Embed Size (px)
Citation preview
Turbulence ahead!Fasten Your Seat Belts!
What Physicians Can Expect from Health Reform
Over the Next Five YearsBob Doherty
SVP, Governmental Affairs and Public Policy, ACP
Virginia Chapter, ACP
March 1, 2013
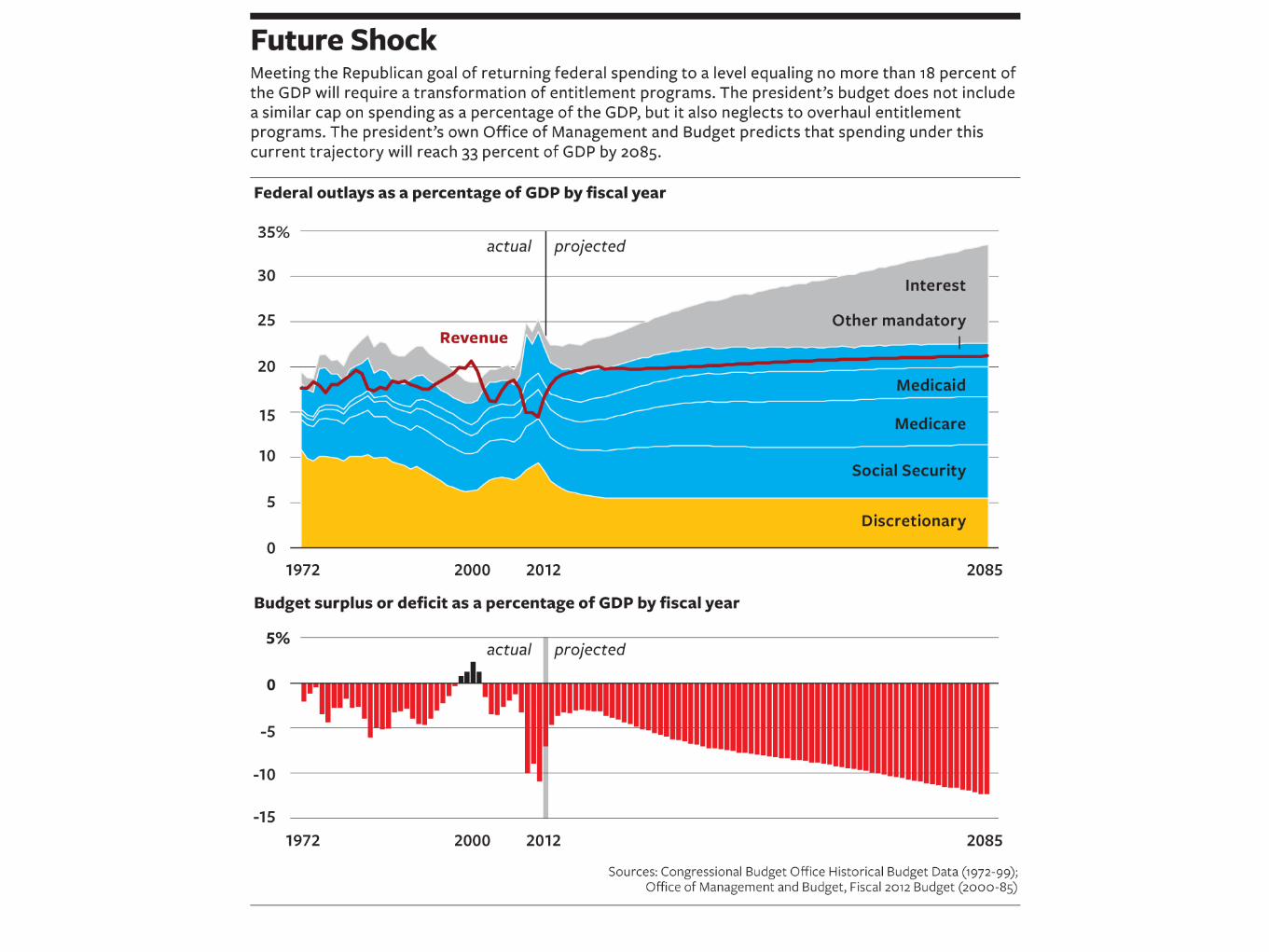
Health reform: from here to there Here: tens of millions uninsured, uneven
quality, rising costs, intrusions on patient-physician relationship
There: near universal coverage--with better quality at a price we can afford? And fewer intrusions on patients and physicians?
How smooth or rough will the journey be?

How we would like it to be . . .
What we expect it will be. . .
What we fear it will be . . .
What we fear it will be . . .

