Embed Size (px)
Citation preview
Understanding the Method Behind the Madness:
An Exploration of Methodologies Designed to Improve the Quality of
Clinical Ethics Consultation
Understanding the Method Behind the Madness:
An Exploration of Methodologies Designed to Improve the Quality of
Clinical Ethics Consultation
Mark Repenshek, PhDHealthcare EthicistColumbia St. Mary’[email protected]
Mark Repenshek, PhDHealthcare EthicistColumbia St. Mary’[email protected]
Context for Ethics ConsultationContext for Ethics Consultation• Columbia St. Mary’s Health System
– Four Acute Care Hospitals ~922 beds– 64 physician clinics with ~360 employed physicians– FY 2009: 404,637 outpatient visits; 68,396 ED visits; 3430
births
– Ethics Consultation Service:• Two Medical Staff Ethics Committees• One PhD Ethicist; Ad Hoc Consultation Model/Advisement
Model
– Ethics Consultation for Database:• 352 consults from January 2003 through December 2009• Cases:
– Identified ethical reason for consultation– Identified discipline requesting– CSM Ethics consultation service engaged– Ethics consultation documented– Ethics recommendations made to case
• Columbia St. Mary’s Health System– Four Acute Care Hospitals ~922 beds– 64 physician clinics with ~360 employed physicians– FY 2009: 404,637 outpatient visits; 68,396 ED visits; 3430
births
– Ethics Consultation Service:• Two Medical Staff Ethics Committees• One PhD Ethicist; Ad Hoc Consultation Model/Advisement
Model
– Ethics Consultation for Database:• 352 consults from January 2003 through December 2009• Cases:
– Identified ethical reason for consultation– Identified discipline requesting– CSM Ethics consultation service engaged– Ethics consultation documented– Ethics recommendations made to case

Previous Conclusions about
Ethics Consultation
Previous Conclusions about
Ethics Consultation
Clinical Consultation Changing Organizational Practice?Clinical Consultation Changing Organizational Practice?
• Ethics Tracker Database– August 2006-October 2006– 3 consults related to Intra/peri-operative Code Status
• MD Association Guidelines – American College of Surgeons: ST-19 Statement on Advance Directive
by Patients: “Do Not Resuscitate” in the Operating Room
– American Society of Anesthesiologists: Ethical Guidelines for the Anesthesia Care of Patients with Do-Not-Resuscitate Orders
• Goal: Initiate opportunity within existing pre-procedure processes for MD to address with patient or designated surrogate(s) existing directives to limit the use of resuscitation procedures
– Dept of Surgery follow-up re: Ethics Case Consultations– Grand Rounds follow-up with CME Accountabilities for CIP
• Ethics Tracker Database– August 2006-October 2006– 3 consults related to Intra/peri-operative Code Status
• MD Association Guidelines – American College of Surgeons: ST-19 Statement on Advance Directive
by Patients: “Do Not Resuscitate” in the Operating Room
– American Society of Anesthesiologists: Ethical Guidelines for the Anesthesia Care of Patients with Do-Not-Resuscitate Orders
• Goal: Initiate opportunity within existing pre-procedure processes for MD to address with patient or designated surrogate(s) existing directives to limit the use of resuscitation procedures
– Dept of Surgery follow-up re: Ethics Case Consultations– Grand Rounds follow-up with CME Accountabilities for CIP
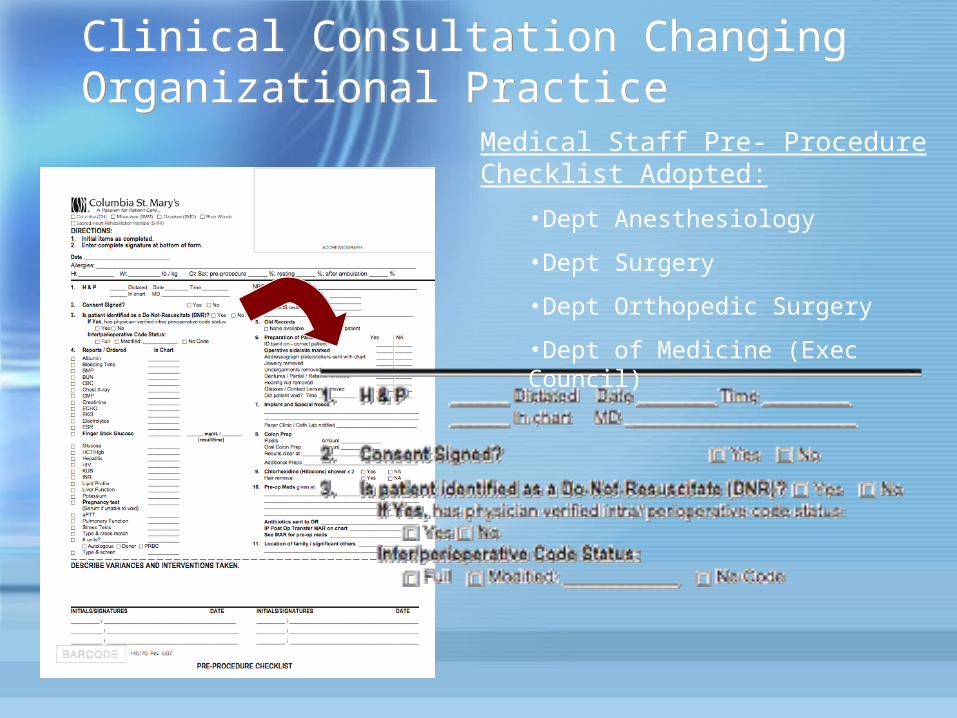
Clinical Consultation Changing Organizational PracticeClinical Consultation Changing Organizational Practice
Medical Staff Pre- Procedure Checklist Adopted:
•Dept Anesthesiology
•Dept Surgery
•Dept Orthopedic Surgery
•Dept of Medicine (Exec Council)

New Model to Measure
Patient/Organization Impact
New Model to Measure
Patient/Organization Impact
Ethics Consultation ModelEthics Consultation ModelEthics Consultation Service:
• Two Medical Staff Ethics Committees• One PhD Ethicist; Ad Hoc Consultation Model/Advisement Model
Ad Hoc Consultation Model/AdvisementAdvisement: Requests include, but not limited to, questions concerning interpretation of the Ethical and Religious
Directives for Catholic Healthcare Services, 5th ed., elaboration on CSM Ethics Policies, or matters of mere procedural clarification.
