Embed Size (px)
Citation preview

Gut, 1992,33,246-251
Functional impairment ofnatural killer cells in activeulcerative colitis: reversion of the defective naturalkiller activity by interleukin 2
L Manzano, M Alvarez-Mon, L Abreu, J Antonio Vargas, E de la Morena, F Corugedo, ADur'antez
AbstractWe have studied the functional characteristicsand clinical importance of the natural killer(NK) cytotoxicity of peripheral blood mono-nuclear cells (PBMNC) from patients withulcerative colitis. Normal NK activity wasobserved in PBMNC from patients withinactive disease, but a pronounced decreasewas found in those with active disease. Clinicalchange from active to inactive disease wasassociated with enhancement of the depressedNK activity. The impairment of NK cyto-toxicity found in patients with active disesecould not be ascribed to a deficient number ofNK cells as the amounts of HNK-1+, CD16+(Leu 11), and CD11b (OKM1) cells in PBMNCwere within normal ranges. This defectivecytotoxic PBMNC activity was normalisedby short term (18 hour) incubation withrecombinant interleukin 2 (rIL-2). Moreover,long term (5 day) incubation of these effectorcells with rIL-2 induced strong cytotoxicactivity against NK resistant and NK sensitivetarget cells in patients with active and inactivedisease. We also found that both precursorsand effectors of cytotoxic activity promoted byshort term and long term incubation with rIL-2of PBMNC from the patients showed thephenotype ofNK cells (CD16+, CD3-). Takentogether, these results show that activeulcerative colitis is associated with a defectivefunction ofNK cells that is found to be normalin the inactive stage of the disease. Thepossible pathogenic and therapeutic impli-cations of these findings are discussed.
Natural killer (NK) cells are subpopulations ofin vivo activated lymphocytes that exert spon-taneous cytotoxic activity against tumoural andvirus infected cells in a major histocompatibilitycomplex (MHC) unrestricted fashion. A4 TheNK effectors are large granular lymphocytes thatcharacteristically express the CD 16 surfaceantigen. ' TheseNK cells have been implicated inimmunosurveillance against growth andhaematogenous spread of tumours and inresistance to viral and other microbialdiseases.'-S The cytotoxic activity ofNK cells canbe induced or enhanced by certain lymphokines,especially interleukin 2 (IL-2).$8 IL-2 can alsogenerate strong non-MHC restricted cytotoxicactivity, referred to as lymphokine activatedkiller (LAK) cytotoxicity,9"' in peripheral bloodmononuclear cells (PBMNC) after longterm (5
day) incubation. There is increasing evidencethat the precursors of this LAK cytotoxicity aremainly CD3-, CD16+ NK cells."2 1
Ulcerative colitis is a chronic systemicinflammatory disease affecting principally themucosa of the rectum and colon, with a clinicalevolution characterised by remissions andexacerbations. The aetiology of this diseaseremains unknown, but it has been suggested thatinfectious agents might be involved in theinduction of the colonic lesion.'" A possiblepathogenic role of the immune system has alsobeen proposed. 142021We have investigated the functional charac-
teristics and the clinical importance of the NKactivity ofPBMNC from patients with ulcerativecolitis.
Methods
PATIENT POPULATIONForty eight patients, 28 men and 20 women,mean (SD) age 40 (15) years, with ulcerativecolitis diagnosed clinically, radiologically, endo-scopically, and pathologically, were studied.Thirty one healthy, age and sex matched subjectswere used as control subjects. Disease activity ineach patient was analysed according to thecriteria of Truelove and Witts.22 Twenty fourpatients, 13 men and 11 women, aged 14-54years, had active disease (13 mild, 8 moderate, 3severe). There were 24 patients with inactivedisease, 15 men and nine women, aged 23-76years. When the experimental study wasperformed 14 patients had been taking steroidsplus sulphasalazine for at least three weeks. Atthe time of the study the remaining 34 patientshad not taken steroids for at least three months.Of these, 28 were taking sulphasalazine and sixwere receiving no specific treatment.
