Embed Size (px)
Citation preview

ST-‐Segment Elevation Myocardial InfarctionChallenges in Diagnosis
&Current Measures of Quality
James M. McCabe, MD, FACC, FAHACath Lab Director, University of Washington

Disclosures
• I, James McCabe, have no relevant financial disclosures

I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
V1
II
V5
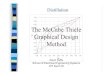
DONNELLY, EILEEN ID:002653467 02-JAN-2010 22:27:29 BRIGHAM & WOMEN'S/FAULKNER HOSP.
Normal sinus rhythm with sinus arrhythmiaMinimal voltage criteria for LVH, may be normal variantCannot rule out Anterior myocardial infarction , age undeterminedAbnormal ECGNo previous ECGs available
25mm/s 10mm/mV 150Hz 8.0.1 12SL 239 CID: 1
Referred by: PETER LIBBY, M.D. Confirmed By: DALE ADLER M.D.
BPM62Vent. ratems202PR intervalms76QRS durationmsQT/QTc 468/475-28025P-R-T axes
03-AUG-1925 (84 yr)Female Unknown
Room:904Loc:206 Option:1
Technician: Test ind:410.12
Page 1 of 1 EID:12 EDT: 15:12 05-JAN-2010 ORDER: ACCOUNT: 002653467

ECG� 51
Analysis of intermediate risk ECGs alone for STEMI diagnosis
• 36 ECGs for which a cath lab activation had occured
• 124 physicians at various levels surveyed• All cases described as ”moderate risk of acute coronary syndrome” without further clinical details provided
• Q: Is there a blocked coronary artery present causing a STEMI? (please provide your best guess)
McCabe et al. JAHA. 2013.

Reader Performance by Experience
Sens Spec PPV NPV Kappa C
Computer Algorithm 45.8 83.3 84.6 43.5 n/a 0.65
Sens Spec PPV NPV Kappa C
Computer Algorithm 45.8 83.3 84.6 43.5 n/a 0.65
All Participants 65.4 79.1 86.3 53.3 0.35 0.72
Sens Spec PPV NPV Kappa C
Computer Algorithm 45.8 83.3 84.6 43.5 n/a 0.65
All Participants 65.4 79.1 86.3 53.3 0.35 0.72
By Training Level
All Residents 61.3 72.5 81.7 48.2 0.27 0.67
All Fellows 62.9 86.1 90 53.7 0.41 0.74
All Attendings 70.3 79.2 87.1 57.1 0.39 0.75
McCabe et al. JAHA . 2013

Accuracy of ECG Read for STEMI
OR 95% CI p Value
Residents -‐-‐ -‐-‐ -‐-‐
Fellows 1.26 1.02-‐1.56 0.03
Attendings 1.45 1.19-‐1.77 <0.01
Experience (per year) 1.01 1.00-‐1.02 0.01
ED & IM Physicians* -‐-‐ -‐-‐ -‐-‐
Non-‐invasive Cardiologists* 0.91 0.67-‐1.22 0.53
Interventional Cardiologists* 1.06 0.73-‐1.53 0.77
* Attendings only
Experience Matters!6% increased odds of accuracy for every 5 years since medical school
Statistical methods: generalized estimatingequations to account for repeated measures

Sensitivity & Specificity by ECG Characteristics
4% éodds of accuracy per ECG lead with diagnostic STE (p = 0.03, 95%CI 1.00-‐1.08)
Maximal height of STE (per mm) doesn’t improve accuracy (p 0.59, 95%CI .95-‐1.03)
Lateral and posterior STE more often inaccurate (vs anterior) – small samples

I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
V1
II
V5
DONNELLY, EILEEN ID:002653467 02-JAN-2010 22:27:29 BRIGHAM & WOMEN'S/FAULKNER HOSP.
Normal sinus rhythm with sinus arrhythmiaMinimal voltage criteria for LVH, may be normal variantCannot rule out Anterior myocardial infarction , age undeterminedAbnormal ECGNo previous ECGs available
25mm/s 10mm/mV 150Hz 8.0.1 12SL 239 CID: 1
Referred by: PETER LIBBY, M.D. Confirmed By: DALE ADLER M.D.
BPM62Vent. ratems202PR intervalms76QRS durationmsQT/QTc 468/475-28025P-R-T axes
03-AUG-1925 (84 yr)Female Unknown
Room:904Loc:206 Option:1
Technician: Test ind:410.12
Page 1 of 1 EID:12 EDT: 15:12 05-JAN-2010 ORDER: ACCOUNT: 002653467

