Embed Size (px)
Citation preview

Ulcerative Colitis
David T. Rubin, MD, AGAFJoseph B. Kirsner Professor of Medicine
Chief, Section of Gastroenterology, Hepatology, and NutritionCo-Director, Digestive Diseases Center
@IBDMD
Disclosures(Last 24 months)• Consultant and Grant Support:
– Abbvie– Amgen– Cellgene– Janssen– Pfizer– Prometheus– Takeda– UCB
Learning Objectives
At the conclusion of this presentation, participants will:• Recognize the common presentation and progression
of ulcerative colitis• Understand the appropriate treatment options for
ulcerative colitis.

Case• 18 year old male• 4 months of rectal
urgency and frequency• Nocturnal symptoms• Blood with bowel
movements• One episode of
incontinence• Nausea
• SH: – Senior in high school– “stressed”– No tobacco
• FH:– No GI or immune
problems– Sister with IDDM
• PSH: – none

Case continued• Physical examination:
– BMI: 21– Abdomen:
• Minimal tenderness in the left lower quadrant
• Tympany on the right side of the abdomen
– Perianal area: • Normal
• Labs:– Hemoglobin 11.1 g/dL– CRP 3.0 mg/L– Albumin 3.4 g/dL– Stool studies: negative
for O and P, C. difficiletoxin
• A diagnostic test is performed


Diffuse, prominent crypt architectural distortion and mucosal atrophy, with foci of crypt dropout.
No granulomas.
Diagnosis: ulcerative colitis

Distal Left-Sided Pancolitis
18%44% 36%*Based on regional cohort of 1,161 patients diagnosed from 1962 to 1987.
Langholz EP, et al. Scand J Gastroenterol. 1991;26:1247.
Anatomic Extent of Disease:Disease Involvement at Diagnosis*

Major Symptoms of UC are Due to an Inflamed Rectum
85% 83% 78%
63%
0%
20%
40%
60%
80%
100%
Urgency Increaseddefecationfrequency
Incompleteevacuation
Tenesmus
Patie
nts,
%Symptom prevalence
Rao SS, et al. Gut. 1988;29:342-345.

Disease Behaviors of Ulcerative Colitis
Solberg IC, et al. Scand J Gastroenterol. 2009;44(4):431-40.
Environmental Associations of UC
• Protective against UC– Appendectomy (for appendicitis)1
– Dietary omega-3-fatty acids2
• Increase UC risk– Dietary linoleic acid (your lunch today?)3
– Ex-smoking4
– Gut infections5
– Possibly antibiotic exposure6
1. Andersson RE, et al. N Engl J Med. 2001;344:808-814.2. Sneha J, et al. Gastroenterology. 2008;134(Suppl 1):A-4.a3. Hart AR, et al. Gut. 2009. 58(12):1606-1.
4. Rubin DT, Hanauer SB. Eur J Gastroenterol Hepatol. 2000;12:855-862.5. Ohkusa T, et al. Int Med. 2004;43:534-539.6. Shaw SY, et al. Am J Gastroenterol. 2011; 106(12):2133-42.

How can we treat our patient’s UC?
Historical Treatment Strategies in IBD
• Symptom-based• Expectant management• Unclear if changed natural history of the disease or
quality of life• Imprecise (“Dirty therapy”)

Historical Treatment StrategiesSymptom Based, Short Term Goals
Disease severityat presentation?
Severe
Moderate
MildAminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine(UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery

Modern Goals of IBD Management
Induction of Remission
•Turning “off” the inflammation•Feeling well•Normalization of labs, growth, development and nutrition
Maintenance of Remission
•Stable disease control and optimization of therapy•NO STEROIDS•Prevention of relapse over time (sustained and durable)•Changing the natural course of the disease
Disease Monitoring and
Prevention
•Monitoring for early relapse•Monitoring therapies•Prevention of infections•Cancer prevention

Medical Treatment Options for Patients With UC
• Aminosalicylates– Mesalamine– Azo-bonded prodrugs
• Sulfasalazine• Olsalazine • Balsalazide
• Corticosteroids– Systemic steroids– Budesonide
• Thiopurines– AZA– 6-MP
• Cyclosporine• TNF-α inhibitors
– Infliximab– Adalimumab– Golimumab
• Anti-integrin therapy– Vedolizumab

5-ASA Therapies
• Mesalamine with different delivery systems– various pH-release mesalamines
– controlled-release mesalamine
– rectal preparations
• Pro-drugs– azo-bonded sulfasalazine, olsalazine, and balsalazide
• Oral PLUS topical (rectal) therapy is better than either alone for induction of remission (distal and extensive)

Advantages of 5-ASA for Mild to Moderate UC
• Efficacy for induction of response is 50% to 70%
• Efficacy for induction of remission is 15% to 40%
• Excellent safety profile
Hanauer SB, et al. Ann Intern Med. 1996;124:204.Hanauer SB, et al. Am J Gastroenterol. 1993;88:1188.Hanauer SB, et al. Am J Gastroenterol. 2005;100:2478.
Levine DS, et al. Am J Gastroenterol. 2002;97:1398.Sninsky CA, et al. Ann Intern Med. 1991;115:350.

