Embed Size (px)
Citation preview
UCLPartners Children, Young People & Maternal Health
Programme Overview
Susan Crane, Programme Manager CYM
Tuesday 10 November 2015
2
Key Objectives for UCLPartners CYM Programme 2015/16
1. Improve child patient safety and parental capacity (Prevention)
2. Improving partners’ access to CYP research and information (Increase personalisation)
3. Improving care for CYP with long term conditions (New models of care)
3
Realising the benefits of the Health Visitor Workforce (HEE NCEL)
New Models: 0-5 Health Programme• Start at the Beginning: A Research pilot trial of a nutrition and lifestyle m-health
intervention in primary care for women planning a pregnancy
• The Perinatal Mental Health Value Scorecard: A quality Improvement pilot of a coproduced value score card of outcomes that are meaningful to all stakeholders and outcome measures that matter most to parents
• DIY Health Model: A Health Education Delivery model that uses co-production as a central principle in empowering parents of children aged 0-5 years with a focus on minor ailments
4
Key Findings / Outcomes
The Perinatal mental health score card • Improve adherence to best practice and identify areas of change to current practice
• Used to improve patient experience
• Economic model: cost-effectiveness of screening for peri-natal depression with necessary follow-up or onward referral post-implementation of the scorecard vs. pre-implementation
• Significant increase in screening for both antenatal and postnatal depression and was shown to be cost-effective in the modelled cost-effectiveness analysis
• Implementation of the scorecard appeared to reduce costs (£3,357) and increase QALYs (0.1 to 0.4)
5
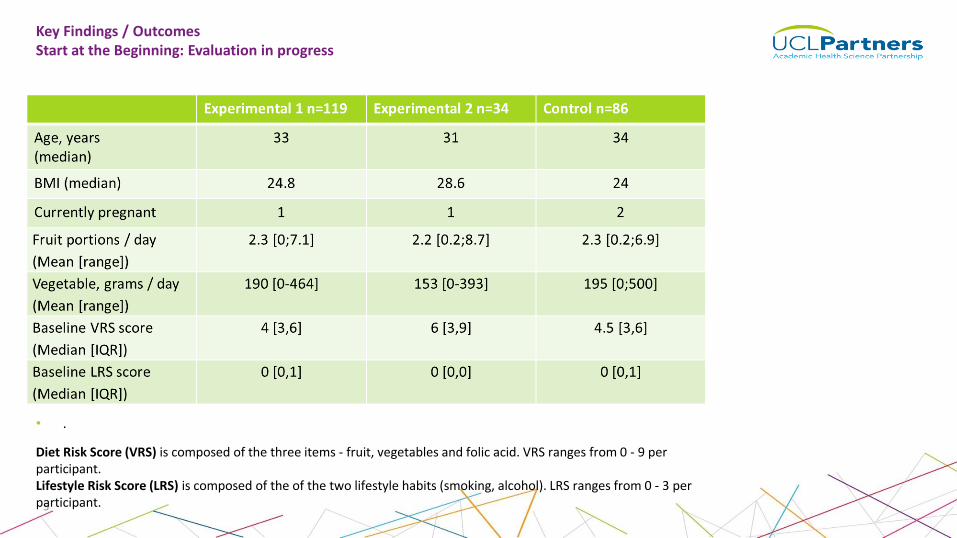
Key Findings / Outcomes Start at the Beginning: Evaluation in progress
• .
Diet Risk Score (VRS) is composed of the three items - fruit, vegetables and folic acid. VRS ranges from 0 - 9 per participant.Lifestyle Risk Score (LRS) is composed of the of the two lifestyle habits (smoking, alcohol). LRS ranges from 0 - 3 per participant.
6
Key Findings/ OutcomesDIY Health Model: Managing Minor ailments in Children 0-5 years
Early qualitative outcomes showed an improved level of confidence in parents
• The aim was to assess if DIY health led to a reduction in GP attendances.
• A small sample size (29 patients) meant that it was hard to assess if any significant differences occurred after parents attended DIY health sessions.
• Total cost of delivering DIY Health was £13,464.96. The cost per session was £561.04 (based on 12 sessions) or £464.31 per child overall (and £19.35 per session).
• Giving parents the skills to manage common illnesses may lead to noticeable improvements in parental anxiety. The intervention may be cost-effective if it leads to significant improvement in parental well-being. Unfortunately this was not assessed as part of the evaluation.
