Embed Size (px)
Citation preview

TYPE 2 DIABETES MELLITUS
REVIEW OF Clinical Practice Guidelines
TYPE 2 DIABETES MELLITUS
REVIEW OF Clinical Practice Guidelines
WEEK 2: TherapyWEEK 2: Therapy
UHN AIMGP CLINIC UHN AIMGP CLINIC SEMINAR SERIES 2007SEMINAR SERIES 2007
Updates Dr. K. TzanetosUpdates Dr. K. Tzanetos
WEEK 2: TherapyWEEK 2: Therapy
UHN AIMGP CLINIC UHN AIMGP CLINIC SEMINAR SERIES 2007SEMINAR SERIES 2007
Updates Dr. K. TzanetosUpdates Dr. K. Tzanetos

T2DM: ReferencesT2DM: References
Canadian Diabetes Association (CDA): 2003 Canadian Diabetes Association (CDA): 2003 Clinical Practice Guidelines for the Clinical Practice Guidelines for the Prevention and Management of diabetes Prevention and Management of diabetes in Canada.in Canada.
Can J Diabetes 2003; 27 (Suppl 2).Can J Diabetes 2003; 27 (Suppl 2). http://www.diabetes.ca/cpg2003http://www.diabetes.ca/cpg2003
American Diabetes Association (ADA): American Diabetes Association (ADA): Clinical Practice Recommendations 2006.Clinical Practice Recommendations 2006.
Diabetes Care 2006; 29 (Suppl 1).Diabetes Care 2006; 29 (Suppl 1).
Canadian Diabetes Association (CDA): 2003 Canadian Diabetes Association (CDA): 2003 Clinical Practice Guidelines for the Clinical Practice Guidelines for the Prevention and Management of diabetes Prevention and Management of diabetes in Canada.in Canada.
Can J Diabetes 2003; 27 (Suppl 2).Can J Diabetes 2003; 27 (Suppl 2). http://www.diabetes.ca/cpg2003http://www.diabetes.ca/cpg2003
American Diabetes Association (ADA): American Diabetes Association (ADA): Clinical Practice Recommendations 2006.Clinical Practice Recommendations 2006.
Diabetes Care 2006; 29 (Suppl 1).Diabetes Care 2006; 29 (Suppl 1).

