Embed Size (px)
Citation preview

Understanding how Jakafi® (ruxolitinib) inhibits* overactive JAK pathway signaling
Indications and Usage
Jakafi is indicated for treatment of patients with polycythemia vera who have had an inadequate response to or are intolerant of hydroxyurea.
Jakafi is indicated for treatment of patients with intermediate or high-risk myelofibrosis, including primary myelofibrosis, post–polycythemia vera myelofibrosis and post–essential thrombocythemia myelofibrosis.
Please see Important Safety Information on the back cover and accompanying Full Prescribing Information.
* Jakafi, a kinase inhibitor, inhibits JAK1 and JAK2 (Janus-associated kinases 1 and 2), which mediate the signaling of cytokines and growth factors important for hematopoiesis and immune function.1

Polycythemia vera (PV) is a chronic, progressive myeloproliferative neoplasm (MPN) characterized by increased myeloid, erythroid, and megakaryocytic cell proliferation without significant bone marrow fibrosis.2,3
Erythrocytosis (elevated total red blood cell mass) is the most prominent clinical expression of PV, and it distinguishes PV from all other MPNs, including essential thrombocythemia and primary myelofibrosis (MF).4
PV may progress to MF as bone marrow becomes more fibrotic.5
MyelofibrosisMF is a serious, progressive hematologic malignancy characterized by bone marrow fibrosis, abnormal cytokine expression, extramedullary hematopoiesis, constitutional symptoms, anemia, and shortened survival.5 All of the signs or symptoms are not necessarily present in all patients.6
Extramedullary hematopoiesis often results in splenomegaly.7 Newly detected or recent growth of a palpable spleen is a sign of disease progression.8
Median overall survival in intermediate-2–risk or high-risk MF is less than 5 years.9
Polycythemia vera
References: 1. Jakafi Prescribing Information. Wilmington, DE: Incyte Corporation. 2. Spivak JL. Polycythemia vera: myths, mechanisms, and management. Blood. 2002;100(13):4272-4290. 3. Michiels JJ. Bone marrow histopathology and biological markers as specific clues to the differential diagnosis of essential thrombocythemia, polycythemia vera and prefibrotic or fibrotic agnogenic myeloid metaplasia. Hematol J. 2004;5(2):93-102. 4. Spivak JL. Narrative review: thrombocytosis, polycythemia vera, and JAK2 mutations: the phenotypic mimicry of chronic myeloproliferation. Ann Intern Med. 2010;152(5):300-306. 5. Tefferi A. Primary myelofibrosis: 2014 update on diagnosis, risk-stratification, and management. Am J Hematol. 2014;89(9):916-925. 6. Scherber R, Dueck AC, Johansson P, et al. The Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF): International Prospective Validation and Reliability Trial in 402 patients. Blood. 2011;118(2):401-408. 7. Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113(13):2895-2901. 8. Tefferi A, Barosi G, Mesa RA, et al. International Working Group (IWG) consensus criteria for treatment response in myelofibrosis with myeloid metaplasia, for the IWG for Myelofibrosis Research and Treatment (IWG-MRT). Blood. 2006;108(5):1497-1503. 9. Tefferi A, Lasho TL, Jimma T, et al. One thousand patients with primary myelofibrosis: the Mayo Clinic experience. Mayo Clin Proc. 2012;87(1):25-33. 10. Tefferi A, Elliott M. Thrombosis in myeloproliferative disorders: prevalence, prognostic factors, and the role of leukocytes and JAK2 V617F. Semin Thromb Hemost. 2007;33(4):313-320. 11. Vannucchi AM, Guglielmelli P, Tefferi A. Advances in understanding and management of myeloproliferative neoplasms. CA Cancer J Clin. 2009;59(3):171-191. 12. Vainchenker W, Delhommeau F, Constantinescu SN, Bernard OA. New mutations and pathogenesis of myeloproliferative neoplasms. Blood. 2011;118(7):1723-1735. 13. Schafer AI. Molecular basis of the diagnosis and treatment of polycythemia vera and essential thrombocythemia. Blood. 2006;107(11):4214-4222. 14. Rampal R, Al-Shahrour F, Abdel-Wahab O, et al. Integrated genomic analysis illustrates the central role of JAK-STAT pathway activation in myeloproliferative neoplasm pathogenesis. Blood. 