TABLE I Decreased NK cytotoxicity isfound in peripheralblood mononuclear cellsfrom patients with ulcerative colitis
Effector to target ratio
50:1 25:1 12:1
Patients 28 (17) 22 (15) 15 (13)Controls 48 (12) 36 (12) 27 (11)p value <0-01 <0-01 <0-01
Peripheral blood mononuclear cells from 48 patients and 31control subjects were used as effector cells in cytotoxic assaysagainst "Cr-labelled K-562 target cells at the indicated effector totarget ratio. The results are expressed as the mean (SD) specificlysis in experiments performed in triplicate in the two groups ofsubjects.
Service of InternalMedicine I and Service ofGastroenterology,Clinica Puerta de Hierro,Universidad Autonomade Madrid; Service ofInternal Medicine,Department of Medicine,Hospital UniversitarioPrmncipe de Asturias,Universidad de Alcala deHenares, Madrid, SpainL ManzanoM Alvarez-MonL AbreuJ Antonio VargasE de la MorenaF CorugedoA DurintezCorrespondence to:Professor Melchor Alvarez-Mon, Departamento deMedicina, Carretera Madrid-Barcelona, km 33,600,Universidad de Alcali deHenares, 28871 Alcala deHenares, Madrid, Spain.Accepted for publication7 May 1991
246

Functional impairment ofnatural killer cells in active ulcerative colitis
ISOLATION OF LYMPHOID CELLSPeripheral blood mononuclear cells wereobtained from the heparinised venous blood ofthe subjects by Ficoll-Hypaque gradient centri-fugation. They were washed twice in phosphatebuffered saline (0-15 mol/l, pH 7-2), counted,and resuspended in complete medium. Whereindicated, PBMNC were treated with anti-CD3or anti-CD 16 monoclonal antibodies plus rabbitcomplement (Behringwerke AG, Marburg,Germany) as previously described.23 ThesePBMNC lacked surface expression of CD3 orCD16 antigens (<I%), as quantitated by indirectfluorescence and flow cytometry.
1 50-
._
.2t._(D 40-U)
30 -
20
10
.
00
0
0
0
0
0
0
so
I.
060
so
0
0
0
0
0
0
000
000ooo
0
0
0
0
0
0
0000
0
0
00
00000000
0
0
00
00
80
0
Active Inactive ControlsPatients
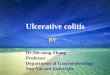
Figure 1: Ulcerative colitis patients with active, but not inactive, disease show impairedNKcytotoxicity in PBMNC. PBMNCfrom patients with active (24) and inactive (24) diseaseandfrom control subjects (31) were used as effector cells against "Cr-labelled K-562 target cells.Closed circles represent patients taking steroids. Each symbol indicates the mean specific lysis oftriplicate cytotoxic assays performed at a 50:1 effector to target ratio for an individual in eachgroup.
REAGENTSHuman recombinant interleukin 2 (rIL-2) wasprovided by Dr J Farrar and Dr P Sorter(Hoffman-La Roche, Nutley, NJ). Anti-CD16(Leu 11) and Leu 7 monoclonal antibodies wereobtained from Becton-Dickinson (MountainView, CA). Anti-CD lb (OKM1) was purchasedfrom Ortho (Raritan, NJ) and anti-CD3 mono-clonal antibody STV-T3b was kindly providedby Dr De Vries (University Hospital, Leiden,The Netherlands).
CULTURE MEDIUMRPMI 1640 (Gibco, Paisley, UK) supplementedwith 1% L-glutamine (Flow Lab, Irvine, UK),0 5% HEPES (Flow Lab), and 1% penicillin-streptomycin (Difco Lab, Detroit, MI) was usedfor cultures. This will be referred to as completemedium.
CELL CULTURESPBMNC (2 x106 cells/ml) were set up in 24macrowell plates (Costar, Cambridge, MA) incomplete medium supplemented with 10% fetalcalfserum (Gibco, Glasgow, UK), in the presenceor absence of different concentrations of IL-2.The cultures were carried out for 18 hours or 5days at 37°C in 5% CO2 humid atmosphere. Theincubated cells were washed twice in completemedium and used as effector cells in the cyto-toxicity assays.