5-ASA Safety Considerations
• Mesalamine intolerance: Rare but important1
• Pancreatitis1
• Pneumonitis2
• Renal insufficiency3,4
1Kornbluth & Sachar, Am J Gastroenterol.2004; 99: 1371–85.2Foster, et al. Inflamm Bowel Dis.2003; 9: 308–15.3Van Staa, et al. Gastroenterology. 2004; 126: 1733–9.4Gisbert, et al. Inflamm Bowel Dis. 2007; 13: 629–38.
.
Current use
Recent use
Past use
Risk of renal events with 5-ASA3
Adjusted odds ratio
0 1 2 3 4 5
Increased risk vs non-use

Oral (2.4 g/d)Rectal (4 g/d)Combined
Focus on the RectumTreatment of Distal UC:
Oral and Rectal Mesalamine Therapy
6 Weeks
*
0
Patie
nts
Rep
ortin
gN
o R
ecta
l Ble
edin
g (%
)100
40
60
20
80
*P<0.002 vs oral alone, P=0.04 vs topical alone
Adapted from Safdi M, et al. Am J Gastroenterol. 1997;92:1867.

Case continued
• Treated with 5-ASA therapy topically and rectally
• Improvement for 3 months– then non-adherence
• Recurrent diseaseAminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine(UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery

Importance of Adherence: Sustained Remission of IBD
Kane S, et al. Am J Med. 2003;114:39.
Patie
nts W
ith
Qui
esce
nt U
C (%
)
0 300
Adherent to 5-ASA therapy
Nonadherent to 5-ASA therapy*
Time (months)
100
75
50
25
10 20
*P<0.001
Lesson learned: maintenance therapy is needed, patients should
be educated
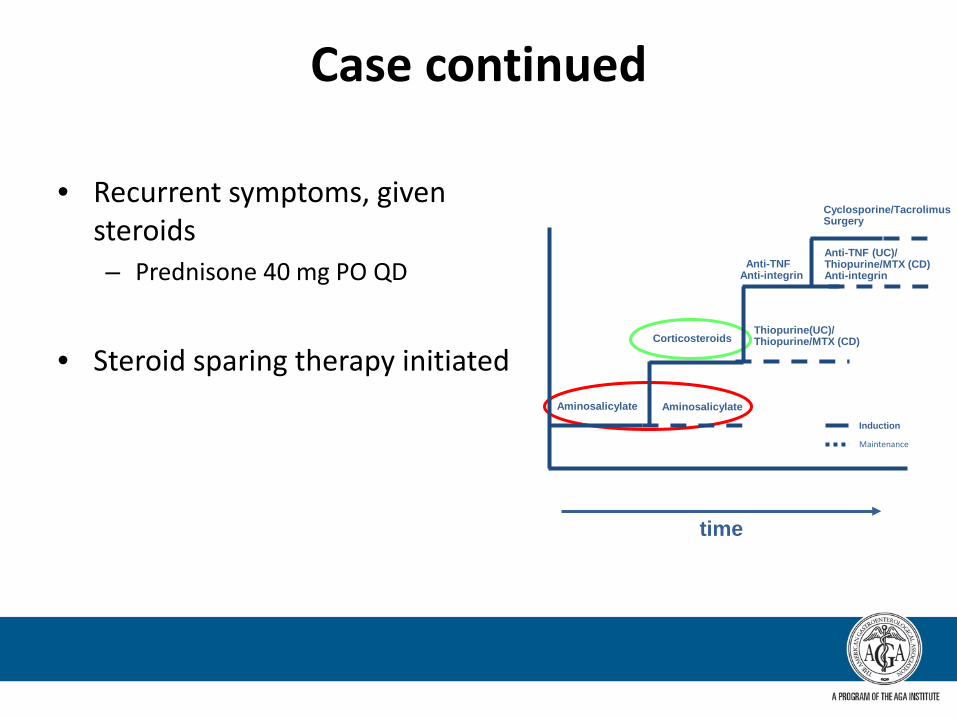
Case continued
• Recurrent symptoms, given steroids– Prednisone 40 mg PO QD
• Steroid sparing therapy initiatedAminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine(UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery

Treatment Revolution: Steroids for UC Reduce Mortality
40
30
20
10
0
Mor
talit
y (%
)
1938–1952
1953–1962
1963–1972
1973–1982
1983–1987
Edwards FC, et al. Gut. 1963;4:299.
Corticosteroids introduced in 1952
• Steroids subsequently associated with worst outcomes in IBD, are used short-term only!
• Initiation of steroids should always prompt an exit strategy (steroid-sparing therapy).