2014;123(22):e123-e133. 15. Keohane C, Radia DH, Harrison CN. Treatment and management of myelofibrosis in the era of JAK inhibitors. Biologics. 2013;7:189-198. 16. Kralovics R, Passamonti F, Buser AS, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med. 2005;352(17):1779-1790. 17. Chaligne R, Tonetti C, Besancenot R, et al. New mutations of MPL in primitive myelofibrosis: only the MPL W515 mutations promote a G1/S-phase transition. Leukemia. 2008;22(8):1557-1566. 18. Scott LM, Tong W, Levine RL, et al. JAK2 exon 12 mutations in polycythemia vera and idiopathic erythrocytosis. N Engl J Med. 2007;356(5):459-468. 19. Pikman Y, Lee BH, Mercher T, et al. MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia. PLoS Med. 2006;3(7):e270. 20. Kralovics R. Genetic complexity of myeloproliferative neoplasms. Leukemia. 2008;22(10):1841-1848. 21. Quintas-Cardama A, Vaddi K, Liu P, et al. Preclinical characterization of the selective JAK1/2 inhibitor INCB018424: therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2010;115(15):3109-3117. 22. Tefferi A, Vaidya R, Caramazza D, Finke C, Lasho T, Pardanani A. Circulating interleukin (IL)-8, IL-2R, IL-12, and IL-15 levels are independently prognostic in primary myelofibrosis: a comprehensive cytokine profiling study. J Clin Oncol. 2011;29(10):1356-1363. 23. Verstovsek S. Therapeutic potential of JAK2 inhibitors. Hematology Am Soc Hematol Educ Program. 2009:636-642. 24. Fourouclas N, Li J, Gilby DC, et al. Methylation of the suppressor of cytokine signaling 3 gene (SOCS3 ) in myeloproliferative disorders. Haematologica. 2008;93(11):1635-1644. 25. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. 26. Hasselbalch HC. Perspectives on chronic inflammation in essential thrombocythemia, polycythemia vera, and myelofibrosis: is chronic inflammation a trigger and driver of clonal evolution and development of accelerated atherosclerosis and second cancer? Blood. 2012;119(14):3219-3225. 27. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. 28. Furqan M, Mukhi N, Lee B, Liu D. Dysregulation of JAK-STAT pathway in hematologicial malignancies and JAK inhibitors for clinical application. Biomark Res. 2013;1(5):1-10. 29. Vainchenker W, Dusa A, Constantinescu SN. JAKs in pathology: role of Janus kinases in hematopoietic malignancies and immunodeficiencies. Semin Cell Dev Biol. 2008;19(4):385-393. 30. Delhommeau F, Jeziorowska D, Marzac C, Casadevall N. Molecular aspects of myeloproliferative neoplasms. Int J Hematol. 2010;91(2):165-173. 31. Kisseleva T, Bhattacharya S, Braunstein J, Schindler CW. Signaling through the JAK/STAT pathway, recent advances and future challenges. Gene. 2002;285(1-2):1-24. 32. Pellegrini S, Dusanter-Fourt I. The structure, regulation and function of the Janus kinases (JAKs) and the signal transducers and activators of transcription (STATs). Eur J Biochem. 1997;248(3):615-633. 33. Quintas-Cardama A, Kantarjian H, Cortes J, Verstovsek S. Janus kinase inhibitors for the treatment of myeloproliferative neoplasias and beyond. Nat Rev Drug Discov. 2011;10(2):127-140. 34. Mascarenhas J, Mughal TI, Verstovsek S. Biology and clinical management of myeloproliferative neoplasms and development of the JAK inhibitor ruxolitinib. Curr Med Chem. 2012;19(26):4399-4413. 35. Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis. N Engl J Med. 2012;366(9):799-807. 36. Harrison C, Kiladjian J-J, Al-Ali HK, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis. N Engl J Med. 2012;366(9):787-798. 37. Verstovsek S, Mesa RA, Gotlib J, et al. The clinical benefit of ruxolitinib across patient subgroups: analysis of a placebo-controlled, phase III study in patients with myelofibrosis. Br J Haematol. 2013;161(4):508-516. 38. Vannucchi AM, Kiladjian JJ, Griesshammer M, et al. Ruxolitinib versus standard therapy for the treatment of polycythemia vera. N Engl J Med. 2015;372(5):426-435. 39. Data on file. Incyte Corporation. Wilmington, DE.
2