Turbulence
Affordable Care Act
Entitlements
Budget and sequestration
Payment/delivery system reform
ACA: the political environment
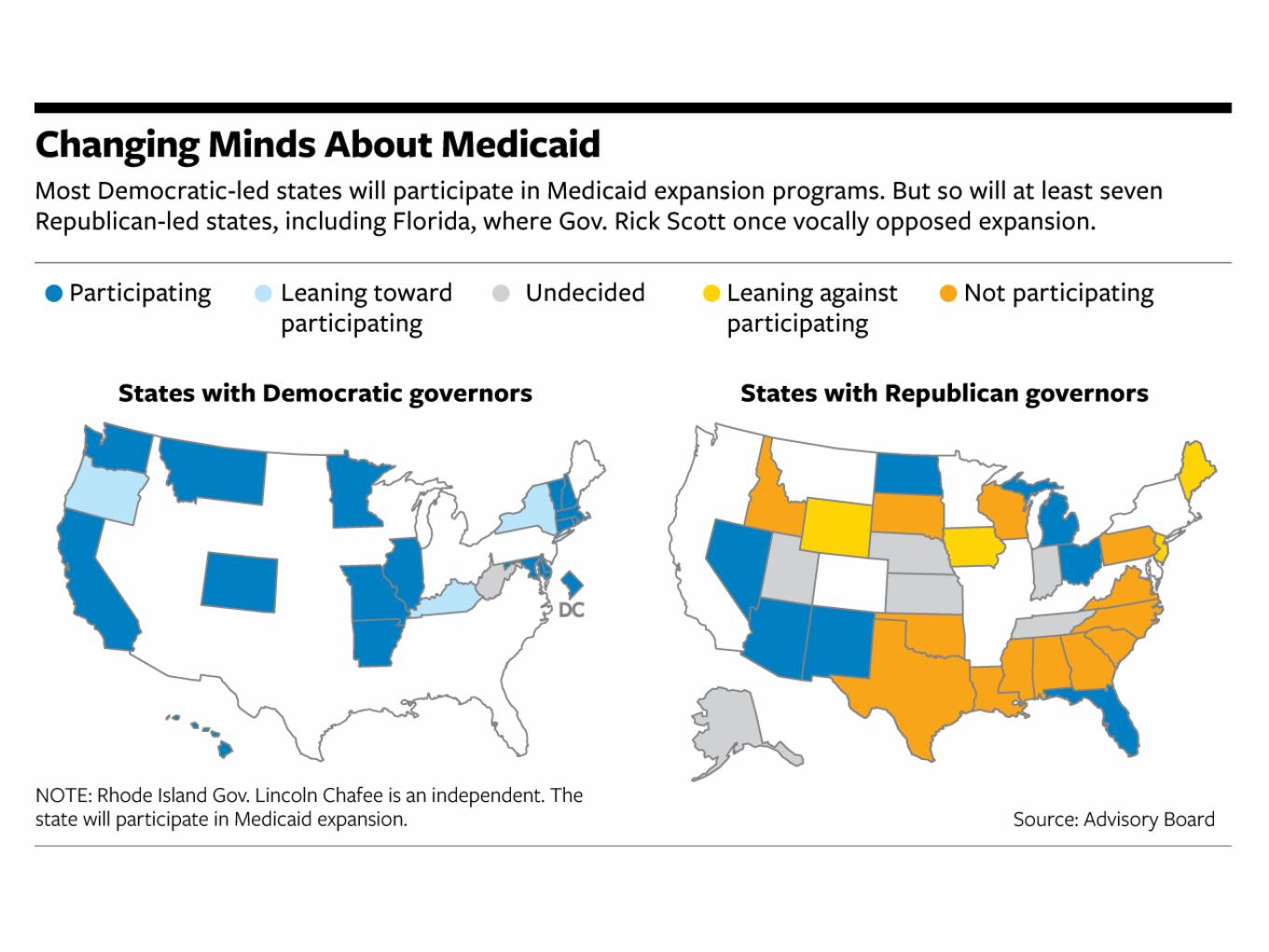
1.No plausible scenario where the ACA will be repealed
2.State engagement/ resistance may determine the law’s effectiveness in expanding coverage
The role of the states Medicaid: Accept/reject federal dollars
Exchanges: Set up own exchange, partner with federal government, or turn it over to the feds
Benefits: Establish “benchmark” for plans to be offered through state-exchanges or let feds determine
Enrollment: help/encourage people to get coverage thru Medicaid or exchanges, or do nothing to help
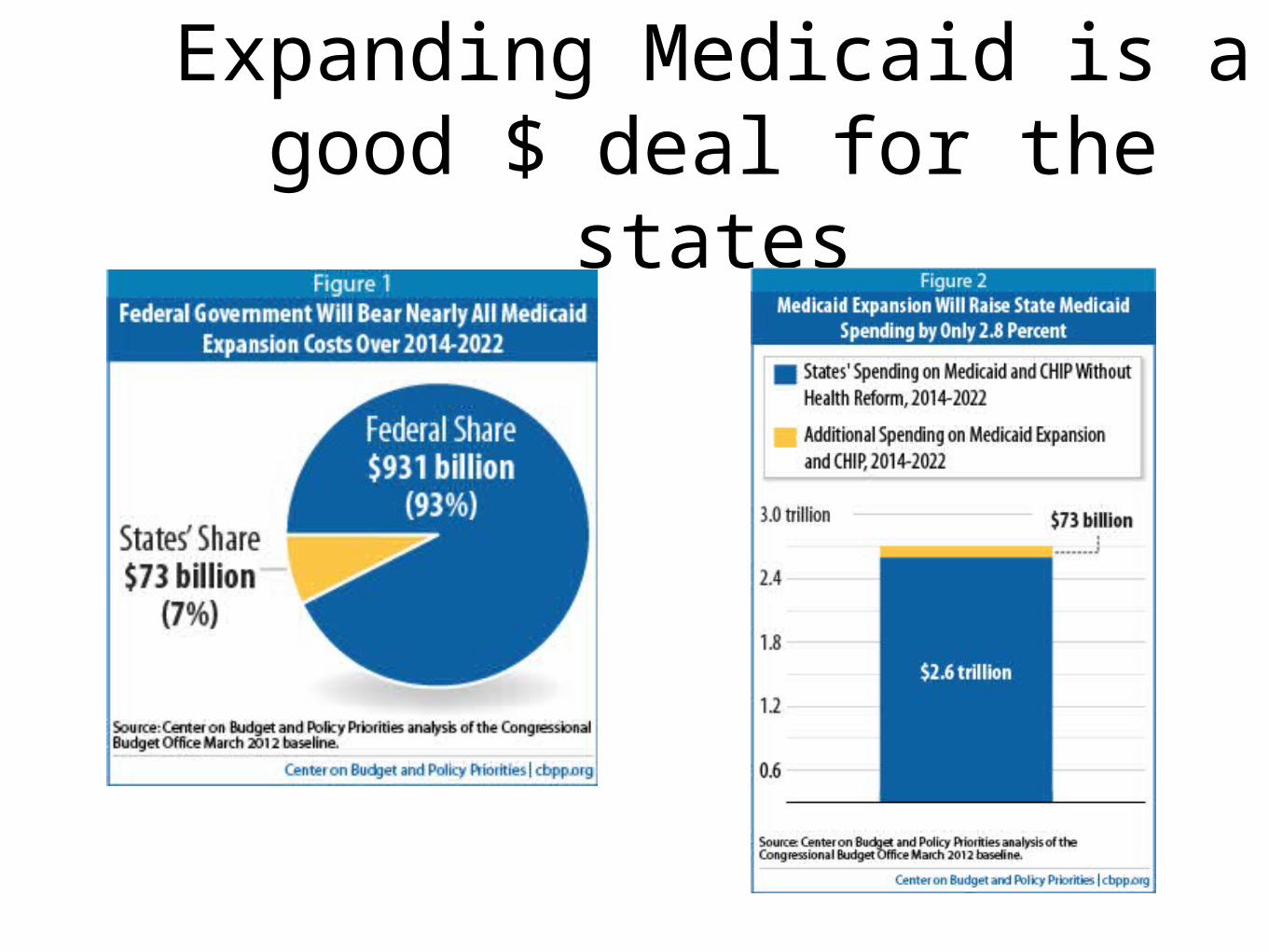
Expanding Medicaid is a good $ deal for the states

Sarah Kliff, Wonkblog, Washington Post, July 3, 2012 http://www.washingtonpost.com/blogs/ezra-klein/wp/2012/07/03/why-hospitals-heart-the-medicaid-expansion-in-one-chart
More on Medicaid=Fewer Deaths, Better Health
Medicaid expansions were associated with a significant reduction in adjusted all-cause mortality (by 19.6 deaths per 100,000 adults, for a relative reduction of 6.1%). Mortality reductions were greatest among older adults, nonwhites, and residents of poorer counties.
Sommers and Baicker, Mortality and Access to Care after State Medicaid Expansions, NEJM, July 25, 2012, http://www.nejm.org/doi/full/10.1056/NEJMsa1202099

