Embed Size (px)
Citation preview
UNDERSTANDING EACH COMPONENT OF THE CBC
COURSE CODE: H020
CONTACT HOURS: 4
COURSE LEVEL: Basic
ASCLS P.A.C.E. #: 511‐620‐17 PACE # Expiration: June 30, 2019
Continuing Education Unlimited 6231 PGA Blvd / Suite 104, #306 / Palm Beach Gardens, FL 33418
888-423-8462 / General Fax: 561-775-4933 / Answer Sheet ONLY Fax: 561-775-4948 / www.4CEUINC.comPROVIDER #s: Florida: 50-2256 | California: 0001 | ASCLS P.A.C.E.: 511
AUTHOR: Deborah L. Buckley, MBA, MT(ASCP)
** T
his
cour
se m
eets
the
1 hr
. Hem
atol
ogy
requ
irem
ent f
or F
lorid
a lic
ense
rene
wal
. **
ii www.4CEUINC.com
1.)
RIGHTSHOLDER:
Author: Deborah L. Buckley, MT(ASCP)
© 2015 Continuing Education Unlimited
Publication Date: May 2015, 2017
PERMISSIONS
Permissions are currently not available for this copyrightedwork.
ARTICLE REPRODUCTION
This course may not be reproduced for any purpose in any medium.
If sharing this written document with colleagues, please share the original document – do not make copies. One copy may be printed from any online file that you purchased.
Unlimited quizzes may be photocopied for sharing purposes only.
CEUINC LICENSE INFO:LABORATORY
CA Department of Health: 0001
Florida Board of Clinical Lab: 50‐2256
ASCLS P.A.C.E.® 511
Our courses are accepted by: AMTIE, AMT, \ASCP, CA, FL, LA, ND, NV, MT, RI, TN, WV
** If you do not see your organization, state, or licensing agency listed above it does not mean that the credits will be unacceptable. Most licensing
bodies accept credits, so please check directly with them for acceptance of our courses.**
PHLEBOTOMY
Most licensing bodies accept credits. Please check with them directly for acceptance of our course credits.
OTHER MEDICAL DISCIPLINES
Many medical licensing bodies will accept credits issued by valid licensed providers of other disciplines. Please check directly with the state, agency, or organization that issued your license for acceptance of our credits.
1. Recall the composition of Human Blood, discussing the liquid and cellular portions.2. List each component of a Complete Blood Count (CBC) and how the test is performed.3. State the normal values for a total red blood cell count (RBC), listing the causes for increased or decreased values.4. List the RBC indicies included in a CBC and recall the causes of increased and decreased values of each.5. State the normal values for a total white blood cell count (WBC), listing the causes for increased or decreased values.6. List the five different types of WBCs and discuss the reasons for increased or decreased values of each.7. State the normal values for Platelets, listing the causes for increased or decreased values.8. Discuss automated and manual differentials
** CEUINC is approved as a provider of continuing education programs in the clinical laboratory sciences by
the ASCLS P.A.C.E.® Program. **
COURSE OBJECTIVES
At the end of this course the learner will be able to:
iii www.4CEUINC.com
Thanks for choosing CEUINC for your continuing education needs! We strive to offer you current course material at the most cost effective price. If you have comments or suggestions, be sure to add them to your evaluation – we appreciate them. If you like our courses pass them on to a coworker or friend.
READ BEFORE COMPLETING MATERIAL
GENERAL:
1.) Check your reading material to make sure that it contains the correct course(s) you ordered.
2.) Carefully read the material before completing your quiz packet. All answers are within the reading material. With few exceptions, quiz questions typically follow in order of the reading.
3.) Courses must be completed within 1 year of purchase date, unless otherwise specified.
4.) All of your records are available to you on our website for 4 years. If you don’t have a login to access your records, please contact our office and we will give you that information. Please do not create a 2nd profile! 5.) When sharing your materials with a coworker, be sure to pass on both the reading material and the quiz.
HOME STUDY COURSES:
1.) Each course should have a corresponding answer sheet(s), course evaluation, and an envelope.
2.) If you have ordered multiple courses, please make sure that you are using the correct answer sheet for that course or course section. The course code will be located on the label of your answer sheet.
3.) After you have completed reading the material, complete the quiz, then fill in the corresponding answer sheet.
4.) Upon completion, send in your answer sheet(s) to our office. Please make copies for your records before sending !
5.) Once we receive your answer sheet in our office we will grade it & mail you back a certificate of completion. Your certificate will arrive in the mail within 4 weeks from the date you mail your answer sheets us.
ONLINE COURSES:
1.) Course materials are offered in Adobe pdf documents, which allow multiple options for accessing & saving the material. You can read the document online, print it out for reference, store it on your hard drive, or copy it to a disk. Please remember to save or print the document before completing your quiz. Once you complete your quiz you will be permanently locked out of that record. Per copyright law, you can print one copy of each online course.
2.) Quizzes can be printed out if you’d like to work offline. Once you are done, simply transfer your results to the active, online quiz and click “Score”. You will receive immediate feedback of your results.
“SITE-BASED” GROUPS:
1.) Coordinators should mail all “Pay As You Go” answer sheets to our facility as a group once per month.
2.) We mail certificates once per month according to the schedule furnished to the educational coordinator.
3.) Be sure to fill in your course code on the Pay As You Go (PAYG) answer sheets.
4.) If you have the online login to your profile, you may purchase online quizzes rather than mail in an answer sheet. This will allow you to immediately print your certificate of completion and will save time & money.
Continuing Education Unlimited 6231 PGA Blvd , Ste 104 / #306 Palm Beach Gardens, FL 33418 General Fax: 561-775-4933 / Answer Sheet Only Fax: 561-775-4933 Phone: 561-775-4944 / Web: www.4CEUINC.com
Last Revised 11/09/12
ALERT:
Please make a copy of your answer sheet before mailing or faxing it! This safeguards you in the event that your answer sheet does not reach its destination.
iv www.4CEUINC.com
FREQUENTLY ASKED QUESTIONS
Q. Your phones are often busy, how can I reach you? A. Because we have a small staff, the most efficient way would be to Schedule a Call Back by clicking the button on the Home Page of our website. You will then be able to select a convenient time for our staff to call you back. Q. What course completion date goes on my certificate? A. The date that we receive your answer sheet in our office.
Q. I need my certificate dated on a certain day how can I be sure that this will happen? A. 1.) Allow adequate mailing time, taking into consideration weekends and holidays when we are not in the office. 2.) Overnight the answer sheet to us - using a “TRACKABLE” service. 3.) Complete the course/quiz online.
Q. What score is considered passing? A. A score of 70% or higher is considered a passing grade. In the event that you do not pass on your first attempt, you are allowed a second attempt to score a passing grade.
Q. Does your company allow me to fax my answer sheet to your office? A. YES, you may now fax your answer sheet to 561-775-4948. Include a cover sheet with your full name, license number and telephone number. Please only fax to the number listed above and NOT to our general fax #. Please keep a record of the time & date you send the fax in the event that there is a problem!
Q. May a course be shared with multiple users? A. Yes. If you are sharing materials, one person will buy the “complete course” package and each of the others will purchase an “answer sheet only” or “online quiz only” packet. Please be sure you have BOTH the reading material and the quiz packet if you’re sharing. Prices are subject to change, please check before ordering.
Q. How long will it take for my certificate to arrive if I’m sending my answers by mail? A. We can’t give an exact date because of variations in mail delivery time, however, we ask that you allow 3-4 weeks from the time you mail it to us until your certificate to arrives in your mailbox. You may also consider email delivery or online quiz completion for faster turnaround.
Q. May I print out an online course? A. Yes, you may print 1 copy of an online course. Copyright laws do not allow more than one copy to be printed!
Q. Where can I find additional information out about a course? A. Basic course information is located on the course cover. Additional information is located on the 2nd page of each course.
Q. What are your most popular courses? A. Currently our most popular courses remain the Unlimited Online Course Package and our Combination Courses.
Q. Does CEUINC offer group discounts or group packages? A. Yes. We require at least 5 participants and a person to act as the educational coordinator for the group. Discount amounts depend on the number of participants and the course or package chosen. Please check our website for details.
Continuing Education Unlimited 6231 PGA Blvd , Ste 104 / #306 Palm Beach Gardens, FL 33418 General Fax: 561-775-4933 / Answer Sheet Only Fax: 561-775-4933 Phone: 561-775-4944 / Web: www.4CEUINC.com
Last Revised 11/09/12
ALERT:
Please make a copy of your answer sheet before mailing or faxing it! This safeguards you in the event that your answer sheet does not reach its destination.
v www.4CEUINC.com
1.) Plasma makes up _____ of whole blood. A. 35% B. 55% C. 75%
2.) Brown or amber colored plasma would most likely be from ___________.
A. a traumatic or difficult blood draw B. elevated chylomicrons C. liver disease
3.) Platelets are part of the Lymphoid cell line. A. True B. False
4.) Lavender top tubes, used for performing a CBC, contain ___________. A. EDTA B. Sodium citrate C. Sodium heparin
5.) Healthy RBCs have an average lifespan of _____ days. A. 50 B. 80 C. 120
6.) An elevated RBC count is known as known as _____________.
A. anemia B. polycythemia C. hematosis
UNDERSTANDING EACH COMPONENT OF THE CBC Categories: Hematology | Contact Hours: 4 | Course Code: H020
vi www.4CEUINC.com
7.) Hemoglobin’s binding affinity for carbon monoxide (CO) is ___ times greater than for oxygen (O2).
A. 25 B. 100 C. 250
8.) A decreased blood volume in a patient with a normal hematocrit would be seen with:
A. Fluid overload B. polycythemia C. Acute blood loss
9.) If a patient has an elevated MCV over 100fl, you would expect to see _______ on
a peripheral smear. A. microcytes B. normal, healthy RBCs C. macrocytes
10.) Acute blood loss would cause a _______________ anemia.
A. normocytic, normochromic B. microcytic, hypochromic C. macrocytic, normochromic
11.) Anemia caused by Folate or B12 deficiency would give the following RDW/MCV pattern:
A. elevated RDW, decreased MCV B. decreased RDW, decreased MCV C. elevated RDW, elevated MCV
12.) Nucleated RBCs can interfere with an automated WBC count.
A. True B. False
13.) A leukemoid reaction is considered a benign syndrome.
A. True B. False
14.) _____ of CML and _____ of CLL patients are initially asymptomatic
A. 90%, 20% B. 20%, 50% C. 40%, 70%
UNDERSTANDING EACH COMPONENT OF THE CBC - QUIZ PAGE 2 -
vii www.4CEUINC.com
15.) In a healthy patient, neutrophils typically make up ______ of the WBCs in the body. A. 15%-20% B. 25%-50% C. 50%-70%
16.) Increased eosinophils are typically found in:
A. Cushing’s syndrome B. Parasitic infections C. Nutritional deficiencies
17.) Basophils have _____ receptors on their surface membranes.
A. IgA B. IgG C. IgE
18.) On a peripheral smear reactive lymphocytes are often mistaken for a __________.
A. monocyte B. neutrophilic band cell C. megakaryocyte
19.) CD8+ T cells are also called ___________.
A. T-helper cells B. natural killer cells C. cytotoxic T cells
20.) Monocytes are the largest of the normal peripheral circulating blood cells.
A. True B. False
21.) When a monocyte moves from the peripheral circulation into the tissues it becomes
a ____________. A. plasma cell B. natural killer cell C. macrophage
22.) Platelet counts performed on blood that’s been drawn in a sodium citrate tube to
prevent platelet clumping, must be multiplied by 2.0 before reporting the corrected platelet count.
A. True B. False
****END OF QUIZ****
UNDERSTANDING EACH COMPONENT OF THE CBC - QUIZ PAGE 3 -
viii www.4CEUINC.com
***THIS PAGE INTENTIONALLY LEFT BLANK***
vii www.4CEUINC.com
Table of Contents
HUMAN BLOOD ...................................................................................................... 1
Composition of Blood ............................................................................................ 1
Plasma ............................................................................................................. 1
Cells ................................................................................................................ 5
COMPLETE BLOOD COUNT ...................................................................................... 7
CBC Specimen ..................................................................................................... 7
Components of the CBC ........................................................................................ 8
Performing the Test .............................................................................................. 8
Total Cell Counts ............................................................................................... 8
Indices ............................................................................................................. 9
Differential ....................................................................................................... 9
RED BLOOD CELL COUNT AND RED BLOOD CELL INDICES ..................................... 9
Total RBC Count .................................................................................................. 10
Low RBC Count ................................................................................................ 11
Elevated RBC Count .......................................................................................... 11
Hemoglobin ........................................................................................................ 14
Structure of Hemoglobin .................................................................................... 14
Decreased Hemoglobin Values ............................................................................ 15
Increased Hemoglobin Values ............................................................................. 15
Signs and Symptoms of Hemoglobin Changes ....................................................... 15
Hematocrit ......................................................................................................... 16
Common interfering Factors ............................................................................... 18
Decreased Hematocrit Values ............................................................................. 19
Increased Hematocrit Values .............................................................................. 19
Signs and Symptoms of Hematocrit Changes ........................................................ 19
viii www.4CEUINC.com
MCV .................................................................................................................. 20
Decreased MCV ................................................................................................ 21
Elevated MCV ................................................................................................... 21
MCH .................................................................................................................. 21
Decreased MCH ................................................................................................ 22
Elevated MCH .................................................................................................. 22
MCHC ................................................................................................................ 22
Normocytic, Normochromic Anemia ..................................................................... 24
Microcytic, Hypochromic Anemia ......................................................................... 24
Macrocytic, Normochromic Anemia ...................................................................... 24
Microcytic, Normochromic Anemia ....................................................................... 24
RDW .................................................................................................................. 25
Disease states that can affect the RDW are: ......................................................... 26
Anemia With Normal RDW ................................................................................. 26
AnemiaS With An Elevated RDW ......................................................................... 26
WHITE BLOOD CELLS ........................................................................................... 27
Total WBC .......................................................................................................... 28
Low WBC Count ................................................................................................ 29
Elevated WBC Count ......................................................................................... 30
Neutrophils ......................................................................................................... 33
Decreased Neutrophil Count ............................................................................... 34
Increased Neutrophil Count ................................................................................ 35
Eosinophils ......................................................................................................... 35
Decreased Eosinophil Counts .............................................................................. 36
Increased Eosinophil Counts ............................................................................... 37
Treatment of Eosinophilia .................................................................................. 37
Basophils ........................................................................................................... 37
viiii www.4CEUINC.com
Decreased Basophil Count .................................................................................. 38
Increased Basophil Count .................................................................................. 39
Lymphocytes ...................................................................................................... 39
Decreased Lymphocyte Count ............................................................................ 42
Increased Lymphocyte Count ............................................................................. 42
Closer Look at the Different Lymphocyte Populations ............................................. 43
Monocytes .......................................................................................................... 45
Monocyte Subpopulations .................................................................................. 46
Decreased Monocyte Count ................................................................................ 46
Increased Monocyte Count ................................................................................. 46
Macrophages ................................................................................................... 47
PLATELETS .......................................................................................................... 48
Platelet Structure ............................................................................................. 49
Total Platelet Count ............................................................................................. 49
Scanning a Peripheral Smear .............................................................................. 50
Low Platelet Count ............................................................................................ 51
Elevated Platelet Count ..................................................................................... 53
MPV .................................................................................................................. 54
Causes of Increased MPV ................................................................................... 54
Causes of Decreased MPV .................................................................................. 54
PDW .................................................................................................................. 54
Causes of Increased PDW .................................................................................. 55
Causes of Decreased PDW ................................................................................. 55
DIFFERENTIAL ..................................................................................................... 56
Manual Differential .............................................................................................. 56
Automated Differential ......................................................................................... 57
viiv www.4CEUINC.com
***THIS PAGE INTENTIONALLY LEFT BLANK***
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
1 www.4CEUINC.com
HUMAN BLOOD
Human blood is the fluid that transports oxygen and nutrients to the cells throughout the body, while transporting metabolic waste away from those same cells. In addition to cells and plasma, blood naturally contains many other constituents including antibodies, electrolytes, hormones, proteins, nutrients, oxygen, etc. It is circulated throughout the body by the pumping action of the heart with oxygenated blood running through arteries to deliver oxygen and other nutrients, while venous blood carries carbon dioxide and other metabolic waste products, to the liver, lungs, and kidneys for elimination.
The amount of blood volume in the human body varies, however on average adults typically have approximately 5 liters (~1.3 gallons) of blood, while a child with a body weight of 80 pounds will have approximately half the amount of blood as an average adult. Overall several factors determine the total volume an individual has, including age, sex, size, overall health status, and even altitude. As a general rule, men tend to have more blood volume than women of comparable size and weight. Blood makes up approximately 7-8% of a patient’s body weight and has a small pH range of 7.35-7.45.