PRE-‐
POST-‐

I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
V1
II
V5
DONNELLY, EILEEN ID:002653467 02-JAN-2010 22:27:29 BRIGHAM & WOMEN'S/FAULKNER HOSP.
Normal sinus rhythm with sinus arrhythmiaMinimal voltage criteria for LVH, may be normal variantCannot rule out Anterior myocardial infarction , age undeterminedAbnormal ECGNo previous ECGs available
25mm/s 10mm/mV 150Hz 8.0.1 12SL 239 CID: 1
Referred by: PETER LIBBY, M.D. Confirmed By: DALE ADLER M.D.
BPM62Vent. ratems202PR intervalms76QRS durationmsQT/QTc 468/475-28025P-R-T axes
03-AUG-1925 (84 yr)Female Unknown
Room:904Loc:206 Option:1
Technician: Test ind:410.12
Page 1 of 1 EID:12 EDT: 15:12 05-JAN-2010 ORDER: ACCOUNT: 002653467
NOT COUNTED BY CMS

Measuring Quality of Care in STEMIIn-‐hospital Mortality• primary outcomemeasure of quality
– Public Reporting (eg COAP) and national registries (NCDR)– CMS began tracking 30 day post-‐MI mortality as part of Value Based Purchasing in 2014
• Typically ‘risk-‐adjusted’• Crude in-‐hospital mortality ~5-‐6%Massachusetts’ Crude In-‐Hospital Mortality following PCI for STEMI or Shock 2003-‐2010

Measuring Quality of Care in STEMI Cont’d
Time to Reperfusion• primary process measure of quality• “Door-‐to-‐Balloon” time• Should maintain relationship with outcome measure• Easily measured• Allows for systemic changes targeting controllable processes– D2B time should be within our control, mortality may not be. – Why mortality is risk-‐adjusted and D2B time is not.

Mr. C.• 59 yo man with no significant PMHx (former tobacco and +FHx early CAD) presented to the ED with chest discomfort.
• Felt well in AM. Went skydiving for first time.– “Queasy and nervous” in plane (approx 1 PM).– Jumped and developed chest pain as parachute deployed.
• Returned home by 2 PM. Continued chest discomfort. Took nap for approx until approximately 5:30 PM. On waking continued discomfort.
• Girlfriend drove him to UW ED. Arrived at 6 PM with continued chest discomfort.

18:05

Mr. C• Code STEMI activated within 6 mins of ECG.• STAT chest CTA to evaluate for aortic dissection was ordered in ED.
• Left ED and arrived in cath lab at 18:50.

Mr. C.• PMHx: Erectile dysfunction• NKA• Meds: Tadalafil PRN• SHx: divorced. Long-‐term girlfriend. 35 pack year tobacco history (quit 20 years
ago)• FHx: Father with MI at age 48. Mother alive with HTN, depression. No children.
• Exam:– 114/56, HR 65, RR 18, 96% RA– Uncomfortable and diaphoretic.– JVP 6 cm. Normal PMI. RRR. normal s1, s2. No gallops or murmurs. No rub. – Normal radial, femoral, DP/PT pulses bilaterally. – Lungs CTA b/l.– Abdomen soft/non-‐tender.– Alert, non-‐focal

Mortality and D2B Time Relationship2nd National Registry of Myocardial Infarctions
(NRMI-‐2)• 1474 Hospitals (only 661 could perform PTCA)• 6/1994-‐3/1998 • All acute MI’s (by ECG and CK-‐MB)• Observational• Angioplasty only

NRMI 2
Cannon CP. JAMA. 2000;283:2941.
Symptom Duration to Balloon Time
Door-‐to-‐Balloon Time
120 Minutes

NRMI 3&4: Confirmed Findings of NRMI 2
McNamara RL. J Am Coll Cardiol. 2006;47:2180
1999-‐200229,222 STEMIs at 395 hospitals
P <0.001 for trend

