Embed Size (px)
Citation preview
hgdال
بسم هللا الرحمن الرحیم
In the name of ALLAH
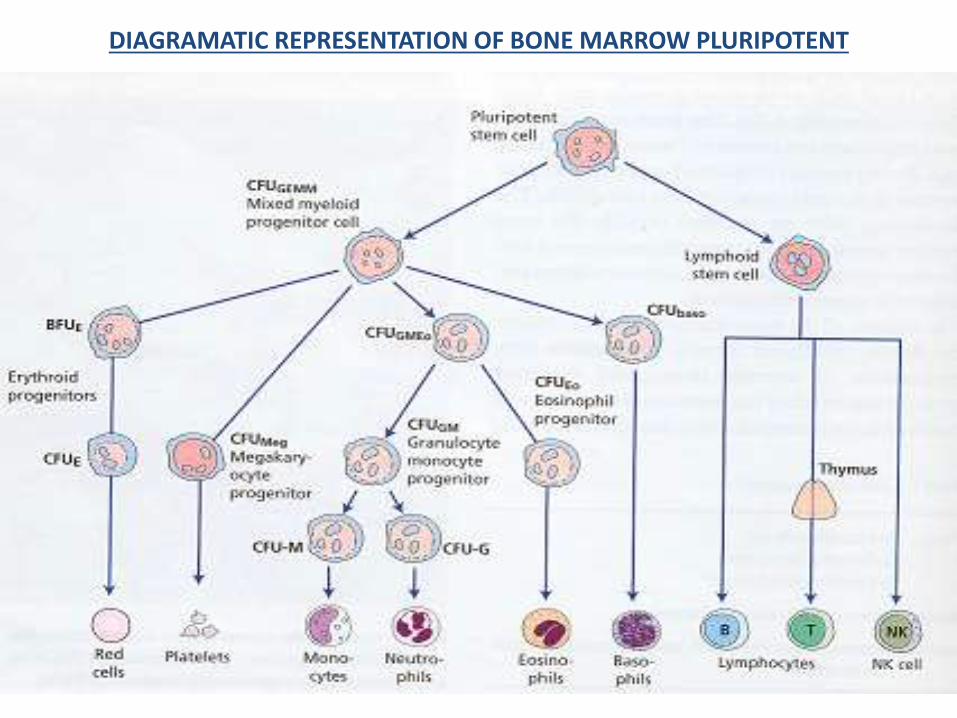
DIAGRAMATIC REPRESENTATION OF BONE MARROW PLURIPOTENT
PCV or Hematocrit
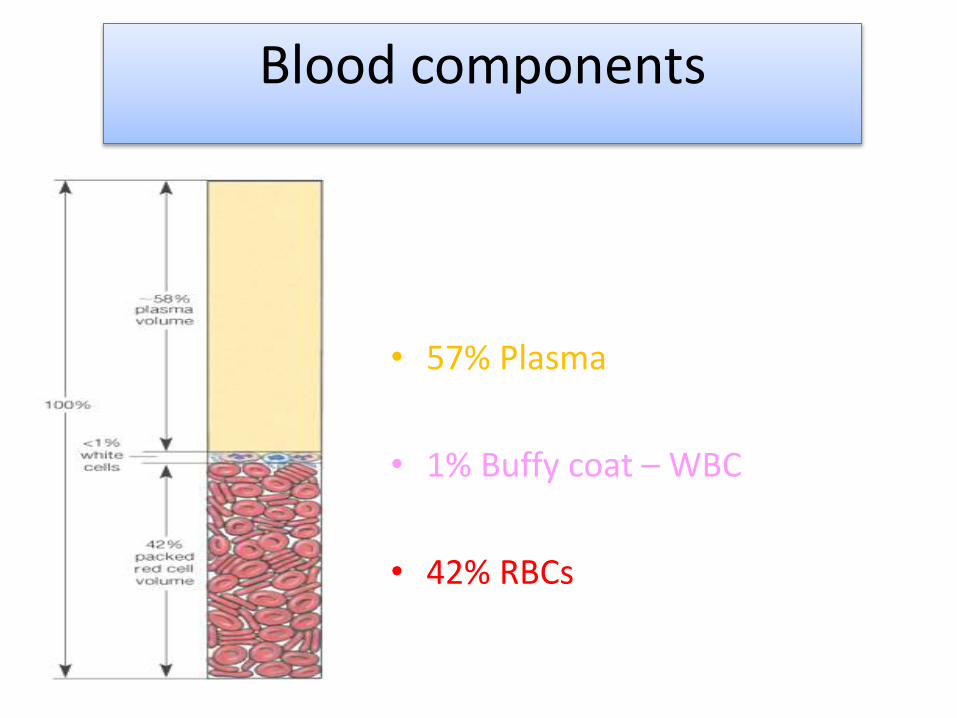
• 57% Plasma
• 1% Buffy coat – WBC
• 42% RBCs
Blood components
Interpretation of
CBC- complete blood count
Component of the CBC
White Blood Cells (WBCs)
Red Blood Cells (RBCs)
Hemoglobin (Hgb)
Hematocrit (Hct)
Mean Corpuscular Volume (MCV)
mean corpuscular hemoglobin(MCH)
Mean Corpuscular Hemoglobin Concentration (MCHC)
Red cell distribution width (RDW)
Platelet ( PLT )
• RBC (varies with altitude):
M: 4.7 to 6.1 x10^12 /L
F : 4.2 to 5.4 x10^12 /L
In : 4.8 to 7.1 x10^12 /L
• Function: - transport hemoglobin which carries oxygen from the lung to the tissues
-acid –base buffer.