Ad Hoc Consultation: required for all consults that are not advisory in nature.
Ethics Consultation Service:• Two Medical Staff Ethics Committees• One PhD Ethicist; Ad Hoc Consultation Model/Advisement Model
Ad Hoc Consultation Model/AdvisementAdvisement: Requests include, but not limited to, questions concerning interpretation of the Ethical and Religious
Directives for Catholic Healthcare Services, 5th ed., elaboration on CSM Ethics Policies, or matters of mere procedural clarification.
Ad Hoc Consultation: required for all consults that are not advisory in nature.
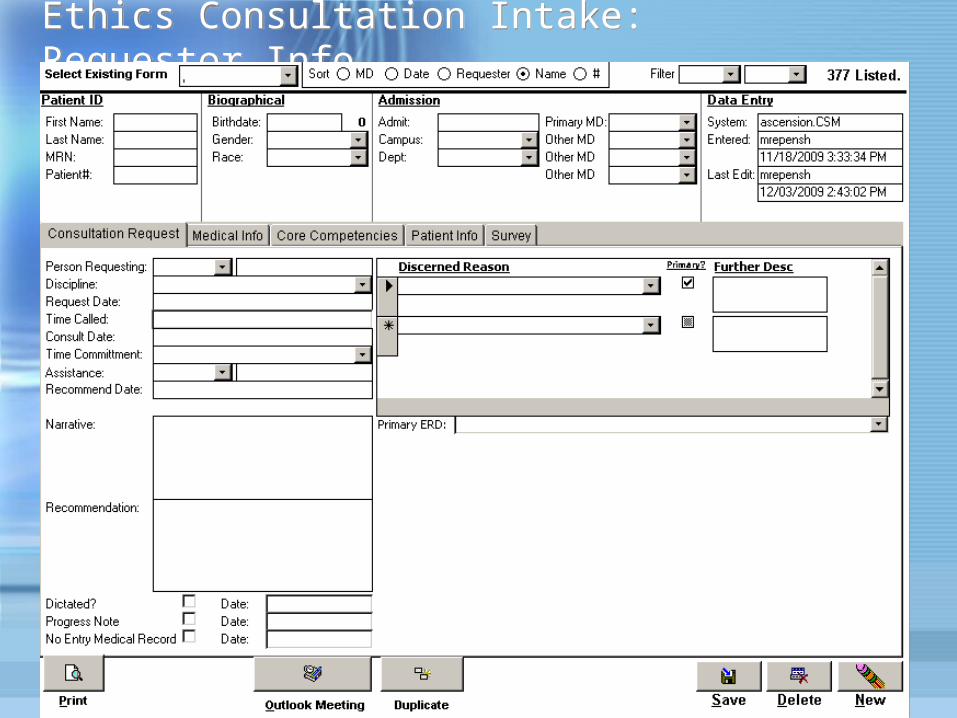
Ethics Consultation Intake: Requestor InfoEthics Consultation Intake: Requestor Info
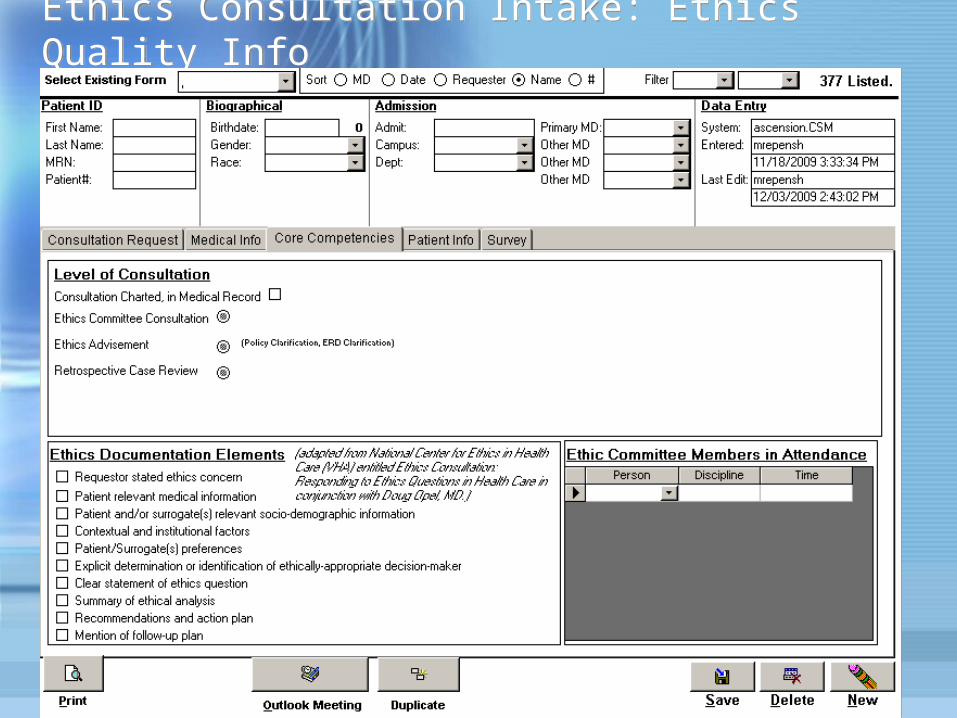
Ethics Consultation Intake: Ethics Quality InfoEthics Consultation Intake: Ethics Quality Info
Clinical Ethics Consultation: Columbia St. Mary’s Health SystemClinical Ethics Consultation: Columbia St. Mary’s Health System
• Ethics Consultation implemented the ASBH Process for Ethics Consultation in 2003
The Report of the ASBH. Core Competencies for Health Care Ethics Consultation. 1998, section 1.2
• Appropriate competencies added re: Skills for Ethics Consultation relative to the Ethical and Religious Directives for Catholic Healthcare Services
The Report of the ASBH. Core Competencies for Health Care Ethics Consultation. 1998, section 2.2
Ascension Health Core Competencies for Ethics Consultation in Catholic Health Care, see: https://www.ascensionhealth.org/ethics/affiliates/main.asp