ACP’s Medicaid Patient Advocacy Campaign
Cover letter from College leadership, seeking 100% U.S. chapter participation
Concise action plan with one-click links to all supporting materials, presentation slides, instructions and timetable
Customized state-specific reports (available now!) and press releases to be issued by all chapters
http://www.acponline.org/cln/medicaid_campaign.htm
Template and web interface to send the report to each state’s governor and legislators
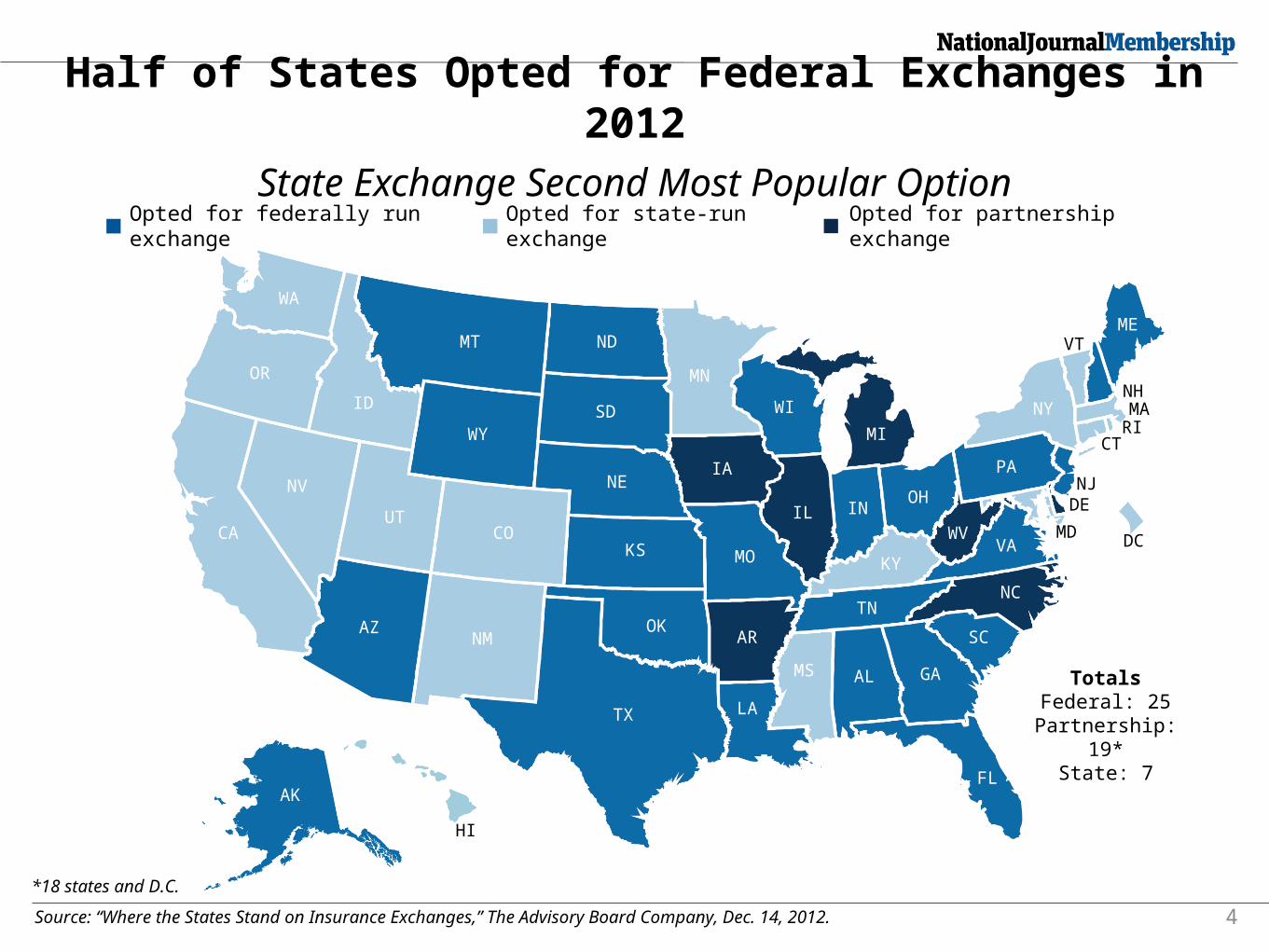
Half of States Opted for Federal Exchanges in 2012
State Exchange Second Most Popular Option
4Source: “Where the States Stand on Insurance Exchanges,” The Advisory Board Company, Dec. 14, 2012.
Opted for partnership exchange
Opted for federally run exchange
Opted for state-run exchange
WA
OR
ID
CA
NV
UT
AZNM
CO
WY
MT ND
SD
NE
KS
OK
TX
AR
LA
MO
IA
MN
WI
IL
AK
INOH
MI
PA
KY
TN
MS AL GA
FL
SC
NC
VAWV
NY
MEVT
NHMARI
CT
NJDE
MD DC
HI
TotalsFederal: 25Partnership:
19*State: 7
*18 states and D.C.