The Schools Health & Wellbeing Research Network
• A free-to-join Network to broker new collaboration between schools and researchers.
• The purpose: to develop research of the highest quality to inform practice, ultimately improving outcomes for children and young people.
• Hosted by UCL Partners for first 18 months; supported by 7 universities and developed in consultation with children and young people.
• Membership of 75 schools, across N & E London, Essex & Herts, & 30 research programmes supported.
• Primary focus = health & wellbeing, (physical, mental and emotional health, social wellbeing & relationships).
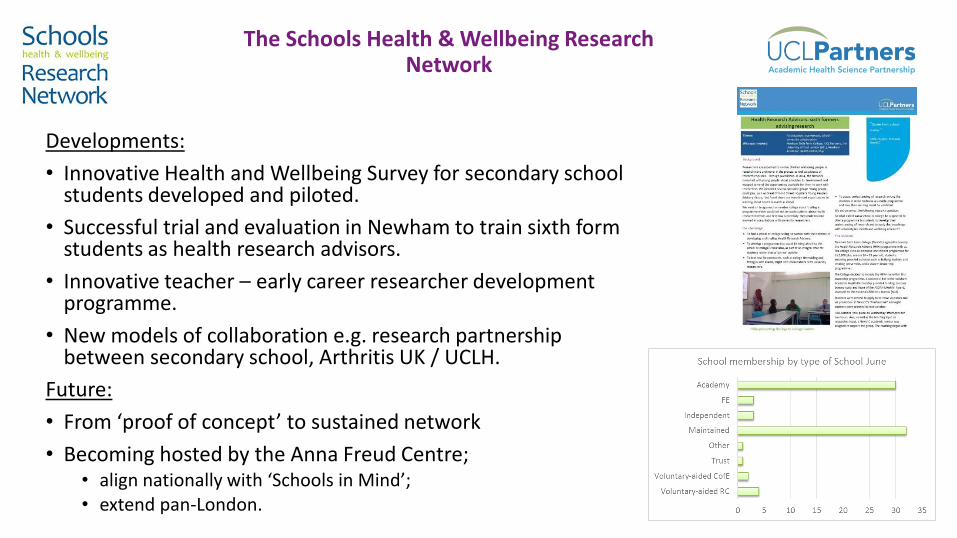
The Schools Health & Wellbeing Research Network
Developments:
• Innovative Health and Wellbeing Survey for secondary school students developed and piloted.
• Successful trial and evaluation in Newham to train sixth form students as health research advisors.
• Innovative teacher – early career researcher development programme.
• New models of collaboration e.g. research partnership between secondary school, Arthritis UK / UCLH.
Future:
• From ‘proof of concept’ to sustained network
• Becoming hosted by the Anna Freud Centre; • align nationally with ‘Schools in Mind’; • extend pan-London.

S.A.F.E. PartnershipClosing the Gap in Paediatric Safety (update)
NHS Trust: GOSH, Royal Free, Bart’s Health, Alder Hey, Sheffield, Royal Manchester, Birmingham, Luton & Dunstable, North Middlesex, Whittington Health, Evelina, Watford
S.A.F.E. Partnership
Expanding S.A.F.E from one to three waves:• Wave 1, original 12 sites (6 SCH, 6 DGH)• Wave 2, seven new sites (3 SCH, 4 DGH)• Wave 3, nine new sites (2 SCH, 7 DGH)
Deliverables• Interim Evaluation Report• Huddle Reflection / Observation tool• Developed S.A.F.E Toolbox, comprising six chapters:
– Introducing Quality Improvement; Theories of Patient Safety; Structured Communication; Recognising Deterioration Early; Implementing Huddles; Evaluating Impact
The Huddle Suite• Escalate leaders daily safety brief• Mitigate ward safety huddle• Identify ward bedside huddles
Evaluating S.A.F.E
Qualitative Evaluation
• Four sites participating in observed huddles, staff and parent/patient interviews.• Initial themes identified:
– Flattened hierarchies, though not prevalent– Improve clarity and communication, including specific language around risk– Encourage proactive management of risks
Quantitative Evaluation
• No emerging patterns in safety indicator data.• Collecting Staff Survey and Experience of Care (PREM) data.
