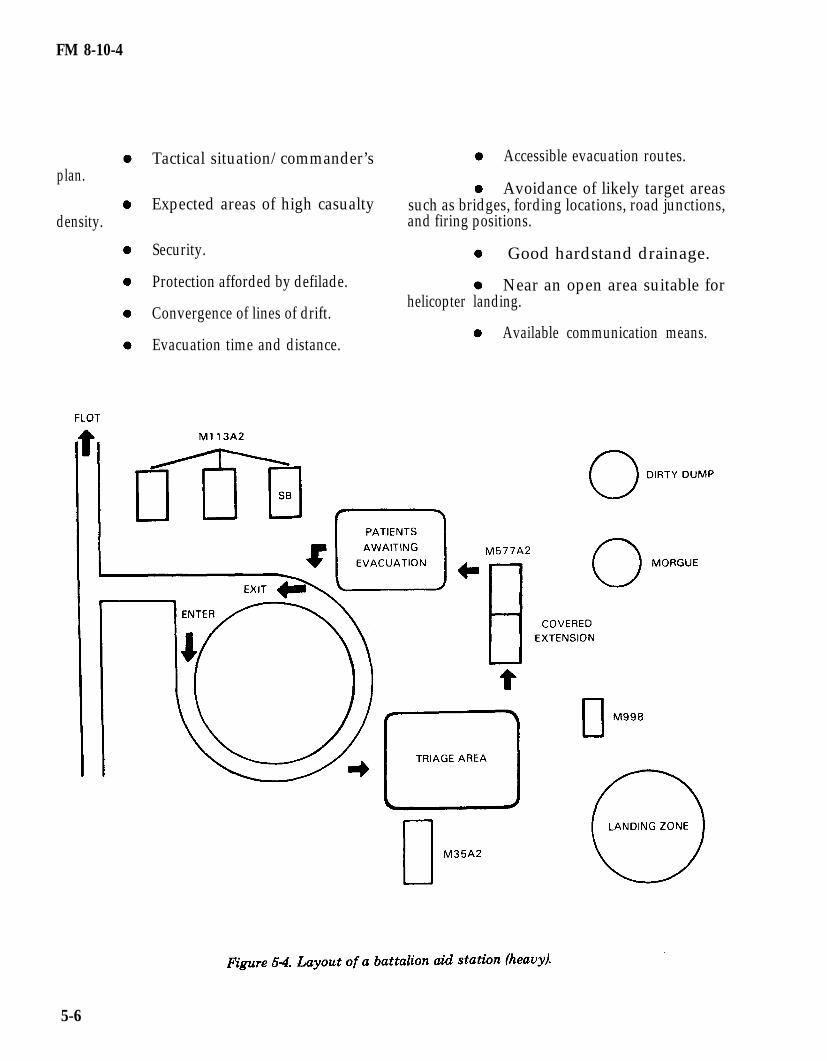
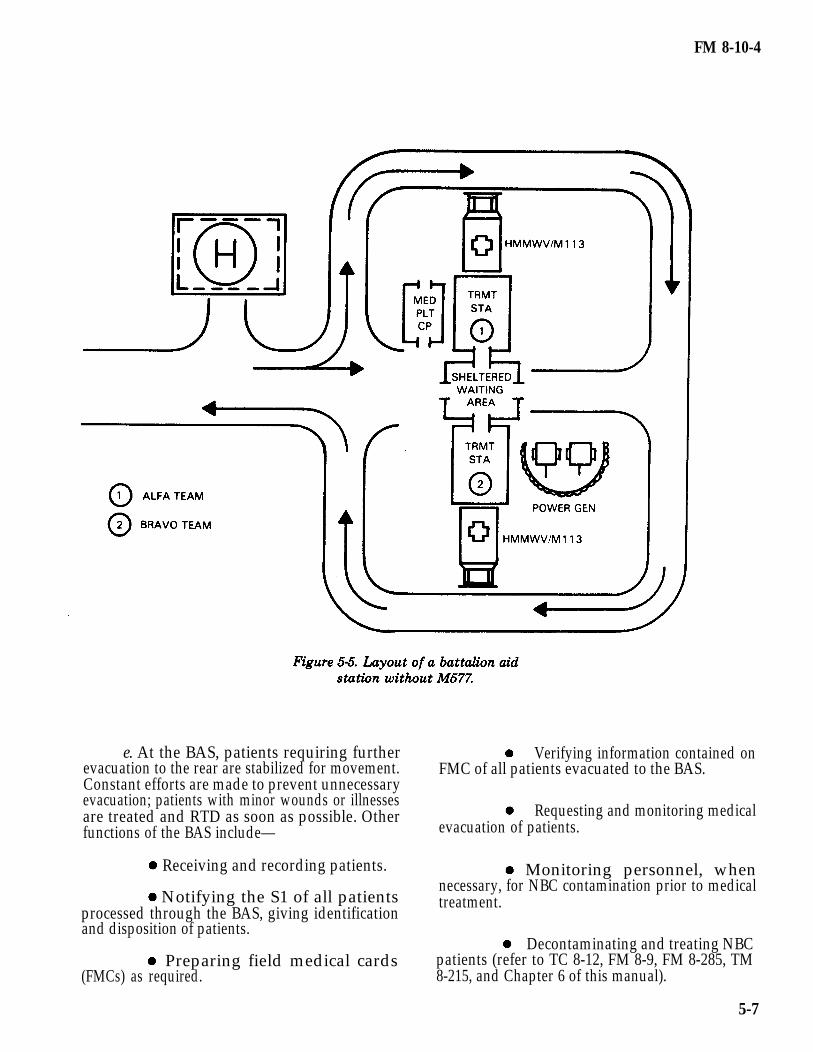
c. The BAS is under the tactical control ofthe battalion S4 and is normally deployed in thevicinity of combat trains (see Figures 5-4 and 5-5 forsuggested layout of a BAS). To reduce ambulanceturnaround time in providing ATM to patientswithin 30 minutes of wounding, the BAS may splitand place its treatment teams as close to maneu-vering companies as tactically feasible. Thebattalion S4 closely coordinates locations forforward positioning CSS elements (includingmedical treatment elements) with the battalion S3.This is to ensure that the location of these elementsis known by commanders of maneuvering and CSforces. Coordination ensures that CSS elements arenot placed in the way of friendly maneuveringforces; in line of direct (incoming) fires or supportingfires (outgoing); or in areas subject to be overrun byrapidly advancing enemy forces. Treatment teamssituated close to (within 1000 meters of)maneuvering companies in contact must beprepared to withdraw to preplanned, alternatepositions on short notice.
d. When maneuvering companies anticipatelarge numbers of casualties, augmentation of themedical platoon with one or more treatment teamsfrom the FSMC should be made. Augmenting treat-ment teams are under the tactical control of thebattalion S4; but are under the operational controlof the battalion surgeon. A suggested scheme ofemployment is to place a team in close support ofeach maneuvering company while locating onetreatment team in the combat trains. Medicaltreatment facilities should not be placed neartargets of opportunity such as ammunition, POLdistribution points, or other targets that may beconsidered lucrative by the opposing force.Considerations for the location of the BAS shouldinclude—
5-5
FM 8-10-4
plan.
density.
Tactical situation/commander’s Accessible evacuation routes.
Avoidance of likely target areasExpected areas of high casualty such as bridges, fording locations, road junctions,
and firing positions.
Security. Good hardstand drainage.
Protection afforded by defilade. Near an open area suitable for
Convergence of lines of drift.helicopter landing.
Available communication means.Evacuation time and distance.
5-6
FM 8-10-4
e. At the BAS, patients requiring furtherevacuation to the rear are stabilized for movement.Constant efforts are made to prevent unnecessaryevacuation; patients with minor wounds or illnessesare treated and RTD as soon as possible. Otherfunctions of the BAS include—
Receiving and recording patients.
Notifying the S1 of all patientsprocessed through the BAS, giving identificationand disposition of patients.
Preparing field medical cards(FMCs) as required.
Verifying information contained onFMC of all patients evacuated to the BAS.
Requesting and monitoring medicalevacuation of patients.
Monitoring personnel, whennecessary, for NBC contamination prior to medicaltreatment.
Decontaminating and treating NBCpatients (refer to TC 8-12, FM 8-9, FM 8-285, TM8-215, and Chapter 6 of this manual).
5-7
FM 8-10-4
NOTE
Patient decontamination(decon) is performed by apretrained decon team. Thisteam is composed of eightnonmedical personnel fromsupported units. Patient deconteams perform best when theytrain and exercise their skillswith the supporting BAS (seeAppendix E).
f. Evacuation from the BAS is performedby the FSMC’s ambulance platoon and by corps airambulance teams.
g. Patient holding and food service is notavailable at the BAS. Therefore, only proceduresnecessary to preserve life or limb, or enable a patientto be moved safely, are performed at the BAS.
h. Ammunition and individual weaponsbelonging to patients evacuated from the BAS aredisposed of as directed by command SOP/policy. Allexcess equipment collected at the BAS is disposedof by the battalion S4 or as directed by commandSOP.
NOTE
Patients will alwaysretain their protectivemask.
i. Patients requiring dental treatment areevacuated to the supporting medical companywhere emergency dental care is provided.
j. Patients requiring optometric servicesinitially report to the BAS. For those patientsrequiring only routine replacement of spectacles,necessary information is obtained from the indi-vidual and forwarded to the division optometrysection. The required spectacles are fabricated andforwarded to the BAS for issue to the patient. Foroptometry services other than routine repair orreplacement of spectacles, patients are transportedto the optometry section, located in the DCS.
5-8. Combat Medic Section
To foster good interpersonal relations and morale ofcombat troops, combat medics are attached tomaneuver companies on a continuing basis.However, during lulls in combat operations, theyshould return to the medical platoon forconsultation and proficiency training. Functions ofcombat medics are as follows:
Performs triage and EMT for the sick andwounded.
Arranges medical evacuation for litterpatients and directs ambulatory patients to patientcollecting points or to the BAS.
Initiates the FMC for the sick andwounded and, as time permits, prepares an FMC ondeceased personnel.
Screens, evaluates, and treats, within hiscapabilities, those patients suffering minor illnessesand injuries. He RTD those patients requiring nofurther attention.
Keeps the company commander and thebattalion surgeon (or the PA in the absence of thesurgeon) informed on matters pertaining to thehealth and welfare of the troops.
Maintains sufficient quantities of medicalsupplies to support the tactical situation.
Serves as a member of the unit fieldsanitation team. In this capacity, he advises thecommander and supervises unit personnel onmatters of personal hygiene and field sanitation(FM 21-10-1).
5-9. Ambulance Section
a. Medical platoon ambulances provideevacuation within the battalion. Ambulance teamsprovide medical evacuation and en route care fromthe soldier’s point of injury to the BAS. In masscasualty situations, nonmedical vehicles may beused to assist in casualty evacuation as directed bythe commander. Plans for the use of nonmedicalvehicles to perform medical evacuation should beincluded in the battalion’s tactical SOP.
5-8

FM 8-10-4
NOTE Director guide ambulatory patientsto the BAS.
Performing operatorsmaintenance on ambu-lances is an importantpart of each ambulanceteam’s duties.
b. Under the modular medical system, theambulance squad consists of two ambulance teams.
(1) The aid/evacuation NCO performs—
Triage and advanced EMTprocedures in the care and management of traumapatients.
Assists in the care andmanagement of battle fatigue patients.
Prepares patient for move-ment.
Provides patient care en route.
Maintains contact withsupported units.
Collects casualties.
Performs NBC detectionprocedures.
(2) The medical specialist/ambulancedriver is trained in EMT procedures. He operatesand maintains the ambulance and all on-boardequipment. He assists the aid/evacuation NCO inthe care and handling of patients.
c. Specific duties of the ambulance team areto—
Maintain contact with supportedelements.
Find and collect the wounded.
Administer EMT as required.
Initiate or complete the FMC.
Evacuate litter patients to the BAS.
Perform triage when necessary.
Provide Class VIII resupply tocombat medics.
Serve as messengers within medicalchannels.
d. The number of ambulance squads in asection varies and is based on the type of parentorganization. The infantry, airborne, and air assaultmaneuver battalions ambulance sections have twoambulance squads; each is equipped with highmobility multipurpose wheeled vehicle (HMMWV)ambulances. The heavy combat maneuverbattalions ambulance sections have eightambulance squads equipped with M-113 trackedambulances.
5-10. Employment and Functions of theAmbulance Team
a. The ambulance team is a mobile combatmedic team. Its function is to collect, treat, andevacuate the sick and wounded to the nearesttreatment station or AXP. For communications, theambulance team employs an FM tactical radiomounted on its assigned ambulance. The team isdeployed in the medical platoon’s operations net;however, in certain circumstances it may operate inthe S4 net or as established by the battalion SOI.
b. The ambulance teams routinely deploywith the maneuver company trains; however, itoperates as far forward as the tactical situationpermits, and frequently finds and treats patientswho have not been seen by the company medic. Thisteam, when operating in a company’s AO, is nor-mally under the tactical control of the company XOor first sergeant, but remains under the technicaland operational control of the medical platoon. Anambulance team is normally designated to support aspecific company. To become familiar with thespecific terrain and battlefield situation, the teammaintains contact with the company during mostcombat operations.
c. During static situations where thecompany is not in enemy contact or is in reserve, the
5-9
FM 8-10-4
team returns to the BAS to serve as back-upsupport for other elements in contact. However,during movement to contact, the ambulance teamimmediately deploys to its regularly supportedcompany. During combat operations, the team maydismount (leaving the ambulance in the trains area),find, treat, and move patients to safety, and laterevacuate them to the BAS. When moving patientsto the ambulance location, patient collecting point,or company aid post, the team is normally assistedby nonmedical personnel.