Enrollment“States are rushing to decide whether to build their own health exchanges and the administration is readying final regulations, but a growing body of research suggests that most low-income Americans who will become eligible for subsidized insurance have no idea what is coming.
Supporters of the health-care law say the plan will not be a success without a massive public relations campaign to build awareness.”Many Americans Unaware of Health-care Law Changes, Sarah Kliff, Washington Post, November 21, 2012, http://www.washingtonpost.com/business/economy/many-americans-unaware-of-health-care-law-changes/2012/11/20/ee02b0bc-3272-11e2-9cfa-e41bac906cc9_story.html?hpid=z2
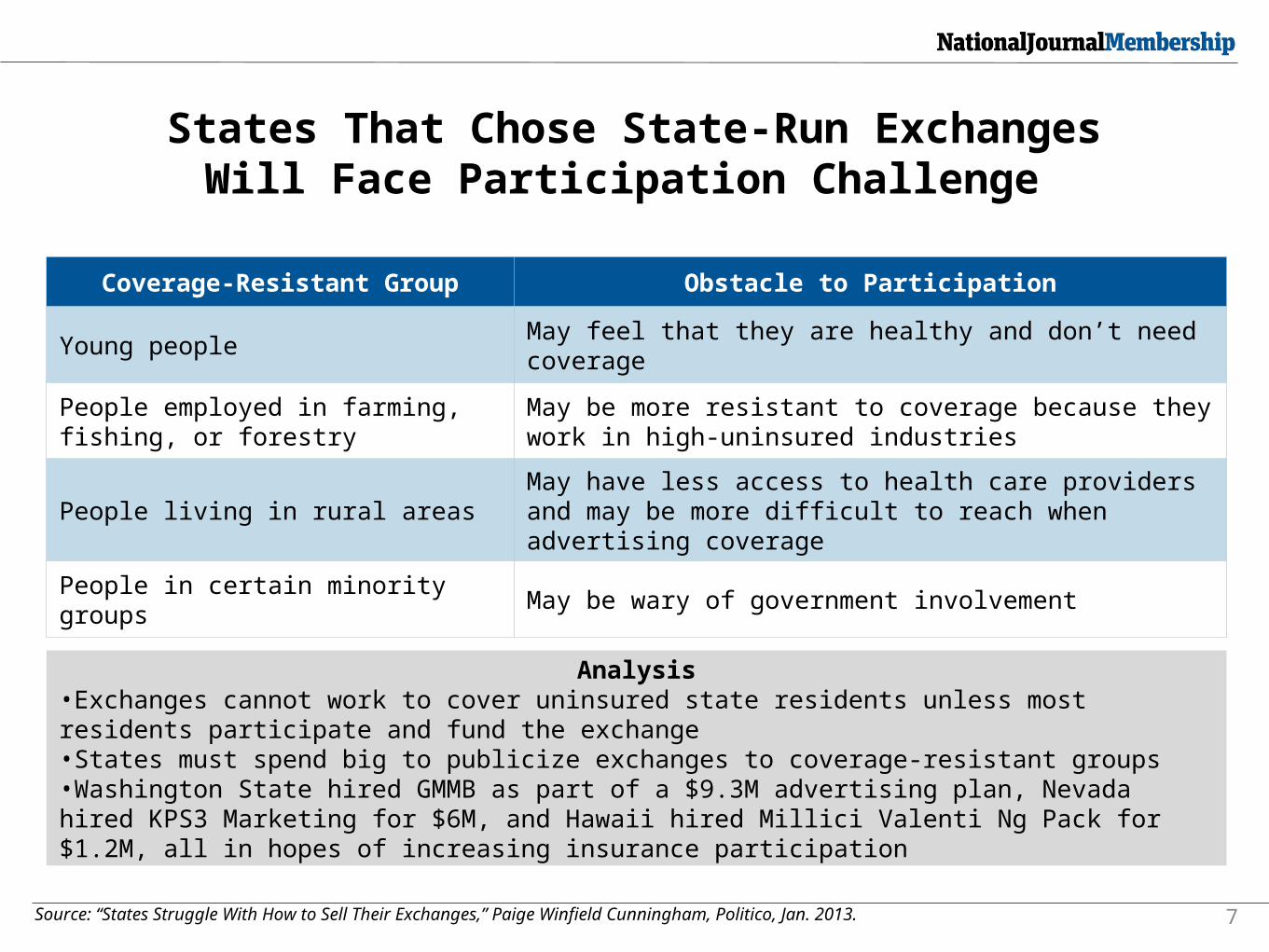
States That Chose State-Run ExchangesWill Face Participation Challenge
7Source: “States Struggle With How to Sell Their Exchanges,” Paige Winfield Cunningham, Politico, Jan. 2013.
Analysis•Exchanges cannot work to cover uninsured state residents unless most residents participate and fund the exchange•States must spend big to publicize exchanges to coverage-resistant groups•Washington State hired GMMB as part of a $9.3M advertising plan, Nevada hired KPS3 Marketing for $6M, and Hawaii hired Millici Valenti Ng Pack for $1.2M, all in hopes of increasing insurance participation
Coverage-Resistant Group Obstacle to Participation
Young peopleMay feel that they are healthy and don’t need coverage
People employed in farming, fishing, or forestry
May be more resistant to coverage because they work in high-uninsured industries
People living in rural areasMay have less access to health care providers and may be more difficult to reach when advertising coverage
People in certain minority groups May be wary of government involvement
New essential benefits rule
Defines benefits that all new individual and small groups must provide
States must select “benchmark” for plans offered through exchanges
• About half the states have already selected the plan they will use as a model, meaning that insurers there can now start designing plans for sale
• States that do not choose a “benchmark” plan will default to one selected by the federal government
Entitlement reform
Having campaigned against Medicare premium support and Medicaid block grants, no prospect that President Obama will agree to them, or that the Senate majority would enact them
But something has to be done: Grand Bargain tied to tax reform/revenue deal? Incremental adjustments?
$60,000
$170,000
$60,000
$357,000
$119,000
$357,000
$0
$50,000
$100,000
$150,000
$200,000
$300,000
$250,000
$350,000
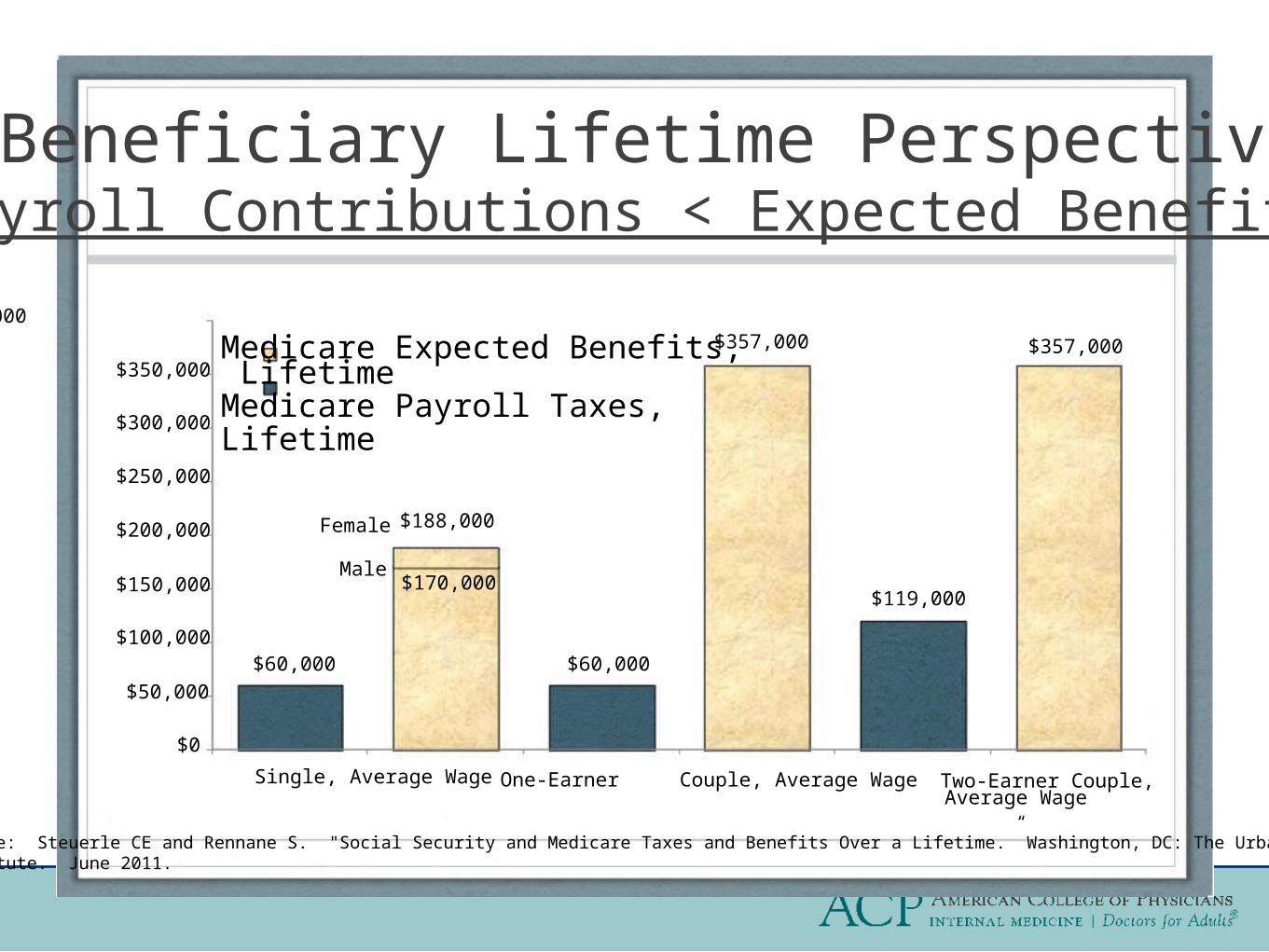
A Beneficiary Lifetime Perspective:Payroll Contributions < Expected Benefits
$400,000
Average Average Wages
Medicare Expected Benefits, LifetimeMedicare Payroll Taxes, Lifetime
$188,000Female
Male
Source: Steuerle CE and Rennane S. "Social Security and Medicare Taxes and Benefits Over a Lifetime.” Washington, DC: The UrbanInstitute. June 2011.
Single, Average WageSingle, Average Wage One-Earner Couple,One-Earner Wage Couple, Average Wage Two-Earner Couple,Two-Earner Couple,
Average Wage
But there is good news on health care costs!
The last time health care costs went up this slowly
Was making hit records!