T2DM: TherapyT2DM: Therapy
WEEK 2 OBJECTIVES:WEEK 2 OBJECTIVES:
Develop familiarity with the indications, goals and Develop familiarity with the indications, goals and therapy progression of treatment:therapy progression of treatment:
1) Non-pharmacologic therapy1) Non-pharmacologic therapy2) Pharmacologic therapy for glycemia2) Pharmacologic therapy for glycemia
- Oral agents: monotherapy and combination- Oral agents: monotherapy and combination - Insulin: monotherapy and in combination with - Insulin: monotherapy and in combination with OHAsOHAs
3) Therapy for nephropathy (if time permits)3) Therapy for nephropathy (if time permits)4) Therapy for neuropathy (if time permits)4) Therapy for neuropathy (if time permits)
Note: HTN, CAD, and Dyslipidemia will be discussed in Note: HTN, CAD, and Dyslipidemia will be discussed in future seminars…future seminars…
WEEK 2 OBJECTIVES:WEEK 2 OBJECTIVES:
Develop familiarity with the indications, goals and Develop familiarity with the indications, goals and therapy progression of treatment:therapy progression of treatment:
1) Non-pharmacologic therapy1) Non-pharmacologic therapy2) Pharmacologic therapy for glycemia2) Pharmacologic therapy for glycemia
- Oral agents: monotherapy and combination- Oral agents: monotherapy and combination - Insulin: monotherapy and in combination with - Insulin: monotherapy and in combination with OHAsOHAs
3) Therapy for nephropathy (if time permits)3) Therapy for nephropathy (if time permits)4) Therapy for neuropathy (if time permits)4) Therapy for neuropathy (if time permits)
Note: HTN, CAD, and Dyslipidemia will be discussed in Note: HTN, CAD, and Dyslipidemia will be discussed in future seminars…future seminars…
T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss…
CASE:CASE: Recall Mrs. X, our 58 yo woman with recently diagnosed Recall Mrs. X, our 58 yo woman with recently diagnosed
Type 2 DMType 2 DM She has completed her diabetes education course and She has completed her diabetes education course and
has learned how to self-monitor her blood glucosehas learned how to self-monitor her blood glucose She has returned to clinic in follow-up…She has returned to clinic in follow-up…
‘‘You explain that overall metabolic control (of You explain that overall metabolic control (of both glycemia and lipids) will be important to both glycemia and lipids) will be important to her future health’her future health’
• How can glycemic control be measured, and what are How can glycemic control be measured, and what are the CDA recommended target values for each test?the CDA recommended target values for each test?
CASE:CASE: Recall Mrs. X, our 58 yo woman with recently diagnosed Recall Mrs. X, our 58 yo woman with recently diagnosed
Type 2 DMType 2 DM She has completed her diabetes education course and She has completed her diabetes education course and
has learned how to self-monitor her blood glucosehas learned how to self-monitor her blood glucose She has returned to clinic in follow-up…She has returned to clinic in follow-up…
‘‘You explain that overall metabolic control (of You explain that overall metabolic control (of both glycemia and lipids) will be important to both glycemia and lipids) will be important to her future health’her future health’
• How can glycemic control be measured, and what are How can glycemic control be measured, and what are the CDA recommended target values for each test?the CDA recommended target values for each test?
RCTs have provided compelling RCTs have provided compelling evidence that long-term complications evidence that long-term complications of DM can be reduced with tight of DM can be reduced with tight glycemic control (DM1: DCCT, DM2: glycemic control (DM1: DCCT, DM2: UKPDS)UKPDS)
HbA1c levels >7% are associated with HbA1c levels >7% are associated with markedly increased risk of both micro markedly increased risk of both micro and macrovascular complications and macrovascular complications (regardless of underlying therapy)(regardless of underlying therapy)
RCTs have provided compelling RCTs have provided compelling evidence that long-term complications evidence that long-term complications of DM can be reduced with tight of DM can be reduced with tight glycemic control (DM1: DCCT, DM2: glycemic control (DM1: DCCT, DM2: UKPDS)UKPDS)
HbA1c levels >7% are associated with HbA1c levels >7% are associated with markedly increased risk of both micro markedly increased risk of both micro and macrovascular complications and macrovascular complications (regardless of underlying therapy)(regardless of underlying therapy)
T2DM: TherapyT2DM: Therapy

TYPE 2 DIABETES MELLITUS: TherapyTYPE 2 DIABETES MELLITUS: Therapy
Table 1. Targets for Glucose control in DM (CDA)Table 1. Targets for Glucose control in DM (CDA)
Ideal = Normal, nondiabeticIdeal = Normal, nondiabeticOptimal = Minimal long-term complications, difficult to achieveOptimal = Minimal long-term complications, difficult to achieveSuboptimal = May not prevent complications, but is attainable for the majority of Suboptimal = May not prevent complications, but is attainable for the majority of
patientspatientsInadequate = Markedly risk of long-term complicationsInadequate = Markedly risk of long-term complications
Table 1. Targets for Glucose control in DM (CDA)Table 1. Targets for Glucose control in DM (CDA)
Ideal = Normal, nondiabeticIdeal = Normal, nondiabeticOptimal = Minimal long-term complications, difficult to achieveOptimal = Minimal long-term complications, difficult to achieveSuboptimal = May not prevent complications, but is attainable for the majority of Suboptimal = May not prevent complications, but is attainable for the majority of
patientspatientsInadequate = Markedly risk of long-term complicationsInadequate = Markedly risk of long-term complications
Ideal Optimal Sub-optimal
Inadequate
HbA1C (%)
< 0.06 <0.07 0.07-0.084
>0.084
FPG or pre-P (mmol/L)
4-6 4-7 7.1-10 >10
2-hr post-P (mmol/L)
5-8 5-10 10.1-14 >14