DBT and 1 year mortality
DeLuca G et al. Circulation. 2004;109:1223
Regression Model of TOTAL ISCHEMIC TIME vs mortality
• 1994-‐2001• 1700 patients• Angioplasty only
Introduced the notion of per minute increases in mortality

D2B Alliance Hospitals
Bradley EH. J Am Coll Cardiol. 2009;54:2423

CMS Codified D2B Time
Centers for Medicaid and Medicare Services (CMS) arguably most important in altering care delivery for STEMI patients• Began tracking D2B in 2005
– Original target 120 min mean D2B per hosp– 2006 changed to 90 min median D2B per hosp
• Reimbursement was tied to performance

Improvements in D2B in U.S. 2005-2010
Krumholz, et al. Circulation. 2011;124:1038-1045
Review of 973 U.S. hospitals providing Primary PCI for STEMI demonstrated dramatic improvement in proportion of patient treated within 90 minutes of emergency department arrival.
48% absolute Δ

What drives DTB time?
McCabe JM. Circ Cardiovasc Qual Outcomes. 2012;5:672
Door-‐to-‐activation ≤ 20 min – 89% achieved D2B <90 minDoor-‐to-‐activation > 20 min – 28% achieved D2B < 90 min
r = 0.97

ED Crowding – Important Predictor of D2B
Adjusted for time of day and physician staffing
p = 0.013
McCabe, unpublished

What drive DTB time:Can We Skip the ED?
Bagai A. Circulation. 2013;128:352
• Action-‐GWTG registry, 2008-‐2011• 83,461 STEMI patients

ED Bypass
Bagai A. Circulation. 2013;128:352
Median times
In hospitals with >25 STEMI/year
• Unadjusted mortality lower in patient who had ED bypass.• Adjusted mortality was similar.

The Price of Doing Business When Focus is Solely on Expedience
Barnes GD. Am J Man Care. 2013;19:671

The confusing semantics of STEMI (mis)diagnoses
False PositiveActivation Over-‐activation
Inappropriate Activation
“[activation] for patients who do not ultimately require emergent catheterization or performing angiography on patients who are ultimately found not to require coronary intervention.” 4
Weighs cases against criteria available at the time of activation; not directly related to outcomes. 5,6
Generally a surrogate for diagnostic accuracy but variously defined in relationship to available angiography, clinical history, and biomarker assays. 1,2,3
1. Larson. JAMA, 20072. Kontos. Am J Em Med,
20113. McCabe. Arch Int Med,
20124. Garvey. Circ, 20125. Rokos. Am Heart J, 20106. Mixon. Circ Qual, 2012

14% No culprit on angio
11% Negative biomarkers

The confusing semantics of STEMI (mis)diagnoses
False PositiveActivation Over-‐activation
Inappropriate Activation
36% 39%
N/A
McCabe et al. JAMA Int Med. 2012;172, 864–871
1. Larson. JAMA, 20072. Kontos. Am J Em Med, 20113. McCabe. JAMA Int Med, 20124. Garvey. Circ, 20125. Rokos. Am Heart J, 20106. Mixon. Circ Qual, 2012
Generally a surrogate for diagnostic accuracy but variously defined in relationship to available angiography, clinical history, and biomarker assays. 1,2,3
“[activation] for patients who do not ultimately require emergent catheterization or performing angiography on patients who are ultimately found not to require coronary intervention.” 4
Weighs cases against criteria available at the time of activation; not directly related to outcomes. 5,6

Factors Independently Associated with False Positives
Multivariate AnalysisAOR 95%CI p value
BMI (per unit kg/m2) 0.91 .86-‐.97 0.004Anginal chief complaint 0.28 .14-‐.57 <0.001Known coronary disease 1.93 1.04-‐3.59 0.037Illicit Drug Abuse 2.67 1.13-‐6.26 0.024Left Ventricular Hypertrophy by ECG Criteria 3.15 1.55-‐6.40 0.001
Known CAD, prior drug abuse, and presence of LVH are strongly associated with false positive diagnoses
Heavier weight and a “classic angina” chief complaint associated with diminished false positive rates
McCabe et al. Arch Int Med, 2012.172, 864–871