CYTOTOXICITY ASSAYSCytotoxicity was quantified by a "Cr-specificrelease assay using the K-562, JY, Molt-4, P815,and LGL lines as target cells, as previouslydescribed.24 The different effector cells usedwere resuspended in complete mediumsupplemented with 10% heat inactivated fetalcalf serum. Target cells were labelled byincubating 2 to 3 x 106 cells with 150 [tCi of "Crfor 90 minutes at 37°C, washed twice, andresuspended in complete medium, sup-plemented with 10% fetal calf serum, at aconcentration of 5x 106 cells/ml. Then 5 x 10'target cells (0- 1 ml) were mixed with effectorcells (0- 1 ml) at different effector/target ratios(50/1, 25/1, 12/1, and 6/1) in triplicate round-bottom microwell plates (Linbro, Hamden,CT). Controls included targets incubated eitherwith complete medium supplemented with 10%fetal calf serum (spontaneous release) or withdetergent (total release). Plates were incubatedfor four hours at 37°C in a 5% CO2 atmosphere;0-1 ml from each well was collected and countedin a gammacounter. The percentages of specificcytotoxicity were calculated as follows:
A-SASx 100
T-Swhere A=mean cpm of test samples, S=meancpm of spontaneous release, and T=mean cpmof total release. In all the experiments included,the mean cpm of spontaneous release was alwaysless than 12% of the mean cpm of total release.
QUANTITATIVE FLOW CYTOMETRIC STUDYCells were incubated with the specific antibodies,followed by subsequent incubation with a secondfluorescein isothiocyanate coupled reagent(Kallestad, Austin, TX), as described else-where.2' The procedure was performed at 4°C in
80
70
60
0
00
0
247

Manzano, Alvarez-Mon, Abreu, Antonio Vargas, de la Morena, Corugedo, Durdntez
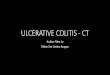
Figure 2: rIL-2 restores theNK cytotoxicity inPBMNCfrom patients withactive ulcerative colitis.2x 106 PBMNC/mlfrom 17patients - nine active andeight inactive - and 11control subjects wereincubated in the presence ofthe indicated amounts ofrIL-2 for 18 hours. Thesecultured cells were used aseffectors against 5"Cr-labelled K-562 target cells.Results represent the mean(SD) ofspecific lysis intriplicate cytotoxic assaysperformed at a 50:1 effectorto target ratio in the differentgroups studied.
1001
80-
.,_
.(A
0.
U)
60-
40-
20-
0-
* Active ulcerative colitis (n = 9)
m Inactive ulcerative colitis (n = 8)
aJControl subjects (n = 1 1)
I I
IBasal
Interleukin 2 (lU/mi)18 hours after incubation
the presence of 0-01% sodium azide. Surfaceimmunofluorescence was quantified using anEPICS-C flow cytometer (Coulter) equippedwith a 2 W Argon-laser tuned at the 488-nmline.
STATISTICAL METHODSThe data from the groups were compared usingthe unpaired Mann-Whitney U test. A p value ofless than 0 05 was considered to indicate asignificant difference.
Results
PATIENTS WITH ACTIVE ULCERATIVE COLITIS HAVEQUANTITATIVELY NORMAL BUT FUNCTIONALLYDEFECTIVE NK CELLS IN PBMNCFirst, the NK cytotoxic activity ofPBMNC frompatients with ulcerative colitis was analysed. AsTable I illustrates, PBMNC from these patientsshow a clearly impaired NK cytotoxicity whencompared with those of healthy control subjects(p<001). Next, we investigated separately theNK activity of PBMNC from ulcerative colitispatients with active and inactive disease. Impair-ment of cytotoxic activity was evident in patientswith active disease, being significantly depressedcompared with both patients with inactive diseaseand healthy control subjects (p<001) (Fig 1).However, there were no significant differencesin theNK activity ofPBMNC from patients withinactive disease when compared with healthycontrols (p>005). Interestingly, the NK cyto-toxicity of PBMNC from patients with activeulcerative colitis who were taking steroids over-lapped with that of patients who were not(p>005).We also investigated the possible variations in
NK activity occurring in PBMNC from ulcer-
ative colitis patients who progress from active toinactive disease. The depressed NK activityfound in PBMNC from patients with activedisease (mean (SD) 11 (4)% of specific lysis at a50:1 effector to target cell ratio in six patients)was significantly enhanced (p<001) when thedisease became inactive (30 (6))% of specific lysisat a 50:1 effector to target cell ratio). Thisincrease inNK cytotoxicity was also found in oneinactive patient who remained on steroid treat-ment (data not shown).