Cytokines and growth factors
MutatedJAK2
JAK2
ActivatedSTAT
Nucleus
JAK1
JAK2
Long-termcomplications
Factors that impact JAK signaling16-24
JAK2 mutationsMPL mutationsExcess cytokinesIncreased
JAK1 signalingImpaired negative signaling mechanisms
(eg, those involving SOCS)
PV25,26 MF5
PV27
Progressive bonemarrow failure
Presence of risk factors leading to worsening prognosisand shortened survival
MF5
Proin�ammatory cytokineexpressionConstitutional symptomsExtramedullary hematopoiesisSplenomegalyAnemiaMarrow �brosis
Hyperproliferation ofhematopoietic cellsSplenomegalyAbnormally elevatedhematocritProin�ammatory cytokineexpression
3
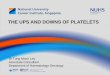
PV and MF: Mechanism of disease10-13
JAK, Janus-associated kinase; MF, myelofibrosis; MPL, myeloproliferative leukemia virus oncogene; PV, polycythemia vera; SOCS, suppressor of cytokine signaling; STAT, signal transducer and activator of transcription.
Overactive JAK pathway signaling is a key mechanism of disease14,15

JAK2
ActivatedSTAT
ActivatedSTATNucleus
DNA
JAK1
JAK signaling beginswhen a cytokine (ligand) binds to its transmembrane receptor
This binding activatesspeci�c JAK proteins
Activated JAK proteinsactivate STATs, whichdimerize and translocate to the nucleus
Inside the nucleus, STATs bind to DNA…
…modulating the expressionof genes related to cell survival, differentiation, and proliferation
Cytokines and growth factors
JAK1JAK2
JAK2
ActivatedSTAT
STATs
STATs
Nucleus
JAK1 JAK2
SOCS proteins
JAK1
DNA
Well-regulated JAKsignaling is essential for normal hematopoiesis, cell proliferation, andimmune function
SOCS proteins act asnegative regulators of JAK-STAT signaling
4
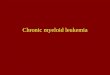
Signaling of the JAK pathway plays a key role in normal cell functioning24,28-301
The importance of the JAK pathway
JAK-STAT signaling activates transcription in the nucleus28,31-332
JAK, Janus-associated kinase; STAT, signal transducer and activator of transcription.
JAK, Janus-associated kinase; SOCS, suppressor of cytokine signaling; STAT, signal transducer and activator of transcription.

3
Excessivecytokinebinding
JAK2V617F mutation causingJAK2 constitutive activation
MPLconstitutiveactivation
MutatedJAK2
JAK2
JAK2
JAK2
JAK2
ActivatedSTATs
Nucleus
JAK1
SOCS
DNA
Impaired negative regulatory mechanisms
Excess cytokines
Receptor mutations, such as MPL mutations
JAK2 mutations
Increased JAK1 signaling
5
Well-regulated JAK signaling is essential for cell production, cell proliferation, and immune function. Intracellular regulators, such as suppressor of cytokine signaling (SOCS), help regulate JAK signaling.24,28
Cytokines bind to receptors and activate JAKs. JAKs activate signal transducers and activators of transcriptions (STATs), which dimerize and enter the nucleus. Inside the nucleus the STATs bind to DNA, stimulating the expression of genes related to cell survival, differentiation, and proliferation.28,31-33
The JAK-STAT pathway may become overactive by a number of mechanisms. Somatic mutations primarily involve JAK2, calreticulin (CALR), or myeloproliferative leukemia virus oncogene (MPL)16-24; approximately 90% of patients with MF carry one of these mutations.5 Approximately 95% of patients with PV have the JAK2V617F mutation.14 Other mechanisms noted may be increased JAK1 signaling, an excess of cytokines activating the receptors, or impaired intracellular regulators such as SOCS.16-24
3
1
2
The complex JAK pathway may become overactivated by many mechanisms16-24
JAK, Janus-associated kinase; MPL, myeloproliferative leukemia virus oncogene; SOCS, suppressor of cytokine signaling; STAT, signal transducer and activator of transcription.