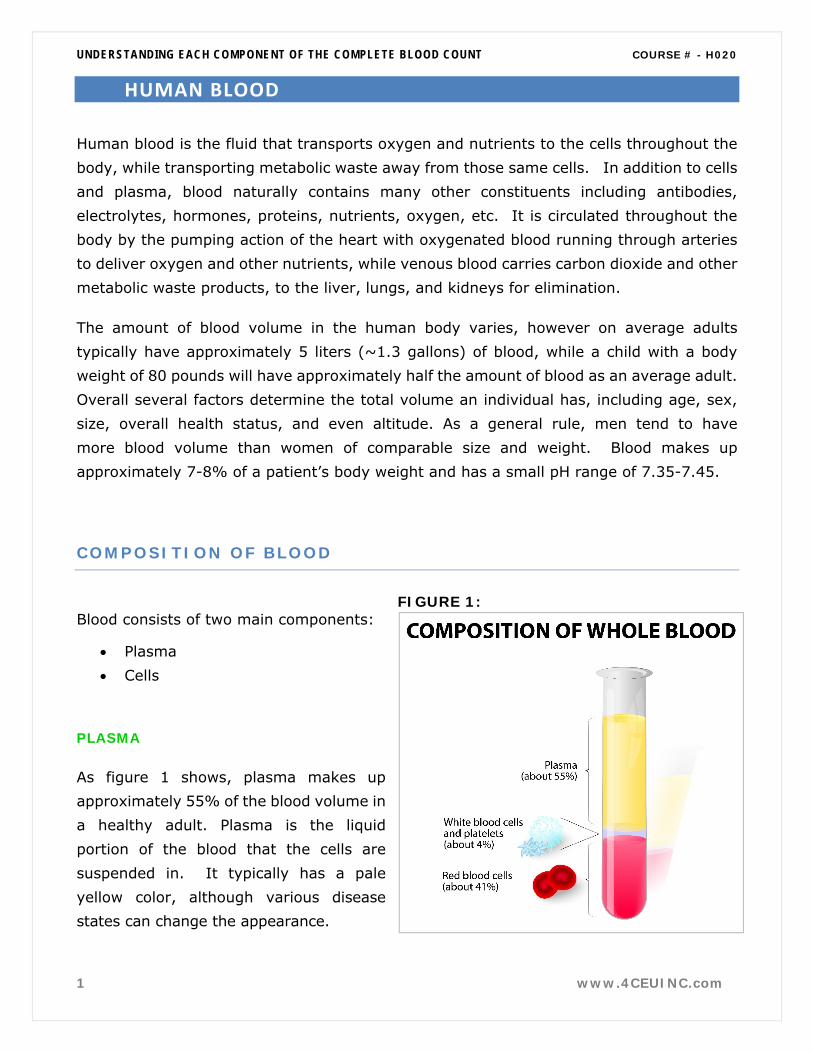
COMPOSITION OF BLOOD
FIGURE 1:
Blood consists of two main components:
Plasma Cells
PLASMA
As figure 1 shows, plasma makes up approximately 55% of the blood volume in a healthy adult. Plasma is the liquid portion of the blood that the cells are suspended in. It typically has a pale yellow color, although various disease states can change the appearance.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
2 www.4CEUINC.com
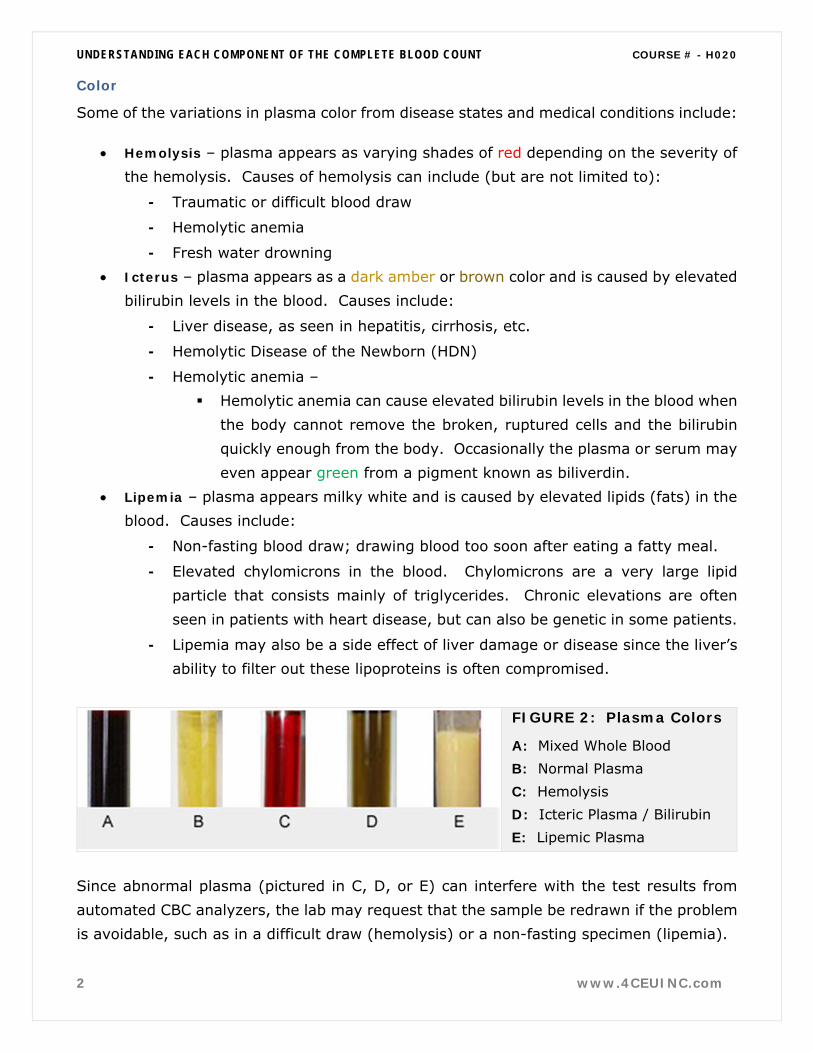
Color
Some of the variations in plasma color from disease states and medical conditions include:
Hemolysis – plasma appears as varying shades of red depending on the severity of the hemolysis. Causes of hemolysis can include (but are not limited to):
- Traumatic or difficult blood draw
- Hemolytic anemia
- Fresh water drowning Icterus – plasma appears as a dark amber or brown color and is caused by elevated
bilirubin levels in the blood. Causes include:
- Liver disease, as seen in hepatitis, cirrhosis, etc.
- Hemolytic Disease of the Newborn (HDN)
- Hemolytic anemia – Hemolytic anemia can cause elevated bilirubin levels in the blood when
the body cannot remove the broken, ruptured cells and the bilirubin quickly enough from the body. Occasionally the plasma or serum may even appear green from a pigment known as biliverdin.
Lipemia – plasma appears milky white and is caused by elevated lipids (fats) in the blood. Causes include:
- Non-fasting blood draw; drawing blood too soon after eating a fatty meal.
- Elevated chylomicrons in the blood. Chylomicrons are a very large lipid particle that consists mainly of triglycerides. Chronic elevations are often seen in patients with heart disease, but can also be genetic in some patients.
- Lipemia may also be a side effect of liver damage or disease since the liver’s ability to filter out these lipoproteins is often compromised.
FIGURE 2: Plasma Colors
A: Mixed Whole Blood B: Normal Plasma C: Hemolysis D: Icteric Plasma / Bilirubin E: Lipemic Plasma
Since abnormal plasma (pictured in C, D, or E) can interfere with the test results from automated CBC analyzers, the lab may request that the sample be redrawn if the problem is avoidable, such as in a difficult draw (hemolysis) or a non-fasting specimen (lipemia).
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
3 www.4CEUINC.com
Plasma Composition
As noted previously, plasma is the liquid portion of the blood. It’s composed of ~92-95% water by volume and 5-8% dissolved solutes. Examples of the dissolved solutes in the plasma include proteins, glucose, electrolytes (sodium, potassium, chloride), hormones, clotting factors, vitamins, minerals, antibodies, etc. Plasma also transports waste products, such as, lactic acid, urea, and carbon dioxide (CO2) away from the cells to be excreted from the body.
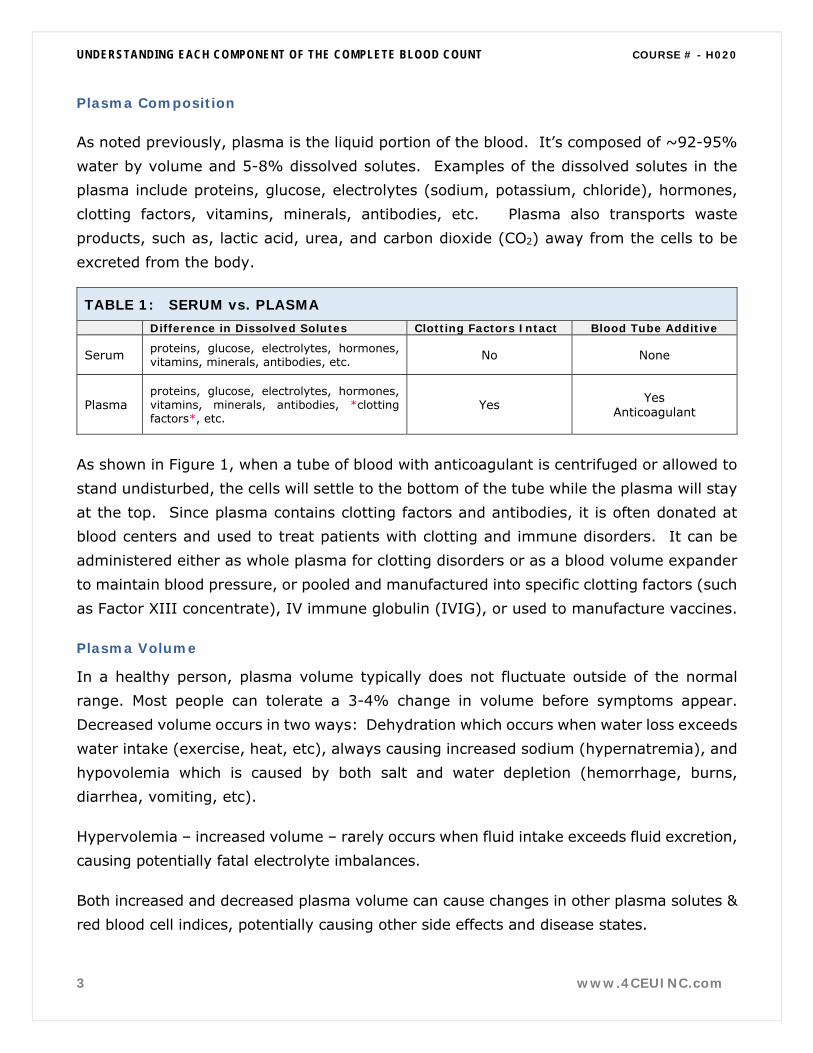
TABLE 1: SERUM vs. PLASMA Difference in Dissolved Solutes Clotting Factors Intact Blood Tube Additive
Serum proteins, glucose, electrolytes, hormones, vitamins, minerals, antibodies, etc. No None
Plasma proteins, glucose, electrolytes, hormones, vitamins, minerals, antibodies, *clotting factors*, etc.
Yes Yes Anticoagulant
As shown in Figure 1, when a tube of blood with anticoagulant is centrifuged or allowed to stand undisturbed, the cells will settle to the bottom of the tube while the plasma will stay at the top. Since plasma contains clotting factors and antibodies, it is often donated at blood centers and used to treat patients with clotting and immune disorders. It can be administered either as whole plasma for clotting disorders or as a blood volume expander to maintain blood pressure, or pooled and manufactured into specific clotting factors (such as Factor XIII concentrate), IV immune globulin (IVIG), or used to manufacture vaccines.
Plasma Volume
In a healthy person, plasma volume typically does not fluctuate outside of the normal range. Most people can tolerate a 3-4% change in volume before symptoms appear. Decreased volume occurs in two ways: Dehydration which occurs when water loss exceeds water intake (exercise, heat, etc), always causing increased sodium (hypernatremia), and hypovolemia which is caused by both salt and water depletion (hemorrhage, burns, diarrhea, vomiting, etc).
Hypervolemia – increased volume – rarely occurs when fluid intake exceeds fluid excretion, causing potentially fatal electrolyte imbalances.
Both increased and decreased plasma volume can cause changes in other plasma solutes & red blood cell indices, potentially causing other side effects and disease states.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
5 www.4CEUINC.com
CELLS
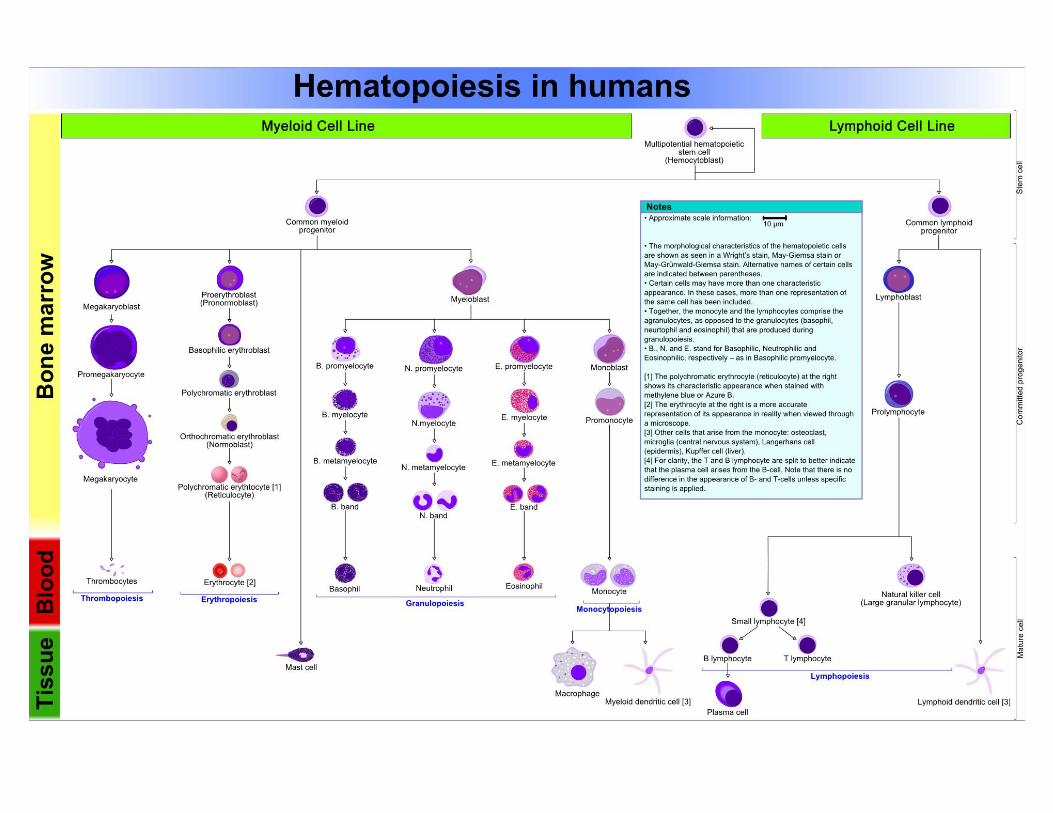
Red cells, White cells, and platelets – the components of the CBC - are all produced in the bone marrow. Figure 3 (previous page) shows the steps those blood cells go through while maturing.
This blood cell maturation process, known as hematopoiesis, starts with a pluripotent stem cell. Pluripotent stem cells have the potential to develop into multiple different cell lines, as shown in Figure 3. By definition, Pluripotent breaks down to mean:
“Pluri” = many or multiple “Potent” = potential
The pluripotent stem cells in the bone marrow are often referred to as hematopoietic stem cells (HSC). These cells give rise to extremely large numbers of “daughter cells” (cells formed from the original stem cell) and typically represent 1 cell for every 10,000 cells found in the bone marrow. In adults, HSCs are found in bone marrow in the pelvis, femur, and sternum, and in newborns are found in the umbilical cord blood. HSCs can also be found in very small numbers in the peripheral, circulating blood.
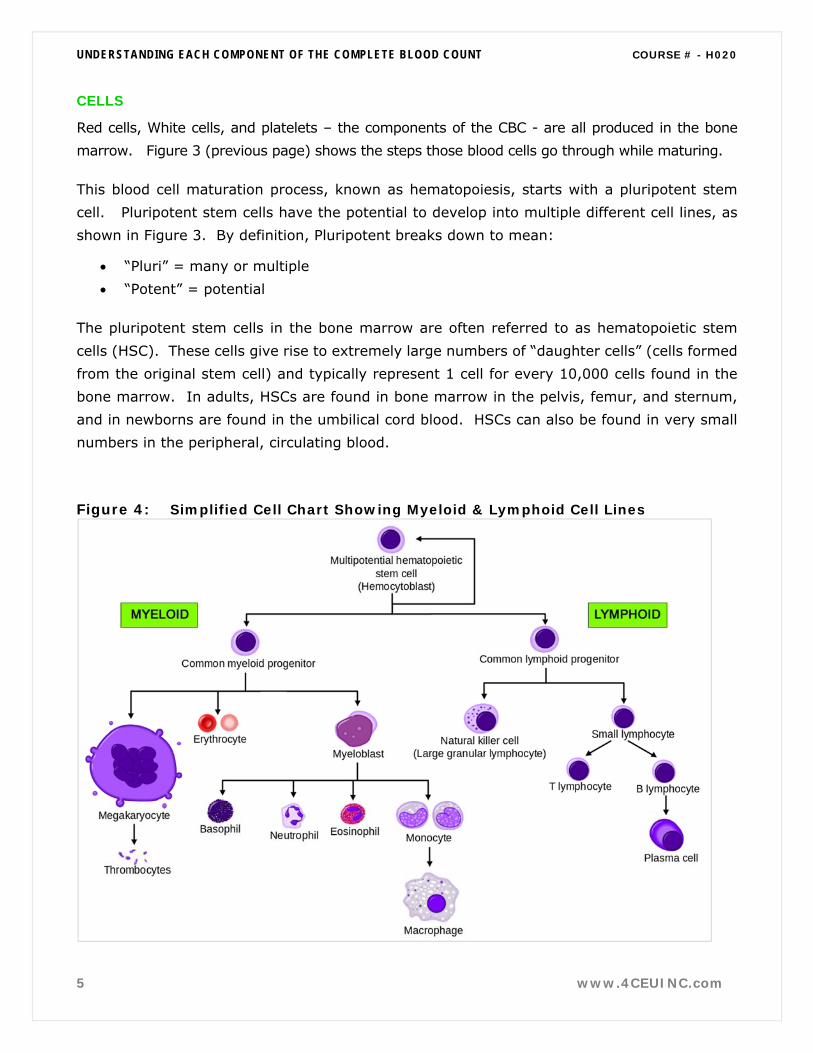
Figure 4: Simplified Cell Chart Showing Myeloid & Lymphoid Cell Lines
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
6 www.4CEUINC.com
As the cells mature, they start to form different “categories” or cell lines (aka - lineage). In some cases, these cell lines branch off multiple times before you get to the mature blood cell that you find in the peripheral circulation, which are the cells that are observed and counted in the Complete Blood Count (CBC). Initially as cells are formed from the pluripotent stem cell, they are categorized into either “myeloid” or “lymphoid” cells lines. Figure 4 shows a simplified graphic of the cells that are included in those two categories. It should be noted that each one of the cells pictured in that graphic has already gone through several maturation steps (as shown in Figure 3) before becoming the mature cells that are released into the blood stream.
As Figure 3 notes, blood cells can normally be found in three areas of the body:
Bone marrow - where cells are formed and mature
Peripheral (circulating) blood *
Tissues - found during injury & other disease states
The Complete Blood Count (CBC) focuses on the cells in the peripheral, circulating blood. As a general rule, blood cells in the peripheral blood are typically mature cells, although on very rare occasions, you may find an immature cell on the differential of a healthy patient. Abnormal, immature cells are seen in the peripheral blood during various disease states. The immature cells observed corresponds to the disease that the patient has, for example:
Immature Red Blood Cells (RBCs)
- Can be seen in anemia or blood loss
- * Immature RBCs are normal finding in a newborn’s blood
Immature White Blood Cells
- Can be seen in leukemia or severe infection
- Immature cells in leukemia are classified by the cell line “Myelocytic” “Lymphocytic”
Immature Platelets
- Can be seen in peripheral blood if a patient is recovering from a clotting disorder & appear larger than normal sized platelets
- Rarely a large megakaryocyte (immature platelet) may be seen
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
7 www.4CEUINC.com
COMPLETE BLOOD COUNT
The complete blood count, referred to as a CBC, is one of the most commonly ordered tests by a physician. It’s used as a broad screening tool providing information on the patient’s general health status. Although it’s routinely ordered during a patient’s annual wellness exam, it’s also used to diagnose and monitor various disease states, such as anemia, leukemia, infections, bleeding disorders, etc.
CBC SPECIMEN
Blood is collected in a lavender top EDTA tube, which is gently inverted 5-10 times immediately after collection to prevent clotting. The specimen should remain at room temperature during transport and the testing process. The CBC is performed on whole blood so just prior to testing, the specimen must be gently mixed to evenly distribute the cells and mix the liquid portion of the blood with the cells. It should be noted that on rare occasions it may be necessary to collect a Sodium Citrate or Sodium
Heparin tube when pseudo (false) platelet clumping occurs in a patient’s specimen. This occurs in <1% of the population who’s platelets react to the EDTA inside the blood tube causing the platelets to stick together and giving a falsely negative platelet count. *Check with your procedure manual or the CBC analyzer’s manufacturer to determine which alternate specimen is acceptable to run on the analyzer at your lab.
Since specimen integrity is important to producing a reliable patient result, CBC specimens may be rejected and a redraw requested if the specimen is compromised in any way. Causes for rejection may include:
Clotted specimen Hemolysis Overfilled or under-filled specimen tube Incorrect specimen tube Tube contaminated or diluted with IV fluid. This can occur if blood is draw above
an active IV site or when the IV has not been turned off long enough for the fluid to clear from the vein prior to venipuncture.
Preferred
* EDTA *
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
8 www.4CEUINC.com
Incorrect specimen temperature (ie - frozen)
Other rejection criteria may apply, however, these are the most common causes.
COMPONENTS OF THE CBC
The complete blood count is a group of different tests that when performed together give the physician an overall picture of the patient’s basic health. The CBC measures three main cell types and different parameters for each:
Red blood cells
- Total RBC count
- Hemoglobin, Hematocrit, and RBC Indices
White blood cells (WBCs)
- Total WBC count
- WBC differential – automated or manually visualizing a peripheral smear. Identifies and quantitates each of the 5 WBC cell types
Platelets
- Total platelet count
- Platelet indices
PERFORMING THE TEST
The individual components of the CBC are each measured or calculated separately. As noted previously, the total cell counts, cellular indices, and WBC differential all make up the CBC.