Quantitative flow cytometry studies wereperformed simultaneously to ascertain thenumber of phenotypically defined NK cells(Table II). The percentages of CD16+ andHNK-1+ cells were similar in PBMNC samplesfrom patients with either low or normal NKcytotoxic levels and from healthy controlsubjects (p>005). The numbers of cells bearingCD1lb, a surface heterodimer shared by NKcells and monocytic lineages, were also similar inthe three groups of subjects (p>005). Con-sequently, patients with active ulcerative colitishad quantitatively normal but functionallydefective NK cells in PBMNC.
IL-2 NORMALISES THE IMPAIRED FUNCTIONALACTIVITY OF NK CELLSIt has been shown that short term incubationwith IL-2 can enhance the cytotoxic activity ofnormal NK cells. Along these lines, we tested theeffect of titrated amounts of rIL-2 on the NKcytotoxicity of PBMNC from patients after 18hours ofincubation. In a dose dependent manner,IL-2 enhanced the NK activity of patients withinactive disease and also increased andnormalised the defective NK activity of patientswith active disease (Fig 2).
It could be argued that the cytotoxicitypromoted by rIL-2 against K-562 found in
248

Functional impairment ofnatural killer cells in active ulcerative colitis
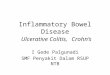
Figure 3: Longtermincubation with rIL-2induces strong lytic activityin PBMNC from ulcerativecolitis patients. 2 x I0^PBMNClmlfrom 17patients - nine active andeight inactive - and 11control subjects wereincubated in the presence ofthe indicated amounts ofrIL-2 for 5 days and used aseffectors against "Cr-labelled K-562. Thecolumns represent the mean(SD) ofspecific lysis at a50:1 effector to target ratio inthe different groups studied.
100 -
90 -
80 -
70 -
C,,0-0-
._
ij
0.
(I)UQ
60 -
50 -
40 -
30 -
20 -
10 -
0-
* Active ulcerative colitis (n = 9)
B Inactive ulcerative colitis (n = 8
L Control subjects (n = 1 1)
I T
I
Interleukin 2 (lU/mI)5 days after incubation
PBMNC from ulcerative colitis patients is medi-ated by lymphocytes other than NK cells. Toinvestigate whether precursor and effector cellsin the IL-2-promoted cytotoxicity belong to NKlineage, PBMNC were selected by means ofCD16 or CD3 monoclonal antibodies and
complement, and tested by cytotoxic assay.Depletion of CD16+ NK cells, but no CD3+ Tlymphocytes, abrogated the lytic activity at bothprecursor and effector levels in PBMNC frompatients with active and inactive disease (TableIII).
Jy
A2iz2izi50 12
Effector:target ratio
P815
50 12
LGL
2z.uz.izS.50 12
Figure 4: Non-MHC restricted cytotoxicity against bothNK sensitive andNK resistant target cells (LAK activity) is promoted in PBMNCfrom ulcerative colitispatients by longterm incubation with rIL-2. In basal conditions (open symbols) or after incubation with 100 IUlml rIL-2 (closed symbols) forfive days, PBMNCfrom ulcerative colitis patients (A) or control subjects (0) were used as effector cells against different "Cr-labelledNK sensitive and NK resistant target cells.Results represent the mean specific lysis in triplicate cytotoxicity assays performed at a 50:1 effector to target ratio with the different targets studied. A representativeexperiment of the three performed in patients with active disease is shown.