5-11. Medical Evacuation
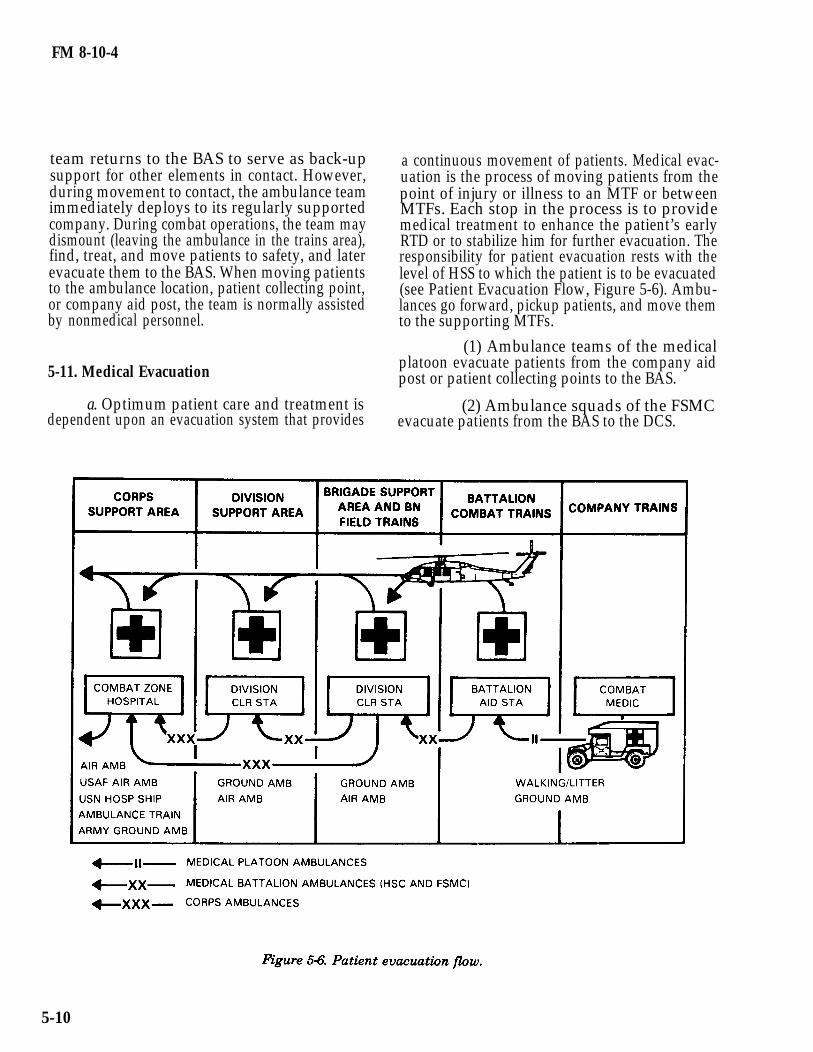
a. Optimum patient care and treatment isdependent upon an evacuation system that provides
a continuous movement of patients. Medical evac-uation is the process of moving patients from thepoint of injury or illness to an MTF or betweenMTFs. Each stop in the process is to providemedical treatment to enhance the patient’s earlyRTD or to stabilize him for further evacuation. Theresponsibility for patient evacuation rests with thelevel of HSS to which the patient is to be evacuated(see Patient Evacuation Flow, Figure 5-6). Ambu-lances go forward, pickup patients, and move themto the supporting MTFs.
(1) Ambulance teams of the medicalplatoon evacuate patients from the company aidpost or patient collecting points to the BAS.
(2) Ambulance squads of the FSMCevacuate patients from the BAS to the DCS.
5-10
FM 8-10-4
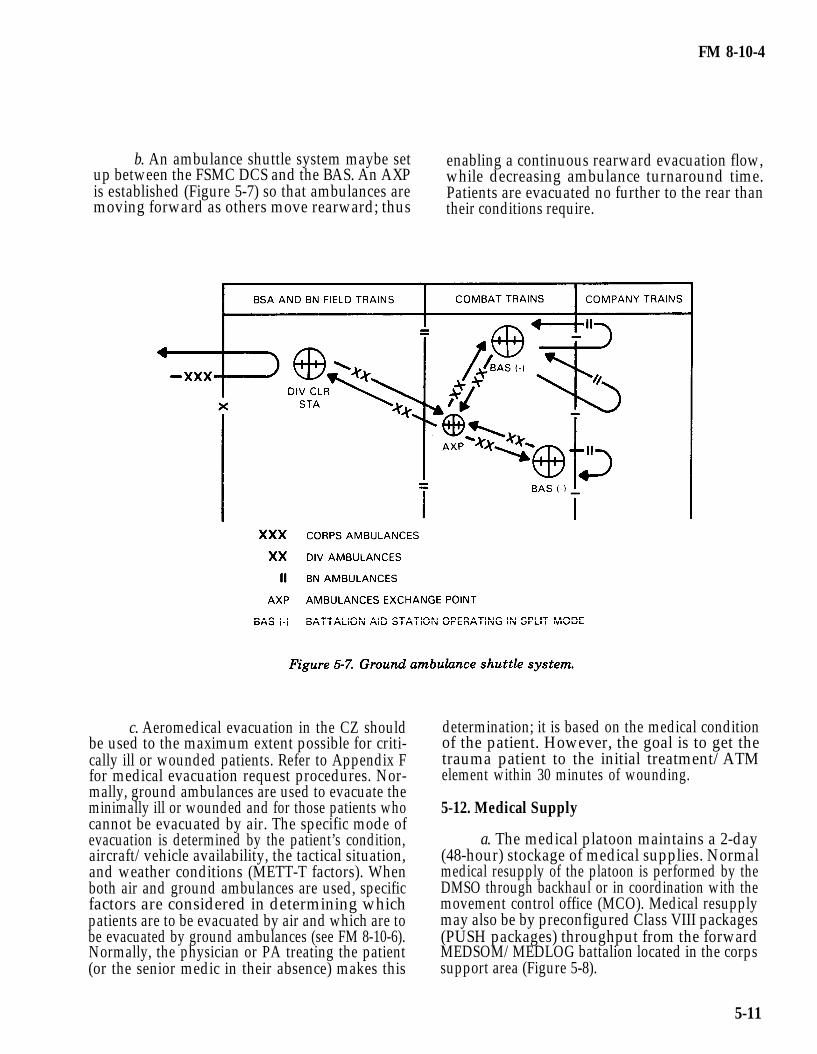
b. An ambulance shuttle system maybe set enabling a continuous rearward evacuation flow,up between the FSMC DCS and the BAS. An AXP while decreasing ambulance turnaround time.is established (Figure 5-7) so that ambulances are Patients are evacuated no further to the rear thanmoving forward as others move rearward; thus their conditions require.
c. Aeromedical evacuation in the CZ shouldbe used to the maximum extent possible for criti-cally ill or wounded patients. Refer to Appendix Ffor medical evacuation request procedures. Nor-mally, ground ambulances are used to evacuate theminimally ill or wounded and for those patients whocannot be evacuated by air. The specific mode ofevacuation is determined by the patient’s condition,aircraft/vehicle availability, the tactical situation,and weather conditions (METT-T factors). Whenboth air and ground ambulances are used, specificfactors are considered in determining whichpatients are to be evacuated by air and which are tobe evacuated by ground ambulances (see FM 8-10-6).Normally, the physician or PA treating the patient(or the senior medic in their absence) makes this
determination; it is based on the medical conditionof the patient. However, the goal is to get thetrauma patient to the initial treatment/ATMelement within 30 minutes of wounding.
5-12. Medical Supply
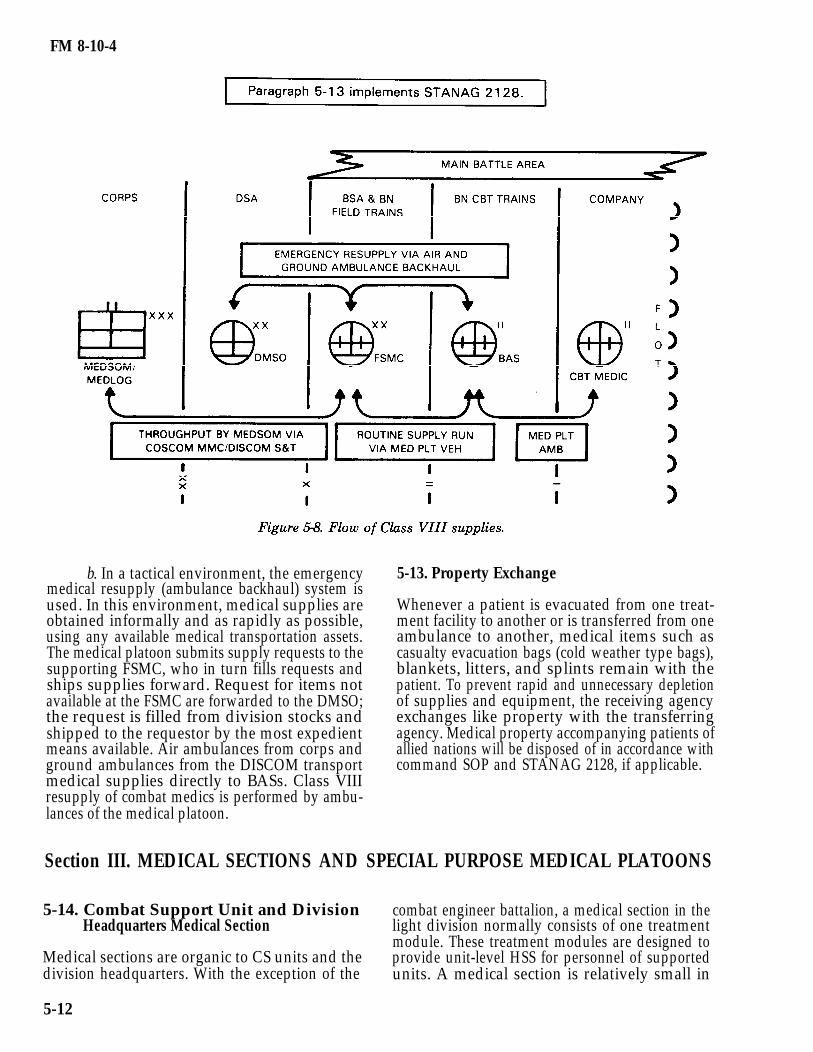
a. The medical platoon maintains a 2-day(48-hour) stockage of medical supplies. Normalmedical resupply of the platoon is performed by theDMSO through backhaul or in coordination with themovement control office (MCO). Medical resupplymay also be by preconfigured Class VIII packages(PUSH packages) throughput from the forwardMEDSOM/MEDLOG battalion located in the corpssupport area (Figure 5-8).
5-11
FM 8-10-4
b. In a tactical environment, the emergencymedical resupply (ambulance backhaul) system isused. In this environment, medical supplies areobtained informally and as rapidly as possible,using any available medical transportation assets.The medical platoon submits supply requests to thesupporting FSMC, who in turn fills requests andships supplies forward. Request for items notavailable at the FSMC are forwarded to the DMSO;the request is filled from division stocks andshipped to the requestor by the most expedientmeans available. Air ambulances from corps andground ambulances from the DISCOM transportmedical supplies directly to BASs. Class VIIIresupply of combat medics is performed by ambu-lances of the medical platoon.
5-13. Property Exchange
Whenever a patient is evacuated from one treat-ment facility to another or is transferred from oneambulance to another, medical items such ascasualty evacuation bags (cold weather type bags),blankets, litters, and splints remain with thepatient. To prevent rapid and unnecessary depletionof supplies and equipment, the receiving agencyexchanges like property with the transferringagency. Medical property accompanying patients ofallied nations will be disposed of in accordance withcommand SOP and STANAG 2128, if applicable.
Section III. MEDICAL SECTIONS AND SPECIAL PURPOSE MEDICAL PLATOONS
5-14. Combat Support Unit and Division combat engineer battalion, a medical section in theHeadquarters Medical Section light division normally consists of one treatment
module. These treatment modules are designed toMedical sections are organic to CS units and the provide unit-level HSS for personnel of supporteddivision headquarters. With the exception of the units. A medical section is relatively small in
5-12

FM 8-10-4
comparison to a medical platoon; therefore, it will organized as shown in Figure 5-9. Personnel staffingrequire augmentation from a supporting medical of this section includes a DIVARTY surgeon/company in mass casualty situations. operational medicine officer, a section sergeant/
EMT NCO, and two medical specialists.
5-15. Medical Section, HHB Division Artillery
a. Organizations and Functions. TheDIVARTY medical section/treatment team is
(1) DIVARTY Surgeon. leaders in the three FA battalions. Certainofficer is the medical advisor to the DIVARTY situations may require that the clinical supervisioncommander and his staff. He is the primary care of PAs in FA units be passed to the physician inphysician of the DIVARTY and is also the charge of the nearest supporting MTF. Suchsupervising physician for PA/medical section requirements, however, are coordinated through the
5-13
FM 8-10-4
division surgeon. The DIVARTY surgeon isresponsible for medical treatment provided byDIVARTY medical personnel (inclusive of medicalpersonnel assigned to FA battalions). His dutiesinclude—
Operating the DIVARTY aidstation.
Planning and directing unit-level HSS for members of the DIVARTYheadquarters and FA battalions.
Arranging for division-levelHSS.
Arranging for patient evac-uation to the DCS.
Supervising the administrationand maintenance of equipment, the supply function,technical training, and the employment of medicalpersonnel.
Examining, diagnosing,treating, and prescribing courses of treatment forpatients to include ATM for the trauma patient.
Coordinating patient evac-uation.
(2) Section Sergeant. The sectionsergeant, who is also an EMT NCO, assists themedical officer in accomplishing his duties andsupervises the medical specialists. He preparesreports, requests general and medical supplies,maintains supply economy procedures, andmaintains authorized stockage level of expendablesupplies. This NCO also performs triage and ATMprocedures in the care of trauma and NBC-insultedpatients, and care and management of battle fatiguepatients. He also performs routine patient care andNBC detection procedures. His duties furtherinclude—
Establishing and operating theDIVARTY aid station.
Maintaining the patientaccountability/casualty reporting system.
Maintaining medical equip-ment sets.
5-14
Conducting tactical andtechnical proficiency training for subordinatemembers of the section.
Conducting sanitation inspec-tions of troop living areas, food service areas, wastedisposal areas, and potable water distributionpoints and equipment.
(3) Medical Specialists. Thesespecialists assist the section sergeant inaccomplishing his duties. They perform triage andEMT. Their specific duties include—
Erecting and breaking downfield medical shelter systems, to includechemical/biological
(FMC).
disposition log.
assigned vehicle,
protective shelters.
Performing patient care.
Initiating patient records
Maintaining the patient daily
Operating and maintainingtactical radio, and power
generation equipment. (Also may serve as a memberon the battery field sanitation team.)
b. Employment. The medical sectionestablishes a BAS near the DIVARTYheadquarters and provides unit-level medicalservice for members of the DIVARTY headquartersand headquarters battery.
(1) The section employs a HMMWVtreatment vehicle, a cargo trailer, and two medicalequipment sets: one trauma treatment set and onegeneral sick call set.