Adjudicated Admission Diagnoses for False Positives
% false PositivesN= 146
Structural/valvular heart disease +/-‐ CHF exacerbation 19
Non-‐specific chest pain, including soft tissue ailments 17
Demand ischemia and severe concomitant illness 14
Primary rhythm disturbance 10
Metabolic derangements (including toxins/drugs) 10
Out of hospital cardiac arrest 6
Myocarditis/Pericarditis 6
Known CAD & stable symptoms 4
Abdominal pathologic condition 3
Hypertensive urgency/emergency 3
Takotsubo 1
Other diagnoses 6
McCabe. Arch Int Med, 2012. 172(11), 864–871

Can we do better than ACC/AHA guidelines in setting of LVH?
Armstrong & McCabe et al. AJC, 2012.110(7), 977–983.
• Goal: create a simple ECG rule to improve specificity while preserving sensitivity for STEMI dx
• 79 of first 411 cases in registry had criteria for LVH (by any standard criteria) and underwent angiography; study cohort
• Assessed test characteristics of multiple schemes against angiographic outcome (reference standard)
REF

Recursive PartitioningAlgorithm
Sensitivity = 77%Specificity = 91%NRI 37%
Armstrong & McCabe et al. AJC, 2012.110(7), 977–983.

LVH
3 29
3/29 = 10%Not a STEMI

Primary Limitation to LVH Algorithm
It has not been validated against an external cohort

Does the attention on Door-to-Balloon time and diagnostic
specificity matter?

•CathPCI data from 2005-‐2009•96,738 STEMI admissions at 515 hospitals

Menees DS. N Engl J Med. 2013;369:901
•No significant association between annual decreases in DTB time and in-‐hospital mortality (odds ratio for 10 min reduction in DTB time: 1.04, 95% CI: 0.99 – 1.14).

Improvements in D2B in U.S. 2005-2010
Krumholz, et al. Circulation. 2011;124:1038-1045
Review of 973 U.S. hospitals providing Primary PCI for STEMI demonstrated dramatic improvement in proportion of patient treated within 90 minutes of emergency department arrival.
48% absolute Δ
CMS Specifications Manual: 9 exclusion criteria for case reporting. Updated 2006.
#9: “Patients who did not receive PCI within 90 minutes and had a reason for delay documented by a physician/APN/PA (e.g., social, religious, initial concern or refusal, cardiopulmonary arrest, balloon pump insertion, respiratory failure requiring intubation)”

Is D2B Time Just a Game?
McCabe JM. Circulation. 2014. 129:194-‐202
Patients excluded from national registries are large, un-‐measured piece of puzzle

“Gaming” the system?
McCabe JM. Circulation. 2014. 129:194-‐202

Different Registry, Same Result:“non-‐system” delays Patients in NCDR
Swaminathan RV. J Am Coll Cardiol. 2013;61:1688
•CathPCI Registry 2009-‐2011
•82,678 STEMIs (12,146 non-‐system delay patients)

D2B Time as Quality
• 10+ years as the primary process measure of quality in pPCI
• Functioned as a surrogate for mortality risk• Have we eroded the D2B-‐mortality relationship by studying only ‘idealized’ patients?
• More fundamentally, is risk-‐adjusted mortality even capable of determining quality?

Fundamental Challenges of Risk Adjusted Mortality (RAM) and Quality
Thomas TJ & Hoffer TP. Med Care. 1999. 37(1): 83-‐92
Sensitivity for poor performers <20%
60-‐70% of identified outliersNot poor performers

The Multiple Axes of Quality in PCI

Other Process Measures: The radial vs. femoral example.
Wimmer NJ. Am Heart J. 2014. in press.

Conclusions: How do we move forward?
• Focus on a single axes of quality (like ED bypass or DTB time) is useful but not sufficient to enhance the overall system of care for STEMI patients.
• Greater coordination among the many pre-‐hospital systems in the care of STEMI patients is crucial and would be facilitated if STEMI was a reportable public health condition.
• Focus on total ischemic time in the care of patients with STEMI important. Patient education is paramount in this endeavor.
• Other advances (hemodynamic support, pharmacologic targeting, cooling [arrest patients], technical innovations) in PCI are likely to provide the next major steps forward in STEMI care.
Antman EM. Circulation. 2013;128:322Grines CL and Schreiber T. J Am Coll Cardiol. 2013;61:1696

Thank you!