1is\\z---I
100
80
70
60
50
40
.-
.,_
C.,.2a)LO
30
20
10
50 12 50 12II.- .-r
249
3)

Manzano, Alvarez-Mon, Abreu, Antonio Vargas, de la Morena, Corugedo, Durdntez
TABLE II Impaired NK activity in patients with ulcerativecolitis does not correlate with reduced numbers ofphenotypically definedNK cells
HNK-I CD16 CDIlb
Patients 21(5) 14(3) 34 (6)Active 19 (5) 12 (3) 31(7)Inactive 23 (4) 15 (4) 37 (6)Controls 18 (4) 13 (5) 36 (4)
Peripheral blood mononuclear cells from 37 ulcerative colitispatients with active (19) or inactive (18) disease and 25 controlsubjects were studied by indirect immunofluorescence with Leu 7(HNK1), Leu 11 (CD16), and OKM1 (CD1 lb) monoclonalantibodies, and a second step fluoresceinated reagent, as indicatedin Methods. The table gives the percentage of cells staining abovethe second step reagent background as quantitated by an EPICS-Cflow cytometer. The data are the mean (SD) ofeach group studied.
TABLE III The precursor and effector lymphocytes oftheNKpromoted cytotoxicity in peripheral blood mononuclear cells(PBMNC)from patients with ulcerative colitis are CD3CD16' NKcells
Patients
ControlActive Inactive subjects
PBMNC (a) 60 68 65Precursor cells (b)CD3-, CD16' 68 72 70CD3', CD16 12 14 10
Effector cells (c)CD3-, CD16' 72 75 72CD3', CD16 8 10 12
PBMNC from three patients with active disease and threepatients with inactive disease and three control subjects were leftuntreated (a) or were treated with anti-CD3 (CD3 -, CD16') oranti-CD16 (CD3+, CD16-) monoclonal antibodies pluscomplement (b). 2x 106 cells/ml were incubated in the presence of100 IU/ml rIL-2 for 18 hours. At the end of the culture period,aliquots of untreated PBMNC were treated with anti-CD3 (CD3-CD16+) or anti-CD16 (CD3+, CD16-) monoclonal antibodiesplus complement (c). Cultured cells were used as effectors against"Cr-labelled K-562 target cells at a 25:1 effector to target ratio.The results are expressed as the mean specific lysis of triplicateexperiments performed with the different cellular subpopulationsstudied in each group of subjects.
TABLE IV CD3-, CD16+ NK cells are the main precursorand effector lymphocytes ofLAK activity
Patients
Active Inactive Controls
Peripheral bloodmononuclear cells (a) 45 43 47
Precursor cells (b)CD3-, CD16' 52 55 56CD3+, CD16 4 6 9
Effector cells (c)CD3 , CD16+ 50 48 52CD3, CD16- 5 4 8
PBMNC from three patients with active disease and threepatients with inactive disease and three control subjects were leftuntreated (a) or were treated with anti-CD3 (CD3 , CD16+) oranti-CD16 (CD3', CD16-) monoclonal antibodies pluscomplement (b). 2 x 106 cells/ml were incubated in the presence of100 IU/ml rIL-2 for 5 days. At the end of the culture period,aliquots of untreated PBMNC were treated with anti-CD3 (CD3-,CD16') or anti-CD16 (CD3 , CD16-) monoclonal antibodiesplus complement (c). Cultured cells were used as effectors against"Cr-labelled NK resistant JY target cells at a 25:1 effector to targetratio. The results are expressed as the mean specific lysis oftriplicate experiments performed with the different cellularsubpopulations studied in each group of subjects.