(2) For communications, the sectionemploys a telephone set (TA 312/PT) and isdeployed in the HHB wire net. It employs an FMtactical radio and is deployed as designated by theDIVARTY SOI. This section also has access to thesupporting medical company’s tactical operationsnet to request division-level HSS.
c. Operations. Paragraph 5-7 describesBAS operations; these are equally applicable to the

FM 8-10-4
DIVARTY BAS. Figures 5-4 and 5-5 showsuggested layouts of a BAS.
d. Medical Evacuation. The DIVARTYHHB medical section has no medical evacuationassets. Evacuation of patients to and from theDIVARTY BAS is provided by the supportingmedical company in the DSA.
e. Medical Supply. The medical sectionmaintains a 2-day (48-hour) stockage level ofmedical supplies for the HHB. Routine requests formedical supplies are submitted through commandchannels to the DMSO. Supplies may be picked upby the requesting unit or forwarded to theDIVARTY BAS during routine ambulance runs.For emergency resupply procedures, see paragraph5-12 b.
5-16.
This
f. Property Exchange. See paragraph 5-13.
Medical Section, Headquarters andHeadquarters Support Company, DirectSupport Field Artillery Battalion
section is organic to the Headquarters andHeadquarters Support Company (HHS) of thedirect support (DS) FA battalions; it is organized asshown in Figure 5-10. Personnel staffing for thismedical section includes a section leader/PA, asection sergeant/EMT NCO, two medicalspecialists, and three combat medics (batteryaidmen).
a. Section Leader/Physicians’ Assistant.The PA is an advisor to the battalion commanderand his staff. He is the primary medical careprovider for the battalion and supervises allactivities of the medical section. The PA is trainedin ATM procedures and works under the clinicalsupervision of a medical officer. He is responsible tothe supervising physician for all treatment providedby medical personnel of theduties include—
EstablishingBAS.
section. His specific
and operating the
Planning and supervising unit-levelHSS and coordinating division-level HSS for thebattalion.
Treating, within his ability, patientsreporting to him.
Referring patients who requiretreatment beyond his capability to the supervisingphysician.
(ATM) for theProviding initial resuscitation
wounded.
Training medical personnel and CLSin emergency medical procedures.
b. Section Sergeant. This NCO assists thePA in accomplishing his duties. The specific dutiesof this NCO are the same as those described for themedical section sergeant in the DIVARTY HHB(refer to paragraph 5-15 a (2).
c. Medical Specialists. The duties andfunctions of these specialists are the same as thosediscussed in paragraph 5-15 a (3).
d. Combat Medics. Combat medics areallocated to a DS FA battalion on the basis of one toeach firing battery. The duties and functions ofcombat medics are described in paragraph 5-8.
e. Employment. The medical sectionestablishes a BAS near the DIVARTYheadquarters and provides unit-level HSS.
(1) The section employs a HMMWVtreatment vehicle, a cargo trailer, and two medicalequipment sets: one trauma treatment set and onegeneral sick call set.
(2) For communications, the sectionemploys a telephone set (TA 312/PT) and isdeployed in the HHS wire communications net. Italso employs an FM tactical radio and is deployed inthe net designated by the DIVARTY SOI. Thissection also has access to the supporting medicalcompany’s tactical operationsdivision-level HSS.
f. Operations. ParagraphBAS operation; these are equallyFA BAS. Figures 5-4 and 5-5layouts of a BAS.
net to request
5-7 describes aapplicable to theshow suggested
5-15

FM 8-10-4
g. Medical Evacuation. The FA battalion’s is provided by the supporting medical company inHHS medical section has no medical evacuation the BSA.assets. Evacuation of patients to and from the BAS
h. Property Exchange. See paragraph 5-13. (1) The flight surgeon (brigade surgeon)
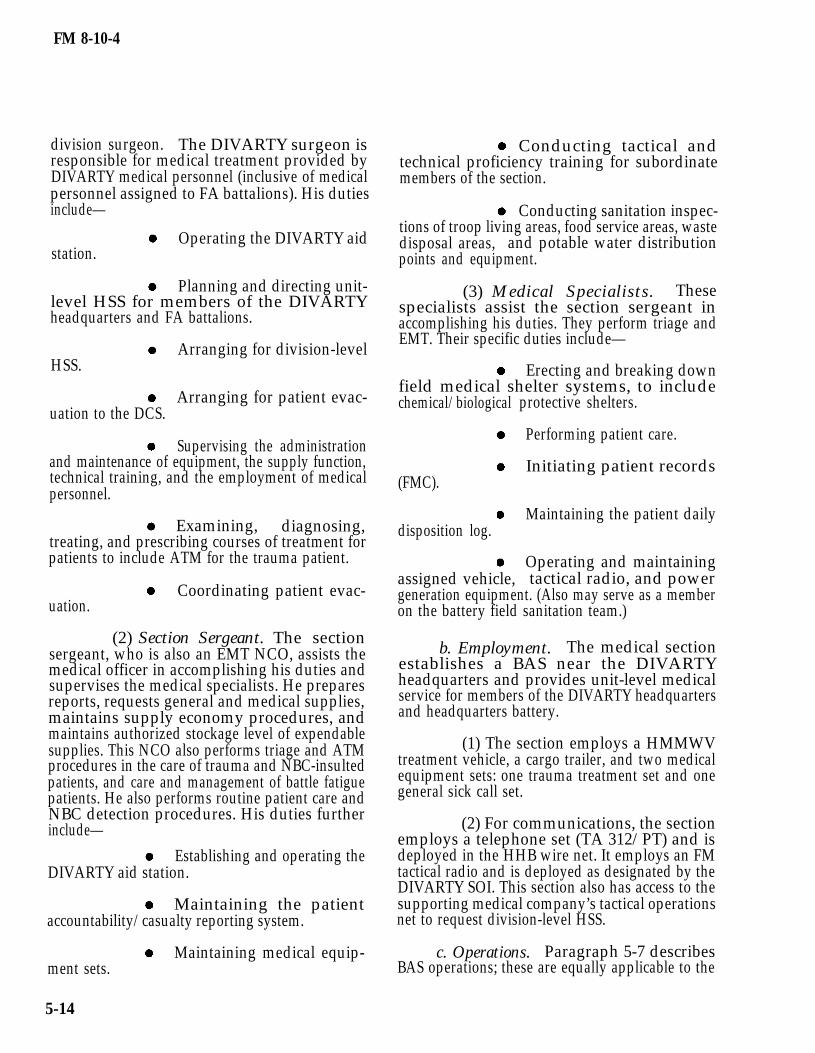
5-17. Medical Section, Headquarters and Head-quarters Company Combat Aviation Brigade/Combat Aviation Squadron
a. Organization and Functions. The CABmedical section is organized as shown in Figure5-11. Personnel staffing this section include a flightsurgeon, an assistant flight surgeon, a sectionsergeant/EMT NCO, and two medical specialists.
5-16
is the medical advisor to the CAB commander andhis staff. He is the primary care physician of thebrigade. The flight surgeon is responsible formedical treatment provided by the medical section(brigade aid station). His duties include—
Operatingstation.
Examiningthe medical qualification for
the brigade aid
and determiningflying status of
FM 8-10-4
aviators within the brigade headquarters; or Examining, diagnosing, treat-aviators referred to him by units without a flight ing, and prescribing courses of treatment forsurgeon. patients to include ATM for trauma patients.
Planning and directing unit-level HSS for members of the brigade headquarters.
Arranging for evacuation ofpatients to the DCS.
Arranging division-level HSS.
Supervising the administrationand maintenance of equipment, the supply function,technical training, and the employment of medicalpersonnel.
(2) The assistant flight surgeon assiststhe flight surgeon in performance of his duties. Heserves as the aviation brigade flight surgeon in theabsence of the flight surgeon. His duties include—
Examining and determiningthe medical qualification for flying status ofaviators within the brigade headquarters; oraviators referred to his treatment section by unitswithout a flight surgeon.
Examining, diagnosing, treat-ing, and prescribing courses of treatment forpatients to include ATM for trauma patients.
5-17
FM 8-10-4
b. Employment. See paragraph 5-15 b foremployment considerations.
c. Operations. Paragraph 5-7 describes aidstation operations; these are equally applicable tothe DIVARTY BAS. Figures 5-4 and 5-5 showsuggested layouts of a BAS.
d. Medical Evacuation. The brigade HHCmedical section has no medical evacuation assets.Evacuation of patients is provided by thesupporting medical company.
e. Medical Supply. See paragraph 5-12.
f. Property Exchange. See paragraph 5-13.
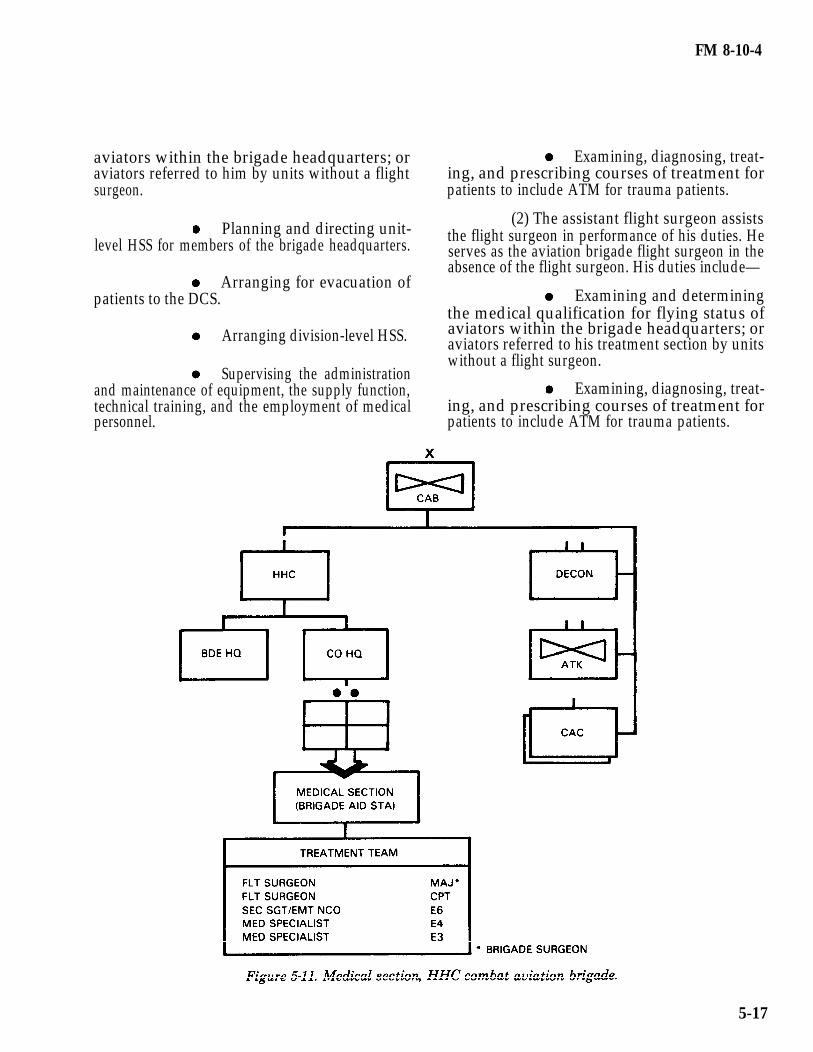
5-18. Medical Section, HHC Attack HelicopterBattalion, CAB.
a. Organization and Functions. The attackhelicopter battalion medical section is organized asshown in Figure 5-12. Personnel staffing this sectioninclude a section sergeant/EMT NCO, and twomedical specialists. For further explanation, seeparagraph 5-15 a.
b. Property Exchange. See paragraph 5-13.
5-18
FM 8-10-4
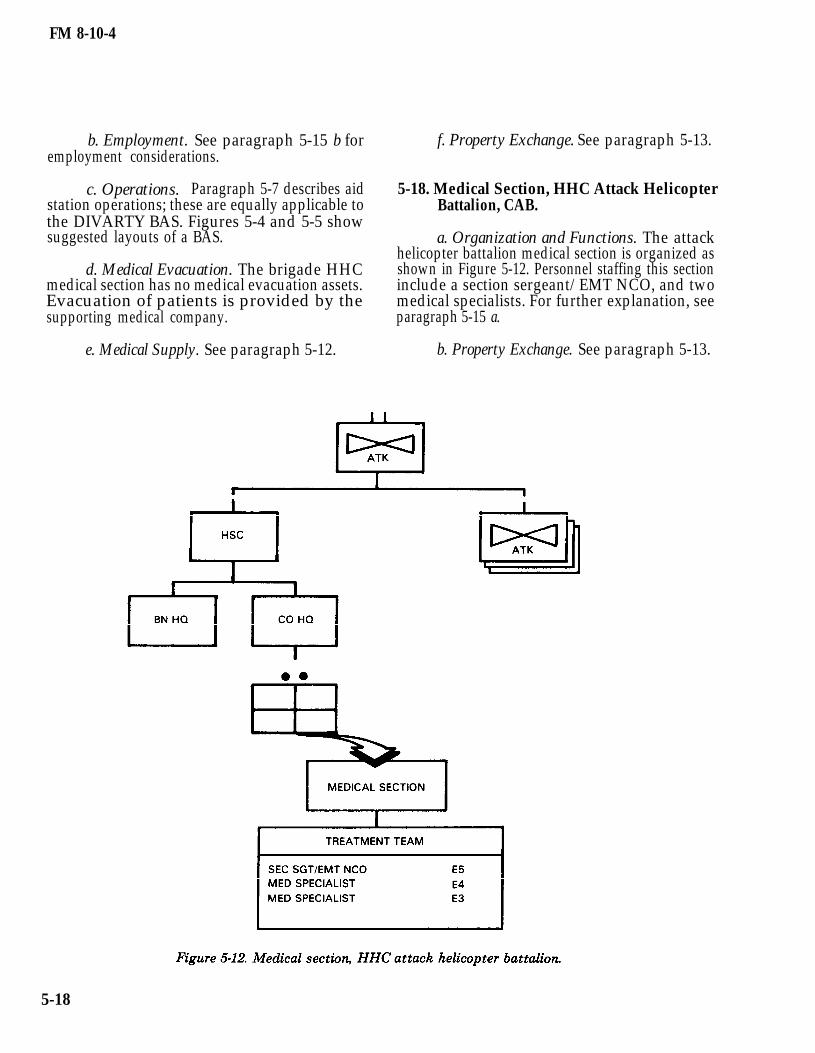
5-19. Medical Platoon, HHT Reconnaissance specialists, six combat medics, four aid evacuationSquadron, CAB. NCOs, and two aid evacuation specialists.