Good news on health care costs! “Fourth consecutive year of record-low growth
compared to all previous years in the 50-plus years of official health spending data.”
Health care prices had the smallest increase in 14 years, rising in December 2012, “by 1.7 percent compared to December 2011, the lowest year-over-year growth since February 1998.”
Altarum Institute. Health Spending Growth Near 4 percent for Fourth Year Price Growth at 14-Year Low. 7 February 2013. Accessed at www.altarum.org/health-systems-research-news-releases/7Feb13-health-spending-growth-4-percent-price-14year-low

Good news on health care costs! Medicare per capita costs went up by only a fraction of a
percent in 2012 (0.4 percent), much less than the rate of growth in the economy (3.4 percent growth per capita). Over the three year period from 2010-2012, Medicare spending per beneficiary grew an average of 1.9 percent annually, or more than 1 percentage point slower than the average annual growth of 3.2 percent in per capita GDP (that is, at GDP-1.3).
Kronick R, Po R. Growth In Medicare Spending Per Beneficiary Continues To Hit Historic Lows. Office of The Assistant Secretary for Planning and Evaluation, U.S. Department of Health & Human Services. 7 January 2013. Accessed at http://aspe.hhs.gov/health/reports/2013/medicarespendinggrowth/ib.cfm
Budget and sequestration
Fiscal cliff averted (for now)
But cuts, effective March 1, will endanger public health, medical research, workforce, and access
Source: Congressional Research Service. 3
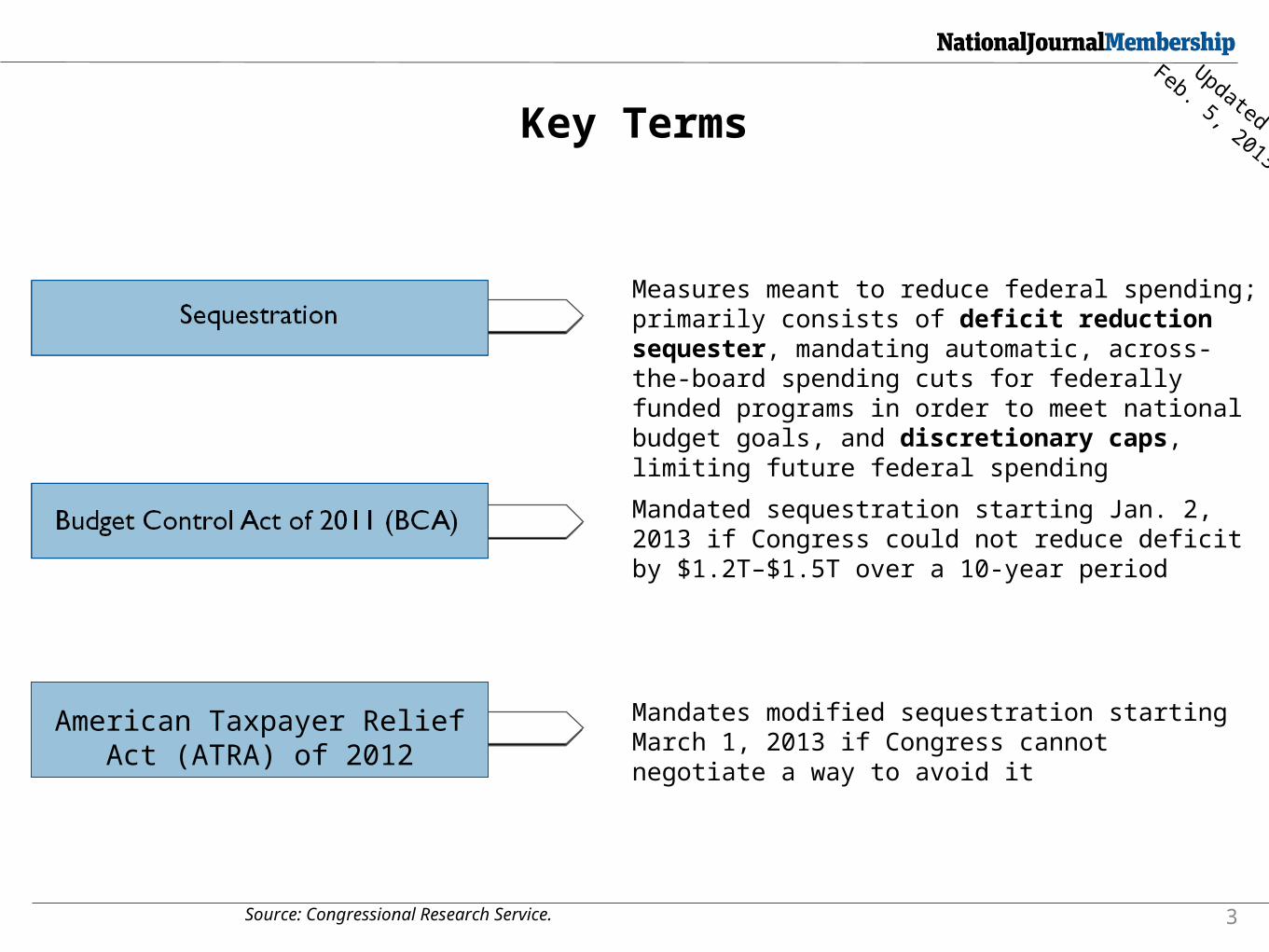
Key Terms
Measures meant to reduce federal spending; primarily consists of deficit reduction sequester, mandating automatic, across-the-board spending cuts for federally funded programs in order to meet national budget goals, and discretionary caps, limiting future federal spending
Mandated sequestration starting Jan. 2, 2013 if Congress could not reduce deficit by $1.2T–$1.5T over a 10-year period
American Taxpayer Relief Act (ATRA) of 2012
Mandates modified sequestration starting March 1, 2013 if Congress cannot negotiate a way to avoid it
Updated
Feb. 5, 2013
Source: Budget Control Act of 2011. 28
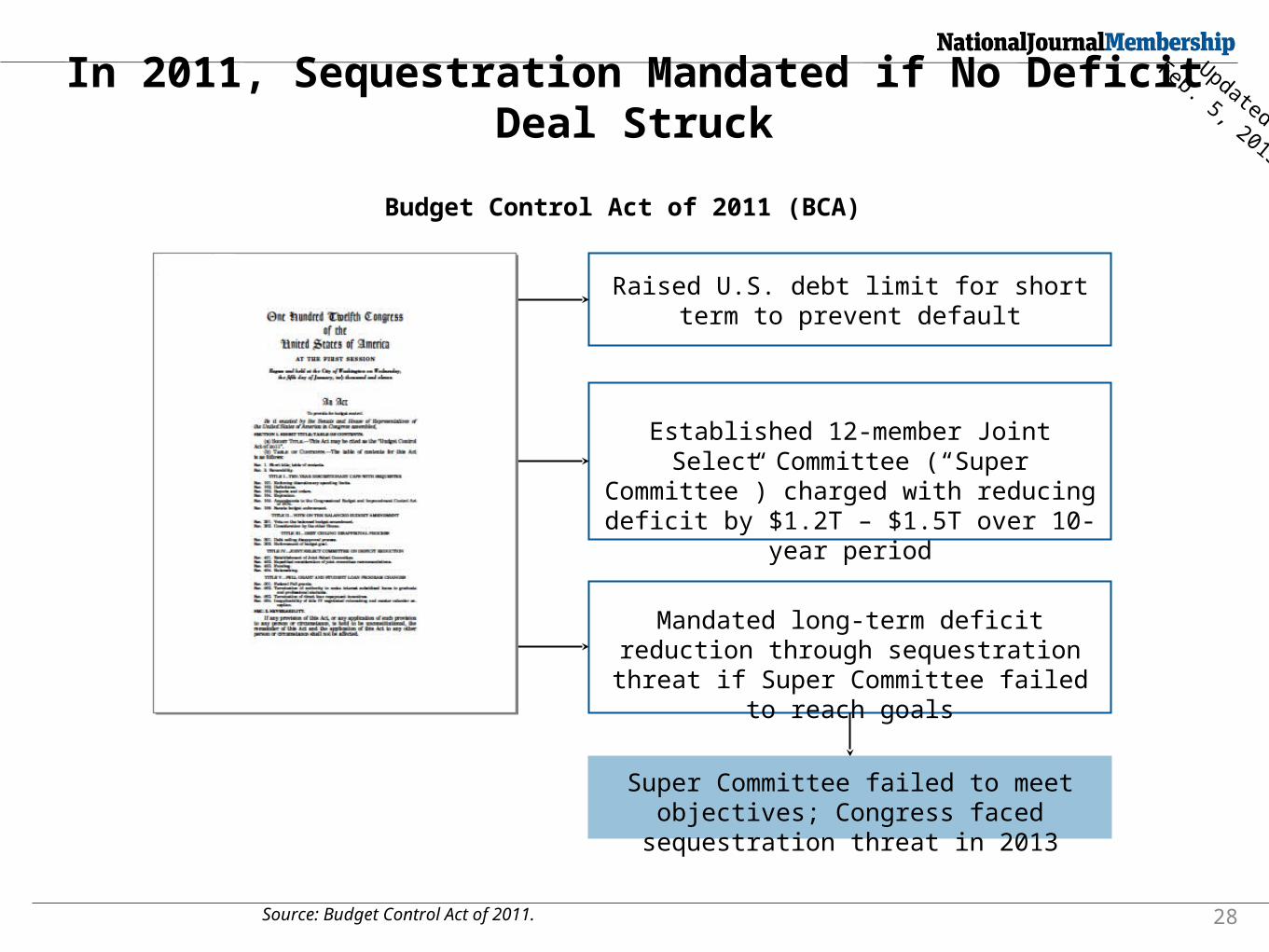
In 2011, Sequestration Mandated if No Deficit Deal Struck
Raised U.S. debt limit for short term to prevent default
Established 12-member Joint Select Committee (“Super Committee”)