(Hgb/Hb)
M: 14 to 18 g/dL
F : 12 to 16 g/dL
In: 14 to 24 g/dl
5>Hgb>20 Emergency
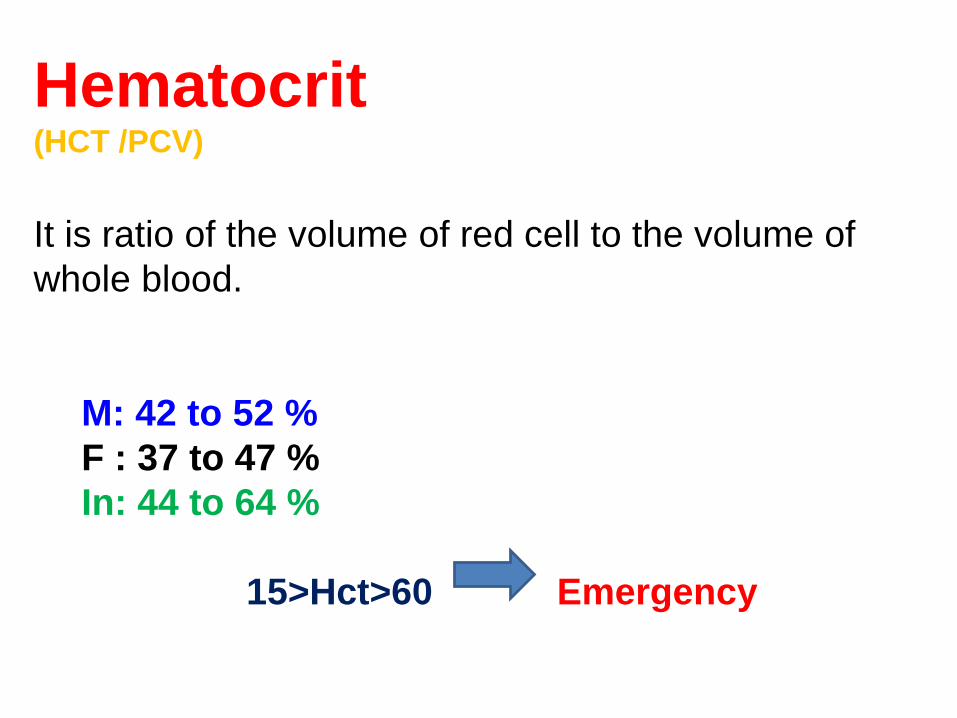
Hematocrit(HCT /PCV)
It is ratio of the volume of red cell to the volume of
whole blood.
M: 42 to 52 %
F : 37 to 47 %
In: 44 to 64 %
15>Hct>60 Emergency
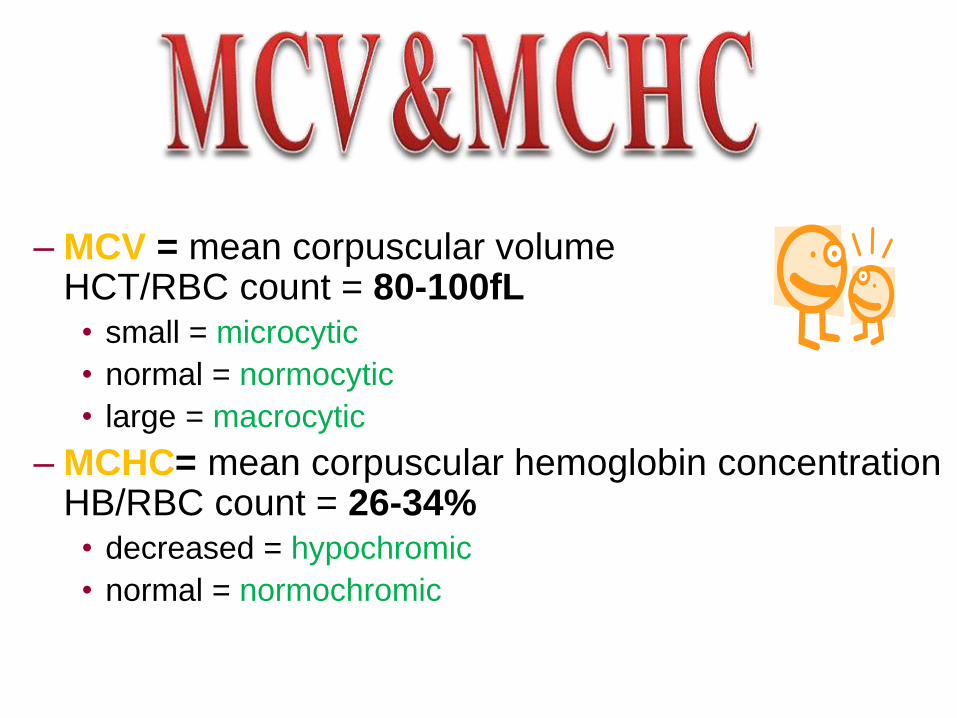
– MCV = mean corpuscular volume HCT/RBC count = 80-100fL• small = microcytic
• normal = normocytic
• large = macrocytic
– MCHC= mean corpuscular hemoglobin concentration HB/RBC count = 26-34%• decreased = hypochromic
• normal = normochromic
• MCH (mean corpuscular hemoglobin)
HB/HCT = 27-32 pg
• RDW (red cell distribution width)