(1) For flight surgeon responsibilities,a. Organization and Functions. The HHT see paragraph 5-17.
reconnaissance squadron CAB medical platoon isorganized as shown in Figure 5-13. Personnel (2) The PA performsstaffing this platoon include a flight surgeon, a PA, health care and administrativea section sergeant/EMT NCO, two medical paragraph 5-5).
general technicalduties (refer to
5-19
FM 8-10-4
b. Section Sergeant. This NCO assists thePA in accomplishing his duties. The specific dutiesof this NCO are the same as those described for themedical section sergeant in the DIVARTY HHB(refer to paragraph 5-15 a (2).
c. Medical Specialists. The duties andfunctions of these specialists are the same as thosediscussed in paragraph 5-15 a (3).
d. Combat Medics. These aidmen areallocated to a squadron on the basis of one to eachfiring troop. The duties and functions of combatmedics are described in paragraph 5-8.
e. Ambulance Squad. Paragraph 5-10describes duties of ambulance squad members.
f. Employment. The medical sectionestablishes a BAS near the squadron headquartersand provides unit-level medical service for membersof the squadron.
(1) The section employs a HMMWVtreatment vehicle, a cargo trailer, and two medicalequipment sets: one trauma treatment set and onegeneral sick call set.
(2) For communications, the sectionemploys a telephone set (TA 312/PT) and isdeployed in the HHS wire communications net. Italso employs an FM tactical radio and is deployed inthe net designated by the squadron SOI. Thissection also has access to the supporting medicalcompany’s tactical operations net for requestingdivision-level HSS.
g. Operations. Paragraph 5-7 describes anBAS operation; these are equally applicable to thesquadron BAS. Figures 5-4 and 5-5 show suggestedlayouts of a BAS.
h. Medical Evacuation. Evacuation ofpatients from the BAS is provided by thesupporting medical company.
i. Medical Supply. The medical sectionmaintains a 2-day (48-hour) stockage level ofmedical supplies for the squadron. Routine requestsfor medical supplies are submitted through com-mand channels to the DMSO. Supplies may bepicked up by the requesting unit or forwarded to the
BAS during routine ambulance runs. For emergencyresupply procedures, see paragraph 5-12.
j. Property Exchange. See paragraph 5-13.
5-20. Medical Section, HHC DivisionHeadquarters
a. Organizations and Functions. The HHCdivision headquarters medical section is organizedas shown in Figure 5-14. Personnel staffing of thissection includes an operational medicine officer, asection sergeant/EMT NCO, two medicalspecialists, and two aid evacuation specialists.
(1) Operational medical officer. Theoperational medical officer is responsible for medicaltreatment provided by HHC medical personnel. Thespecific duties of this medical officer are the same asthose described in the DIVARTY HHB (refer toparagraph 5-15 a (l)).
(2) Section sergeant. Refer toparagraph 5-15 a (2).
(3) Medical specialists. Refer toparagraph 5-15 a (3).
(4) Aid evacuation team. Paragraph5-10 describes employment of ambulance teams.
b. Employment. The medical sectionestablishes a BAS near the division headquartersand provides unit-level HSS for members of thedivision headquarters and headquarters company.
(1) The section employs a HMMWVtreatment vehicle, a cargo trailer, and two medicalequipment sets: one trauma treatment set and onegeneral sick call set.
(2) For communications, the sectionemploys a telephone set (TA 312/PT) and isdeployed in the HHB wire communications net. Italso employs a FM tactical radio and is deployed inthe net designated by the division SOI. This sectionalso has access to the supporting medicalcompany’s tactical operations net to requestdivision-level HSS.
5-20

FM 8-10-4
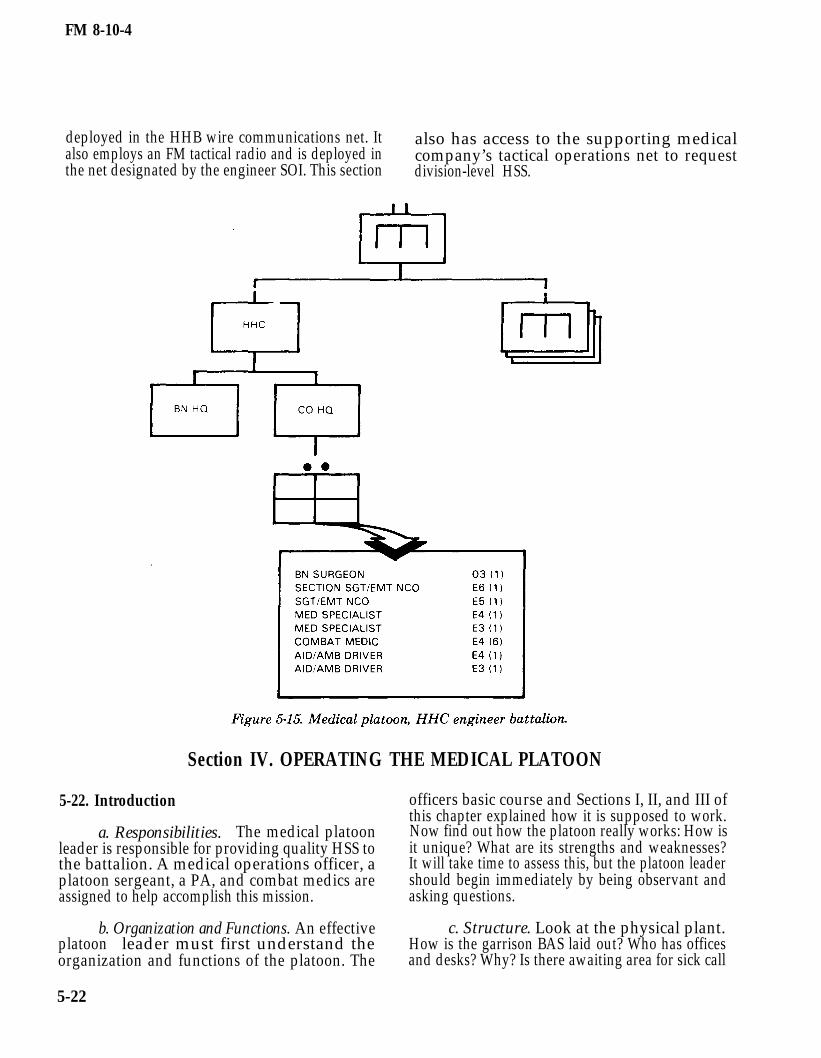
5-21. Medical Platoon, HHC Combat EngineerBattalion
a. Organization and Functions. The combatengineer battalion medical platoon is organized asshown in Figure 5-15. Personnel staffing this sectioninclude an operational medical officer, a sectionsergeant/EMT NCO, a emergency medical NCO,two medical specialists, six combat medics, and twoaid evacuation specialists. The operational medicalofficer (battalion surgeon) is the medical advisor tothe combat engineer battalion commander and hisstaff. He is the primary care physician of thebattalion. He is responsible for medical treatmentprovided by the medical platoon. The specific dutiesof this medical officer are the same as thosedescribed in the DIVARTY HHB (refer toparagraph 5-15 a (l).
b. Section Sergeant. Refer to paragraph5-15 a (2).
c. Medical Specialists. Refer to paragraph5-15 a (3).
d. Combat Medics. The duties and functionsof combat medics are described in paragraph 5-8.
e. Aid Evacuation Specialist. The duties ofthe aid evacuation specialist are described inparagraph 5-10.
f. Employment. The medical sectionestablishes a BAS near the engineer battalion andprovides unit-level HSS.
(1) The section employs a HMMWVtreatment vehicle, a cargo trailer, and two medicalequipment sets: one trauma treatment set and onegeneral sick call set.
(2) For communications, the sectionemploys a telephone set (TA 312/PT) and is
5-21
FM 8-10-4
deployed in the HHB wire communications net. It also has access to the supporting medicalalso employs an FM tactical radio and is deployed in company’s tactical operations net to requestthe net designated by the engineer SOI. This section division-level HSS.
Section IV. OPERATING THE MEDICAL PLATOON
5-22. Introduction
a. Responsibilities. The medical platoonleader is responsible for providing quality HSS tothe battalion. A medical operations officer, aplatoon sergeant, a PA, and combat medics areassigned to help accomplish this mission.
b. Organization and Functions. An effectiveplatoon leader must first understand theorganization and functions of the platoon. The
officers basic course and Sections I, II, and III ofthis chapter explained how it is supposed to work.Now find out how the platoon really works: How isit unique? What are its strengths and weaknesses?It will take time to assess this, but the platoon leadershould begin immediately by being observant andasking questions.
c. Structure. Look at the physical plant.How is the garrison BAS laid out? Who has officesand desks? Why? Is there awaiting area for sick call
5-22
FM 8-10-4
patients? Is it adequate? Where are patientsscreened? Where does the PA see patients? Arethere exam tables? Does the layout make the bestuse of the available space? Is the lighting adequate?Where are medical records maintained and are theysecure? Where are the sets, kits, and outfits (SKOs)kept? Where are the medical supplies kept? Is theaid station clean? Does it need to be painted?
d. Getting to Know the Platoon.
How do assigned soldiers interact?Are they cohesive? Who are the informal leaders?Ask the S3 how the platoon performed on the lastArmy Training Evaluation Plan (ARTEP); how itdid at Combat Training Center (CTC); how itperformed on other major field training exercises.What does the HHC commander think of theplatoon? What does the HHC first sergeant think ofit? Are the line company commanders satisfied withthe HSS they are receiving? What does thebrigade’s medical company commander think of theunit? What are the division surgeon’s/DMOC’sevaluations? Is the battalion commander satisfiedwith the HSS he is receiving?
These are just some of the manyquestions a platoon leader should begin to answer.As he becomes familiar with the platoon, he will findother areas which need attention. The key is toLEARN!
Mistakes are part of the learningprocess. A platoon leader should not be afraid tomake mistakes; however, the key is to learn frommistakes and not make the same one twice.
e. Personnel. A platoon leader must get toknow his platoon members.
(1) Medical operations officer. What isthe medical operations officer’s background? Whatwere his previous assignments? Has he participatedin operational planning for employment of medicalunits? Does he understand tactical operationalprocedures and maneuvers? Can he organize unitloading plans for best support operations? Does heunderstand the Army Equipment MaintenanceProgram? Does he have a working knowledge ofgeneral and medical supply operations? How doeshe get along with other members of the platoon?Does he train personnel in administrative,
maintenance, and logistical procedures? Does heprovide tactical training for platoon personnel?
(2) Platoon sergeant. What is theplatoon sergeant’s background? What were hisprevious assignments? How long has he been in theunit? What is his education level? Is he EMTcertified? Does he have the EFMB? What did hescore on his last SQT? Is he physically fit? Does hepossess a good military appearance? What is hismanagement style? How do the soldiers react tohim? How does he see his role? What does he thinkof his own previous performance? What does hethink of the platoon? What does he expect of theplatoon leader? How does he see the leader’s role?The platoon sergeant-platoon leader relationship isvital, especially knowing, understanding, andtrusting one another. If the platoon sergeant isgood, learn from him. If he is mediocre, push him. Ifhe is bad, counsel him (document the counseling andcoordinate further actions with the HHCcommander).
(3) Physicians’ assistant. Many of thesame questions asked of the platoon sergeantshould be asked of the PA. Many of the sameobservations should be made. Additionally, anattempt should be made to evaluate the PA’stechnical expertise. Does he train the medics? Doeshe “teach” the medics? How does he handle himselfwith patients? The brigade surgeon should be askedfor his evaluation of the assigned PA; the platoonleader should keep the brigade surgeon informed ofhis impressions of the PA, positive or negative.
(4) Combat medics. Why are theymedics? Why are they in the Army? What do theythink of the platoon? Do they have EMT/EFMBcertifications? Can they read a map? Can they use aradio properly? How did they score on their lastSQT? How did they score on their last ArmyPhysical Readiness Test (APRT)? Married?Children? Previous assignments? Age? How is theirhaircut, uniform, weight? Do they want to stay inthe Army? What is their job (in their own words)?How do they like their jobs? Are they satisfied withtheir own performance? What are their goals?
f. Transportation. Getting to know thevehicles.
(1) Status. Does the platoon have all thevehicles it is authorized? If not, why? Do the
5-23
FM 8-10-4
vehicles have communications (commo)? Does itwork? What is the maintenance status of thevehicles? Are they generally well maintained? (Askthe XO or motor sergeant.) Are the vehicles paintedwith the appropriate color scheme? Do they havethe Geneva emblem?
(2) Preventive maintenance checks andservices. Have the platoon sergeant teachpreventive maintenance checks and services(PMCS) for each of the assigned vehicles using the-10 technical manual standards. Spend a Saturdaymorning doing this if necessary. Get with the motorsergeant or XO and become familiar withmaintenance procedures. Spend time in the motorpool every day. Learn to operate all of the vehicles.The more knowledge the platoon leader has aboutmaintenance in general and the status of each of theassigned vehicles, the better off the platoon will be.
g. Learn Standard Procedures. A platoonleader must familiarize himself with the unit’sSOPs; the tactical SOP, administrative-logisticsSOP, and maintenance SOP. What additional SOPsdoes the platoon use; sick call, deployment,maintenance, training, and Medical ProficiencyTraining Program (MPTP)? Are the SOPs adequate.Are they simple and understandable?
operations, visit other aid stations to see how theyconduct sick call. A sequence in which sick call maybe conducted is—
Patient reports to the aid stationwith a sick slip (DA Form 689) signed by hiscompany commander/representative.
The patient is met at reception desk;a medic takes the sick slip, and directs the patient toa seat in the waiting area.
Receptionist “logs patient in” usingsome type of aid station log book.
Receptionist pulls patient’s healthrecord (HREC) from the file and annotates the dateand patient’s unit of assignment on a SF 600(Health Record-Chronological Record of MedicalCare).
Receptionist places a sign-out card(OF 23) in place of the HREC in the file drawer.
Receptionist places patient’s sickslip in HREC folder and gives HREC to medicdesignated to take vital signs.
Prior to taking vital signs, medicensures that the SF 600 is filled out correctly.
5-23. Garrison OperationsMedic calls for patient by name.
a. Routine Activities. The primary job forsoldiers is to be prepared for war. They prepare forwar by training, which means frequent fieldexercises. Field exercises are vitally important;however, the majority of most soldiers’ time is spentin garrison. The manner in which routine garrisonactivities are conducted is indicative of the waysoldiers will perform during training exercises andin combat. Run a tight ship in garrison; it will paybig dividends in combat.
b. Battalion Aid Station Administration.Sick call is a daily activity which usually takes placefirst thing in the morning. It is normally scheduledfor 1 hour, starting between 0530 and 0730. There isno standard method of conducting sick call. An aidstation should have a sick call SOP which explainsthe unit’s sick call procedures. Review the SOP withthe PA and other members of the unit to ensuretheir satisfaction with it. To improve your
Medic checks vital signs and recordsthem on the SF 600.
