Embed Size (px)
Citation preview

Unintentional Weight Loss
AIMGP Seminar MSH/UHNJanuary 2008Yash Patel

Seminar Objectives
Develop an approach to unintentional weight loss
Define unintentional weight loss Review the incidence and prevalence
of weight loss Review the common causes of weight
loss Cover treatment strategies

Selected References
An approach to the management of unintentional weight loss in elderly people. Alibhai S. et al; CMAJ: Mar 15, 2005
Rational approach to patients with unintentional weight loss. Bouras E. et al; Mayo Clin Proc: Sept 2001
Evaluating and treating unintentional weight loss in the elderly. Huffman G.; Am Fam Physician: Feb 15, 2002

Case
You are referred a 69 F for evaluation of unintentional weight loss.
She has lost 5 kg in the past 12 months, her current weight is 60 kg.
Is her weight loss clinically important? How common is weight loss in the
elderly?

Is her weight loss clinically important? Definition
Clinically important weight loss can be defined as loss of 5 kg or more than 5% of usual weight over 6-12 months
Why it’s important! Unintentional weight loss may reflect disease
severity of a chronic illness or a yet undiagnosed illness.
Even after adjusting for co-morbidities weight loss of 5% or more of body weight is associated with increased mortality (approx increase in RR 1.6)

How common is weight loss in the elderly?
Prevalence estimates of weight loss are quite variable 15-20% elderly patients experience weight loss
(defined as loss of 5 kg or 5% body wt over 5-10 years)
The prevalence can be as high as 27% in high-risk populations such as the frail elderly
The incidence of unintentional weight loss in clinical studies of adults seeking health care is also quite variable Depending on the setting and definition it varies
from 1.3 to 8%

Case
HPI: She confirms that her weight was 65 kg
1 year ago when it was measured at the family doctors office
Her appetite is “normal” and she reports no other constitutional symptoms
The clinical review is negative for cardiac, respiratory, gastrointestinal, and neurologic symptoms

Case PMHx:
Hypertension (on ACEI and HCTZ) Dyslipidemia (on statin) OA of both kness (on prn acetominophen)
Social Hx: Widowed 3 years ago Lives in apartment, independent in ADLs and
iADLs X-smoker (quit 10 years ago), occasional ETOH
use

Case
Physical Exam: VS: BP-118/74, HR-74 regular, T-37.3 C H+N: normal thyroid and no lymph
nodes CV/RS: normal heart sounds, clear lungs GI: negative Castell’s sign, and normal
liver span NE: normal muscle bulk, strength, and
tone

Case
Now What? What are the common causes of
unintentional weight loss?

What are the common causes of unintentional weight loss?
Causes of unintentional weight loss can classified into 3 broad groups Organic Psychosocial Idiopathic (up to 10-36% of cases)

What are the common causes of unintentional weight loss?
Organic Causes - top three Malignancy (16-36%)
Usually it’s clear from the history, physical, or routine lab data that malignancy is a potential cause
Gastrointestinal (most common non-malignant organic cause, 6-19%) PUD, IBD, dysmotility, hepatobiliary/pancreatic
disease, or oral problems Endocrine (4-11%)
DM, thyroid disease, and adrenal insufficiency

What are the common causes of unintentional weight loss?
Organic causes (less common) Cardiovascular disease (2-9%) Respiratory disease (~6%) Chronic infections (2-5%) Renal disease (~4%) Drugs/Medication Side effects (~2%) Neurologic disorder (2-7%)

What are the common causes of unintentional weight loss?
Psychosocial Causes Psychiatric disorder (9-42%)
Depression Dementia (2-5%) Poor nutritional intake
Due to poverty or inadequate access to meals

What are the common causes of unintentional weight loss?
Psychosocial Causes Depression and dementia are poorly recognized
in clinical practice All elderly patients with weight loss should
undergo screening for dementia with the MMSE depression with the Geriatric Depression Scale
Screen for malnutrition with one of these validated tools (ENS or SCREEN) at www.dietitians.ca/seniors/index.asp

What are the common causes of unintentional weight loss?
Several key concepts emerge from etiologic studies of unintentional weight loss Among organic causes cancer is most
common Etiology of weight loss is evident without
extensive evaluation in most patients Psychiatric illness and nondiagnostic
evaluations are common

Case So far her history and physical is
unremarkable You explore other issues…
You ask her about medication side effects - she reports none.
You do a MMSE and she scores 30/30! Access to food and meals is not an issue for her.
What further assessment or investigations are now indicated?