• Ethics Consultation implemented the ASBH Process for Ethics Consultation in 2003
The Report of the ASBH. Core Competencies for Health Care Ethics Consultation. 1998, section 1.2
• Appropriate competencies added re: Skills for Ethics Consultation relative to the Ethical and Religious Directives for Catholic Healthcare Services
The Report of the ASBH. Core Competencies for Health Care Ethics Consultation. 1998, section 2.2
Ascension Health Core Competencies for Ethics Consultation in Catholic Health Care, see: https://www.ascensionhealth.org/ethics/affiliates/main.asp
Clinical Ethics Consultation: Columbia St. Mary’s Health SystemClinical Ethics Consultation: Columbia St. Mary’s Health System
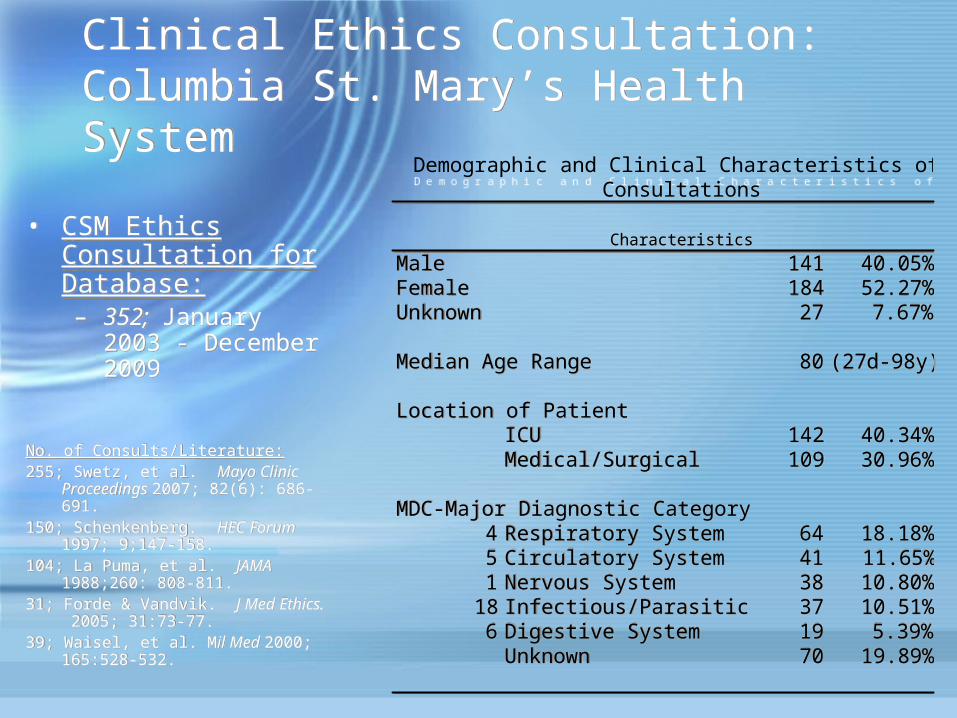
• CSM Ethics Consultation for Database:– 352; January 2003
- December 2009
No. of Consults/Literature:255; Swetz, et al. Mayo Clinic
Proceedings 2007; 82(6): 686-691.
150; Schenkenberg. HEC Forum 1997; 9;147-158.
104; La Puma, et al. JAMA 1988;260: 808-811.
31; Forde & Vandvik. J Med Ethics. 2005; 31:73-77.
39; Waisel, et al. Mil Med 2000; 165:528-532.
• CSM Ethics Consultation for Database:– 352; January 2003
- December 2009
No. of Consults/Literature:255; Swetz, et al. Mayo Clinic
Proceedings 2007; 82(6): 686-691.
150; Schenkenberg. HEC Forum 1997; 9;147-158.
104; La Puma, et al. JAMA 1988;260: 808-811.
31; Forde & Vandvik. J Med Ethics. 2005; 31:73-77.
39; Waisel, et al. Mil Med 2000; 165:528-532.