TOTAL CELL COUNTS
Total blood cell counts can be performed manually (counting cells under the microscope) or using an automated analyzer which does the counting for you. It’s very rare that the blood count portion of the test is performed manually since automated analyzers can produce faster, more accurate results. When automated results are questionable, or when
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
9 www.4CEUINC.com
there’s some type of interfering factor, cell counts can still be performed manually using a thick glass slide called a hemocytometer, which is placed under a microscope so the cells in the blood can be counted.
Automated analyzers work by passing a diluted amount of blood through an electrical current inside the analyzer. As the cells are passed through the current, the voltage changes and is proportional to the size of the blood cell passing by; this is known as impedance. Since each cell type has its own normal size range, the total electrical impulses for a certain cell size will correspond to the total cell count for that cell population. Abnormal size cells, immature cells, platelet clumping, and various other issues may cause interference in the automated reading requiring a manual cell count to be performed.
INDICES
Red blood cell and platelet indices are calculated values, each with its own formula. Those formulas are listed later in the course under each parameter.
DIFFERENTIAL
In addition to counting the total cells and measuring the indices, WBCs are further separated by cell type in a test called a differential. This can be done by an automated CBC analyzer as noted above or manually using a microscope. A microscopic differential is performed on a blood slide called a peripheral smear. When performing a peripheral smear, 100 WBCs are counted and numbers for each cell type are recorded. The results from an automated differential give a value known as an “absolute” number.
RED BLOOD CELL COUNT AND RED BLOOD CELL INDICES RBC is an abbreviation for “Red Blood Cell”, also known as an erythrocyte. Of the three main cell categories, RBCs are the most numerous blood cell and function in the body by transporting oxygen to the cells and tissues, while transporting carbon dioxide to the lungs for removal.
The classic red color of RBCs is from the iron content of the hemoglobin contained within each cell. Each hemoglobin molecule carries four heme groups, which comprises about 1/3 of the total cell volume and is responsible for transporting 98% of the oxygen within the body. The blood cells of an average male store approximately 2.5 grams of iron which represents about 65% of the total iron contained in the body.

UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
10 www.4CEUINC.com
Unlike other cells, RBCs do not have a nucleus and appear as round, biconcave (indented) discs as shown below. The concave central area appears pale, while the rest of the cell appears as a reddish-brown color. Their biconcave shape allows them the flexibility to bend and fold, flowing smoothly through even the narrowest blood vessels.
Average Size: 7 µm (micrometers) in diameter and approximately 2.5 µm in height
Average Lifespan: It takes approximately 7 days for a red blood cell to mature from a stem cell to an erythrocyte in the peripheral blood. Healthy RBCs have an average lifespan of 120 days. Once they die, they’re removed from the circulation by the spleen, while their iron content is recycled and used in new RBCs that are formed in the bone marrow.
TOTAL RBC COUNT
The total RBC count measures how many red blood cells a person has in their peripheral circulation. As noted above, these cells are responsible for transporting oxygen in the body, so it’s important to have a normal count to feel healthy.
NORMAL TOTAL RBC COUNTS: measured in microliters
Adult Male: 4.7-6.1 X 106 / µl Adult Female: 4.2-5.4 X 106 / µl Newborns: 4.8-7.1 X 106 / µl 2-8 weeks old: 4.0-6.0 X 106 / µl 2-12 months: 3.5-5.4 X 106 / µl 1-18 years: 4.0-5.5 X 106 / µl - Normal values may vary slightly from lab to lab depending on the analyzer. - Measured in microliters. Micro = 10-6.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
11 www.4CEUINC.com
Total RBC Calculation: Total RBC Count = RBC x 106 / µl
LOW RBC COUNT
A low RBC count is known as anemia and occurs when there is a decrease of more than 10% of the normal expected value. Low RBC counts can be caused by many factors and disease states including:
Blood loss – Chronic or hemorrhage Dietary deficiencies – iron, vitamin B12, or folate Medical conditions – kidney failure, spleen injury, sepsis, tumor, leukemia, etc. Hemolysis – autoimmune, G6PD deficiency, or spherocytosis Medications – chloramphenicol, chemotherapy, quinidine, etc. Transient or benign conditions – pregnancy or dehydration
Signs and Symptoms of Low RBC Count
Dizziness Shortness of breath Pallor (pale skin) Other symptoms may also be present if the anemia is caused by another disease.
Treatment of Anemia: The specific treatment of the anemia depends on the underlying cause, but can include blood transfusion of packed RBCs (PRBC), supplementation of iron, B12, or folate, discontinuation of medications causing the anemia, or erythropoietin injection to stimulate RBC production.
ELEVATED RBC COUNT
An elevated RBC count is known as polycythemia and typically has a hematocrit near or over 55% in approximately 85% of the cases diagnosed. Types of polycythemia:
Primary polycythemia Secondary polycythemia Relative polycythemia
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
12 www.4CEUINC.com
Primary Polycythemia
Primary polycythemias are due to factors within or related to the RBC precursors (before production), such as the bone marrow or the patient’s genes. There are essentially two types of primary polycythemia:
Polycythemia Vera (aka: Polycythemia Rubra Vera) - This increase in red blood cell production is due to an abnormality in the bone marrow and can often produce increased WBCs and platelets as well. Polycythemia vera is classified as a myeloproliferative disease and carries non-hereditary mutation, V617F, in the JAK2 gene. This mutation is found in 95% of the cases of polycythemia vera, as well as other myeloproliferative disorders.
Primary Familial Polycythemia – This is a benign hereditary condition and may be due to an autosomal dominant mutation of the erythropoietin receptor gene (EPOR). This condition may cause an increase in the oxygen-carrying capacity in the blood by up to 50%.
Secondary Polycythemia
Secondary polycythemia is caused by an increase in the production of erythropoietin. Erythropoietin is a glycoprotein hormone that is produced by the kidney to stimulate red blood cell production. Secondary polycythemia may be caused by natural or artificial causes and will resolve when the underlying cause is treated or resolved. In secondary polycythemia the red cell count is typically 6 to 8 million RBCs per cubic millimeter of blood, with occasional counts slightly higher.
Conditions that cause secondary polycythemia usually produce an increased need for oxygen, which triggers an increase in erythropoietin release. These can include:
High altitude – this is a normal adaptation to lowered oxygen levels at elevations. Smoking, which falsely decreases oxygen levels in the body. Hypoxic diseases – heart disease, COPD, chronic obstructive sleep apnea. Genetic causes - Although relatively uncommon, there are genetic causes of
secondary polycythemia that are associated with abnormalities in hemoglobin oxygen release. These abnormalities may reduce oxygen delivery to the kidneys causing an increase in erythropoietin production.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
13 www.4CEUINC.com
There are also other conditions that cause secondary polycythemia without an increased need for oxygen and can include:
Tumors, including
- Renal-cell carcinoma (kidney cancer)
- Liver tumors
- Benign adrenal gland tumor (adrenal adenoma), which causes Cushing’s disease
- Pheochromocytoma (neuroendocrine tumor) Elevated testosterone levels due to:
- Testosterone replacement therapy
- Anabolic steroid abuse
Relative Polycythemia
Relative polycythemia is caused by reduced blood plasma in the body due to fluid loss, such as, burns, dehydration or stress.
Signs and Symptoms of an Elevated RBC Count
Headache Dizziness Severe itching – seen with polycythemia vera Abnormally enlarged spleen and/or liver Possible blood clot formation (thrombosis) Possible high blood pressure
Treatment of Polycythemia: When treatment is necessary, a “therapeutic phlebotomy” is typically performed. The volume of blood taken will depend on the severity of the polycythemia and is usually directed by the ordering physician. When therapeutic phlebotomies don’t work or can’t be routinely performed, Cytostatic medications, such as bisulfan or hydroxurea, may be administered.

UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
14 www.4CEUINC.com
HEMOGLOBIN
Hemoglobin is found inside each red blood cell and has the main function of carrying oxygen to the tissues, while transporting carbon dioxide back to the lungs for excretion from the body. Hemoglobin is part of the CBC, but is often ordered as an individual test along with the hematocrit to monitor the status of anemia or blood loss in a patient.
STRUCTURE OF HEMOGLOBIN
In adults without any genetic abnormalities, hemoglobin A is the predominant hemoglobin in the body at 97%. Hemoglobin is a large protein that’s made up of four subunits, each with a globin chain and a heme molecule. Of the four globin chains there are 2 α (alpha) and 2 β (beta) chains, each containing one heme molecule. The heme molecule is composed of a porphyrin ring containing four pyrrole molecules with an iron ion in the center. The iron (Fe2+) in the heme molecule is the portion of the protein that actually binds to the oxygen within the cells. Each RBC can transport four oxygen molecules, one bound to each heme molecule.
It should be noted here that in addition to oxygen, heme can also bind to carbon monoxide (CO) and if present, will compete for the heme binding site. Since hemoglobin’s binding affinity for CO is 250 times greater than for oxygen (O2), even small amounts of CO can reduce hemoglobin’s ability to transport oxygen. Since hemoglobin “prefers” binding to CO, it’s easy for carbon monoxide poisoning to occur when it’s present in high enough concentrations in the air. CO can be found in tobacco smoke, car exhaust, and incomplete furnace combustion, with CO poisoning occurring from the latter two if exposure occurs.
Common Abbreviations or Nicknames: Individually it’s abbreviated as Hb or Hgb, but when ordered along with a hematocrit, can be abbreviated as an H & H, HH, or H and H.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
15 www.4CEUINC.com
DECREASED HEMOGLOBIN VALUES
Decreased hemoglobin levels can be caused by various conditions, including:
Carbon monoxide poisoning Blood Loss – acute or chronic Anemia – seen in iron, B12, and folate deficiency Medical conditions – kidney disease, hypothyroidism, hemoglobinopathies, cancer,
certain autoimmune diseases, etc Medications – antineoplastic drugs, some antibiotics, aspirin, sulfonamides, etc. Pregnancy
INCREASED HEMOGLOBIN VALUES
Increased hemoglobin levels can be caused by various conditions, including:
High altitudes Polycythemia Smoking Hypoxic diseases – heart disease, COPD, chronic obstructive sleep apnea. Fluid loss – severe burns or dehydration Medications – gentamicin, Aldomet, testosterone replacement, etc.
SIGNS AND SYMPTOMS OF HEMOGLOBIN CHANGES
Although shortness of breath and fatigue are the hallmark symptoms, the signs and symptoms of either high or low hemoglobin levels are generally similar to those seen with a high or low red cell count. If there is an underlying disease state causing the change in hemoglobin status, the patient may also have symptoms from those diseases as well.
NORMAL HEMOGLOBIN VALUES: Adult Male: 14 – 17 g/dl Adult Female: 12.5 – 15 g/dl Newborn: 14 – 24 g/dl 0 to 2 weeks: 12 – 20 g/dl 6 months to 6 years: 9.5 – 14 g/dl 6 to 18 years: 10 – 15.5 g/dl - Normal values may vary slightly from lab to lab depending on the analyzer.
- Measured in grams per deciliter. Deci = 10-1.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
16 www.4CEUINC.com
HEMATOCRIT
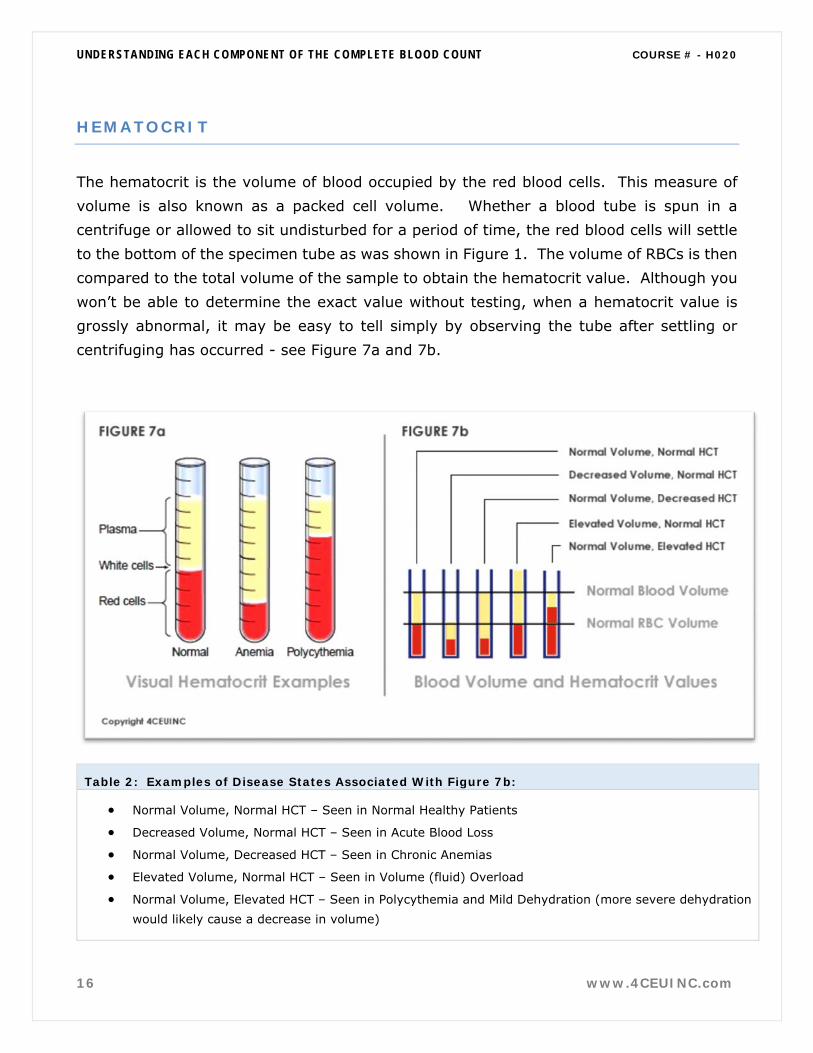
The hematocrit is the volume of blood occupied by the red blood cells. This measure of volume is also known as a packed cell volume. Whether a blood tube is spun in a centrifuge or allowed to sit undisturbed for a period of time, the red blood cells will settle to the bottom of the specimen tube as was shown in Figure 1. The volume of RBCs is then compared to the total volume of the sample to obtain the hematocrit value. Although you won’t be able to determine the exact value without testing, when a hematocrit value is grossly abnormal, it may be easy to tell simply by observing the tube after settling or centrifuging has occurred - see Figure 7a and 7b.
Table 2: Examples of Disease States Associated With Figure 7b:
Normal Volume, Normal HCT – Seen in Normal Healthy Patients Decreased Volume, Normal HCT – Seen in Acute Blood Loss Normal Volume, Decreased HCT – Seen in Chronic Anemias Elevated Volume, Normal HCT – Seen in Volume (fluid) Overload Normal Volume, Elevated HCT – Seen in Polycythemia and Mild Dehydration (more severe dehydration
would likely cause a decrease in volume)
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
17 www.4CEUINC.com
On average, the hematocrit is typically three times the value of the hemoglobin measurement when the patient’s RBC and hemoglobin values are normal. For example, if the hemoglobin value is 15g/dl, the hematocrit should be somewhere around 45%. When there is a deviation from that 3X calculation, it commonly indicates that there is a change in the morphology of the RBCs including the presence of microcytes, macrocytes, or anisocytosis or a change in the RBC or hemoglobin status. Abnormal changes in any of these measurements will affect the hematocrit value.
The hematocrit value can be determined either on an automated analyzer by calculating the value or by performing a manual hematocrit. When an automated hematocrit value is flagged as abnormal, it should always be confirmed by a manual hematocrit.
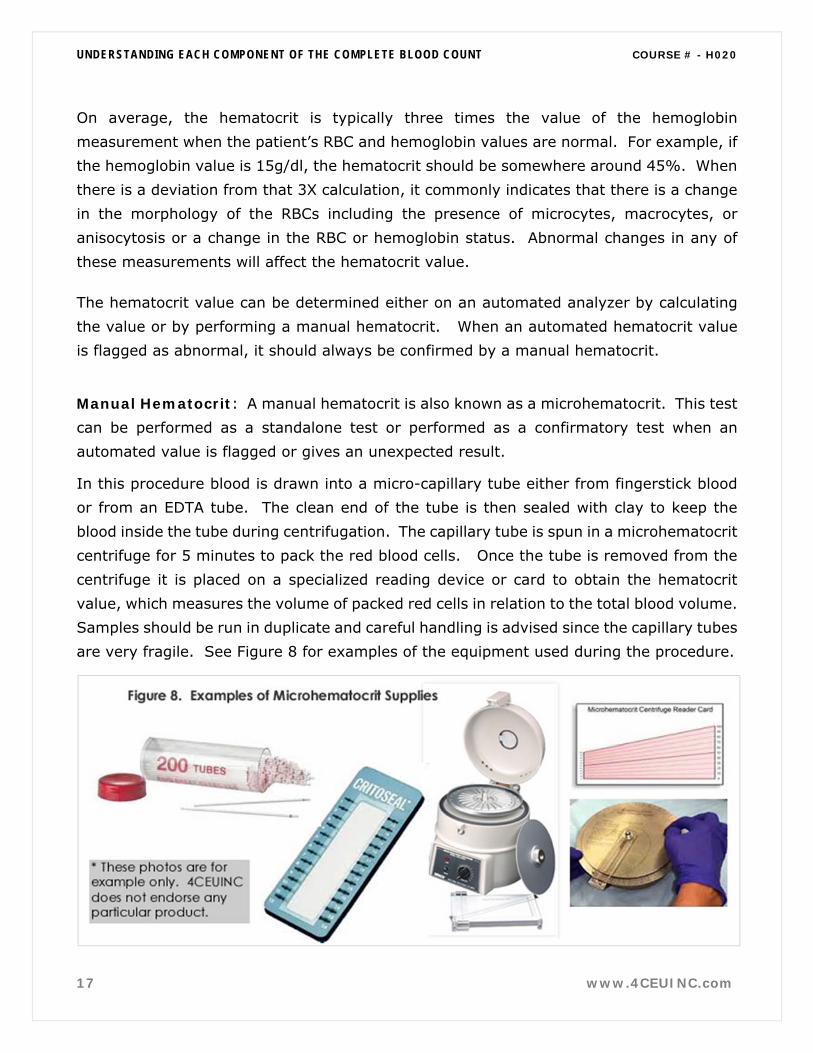
Manual Hematocrit: A manual hematocrit is also known as a microhematocrit. This test can be performed as a standalone test or performed as a confirmatory test when an automated value is flagged or gives an unexpected result.
In this procedure blood is drawn into a micro-capillary tube either from fingerstick blood or from an EDTA tube. The clean end of the tube is then sealed with clay to keep the blood inside the tube during centrifugation. The capillary tube is spun in a microhematocrit centrifuge for 5 minutes to pack the red blood cells. Once the tube is removed from the centrifuge it is placed on a specialized reading device or card to obtain the hematocrit value, which measures the volume of packed red cells in relation to the total blood volume. Samples should be run in duplicate and careful handling is advised since the capillary tubes are very fragile. See Figure 8 for examples of the equipment used during the procedure.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
18 www.4CEUINC.com
Common Abbreviations or Nicknames: The hematocrit has several abbreviations and nicknames. Its most commonly abbreviated as Hct, but as previously noted when ordered along with a hemoglobin, can be abbreviated as an H & H, HH, or H and H.
On occasion, the word hematocrit is simply shortened and referred to as a ‘crit. When it’s referred to as a packed cell volume, it is abbreviated as PCV. Regardless of which abbreviation or nickname is used, they all refer to the same measurement.