What further assessment or investigations are now indicated?
The diagnostic utility of the medical history and physical examination in identifying the cause of weight loss has not been evaluated
The same can be said about screening investigations
Despite the lack of systematic evaluation, a complete history, physical examination and selected “routine” investigations are recommended

What further assessment or investigations are now indicated?
Routine Investigations CBC Biochemistry (lytes, glucose, Ca, PO4) TSH Liver enzymes Urinalysis CXR

What further assessment or investigations are now indicated? Additional tests are ordered as clinically
indicated HIV test SPEP PSA, mammogram GI investigations (if there are symptoms,
microcytic anemia, or abnormal liver enzymes) OGD or colonoscopy plus biopsies Stool analysis Celiac serology Abdominal imaging

Case
She is send for the “routine investigations” and returns for follow-up All the investigations are normal or
negative She is relieved, but still wants to know
why she has lost 5 kg? Now What?

Case You pursue the assessment further and ask
about symptoms of depression She does occasionally feel lonely since her
husband passed away but…the Geriatric Depression Scale is negative
You reassure her that she does not have an organic or pyschosocial cause for her weight loss Her diagnosis is idiopathic unintentional weight
loss How should weight loss be treated? What follow up does she need?

How should weight loss be treated?
Treat the underlying organic cause When pyschosocial issues are involved then
a multi-disciplined approach is required to address the key issues including social work, dietician, community
services and psychiatrist For idiopathic weight loss seek advice from
a dietician for strategies to increase caloric intake

What follow up does she need?
Reassess her weight in 3 months If it remains stable or goes up then
further assessment is not necessary If she is continuing to lose weight then
repeat the evaluation process, with emphasis on searching for an organic or psychosocial cause

Case She returns after 3 months and her weight
has remained stable She is following the advice of the dietician to
increase her caloric intake You feel confident that she has idiopathic
weight loss At this point you discharge her from clinic
and ask her family doctor to monitor her weights every 3-6 months.

Summary Unintentional weight loss is a common
concern especially in the elderly Common causes can be grouped into one of
3 categories: organic, psychosocial, or idiopathic
Psychosocial causes are under appreciated by clinicians
Extensive investigations are usually not necessary

Appendix
The following are some figures and tables from Shabir Alibhai’s review article from the CMAJ
And my approach to weight loss summarized in a figure

Copyright ©2005 CMA Media Inc. or its licensors
Alibhai, S. M.H. et al. CMAJ 2005;172:773-780

Copyright ©2005 CMA Media Inc. or its licensors
Alibhai, S. M.H. et al. CMAJ 2005;172:773-780

Copyright ©2005 CMA Media Inc. or its licensors
Alibhai, S. M.H. et al. CMAJ 2005;172:773-780
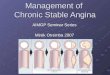
Fig. 1: Strategies for treating weight loss in elderly patients

Copyright ©2005 CMA Media Inc. or its licensors
Alibhai, S. M.H. et al. CMAJ 2005;172:773-780
Table 3.

Approach to Weight Loss
Weight Loss (>5% body wt)
Voluntary…dieting, anorexia/bulimia
Involuntary
Increased Appetite…DM, malabsorption, hyperthyroidism
Decreased Appetite
Idiopathic(25%)
Psychiatric…depression, dementia(15%)
Organic
Cancer(20%)
Noncancer(40%)
GIEndocrineInfectiousMedicationsCVNeurologicPulmonaryRenalCTD