Male 141 40.05%Female 184 52.27%Unknown 27 7.67%
Median Age Range 80 (27d-98y)
Location of PatientICU 142 40.34%Medical/Surgical 109 30.96%
MDC-Major Diagnostic Category4 Respiratory System 64 18.18%5 Circulatory System 41 11.65%1 Nervous System 38 10.80%
18 Infectious/Parasitic 37 10.51%6 Digestive System 19 5.39%
Unknown 70 19.89%
Demographic and Clinical Characteristics of 352 Ethics Consultations
Characteristics
Male 141 40.05%Female 184 52.27%Unknown 27 7.67%
Median Age Range 80 (27d-98y)
Location of PatientICU 142 40.34%Medical/Surgical 109 30.96%
MDC-Major Diagnostic Category4 Respiratory System 64 18.18%5 Circulatory System 41 11.65%1 Nervous System 38 10.80%
18 Infectious/Parasitic 37 10.51%6 Digestive System 19 5.39%
Unknown 70 19.89%
Demographic and Clinical Characteristics of 352 Ethics Consultations
Characteristics
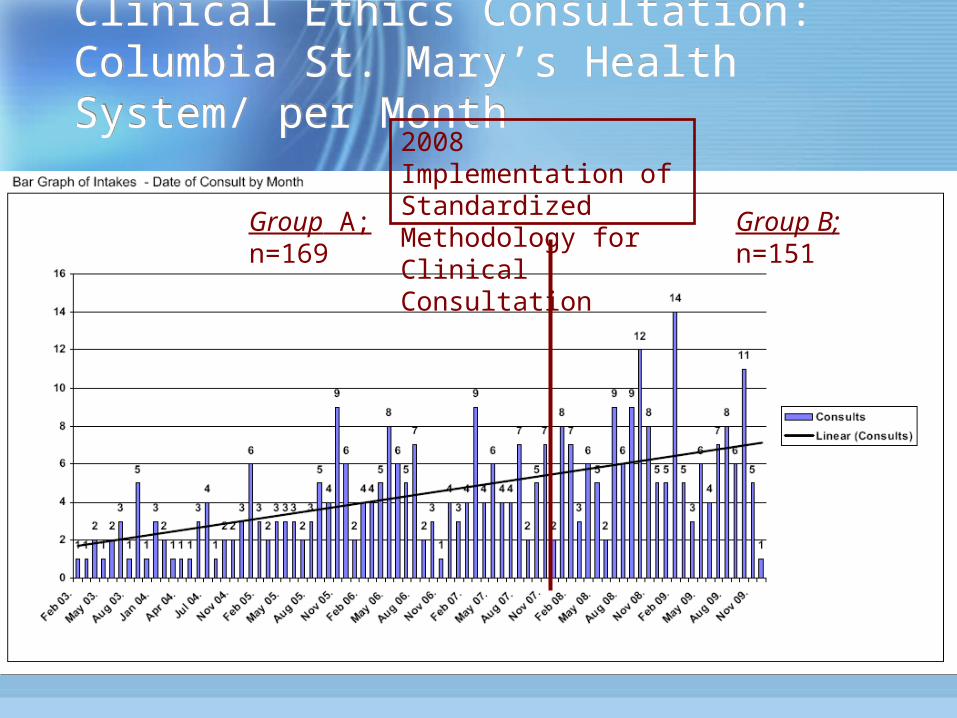
Clinical Ethics Consultation: Columbia St. Mary’s Health System/ per Month
Clinical Ethics Consultation: Columbia St. Mary’s Health System/ per Month
Group A; n=169
Group B; n=151
2008 Implementation of Standardized Methodology for Clinical Consultation
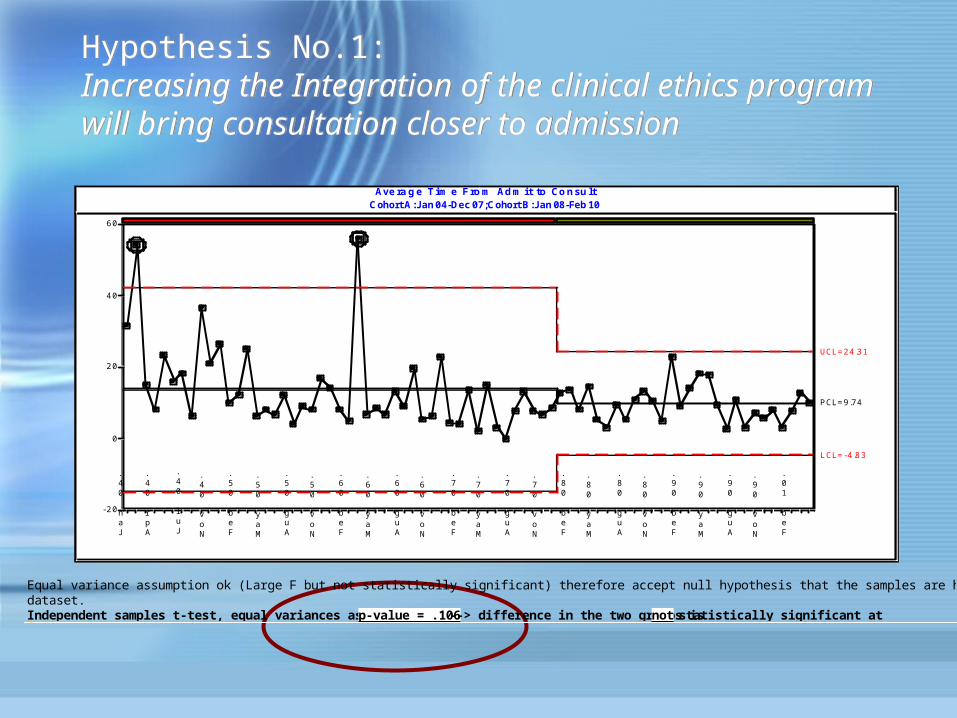
Hypothesis No.1: Increasing the Integration of the clinical ethics program will bring consultation closer to admission
Hypothesis No.1: Increasing the Integration of the clinical ethics program will bring consultation closer to admission
Ave ra g e T im e F ro m Ad m it to Co n su ltCohort A: Jan 04-Dec 07; Cohort B: Jan 08-Feb 10
- 2 0
0
2 0
4 0
6 0
Jan 04.
Apr 04.
Jul 04.
Nov 04.
Feb 05.
May 05.
Aug 05.
Nov 05.
Feb 06.
May 06.
Aug 06.
Nov 06.
Feb 07.
May 07.
Aug 07.
Nov 07.
Feb 08.
May 08.
Aug 08.
Nov 08.
Feb 09.
May 09.
Aug 09.
Nov 09.
Feb 10.
UCL= 2 4 .3 1
L CL= - 4 .8 3
PCL= 9 .74
Ave ra g e T im e F ro m Ad m it to Co n su ltCohort A: Jan 04-Dec 07; Cohort B: Jan 08-Feb 10
- 2 0
0
2 0
4 0
6 0
Jan 04.
Apr 04.
Jul 04.
Nov 04.
Feb 05.
May 05.
Aug 05.
Nov 05.
Feb 06.
May 06.
Aug 06.
Nov 06.
Feb 07.
May 07.
Aug 07.
Nov 07.
Feb 08.
May 08.
Aug 08.
Nov 08.
Feb 09.
May 09.
Aug 09.
Nov 09.
Feb 10.