T2DM: TherapyT2DM: Therapy
CASE:CASE: Mrs. X. has an HbA1c of Mrs. X. has an HbA1c of 0.950.95!!!!
Here are the BG levels from her record book for the last Here are the BG levels from her record book for the last few days:few days:
CASE:CASE: Mrs. X. has an HbA1c of Mrs. X. has an HbA1c of 0.950.95!!!!
Here are the BG levels from her record book for the last Here are the BG levels from her record book for the last few days:few days:
FBGFBG LunchLunch DinnerDinner
MM 1010 1414 1616
TT 9.59.5 1414 15.215.2
WW 1212 1212 1818

T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss…
Given the CDA goals, how would you Given the CDA goals, how would you characterize her glycemic control ?characterize her glycemic control ?
How would you begin to lower her blood How would you begin to lower her blood glucose levels ?glucose levels ?
Given the CDA goals, how would you Given the CDA goals, how would you characterize her glycemic control ?characterize her glycemic control ?
How would you begin to lower her blood How would you begin to lower her blood glucose levels ?glucose levels ?

T2DM: TherapyT2DM: Therapy
Mrs. X.’s glycemic control is INADEQUATE Mrs. X.’s glycemic control is INADEQUATE according to the CDA guidelines for both according to the CDA guidelines for both HbA1c and FBG (or post-prandial)HbA1c and FBG (or post-prandial)
The first step in improved glycemic control is The first step in improved glycemic control is to initiate non-pharmacologic therapyto initiate non-pharmacologic therapy
Mrs. X.’s glycemic control is INADEQUATE Mrs. X.’s glycemic control is INADEQUATE according to the CDA guidelines for both according to the CDA guidelines for both HbA1c and FBG (or post-prandial)HbA1c and FBG (or post-prandial)
The first step in improved glycemic control is The first step in improved glycemic control is to initiate non-pharmacologic therapyto initiate non-pharmacologic therapy

T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss… What are the major components of non-What are the major components of non-
pharmacologic therapy?pharmacologic therapy? What are the major components of non-What are the major components of non-
pharmacologic therapy?pharmacologic therapy?
Diet
Weight loss
Exercise
T2DM: Nutritional approaches (CDA)T2DM: Nutritional approaches (CDA)
Individualized counseling by registered Individualized counseling by registered dieticiandietician
Weight reduction to target (0.25-1 kg/week)Weight reduction to target (0.25-1 kg/week) for all patients with BMI > 25for all patients with BMI > 25 loss of 5% body weight can have significant loss of 5% body weight can have significant
health benefitshealth benefits
Individualized counseling by registered Individualized counseling by registered dieticiandietician
Weight reduction to target (0.25-1 kg/week)Weight reduction to target (0.25-1 kg/week) for all patients with BMI > 25for all patients with BMI > 25 loss of 5% body weight can have significant loss of 5% body weight can have significant
health benefitshealth benefits

Balanced diet from the Balanced diet from the 4 food groups with:4 food groups with: fat <30% of caloric fat <30% of caloric
intake (saturated fats intake (saturated fats <10%) <10%)
carbohydrates 50-carbohydrates 50-55%55%
protein 15-20% protein 15-20% sucrose containing sucrose containing
foods up to a foods up to a maximum of 10% of maximum of 10% of calories (< 10 g/d of calories (< 10 g/d of sugar alcohols)sugar alcohols)
Balanced diet from the Balanced diet from the 4 food groups with:4 food groups with: fat <30% of caloric fat <30% of caloric
intake (saturated fats intake (saturated fats <10%) <10%)
carbohydrates 50-carbohydrates 50-55%55%
protein 15-20% protein 15-20% sucrose containing sucrose containing
foods up to a foods up to a maximum of 10% of maximum of 10% of calories (< 10 g/d of calories (< 10 g/d of sugar alcohols)sugar alcohols)
T2DM: Nutritional approaches (CDA)T2DM: Nutritional approaches (CDA)