COMMON INTERFERING FACTORS
Extremely elevated WBC counts Living in high altitudes Pregnancy may cause slightly decreased values due to hemodilution Medications, including penicillin and chloramphenicol Hemodilution from fluid overload Dehydration Abnormalities in: RBC size, RBC numbers, and Hemoglobin Values immediately after hemorrhage may not be accurate, since blood cell and
NORMAL HEMATOCRIT VALUES:
Adult Male: 42–52% Adult Female: 37–47% Pregnancy: Slightly lower values averaging 33-42% Elderly: Values may be slightly decreased Children: Newborn: 44-64% 2 to 8 weeks: 39-59% 2 to 6 months: 35-50% 6 months to 1 year: 29-53% 1 to 6 years: 30-40% 6 to 18 years: 32-44%
- Normal values may vary slightly from lab to lab depending on the analyzer.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
19 www.4CEUINC.com
fluid loss is initially equal and would not reflect a true picture. In the hours after the loss however, the body replaces the plasma, but cannot replace the cellular portion quickly enough to alleviate the lost cell volume. When a patient receives packed red blood cells after acute blood loss, their hematocrit will rise approximately 3-4% for each unit received provided that active bleeding has stopped.
DECREASED HEMATOCRIT VALUES
Decreased hematocrit levels can be caused by various conditions, including:
Carbon monoxide poisoning Blood Loss – acute or chronic Anemia – seen in iron, B12, and folate deficiency Medical conditions – kidney disease, hypothyroidism, hemoglobinopathies, cancer,
certain autoimmune diseases, etc. Medications – antineoplastic drugs, some antibiotics, aspirin, sulfonamides, etc. Pregnancy
INCREASED HEMATOCRIT VALUES
Increased hemoglobin levels can be caused by various conditions, including:
High altitudes Polycythemia Smoking Hypoxic diseases – heart disease, COPD, chronic obstructive sleep apnea. Fluid loss – severe burns or dehydration Medications – gentamicin, Aldomet, testosterone replacement, etc.
SIGNS AND SYMPTOMS OF HEMATOCRIT CHANGES
As with hemoglobin, the signs and symptoms of either a high or low hematocrit level are generally similar to those seen with a high or low red cell count. Although shortness of breath and fatigue are hallmark symptoms, when there is an underlying disease state causing the change in hematocrit status, the patient may also experience symptoms related to those diseases as well.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
20 www.4CEUINC.com
MCV
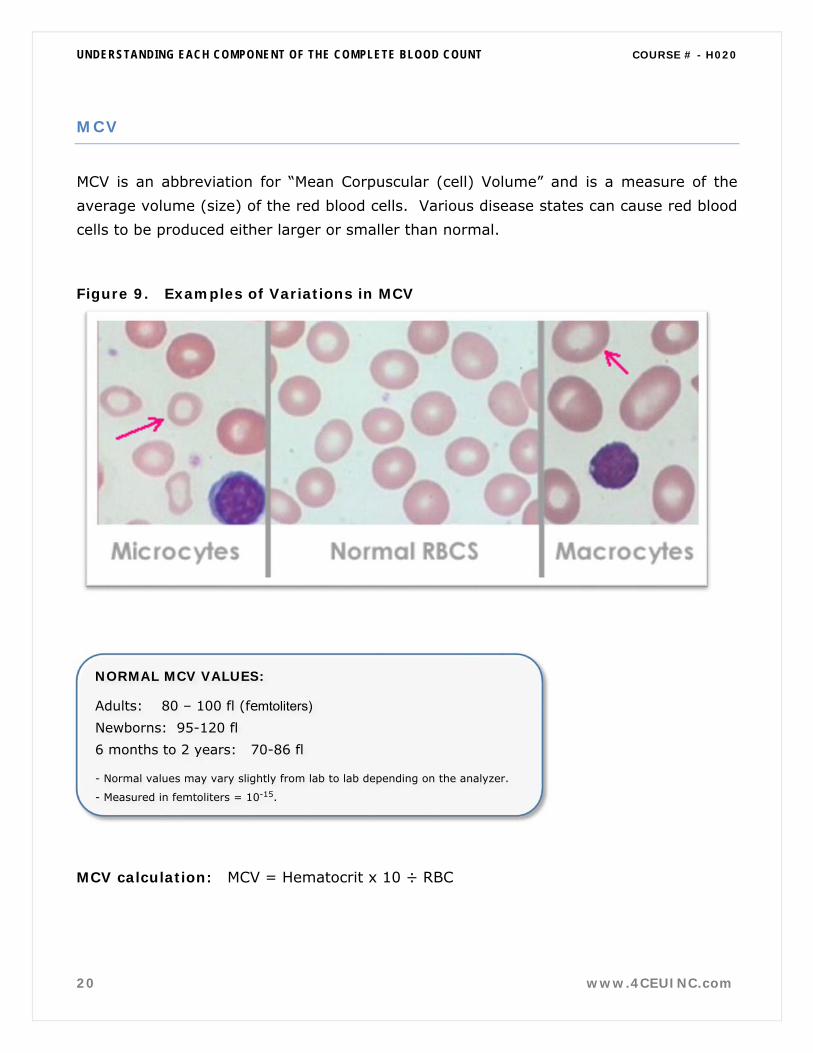
MCV is an abbreviation for “Mean Corpuscular (cell) Volume” and is a measure of the average volume (size) of the red blood cells. Various disease states can cause red blood cells to be produced either larger or smaller than normal.
Figure 9. Examples of Variations in MCV
MCV calculation: MCV = Hematocrit x 10 ÷ RBC
NORMAL MCV VALUES:
Adults: 80 – 100 fl (femtoliters)
Newborns: 95-120 fl 6 months to 2 years: 70-86 fl
- Normal values may vary slightly from lab to lab depending on the analyzer.
- Measured in femtoliters = 10-15.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
21 www.4CEUINC.com
DECREASED MCV
A red blood cell with a decreased MCV is call a Microcyte and microscopically appears smaller than a normal RBC. In comparison, microcytes are usually 6 µm or less. Microcytes can be seen with the following conditions and disease states:
Iron deficiency anemia Chronic blood loss Thalassemia Lead poisoning
ELEVATED MCV
A red blood cell with an elevated MCV is called a Macrocyte and microscopically appears larger than a normal RBC. In comparison, macrocytes are usually 8 µm or more. Macrocytes may be seen with the following conditions and disease states:
Immature red blood cells in the peripheral circulation - These immature cells are called reticulocytes and commonly appear in the peripheral blood after blood loss or anemia while the body is increasing production to replace the RBCs that were lost.
Megaloblastic anemias – These anemias are caused by Vitamin B12 or Folate deficiencies, but may also be seen in alcohol and drug induced liver disease.
MCH
MCH is an abbreviation for “Mean Corpuscular Hemoglobin” and is the measure of the average amount (weight) of hemoglobin within a red blood cell. Since microcytes are smaller, they will have a decreased amount of hemoglobin, while macrocytes will have an increased amount of hemoglobin.
MCH Calculation: MCH = (Hemoglobin x 10) ÷ RBC
NORMAL MCH VALUES: 27 – 31 pg (picograms)
- Normal values may vary slightly from lab to lab depending on the analyzer.
- pico = 10-12
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
22 www.4CEUINC.com
Since the MCH corresponds to the size of the red blood cell, many of the disease states that cause changes in the MCV also cause changes in the MCH.
DECREASED MCH
The following disease states will cause a decreased MCH since they include Microcytes:
Iron deficiency anemia Chronic blood loss Thalassemia Lead poisoning
ELEVATED MCH
The following disease states will cause a decreased MCH since they include Macrocytes:
Megaloblastic anemias – These anemias are caused by Vitamin B12 or Folate deficiencies. May also be seen in alcohol and drug induced liver disease.
MCHC
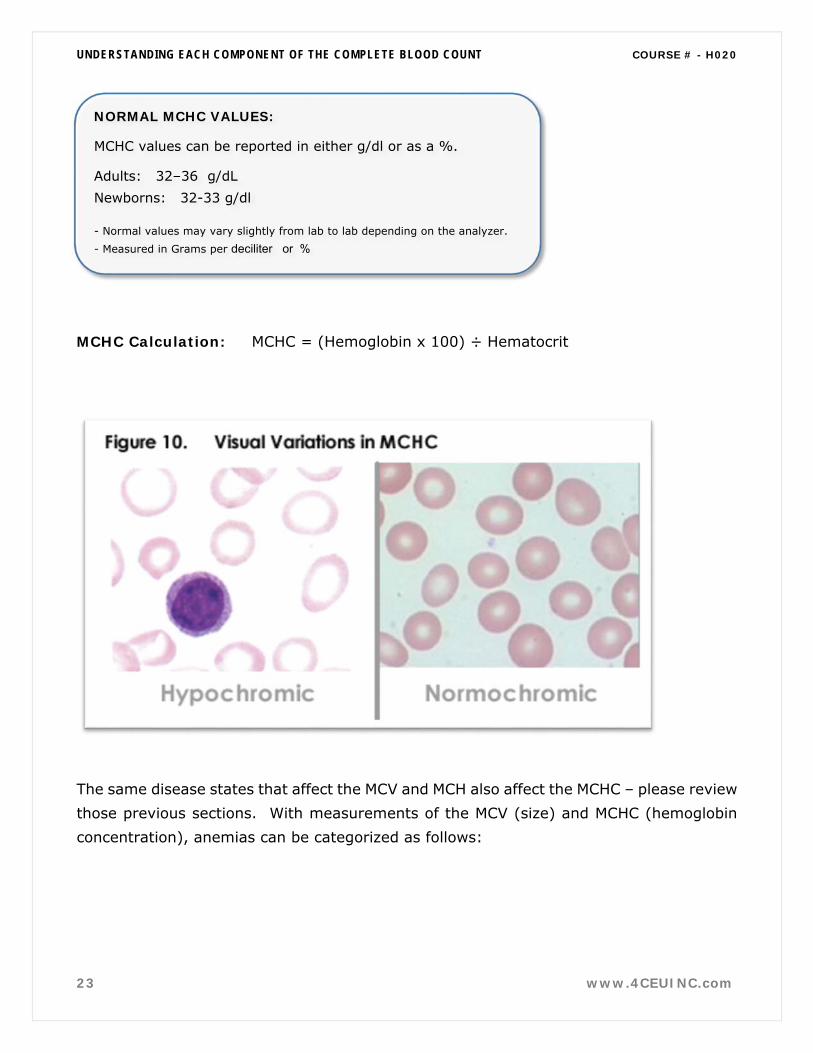
MCHC is an abbreviation for “Mean Corpuscular Hemoglobin Concentration” and is the average concentration of hemoglobin within a red blood cell. Since hemoglobin is what gives RBCs their red color, any variation from the normal concentration will affect the overall appearance of the cell.
When the MCHC is decreased, cells will have a deficient amount of hemoglobin so they will be “hypochromic” and appear pale and “washed out” on a peripheral blood slide. Cells with a normal MCHC are considered “normochromic” and appear normal on a peripheral blood smear. Since RBCs can only fit a maximum of 37 g/dl into a cell, they technically cannot become “hyperchromic”.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
23 www.4CEUINC.com
MCHC Calculation: MCHC = (Hemoglobin x 100) ÷ Hematocrit
The same disease states that affect the MCV and MCH also affect the MCHC – please review those previous sections. With measurements of the MCV (size) and MCHC (hemoglobin concentration), anemias can be categorized as follows:
NORMAL MCHC VALUES:
MCHC values can be reported in either g/dl or as a %.
Adults: 32–36 g/dL Newborns: 32-33 g/dl
- Normal values may vary slightly from lab to lab depending on the analyzer. - Measured in Grams per deciliter or %
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
24 www.4CEUINC.com
NORMOCYTIC, NORMOCHROMIC ANEMIA
Cells are normal size and have a normal appearance (color) microscopically.
Acute blood loss
Aplastic anemia – caused by factors, such as, chloramphenicol toxicosis, pesticide exposure, certain chemotherapy agents, etc.
Acquired hemolytic anemia – autoimmune diseases, drug induced anemias, hemolytic disease of the newborn (HDN), etc.
Iron deficiency anemia - *when detected early
Anemia from illness – caused by factors, such as, sepsis, tumors, etc.
Hereditary – certain diseases can cause anemia, such as, sickle cell disease, hereditary spherocytosis, etc.
MICROCYTIC, HYPOCHROMIC ANEMIA
Cells have a smaller size and have a pale appearance (color) microscopically.
Thalassemia Lead Poisoning Pyridoxine deficiency (Vitamin B6) Iron deficiency anemia - *when detected later in the disease process
MACROCYTIC, NORMOCHROMIC ANEMIA
Cells have a larger size and have a normal appearance (color) microscopically.
Anemia caused by Vitamin B12 or Folic Acid deficiency Chemotherapy
MICROCYTIC, NORMOCHROMIC ANEMIA
Cells have a smaller size and have a normal appearance (color) microscopically.
Anemia from renal disease - caused by a loss of erythropoietin
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
25 www.4CEUINC.com
RDW
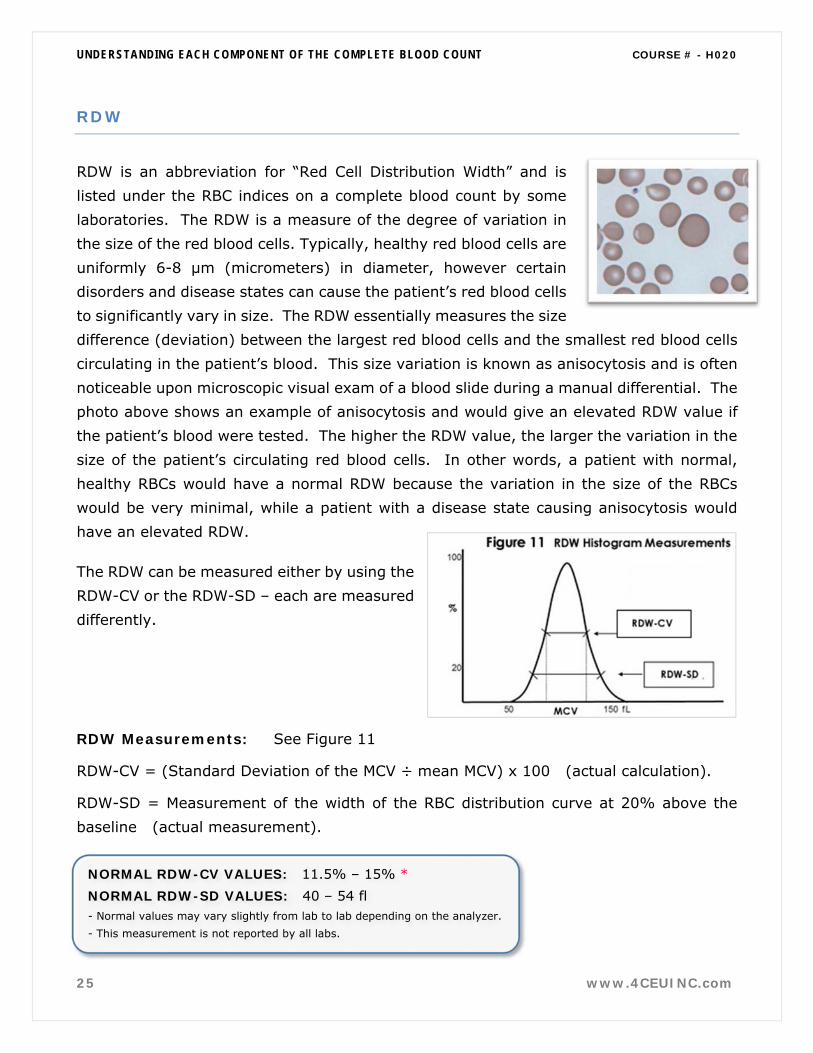
RDW is an abbreviation for “Red Cell Distribution Width” and is listed under the RBC indices on a complete blood count by some laboratories. The RDW is a measure of the degree of variation in the size of the red blood cells. Typically, healthy red blood cells are uniformly 6-8 µm (micrometers) in diameter, however certain disorders and disease states can cause the patient’s red blood cells to significantly vary in size. The RDW essentially measures the size difference (deviation) between the largest red blood cells and the smallest red blood cells circulating in the patient’s blood. This size variation is known as anisocytosis and is often noticeable upon microscopic visual exam of a blood slide during a manual differential. The photo above shows an example of anisocytosis and would give an elevated RDW value if the patient’s blood were tested. The higher the RDW value, the larger the variation in the size of the patient’s circulating red blood cells. In other words, a patient with normal, healthy RBCs would have a normal RDW because the variation in the size of the RBCs would be very minimal, while a patient with a disease state causing anisocytosis would have an elevated RDW.
The RDW can be measured either by using the RDW-CV or the RDW-SD – each are measured differently.
RDW Measurements: See Figure 11
RDW-CV = (Standard Deviation of the MCV ÷ mean MCV) x 100 (actual calculation).
RDW-SD = Measurement of the width of the RBC distribution curve at 20% above the baseline (actual measurement).
NORMAL RDW-CV VALUES: 11.5% – 15% * NORMAL RDW-SD VALUES: 40 – 54 fl - Normal values may vary slightly from lab to lab depending on the analyzer.- This measurement is not reported by all labs.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
26 www.4CEUINC.com
DISEASE STATES THAT CAN AFFECT THE RDW ARE:
Any anemia can cause an abnormal RDW, especially when the disease state is observed before it becomes chronic, at which point most cells will be a more uniform size.
ANEMIA WITH NORMAL RDW
When a normal RDW is seen during anemia, thalassemia should be suspected.
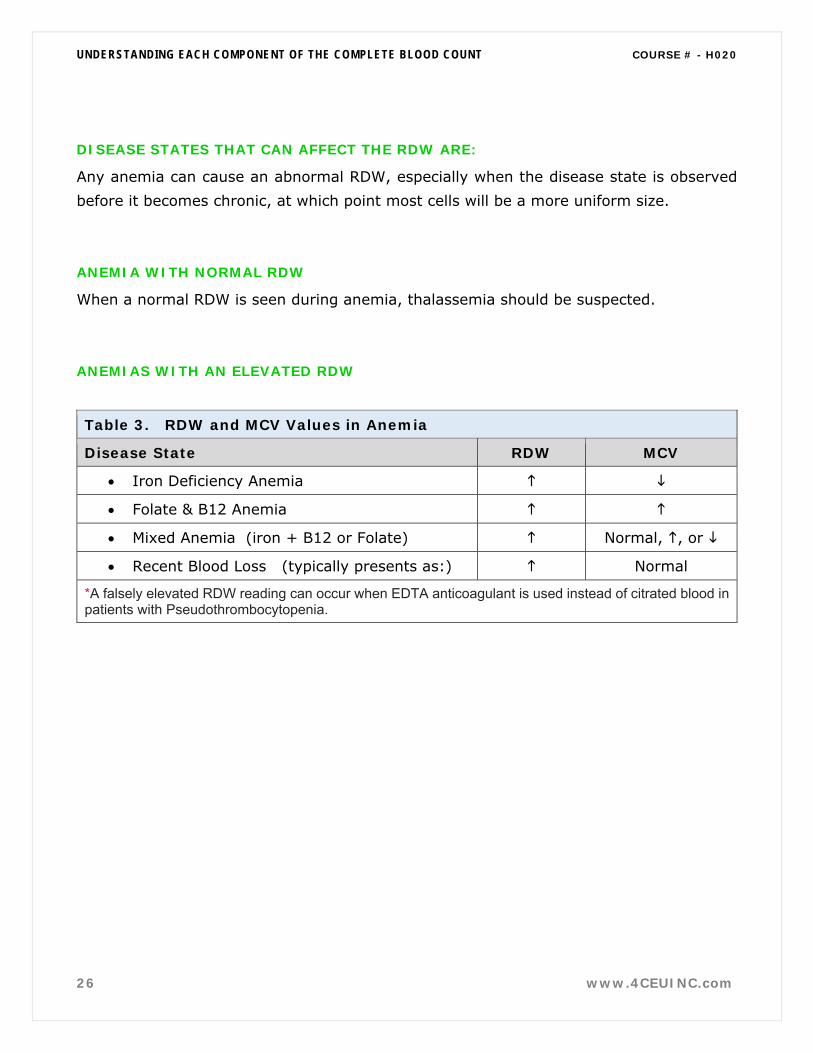
ANEMIAS WITH AN ELEVATED RDW
Table 3. RDW and MCV Values in Anemia
Disease State RDW MCV
Iron Deficiency Anemia
Folate & B12 Anemia
Mixed Anemia (iron + B12 or Folate) Normal, , or
Recent Blood Loss (typically presents as:) Normal
*A falsely elevated RDW reading can occur when EDTA anticoagulant is used instead of citrated blood in patients with Pseudothrombocytopenia.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
27 www.4CEUINC.com
WHITE BLOOD CELLS WBC is an abbreviation for “White Blood Cell”, also referred to as a leukocyte. WBCs are cells of the immune system that help with protecting the body against pathogens, such as bacteria, yeasts, viruses, and parasites. WBCs also play a role in allergies and inflammation.