UCL= 2 4 .3 1
L CL= - 4 .8 3
PCL= 9 .74
Equal variance assumption ok (Large F but not statistically significant) therefore accept null hypothesis that the samples are homegeneous. Use equal variances dataset.Independent samples t-test, equal variances assumed, p-value = .106 --> difference in the two groups is not statistically significant at 95%
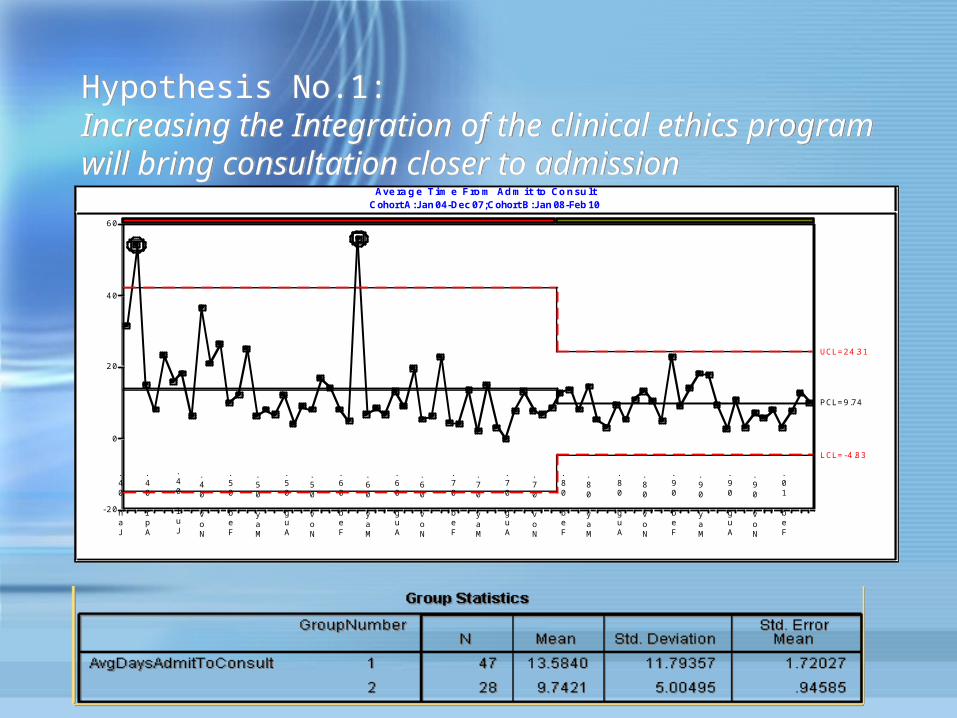
Hypothesis No.1: Increasing the Integration of the clinical ethics program will bring consultation closer to admission
Hypothesis No.1: Increasing the Integration of the clinical ethics program will bring consultation closer to admission
Ave ra g e T im e F ro m Ad m it to Co n su ltCohort A: Jan 04-Dec 07; Cohort B: Jan 08-Feb 10
- 2 0
0
2 0
4 0
6 0
Jan 04.
Apr 04.
Jul 04.
Nov 04.
Feb 05.
May 05.
Aug 05.
Nov 05.
Feb 06.
May 06.
Aug 06.
Nov 06.
Feb 07.
May 07.
Aug 07.
Nov 07.
Feb 08.
May 08.
Aug 08.
Nov 08.
Feb 09.
May 09.
Aug 09.
Nov 09.
Feb 10.
UCL= 2 4 .3 1
L CL= - 4 .8 3
PCL= 9 .74
Ave ra g e T im e F ro m Ad m it to Co n su ltCohort A: Jan 04-Dec 07; Cohort B: Jan 08-Feb 10
- 2 0
0
2 0
4 0
6 0
Jan 04.
Apr 04.
Jul 04.
Nov 04.
Feb 05.
May 05.
Aug 05.
Nov 05.
Feb 06.
May 06.
Aug 06.
Nov 06.
Feb 07.
May 07.
Aug 07.
Nov 07.
Feb 08.
May 08.
Aug 08.
Nov 08.
Feb 09.
May 09.
Aug 09.
Nov 09.
Feb 10.
UCL= 2 4 .3 1
L CL= - 4 .8 3
PCL= 9 .74
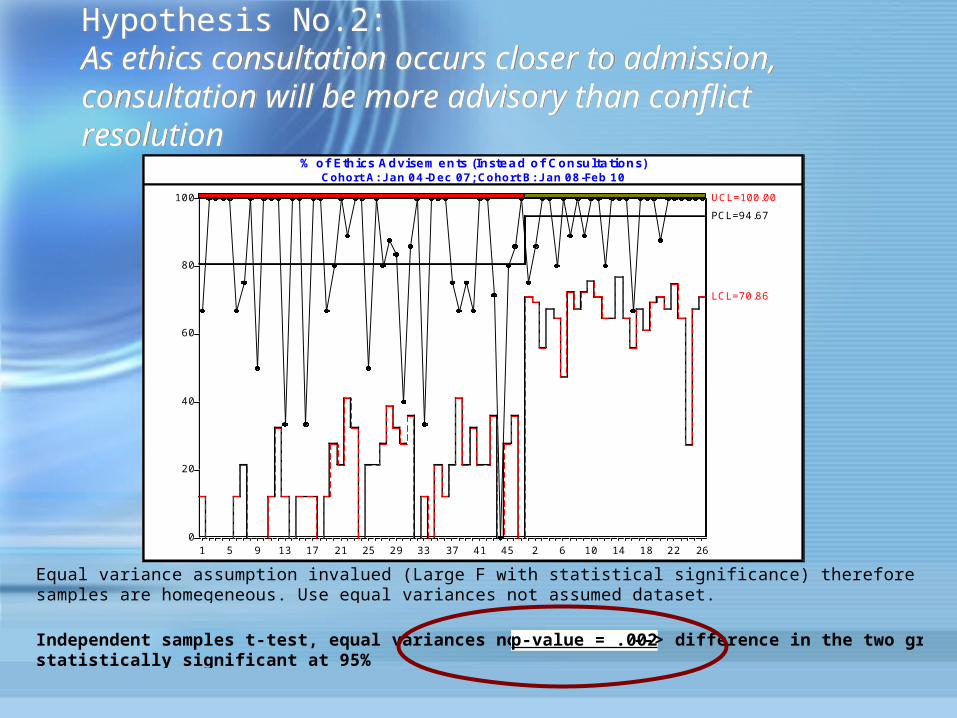
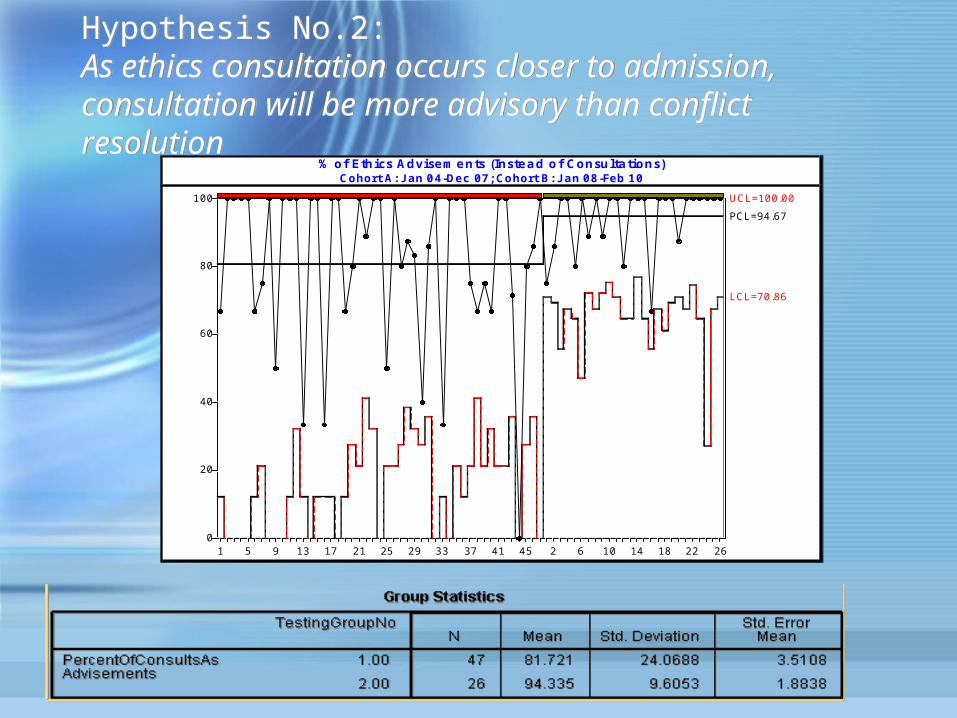
Hypothesis No.2: As ethics consultation occurs closer to admission, consultation will be more advisory than conflict resolution
Hypothesis No.2: As ethics consultation occurs closer to admission, consultation will be more advisory than conflict resolution
% of Eth ics Advise m e nts (Inste a d o f Consulta tions)Cohort A: Jan 0 4 -Dec 07 ; Cohort B: Jan 08 -Feb 10