LAK ACTIVITY IS INDUCED IN PBMNC FROMPATIENTS WITH ACTIVE AND INACTIVE DISEASELongterm incubation with IL-2 can induce non-MHC restricted cytotoxic activity directedagainst either NK sensitive or NK resistanttarget cells in PBMNC.9 Thus we investigatedthe effect of titrated quantities of rIL-2 on thenon-MHC restricted lytic cytotoxicity ofPBMNC from ulcerative colitis patients afterfive days of incubation. As shown in Figure 3,
IL-2 induced strong lytic activity against the NKsensitive K-562 target cells in PBMNC frompatients with either active or inactive disease.Furthermore, this cytotoxic activity is alsodirected against different NK sensitive and NKresistant target cells in a non-MHC-restrictedfashion (Fig 4).
It has been shown that the lymphocyticprecursors and effectors of LAK activity innormal control subjects are mainly CD16+,CD3- NK cells.'2 We also investigated whetherprecursor and effector cells of the LAK activityinduced in PBMNC from ulcerative colitispatients belong to this lymphocytic subset. Weperformed a negative selection ofPBMNC usingCD16 or CD3 monoclonal antibodies pluscomplement and tested them in the cytotoxicityassay. Both pre- and post-IL-2 incubatedPBMNC from ulcerative colitis patients treatedwith CD16 monoclonal antibody and com-plement failed to mediate cytotoxic activity.However, the lytic activity of PBMNC was notmodified by the initial or final treatment withCD3 monoclonal antibody and complement(Table IV).
DiscussionIn this study we have shown that the levels ofNKcytotoxicity in PBMNC from ulcerative colitispatients are related to the clinical activity of thedisease. Active disease is associated with thepresence in PBMNC of NK cells in normalnumbers but functionally defective. However, inpatients with inactive disease, these NK cellsdisplay normal cytotoxic activity. We also foundthat the NK cell functional defect found inpatients with active disease can be reversed uponin vitro incubation with IL-2.
Previous reports have presented contradictoryresults concerning the NK activity of PBMNCfrom ulcerative colitis patients.2"3' Our findingsof normal NK cytotoxicity in patients withinactive disease but deficient lytic levels inpatients with active disease clarify the hetero-geneous results in previous series dealing withsmall numbers of cases which, clinically, wereonly partially defined.Our results show that the percentages ofNK
cells in PBMNC from patients with either activeor inactive disease are normal as defined bymonoclonal antibodies HNK-1, CD16, andCDIlb, and by quantitative flow cytometry.The simultaneous finding of low levels of NKcytotoxic activity inPBMNC from active patientsindicates a diminished lytic efficiency in NKcells from these ulcerative colitis patients. How-ever, we have found in vivo normalisation of thecytotoxicity in patients whose disease progressesfrom active to inactive. We also show here howshort term in vitro incubation of PBMNC withIL-2 from patients with active disease reversesthe deficient NK activity. Furthermore, long-term incubation of PBMNC with this lympho-kine generates a strong LAK cytotoxicity that ismainly induced and displayed by CD16+, CD3-NK cells in patients with active and inactivedisease. Taken together, these results couldsuggest that in patients with active disease thereis a functional defect in the NK cell maturation
250

Functional impairment ofnatural killer cells in active ulcerative colitis 251
from non-cytotoxic precursors to cells that arealready cytotoxic and/or in the activation of theselytic effector cells.NK cells have been involved in the immuno-
surveillance against neoplasias and infections.' 2In tumour patients there is increasing evidencethat diminution of NK activity in PBMNC isassociated with local progression and dissemi-nation of the disease.3233 Defective NK activityin PBMNC has also been associated with a highincidence of severe viral infections.34 Low levelsofNK activity have been found in PBMNC frompatients with chronic viral infections.35 However,the pathogenic importance of the NK celldeficiency observed in different inflammatorydiseases of unknown aetiology with pronounceddisorders of the immune system remainsunclear.3637 Thus our demonstration of theexistence of altered NK cells in patients withactive ulcerative colitis could be implicated in apredisposition toward the suggested pathogenicaction of microbial agents at the intestinal wall.Nevertheless, the functional defect in the NKcells could also be secondary to the pathogenicaction of these microbiological agents. Furtherstudies are needed to define the molecular basesand the cause of the functional impairment ofNK cells found in patients with active disease. Itis feasible to suggest that the defect in NKactivity of PBMNC from such patients could becorrected in vivo by treatment with biologicalimmunomodulators such as IL-2, with possibleclinical improvement of the disease.