T2DM: Physical activity and Diabetes (CDA)T2DM: Physical activity and Diabetes (CDA)
Accumulate at least Accumulate at least 150 minutes (up to > 150 minutes (up to > 4 hrs) of moderate 4 hrs) of moderate intensity aerobic intensity aerobic exercise each week exercise each week (spread over at least (spread over at least 3 non-consecutive 3 non-consecutive days)days)
Encourage to Encourage to perform resistance perform resistance exercise training exercise training 3x/wk3x/wk
Accumulate at least Accumulate at least 150 minutes (up to > 150 minutes (up to > 4 hrs) of moderate 4 hrs) of moderate intensity aerobic intensity aerobic exercise each week exercise each week (spread over at least (spread over at least 3 non-consecutive 3 non-consecutive days)days)
Encourage to Encourage to perform resistance perform resistance exercise training exercise training 3x/wk3x/wk
T2DM: Physical Activity And Exercise (CDA)T2DM: Physical Activity And Exercise (CDA) Consider the need for a pre-emptive EST in Consider the need for a pre-emptive EST in
patients at high risk of occlusive vascular patients at high risk of occlusive vascular disease, neuropathy or microvascular disease disease, neuropathy or microvascular disease (or previously sedentary)(or previously sedentary)
NB: Exercise may induce short-term NB: Exercise may induce short-term hypoglycemiahypoglycemia
Emphasize: Emphasize: Proper foot careProper foot care Avoidance of exercise at times of poor metabolic Avoidance of exercise at times of poor metabolic
control or extreme heat or coldcontrol or extreme heat or cold The need to take rapid-acting CHO if pre-exercise BG The need to take rapid-acting CHO if pre-exercise BG
<5<5 Insulin injections at a site remote from the exercising Insulin injections at a site remote from the exercising
limblimb
Consider the need for a pre-emptive EST in Consider the need for a pre-emptive EST in patients at high risk of occlusive vascular patients at high risk of occlusive vascular disease, neuropathy or microvascular disease disease, neuropathy or microvascular disease (or previously sedentary)(or previously sedentary)
NB: Exercise may induce short-term NB: Exercise may induce short-term hypoglycemiahypoglycemia
Emphasize: Emphasize: Proper foot careProper foot care Avoidance of exercise at times of poor metabolic Avoidance of exercise at times of poor metabolic
control or extreme heat or coldcontrol or extreme heat or cold The need to take rapid-acting CHO if pre-exercise BG The need to take rapid-acting CHO if pre-exercise BG
<5<5 Insulin injections at a site remote from the exercising Insulin injections at a site remote from the exercising
limblimb
T2DM: TherapyT2DM: Therapy
CASE:CASE: Mrs. X. has followed your adviceMrs. X. has followed your advice
She has improved her diet and now walks 1.5 She has improved her diet and now walks 1.5 kms/d (She has lost 4 kg) kms/d (She has lost 4 kg)
However, her SMBG levels have not markedly However, her SMBG levels have not markedly improved and she has developed symptoms of improved and she has developed symptoms of sensory peripheral neuropathysensory peripheral neuropathy
Her electrolytes, creatinine and liver function Her electrolytes, creatinine and liver function tests and enzymes are normaltests and enzymes are normal
CASE:CASE: Mrs. X. has followed your adviceMrs. X. has followed your advice
She has improved her diet and now walks 1.5 She has improved her diet and now walks 1.5 kms/d (She has lost 4 kg) kms/d (She has lost 4 kg)
However, her SMBG levels have not markedly However, her SMBG levels have not markedly improved and she has developed symptoms of improved and she has developed symptoms of sensory peripheral neuropathysensory peripheral neuropathy
Her electrolytes, creatinine and liver function Her electrolytes, creatinine and liver function tests and enzymes are normaltests and enzymes are normal

T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss…
How can we further improve Mrs. X.’s How can we further improve Mrs. X.’s glycemic control ? glycemic control ?
What agents are available and how What agents are available and how would you choose one from among would you choose one from among them?them?
How can we further improve Mrs. X.’s How can we further improve Mrs. X.’s glycemic control ? glycemic control ?
What agents are available and how What agents are available and how would you choose one from among would you choose one from among them?them?