0
20
40
60
80
100
1 5 9 13 17 21 25 29 33 37 41 45 2 6 10 14 18 22 26
UCL=100.00
LCL=70.86
PCL=94.67
Equal variance assumption invalued (Large F with statistical significance) therefore reject the null hypothesis that the samples are homegeneous. Use equal variances not assumed dataset.
Independent samples t-test, equal variances not assumed, p-value = .002 --> difference in the two groups is statistically significant at 95%
Hypothesis No.2: As ethics consultation occurs closer to admission, consultation will be more advisory than conflict resolution
Hypothesis No.2: As ethics consultation occurs closer to admission, consultation will be more advisory than conflict resolution
% of Eth ics Advise m e nts (Inste a d o f Consulta tions)Cohort A: Jan 0 4 -Dec 07 ; Cohort B: Jan 08 -Feb 10
0
20
40
60
80
100
1 5 9 13 17 21 25 29 33 37 41 45 2 6 10 14 18 22 26
UCL=100.00
LCL=70.86
PCL=94.67
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Assumptions:– Identified ethical reason for consultation– Identified discipline requesting– CSM Ethics consultation service engaged– Ethics consultation documented– Ethics recommendations made to case
Inclusion Criteria:• Acuity of patient population: ICU• Complexity of patient population: 2 hospitalizations within past six
months for same primary DRG
Exclusion Criteria:• No retrospective reviews--level of consult request
Assumptions:– Identified ethical reason for consultation– Identified discipline requesting– CSM Ethics consultation service engaged– Ethics consultation documented– Ethics recommendations made to case
Inclusion Criteria:• Acuity of patient population: ICU• Complexity of patient population: 2 hospitalizations within past six
months for same primary DRG
Exclusion Criteria:• No retrospective reviews--level of consult request