charged with reducing deficit by $1.2T – $1.5T over 10-year period
Mandated long-term deficit reduction through sequestration threat if Super
Committee failed to reach goals
Super Committee failed to meet objectives; Congress faced
sequestration threat in 2013
Budget Control Act of 2011 (BCA)
Updated
Feb. 5, 2013
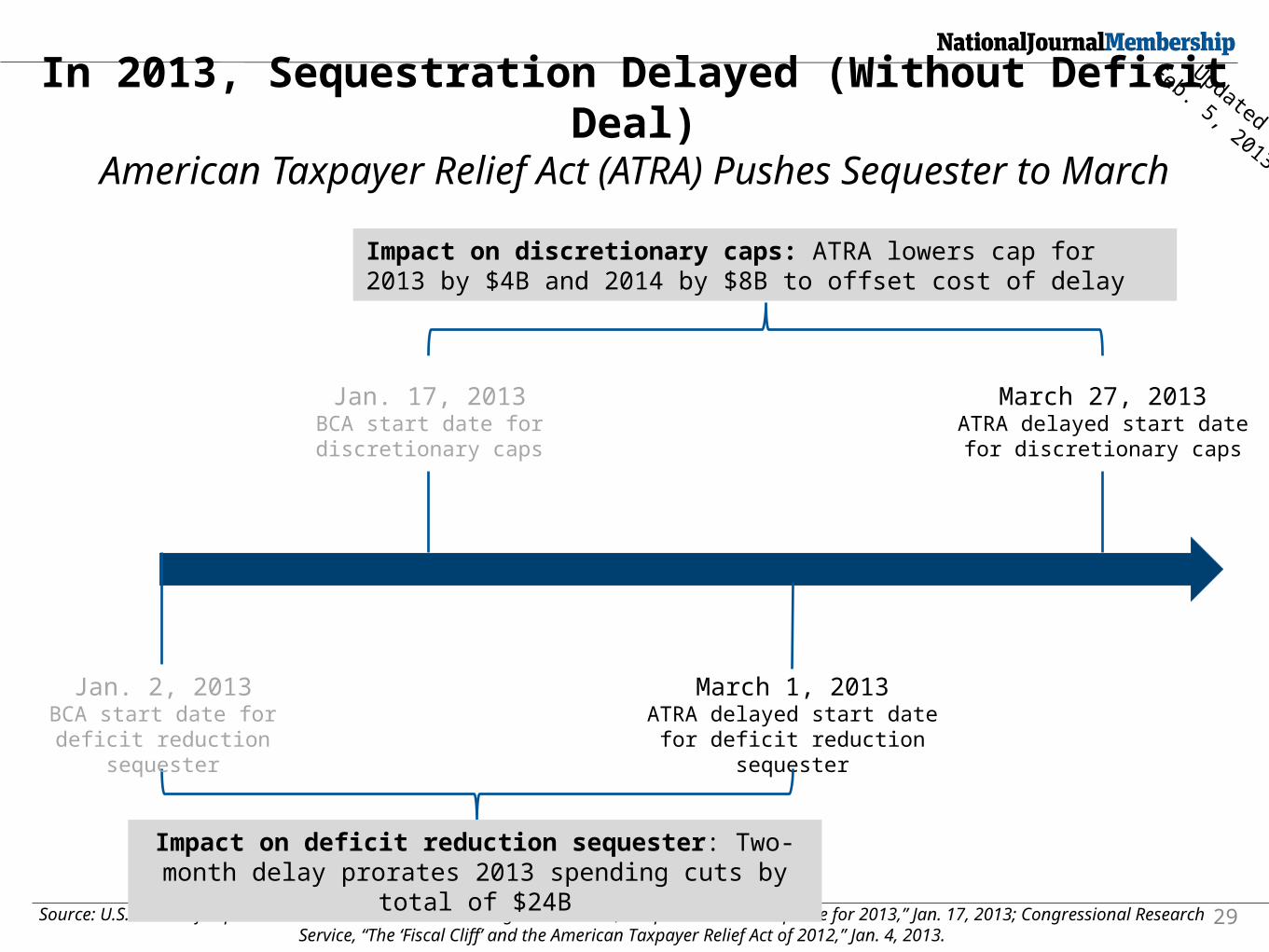
In 2013, Sequestration Delayed (Without Deficit Deal)
Source: U.S. House of Representatives Committee on the Budget Democrats, “Sequestration: An Update for 2013,” Jan. 17, 2013; Congressional Research Service, “The ‘Fiscal Cliff’ and the American Taxpayer Relief Act of 2012,” Jan. 4, 2013.
29
Jan. 17, 2013BCA start date for discretionary caps
March 1, 2013ATRA delayed start date for deficit reduction sequester
March 27, 2013ATRA delayed start date for
discretionary caps
Impact on deficit reduction sequester: Two-month delay prorates 2013 spending cuts by total of
$24B
Impact on discretionary caps: ATRA lowers cap for 2013 by $4B and 2014 by $8B to offset cost of delay
Jan. 2, 2013BCA start date for deficit
reduction sequester
American Taxpayer Relief Act (ATRA) Pushes Sequester to March
Updated
Feb. 5, 2013
ATRA: impact on physicians
No 27% Medicare pay cut (through 2013)
Does not advance permanent SGR reform
Paid for by cuts in disproportionate share payments to hospitals, Medicare Advantage, ambulance services, other non-physician providers
Reduces physician practice expense payments for advanced imaging
ATRA: impact on physicians
Does NOT cancel Medicaid primary care increases to offset cost of blocking SGR cut
Directs HHS to improve advanced clinical data registries for Medicare reporting proposals
Sequestration, postponed only until March, could result in cuts in critically important health programs
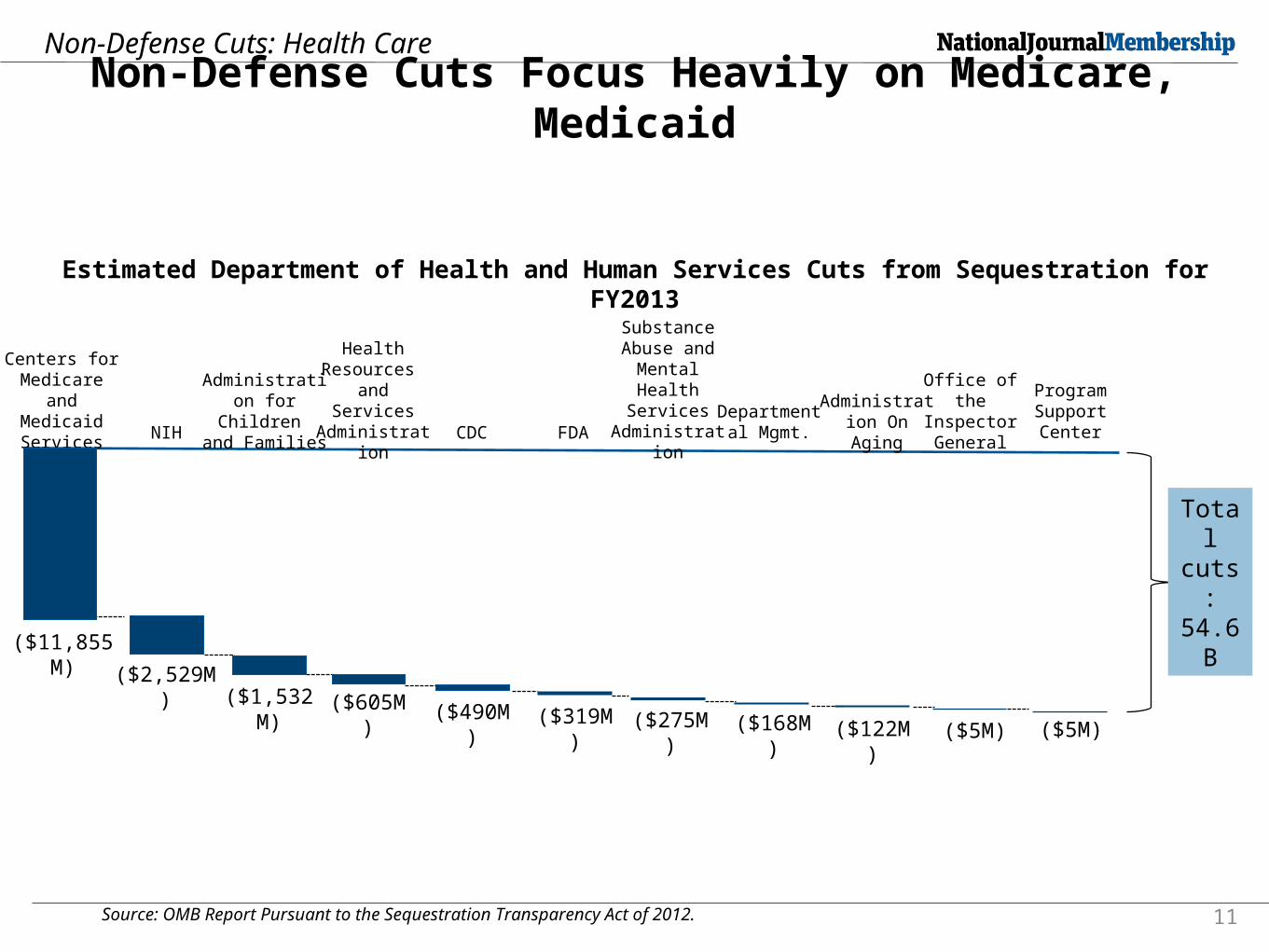
Source: OMB Report Pursuant to the Sequestration Transparency Act of 2012. 11
Non-Defense Cuts Focus Heavily on Medicare, Medicaid
Non-Defense Cuts: Health Care
Estimated Department of Health and Human Services Cuts from Sequestration for FY2013
($11,855M) ($2,529M
) ($1,532M)
($605M)
($490M)
($275M)
Centers for Medicare and
Medicaid Services NIH
Health Resources
and Services Administratio
n FDACDC
Administration for Children and Families
($168M)
Substance Abuse and
Mental Health
Services Administrati
on
Departmental Mgmt.