T2DM: TherapyT2DM: Therapy
• Oral Hypoglycemic Agents (OHAs) are the Oral Hypoglycemic Agents (OHAs) are the next step in managementnext step in management
• The 5 main classes of OHAs are:The 5 main classes of OHAs are:• Alpha-glucosidase inhibitors (acarbose)Alpha-glucosidase inhibitors (acarbose)• Biguanides (metformin)Biguanides (metformin)• Sulfonylureas (glyburide)Sulfonylureas (glyburide)• Meglitinides (repaglinide)Meglitinides (repaglinide)• Thiazolidinediones (rosiglitazone)Thiazolidinediones (rosiglitazone)
• Each has a unique mechanism of actionEach has a unique mechanism of action
• Oral Hypoglycemic Agents (OHAs) are the Oral Hypoglycemic Agents (OHAs) are the next step in managementnext step in management
• The 5 main classes of OHAs are:The 5 main classes of OHAs are:• Alpha-glucosidase inhibitors (acarbose)Alpha-glucosidase inhibitors (acarbose)• Biguanides (metformin)Biguanides (metformin)• Sulfonylureas (glyburide)Sulfonylureas (glyburide)• Meglitinides (repaglinide)Meglitinides (repaglinide)• Thiazolidinediones (rosiglitazone)Thiazolidinediones (rosiglitazone)
• Each has a unique mechanism of actionEach has a unique mechanism of action
T2DM: TherapyT2DM: Therapy
Secretagogues:Secretagogues: Sulfonylureas and meglitinides stimulate Sulfonylureas and meglitinides stimulate
pancreatic insulin releasepancreatic insulin release Insulin Sensitizers:Insulin Sensitizers:
Biguanides decrease hepatic glucose Biguanides decrease hepatic glucose production and enhance insulin-mediated production and enhance insulin-mediated glucose uptakeglucose uptake
Thiazolidinediones decrease insulin resistanceThiazolidinediones decrease insulin resistance Absorption Inhibitors:Absorption Inhibitors:
Alpha-glucosidase inhibitors slow absorption Alpha-glucosidase inhibitors slow absorption of starch and sucrose in the gutof starch and sucrose in the gut
Secretagogues:Secretagogues: Sulfonylureas and meglitinides stimulate Sulfonylureas and meglitinides stimulate
pancreatic insulin releasepancreatic insulin release Insulin Sensitizers:Insulin Sensitizers:
Biguanides decrease hepatic glucose Biguanides decrease hepatic glucose production and enhance insulin-mediated production and enhance insulin-mediated glucose uptakeglucose uptake
Thiazolidinediones decrease insulin resistanceThiazolidinediones decrease insulin resistance Absorption Inhibitors:Absorption Inhibitors:
Alpha-glucosidase inhibitors slow absorption Alpha-glucosidase inhibitors slow absorption of starch and sucrose in the gutof starch and sucrose in the gut