Medic obtains patient history,performs evaluation, and records the information onSF 600. Medic must sign the entry.
Physician/PA reviews the record,discusses the case with the medic, and either treatsthe patient or directs the medic as to propertreatment. Physician/PA makes notes asappropriate and countersigns the SF 600.
Patient is treated/medicationsdispensed.
Patient is returned to duty (RTD),put on quarters, or sent to troop medical clinic(TMC).
5-24

FM 8-10-4
Receptionist “signs patient out” inlog book.
NOTE
When physician/PA is notpresent, medics may useDA Form 5181-R (Screen-ing Notes of AcuteMedical Care [ LRA ] ) inaccordance with instruc-tions to evaluate patientand countersign notes.
c. Medical Records Administration.
(1) Purpose.
The HREC is a permanent andcontinuous file which is begun when a soldier entersthe service. The records kept in it are prepared asthe member receives medical and dental care ortakes part in research.
The primary purpose of theHREC is to ensure that AMEDD personnel have aconcise but complete medical history of everyone onactive duty or in a Reserve Component.
(2) Terminal digit filing system.
(a) Medical record folders (DAForm 3444-series) are 10 differently colored folders.The color of the folder represents the last two digits(the primary group) of the patient’s social securitynumber (examples: orange folder—00-09; lightgreen—10-19). Using the terminal digit filingsystem (TDFS), HRECs are filed with those of likecolor.
(b) Under the TDFS, the sponsor’s(soldier’s) SSN is divided into three groups. Recordsare filed using the last two groups; these are the lastfour digits of the social security number. The lasttwo digits are known as the primary group; thenext-to-last two digits are the secondary group.Records are arranged first by their primary groupnumbers, resulting in folders of like colors beingfiled together. Within each primary group, therecords are arranged in order of their secondarygroup numbers. Within the secondary group,
records are filed numerically by the first five digitsof the SSN.
(3) Policies and procedures. ArmyRegulation 40-66 sets policies and procedures forpreparing and using Army medical records. Theseregulations should be read and kept handy. Theyprovide the "what" and "how to" of medical recordsadministration.
(4) Inventories and records review.HRECs should be inventoried monthly foraccountability and quarterly for compliance withAR 40-66. When conducting the quarterly review ofHRECs, medics should ensure the following criteriaare met:
Medical records jacket is filledout correctly (AR 40-66).
All forms in the medical recordare in correct order as shown in AR 40-66.
The privacy act statement (DDForm 2005) which is printed on the inside (back) ofthe DA Form 3444-series jacket is signed and datedas required by AR 40-2.
A completed SF 88 and SF 93(as required) are in the medical record and have aphysician’s signature (AR 40-501).
Medical records for personnelwith allergies are identified with DA Label 162 anda DD Form 3365 present (AR 40-15).
Ensure that DA Form3444-series record jackets are being used for activeduty personnel. This includes all temporary/newmedical records.
Immunizations are recorded inthe medical record and in the PHS-731 as prescribedin AR 40-66.
Ensure that immunizations aregiven to all personnel in accordance with AR 40-562and as directed by the surgeon.
Ensure that TB Tine testshave been administered with every periodic physical(AR 40-26).
5-25
FM 8-10-4
Ensure that at least one set offitted earplugs is in the soldiers’ possession uponarrival.
Ensure that service member’sblood type is entered on front of medical recordjacket (AR 40-66).
Determine if personnel whowear glasses need CB mask inserts ordered, or needa new prescription if the last one is over 2 years old?
Ensure laboratory reports andx-ray report forms are mounted on their respectivedisplay sheets.
Ensure that the medical recordjacket has the correct tape coding (AR 40-66).
Ensure medical records re-moved from the files are accounted for by use of asigned card (OF 23).
Records for personnel who PCS(Permanent Change of Station) or ETS (ExpirationTerm of Service) are logged in the PCS/ETS book.
Medical record files arescreened at least quarterly (AR 40-66).
5-24. Medical Assemblage and Equipment SetsManagement
a. Assemblage. Medical assemblagemanagement is not a difficult task. Yet, this is onearea in which medical platoon leaders frequently runinto trouble. Failure to account for materiel isinexcusable. The best way to prevent accountabilityproblems is to become thoroughly familiar with theproperty management system and then use it. Themedical platoon leader is accountable for thesupplies and equipment issued to the platoon. Themedical platoon leader has supervisoryresponsibility for all property; he may be held liablefor damage or loss even if he has not signed for anyproperty.
b. Equipment Sets. The medical equipmentset (ME S), frequently referred to as sets, kits, andoutfits (SKO), provides the capability for the
medical platoon to perform its mission. The MEScontains the medical supplies and equipment used inproviding HSS to the battalion. It is contained inmetal chests which are stored in the BAS.
(1) Types of sets. There are two types ofmedical equipment sets: service-unique MES andmulti service MES. The set issued to the battalionmedical platoon is a service-unique MES. It ismanaged by the Army Medical Department andconsists of medical and nonmedical items under asingle stock number. Service-unique MES areidentified in Volume I of the Department of Defense(DOD) medical catalog. Revisions to components ofthe MES are published annually in the supplybulletin (SB) 8-75 series. The supply bulletinrevisions constitute authority for updatingassemblages.
(2) Component accountability. Themedical platoon MES (National Stock Number6545-00-457-6858) consists of expendable, durable,and nonexpendable items. It is important tomaintain control of all types of supplies; however,property accounting records of nonexpendableitems must be kept. DA Pamphlet 710-2-1 explainsprocedures to use in maintaining these records.
(3) Inventory. Components of the MESare inventoried at least every six months and aftereach FTX. This is done to maintain accountability yand assure readiness. During the inventory, aserviceability inspection is also conducted. Replaceobsolete, deteriorated, and outdated items; repair orreplace unserviceable items. Ensure that the MESstorage area provides adequate security and protec-tion from extreme temperatures.
(4) Control of medications.
(a) A DD Form 4998-RControl and Surveillance Records for TOEAssemblages) is prepared for each dated
(QualityMedicalitem of
medical supply. Inventory these medicationsregularly to ensure 100 percent accountability.Check with the DMSO and ask for the local proce-dures for drug rotation. The DMSO should allowrotation of medications which are nearing theirexpiration date (example: 90 days from expiration).Effective drug rotation requires management ofquality control cards and coordination with the
5-26

FM 8-10-4
DMSO. It increases the efficiency of the medicalsupply system and saves battalion budget dollars.
(b) Controlled medical items(scheduled drugs) may not be stored at the BASduring peacetime. However, a prepared DA Form2765-1 (Request for Issue or Turn-in), less documentnumber, with an 06/05 priority designator forrequired medications (code R&Q items) ismaintained. The DMSO will fill these requests uponnotification of the unit’s deployment.
(c) Expired stocks of medicalsupplies and items determined to be unsafe orunsuitable for use will be destroyed in accordancewith AR 40-61. Destruction is normally accom-plished at the DMSO, not the BAS; usually on amonthly basis and requires a DA Form 3161(Request for Issue or Turn-in) from the supportedunit.
5-25. The Division Medical Supply System
a. Health Services Materiel Officer. TheHSMO is a special staff officer who providesmedical logistical support to the division. Thissupport is in the form of both medical supply andmaintenance of medical equipment. The HSMO alsoprovides advice and assistance on matterspertaining to medical materiel. The HSMO is amember of the division medical supply section of theMSMC.
b. Mission. In peacetime, the DMSOresupplies the DISCOM medical companies and thedivision medical platoons using supply pointdistribution. (This means supported units pick upsupplies from the supply point.) The Class VIIIsupply point (DMSO warehouse) is normally locatedin the MSMC’s AO. Each supported unit has asupply account with the DMSO. Routine supplyrequests come from the supported unit directly tothe DMSO. However, requests for nonexpendableitems must go through the requestor’s unit propertybook officer (PBO). Refer to the battalion SOP forspecific procedures.
c. Receipt for Supplies. To establish a ClassVIII supply account, the supported unit mustprovide the DMSO a DA Form 1687 (Notice ofDelegation of Authority-Receipt for Supplies). TheDA Form 1687 is prepared in accordance with AR
710-2 and AR 40-61. A new DA Form 1687 must besubmitted upon change of approving authority;upon the addition or deletion of a designatedindividual; or at a minimum, every 12 months. Onlythose individuals designated on the DA Form 1687are authorized to receipt for medical supplies.
d. Request Document. The DA Form 2765-1is used to request medical supplies. Informationneeded to complete this form can be found in theArmy Master Data File (AMDF). The originalcompleted DA Form 2765-1 should be given to thePBO/DMSO. The BAS should retain the third copy(flimsy) of the DA Form 2765-1 in a due-in statusfile.
e. Durable Items. Request for durable itemsof medical supply are handled in much the sameway. Some additional documentation, such as amemorandum explaining why the item is needed, isnormally required for durable items. Request fordurable medical items are sent from the unit supplyroom to the DMMC. Upon receipt of the item, theDMMC notifies the unit supply room and adesignated individual from the unit receipts for theitem. The item is then placed on the unit’s propertybook (hand receipt) and issued to the medicalplatoon.
f. Document Register. The BAS mustmaintain a DA Form 2064 (Document Register)which lists all medical supply transactions. Thedocument register should be kept in accordancewith DA Pam 710-2-1 and should be reconciledmonthly. The DMSO can provide assistance inestablishing or reconciling the document register.
g. Priority Designator System. In medicalsupply, a priority designator system is used toestablish priority for requested supplies. Thepriority designators authorized for use are the sameas used in requesting other classes of supplies.Priority designators and their uses are—
13 (12 in USAREUR and someCONUS units) —this number is used for all normalsupply transactions.
06 (05 in USAREUR and someCONUS units) —this number is used for itemswhich, by their absence, cause a unit’s mission to be
5-27
FM 8-10-4
impaired. The DMSO will attempt to immediatelyfill an 06/05 request. The company commander ofthe requesting unit must sign the back of the DAForm 2765-1 for 06/05 requests.
03 (02 in USAREUR and someCONUS units) —this is the highest priority availablefor medical supplies and denotes a life or limbemergency. Supply requests with an 03/02 prioritymust be signed by a physician and authenticated bythe battalion commander of the requesting unit. TheDMSO will immediately fill an 03/02 request. If theitem is not available, the DMSO stops all otheractivity and uses every available means to securethe needed item. Thousands of dollars may beexpended to get the high priority item to thelocation in which it is needed by the most rapidmeans; therefore, ensure that the correct prioritydesignator is used on a supply request.
h. Excess Materiel. It is important thatunits not maintain more medical supplies than theyare authorized. However, situations arise where aunit acquires excess supplies. Turn in these suppliesto the DMSO using a DA Form 2765-1. Check withthe DMSO for local policies governing the turn-in ofexcess medical materiel.
5-26. Immunizations
a. Responsibility. Commanders areresponsible for assuring that all unit personnelreceive required immunizations and that records ofsuch immunizations are maintained.
b. Immunization Records. Soldiers areissued PHS Form 731 (International Certification ofVaccination, II Personal Health History) when theyreceive initial immunizations upon entering themilitary service. At the same time, a SF 601(Immunization Record) is initiated and placed in thesoldier’s health record. These forms are comparedfor accuracy when the soldier in processes to a newunit. If the soldier requires immunizations, referhim to the supporting TMC or hospital.
c. Administering Immunizations. Onoccasion, immunizations may be given at the BAS,such as flu shots. When this is done, a “member ofthe medical department/service trained andqualified in emergency resuscitative techniques”(this normally means a physician or PA) must be
present. An emergency tray (shock tray) must alsobe on hand for immediate treatment of seriousreactions. Personnel administering immunizationsmust be trained in immunization procedures. A listof personnel authorized to administer immuni-zations should be maintained at the BAS. Whenplanning to give immunizations at the BAS,coordinate with the supporting TMC andbrigade/division surgeon.
d. Status of Personnel. The BAS maintainsan immunization status composite record of allpersonnel in the unit. AR 40-66 and DA Pam 600-8require that this record be inspected by the unitcommander at specific intervals.
5-27. Maintenance
a. Maintenance Program. An effectivemaintenance program is essential to ensure a unit’sability to perform its mission. The most importantelement in a unit maintenance program is theequipment operator. He must be familiar with hisequipment and able to maintain it. Leaders ensurethat operators are trained in equipment mainte-nance procedures.
b. Procedures. This section represents abasic overview of maintenance procedures. Use it asa starting point from which to learn maintenanceand maintenance management procedures. To learnwhat you need to know requires that you “learn bydoing.”
c. Levels of Maintenance. Maintenanceoperations are divided into three levels (unit,intermediate, and depot) to efficiently coordinatethem with other military operations.
Unit maintenance. Unit mainte-nance is similar to the maintenance applied toprivately - owned vehicles. It focuses primarily onminor repairs, adjustments, and replacing minorcomponents, such as starters, generators, brakes,and spark plugs. The equipment operator/crew withthe aid of unit mechanics perform unit maintenance.This is the level of maintenance with which aplatoon leader is primarily involved.
intermediateIntermediate maintenance. Thelevel of maintenance has two
5-28

FM 8-10-4
orientations, direct support (DS) and generalsupport (GS).
Direct support maintenanceunits perform repair and return to the userfunctions. They are organic to the division and focuson far forward support. Direct support maintenanceunits perform repair work beyond the capability ofunit maintenance.
General support maintenanceunits perform major repairs and overhauls. Itemsrepaired at the GS level are returned to the supplysystem. General support maintenance does notperform a repair and return to the user function.
Depot maintenance. Depot mainte-nance is performed at fixed facilities in CONUS andmajor overseas areas. Depot maintenance ischaracterized by overhaul and rebuild functions.
d. Maintenance Terms and Functions. Tounderstand maintenance, a platoon leader must firstbecome familiar with terms used to describe variousmaintenance functions.
Prescribed load list. A prescribedload list (PLL) is the unit’s repair parts stockage. Itis composed of an authorized stockage list (ASL)which is a list of parts prescribed for a unit; alsodemand supported and command supported items.Demand supported items are parts for whichsufficient need has been historically established tojustify their stockage. Command supported itemsare parts which the unit commander has directed bestocked.
Preventive maintenance checks andservices. Preventive maintenance checks andservices (PMCS) consist of periodic checks (before,during, and after operations; daily, weekly,monthly) and scheduled services (Q-services). Theoperator’s technical manual (-10) for each item ofequipment lists the PMCS to be conducted and theirfrequency.
Cannibalization. Authorizedremoval of serviceable parts from unrepairableequipment by maintenance units.