• It is correlates with the degree of anisocytosis
_ Normal range from 10-15%
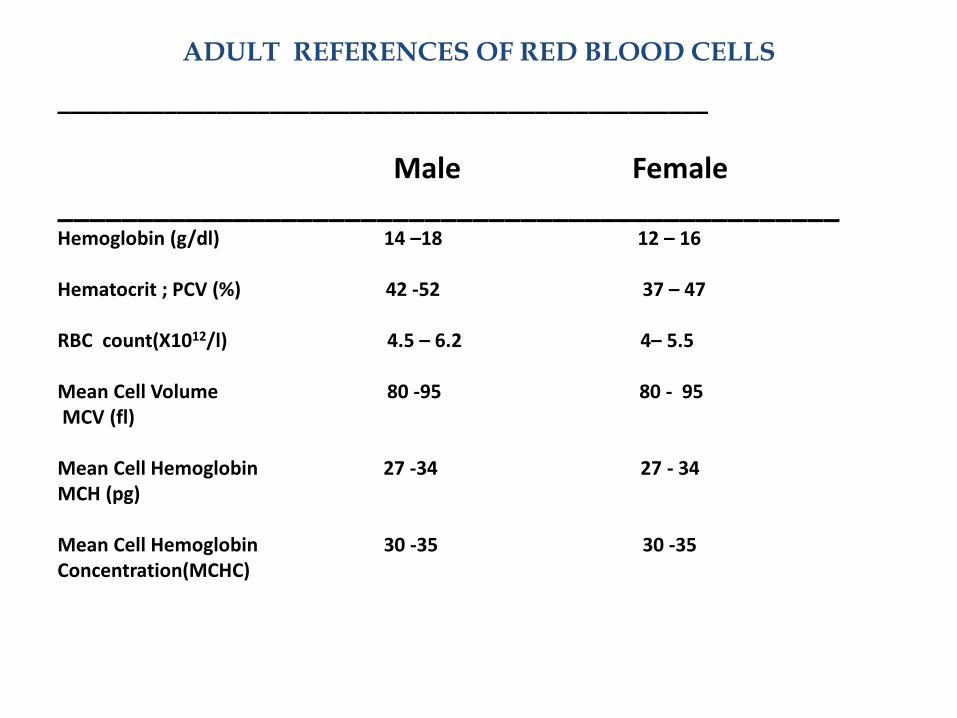
ADULT REFERENCES OF RED BLOOD CELLS
_________________________________________________
Male Female_________________________________________________Hemoglobin (g/dl) 14 –18 12 – 16
Hematocrit ; PCV (%) 42 -52 37 – 47
RBC count(X1012/l) 4.5 – 6.2 4– 5.5
Mean Cell Volume 80 -95 80 - 95MCV (fl)
Mean Cell Hemoglobin 27 -34 27 - 34MCH (pg)
Mean Cell Hemoglobin 30 -35 30 -35Concentration(MCHC)
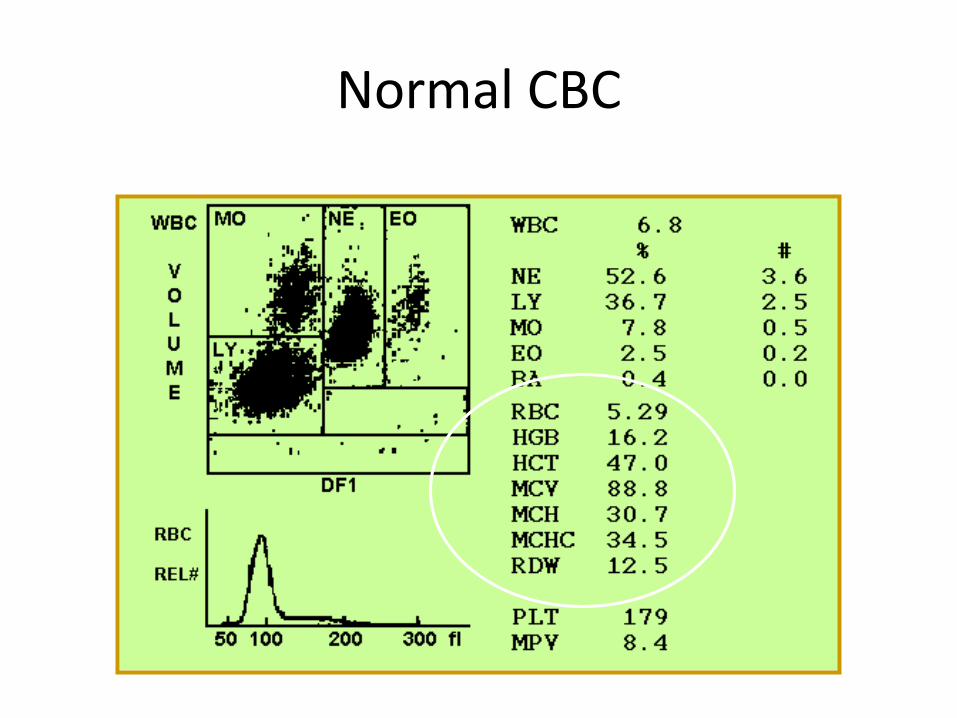
Normal CBC
RBC
Physiological responseHypoxiaPOLYCYTHEMIA VERAAcute dehydration
RBC
AnemiaHemorrhage.