T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss…
How would you choose one medication How would you choose one medication from among the OHAs?from among the OHAs? Vary your choice according to your patient’s Vary your choice according to your patient’s
individual characteristicsindividual characteristics
How would you choose one medication How would you choose one medication from among the OHAs?from among the OHAs? Vary your choice according to your patient’s Vary your choice according to your patient’s
individual characteristicsindividual characteristics
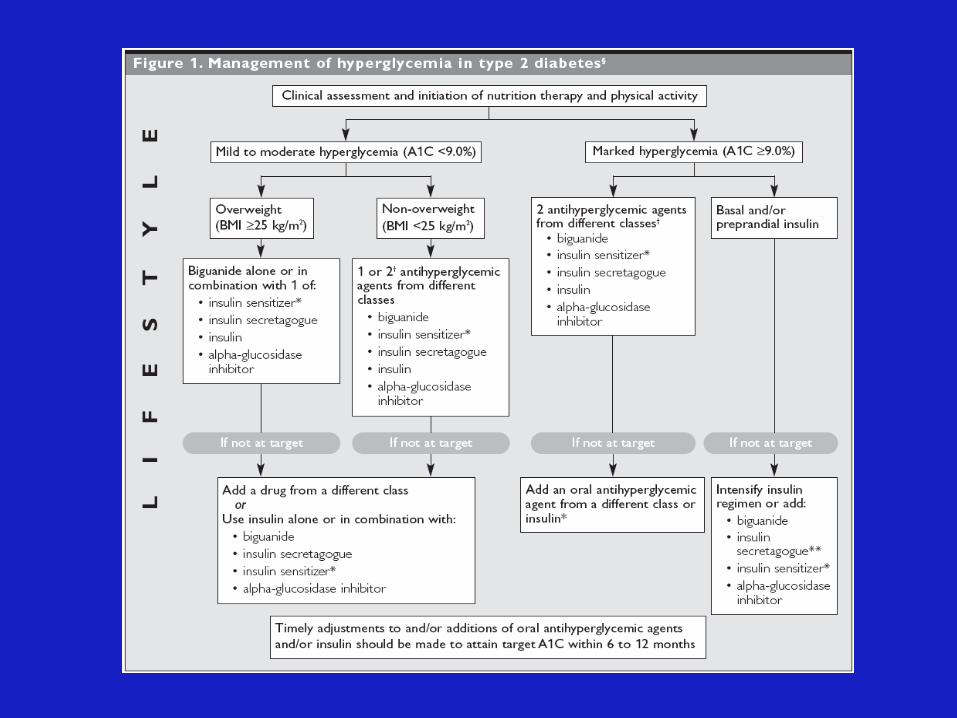

T2DM: Pharmacologic TherapyT2DM: Pharmacologic Therapy
With significant hyperglycemia (FPG > 10) With significant hyperglycemia (FPG > 10) →→ initiation of metformin and/or a sulfonylurea initiation of metformin and/or a sulfonylurea should be consideredshould be considered
Metformin is associated with both decreased Metformin is associated with both decreased weight gain and hypoglycemic eventsweight gain and hypoglycemic events
Metformin is contraindicated however in the Metformin is contraindicated however in the presence of significant renal or hepatic presence of significant renal or hepatic insufficiencyinsufficiency
With significant hyperglycemia (FPG > 10) With significant hyperglycemia (FPG > 10) →→ initiation of metformin and/or a sulfonylurea initiation of metformin and/or a sulfonylurea should be consideredshould be considered
Metformin is associated with both decreased Metformin is associated with both decreased weight gain and hypoglycemic eventsweight gain and hypoglycemic events
Metformin is contraindicated however in the Metformin is contraindicated however in the presence of significant renal or hepatic presence of significant renal or hepatic insufficiencyinsufficiency

• typically used in combination• GI SEs
• contraindicated in hepatic dysfunction• used in combination with insulin – may increase edema and CHF
• contraindicated in persons with renal or hepatic dysfunction• less weight gain• GI SEs
• risks of hypoglycemia and weight gain • use with caution in the elderly
T2DM: Therapy – Take a minute to discuss…T2DM: Therapy – Take a minute to discuss…
CASE:CASE: You choose metformin for Mrs. X. and You choose metformin for Mrs. X. and
maximize the dose to 1 g po bidmaximize the dose to 1 g po bid Unfortunately, she still has not Unfortunately, she still has not
achieved her target glucose goalsachieved her target glucose goals
What is the next step?What is the next step?
CASE:CASE: You choose metformin for Mrs. X. and You choose metformin for Mrs. X. and
maximize the dose to 1 g po bidmaximize the dose to 1 g po bid Unfortunately, she still has not Unfortunately, she still has not
achieved her target glucose goalsachieved her target glucose goals
What is the next step?What is the next step?
T2DM: Pharmacologic TherapyT2DM: Pharmacologic Therapy
1. Add agents from different classes and maximize the doses (glyburide, acarbose and/or rosiglitazone)
2. Consider adding an insulin HS dose to the OHAs
3. Switch to multi-injection insulin therapy alone or with concomitant oral acarbose, biguanide or thiazolidinedione therapy
1. Add agents from different classes and maximize the doses (glyburide, acarbose and/or rosiglitazone)
2. Consider adding an insulin HS dose to the OHAs
3. Switch to multi-injection insulin therapy alone or with concomitant oral acarbose, biguanide or thiazolidinedione therapy