Controlled exchange. Removal ofserviceable parts from unserviceable but repairable
equipment to bring a like piece of equipment tooperational status. This requires commandauthorization.
Technical manuals. Technicalmanuals (TMs) provide technical information(operator instructions, repair procedures, and repairparts) about specific pieces of equipment. Technicalmanuals are referred to as -10s (operator’s manual),-20s (unit and DS maintenance manuals), -30 (DS/GS manuals), -40 (GS and depot manuals), and -14(applies to all levels).
e. Battle Damage Assessment and Repair.Battle damage assessment and repair (BDAR)techniques expedite return of a damaged piece ofequipment to the current battle.
Battle damage assessment is usedto determine the extent of damage to equipment.Equipment is classified according to the type ofrepair needed; plans are made for repair of eachitem. Priorities for repair of battle damaged itemsare usually—
Most essential to the imme-diate mission.
Repairable in the least time.
Repairable but not in time forthe immediate mission.
Battle damage repair involves use ofemergency repair techniques to return a system to amission capability. Normally BDAR is only used incombat at the direction of the commander. Itincludes—
Shortcuts in parts removal orinstallation.
Modifying components fromother items.
Using parts from a noncriticalfunction elsewhere on an item to restore a criticalfunction.
Bypassing noncriticalcomponents to restore basic function capability.
Cannibalization.
5-29
FM 8-10-4
Making parts from kits oravailable material.
Using substitute fuels, fluids,or lubricants.
The BDAR program is not to beused in the repair of medical equipment. Onlymedical equipment repair personnel are adequatelytrained to effect the type of temporary fixesassociated with this concept. Due to the delicate,technological complex nature of most medical equip-ment, temporary fixes even by a medical equipmentrepairer is discouraged.
5-28. Maintenance Forms and Records
Numerous forms and records are used to documentmaintenance activities. These records are main-tained for historical purposes, to ensure necessaryservices are performed, and to establish require-ments for repair parts stockage.
a. Dispatch. DD Form 1970 (MotorEquipment Utilization Record) is commonlyreferred to as a "dispatch." It is issued to thevehicle operator by the unit maintenance clerkbefore the vehicle is used.
b. Inspection and Maintenance Worksheet.DA Form 2404 (Equipment Inspection andMaintenance Worksheet) is the “bread and butter”form of unit level maintenance (see TM 38-750). Theoperator uses this form to record faults that hecannot correct. Unit maintenance personnel refer tothe form to identify necessary repairs and annotatecorrective actions. It is used when conductingscheduled service and during other technicalinspections. The DA Form 2404 is quite versatileand is the most frequently used form in the motorpool.
c. Maintenance Request. DA Form 2407(Maintenance Request) is used by unit maintenancepersonnel as a request to support units (DS) forrepair work.
d. Lubrication Order. Lubrication order(LO) is more like a technical manual than amaintenance form. It details how to lubricate thevehicle, the types of lubricants to use, intervals to
be observed, and special precautions. An LO shouldbe kept on each vehicle with the appropriate TM.
5-29. Unit Maintenance Organization
a Battalion Maintenance Assets. Thebattalion’s maintenance assets (unit - levelmaintenance) are organized somewhat similar to itsmedical assets. All maintenance assets are organicto the battalion maintenance platoon. They areapportioned out to support the various companies.
b. Company Maintenance Section. Withinthe company maintenance section, the key playersare the battalion motor sergeant, normally an E-8,and the motor officer, usually the company XO. Themotor sergeant allocates jobs to his mechanics andsupervises their activities. He also runs the motorpool shop office. The motor officer is responsible tothe company commander for the unit’s maintenancestatus.
c. Battalion Maintenance Platoon. Thebattalion maintenance platoon is run by thebattalion motor officer (BMO). The battalion motorsergeant, an E-8, and the battalion maintenancetechnician, a warrant officer, assist the BMO. Thebattalion maintenance technician is the technicalexpert in the field of maintenance. He frequentlyinterfaces with DS maintenance and maintenancesupport teams.
5-30. Training
a. Importance. "The more you sweat intraining, the less you bleed in war." This ancientChinese proverb expresses the importance oftraining very simply and accurately. Much more hasbeen said and written about training, the bottomline of which is that to be prepared for war, we musttrain. Leaders have an obligation to ensure thateffective training takes place in the unit. Fortraining procedures, see Appendix A.
b. How to Train. Army trainingmanagement can be a difficult task, particularly fora new platoon leader. Do not expect to become animmediate expert. Study the system read Armytraining literature (AR 350-1, 25-series fieldmanuals, 8-series field manuals, local policies,
5-30

FM 8-10-4
regulations, and SOPs); talk with supervisors; andlearn from NCOs.
c. Get Involved in Training. The importanceof a leader’s involvement in training cannot beoveremphasized. Officers and NCOs do not onlyplan and present training, they also participate.Leader participation motivates soldiers; itemphasizes the importance of the training event. Asa participant, the leader can evaluate the quality ofthe training being presented. Participating intraining allows officers and NCOs to brush-up ontheir skills and, in many cases, to develop new skills.
d. Training Responsibilities. Unit trainingconsists of individual and collective training.Individual training is conducted for tasks which thesoldier must be able to complete unassisted, such asapplying a pressure dressing. Individual trainingdevelops the technical proficiency of the soldier.Collective training builds on individual skills andprovides the basis for unit proficiency in executingits missions, such as establishing an aid station andproviding HSS in a mass casualty situation.Generally, officers are responsible for collectivetraining and NCOs are responsible for individualtraining.
e. Battle Focus. The unit’s wartimemissions are the source from which all trainingactivities are derived. This is known as battle focus.A successful training program is achievable bynarrowing the focus to vital tasks that are missionessential. This is accomplished through thedevelopment of a mission essential task list(METL).
f . Mission Essential Task ListDevelopment.
The commander of each unit in theArmy from corps to company level must develop aMETL. The medical platoon, being a uniqueorganization in a combat arms battalion, should alsodevelop a METL. This is done by first consideringthe battalion’s mission and reviewing the battalionMETL. The medical platoon METL must supportthe battalion METL. The next step is to get a copyof the FSMC’s METL and discuss it with the FSMCcommander. The medical platoon METL must becoordinated with the FSMC METL. Other sourcesto consider are SOPs; emergency deployment
readiness exercise (EDRE) plans; and divisionsurgeon and DMOC plans and policies. The finalstep is to present the medical platoon METL (whichshould consist of roughly a half-dozen tasks) to thebattalion commander. Once the battalioncommander approves the METL, it becomes thesource document for developing the medical platoontraining plans. It should be changed only when theunit’s mission changes.
Involve the PA, medical operationsofficer, platoon sergeant, and other platoonmembers in the METL development process. Thiscreates a common understanding of the unit’scritical wartime requirements; it is essential indeveloping the platoon training plans.
A condition statement andstandards list for each mission essential task isdeveloped. The resulting training objective providesa clear list of expected training performance. Theplatoon sergeant will take the METL and develop asupporting individual task list for each missionessential task. Some documents which will assist indeveloping these collective and individual tasksare—
Mission training plans.
Soldiers training publications.
Deployment or mobilizationplans.
General defense plan.
Army, MACOM, and localregulations.
Local SOPs.
g. Planning.
(1) Needs assessment. The first step inplanning for training is the assessment. Assesscurrent training proficiency by reviewing trainingevaluations, such as CTC take-home packages, FTXafter-action reports, and inspection results. Alsoconsider recent or projected personnel turnover ornew equipment fielding. Finally, ask subordinatesfor their opinions and consider your ownobservations and impressions. Rate each task “T”
5-31

FM 8-10-4
(trained), “P” (needs practice), “U” (untrained), or“?” (unknown). The training requirements aresimply the training necessary to achieve and sustainthe desired levels of proficiency for each missionessential task.
(2) Training strategy. With theassistance of platoon members, develop a strategyto accomplish each training requirement. Thisshould include plans to improve proficiency in sometasks and sustain proficiency in others. The trainingstrategy establishes priorities by indicating thefrequency each mission essential task will beperformed during the training period. The strategyincludes guidance that links METL with trainingevents (coordinate training with the HHB/HHC/HHT/HHS commanders, S3 and, if necessary,battalion commander).
h. Planning Calendars.
(1) Battalion training schedules. Thebattalion produces long-range, short-range, andnear-term training schedules covering 1 year, 3months, and 1 week respectively. The weeklytraining schedules are normally provided for eachcompany. The medical platoon should get a copy ofthese schedules.
(2) Medical platoon input. The medicalplatoon should hold regular training meetings of keyleaders within the platoon to develop medicalplatoon input to the battalion’s training schedules.Before the long-range training schedule is prepared,the medical platoon leader should tell the HHCcommander, in general terms, what training themedical platoon needs during the upcoming year.Upon receipt of the long-range training calendar, themedical platoon should meet and refine plans fortraining in the first quarter. The medical platoonleader then provides specific information to theHHC commander for inclusion in the battalionquarterly training schedule. The medical platoonthen holds weekly training meetings to—
Review training conductedduring the previous week.
Discuss training plannedthe current week.
Make firm coordinationtraining scheduled for the upcoming week.
5-32
for
for
Provide final details of medical platoon trainingplans for the upcoming week for inclusion in theweekly HHC training schedule.
(3) Coordinating medical platoontraining. Remember, all medical platoon trainingmust be conducted within the parametersestablished by the battalion/company trainingschedule. For example, the battalion trainingschedule calls for a FTX with a company force-on-force exercise; perhaps the medical platoon canconduct an evacuation exercise concurrently. Thisrequires coordination with the S3, companycommander, and possibly the FSMC commanderand others. Most of all, conforming medical platoontraining plans and activities to the parent unitactivities require creativity, flexibility, andinitiative on the part of the medical platoon leader.Training must be conducted without detractingfrom the HSS being provided the companiesundergoing training.
i. Expert Field Medical Badge.
(1) The program. The Expert FieldMedical Badge (EFMB) program has received highlevel attention in recent years. In many units, themedical platoon leader’s evaluation is directly tiedto the percentage of his platoon which passed theEFMB test. In some divisions, awards are given tothe battalion with the highest EFMB pass rate.Aside from these facts, the EFMB is an excellentprogram and is a good measure of training successand unit motivation. If planned and administeredcorrectly, EFMB training can tie directly into yourplatoons METL-based training program.
(2) Training and test management.EFMB training is managed differently at variousposts around the Army. Some provide centralizedEFMB training, while others leave it to the unit. Inmost divisions, EFMB training is conducted in theunit with some type of centralized training for alldivision EFMB candidates. EFMB testing isstandardized; however, the frequency of testingmay vary. For additional information on EFMBtraining and testing, see TC 8-100.
(3) Command. The medical platoonleader should find out how much emphasis thebattalion commander places on the EFMB and plantraining accordingly. Call the division surgeon or

FM 8-10-4
DMOC to get details of local EFMB training andtesting procedures.
j. Army Medical Department SystematicModular Approach to Realistic Training. The ArmyMedical Department Systematic Modular Approachto Realistic Training (ASMART) was created toprovide hospital-based clinical skills training anddevelopment to medical personnel. The programallows an established number of medics from eachunit to rotate through the hospital at set intervals.
Normally, medics will be enrolled in ASMART for aperiod of 90-180 days. The ASMART offers anexcellent opportunity for medical personnel tosharpen their clinical skills through work in theemergency room or in a hospital ward or clinic.However, the program must be closely monitored toensure that the participants are receiving goodtraining. If, as medical platoon leader, you are notsatisfied with the training being provided throughthe ASMART, discuss your concerns with thedivision surgeon and/or hospital commander.
Section V. EMPLOYMENT OF THE MEDICAL PLATOON
5-31. Planning and the Health Service SupportPlan
a. Planning. To ensure that HSS isresponsive to the battalion (squadron), the medicalplatoon leader or the medical operations officermust attend all operational briefings and planningsessions. They are responsible for providing theHSS portion of battalion SOPs, OPLANs, andoperation orders (OPORDs). The HSS planned fortactical operations is addressed in theadministrative and logistics annex of the battalionOPORD. It should include—
Location of forward treatment sites.
Ground and air medical evacuationroutes, ambulance exchange points, and far forwardpatient collecting points.
Location of the supporting DCS(medical company).
NOTE
The battalion surgeonand the medicaloperations officer mustkeep the medical platoonpersonnel informed of thetactical situation.
b. Health Service Support Plan. The healthservice support plan (HSSPLAN) must beresponsive and support the maneuver commander’sintent. The HSSPLAN is best disseminatedthrough the use of an overlay showing preplannedtreatment team/BAS locations and ambulanceexchange points. The HSSPLAN is keyed to themaneuver battalion’s OPORD. Once approved, theoverlay is distributed to maneuver companycommanders, elements of the medical platoon, thetactical operations center, and the ambulanceplatoon leader of the supporting FSMC. A sampleoverlay (HSSPLAN) depicting preplanned positionsfor ALFA and BRAVO treatment teams of a BASand AXPs of a FSMC ambulance platoon is shownin Figure 5-16. To effectively execute theHSSPLAN, the medical operations officer monitorsthe tactical situation. He maneuvers the treatmentteams and coordinates changes for AXP locationsbased on the progress of the battle. This allows theHSS system to rapidly clear the battlefield ofcasualties; to treat patients early; and to returnminimally injured soldiers to the fight.
5-32. Combat Medic
a. Allocation. As was mentioned previously,combat medics are allocated to mechanized infantryon the basis of one medic per platoon and a seniormedic for each company. In armor units, the alloca-tion is one medic per company. Normally, oneambulance team is positioned in the company area.