Cytokines and growth factors
JAK2
ActivatedSTAT
Nucleus
JAK1JAK2 JAK1
Jaka�, a kinaseinhibitor, inhibitsJAK1 and JAK2,which mediate thesignaling of cytokinesand growth factorsimportant forhematopoiesis andimmune function1
6
Jakafi inhibits JAK pathway signaling.1 Because it binds in the JAK2 kinase domain, not at the site of the JAK2V617F mutation within the pseudokinase domain, it inhibits both mutant and wild-type JAK234
Clinical studies with Jakafi included patients who were JAK2V617F positive or negative35-37
Jakafi® (ruxolitinib) is an oral JAK1 and JAK2 inhibitor1
Risk for thrombocytopenia, anemia, and neutropenia1
Treatment with Jakafi can cause thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC), and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
Please see related and other Important Safety Information on back cover and accompanying Full Prescribing Information.
Jakafi: Mechanism of action1
JAK, Janus-associated kinase; STAT, signal transducer and activator of transcription.

When patients with polycythemia vera demonstrate an inadequate response to or are intolerant of hydroxyurea, consider JakafiApproval in PV was based on evidence from the RESPONSE (Randomized study of Efficacy and Safety in POlycythemia vera with JAK iNhibitor ruxolitinib verSus bEst available care) trial, a randomized, open-label, active-controlled phase 3 trial comparing Jakafi with best available therapy in 222 patients with PV who had an inadequate response to or were intolerant of hydroxyurea, required phlebotomy, and exhibited splenomegaly.1,38
Primary end point* A significantly larger proportion of patients in the group receiving Jakafi achieved the primary end point—a composite of hematocrit control and a ≥35% reduction in spleen volume at week 32—compared with best available therapy† (23% vs <1%, P < 0.0001)1
— 60% of patients receiving Jakafi and 19% of patients receiving best available therapy achievedhematocrit control
— 40% of patients receiving Jakafi and <1% of patients receiving best available therapy achieved a ≥35% reduction in spleen volume
Week-80 results1‡
19 of 25 (76%) patients in the Jakafi arm who achieved a primary response at week 32 maintained their response
51 of 66 (77%) patients in the Jakafi arm who achieved hematocrit control at week 32 maintained their response
43 of 44 (98%) of patients in the Jakafi arm who had a reduction in spleen volume at week 32 maintained their response
In patients with intermediate-2–risk or high-risk myelofibrosis In COMFORT-I,§ 42% of patients taking Jakafi achieved the primary end point, a ≥35% reduction
in spleen volume at week 24, compared with 0.7% of patients receiving placebo (P < 0.0001)1,35
In COMFORT-II,|| 29% of patients receiving Jakafi achieved a ≥35% reduction in spleen volume at week 48, compared with 0% of patients receiving best available therapy ¶ (P < 0.0001)1,36
Jakafi Prescribing Information includes Kaplan-Meier overall survival curves from COMFORT-I and COMFORT-II
* The composite primary end point was defined as hematocrit control without phlebotomy eligibility and a ≥35% spleen volume reduction as measured by CT or MRI. To achieve the hematocrit control end point, patients could not become eligible for phlebotomy between weeks 8 and 32. Phlebotomy eligibility was defined as hematocrit >45% that is ≥3 percentage points higher than baseline or hematocrit >48% (lower value).1
† Best available therapy included hydroxyurea (60%), interferon/pegylated interferon (12%), anagrelide (7%), pipobroman (2%), lenalidomide/thalidomide (5%), and observation (15%).1‡ A durability analysis was performed at week 80. Although all patients originally assigned to the best available therapy arm had crossed over by week 80, the week-80
analysis was only completed on the original Jakafi arm.1
§ COMFORT-I (COntrolled MyeloFibrosis study with ORal JAK inhibitor Treatment-I) was a randomized, double-blind, placebo-controlled phase 3 study with 309 total patients with intermediate-2–risk or high-risk myelofibrosis. The primary end point was the proportion of subjects achieving a ≥35% reduction in spleen volume from baseline to week 24 as measured by CT or MRI.1,35
|| COMFORT-II (COntrolled MyeloFibrosis study with ORal JAK inhibitor Treatment-II) was a randomized, open-label phase 3 study with 219 patients with intermediate-2–risk or high-risk myelofibrosis. The primary end point was the proportion of patients achieving a ≥35% reduction in spleen volume from baseline at week 48 as measured by CT or MRI.1,36
¶ Best available therapy in COMFORT-II included hydroxyurea (46.6%) and glucocorticoids (16.4%), as well as no medication, anagrelide, epoetin alfa, thalidomide, lenalidomide, mercaptopurine, thioguanine, danazol, peginterferon alfa-2a, interferon-α, melphalan, acetylsalicylic acid, cytarabine, and colchicine.39
7