Administration On Aging
Office of the Inspector General
Program Support Center
($319M)
($122M)
($5M) ($5M)
Total cuts: 54.6
B
Payment reform Policymakers across the spectrum
want to get rid of the SGR (but can’t agree on how to pay for it)
And move away from “volume” to “value”
But FFS will be a component of value-based payments, even as FFS itself will change
“New” approaches
ACOs
Episode-of-care bundles (new rule expected soon)
Risk-adjusted global capitation
PCMH and PCMH-N practices
Light at the end of the SGR tunnel? House GOP committee chairs offer plan to
eliminate SGR, seeking bipartisan support—August vote (?)
Bipartisan Medicare Physician Payment Innovation Act re-introduced, supported by ACP (no cuts for five years, higher updates for E/M, transition to new models)
Medicine unified: 133 physician organizations, including AMA and ACP, offer principles for reform, commitment to new approaches
ACP advocacy
Build upon and ensure coverage gains from the Affordable Care Act
Reduce intrusions on Patient-Physician relationship
Improve fee-for-service AND influence new models of payment
SNHC 2013: improving the system1.Renew commitment at both the national
and state levels to effectively implement the coverage expansions and related policies under the ACA, with particular attention to ensuring the poorest and most vulnerable patients have access to affordable coverage.
2.Replace across-the-board sequestration cuts, prevent future disruptions and instead enact fiscally-and socially-responsible alternatives.
SNHC 2013: improving the system3.Eliminate Medicare’s SGR formula and
support the medical profession’s commitment to transition to new payment models.
4. Implement policies to recruit and retain primary care physicians.
5.Reduce firearms-related injuries and deaths by improving access to mental health services, supporting research, and enacting reasonable controls over access to firearms
SNHC 2013: reducing barriers to patient-physician relationship1.Ensure that any payment reforms have, as
an explicit goal, allowing physicians to spend more appropriate clinical time with their patients.
2. Reforms to hold physicians accountable for the outcomes of care (measurable performance on quality, cost, satisfaction and experience with care) should concurrently eliminate the layers of review and second-guessing of their clinical decisions.