5-33
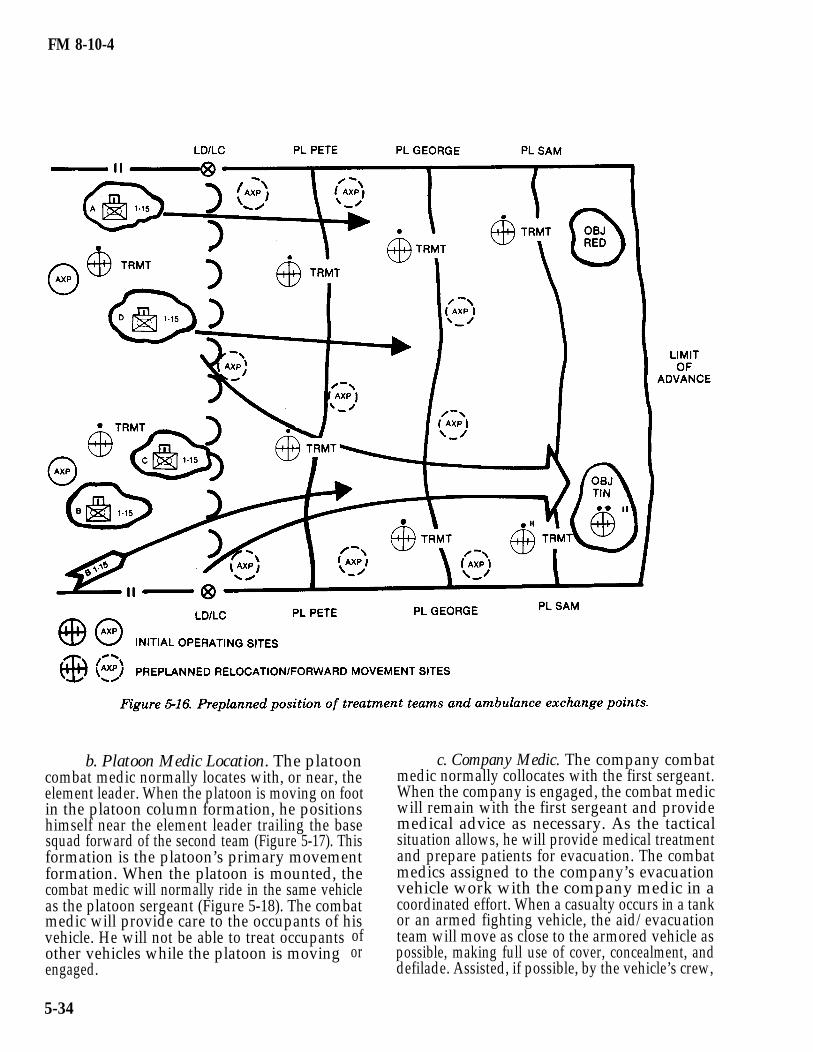
FM 8-10-4
b. Platoon Medic Location. The platooncombat medic normally locates with, or near, theelement leader. When the platoon is moving on footin the platoon column formation, he positionshimself near the element leader trailing the basesquad forward of the second team (Figure 5-17). Thisformation is the platoon’s primary movementformation. When the platoon is mounted, thecombat medic will normally ride in the same vehicleas the platoon sergeant (Figure 5-18). The combatmedic will provide care to the occupants of hisvehicle. He will not be able to treat occupantsother vehicles while the platoon is movingengaged.
ofor
c. Company Medic. The company combatmedic normally collocates with the first sergeant.When the company is engaged, the combat medicwill remain with the first sergeant and providemedical advice as necessary. As the tacticalsituation allows, he will provide medical treatmentand prepare patients for evacuation. The combatmedics assigned to the company’s evacuationvehicle work with the company medic in acoordinated effort. When a casualty occurs in a tankor an armed fighting vehicle, the aid/evacuationteam will move as close to the armored vehicle aspossible, making full use of cover, concealment, anddefilade. Assisted, if possible, by the vehicle’s crew,
5-34
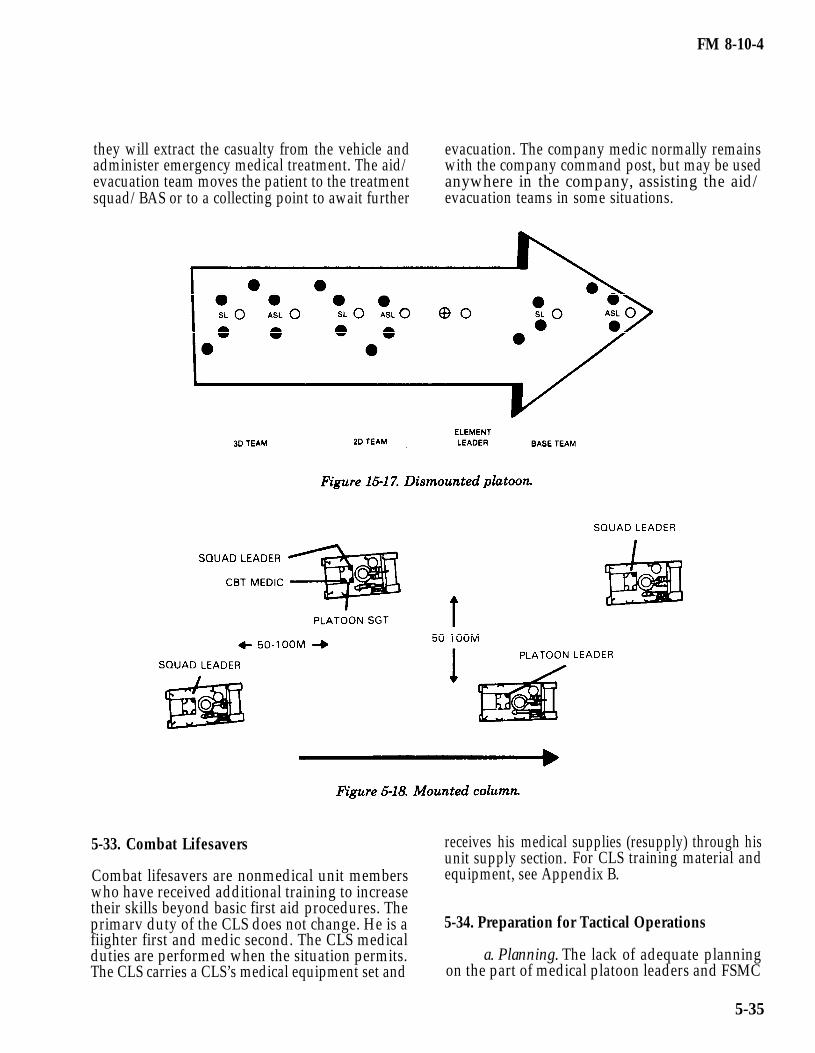
FM 8-10-4
they will extract the casualty from the vehicle and evacuation. The company medic normally remainsadminister emergency medical treatment. The aid/ with the company command post, but may be usedevacuation team moves the patient to the treatment anywhere in the company, assisting the aid/squad/BAS or to a collecting point to await further evacuation teams in some situations.
5-33. Combat Lifesavers receives his medicalunit supply section.
supplies (resupply) through hisFor CLS training material and
Combat lifesavers are nonmedical unit members equipment, see Appendix B.who have received additional training to increasetheir skills beyond basic first aid procedures. Theprimarv duty of the CLS does not change. He is a 5-34. Preparation for Tactical Operationsfiighter first and medic second. The CLS medicalduties are performed when the situation permits.The CLS carries a CLS’s medical equipment set and
a. Planning. The lack of adequate planningon the part of medical platoon leaders and FSMC
5-35

FM 8-10-4
commanders has been repeatedly noted at theNational Training Center.
b. Tailoring Medical Platoon Organizationto Mission. The platoon organization best suited forspecific combat operations are discussed in SectionsII and III of this chapter. However, it is importantto realize that although the medical platoon isauthorized a certain number of personnel andamount of equipment with which to accomplish itsmission, on-hand figures seldom match thoseauthorized. The ability to accomplish the missionwith less personnel and equipment than authorizedis one of the greatest challenges which leaders faceArmywide.
c. Reconnaissance. All key personnel withinthe medical platoon, especially evacuation NCOs,conduct personnel through reconnaissance beforeand between phases of an operation. If an on-sitereconnaissance is not possible, a map recon isconducted. During the map recon, primary andsecondary evacuation routes through eachcompany’s sector are designated. Prepare anoverlay displaying evacuation routes, BASlocations at various points in the operation, and ifpossible, the FSMC location. In developing the HSSoverlay, use phase lines designated for themaneuver elements. Key BAS relocation uponmaneuver units crossing certain phase lines. Referto FM 101-5-1, Operational Terms and Symbols, forcorrect overlay symbols and techniques. Distributea completed overlay to each company commander,the S3, the FSMC commander, and ensure thatsenior company medics and evacuation NCOs havecopies.
d. Medical Platoon Operations Order. ASthe map recon is conducted, also develop themedical platoon OPORD. The medical platoonOPORD must be tied to the parent battalionOPORD and should be coordinated with the FSMC.It may be written or oral, but must use the fiveparagraph OPORD format. Prior to the operation,issue this order to members of the medical platoonand attached/supporting medical personnel.
5-35. Deployment
a. Complexity of Deployment. Fieldoperations begin with a deployment. This may be assimple as loading vehicles and convoying to a
training area on-post, or as complicated as loadingthe entire unit for an overseas deployment.
b. Movement Plans. The key to a successfuldeployment is accurate movement plans. Eachcompany should have a movement officer respon-sible for maintaining a unit movement file. This filecontains detailed information on the unit’scapability to deploy. It specifies transportationrequirements necessary to support the unit’smovement by various modes of travel, such as air,rail, or convoy. Among the most basic and mostimportant information assembled by the unitmovement officer is a list of prime movers (trucksdesignated to move trailers) and their designatedtrailers, and load plans for each vehicle.
c. Medical Platoon Loading Plans. Themedical platoon must be able to move all of itspersonnel (less company and platoon medics) andequipment to the field with its organic vehicles. Theplatoon’s load plans prescribe the method by whichthis is done. The load plan specifies exactly whatsupplies and equipment will be carried on whichvehicle. It specifies a prime mover for each trailer.The MES, BAS is divided between the platoon’s aidstation vehicles to give each treatment team equalcapability. The load plan allows for personalbaggage, tentage, camouflage nets and poles,heaters/stoves, tools, and any other miscellaneoussupplies and equipment. See Appendix D for anexample.
d. Evaluate Load Plan. The platoon loadplan must be accurate and workable. The only wayto be sure load plans are valid is to test them.Periodically, the medical platoon should load-out allof its supplies and equipment in accordance with theplatoon load plan (FTX deployments are goodopportunities to do this). This will reveal anyshortcomings in the load plans and will result inmore workable loading arrangements. Any changesmade during these practice load-outs should bereported to the company movement officer. Once anefficient load plan is developed for each vehicle, it ispublished so that the crew becomes familiar withthe configuration. Before deployment, inspect eachvehicle to ensure its configuration matches the loadplan.
e. Convoy. The final step in the deploymentprocess is normally a convoy to the maneuver area.
5-36
FM 8-10-4
The convoy will most likely be conducted as atactical road march consisting of several marchunits dispersed over various routes. The battaliontactical SOP prescribes convoy procedures; itincludes intervals between vehicles, speed, rest haltintervals, safety briefings, and night and blackoutdrive procedures. Convoys are relatively simpleoperations but require much coordination, closecontrol, and active attentive participation bydrivers.
5-36. Establishing the Battalion AidStation/Company Aid Post
a. Site Selection. Prior to deployment, aninitial site for the BAS is designated as well asfuture sites to be used as the operation progresses.This is done during the map recon, is coordinatedwith other staff members, and is published in thebattalion’s OPORD and the HSS overlay. Anexample of a BAS arrangement is depicted inFigures 5-4 and 5-5. Some factors to consider whenselecting a site for the BAS include—
Cover and concealment. The areaselected should provide maximum cover andconcealment without hampering mission orcommunications. Overhead cover is desirable forprotection from biological/chemical contamination,if attacked.
Accessibility. The site shouldprovide adequate access to all approach andevacuation routes.
Space. The site should haveadequate space for the unit’s operation andexpeditious loading and unloading patients,supplies, and equipment.
Drainage. The site should providegood drainage during inclement weather.
Decontamination area. The areashould be large enough to provide an area forpatient decontamination, if required.
Landing site. Provide an area for ahelicopter landing site.
Security. The site should providesecurity and be defendable.
Communications. When consideringall factors of site selection, remember that terraincan impede FM communication systems.
NOTE
If the BAS is collocatedwith the combat trains orif another staff memberselects the BAS site, themedical platoon leadermust ensure the abovefactors are considered.
b. Establish Battalion Aid Station. Whenthe BAS elements arrive at the operational site, thefollowing actions are taken:
An advance party is on location andhas the area secured.
Move BAS vehicles(covered and concealed, if possible).
Establish perimeternecessary.
into position
security, if
Configure supplies and equipmentinto tailgate medicine operational posture.
Establish helicopter landing siteand equipment to support patient care.
Report to the main CP, combattrains CP, and FSMC that the BAS is operational.
Make radio check with eachcompany senior medic.
Erect extension/tentage. Anexample of a M577 extension configured as a BAS(treatment station) is depicted in Figure 5-19.
Erect camouflage nets.
Operators perform after operationcheck of vehicles.
Complete final preparation toreceive patients, incorporate sleep/work schedule toensure radios are continuously monitored.
5-37
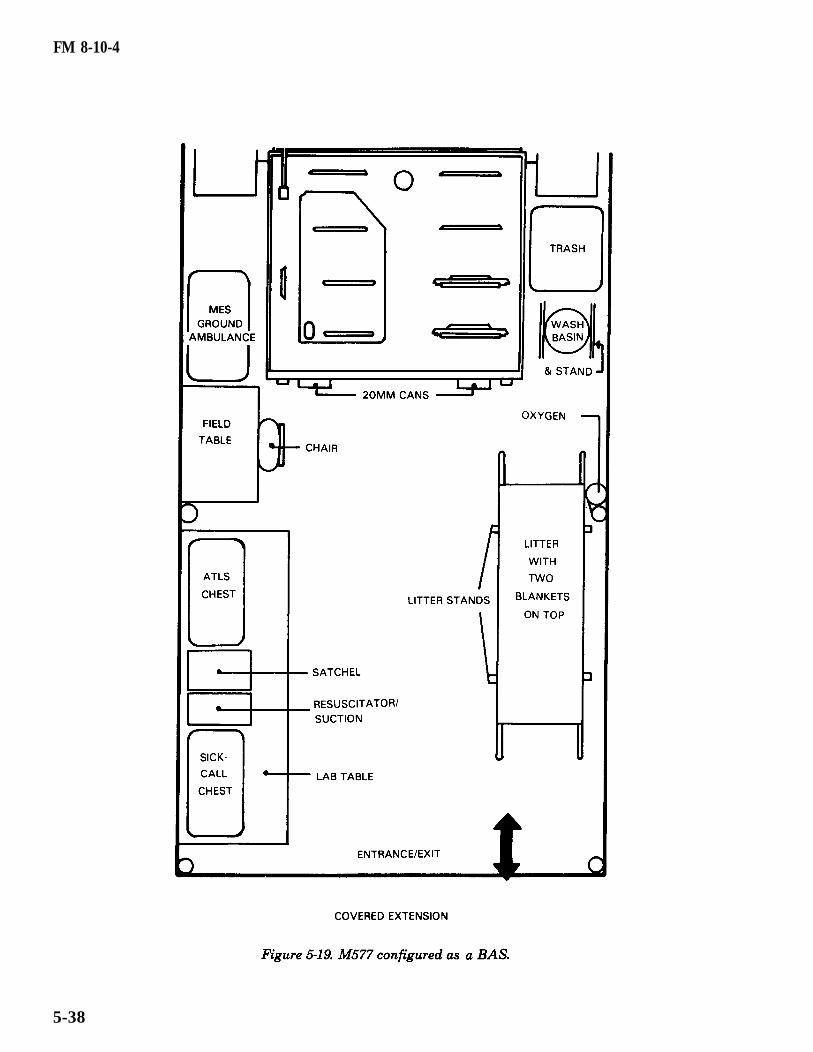
FM 8-10-4
5-38
FM 8-10-4
c. Establish Company Aid Post. Whenestablishing a company aid post, take the followingactions:
Company medic remains with ornear first sergeant; this is his transportation.