Jakafi is a registered trademark of Incyte.© 2017, Incyte Corporation. All rights reserved. RUX-2211a 11/17
Important Safety Information Treatment with Jakafi® (ruxolitinib) can cause
thrombocytopenia, anemia and neutropenia, which are each dose-related effects. Perform a pre-treatment complete blood count (CBC) and monitor CBCs every 2 to 4 weeks until doses are stabilized, and then as clinically indicated
Manage thrombocytopenia by reducing the dose or temporarily interrupting Jakafi. Platelet transfusions may be necessary
Patients developing anemia may require blood transfusions and/or dose modifications of Jakafi
Severe neutropenia (ANC <0.5 × 109/L) was generally reversible by withholding Jakafi until recovery
Serious bacterial, mycobacterial, fungal and viral infections have occurred. Delay starting Jakafi until active serious infections have resolved. Observe patients receiving Jakafi for signs and symptoms of infection and manage promptly
Tuberculosis (TB) infection has been reported. Observe patients taking Jakafi for signs and symptoms of active TB and manage promptly. Prior to initiating Jakafi, evaluate patients for TB risk factors and test those at higher risk for latent infection. Consult a physician with expertise in the treatment of TB before starting Jakafi in patients with evidence of active or latent TB. Continuation of Jakafi during treatment of active TB should be based on the overall risk-benefit determination
Progressive multifocal leukoencephalopathy (PML) has occurred with Jakafi treatment. If PML is suspected, stop Jakafi and evaluate
Advise patients about early signs and symptoms of herpes zoster and to seek early treatment
Increases in hepatitis B viral load with or without associated elevations in alanine aminotransferase and aspartate aminotransferase have been reported in patients with chronic hepatitis B virus (HBV) infections. Monitor and treat patients with chronic HBV infection according to clinical guidelines
When discontinuing Jakafi, myeloproliferative neoplasm-related symptoms may return within one week. After discontinuation, some patients with myelofibrosis have experienced fever, respiratory distress, hypotension, DIC, or multi-organ failure. If any of these occur after discontinuation or while tapering Jakafi, evaluate and treat any intercurrent illness and consider restarting or increasing the dose of Jakafi. Instruct patients not to interrupt or discontinue Jakafi without consulting their physician. When discontinuing or interrupting Jakafi for reasons other than thrombocytopenia or neutropenia, consider gradual tapering rather than abrupt discontinuation
Non-melanoma skin cancers including basal cell, squamous cell, and Merkel cell carcinoma have occurred. Perform periodic skin examinations
Treatment with Jakafi has been associated with increases in total cholesterol, low-density lipoprotein cholesterol, and triglycerides. Assess lipid parameters 8-12 weeks after initiating Jakafi. Monitor and treat according to clinical guidelines for the management of hyperlipidemia
The three most frequent non-hematologic adverse reactions (incidence >10%) were bruising, dizziness and headache
A dose modification is recommended when administering Jakafi with strong CYP3A4 inhibitors or fluconazole or in patients with renal or hepatic impairment. Patients should be closely monitored and the dose titrated based on safety and efficacy
Use of Jakafi during pregnancy is not recommended and should only be used if the potential benefit justifies the potential risk to the fetus. Women taking Jakafi should not breastfeed during treatment and for two weeks after the final dose
Please see accompanying Full Prescribing Information for Jakafi.
Jakafi.com/HCP


























![Ruxolitinib - Elsevier...ruxolitinib arm occurred in 85.7% of patients in the best standard therapy arm at or after week 32.[58808] In an extended analysis at week 80, 76% of patients](https://img.pdfslide.us/doc/110x75/6112927320cf746dca4de4fd/ruxolitinib-elsevier-ruxolitinib-arm-occurred-in-857-of-patients-in-the.jpg)