SNHC 2013: reducing barriers to patient-physician relationship3.Harmonize (and reduce to the extent
possible) the measures used in the different reporting programs, work toward overall composite outcomes measures rather than a laundry-list of process measures.
4.Provide more clinically relevant ways to satisfy the requirement that physicians must transition to using ICD-10 codes.
SNHC 2013: reducing barriers to patient-physician relationship5.CMS must reduce administrative barriers,
improve bonuses to incentivize ongoing quality improvements, and broaden hardship exemptions. If necessary, Congress and CMS should consider delaying the penalties for not successfully participating in quality reporting programs, if it appears that the vast majority of physicians will be subject to penalties because of limitations in the programs themselves.
SNHC 2013: reducing barriers to patient-physician relationship6. Improve the functional capabilities of
EHR systems, the ability of those systems to report on quality measures and ensure that those systems improve rather than add to workflow inefficiency.
7. Payers should standardize claims administration requirements, pre-authorization, and other administrative requirements even in advance of, and in addition to, the ACA’s simplification rules.

SNHC 2013: reducing barriers to patient-physician relationship8.Congress should enact meaningful
medical liability reforms including health courts, early disclosure of errors, and caps on non-economic damages.
9. State and federal authorities should avoid enactment of mandates that interfere with physician free speech and the patient-physician relationship.

ACP advocacy on payment reform
It’s not just about new payment models—ACP advocacy has resulted in big wins for internists on improving Medicare and Medicaid fee-for-service

New CMS rules: big wins for IM!
New CPT codes 99495-99496: Medicare will pay physicians for transitional care management services, the non-face-to-face time they and their clinical staff spend on patient cases. Until now, only the face-to-face reimbursed
• National pay of $164-$231, depending on whether a patient is seen within 7 or 14 days of discharge, prior to geographic adjustment
• Combined with other changes in the Medicare fee schedule, total 2013 gain for IM of 4-5% in total Medicare payments
• These gains are on top of ACA’s 10% Medicare primary care bonus (Average of $8000 more each year for qualified internists, 2011-15)
New CMS rules: big wins for IM! Medicaid pay parity rule, effective 2013-2014:
increases payments for evaluation and management and vaccine services to no less than Medicare rates, paid fully by federal government
• CMS agreed with ACP that increases should apply to both primary care internists and IM subspecialists
• Applies to E&M codes 99201 through 99499 to the extent that those codes are covered by the approved Medicaid state plan or included in a managed care contract
• Also, applies to services not covered by Medicare: New and Established Patient Preventive Medicine; Counseling Risk Factor Reduction and Behavior Change Intervention; and Consultations

Medicare to Medicaid fee ratios, by state
<.60 (8 states. 61 ‐.75 (14 states
.76‐.85 (16 states and DC) .86‐1.00 (8 states)
>1.00(3 states)
How Much Will Medicaid Physician Fees for Primary Care Rise in 2013? Evidence from a 2012 Survey of Medicaid Physician Fees, Kaiser Family Foundation, December 2012
ORG
ACP: “go to” resource for members to prepare for changes Practical guides
Social media
Policy summaries
Advocate newsletter
Coming soon: timeline of pending changes (regulation, payment, MOC) and promotion of resources from ACP

NEWLY UPDATED!

http://advocacyblog.acponline.org/
Summary
2012 election: the ACA is here to stay, only a minority of voters favor full repeal, but electorate remains divided, and law remains deeply unpopular in some states
States are the new battleground: decisions on Medicaid and exchanges may determine how effective the ACA is in covering uninsured
Summary
Coming up: new battles on spending and revenue, immediate cuts to essential programs including 2% Medicare pay cut
Entitlement reform will (must) happen—but how and when? Cuts in GME, other ACP priorities?

Summary
ACP advocacy: improve the system, reduce barriers to patient-physician relationships
ACP advocacy is paying off: big wins for internists in Medicare and Medicaid pay
The destination
“A nationwide program is needed to assure access to health care for all Americans, and we recommend that developing such a program be adopted as a policy goal for the nation. The College believes that health insurance coverage for all persons is needed to minimize financial barriers and assure access to appropriate health care services.” Ginsburg, et al, American College of Physicians, Position Paper, Annals of Internal Medicine, May 1, 1990 www.annals.org/search?fulltext=ACP+universal+health+insurance&submit=yes&x=15&y=9
Elaine Dickinson (flight attendant): There's no reason to become alarmed, and we hope you'll enjoy the rest of your flight. By the way, is there anyone on board who knows how to fly a plane?