Second and Third Waves• Wave Two: Basildon and Thurrock University Hospital; Great North Children’s Hospital, Newcastle; Leicester Royal
Infirmary; Princess Royal University Hospital, Orpington; Royal Lancaster Infirmary; Southampton Children’s Hospital; and York Teaching Hospital
• Wave Three: Bedford Hospital; John Radcliffe Hospital, Oxford; Leeds Children’s Hospital; Nottingham Children’s Hospital; Ormskirk Hospital; Rotherham Hospital; Royal United Hospital, Bath; Torbay Hospital; and University College London Hospital
12
London Neonatal Operational Delivery Network
Reducing variation in practice / improving access
(Update)
• Development & implementation of Band 5 neonatal nurse competency toolkit
- Toolkit aligned to RCN Career framework. Identifies the skills, knowledge and resourcesrequired for assessing competency of newly qualified nurses.
- Skills are evidenced through the roll-out of London wide nurse induction days
- Where gaps are identified neonatal nurses work with their PDNs / senior nurses to improve skills straight away
Key Findings: Works towards consistency in care. Highlights to novice nurses the role theyPlay in the delivery of high quality neonatal care. Novice nurses feel part of the wider London system and share best practice
13
• Enhanced Peer Review of Infection Prevention & Control (NCEL Pilot)- Review to establish high level overview of infection prevention
control managements and standards
- Development of audit tool which took into account the current research base, NHScampaigns, recommendations and standards
- Enhanced collaboration between units, uplifted and supported openness and interaction. ‘Fresh eyes’ approach to audit
- Following publication of reports units are encouraged to review and assess their practiceagain.
http://www.infantgrapevine.co.uk/journal_article.html?RecordNumber=6818&number=62
Key findings: The variation in infection control management despite nationallyAgreed policy. Individual trust level recommendations published, units supported to make The necessary changes. For roll-out across NWL and South London 2016.
14
• Reducing length of stay on neonatal units
- QiPP project to increase the number of babies discharged at < 36 weeks gestation.
- Consistent approach to discharge planning
- Improve patient flow / efficiency / cot utilisation
- Effective resource utilisation / role
- Potential for reduced admissions to A&E / readmission to NNU
Key findings: Helps facilitate national standard that 95% of women booked should have all
Their neonatal care within the ODN. Evaluation due March 2016.
15
Child Health Informatics Platform (CHIP) Overview
• Commissioners of children’s services can lack the capacity, time or opportunity to find the necessary data to make the most informed commissioning decisions.
• UCLPartners is developing a child health data platform to move beyond data capture to the interpretation & presentation of data in a meaningful, relevant way to inform LAs/CCGs on how to provide the best care for children.
• Based on successful UCLPartners Mental Health Informatics Platform
• In consultation with Public Health England and a wide range of child health data experts across London
16
Why is CHIP needed?
• Decrease the mortality and morbidity experienced in the 1.34 million children within our geography and beyond
• Improve the life chance of children aged under age 19 and promote better health and wellbeing
• Increase the social and economic potential of children with poor health outcomes and decrease healthcare spending through cost analysis and early intervention
• Analyze the indicators of poor health outcomes experienced by children due to disadvantage, which occur at birth and accumulate throughout their lifespan
17
Indicators of Poor Health Outcomes
• Inequality is the main cause of inadequate health outcomes
o It affects infant mortality, obesity, childhood accidents, and teenage pregnancy (for example)
• Indicator types for specific outcomes
o Development, education, health, home life, lifestyle, mental health, perinatal, population, social care, air quality and green spaces
• Looking at this data through 5 year age bands from childhood through teenage years
18
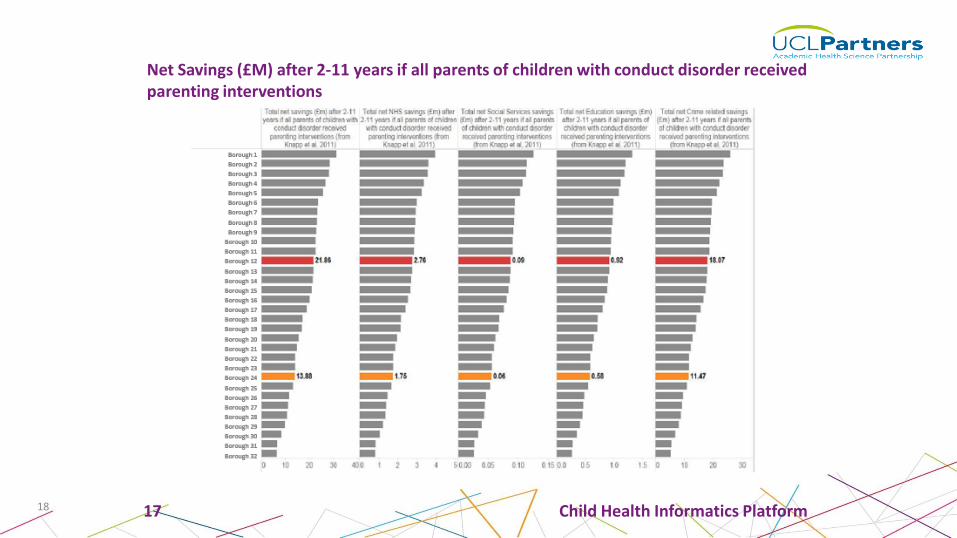
Net Savings (£M) after 2-11 years if all parents of children with conduct disorder received parenting interventions
17 Child Health Informatics Platform

Children & Young People’s Services: reminder of the case for change Dec 2014 Newham CCG Diabetes Youth Project – November 2015 Update
VISIONTo co-design diabetes services for youth with young people, based on a modern andsustainable approach, achieved through cross-organisational partnership working.