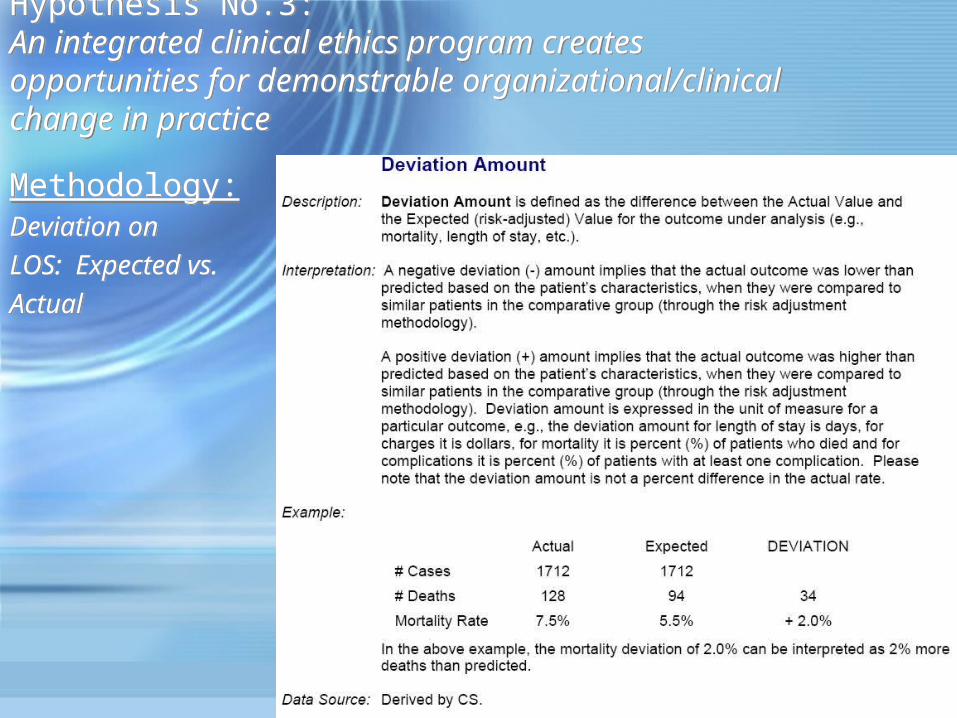
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
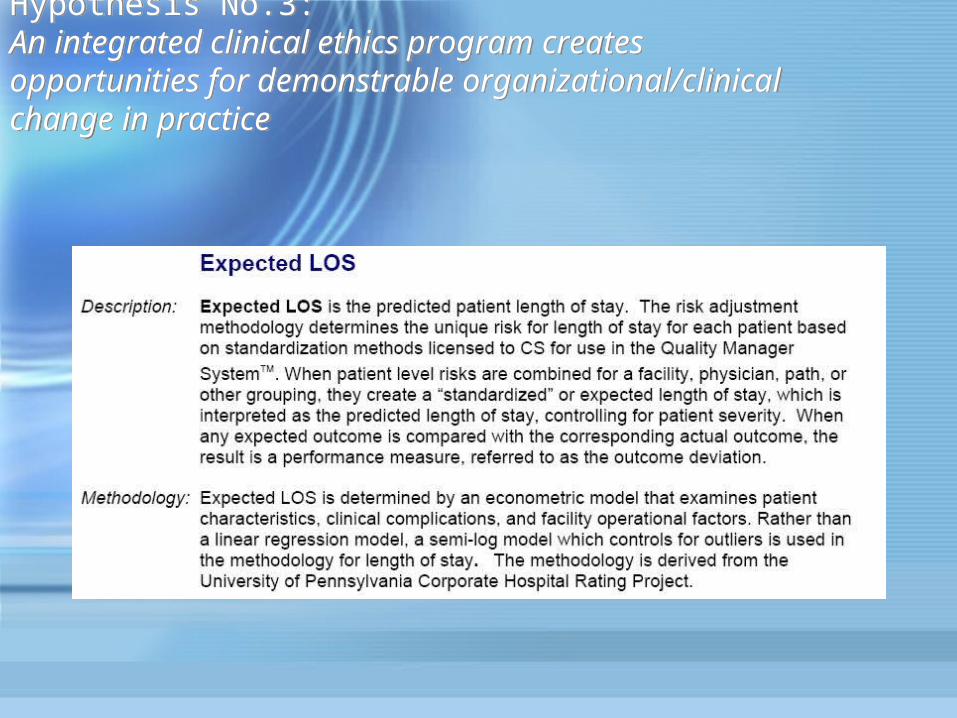
Methodology:Deviation on LOS: Expected vs. Actual
Methodology:Deviation on LOS: Expected vs. Actual
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Facility# of
Stays
# of Unique Patients
Actual LOS
Standard
Practice Expected LOS
LOS Deviation
# of Stays
# of Unique Patients
Actual LOS
Standard
Practice Expected LOS
LOS Deviation
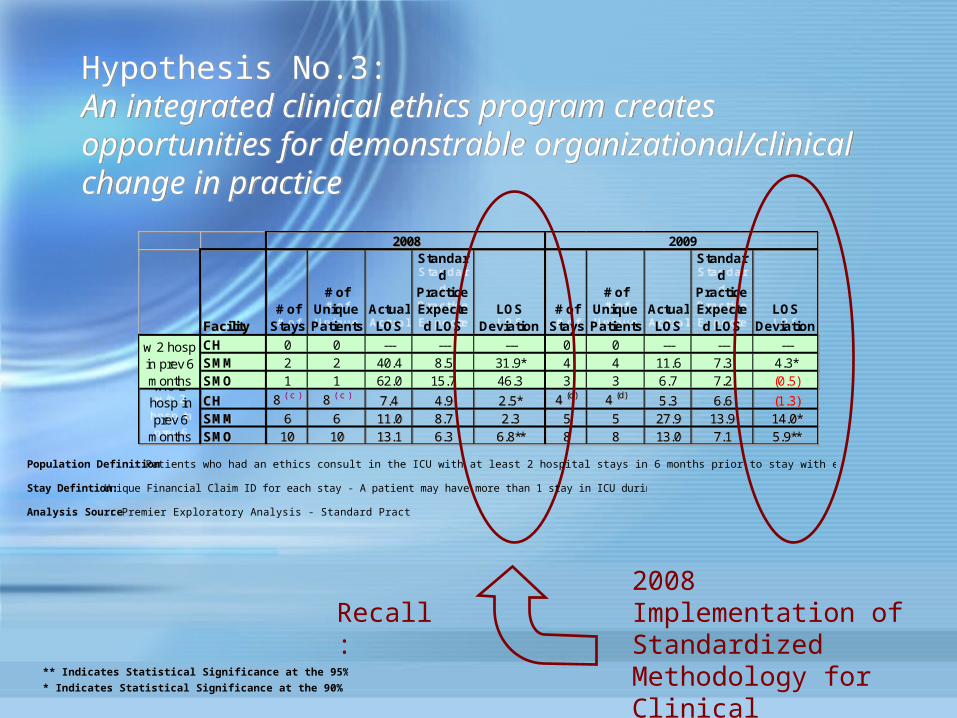
CH 0 0 --- --- --- 0 0 --- --- ---SMM 2 2 40.4 8.5 31.9* 4 4 11.6 7.3 4.3*SMO 1 1 62.0 15.7 46.3 3 3 6.7 7.2 (0.5)
CH 8 ( c ) 8 ( c ) 7.4 4.9 2.5* 4 (d) 4 (d) 5.3 6.6 (1.3)SMM 6 6 11.0 8.7 2.3 5 5 27.9 13.9 14.0*SMO 10 10 13.1 6.3 6.8** 8 8 13.0 7.1 5.9**
w 2 hosp in prev 6 monthsw/o 2 hosp in prev 6
months
2008 2009
Facility# of
Stays
# of Unique Patients
Actual LOS
Standard
Practice Expected LOS
LOS Deviation
# of Stays
# of Unique Patients
Actual LOS
Standard
Practice Expected LOS
LOS Deviation
CH 0 0 --- --- --- 0 0 --- --- ---SMM 2 2 40.4 8.5 31.9* 4 4 11.6 7.3 4.3*SMO 1 1 62.0 15.7 46.3 3 3 6.7 7.2 (0.5)
CH 8 ( c ) 8 ( c ) 7.4 4.9 2.5* 4 (d) 4 (d) 5.3 6.6 (1.3)SMM 6 6 11.0 8.7 2.3 5 5 27.9 13.9 14.0*SMO 10 10 13.1 6.3 6.8** 8 8 13.0 7.1 5.9**
w 2 hosp in prev 6 monthsw/o 2 hosp in prev 6
months
2008 2009
2008 Implementation of Standardized Methodology for Clinical Consultation
Recall:
Population Definition : Patients who had an ethics consult in the ICU with at least 2 hospital stays in 6 months prior to stay with ethics consult (LOS aggregate for stay with ethics consult)
** Indicates Statistical Significance at the 95% Confidence Level
* Indicates Statistical Significance at the 90% Confidence Level