nutritional deficiency Kidney diseaseLeukemia
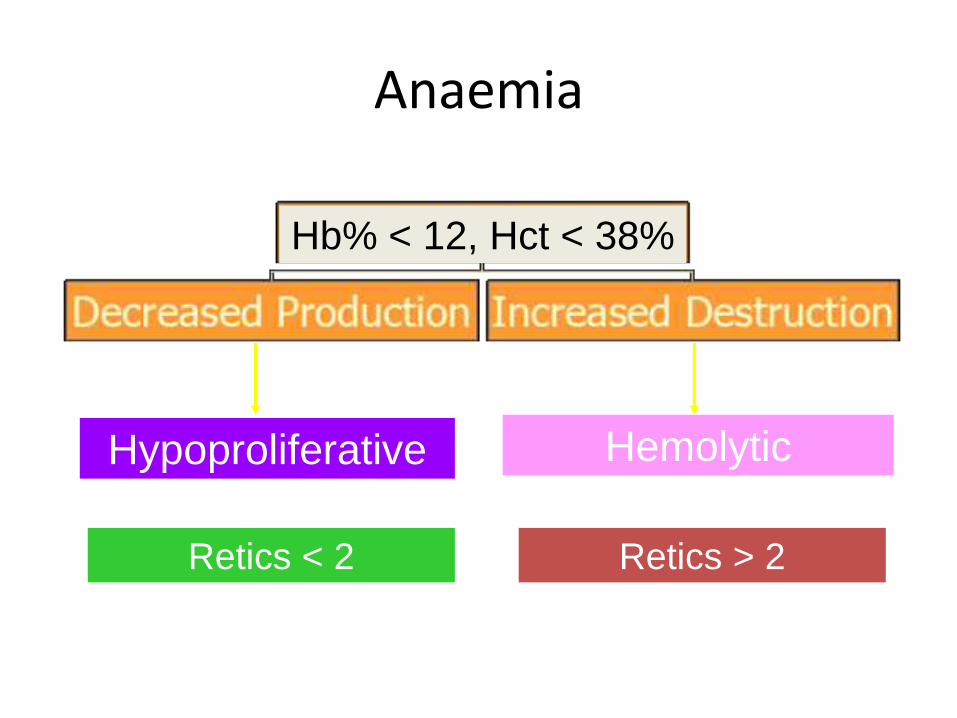
Anaemia
Hypoproliferative Hemolytic
Retics < 2 Retics > 2
Hb% < 12, Hct < 38%
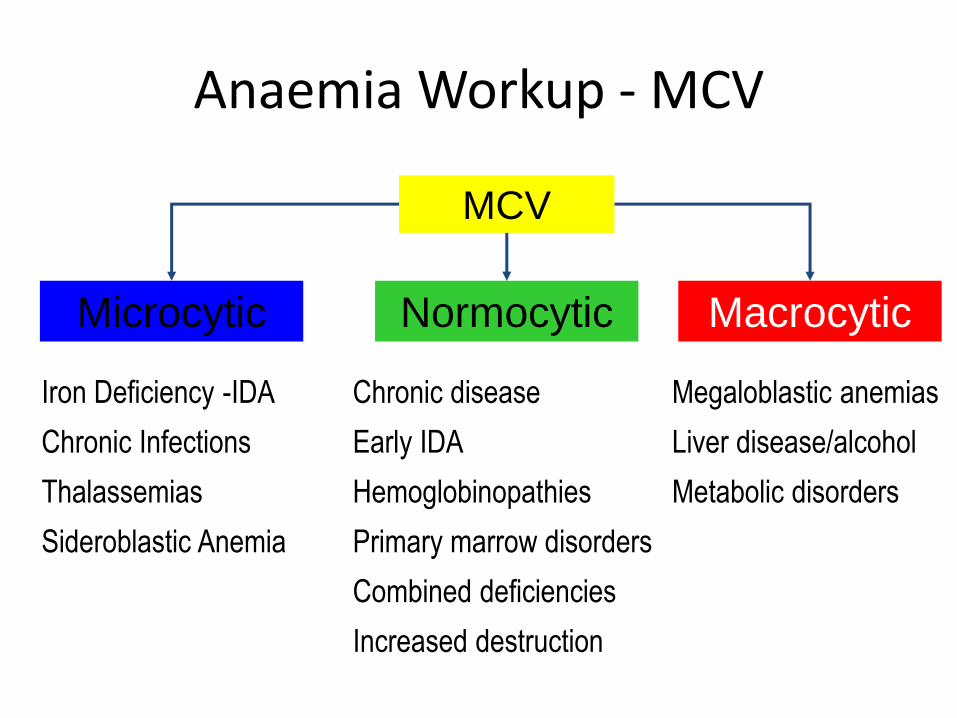
Anaemia Workup - MCV
Microcytic
MCV
Normocytic Macrocytic
Iron Deficiency -IDA
Chronic Infections
Thalassemias
Sideroblastic Anemia
Chronic disease
Early IDA
Hemoglobinopathies
Primary marrow disorders
Combined deficiencies
Increased destruction
Megaloblastic anemias
Liver disease/alcohol
Metabolic disorders
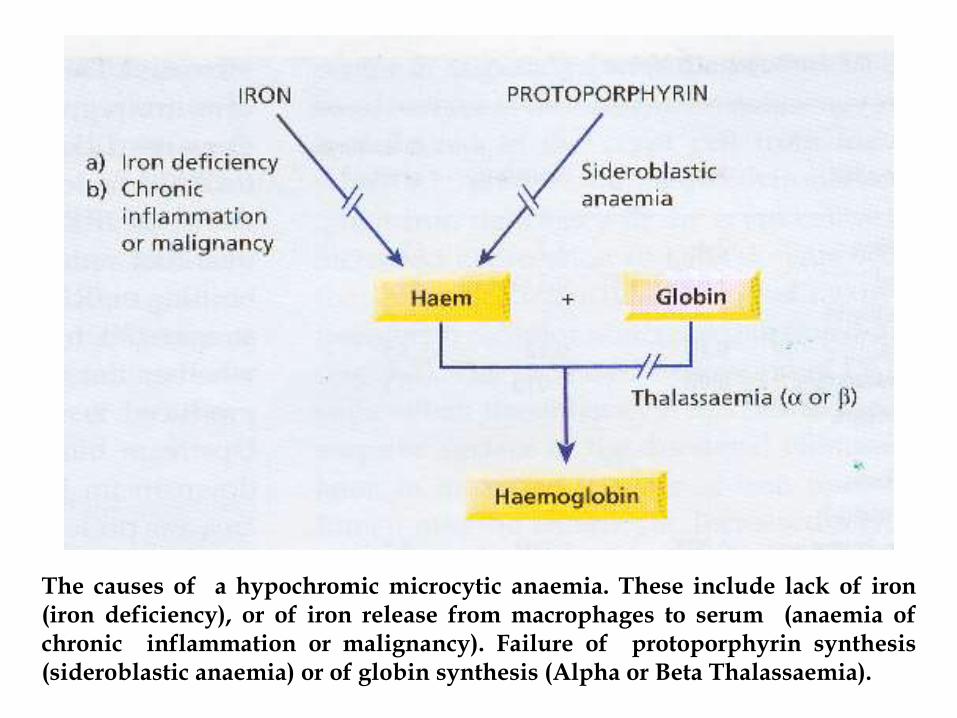
The causes of a hypochromic microcytic anaemia. These include lack of iron(iron deficiency), or of iron release from macrophages to serum (anaemia ofchronic inflammation or malignancy). Failure of protoporphyrin synthesis(sideroblastic anaemia) or of globin synthesis (Alpha or Beta Thalassaemia).