PURPOSE AND JUSTIFICATION
• Newham has the youngest borough population in the UK andhosts the highest prevalence of diabetes in young peopleunder 25 in the country.
• An UCLPartners sponsored event in December 2014 broughttogether young people and their families who outlinedconcerns with the existing service model and madeimprovement recommendations.
• This project is designed to explore those ideas in more detail
and drive them forward to implementation. Partnership organisations
PHASES
This project has bold ambitions to change the way that young
people diabetes services are commissioned across London.
The ambition is segmented into three phases:
Phase 1
A. Newham CCG implemented guidance 3
B. Implementation across Tower Hamlets and Waltham
Forest
Phase 2 Implementation across UCLPartners member
organisations
Phase 3 London-wide adoption of commissioning
guidance.
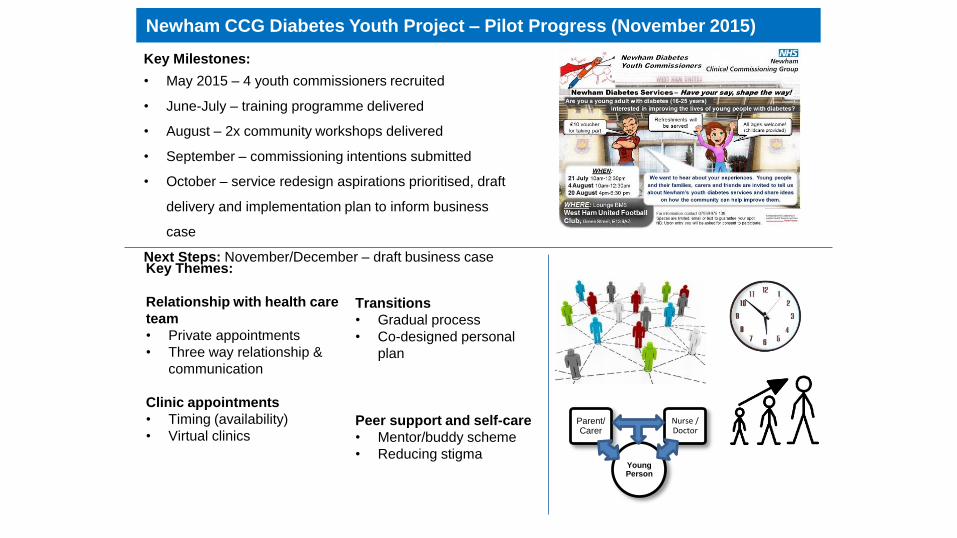
Children & Young People’s Services: reminder of the case for change Dec 2014 Newham CCG Diabetes Youth Project – Pilot Progress (November 2015)
Young Person
Parent/ Carer
Nurse / Doctor
Key Themes:
Relationship with health care
team
• Private appointments
• Three way relationship &
communication