We thank C Lorences, G Peraile, and B Alvarez for their technicalhelp, I Millin for the statistical analysis, and M Messman for herexpert editorial assistance. This work was partially supported bygrants from the Fondo de Investigaciones Sanitarias de la SeguridadSocial, Spain.
1 Ritz J. The role of natural killer cell in immune surveillance. NEngJ Med 1989; 320: 1748-9.
2 Janeway CA. Natural killer cells. A primitive immune system.Nature 1989; 341: 108.
3 Hercend T, Schmidt RE. Characteristics and uses of naturalkiller cells. Immunol Today 1988; 9: 291-3.
4 Ortaldo JR, Longo DL. Human natural lymphocyte effectorcells: definition, analysis of activity, and clinical effective-ness.J Natl CancerInst 1988; 80: 999-1010.
5 Garcia-Peflarrubia P, Koster FT, Kelley RO, McDowell TD,Bankhurst AD. Antibacterial activity of human naturalkiller cells.J Exp Med 1989; 169: 99-113.
6 Alvarez de Mon M, Casas J, Laguna R, Toribio ML, 0 deLanddzuri M, Durantez A. Lymphokine induction of NK-like cytotoxicity in T cells from B-CLL. Blood 1986; 67:228-32.
7 Trinchieri G, Kobayashi M, Seehra J, London L, Perussia B.Response of resting human peripheral blood natural killercells to interleukin 2. J Exp Med 1984; 160: 1147-69.
8 Sancho L, Martinez-A C, Nogales A, de la Hera A, Alvarez-Mon M. Reconstitution of natural-killer cell activity in thenewborn by interleukin-2. N Englj Med 1986; 314: 57.
9 Grimm EA, Mazumder A, Zhang HZ, Rosemberg SA.Lymphokine-activated killer cell phenomenon. Lysis ofnatural killer-resistant fresh solid tumor cells by interleukin2-activated autologous human peripheral blood lympho-cytes. J Exp Med 1982; 155: 1823-41.
10 Bonilla F, Alvarez-Mon M, Merino F, et al. Interleukin-2induces cytotoxic activity in lymphocytes from regionalaxillary nodes of breast cancer patients. Cancer 1988; 61:629-34.
11 Kanof ME, Strober W. Lymphokine-activated killer-cell
cytotoxicity in the intestinal immune system. Gastroenter-ology 1989; 97: 222-4.
12 Herberman RB. Lymphokine-activated killer cell activity.Characteristics of effector cells and their progenitors inblood and spleen. Immunol Today 1987; 8: 178-81.
13 Phillips JH, Lanier LL. Dissection of the lymphokine-activated killer phenomenon. Relative contribution of peri-pheral blood natural killer cells and T lymphoctyes tocytolysis.I Exp Med 1986; 164: 814-25.
14 Kirsner JB, Shorter RG. Recent developments in nonspecificinflammatory bowel disease. N EnglJr Med 1982; 306: 837-48.
15 Harries AD, Myers B, Cook GC. Inflammatory bowel disease:a common cause of bloody diarrhoea in visitors to thetropics. BMJ 1986; 291: 1686-7.
16 Cave D, Mitchell D, Brooke B. Evidence of an agent trans-missible from ulcerative colitis tissue. Lancet 1976; i: 1311-4.
17 Gitnick GL, Rosen VJ, Arthur MH, Hertweck SA. Evidencefor the isolation of a neW virus from ulcerative colitispatients. DigDisSci 1979; 24: 609-19.
18 Dickinson RJ, Varian SA, Axon ATR, Cooke EM. Increasedincidence of faecal coliforms with in vitro adhesive andinvasive properties in patients with ulcerative colitis. Gut1980; 21: 787-92.
19 Taylor-Robinson S, Miles R, Whitehead A, Dickinson RJ.Salmonella infection and ulcerative colitis. Lancet 1989; i:1145.