RDW
Megaloblastic anemias
IDA
Hemoglobinopathies
Hemolotic anemia
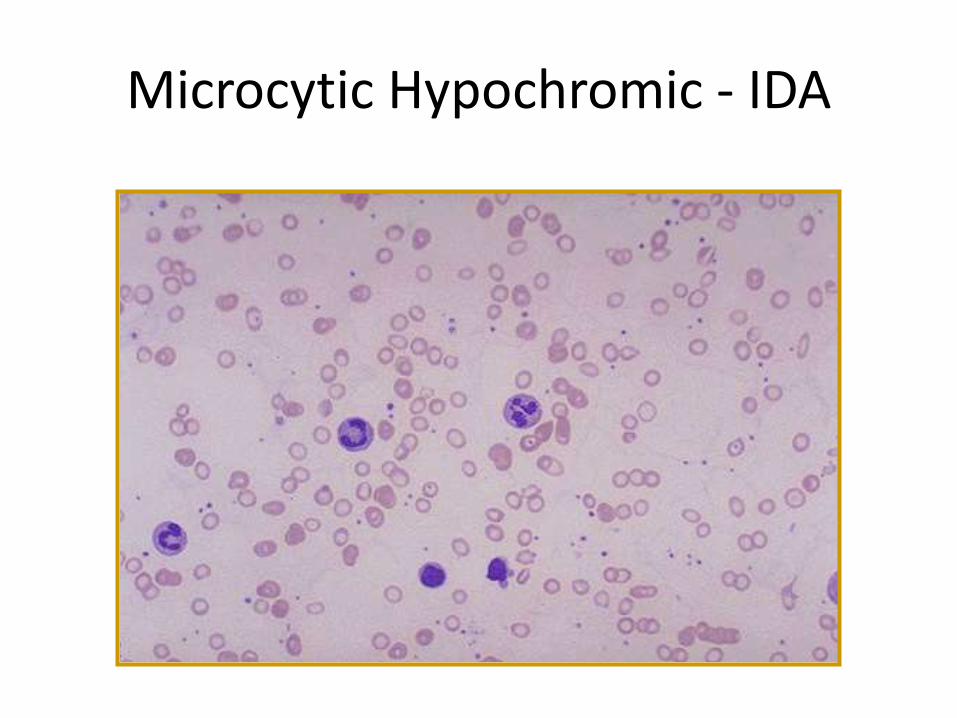
Microcytic Hypochromic - IDA
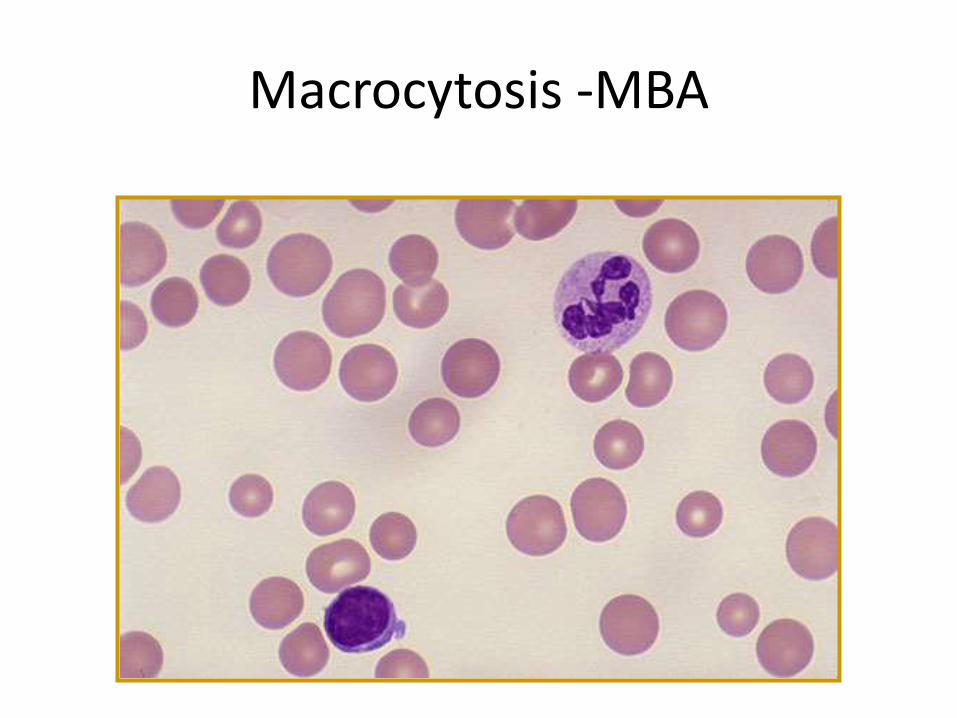
Macrocytosis -MBA

Norms of leukocytes(WBC)
30000<WBC<2500
Emergency
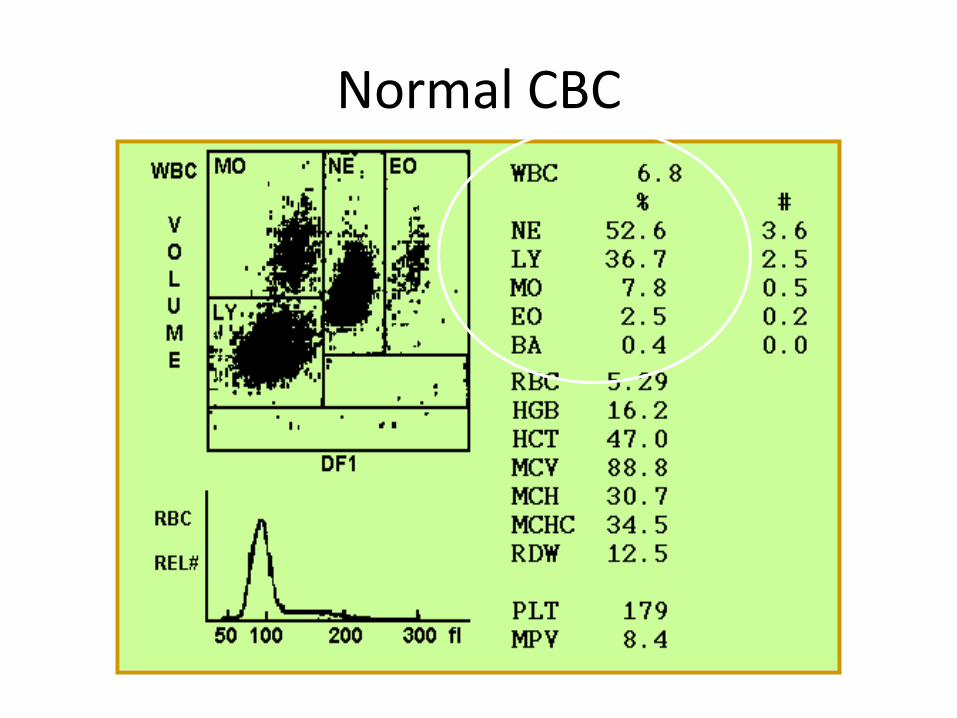
Normal CBC
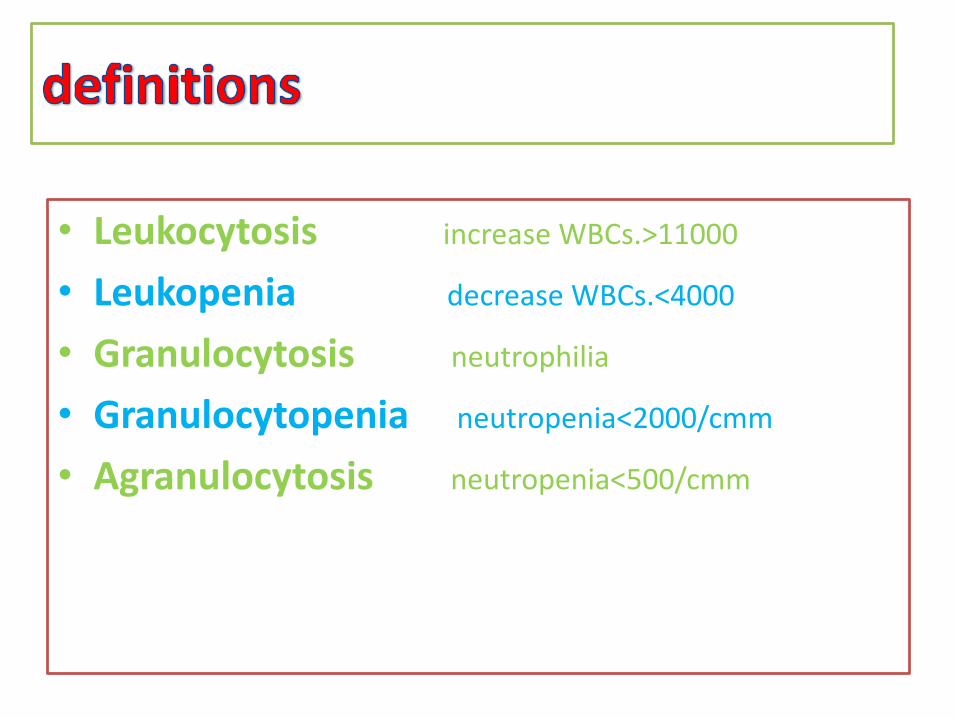
• Leukocytosis increase WBCs.>11000
• Leukopenia decrease WBCs.<4000
• Granulocytosis neutrophilia
• Granulocytopenia neutropenia<2000/cmm
• Agranulocytosis neutropenia<500/cmm
The type of cell affected depends upon its primary
function:
In bacterial infections, neutrophils are most
commonly affected
In viral infections, lymphocytes are most
commonly affected
In parasitic infections, eosinophils are most
commonly affected.
Abnormal result of WBC
Leukocytosis
_ Infectious diseases
_Inflammatory disease(such as RA &allergy)
_Leukemia
_Severe emotional or physical stress
_Tissue damage (e.g. necrosis,or burns)
Leukopenia:
Decreased WBC production from BM
Irradiation
Exposure to chemical or drugs
Autoimmune disease
Acute infection
• Function: Phagocytosis of bacteria
and cell debris
Neutrophilia
– Conditions associated with :
1-Bacterial infections (most common cause)
2-Tissue destruction
e.g. tissue infarctions, burns.