T2DM: Insulin Therapy
T2DM Complications: NephropathyT2DM Complications: Nephropathy
CASE: Mrs. X. was noted to have trace proteinuria on
dipstick by the family MD (You obtain a subsequent albumin:creatinine ratio of 3.0 on a random daytime urine)
Over the next 3 months two further ACRs of 2.8 and 2.7 are obtained (a 24-hr urine collection confirms microalbuminuria at 225 mg/d)
CASE: Mrs. X. was noted to have trace proteinuria on
dipstick by the family MD (You obtain a subsequent albumin:creatinine ratio of 3.0 on a random daytime urine)
Over the next 3 months two further ACRs of 2.8 and 2.7 are obtained (a 24-hr urine collection confirms microalbuminuria at 225 mg/d)

T2DM Complications: Nephropathy – Take a minute to discuss…T2DM Complications: Nephropathy – Take a minute to discuss…
How would you minimize any further How would you minimize any further progression of Mrs. X.’s nephropathy?progression of Mrs. X.’s nephropathy?
How would you minimize any further How would you minimize any further progression of Mrs. X.’s nephropathy?progression of Mrs. X.’s nephropathy?

T2DM Complications: NephropathyT2DM Complications: Nephropathy

T2DM Complications: NephropathyT2DM Complications: Nephropathy
1) ACE-I/ARB • adjust dose to obtain target BP if the patient is hypertensive
2) Intensify glucose control
3) Consider dietary protein restriction • controversial
• mentioned in CDA guidelines• ADA guidelines suggest 10% of calories should be
protein with overt nephropathy [0.8 g/kg/d] with a reduction to 0.6 g/kg/d with further decline in creatinine clearance
4) Referral to nephrology with greater than 50% decrease in creatinine clearance
1) ACE-I/ARB • adjust dose to obtain target BP if the patient is hypertensive
2) Intensify glucose control
3) Consider dietary protein restriction • controversial
• mentioned in CDA guidelines• ADA guidelines suggest 10% of calories should be
protein with overt nephropathy [0.8 g/kg/d] with a reduction to 0.6 g/kg/d with further decline in creatinine clearance
4) Referral to nephrology with greater than 50% decrease in creatinine clearance