Corticosteroid Therapy in UC
StudyDisease
StateSteroid/
DoseResponse (%)*
Steroid PlaceboTruelove1
(6 weeks)Active Cortisone
≥100 mg69
(n=109)41
(n=101)
Lennard-Jones2
(6 months)Maintenance Prednisone
15 mg 38
(n=32)40
(n=30)
Truelove3
(5 days)Severely
activePrednisolone
40–60 mg (Total n=49)
73 N/A
* Response defined as: Truelove: Patients who improved and/or were in remission Lennard-
Jones: Maintenance of remissionTruelove: Patients in remission
1. Truelove SC, et al. Br Med J. 1955;2:1041.2. Lennard-Jones JE, et al. Lancet. 1965;1:188.3. Truelove SC, Jewell DP. Lancet. 1974;1:1067.

Corticosteroids: Short- and Long-Term Efficacy for UC
*30 days after initiating corticosteroid therapy
Faubion W, et al. Gastroenterology. 2001;121:255.
1-month outcomes*(n=63)
1-yearoutcomes(n=63)
Prolonged response
49%(n=31)
Steroid dependent
22%(n=14)
Surgery 29%
(n=18)
Complete remission
54%(n=34)
Partial remission
30%(n=19)
No response 16%
(n=10)

Budesonide MMX for active ulcerative colitis odds ratios for different endpoints
US trial: 9 mg vs placeboOR (95%CI)
Remission 2.71 (1.19, 6.16)
Clinical improvement 1.52 (0.87, 2.65)
Endoscopic improvement 1.43 (0.85, 2.42)
Symptom resolution 2.01 (1.08, 3.73)
Histologic healing 0.60 (0.19, 1.88)
EU trial: 9 mg vs placeboOR (95%CI)
Remission 4.49 (1.47, 13.72)
Clinical improvement 1.44 (0.80, 2.57)
Endoscopic improvement 1.59 (0.88, 2.86)
Symptom resolution 2.47 (1.12, 5.46)
Histologic healing 2.74 (1.04, 7.22)
Placebo better MMX 9 mg better 0.1 1 10
Placebo better MMX 9 mg better 0.1 1 10010
Sandborn, et al. Gastroenterology. 2011. 142(2):257-65.

Case continued
• Thiopurine therapy started (azathioprine)
• TPMT enzyme activity obtained prior to dosing
Aminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine(UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery
Frequency Enzyme Activity Allele89% normal to high TPMTH/TPMTH
11% intermediate TPMTH/TPMTL
0.33% low to absent TPMTL/TPMTL

TPMT Polymorphism and Metabolism of Azathioprine/6-MP
Azathioprine
6-Methyl-mercaptopurine
6-Mercaptopurine Thioinosinicacid
6-Thioguaininenucleotides
6-Thiouricacid
TPMT
HPRT
XO
Chan GL, et al. J Clin Pharmacol. 1990;30:358.

Use of Metabolites to Optimize Thiopurine Therapy
6-TG 6-MMP Possible cause
undetectable undetectable Non-adherentorunderdosed
Low (<230) Low or undetectable Non-adherent or underdosed
Low (<230) High (>5700) 6-MMP shunter
“Therapeutic” (>230-<400) orHigh (>400)
Normal range or high Primary non-responder
Dubinsky. Curr Gastroenterol Rep. 2003;5(6):506-11.

6-TG 6-MMP Possible cause
undetectable undetectable Non-adherentorunderdosed
Low (<230) Low or undetectable Non-adherent or underdosed
Low (<230) High (>5700) 6-MMP shunter
“Therapeutic” (>230-<400) orHigh (>400)
Normal range or high Primary non-responder
Dubinsky. Curr Gastroenterol Rep. 2003;5(6):506-11.
Use of Metabolites to Optimize Thiopurine Therapy

Case continued
• Doesn’t respond to “optimized” azathioprine
• Flexible sigmoidoscopy shows worsening mucosal disease
• C. difficile and CMV ruled out

Severity of Disease Correlates With Colectomy
Severe EndoscopicColitis(n=46)
Moderate EndoscopicColitis(n=39)
Carbonnel F, et al. Dig Dis Sci. 1994;39:1550.
100
80
60
40
20
0
Patie
nts
(%)
Deep/Extensive
Ulcers
93%
MucosalDetachment
30%
LargeMucosal
Abrasions
26%
Well-likeUlcers
17%
93% underwentcolectomy
100
80
60
40
20
0
Patie
nts
(%)
SuperficialUlcers
77%
Deep ButNonextensive
Ulcers
8%
23% underwentcolectomy