3- leukemoid reaction
4-Leukemia
Neutropenia
– this may result from:
1-Decreased bone marrow production
e.g. BM hypoplasia.
2-Ineffective bone marrow production
–E.g. megaloblastic anemias and
myelodysplastic syndromes.
3- post acute infection
_ e.g. typhoid fever, brucellosis.
• Function: Involved in allergy
, parasitic infections
Eosinophilia
may be found in
• Parasitic infections
• Allergic conditions and hypersensitivity
reaction
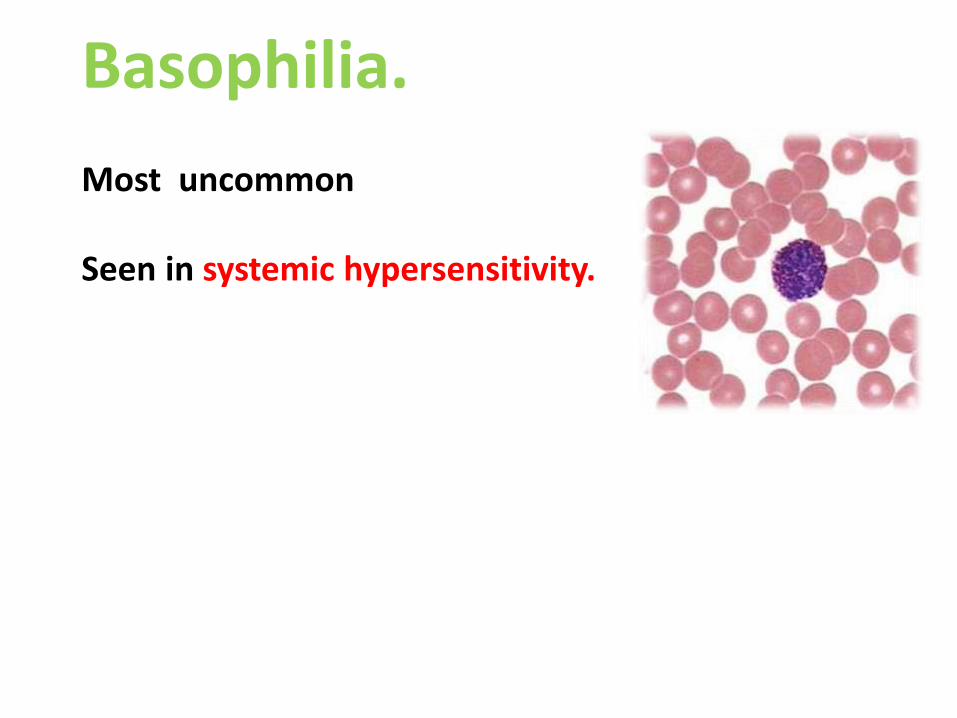
Basophilia.
Most uncommon
Seen in systemic hypersensitivity.
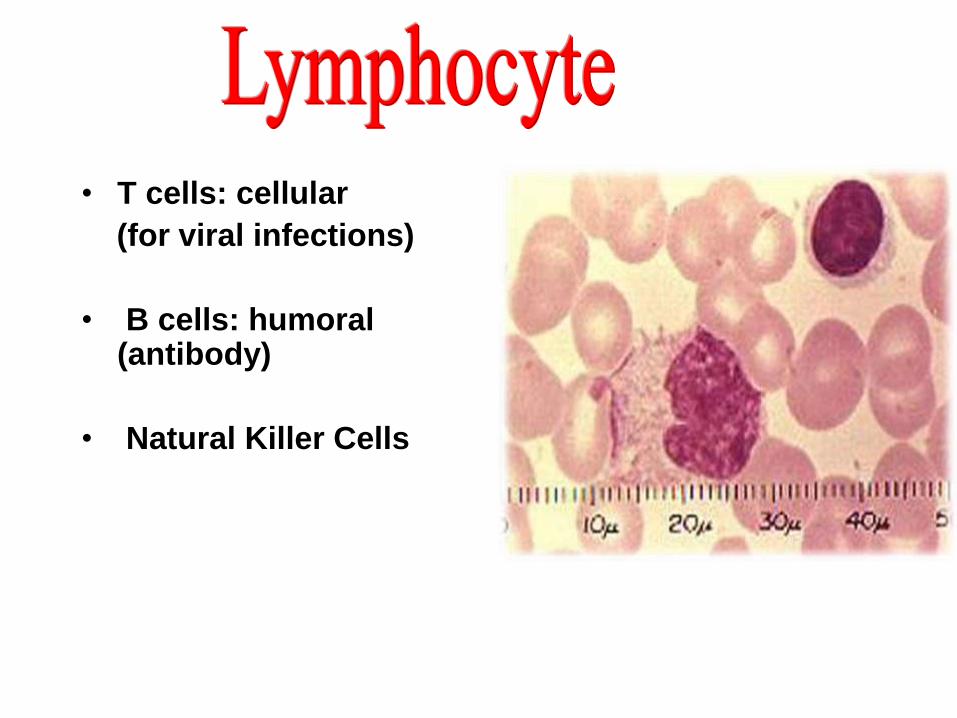
• T cells: cellular
(for viral infections)
• B cells: humoral(antibody)
• Natural Killer Cells
Lymphocytosis
_ Viral infection
e.g. Infectious mononucleosis, CMV or pertussis.