White blood cells can be found in the bone marrow, peripheral blood, and can also migrate to the tissues when needed during bouts of allergy, inflammation, or infection. All WBCs start out in the bone marrow from a stem cell and mature through either the Myeloid pathway or the Lymphoid pathway.
The Myeloid pathway produces:
Neutrophils Eosinophils Basophils Monocytes
o Macrophages
The Lymphoid pathway produces:
Lymphocytes o Natural Killer Cells o Plasma Cells
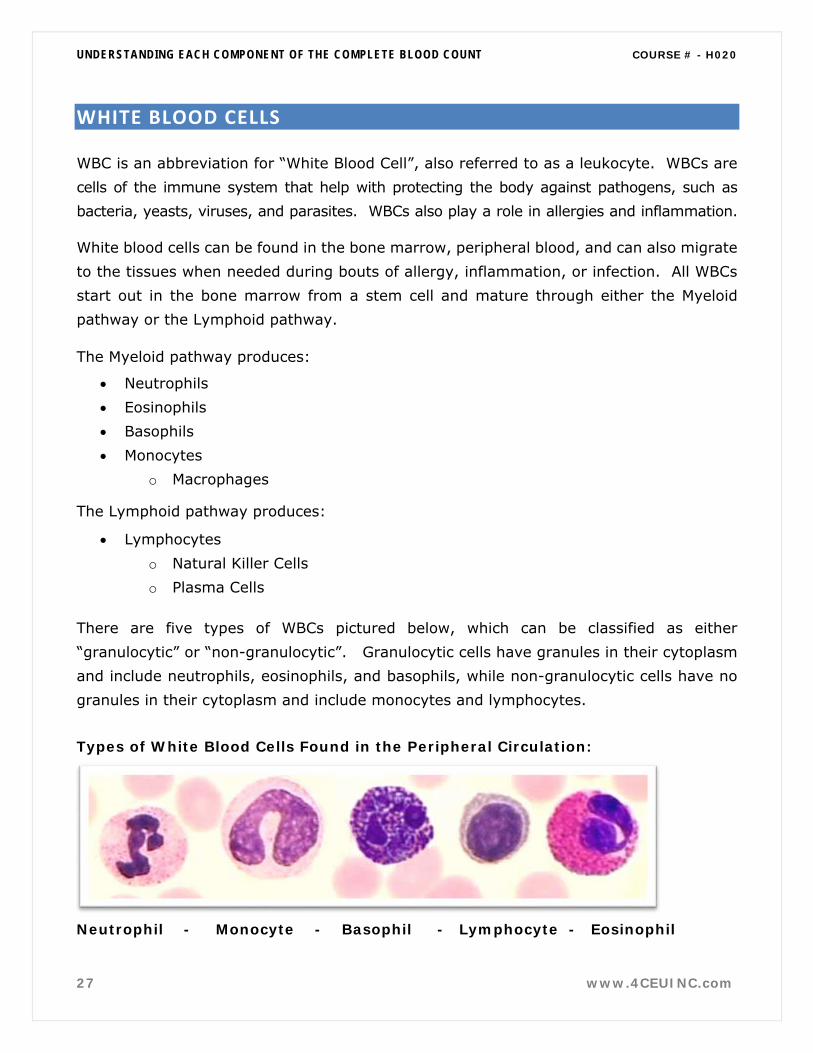
There are five types of WBCs pictured below, which can be classified as either “granulocytic” or “non-granulocytic”. Granulocytic cells have granules in their cytoplasm and include neutrophils, eosinophils, and basophils, while non-granulocytic cells have no granules in their cytoplasm and include monocytes and lymphocytes.
Types of White Blood Cells Found in the Peripheral Circulation:
Neutrophil - Monocyte - Basophil - Lymphocyte - Eosinophil
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
28 www.4CEUINC.com
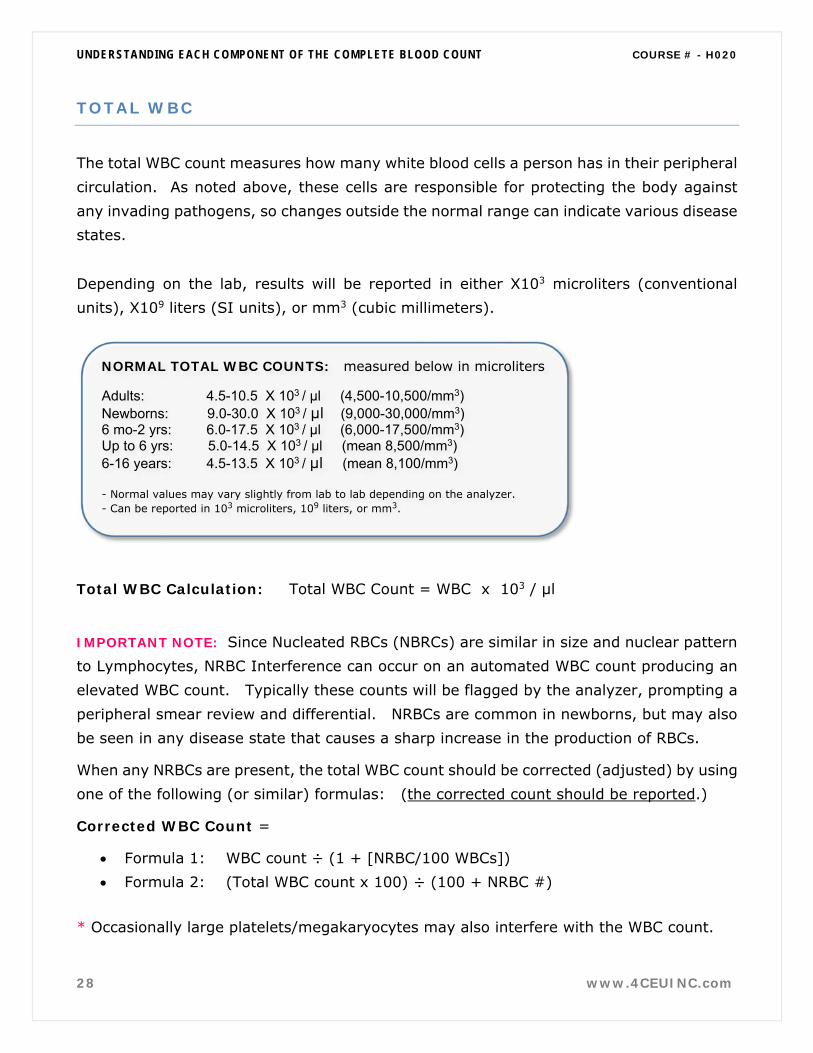
TOTAL WBC
The total WBC count measures how many white blood cells a person has in their peripheral circulation. As noted above, these cells are responsible for protecting the body against any invading pathogens, so changes outside the normal range can indicate various disease states.
Depending on the lab, results will be reported in either X103 microliters (conventional units), X109 liters (SI units), or mm3 (cubic millimeters).
Total WBC Calculation: Total WBC Count = WBC x 103 / µl
IMPORTANT NOTE: Since Nucleated RBCs (NBRCs) are similar in size and nuclear pattern to Lymphocytes, NRBC Interference can occur on an automated WBC count producing an elevated WBC count. Typically these counts will be flagged by the analyzer, prompting a peripheral smear review and differential. NRBCs are common in newborns, but may also be seen in any disease state that causes a sharp increase in the production of RBCs.
When any NRBCs are present, the total WBC count should be corrected (adjusted) by using one of the following (or similar) formulas: (the corrected count should be reported.)
Corrected WBC Count =
Formula 1: WBC count ÷ (1 + [NRBC/100 WBCs]) Formula 2: (Total WBC count x 100) ÷ (100 + NRBC #)
* Occasionally large platelets/megakaryocytes may also interfere with the WBC count.
NORMAL TOTAL WBC COUNTS: measured below in microliters
Adults: 4.5-10.5 X 103 / µl (4,500-10,500/mm3) Newborns: 9.0-30.0 X 103 / µl (9,000-30,000/mm3) 6 mo-2 yrs: 6.0-17.5 X 103 / µl (6,000-17,500/mm3) Up to 6 yrs: 5.0-14.5 X 103 / µl (mean 8,500/mm3) 6-16 years: 4.5-13.5 X 103 / µl (mean 8,100/mm3) - Normal values may vary slightly from lab to lab depending on the analyzer. - Can be reported in 103 microliters, 109 liters, or mm3.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
29 www.4CEUINC.com
LOW WBC COUNT
A low WBC count is known as leukopenia and is recognized typically when the WBC count goes below 2,000/mm3. Low WBC counts can occur from many different factors, including:
Cancer – especially when it originates in the bone marrow Bone marrow deficiency, failure, or infiltration Chemotherapy Radiation exposure or radiation treatment for cancer Autoimmune illness – Lupus, rheumatoid arthritis, Crohn’s disease, etc. Certain infections including, TB, HIV, Mononucleosis, Lyme disease, etc. Severe bacterial infections, including sepsis Certain medications including antibiotics, high blood pressure medications, seizure
medications, histamine-2 blockers, etc.
When a WBC count falls to 500/mm3 or below, it’s considered critical and special precautions need to be taken. Often this is seen with patients on chemotherapy or organ transplantation, although there can be other medical causes. These patients need to take extra precautions if they’re among the normal population, such as wearing a mask, not shaking hands, avoiding pets, etc. When the patient is in the hospital, they will be placed in strict isolation, sometimes referred to as “reverse isolation” in order to protect them from infections that others may expose them to.
Signs of Low WBC Count
Although the signs below are not caused directly by a low WBC count, it is a contributing factor when the patient’s frail immune system predisposes them to increased infections. Many of these signs or symptoms indicate an infection or infectious process taking place. This is not an all-inclusive list:
Fever, chills, or sweats Severe nausea and vomiting Weakness or low blood pressure – can be caused by severe infection or sepsis Cough or shortness of breath Skin rash or blisters Redness, swelling, heat, or drainage at any injection site, IV site, incision, or cut Burning and frequency during urination An increased frequency of infections
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
30 www.4CEUINC.com
Treatment of Leukopenia: The specific treatment of leukopenia depends on the underlying cause, but can include stopping a medication that’s causing the problem, treating the disease contributing to the low WBC count, delaying radiation treatments until the WBC count rises, treating infections such as TB or HIV, etc.
In addition, there are also medications, such as Neulasta, that help increase a WBC count when it’s too low and are commonly given during chemotherapy treatment. Neulasta, a biologic response modifier, is also known as a granulocyte colony stimulating factor (G-CSF) and is responsible for the increased production of WBCs in the bone marrow.
It should be noted that Zinc, Vitamin C, Vitamin D, Selenium, and probiotics also play a role in stimulating the immune system aiding in the production of WBCs.
ELEVATED WBC COUNT
An elevated WBC count is known as Leukocytosis and typically represents a value over 10,000/mm3. Leukocytosis may be caused by a number of factors, including:
Infection Leukemia Trauma Severe mental or physical stress Tissue damage (ie: burns) or necrosis Inflammation Cigarette smoking Certain medications – Epinephrine, heparin, lithium, beta adrenergic agonists (ie:
buterol), corticosteroids (note: steroids may decrease the WBC during severe sepsis), allopurinol, etc.
Pregnancy can sometimes cause a slight elevation in the WBC count during the final month.
Elevated WBC counts can be categorized as being either Benign or Malignant depending on the cause. This distinction will also dictate the treatment and prognosis of the disease. Elevated WBC changes are classified as follows:
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
31 www.4CEUINC.com
Benign Syndromes Causing Leukocytosis
Benign leukocytosis syndromes include:
1.) Leukemoid Reaction o Noted when the WBC count exceeds 50,000/mm3 (some doctors may use
30,000/mm3 as a guideline)
o The cause does not involve the bone marrow, as does leukemia o Typically due to non-malignant causes o Physiological response to stress or infection o Elevation can be of the lymphoid or myeloid line of cells
Morphologically a leukemoid reaction is often indistinguishable from chronic myelogenous leukemia (CML), and less often acute myeloid leukemia (AML), or myeloproliferative disorders. Peripheral blood smears often have many immature WBCs including promyelocytes, myelocytes, and metamyelocytes. Additional testing is needed to distinguish between the disease states (usually a leukemoid reaction and CML), which includes a leukocyte alkaline phosphatase (LAP) and testing for the presence of the Philadelphia chromosome using cytogenetics and FISH or by PCR.
The LAP score is high in reactive states, but low in CML. Approximately 95% of the patients with CML carry the Philadelphia chromosome, which should be tested.
Causes: Leukemoid reactions are typically caused by an underlying medical condition, including:
Infection - TB, Pertussis, Clostridium difficile, Visceral Larva Migrans, etc. Hemorrhage Medications - Dapsone, Sulfa drugs, glucocorticoids, use of granulocyte colony
stimulating factors (G-CSF) or related growth factors, etc. Diabetic ketoacidosis Organ necrosis - especially hepatic necrosis and ischemic colitis
2.) Reactive Leukocytosis o Patient usually has a fever o Exhibits signs of infection o Patient has a normal platelet count and hemoglobin, with a left shift that is
usually fairly mild o WBC count >10,000/mm3, but usually lower than those seen in a leukemoid
reaction
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
32 www.4CEUINC.com
Although similar to a leukemoid reaction in many ways, reactive leukocytosis is less pronounced, more common, and is the body’s response to the offending agent. Causes: Reactive leukocytosis is the body’s response to:
Infection Inflammation Medications - epinephrine, corticosteroids, heparin, etc. Toxins
Malignancy
Malignancy as a cause of leukocytosis includes the following, along with common findings:
1.) Acute leukemia o Abrupt onset o Thrombocytopenia o Peripheral smear with many immature WBCs o Hypercellular marrow with >30% blasts o Hyperuricemia
Types of Acute Leukemia:
Acute Myelogeous Leukemia (AML) – Occurs mostly in adults Acute Lymphocytic Leukemia (ALL) – Occurs mostly in children
Signs and Symptoms of Acute Leukemia Include:
Anemia – dyspnea, pale complexion, fatigue Bleeding – GI tract, gums, easy bruising, petechiae, etc Other hematologic signs- hepatomegaly, splenomegaly, lymphadenopathy Increased infections – body-wide infections can occur even from minor cuts Chloroma – leukemic cell masses in soft tissues Bone pain – from expanding cell mass Kidney problems may develop
2.) Chronic leukemia o Abrupt onset o Normal platelet count o Normal hemoglobin
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
33 www.4CEUINC.com
Types of Chronic Leukemia:
Chronic Myelogeous Leukemia (CML) – Primarily adults (peak 30-50 yrs) Chronic Lymphocytic Leukemia (CLL) – Occurs primarily in adults
Signs and Symptoms of Chronic Leukemia Include:
20% of CML and 50% of CLL patients are initially asymptomatic Weakness & fatigue Itching Weight loss Other hematologic signs- hepatomegaly, splenomegaly, lymphadenopathy Increased infections – body-wide infections can occur even from minor cuts Chloroma – leukemic cell masses in soft tissues Bone pain – from expanding cell mass Kidney problems may develop
PLEASE NOTE: Due to the large amount of information available on the various types of leukemia, we have not included a detailed summary above for leukemia.
NEUTROPHILS
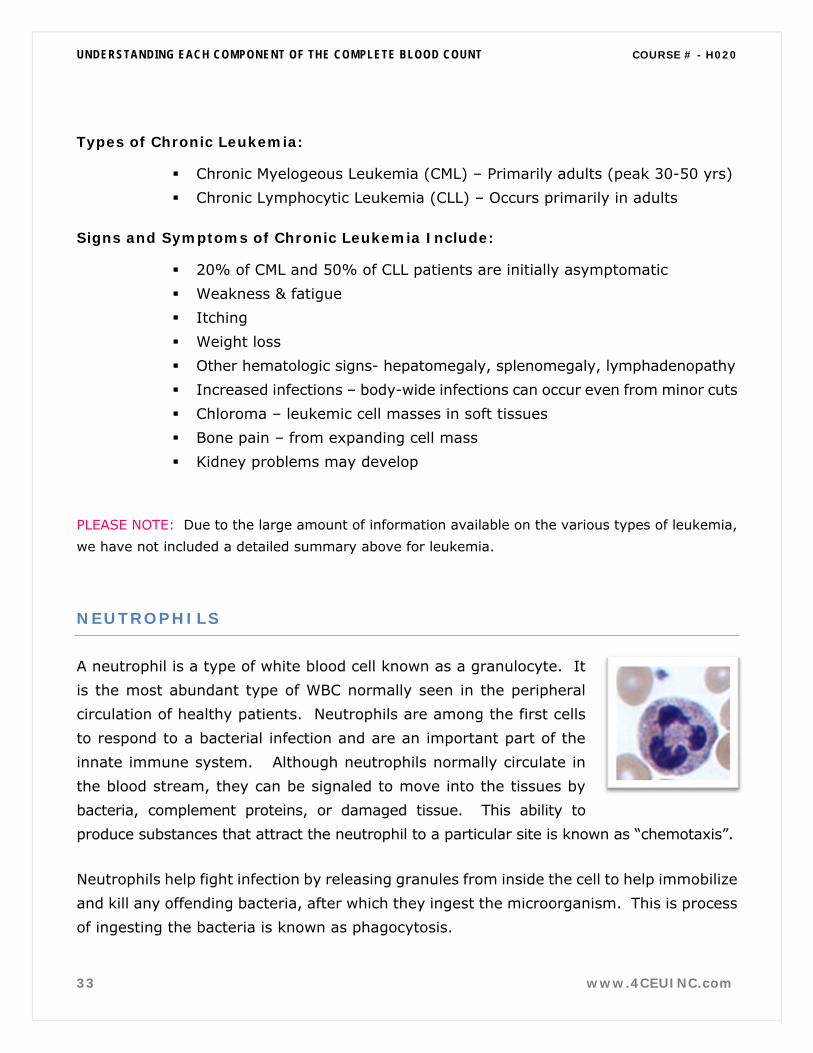
A neutrophil is a type of white blood cell known as a granulocyte. It is the most abundant type of WBC normally seen in the peripheral circulation of healthy patients. Neutrophils are among the first cells to respond to a bacterial infection and are an important part of the innate immune system. Although neutrophils normally circulate in the blood stream, they can be signaled to move into the tissues by bacteria, complement proteins, or damaged tissue. This ability to produce substances that attract the neutrophil to a particular site is known as “chemotaxis”.
Neutrophils help fight infection by releasing granules from inside the cell to help immobilize and kill any offending bacteria, after which they ingest the microorganism. This is process of ingesting the bacteria is known as phagocytosis.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
34 www.4CEUINC.com
Average Cell Size: 10 – 15 µm (micrometers)
Average Lifespan: Neutrophils are produced in large numbers every day since they are removed from the circulation rather quickly. Although there’s been some debate about the lifespan of a neutrophil, most sources report 5.4 days as the average. When a neutrophil becomes “activated” to fight disease or injury, that timeframe becomes much shorter and averages 12—24 hours.