Stay Defintion: Unique Financial Claim ID for each stay - A patient may have more than 1 stay in ICU during measurement timeframe
Analysis Source: Premier Exploratory Analysis - Standard Practice Comparison
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
Hypothesis No.3: An integrated clinical ethics program creates opportunities for demonstrable organizational/clinical change in practice
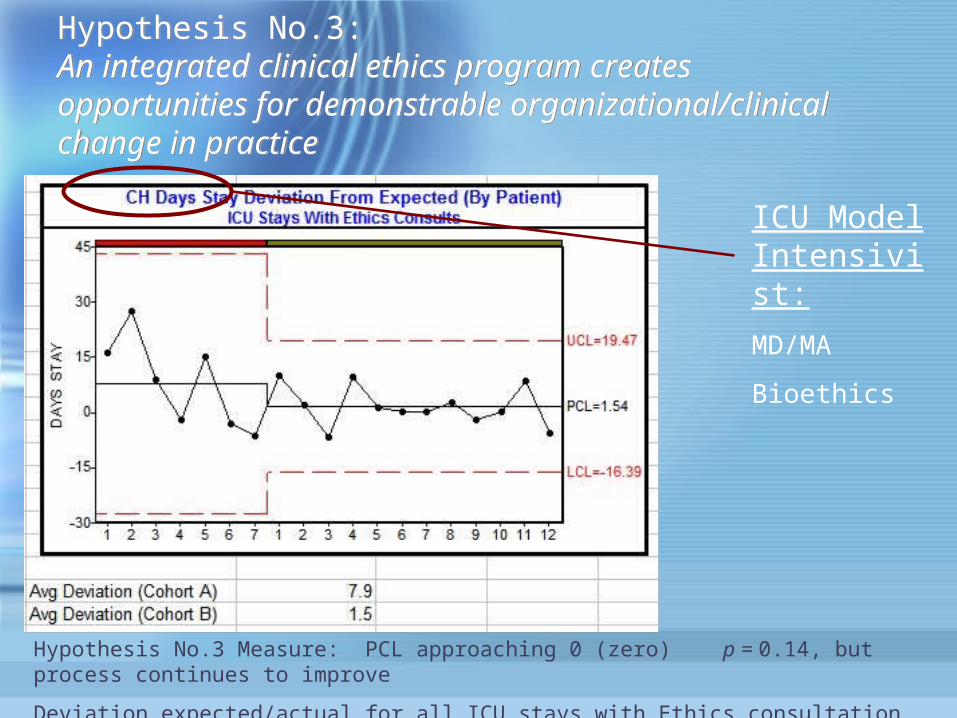
Hypothesis No.3 Measure: PCL approaching 0 (zero) p = 0.14, but process continues to improve
Deviation expected/actual for all ICU stays with Ethics consultation Cohort A/Cohort B--CH
ICU Model Intensivist:
MD/MA
Bioethics

ConclusionsConclusions• Ethics consultation can be measured both in process and
impact--No free pass on quality measures;
• Conversation has and must continue to move from whether to measure to how to measure;
• Rigorous debate on whether these methodologies are on target in terms of capturing process/impact of ethics consultation;
• Implement methodologies or adaptations thereof to larger sample sets (i.e., VHA, Ascension, etc.) to test the validity with larger n.
• Ethics consultation can be measured both in process and impact--No free pass on quality measures;
• Conversation has and must continue to move from whether to measure to how to measure;
• Rigorous debate on whether these methodologies are on target in terms of capturing process/impact of ethics consultation;
• Implement methodologies or adaptations thereof to larger sample sets (i.e., VHA, Ascension, etc.) to test the validity with larger n.





















![The Games! The Upsets! The Madness!: March Madness [INFOGRAPHIC]](https://img.pdfslide.us/doc/110x75/577cdcc71a28ab9e78ab621f/the-games-the-upsets-the-madness-march-madness-infographic.jpg)