_ Bacterial infection
e.g. TB
Lymphopenia
_Stress
_Steroid therapy
_ Irradiation & immunodeficincy disease
•Normal range; 150-400x10^3 /mm3
•Destroyed by macrophage cells in
the spleen.
•Function; involved in coagulation and
blood haemostasis.
50000 >PLT>1x10^6 Emergency
Thrombocytosis• Exercise.
• High attitudes.
• Splenectomy
• RA
Thrombocytopenia• Hypersplenism
• Haemorrhage.
• Bone marrow destruction or suppression e.g. Leukemia
• DIC
• Anemia
• Petechial hemorhage.
• Easy bruising.
• Mucosal bleeding
e.g. _ epistaxes.
_ gum bleeding
PANCYTOPENIA
1. Aplastic Anaemia
2. Megloblastic Anaemia
3. Bone marrow infiltration by leukaemias, lymphomas, multiple myeloma etc.
4. Myelofibrosis
5. Hypersplenism( peripheral blood pancytopenia with normocellular or hypercellular marrow and splenomegaly)
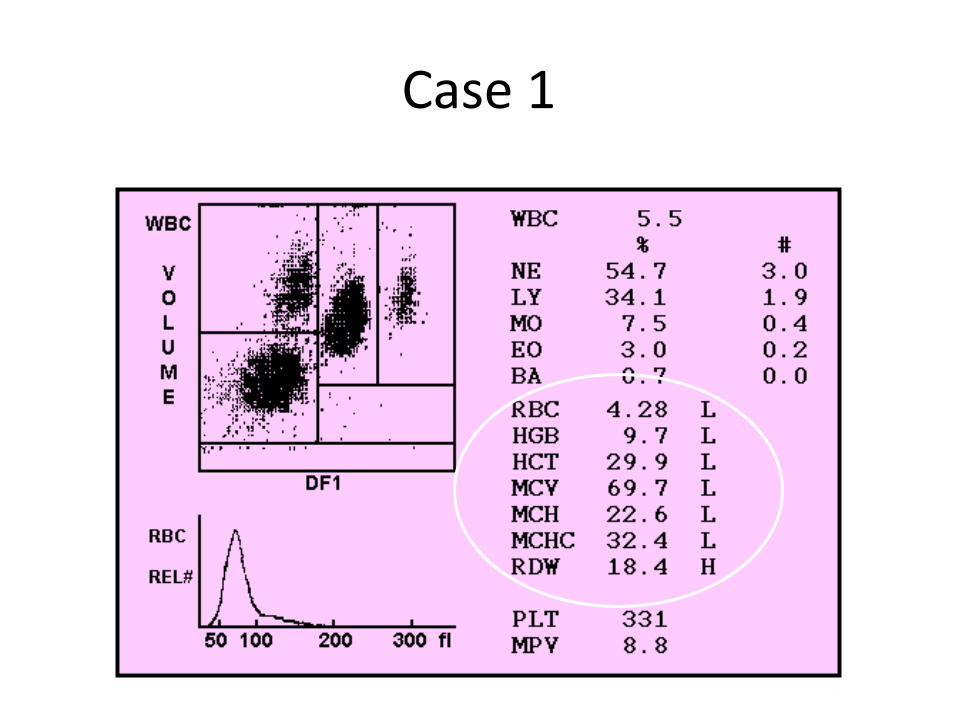
Case 1
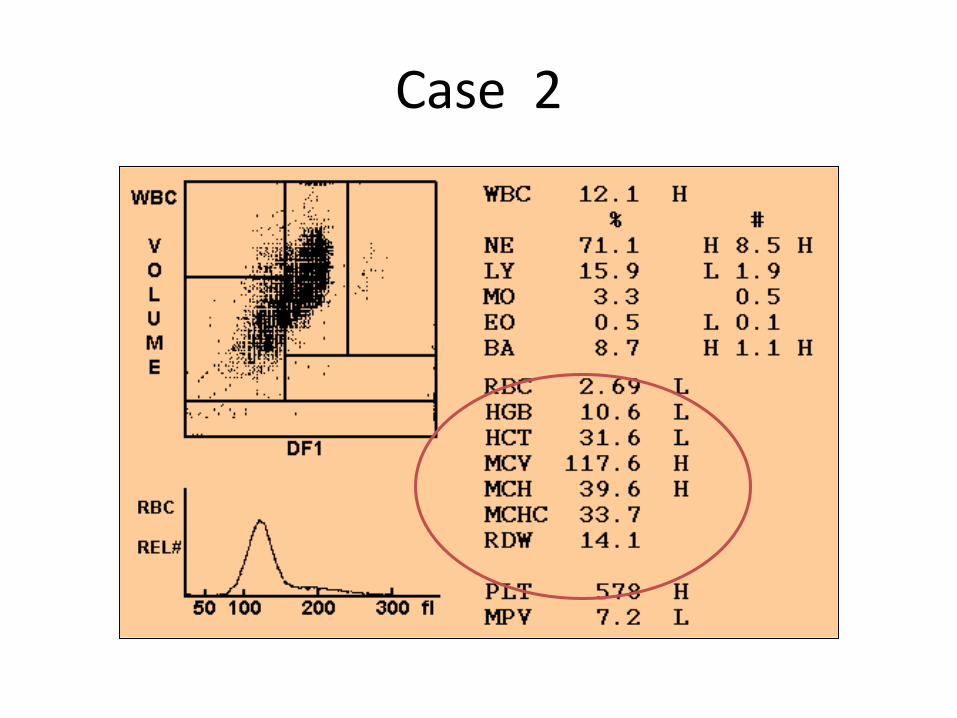
Case 2

Any Question ?
Tnx4 yrattention
Be happy





