Common Abbreviation or Nicknames: Polymorphonuclear cells (PMNs), Segs, or Polys
Cellular Morphology on a Blood Smear:
Dark blue nucleus with 3-5 lobes connected by thin chromatin (see photo above) Pinkish cytoplasm with fine granules Nuclear to cytoplasmic ratio is 1:3
DECREASED NEUTROPHIL COUNT
A low neutrophil count is known as neutropenia and occurs when the actual count dips below the normal expected value with most physicians recognizing a true neutropenia with a count below 1,700. A neutrophil count below 500 leaves the patient at risk of severe infection. Low neutrophil counts can be caused by many factors and disease states including:
Decreased bone marrow production – hereditary causes, arsenic poisoning, blood cancers, radiation, etc.
Nutritional deficiency - vitamin B12, folate, or copper Increased destruction - chemotherapy, autoimmune neutropenia Medication - Phenytoin, chemotherapy, Bactrim, etc. Overwhelming bacterial infection, especially in the elderly Hemodialysis Any disease causing pancytopenia (a decrease in all cell lines)
NORMAL NEUTROPHIL COUNT: Segmented neutrophils as percent of the differential: 50%-70% Bands (immature neutrophils) as a percent of the differential: 2%-5% As an absolute count - 1.8-7.5 cells per µl (microliter)
- Normal values may vary slightly from lab to lab.

UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
35 www.4CEUINC.com
INCREASED NEUTROPHIL COUNT
An increased neutrophil count is known as neutrophilia and occurs when the neutrophil count goes above 7500. Although neutrophilia is the hallmark of a bacterial infection, high neutrophil counts can be caused by many factors and disease states including:
Acute bacterial or fungal infection Tissue injury and inflammation - burns, trauma, myocardial infarction, autoimmune
collagen vascular diseases, hypersensitivity reaction Physical or Emotional Stress - Exercise, anxiety, epinephrine Metabolic disorders - Ketoacidosis, gout, eclampsia, acute renal failure Myeloproliferative disorders - Myelocytic leukemia, polycythemia vera, etc. Medications – Corticosteroids, lithium, beta agonists (airway medications)
Although normally found in small numbers, when there is an acute infection or other disease causing a large number of neutrophils to be produced, immature neutrophils called “bands” will be found in elevated numbers in the peripheral circulation. This is known as a “Left Shift” and is significant to the physician, suggesting acute inflammation or infection. Visually, the band differs from a segmented neutrophil only by the appearance of the nucleus. Rather than having lobes or segments as a mature neutrophil has, a band will not have any segments or thin chromatin fibers, but rather appear as one solid, curved, nucleus as pictured to the right.
EOSINOPHILS
An eosinophil is a type of white blood cell known as a granulocyte and is the 2nd least common cell (in quantity) found in the peripheral blood, only behind basophils. Visually it is very distinctive under the microscope with its bright red granules, as shown in the photo to the left. Although the eosinophil can be found in the peripheral circulation, it is primarily a tissue-dwelling cell and in humans the
eosinophil tissue/blood ratio is about 100:1. When in the tissues they tend to migrate mainly to the lungs, gastrointestinal tract, and skin.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
36 www.4CEUINC.com
Eosinophils are found in numerous inflammatory processes, especially allergic disorders and parasitic infections. Once they move to the areas of inflammation they are capable of phagocytosis (killing & ingesting microorganisms, especially parasites), as well as, participating in immediate allergic reactions, and modulating inflammatory responses. The numerous granules located inside the eosinophils play a large part in the roles they play in both inflammatory and allergic responses. Eosinophilic granules include cytokines, chemokines, growth factors, cationic proteins, etc. In addition to their inflammatory and phagocytic properties, their granules also assist in regulating the function of mast cells found in tissues.
Average Cell Size: 10 – 17 µm (micrometers)
Average Lifespan: In the peripheral circulation eosinophils have a short half-life of 8-12 hours, while the lifespan of tissue dwelling eosinophils ranges from 2-5 days on average. Lab studies have shown that when a tissue eosinophil becomes “activated” by surrounding cytokines, that timeframe can increase to 14 days or longer in some cases.
Common Abbreviation or Nicknames: eo or eos
Cellular Morphology on a Blood Smear:
Deep blue-purple nucleus with 2 lobes Pink cytoplasm with bright red granules, which often obscure the cytoplasmic
background Nuclear to cytoplasmic ratio is 1:3
DECREASED EOSINOPHIL COUNTS
A decreased eosinophil count is known as eosinopenia. Because there are so few eosinophils in the blood a decreased count is uncommon and often hard to determine, however, there are a few disease states that have lowered eosinophil production and activity including:
Stress Steroid use
NORMAL EOSINOPHIL COUNT: As a percent of a manual differential: 1%-4% As an absolute count - 0.0-0.4 cells per µl (microliter)
- Normal values may vary slightly from lab to lab.
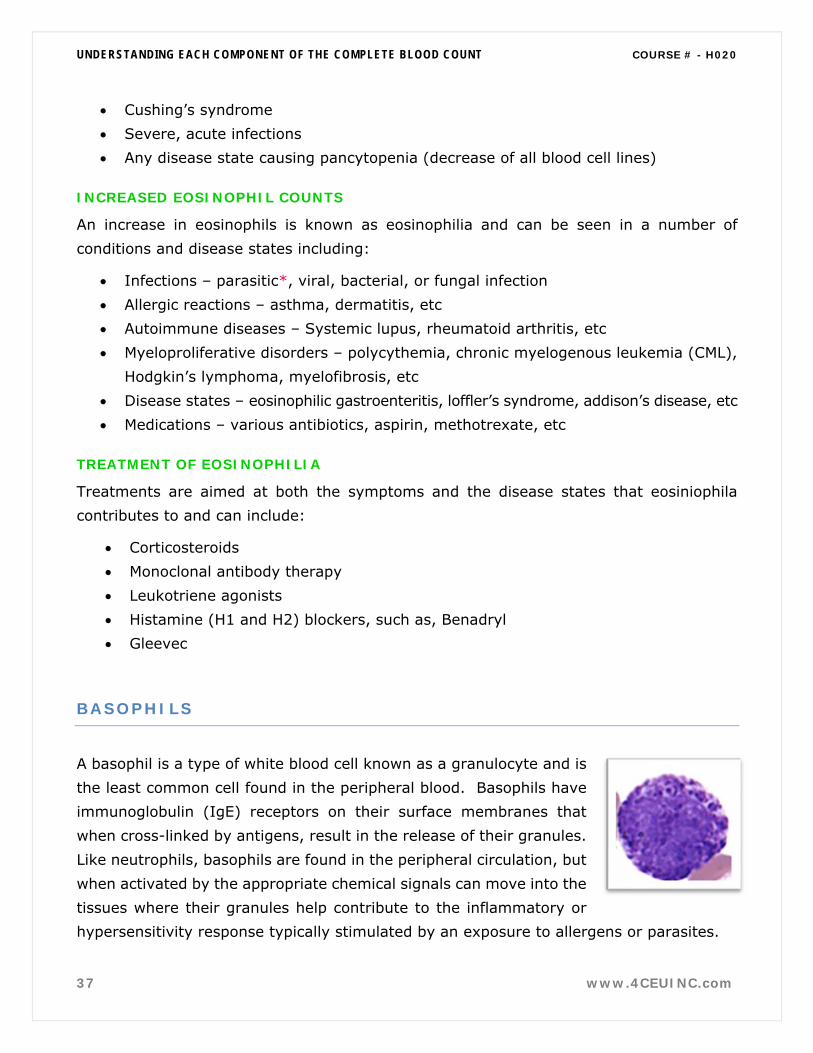
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
37 www.4CEUINC.com
Cushing’s syndrome Severe, acute infections Any disease state causing pancytopenia (decrease of all blood cell lines)
INCREASED EOSINOPHIL COUNTS
An increase in eosinophils is known as eosinophilia and can be seen in a number of conditions and disease states including:
Infections – parasitic*, viral, bacterial, or fungal infection Allergic reactions – asthma, dermatitis, etc Autoimmune diseases – Systemic lupus, rheumatoid arthritis, etc Myeloproliferative disorders – polycythemia, chronic myelogenous leukemia (CML),
Hodgkin’s lymphoma, myelofibrosis, etc Disease states – eosinophilic gastroenteritis, loffler’s syndrome, addison’s disease, etc Medications – various antibiotics, aspirin, methotrexate, etc
TREATMENT OF EOSINOPHILIA
Treatments are aimed at both the symptoms and the disease states that eosiniophila contributes to and can include:
Corticosteroids Monoclonal antibody therapy Leukotriene agonists Histamine (H1 and H2) blockers, such as, Benadryl Gleevec
BASOPHILS
A basophil is a type of white blood cell known as a granulocyte and is the least common cell found in the peripheral blood. Basophils have immunoglobulin (IgE) receptors on their surface membranes that when cross-linked by antigens, result in the release of their granules. Like neutrophils, basophils are found in the peripheral circulation, but when activated by the appropriate chemical signals can move into the tissues where their granules help contribute to the inflammatory or hypersensitivity response typically stimulated by an exposure to allergens or parasites.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
38 www.4CEUINC.com
The granules inside basophils contain multiple chemicals, each with their own immune task. Those granules include heparin, histamine, platelet activating factor (PAF), interleukin-4, and peroxidase, just to name a few. Those chemicals contribute to immediate hypersensitivity reactions, as well as, prolonged allergic responses capable of triggering smooth muscle contraction, as seen in asthma. The histamine serves as a vasodilator bringing more blood to the area of inflammation. As part of the allergic response, basophils are also known to attract eosinophils to the area, as is seen in both allergic responses and parasitic infections.
Average Cell Size: 10 – 15 µm (micrometers)
Average Lifespan: : According to most sources, basophils spend approximately 3.5 days in the peripheral circulation, however, when “activated” to an area of allergy or inflammation, that timeframe can lengthen.
Common Abbreviation or Nickname: baso or basos
Cellular Morphology on a Blood Smear:
Dark purple nucleus with 2 lobes Pale blue cytoplasm with dark purple-black course granules , which often obscure
the view of the nucleus & cytoplasm Nuclear to cytoplasmic ratio is 1:3
DECREASED BASOPHIL COUNT
A decreased basophil count is known as basopenia. Because there are so few basophils in the blood a decreased count is often hard to determine, however, there are a few disease states that have lowered basophil production and activity including:
Hyperthyroidism Stress Pregnancy
NORMAL BASOPHIL COUNT: As a percent of a manual differential: 0%-2% As an absolute count - 0.0-0.2 cells per µl (microliter)
- Normal values may vary slightly from lab to lab.
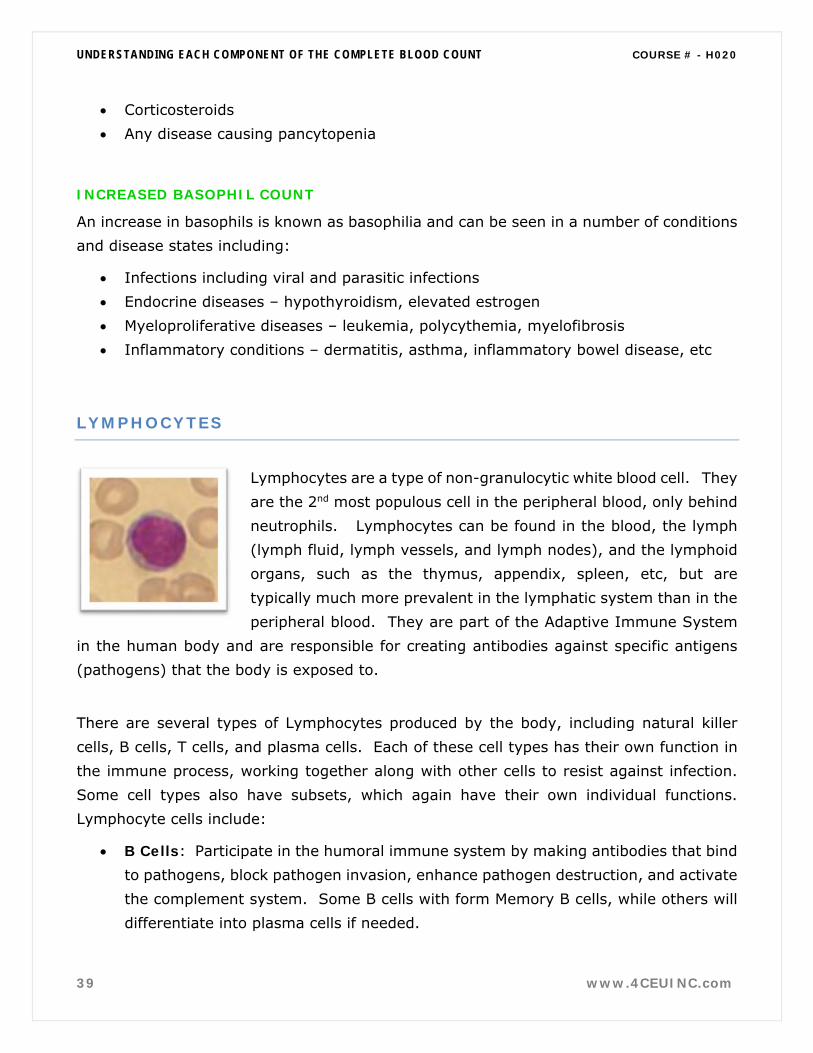
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
39 www.4CEUINC.com
Corticosteroids Any disease causing pancytopenia
INCREASED BASOPHIL COUNT
An increase in basophils is known as basophilia and can be seen in a number of conditions and disease states including:
Infections including viral and parasitic infections Endocrine diseases – hypothyroidism, elevated estrogen Myeloproliferative diseases – leukemia, polycythemia, myelofibrosis Inflammatory conditions – dermatitis, asthma, inflammatory bowel disease, etc
LYMPHOCYTES
Lymphocytes are a type of non-granulocytic white blood cell. They are the 2nd most populous cell in the peripheral blood, only behind neutrophils. Lymphocytes can be found in the blood, the lymph (lymph fluid, lymph vessels, and lymph nodes), and the lymphoid organs, such as the thymus, appendix, spleen, etc, but are typically much more prevalent in the lymphatic system than in the peripheral blood. They are part of the Adaptive Immune System
in the human body and are responsible for creating antibodies against specific antigens (pathogens) that the body is exposed to.
There are several types of Lymphocytes produced by the body, including natural killer cells, B cells, T cells, and plasma cells. Each of these cell types has their own function in the immune process, working together along with other cells to resist against infection. Some cell types also have subsets, which again have their own individual functions. Lymphocyte cells include:
B Cells: Participate in the humoral immune system by making antibodies that bind to pathogens, block pathogen invasion, enhance pathogen destruction, and activate the complement system. Some B cells with form Memory B cells, while others will differentiate into plasma cells if needed.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
40 www.4CEUINC.com
o Memory B Cells: Memory B cells are responsible for carrying immunity to
certain diseases for decades through a person’s life. Immunity can come either by exposure to an illness or through vaccination.
o Plasma Cells: Plasma cells form from some B cells. During a pathogen invasion, plasma cells basically become antibody producing factories that flood the body with antibody to that specific antigen, marking it for destruction.
T Cells: Play a central role in cell-mediated immunity. Distinguished from other lymphocytes by the presence of T cell receptors (TCR).
o T Helper Cells: Also referred to as CD4+ cells. They interact with Macrophages, secreting interleukin-2. The interleukin-2 helps proliferate Cytotoxic T cells & certain B cells, further activating those B cells to differentiate into Plasma cells.
o Cytotoxic T Cells: Also referred to as CD8+ T cells. Critical for removing virus and cancer from infected cells by use of cytotoxins that cause apoptosis.
o Regulatory T Cells: A type of T helper cell that monitors and inhibits the activity of other T cells. They help to prevent adverse immune responses, including autoimmunity.
Natural Killer Cells: Able to kill infected cells (usually virus infected) and tumor cells in the body without destroying surrounding cells. NK cells are the only Lymphocyte that has granules, which they use to accomplish cell destruction by punching holes in the cells, causing apoptosis to occur.
PLEASE NOTE: In general Hematology departments neither electronic counting methods nor manual differentials can differentiate between the various types of Lymphocytes on a CBC.
NORMAL LYMPHOCYTE COUNT: As a percent of a manual differential: 20%-40% As an absolute count - 1.0-3.5 cells per µl (microliter)
- Normal values may vary slightly from lab to lab.
The website link listed below connects to a fabulous video of how the immune response takes place. It describes in detail how Macrophages work with Lymphocytes to overcome & destroy a pathogen in the body: https://www.youtube.com/watch?v=Bf2t8n1ibwQ
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
41 www.4CEUINC.com
Average Lifespan: Since there are several subsets of lymphocytes the average lifespan can range from weeks to decades depending on the cell. Memory B Cells can last for decades and are what’s responsible for secondary immunity post-vaccination or post-illness.
Common Abbreviation or Nicknames: Lymph(s)
Cellular Morphology on a Blood Smear:
Small Lymphocytes: Round to slightly oval shape Deep blue-purple nucleus Scant blue cytoplasm May have a few “reddish” colored granules around the edges of the cytoplasm Nuclear to Cytoplasmic ration is 4:1 Average size - 7 – 9 µm (micrometers)
Large Lymphocytes: Round to slightly oval shape Blue-purple nucleus Moderate amount of light blue cytoplasm Nuclear to cytoplasmic ratio is approximately 3½:1 Average size - 9 – 15 µm (micrometers)
Reactive Lymphocytes: Typically has an oval to irregular shape, with peripheral edges that indent as
they wrap around surround cells (usually RBCs) Purple nucleus Cytoplasm can be light to dark blue, typically with dark edges May have a few light purple granules in the cytoplasm Nuclear to cytoplasmic ratio varies between 3:1 to 1:1 depending on the cell Often confused for a monocyte Average size - 9 – 30 µm (micrometers)
Plasma Cell: Round to slightly oval shape Deep blue-purple nucleus which is typically off center Dark blue cytoplasm; may contain vacuoles and a slight clearing next to the nucleus Nuclear to cytoplasmic ratio varies from 1:1 to 1:2 Average size - 10 – 20 µm (micrometers)
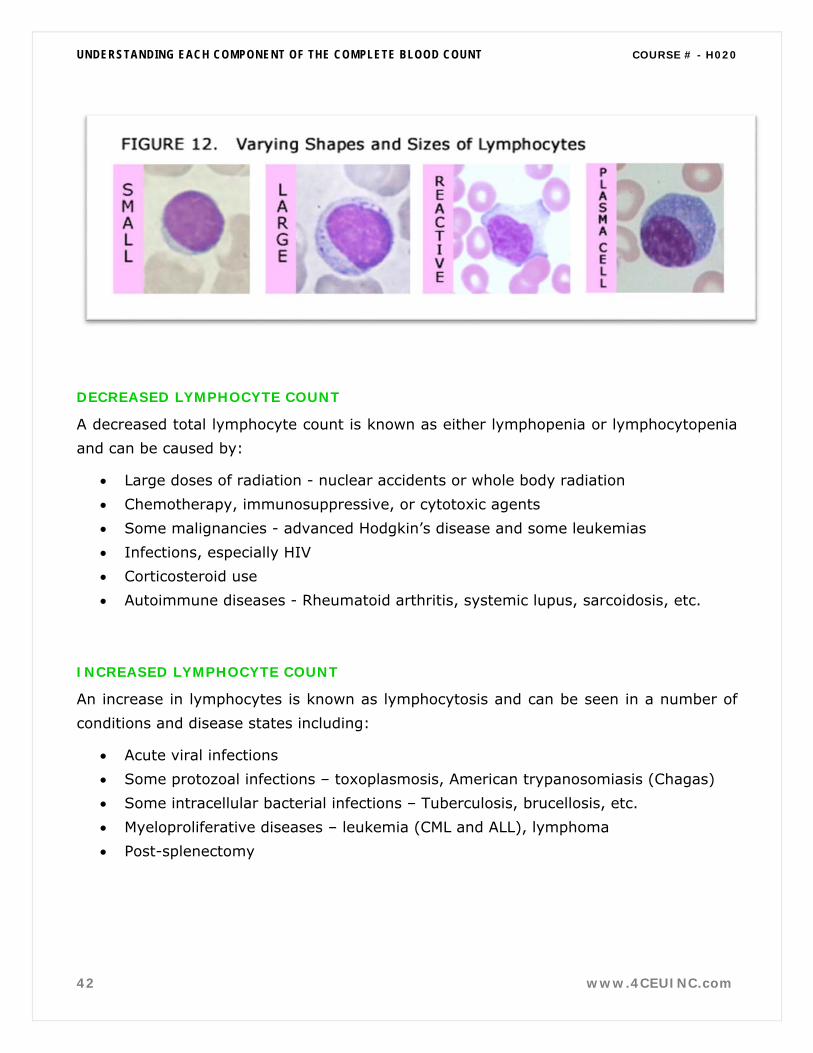
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
42 www.4CEUINC.com
DECREASED LYMPHOCYTE COUNT
A decreased total lymphocyte count is known as either lymphopenia or lymphocytopenia and can be caused by:
Large doses of radiation - nuclear accidents or whole body radiation Chemotherapy, immunosuppressive, or cytotoxic agents Some malignancies - advanced Hodgkin’s disease and some leukemias Infections, especially HIV Corticosteroid use Autoimmune diseases - Rheumatoid arthritis, systemic lupus, sarcoidosis, etc.