Case continued
Aminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine (UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)/Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery
• An anti-TNFα therapy is now added to his azathioprine
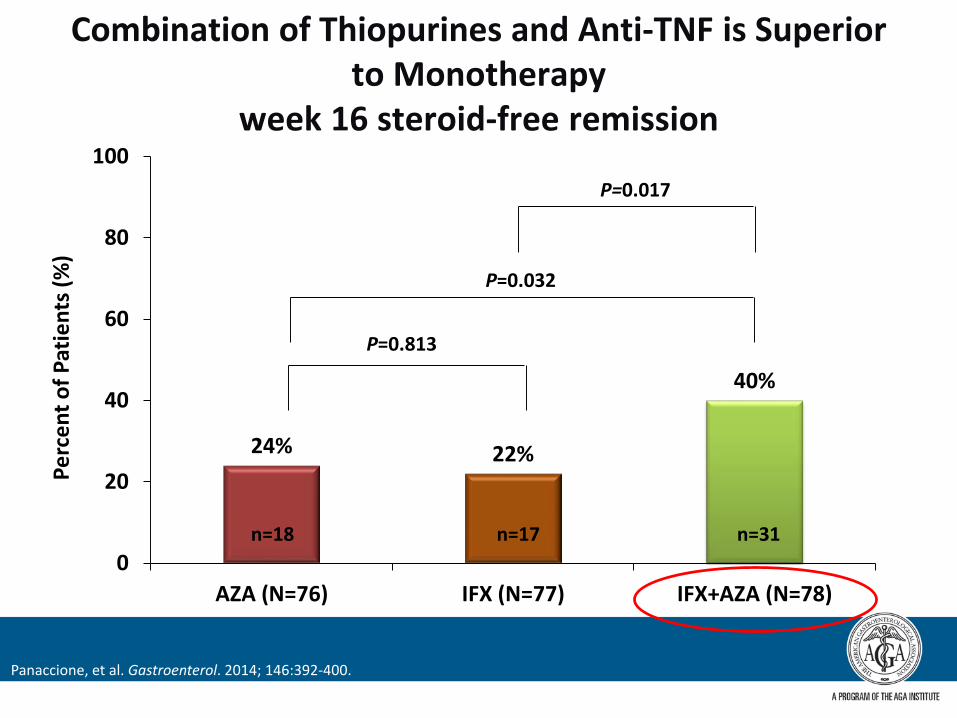
24% 22%
40%
0
20
40
60
80
100
AZA (N=76) IFX (N=77) IFX+AZA (N=78)
Perc
ent o
f Pat
ient
s (%
)
n=18 n=17 n=31
P=0.017
P=0.813
P=0.032
Panaccione, et al. Gastroenterol. 2014; 146:392-400.
Combination of Thiopurines and Anti-TNF is Superior to Monotherapy
week 16 steroid-free remission

Case continued
• After loading doses of infliximab, feeling better, starts maintenance dosing
• Responds well- feeling good…for six months….
• Calls us to say he is not well again
Aminosalicylate
Corticosteroids
Anti-TNFAnti-integrin
Thiopurine (UC)/Thiopurine/MTX (CD)
Aminosalicylate
Anti-TNF (UC)/Thiopurine/MTX (CD)/Anti-integrin
Induction
Maintenance
time
Cyclosporine/TacrolimusSurgery

What happened?

Possible Reasons for Loss of Response to Infliximab and Azathioprine in our Patient• Non-adherence to his therapies (again)
• “Feeling good” not the same as actually healed
• pK issues of monoclonal antibodies: – Development of anti-drug antibodies– Progression of disease (getting worse instead of better)
• Role of loss of protein from bowel– Weight gain (getting better, eating more)
• “Mechanistic escape”

Case continued
• Infliximab level: 40 mcg/mL (very high)• Anti-infliximab antibodies not present
• Hgb 9.5 g/dL• CRP 12 mg/L• Albumin 3.0 g/dL
• Consider a different mechanism of management

Leukocyte Trafficking Inhibition
Action of Adhesion molecules (eg. Integrins) in the intestinal endothelium
Lobatón T, et al. Aliment Pharmacol Ther.2014; 39:579-594.
Vedolizumab

Our patient on vedolizumab plus azathioprine therapy
Now What?
Disease monitoringTherapeutic monitoring
Maintenance care, cancer prevention

Download Cornerstones’ Checklist for IBD Patients by visiting: cornerstoneshealth.org/checklist/
Summary: Ulcerative Colitis
• Know the disease activity of your patient• Choose therapies wisely, and target the areas of
activity• Understand the reasons for loss of response• Monitor disease, treatment and enroll in prevention
programs

Thank you