T2DM Complications: NeuropathyT2DM Complications: Neuropathy
CASE:CASE: During follow-up, you confirm that Mrs. X. has During follow-up, you confirm that Mrs. X. has
mild to moderate stocking-glove sensory mild to moderate stocking-glove sensory neuropathy with decreased vibration at the great neuropathy with decreased vibration at the great toes and midfoot, and a loss of sensitivity to 10 toes and midfoot, and a loss of sensitivity to 10 gm monofilament at the great toesgm monofilament at the great toes
She also complains of a constant prickly, painful She also complains of a constant prickly, painful sensation over the same distribution which sensation over the same distribution which keeps her awake at nightkeeps her awake at night
CASE:CASE: During follow-up, you confirm that Mrs. X. has During follow-up, you confirm that Mrs. X. has
mild to moderate stocking-glove sensory mild to moderate stocking-glove sensory neuropathy with decreased vibration at the great neuropathy with decreased vibration at the great toes and midfoot, and a loss of sensitivity to 10 toes and midfoot, and a loss of sensitivity to 10 gm monofilament at the great toesgm monofilament at the great toes
She also complains of a constant prickly, painful She also complains of a constant prickly, painful sensation over the same distribution which sensation over the same distribution which keeps her awake at nightkeeps her awake at night
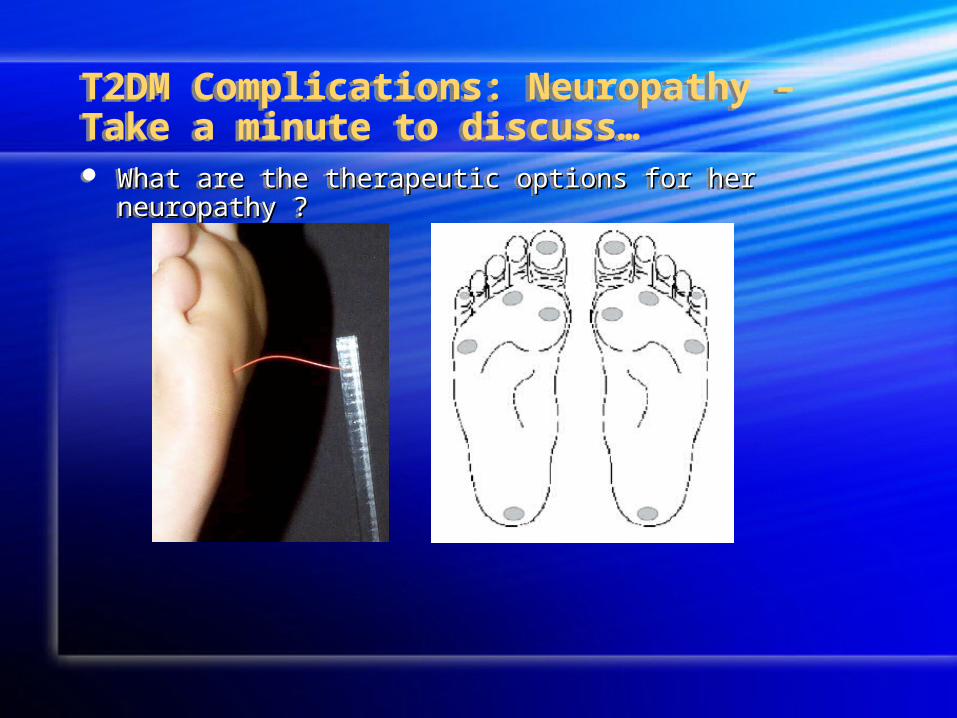
T2DM Complications: Neuropathy – Take a minute to discuss…T2DM Complications: Neuropathy – Take a minute to discuss… What are the therapeutic options for her neuropathy ?What are the therapeutic options for her neuropathy ? What are the therapeutic options for her neuropathy ?What are the therapeutic options for her neuropathy ?
T2DM: Complications: NeuropathyT2DM: Complications: Neuropathy
TreatmentTreatment1) Intensify glucose control1) Intensify glucose control
2) Low dose tricyclic antidepressant or 2) Low dose tricyclic antidepressant or carbamazepinecarbamazepine
3) Topical capsaicin ointment3) Topical capsaicin ointment
TreatmentTreatment1) Intensify glucose control1) Intensify glucose control
2) Low dose tricyclic antidepressant or 2) Low dose tricyclic antidepressant or carbamazepinecarbamazepine
3) Topical capsaicin ointment3) Topical capsaicin ointment

T2DM: Week Two ObjectivesT2DM: Week Two Objectives
We have reviewed:We have reviewed:
1) Non-pharmacologic therapy1) Non-pharmacologic therapy2) Pharmacologic therapy for glycemia2) Pharmacologic therapy for glycemia
- Oral agents: monotherapy and Oral agents: monotherapy and combinationcombination
- Insulin: monotherapy and in combination Insulin: monotherapy and in combination with OHAswith OHAs
3) Therapy for nephropathy3) Therapy for nephropathy4) Therapy for neuropathy4) Therapy for neuropathy
We have reviewed:We have reviewed:
1) Non-pharmacologic therapy1) Non-pharmacologic therapy2) Pharmacologic therapy for glycemia2) Pharmacologic therapy for glycemia
- Oral agents: monotherapy and Oral agents: monotherapy and combinationcombination
- Insulin: monotherapy and in combination Insulin: monotherapy and in combination with OHAswith OHAs
3) Therapy for nephropathy3) Therapy for nephropathy4) Therapy for neuropathy4) Therapy for neuropathy