INCREASED LYMPHOCYTE COUNT
An increase in lymphocytes is known as lymphocytosis and can be seen in a number of conditions and disease states including:
Acute viral infections Some protozoal infections – toxoplasmosis, American trypanosomiasis (Chagas) Some intracellular bacterial infections – Tuberculosis, brucellosis, etc. Myeloproliferative diseases – leukemia (CML and ALL), lymphoma Post-splenectomy

UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
43 www.4CEUINC.com
CLOSER LOOK AT THE DIFFERENT LYMPHOCYTE POPULATIONS
As Figures 3 and 4 show, the Lymphocyte cell line breaks off into several different subsets, each discussed below:
B Cells
B cells have two major functions: They present antigens to T cells, and more importantly, they produce antibodies to neutralize infectious microbes. Antibodies coat the surface of a pathogen and serve three major roles: neutralization, opsonization, and complement activation.
Neutralization occurs when the pathogen, because it is covered in antibodies, is unable to bind and infect host cells. In opsonization, an antibody-bound pathogen serves as a red flag to alert immune cells like neutrophils and macrophages, to engulf and digest the pathogen. Complement is a process for directly destroying, or lysing, bacteria.
Antibodies are expressed in two ways. The B-cell receptor (BCR), which sits on the surface of a B cell, is actually an antibody. B cells also secrete antibodies to diffuse and bind to pathogens. This dual expression is important because the initial problem, for instance a bacteria, is recognized by a unique BCR and activates the B cell. The activated B cell responds by secreting antibodies, essentially the BCR but in soluble form. This ensures that the response is specific against the bacterium that started the whole process.
Every antibody is unique, but they fall under general categories: IgM, IgD, IgG, IgA, and IgE - Ig is short for immunoglobulin, which is another word for antibody. While they have overlapping roles, IgM generally is important for complement activation; IgD is involved in activating basophils; IgG is important for neutralization, opsonization, and complement activation; IgA is essential for neutralization in the gastrointestinal tract; and IgE is necessary for activating mast cells in parasitic and allergic responses.
T Cells
T cells have a variety of roles and are classified by subsets. T cells are divided into two broad categories: CD8+ T cells or CD4+ T cells, based on which protein is present on the cell's surface. T cells carry out multiple functions, including killing infected cells and activating or recruiting other immune cells.
CD8+ T cells are also called cytotoxic T cells or cytotoxic lymphocytes (CTLs). They are crucial for recognizing and removing virus-infected cells and cancer cells. CTLs have specialized
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
44 www.4CEUINC.com
compartments, or granules, containing cytotoxins that cause apoptosis, i.e., programmed cell death. Because of its potency, the release of granules is tightly regulated by the immune system.
The four major CD4+ T-cell subsets are TH1, TH2, TH17, and Treg, with "TH" referring to "T helper cell." TH1 cells are critical for coordinating immune responses against intracellular microbes, especially bacteria. They produce and secrete molecules that alert and activate other immune cells, like bacteria-ingesting macrophages. TH2 cells are important for coordinating immune responses against extracellular pathogens, like helminths (parasitic worms), by alerting B cells, granulocytes, and mast cells. TH17 cells are named for their ability to produce interleukin 17 (IL-17), a signaling molecule that activates immune and non-immune cells. TH17 cells are important for recruiting neutrophils.
Natural Killer Cells
Natural killer (NK) cells have features of both innate and adaptive immunity. They are important for recognizing and killing virus-infected cells or tumor cells. They contain intracellular compartments called granules, which are filled with proteins that can form holes in the target cell and also cause apoptosis, the process for programmed cell death. It is important to distinguish between apoptosis and other forms of cell death like necrosis. Apoptosis, unlike necrosis, does not release danger signals that can lead to greater immune activation and inflammation. Through apoptosis, immune cells can discreetly remove infected cells and limit bystander damage. Recently, researchers have shown in mouse models that NK cells, like adaptive cells, can be retained as memory cells and respond to subsequent infections by the same pathogen.
Plasma cells
Some B cells differentiate into Plasma cells once they are activated by T-helper cells. As more and more cells are produced, they flood the body with millions of antibodies specific to the antigen (pathogen) that’s causing infection. It should be noted that not all B cells turn into plasma cells, so remain as memory B cells.
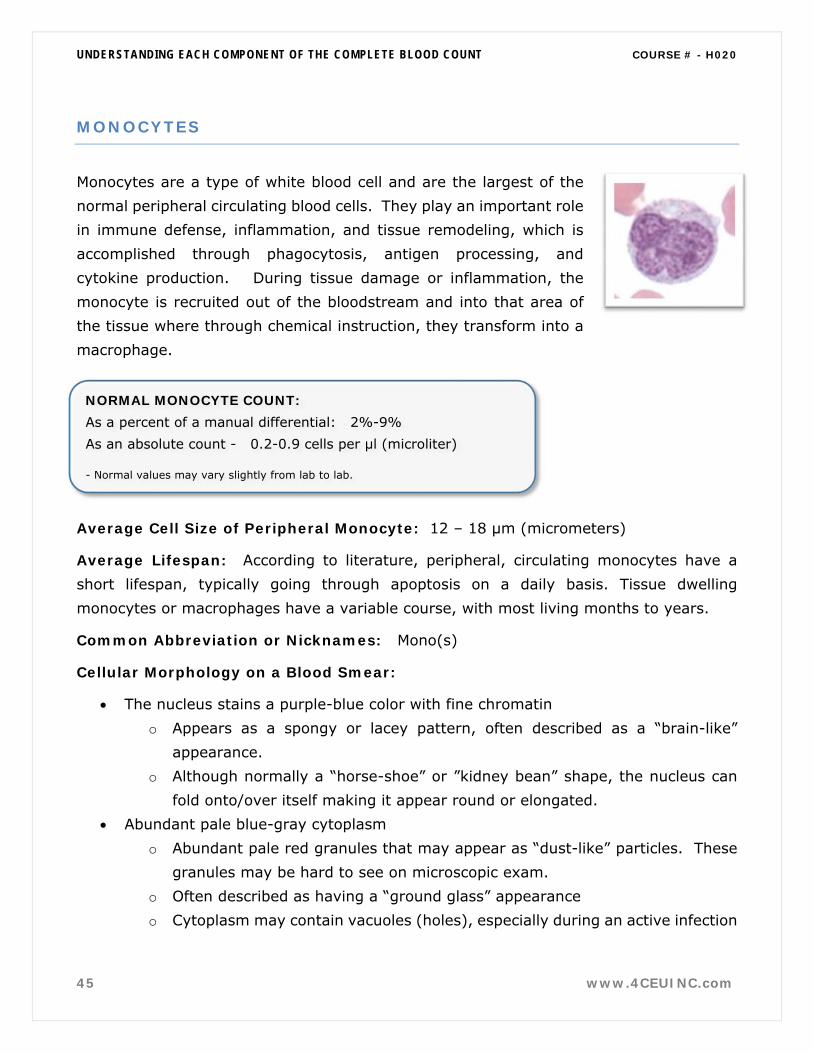
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
45 www.4CEUINC.com
MONOCYTES
Monocytes are a type of white blood cell and are the largest of the normal peripheral circulating blood cells. They play an important role in immune defense, inflammation, and tissue remodeling, which is accomplished through phagocytosis, antigen processing, and cytokine production. During tissue damage or inflammation, the monocyte is recruited out of the bloodstream and into that area of the tissue where through chemical instruction, they transform into a macrophage.
Average Cell Size of Peripheral Monocyte: 12 – 18 µm (micrometers)
Average Lifespan: According to literature, peripheral, circulating monocytes have a short lifespan, typically going through apoptosis on a daily basis. Tissue dwelling monocytes or macrophages have a variable course, with most living months to years.
Common Abbreviation or Nicknames: Mono(s)
Cellular Morphology on a Blood Smear:
The nucleus stains a purple-blue color with fine chromatin o Appears as a spongy or lacey pattern, often described as a “brain-like”
appearance. o Although normally a “horse-shoe” or ”kidney bean” shape, the nucleus can
fold onto/over itself making it appear round or elongated. Abundant pale blue-gray cytoplasm
o Abundant pale red granules that may appear as “dust-like” particles. These granules may be hard to see on microscopic exam.
o Often described as having a “ground glass” appearance o Cytoplasm may contain vacuoles (holes), especially during an active infection
NORMAL MONOCYTE COUNT: As a percent of a manual differential: 2%-9% As an absolute count - 0.2-0.9 cells per µl (microliter)
- Normal values may vary slightly from lab to lab.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
46 www.4CEUINC.com
o Since monocytes are motile cells they may have visible arm-like projections or pseudopods, which help them to move about and also assist in engulfing pathogens.
Nuclear to cytoplasmic ratio is approximately 2:1 Often hard to distinguish from a reactive lymphocyte
MONOCYTE SUBPOPULATIONS
There are three types of monocytes in the blood:
Classical monocytes are characterized by high level expression of the CD14 cell surface receptor: CD14++ CD16- monocyte
Non-Classical monocytes show low level expression of CD14 and additional co-expression of the CD16 receptor: CD14+ CD16++ monocyte
Intermediate monocytes with high level expression of CD14 and low level expression of CD16: CD14++ CD16++ monocytes
o There’s evidence to suggest that intermediate monocytes have been shown to contribute to the development of atherosclerosis in the general population, especially patients with chronic kidney disease (CKD).
o Predisposed to secrete pro-inflammatory cytokines o When increasing numbers are found in CKD patients, it indicates worsening
renal function.
DECREASED MONOCYTE COUNT
A decrease in the number of monocytes is known as monocytopenia and can be seen in:
Certain medications, including prednisone Anemias: Aplastic anemia and Lymphocytic leukemia
INCREASED MONOCYTE COUNT
An increase in the number of monocytes is known as monocytosis and can be seen in a number of disease states including:
Chronic inflammatory conditions Infections, including: tuberculosis, parasites, viral infections, rickettsial infections, etc.
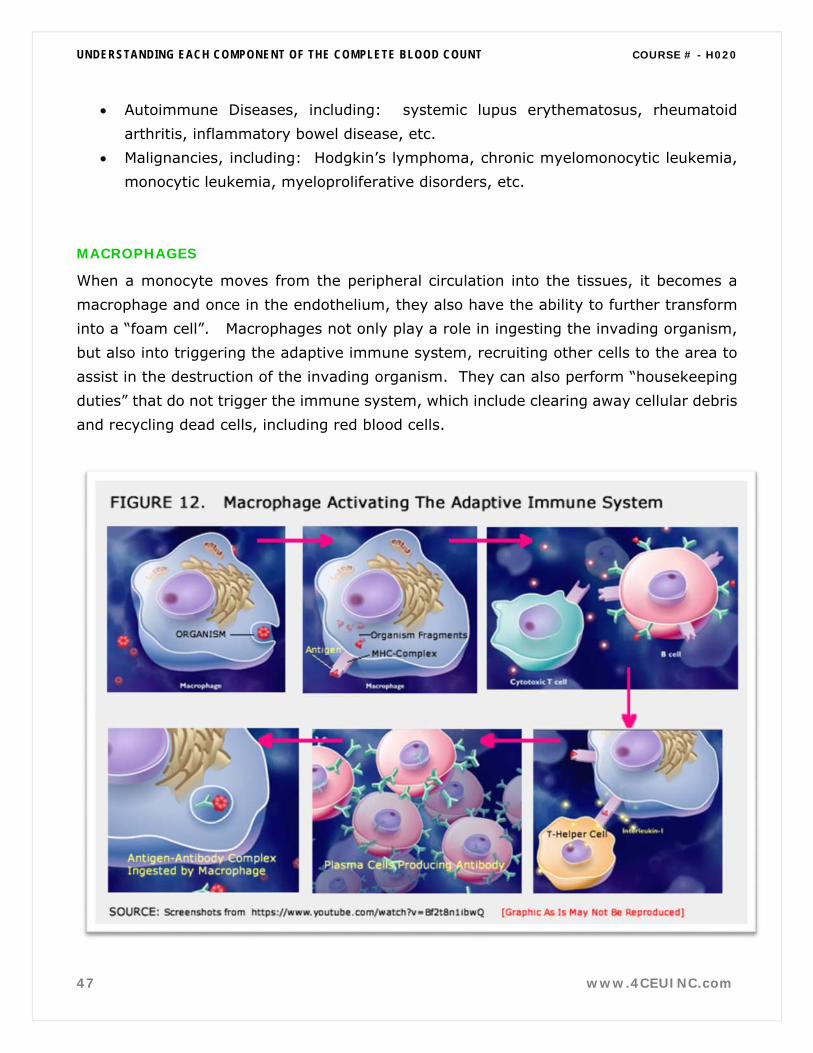
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
47 www.4CEUINC.com
Autoimmune Diseases, including: systemic lupus erythematosus, rheumatoid
arthritis, inflammatory bowel disease, etc. Malignancies, including: Hodgkin’s lymphoma, chronic myelomonocytic leukemia,
monocytic leukemia, myeloproliferative disorders, etc.
MACROPHAGES
When a monocyte moves from the peripheral circulation into the tissues, it becomes a macrophage and once in the endothelium, they also have the ability to further transform into a “foam cell”. Macrophages not only play a role in ingesting the invading organism, but also into triggering the adaptive immune system, recruiting other cells to the area to assist in the destruction of the invading organism. They can also perform “housekeeping duties” that do not trigger the immune system, which include clearing away cellular debris and recycling dead cells, including red blood cells.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
48 www.4CEUINC.com
Macrophages are essentially scavengers that ingest microorganisms (antigen) and disassemble them. Once the organism is ingested and broken apart, the macrophage presents the chemical makeup of that organism on its cell surface as an antigen for the body to remember during future attacks. Macrophages with antigen fragments displayed on their surfaces are called “antigen presenting cells”, which in turn interact with T-helper cells. During this interaction, the macrophage releases interleukin-1 to stimulate the T-helper cell to release interleukin-2, causing proliferation of certain cytotoxic T and B cells. Since each of the cytotoxic T cells recognize a certain antigen, it’s capable of linking to any infected cell in the body, destroying the cell and killing the pathogen. B cells also come in millions of different types that recognize an individual antigen, which when activated by a T-helper cell, differentiate into a plasma cell which floods the body with antibodies against the invading organism. Once that antibody links to the antigen, a macrophage will ingest the antigen antibody complex, removing it from the body. During this process, inflammation is normally produced on some level depending on the severity of infection.
PLATELETS
Platelets, also known as thrombocytes, are cells whose main function is to stop bleeding by binding together when a blood vessel is damaged.
Circulating platelets are actually cell fragments from the cytoplasm of a Megakaryocyte, which is normally found in the bone marrow. Circulating platelets are systematically fragmented off the edges of their peripheral cytoplasm and released into the circulation.
When a vessel is damaged platelets circulate to the injury site then go through several steps to form a clot. An overly simplified version of those steps are listed below:
Adhesion: Platelets attach to the surface around the injury site Activation: Platelets alter their shape to better adhere to the injury site and to one
another, they then turn on receptors, and secrete chemical messengers to signal other chemical processes.
Aggregation: Platelets adhere to one another and the surrounding tissue. The mass is held together with fibrin, forming a ‘platelet plug’.
Formation of the platelet plug sets the coagulation cascade into motion.
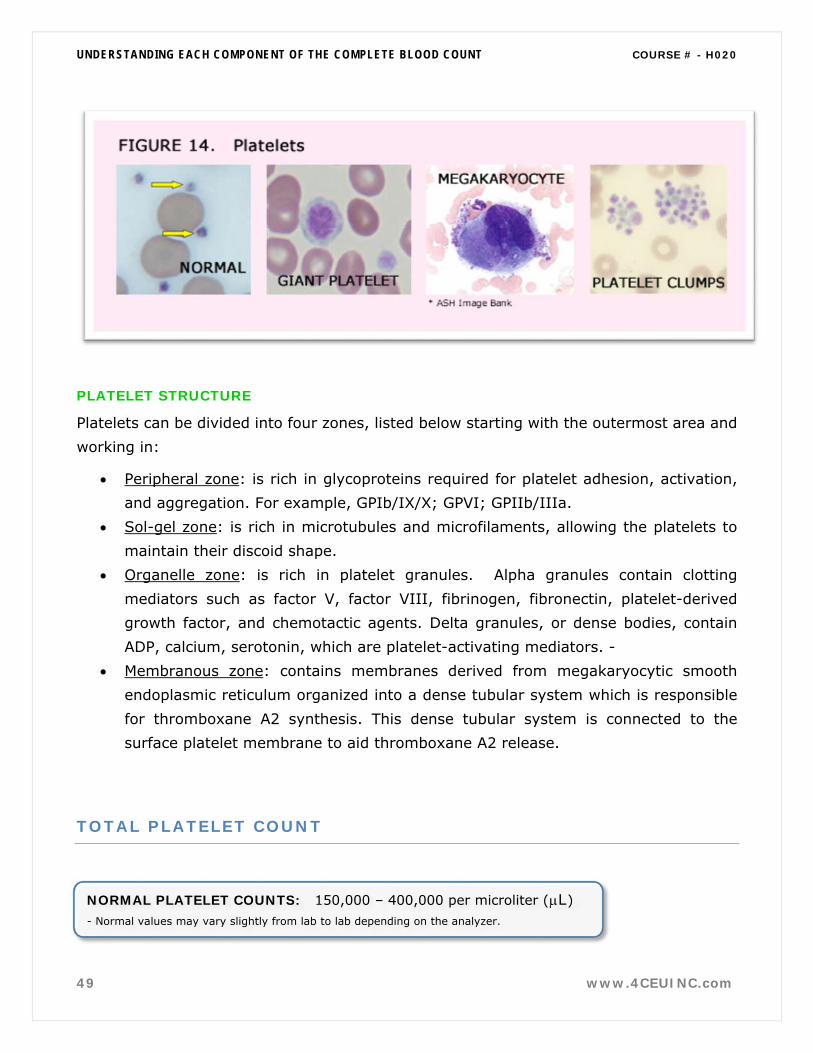
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
49 www.4CEUINC.com
PLATELET STRUCTURE
Platelets can be divided into four zones, listed below starting with the outermost area and working in:
Peripheral zone: is rich in glycoproteins required for platelet adhesion, activation, and aggregation. For example, GPIb/IX/X; GPVI; GPIIb/IIIa.