If possible, collocate aid post withmedical evacuation vehicle (company medic mustnot depend upon this vehicle for his transportation).The company medic must remain with the company.
Prepare area to receive patients.
Make radio check with platoonmedics, if possible.
Camouflage as necessary.
5-37. Treat and Evacuate Patients
a. Combat Medic Care. When casualtiesoccur, first aid will usually be rendered by buddy aidor perhaps CLS care. The platoon medic/companymedic will then go to the casualty’s location or thecasualty will be brought to the medic. The combatmedic makes his assessment; administers initialmedical care; initiates a DD Form 1380 (FieldMedical Card); then requests evacuation or returnsthe individual to duty. A vehicle from theevacuation section (usually pre-positioned forward)picks-up the patient and transports him to the BAS.
b. Battalion Aid Station Care. When thepatient arrives at the BAS, initially he is taken to atriage point. When the treatment teams arecollocated, the PA usually performs triage (if thetreatment teams are separated or a mass casualtysituation exists, an EMT NCO performs triage). Thepatient is categorized as immediate, delayed,minimal, or expectant. Depending upon his triagecategory and the patient load, the patient is thentaken to either the patient holding area or thetreatment area. Ultimately, medical treatment isadministered and the patient is either evacuated tothe DCS or returned to duty.
c. Mass Casualty Situation. Keep in mindthat the type of operation being supported will to agreat extent determine the rate of casualtiesgenerated. In a high-intensity conflict, mass
casualty situations will develop. Medical treatmentand evacuation capabilities may be temporarilyoverwhelmed. Self/buddy aid and CLS care will becritical. Nonmedical vehicles may be required toevacuate casualties (FM 8-10-6). It is possible that adecision will have to be made to abandon patients;however, if patients have to be abandoned, a medicwith medical supplies must remain with them. Inany scenario, the guiding principle is to provide thegreatest good for the greatest number of patients.
5-38. Disestablish a Field Medical TreatmentFacility
When a unit receives orders to relocate, loadvehicles according to loading plans in order toprovide HSS while en route or at the relocation site.All potential sources of intelligence which could beused by enemy forces are removed before leavingthe area. All wires that were used for communica-tions are recovered and serviced. Prior to departing,all personnel are briefed on the move and issuedstrip maps. Patients awaiting evacuation are movedwith the BAS, if possible. The BAS must maintaincommunications and continue to monitor the battle.
5-39. Field Sanitation
a. Medical Threat. Poor field hygiene andsanitary practices pose a very real threat to unitsboth in training and combat. In fact, throughoutrecorded history, DNBI have accounted for a higherpercentage of casualties than have battle injuries.(In US history, this ratio is three to one.) Eventoday, outbreaks of diarrheal disease, foodpoisonings, arthropod bites, and environmentalinjuries (heat and cold) account for significanttraining time loss. Although the medical threatconsists of hundreds of casualty-producing injuriesand illnesses, the causes can be, reduced to sixprimary categories.
Heatcombinations of heatconsumption.
injuries causedstress and insufficient
Cold injuries caused bycombinations of inadequate clothing, low
bywater
temperatures, wind, and wetness.
5-39

FM 8-10-4
Diseases caused by bitingarthropods.
Diarrheal diseases caused bydrinking impure water, eating contaminated foods,or not practicing good individual and unitPVNTMED measures.
Diseases, trauma, or injuries causedby physical or mental unfitness.
Environmental or occupationalinjuries caused by carbon monoxide, noise, blastoverpressure, and solvents.
b. Preventive Medicine Measures. Themedical platoon leader is responsible for monitoringthe health of the soldiers in his battalion. He can beproactive in this regard by ensuring the provision ofthe following PVNTMED measures.
Large amounts of water to combatthe threat of heat injury. Joint planning factorsindicate that as much as 20 gallons per person perday will be required during operations in hotweather environments.
Adequate changes of socks andclothing to prevent cold injuries caused by wetclothing.
Arthropod repellents, aerosolinsecticide, bed nets, and louse powder for theindividual; pesticides and associated equipment forfield sanitation teams; and PVNTMED unitssupport to prevent arthropod-borne disease.
Iodine tablets and calciumhypochlorite to maintain water potability.
Adequate fresh air ventilation inconfined vehicles and in maintenance and sleepingareas. Proper ventilation prevents carbon monoxidepoisoning.
Adequate hearing protection.
Adequate vision protection toprevent traumatic eye injury from laser devices,sighting devices, and secondary projectiles.
(1) Individual protective measures.The mobility and dispersion of modern fightingforces require that individual soldiers take actionsto protect themselves against the medical threat.These simple individual actions are calledPVNTMED measures. Applying these measurescan significantly reduce the time loss due to DNBI.The soldier should—
Protect himself against heatby–
Drinking plenty of water.
Using the correctwork/rest cycle as directed by his leader.
Eating all meals toreplace salt.
Recognizing the riskassociated with wearing mission-oriented protectionposture (MOPP) clothing, body armor, or wheninside armored vehicles.
Modifying his uniform asdirected/authorized by his leader.
Protect himself against thecold by—
Drinking plenty of waterto replace loss of fluids during periods of strenuousexercise.
Wearing his uniformproperly in loose layers to hold maximum body heat.
Washing his feet dailyand keeping them dry by changing socks severaltimes a day.
Keeping his body warmby exercising his trunk and limbs wheneverpossible. Exercising his feet, hands, and face toincrease circulation.
Protect himself against bitingarthropods by—
Using his uniform as abarrier.
Using arthropod/insectrepellent.
5-40
FM 8-10-4
Takingor tablets as prescribed.
Usingaerosol insecticide at night.
antimalarial pills
a bed net and
Keeping himself and hisuniform clean.
Protect himself againstdiarrhea by—
Only consuming food,drink, or ice approved by medical authorities.
Using treated water whenavailable. When not available, treating water byusing iodine tablets or chlorine ampules, or boilingit.
Washing his hands.
Washing his mess kit.
Burying his waste.
Maintain physicalfitness by—
Exercising.
Preventinginfections.
Preventingdisease.
and mental
skin
dental
Preventing genital andurinary tract infections (drinking plenty of water).
Bathing when possible.
Minimizing sleep loss.
Improving resistance tostress.
Ensuring adequateventilation while in closed spaces such as whenfiring weapons from inside an armored vehicle.
Wearing hearingprotection while associated with source of noise(that is, aircraft, tactical vehicles, and all calibers ofweapons).
Wearing eye protectionwhen exposed to sources of traumatic injury such aslasers.
(2) The field sanitation team. Thecompany field sanitation team consists of organicmedical personnel; or at least two soldiers, one ofwhom is an NCO, when organic medical personnelare not available. The team is specially trained inwater supply, food service sanitation, wastedisposal, pest management, environmental injuries,and non-NBC chemical hazards (see FM 21-10-1).The field sanitation team serves as an aid to the unitcommander in protecting the health of his company.Through regular inspections, the field sanitationteam ensures sanitary standards are maintainedand PVNTMED measures are practiced. Table 5-1 ishelpful in identifying activities which are ofPVNTMED significance.
5-40. Medical Training in the Field
a. Importance. Conducting medical trainingduring a battalion FTX can be a challenge. Whenproperly conducted, however, medical play can lendsignificant realism to training exercises. Thisbenefits both the medical platoon and the battalionas a whole. The medical platoon learns to performmedical treatment and evacuation operations undersimulated combat conditions. The battalion learnsto complete its mission under situations in which itis suffering casualties. For information on planningfor deployment to CTC, see Appendix G.
b. Lessons Learned. Previously, the keychallenge in incorporating medical play intotraining exercises was sometimes convincing thebattalion commander to do it. Fortunately, CombatTraining Center experience has shown the need forrealistic training to include medical play. Now, thechallenge is in operating and reacting to realisticcasualty scenarios. Again, this tests the initiative,creativity, and flexibility of medical platoon leaders.Observations and lessons learned at CTC arepresented in Appendix G.
5-41
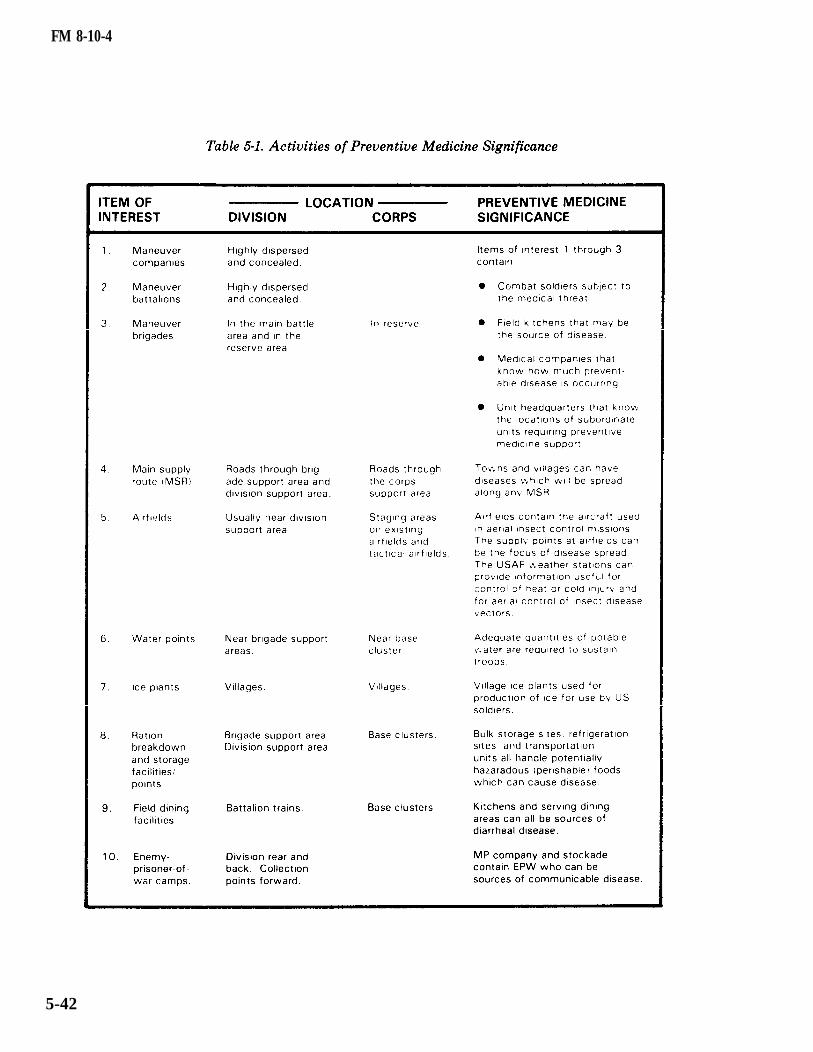
FM 8-10-4
5-42
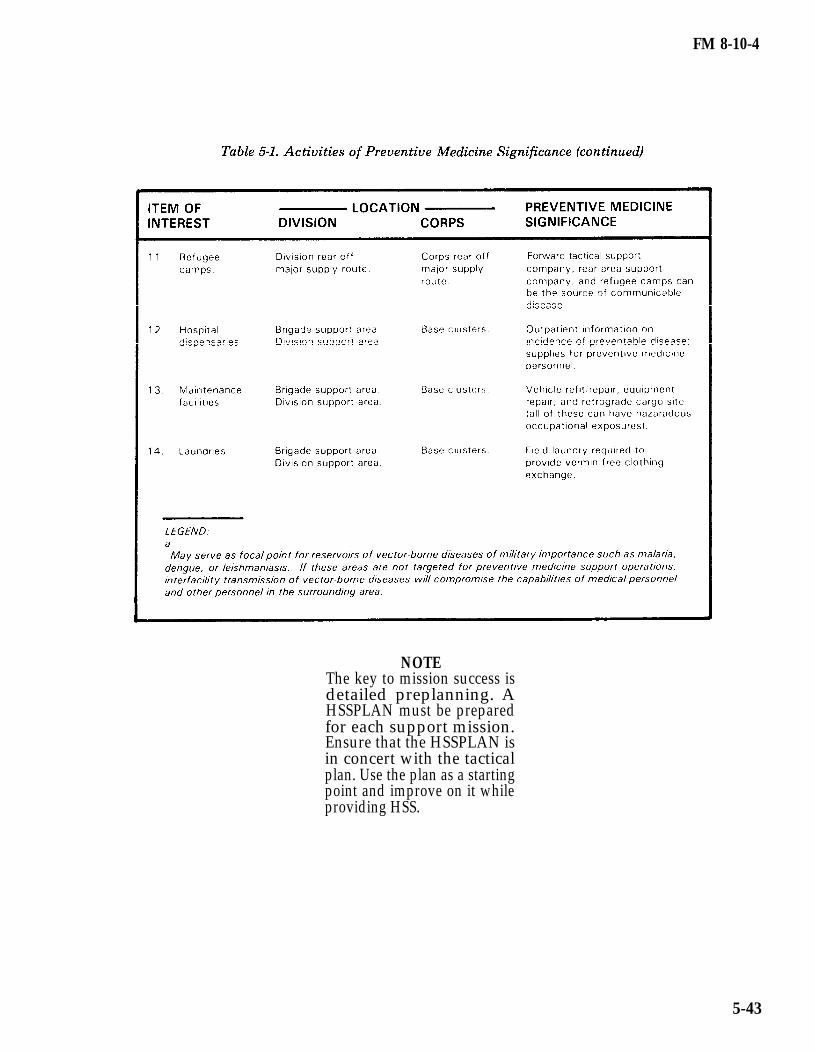
FM 8-10-4
NOTEThe key to mission success isdetailed preplanning. AHSSPLAN must be preparedfor each support mission.Ensure that the HSSPLAN isin concert with the tacticalplan. Use the plan as a startingpoint and improve on it whileproviding HSS.
5-43