20 Shorter RG, McGill DB, Bahn RC. Cytotoxicity of mono-nuclear cells for autologous colonic epithelial cells in colonicdiseases. Gastroenterology 1984; 86: 13-22.
21 MacDermott RP, Stenson WF. Alterations of the immunesystem in ulcerative colitis and Crohn's disease. Adv Immunol1988; 42: 285-328.
22 Truelove SC, Witts LJ. Cortisone in ulcerative colitis. Reporton therapeutic trial. BMJ 1955; 2: 1041-8.
23 Solovera JJ, Alvarez-Mon M, Casas J, Carballido J, DurantezA. Inhibition of human natural killer (NK) activity bycalcium channel modulators and a calmodulin antagonist.J. Immunol 1987; 139: 876-80.
24 Merino F, Alvarez-Mon M, de la Hera A, Ales JE, Bonilla F,Durantez A. Regulation of natural killer cytotoxicity by1,25-dihydroxyvitamin D3. Cell Immunol 1989; 118: 328-36.
25 Alvarez-Mon M, de la Hera A, Gaspar ML, et al. Proliferationof B cells from chronic lymphocytic leukemia is selectivelypromoted by B cell growth factor. Acta Haematol 1989; 81:91-7.
26 Kemler BJ, Alpert E. Inflammatory bowel disease: study ofcell mediated cytotoxicity for isolated human colonicepithelial cells. Gut 1980; 21: 353-9.
27 Ginsburg CH, Dambrauskas JT, Ault KA, Falchuk ZM.Impaired natural killer cell activity in patients with inflam-matory bowel disease: evidence for a qualitative defect.Gawtroenterology 1983; 85: 846-51.
28 Fiocchi C, Tubbs RR, Youngman K. Human intestinalmu.osal mononuclear cells exhibit lymphokine-activatedkiller cell activity. Gastroenterology 1985; 88: 625-37.
29 Gibson PR, Jewell DP. Local immune mechanisms in inflam-matory bowel disease and colorectal carcinoma. Naturalkiller cells and their activity. Gastroenterology 1986; 90: 12-9.
30 MacDermott RP, Bragdon MJ, Kodner IJ, Bertovich J.Deficient cell-mediated cytotoxicity and hyporesponsive-ness to interferon and mitogenic lectin activation by inflam-matory bowel disease peripheral blood and intestinal mono-nuclear cells. Gastroenterology 1986; 90: 6-11.
31 Egawa S, Hiwatashi N. Natural killer cell activity in patientswith inflammatory bowel disease. J Clin Lab Immunol 1986;20: 187-92.
32 Alvarez-Mon M, Casas J, Laguna R, Jorda J, Durantez A.Clinical signification of natural killer activity in B-cellchronic lymphocytic leukemia. Eur J Haematol 1987; 38:268-73.
33 Carballido J, Alvarez-Mon M, Solovera J, Menendez-OndinaL, Durdntez A. Clinical significance of natural killer activityin patients with transitional cell carcinoma of the bladder.J Urol 1990; 143: 29-33.
34 Biron CA, Byron KS, Sullivan JL. Severe herpesvirusinfections in an adolescent without natural killer cells.NEngljMed 1989; 320: 1731-5.
35 Quinnan GV, Kirmani N, Rook AM, et al. Cytotoxic T cells incytomegalovirus infection: HLA-restricted T lymphocyteand non-T-lymphocyte cytotoxic responses correlate withrecovery from cytomegalovirus infection in bone-marrowtransplant recipients. N EnglJ Med 1982; 307: 7-13.
36 Gaspar ML, Alvarez-Mon M, Gutierrez C. Role of interleukin2 in inducing normalization of natural killer activity insystemic lupus erythematosus. Clin Immunol Immunopathol1988; 49: 204-14.
37 Hauser SL, Ault KA, Levin MJ, Garovoj MR, Weiner HL.Natural killer cell activity in multiple sclerosis. I Immunol1981; 127: 1114-7.