Sol-gel zone: is rich in microtubules and microfilaments, allowing the platelets to maintain their discoid shape.
Organelle zone: is rich in platelet granules. Alpha granules contain clotting mediators such as factor V, factor VIII, fibrinogen, fibronectin, platelet-derived growth factor, and chemotactic agents. Delta granules, or dense bodies, contain ADP, calcium, serotonin, which are platelet-activating mediators. -
Membranous zone: contains membranes derived from megakaryocytic smooth endoplasmic reticulum organized into a dense tubular system which is responsible for thromboxane A2 synthesis. This dense tubular system is connected to the surface platelet membrane to aid thromboxane A2 release.
TOTAL PLATELET COUNT
NORMAL PLATELET COUNTS: 150,000 – 400,000 per microliter ( L ) - Normal values may vary slightly from lab to lab depending on the analyzer.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
50 www.4CEUINC.com
Average Cell Size of Platelet: 1 – 3 µm (micrometers)
Average Lifespan: The average lifespan of a platelet is approximately 10 days.
Common Abbreviation or Nicknames: Platelet is abbreviated as “PLT”
Cellular Morphology on a Blood Smear:
Dark purple in color No nucleus Normally small, round, pinpoint cells Approximately 20% of the diameter of an RBC Normal ratio of platelets to RBCs is 1:10 to 1:20 in healthy adults
SCANNING A PERIPHERAL SMEAR
When peripheral smears are performed, they should be scanned for platelet characteristics, such as size, shape, number, clumping, satellitism, etc.
Platelet Estimates and Distribution
When a peripheral smear is viewed microscopically a platelet review should be performed, as noted above. With 8-10 fields scanned, a comment about the platelets should be made reporting them as normal, increased, or decreased or by some other suitable method used by your lab regarding quantity. When the size, shape, or color is abnormal, that should be noted also.
When a more accurate platelet estimate needs to be performed, you can use a formula that would calculate a more accurate result. Since there are multiple methods available for calculating a platelet estimate, you should familiarize yourself with what your lab uses.
Giant Platelets
Giant platelets, as shown above, are sometimes seen on a peripheral blood smear. They can indicate Bernard-Soulier syndrome, gray platelet syndrome, May-Hegglin anomaly, and post bleeding episodes when there is increased production. They are typically a rare phenomenon and may accompany thrombocytopenia and easy bleeding.
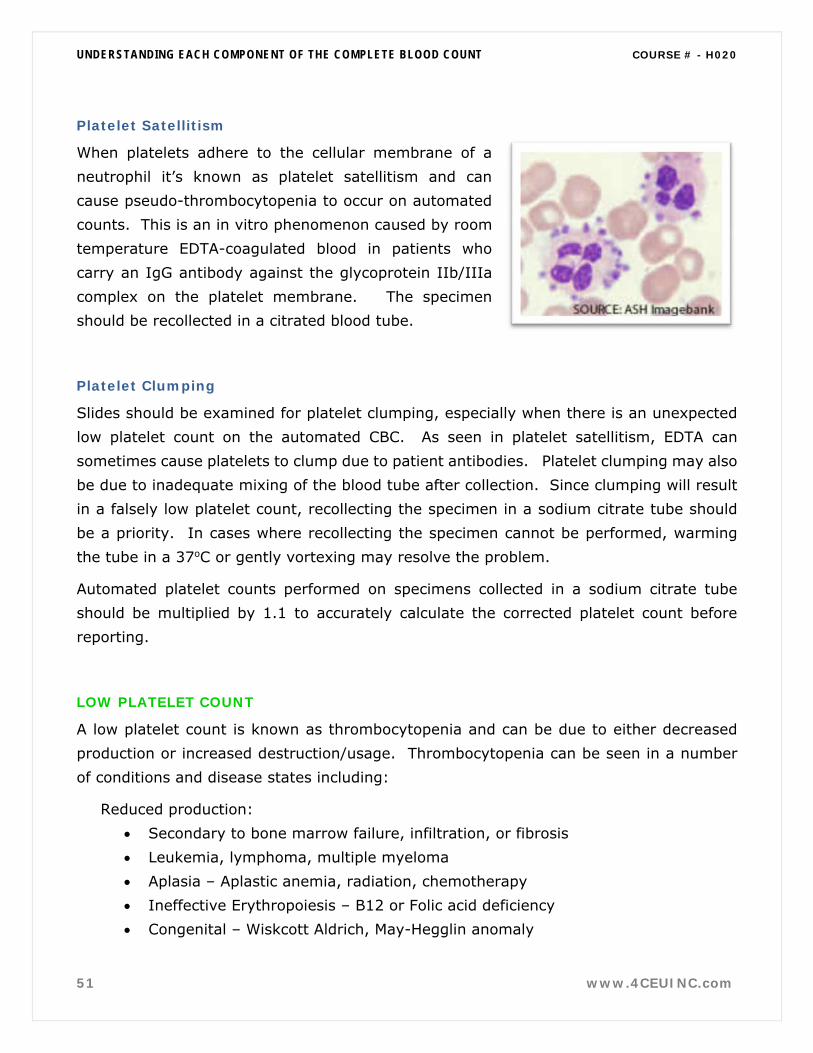
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
51 www.4CEUINC.com
Platelet Satellitism
When platelets adhere to the cellular membrane of a neutrophil it’s known as platelet satellitism and can cause pseudo-thrombocytopenia to occur on automated counts. This is an in vitro phenomenon caused by room temperature EDTA-coagulated blood in patients who carry an IgG antibody against the glycoprotein IIb/IIIa complex on the platelet membrane. The specimen should be recollected in a citrated blood tube.
Platelet Clumping
Slides should be examined for platelet clumping, especially when there is an unexpected low platelet count on the automated CBC. As seen in platelet satellitism, EDTA can sometimes cause platelets to clump due to patient antibodies. Platelet clumping may also be due to inadequate mixing of the blood tube after collection. Since clumping will result in a falsely low platelet count, recollecting the specimen in a sodium citrate tube should be a priority. In cases where recollecting the specimen cannot be performed, warming the tube in a 37oC or gently vortexing may resolve the problem.
Automated platelet counts performed on specimens collected in a sodium citrate tube should be multiplied by 1.1 to accurately calculate the corrected platelet count before reporting.
LOW PLATELET COUNT
A low platelet count is known as thrombocytopenia and can be due to either decreased production or increased destruction/usage. Thrombocytopenia can be seen in a number of conditions and disease states including:
Reduced production: Secondary to bone marrow failure, infiltration, or fibrosis Leukemia, lymphoma, multiple myeloma Aplasia – Aplastic anemia, radiation, chemotherapy Ineffective Erythropoiesis – B12 or Folic acid deficiency Congenital – Wiskcott Aldrich, May-Hegglin anomaly
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
52 www.4CEUINC.com
Increased Destruction:
Immune - o Idiopathic thrombocytopenia purpura (ITP) o Heparin induced thrombocytopenia (HIT) o Post-transfusion reaction o Viral illness
Nonimmune - o Hemorrhage o Increased consumption due to disseminated intravascular coagulation (DIC) o Hemolytic uremic syndrome (HUS) o Dilution – during large volume blood transfusions with little to no platelets o Mechanical destruction – caused by prosthetic heart valve o Drug induced – (most cause only a slight decrease) aspirin, chemotherapeutic
agents, Histamine-2 (H2) blocking agents, quinidine, sulfonamides, thiazide diuretics, etc.
Signs and Symptoms of Thrombocytopenia
Petechiae Easy bruising Nosebleeds Mild to moderate bleeding (depending on the thrombocytopenia severity) Excessive bleeding from superficial wounds
Treatment of Thrombocytopenia
Treatment of thrombocytopenia depends on the cause and the severity. The main goal is to prevent uncontrolled bleeding and/or death.
Mild Thrombocytopenia: If mildly decreased, treatment may not be necessary When medication is the cause, changing medication usually resolves the problem Medications – corticosteroids, immune modulators, immunoglobulins, eltombopag,
etc.
Severe Thrombocytopenia: Platelet transfusion Splenectomy
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
53 www.4CEUINC.com
ELEVATED PLATELET COUNT
An elevated platelet count is known as thrombocytosis and can be due to primary or secondary causes including:
Primary Thrombocytosis: Essential thrombocythemia (ET) Polycythemia vera Myeloproliferative disorders Chronic Myelogenous Leukemia (CML)
Secondary (Reactive) Thrombocytosis: Post-splenectomy Surgery Inflammation or infection Acute hemorrhage Cancer Living at high altitudes (may cause a slight increase)
Signs and Symptoms of Thrombocytosis
Most patients don’t experience any signs or symptoms Thrombosis (blood clot) – may lead to stroke, heart attack, etc. Bleeding may also occur Secondary thrombocytosis usually resolves once the underlying cause resolves
Thrombocytosis Treatment
Careful observation for asymptomatic patients Low dose aspirin for prevention of blood clots With essential thrombocythemia (ET) hydroxyurea or anagrelide can be used
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
54 www.4CEUINC.com
MPV
MPV is an abbreviation for “Mean Platelet Volume”. The MPV is a value that is calculated by an automated CBC analyzer and is a general measurement of the average platelet size. The MPV can be used by the physician to make determinations about platelet production or destruction in the patient.
MPV Calculation: MPV = PDW ÷ [Total platelet Count x 10]
CAUSES OF INCREASED MPV
The MPV is increased when the body is producing an increased numbers of platelets, usually secondary to platelet destruction or usage during activation.
It may be seen with disease states such as immune thrombocytic purpura (ITP), myeloproliferative diseases, Bernard-Soulier syndrome, etc. It was noted in some studies that MPV increased during storage, so changes may occur on blood that is not freshly collected.
CAUSES OF DECREASED MPV
Abnormally low MPV values primarily correlate with thrombocytopenia when it is due to impaired platelet production as in aplastic anemia.
PDW
PDW is an abbreviation for “Platelet Distribution Width” and is a measurement calculated by an automated CBC analyzer. The PDW gives the physician information on the variation in the size of the platelets, reflecting how uniform the size of the platelet population is. Like the RDW, it measures the size variation among the cells in the blood sample.
NORMAL MPV: 7 – 11 fL (femtoliter)
- Normal values may vary slightly from lab to lab depending on the analyzer. - Not all labs report this parameter.
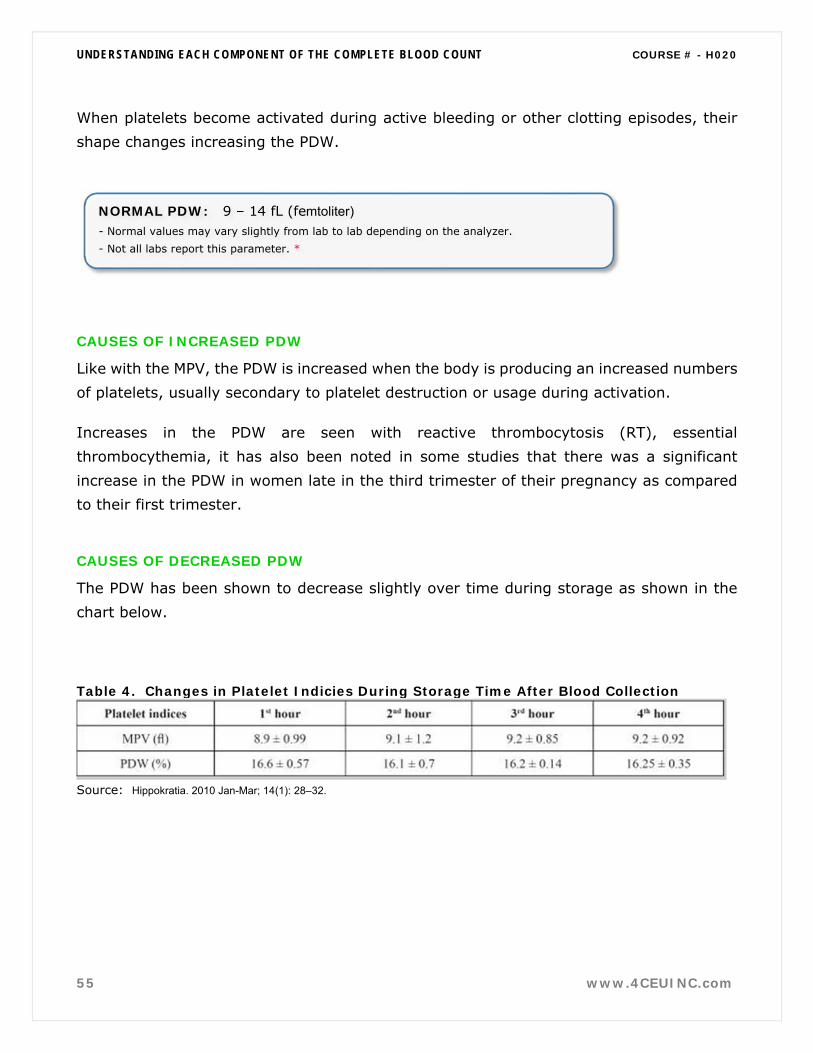
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
55 www.4CEUINC.com
When platelets become activated during active bleeding or other clotting episodes, their shape changes increasing the PDW.
CAUSES OF INCREASED PDW
Like with the MPV, the PDW is increased when the body is producing an increased numbers of platelets, usually secondary to platelet destruction or usage during activation.
Increases in the PDW are seen with reactive thrombocytosis (RT), essential thrombocythemia, it has also been noted in some studies that there was a significant increase in the PDW in women late in the third trimester of their pregnancy as compared to their first trimester.
CAUSES OF DECREASED PDW
The PDW has been shown to decrease slightly over time during storage as shown in the chart below.
Table 4. Changes in Platelet Indicies During Storage Time After Blood Collection
Source: Hippokratia. 2010 Jan-Mar; 14(1): 28–32.
NORMAL PDW: 9 – 14 fL (femtoliter)
- Normal values may vary slightly from lab to lab depending on the analyzer. - Not all labs report this parameter. *
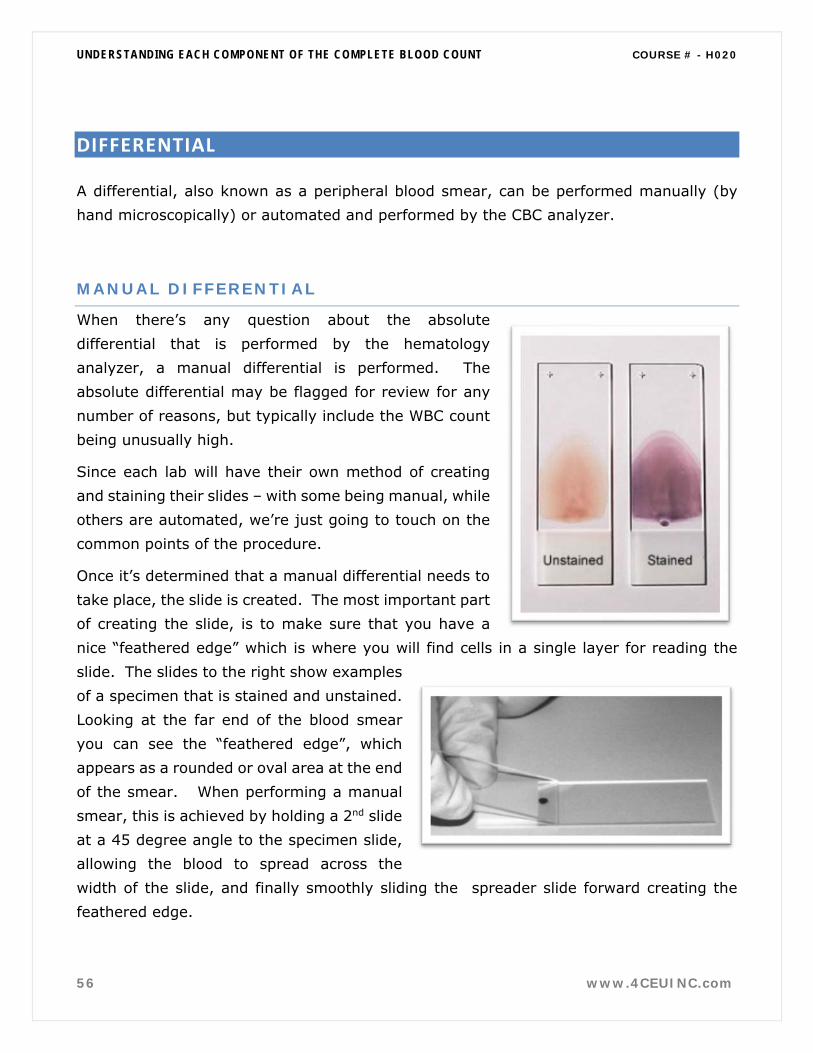
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
56 www.4CEUINC.com
DIFFERENTIAL A differential, also known as a peripheral blood smear, can be performed manually (by hand microscopically) or automated and performed by the CBC analyzer.
MANUAL DIFFERENTIAL
When there’s any question about the absolute differential that is performed by the hematology analyzer, a manual differential is performed. The absolute differential may be flagged for review for any number of reasons, but typically include the WBC count being unusually high.
Since each lab will have their own method of creating and staining their slides – with some being manual, while others are automated, we’re just going to touch on the common points of the procedure.
Once it’s determined that a manual differential needs to take place, the slide is created. The most important part of creating the slide, is to make sure that you have a nice “feathered edge” which is where you will find cells in a single layer for reading the slide. The slides to the right show examples of a specimen that is stained and unstained. Looking at the far end of the blood smear you can see the “feathered edge”, which appears as a rounded or oval area at the end of the smear. When performing a manual smear, this is achieved by holding a 2nd slide at a 45 degree angle to the specimen slide, allowing the blood to spread across the width of the slide, and finally smoothly sliding the spreader slide forward creating the feathered edge.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
57 www.4CEUINC.com
Staining of the peripheral blood smear is typically done using a Romanowsky, Wright's, or Giemsa stain; occasionally, other stains are also used. The stained blood smear is then analyzed under the microscope where the tech will scan the slide at a low power, then view cells in the “feathered edge” at a higher power, looking at the RBC morphology, and performing a 100 cell WBC count, and a platelet estimate. As the tech scans back and forth during the WBC count, the slide is observed for any abnormalities in cellular shape, size, inclusions, clumping, or other foreign matter (bacteria, parasites, etc) in the cells or surrounding material.
AUTOMATED DIFFERENTIAL
In today’s lab, most of the differentials are performed by the hematology analyzer. Exceptions to that rule would be any results that are flagged by the analyzer as abnormal, triggering a peripheral blood smear to be performed. Occasionally, physicians may also order a peripheral smear to be performed directly if they already know that the patient has a condition that may warrant visual inspection of the peripheral slide, such as iron deficiency anemia, malaria, cold agglutinins, NRBCs, etc.
Automated differentials are reported as both a percentage and as an absolute number.
UNDERSTANDING EACH COMPONENT OF THE COMPLETE BLOOD COUNT COURSE # - H020
58 www.4CEUINC.com
***THIS PAGE INTENTIONALLY LEFT BLANK***

![NAME SYNOPSIS −AdDeflLnNOpqRStuUvxX ][esj/cnt4504/reading/tcpdump.1.pdf · TCPDUMP(8) TCPDUMP(8) Algorithms may bedes-cbc, 3des-cbc, blowfish-cbc, rc3-cbc, cast128-cbc,ornone.The](https://img.pdfslide.us/doc/110x75/604e8bc7dec7c8115c72cbfe/name-synopsis-aaddeilnnopqrstuuvxx-esjcnt4504readingtcpdump1pdf-tcpdump8.jpg)



























