-
8/14/2019 Tugas Kuliah Implant .txt
1/3
Socket preservationSocket preservation is a relatively new term
in implantdentistry, which implies the placement of
variousimplantable materials within extraction sockets tomaintain
the socket anatomy. To date, there isinconclusive evidence that
this procedure maintainsthe original socket dimensions. In
contrast, evidenceexists that placement of foreign materials
intoextraction sockets may interfere with normal boneformation (6,
8). Iasella et al. (36) compared normalsocket healing with those
grafted with demineralizedfreeze-dried bone and covered with a
collagen barriermembrane. Unaugmented sockets decreased in widthby
an average of 1.7 mm, while grafted sites decreasedby 1.2 mm (a
difference of 0.5 mm). The quantity ofbone observed on histological
analysis was slightlygreater in preservation sites, although these
sites includedboth vital and nonvital bone. Other researchershave
compared alveolar ridge dimensions andhistological characteristics
of ridges preserved withtwo different graft materials (83).
Twenty-four subjects,each requiring a nonmolar extraction and
delayedimplant placement, were randomly selected toreceive ridge
preservation treatment with either an
allograft in an experimental putty carrier plus a calciumsulfate
barrier, or a bovine-derived xenograftplus a collagen membrane.
Horizontal and verticalridge dimensions were determined using a
digitalcaliper and a template. At 4 months post-extraction,
atrephine core of bone was obtained for histologicalanalysis.
Allograft mixed with an experimental puttycarrier produced
significantly more vital bone fill thandid the use of a xenograft
with no carrier material.Ridge width and height dimensions were
similarlypreserved with both graft materials.There is evidence that
resorbable barriers, withoutconcomitant grafting, reduce alveolar
ridge resorption
after tooth extraction (45, 85). Following elevation ofbuccal
and lingual full-thickness flaps and extractionof teeth,
experimental sites were covered with bioabsorbablemembranes;
control sites received nobarrier membrane. Titanium pins served as
fixed referencepoints for measurements. Flaps were advancedto
achieve primary closure of the surgical wound, andno membrane
exposure occurred during the course ofhealing. Re-entry surgery
performed after 6 monthsshowed that experimental sites presented
with significantlyless loss of alveolar bone height, more
internalsocket bone fill, and less horizontal resorption of
thealveolar bone ridge. This study suggests that treatment
of extraction sockets with membranes made of glycolideand
lactide polymers is of value in preservingalveolar bone in
extraction sockets and preventingalveolar ridge defects. Use of
barrier membranes maybe indicated to minimize crestal alveolar
boneresorption in cases where dental implants are not partof the
treatment plan. However, placement of implantsinto membrane-treated
sites may cause limitedosseointegration as the result of formation
of suboptimalbone. Until there is sufficient evidence that
-
8/14/2019 Tugas Kuliah Implant .txt
2/3
barrier membranes can maintain socket anatomywithout interfering
with osseointegration, cautionshould be exercised when using such
treatment inimplant dentistry.84Becker & GoldsteinSoft tissue
management forimmediate implantsPrimary flap closure over
immediately placed implantswas considered important for many years
(4,22, 31). The discrepancy of size and form between theextraction
socket and an immediate implant ensuresthat a space usually exists
around the coronal portionof the implant. Frequently, pre-existing
bony defectscan also be found in the extraction area. Dependingon
size, the bony defects may be treated withregenerative techniques
(5, 49). Soft tissue coverageof the implant area was considered
necessary toachieve bone fill adjacent to the implant. The
presenceof interdental bone, soft tissue anatomy, smileline,
occlusion, and interdental space are all importantfactors in the
placement of immediate implantsin the esthetic zone (30, 39, 47,
66, 74).Various surgical techniques have been proposed to
achieve primary soft tissue closure with immediateimplants (4,
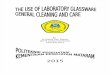
70, 71, 73). Use of a rotated buccal flap(A) (B)(C) (D)(E) (F)Fig.
3. (A) Maxillary second bicuspid with a verticalfracture (arrow)
and buccal dehiscence. (B) A machinedsurfaceimplant has been
installed in the osteotomy.There were 13 threads exposed and the
implant was stable.(C) A collagen membrane has been adapted over
theallograft and implant site. (D) A pedicle flap has beenrotated
from the palate and sutured over the implant andgrafted site. (E)
At 6 months the implant was uncovered
and the final restoration was placed. There is slight
marginalinflammation. (F) Radiograph taken after 6 monthsof healing
and before final restoration.85Immediate implant placementfrom an
adjacent tooth can be used to achieve closureover implants placed
at the time of extraction.This procedure can be applied for single
or multipleimplant sites and can be employed in conjunctionwith
membrane barriers or various grafting materials.The main
disadvantage of this technique is therequirement for an adequate
width of keratinizedmucosa and vestibule depth. Edel (27) was the
first
to publish on the use of a connective tissue graft forcoverage
of immediately placed implants. A potentialproblem is the
limitation of donor tissue size. Inperiodontal plastic surgery, an
acellular dermalmatrix allograft is sometimes employed as an
alternativeto autologous connective tissue. Acellulardermal matrix
has also been used alone or withvarious grafting materials to cover
immediatelyplaced implant sites (28, 29, 64). Gingival graftshave
been used as well to augment sites that have
-
8/14/2019 Tugas Kuliah Implant .txt
3/3
received immediately placed implants. Estheticoutcomes from this
technique are good, but theprocedure requires a second surgery for
graft procurement(40). The palatal advanced flap or pediculatedflap
is another useful surgical technique formaxillary immediate implant
cases (Fig. 3A F) (32,48, 54 59). The technique provides adequate
tissuemobility and bulk, facilitating a complete, precise,and
highly predictable coverage of the extractionsite in large defect
areas, and in cases of multipleimplants. The main disadvantage of
this techniqueis the prolonged and uncomfortable secondarypalatal
tissue healing.ConclusionsThis paper has reviewed the history,
predictability,rationale, treatment planning steps, and
treatmentfor implant placement immediately after toothextraction.
Multicenter studies have validated thepredictability of placing
implants at the time ofextraction provided these procedures are
appropriatelyplanned. To date, evidence for placement ofbone
substitutes adjacent to small bone defects relatedto immediately
placed implants indicates thatthis technique appear safe, although
these materials
do not appear predictably to promote osseointegration.There is
insufficient evidence that socket preservation procedures
predictably maintain socketanatomy without crestal resorption. Bone
substitutesimplanted into extraction sockets may interfere
withnormal bone healing and ultimately osseointegration.A minimally
invasive surgical technique in theplacement of immediate implants
offers severaladvantages and should be employed
whereverpossible.