Clinic appointments
• Timing (availability)
• Virtual clinics
Key Milestones:
• May 2015 – 4 youth commissioners recruited
• June-July – training programme delivered
• August – 2x community workshops delivered
• September – commissioning intentions submitted
• October – service redesign aspirations prioritised, draft
delivery and implementation plan to inform business
case
Next Steps: November/December – draft business case
Transitions
• Gradual process
• Co-designed personal
plan
Peer support and self-care
• Mentor/buddy scheme
• Reducing stigma
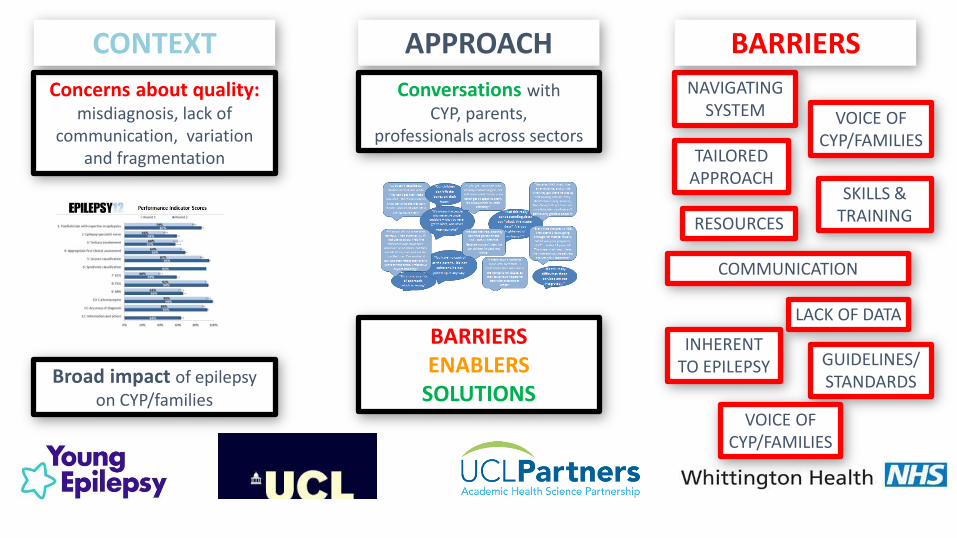
Concerns about quality: misdiagnosis, lack of
communication, variation and fragmentation
Broad impact of epilepsy on CYP/families
CONTEXT APPROACH
BARRIERSENABLERS
SOLUTIONS
Conversations with CYP, parents,
professionals across sectors
NAVIGATING SYSTEM
BARRIERS
RESOURCES
SKILLS & TRAINING
TAILORED APPROACH
COMMUNICATION
VOICE OF CYP/FAMILIES
INHERENT TO EPILEPSY GUIDELINES/
STANDARDS
LACK OF DATA
VOICE OF CYP/FAMILIES
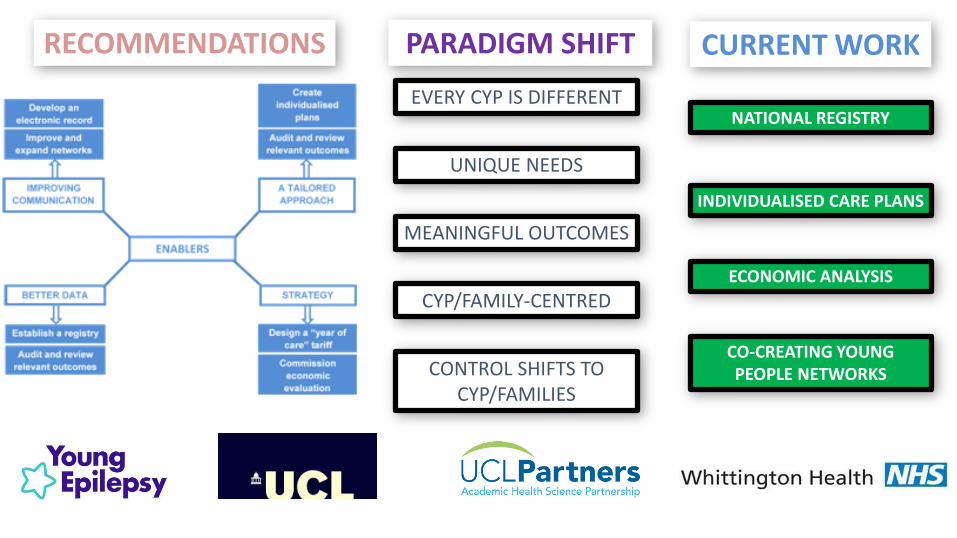
RECOMMENDATIONS PARADIGM SHIFT
EVERY CYP IS DIFFERENT
UNIQUE NEEDS
CYP/FAMILY-CENTRED
MEANINGFUL OUTCOMES
CONTROL SHIFTS TO CYP/FAMILIES
CURRENT WORK
NATIONAL REGISTRY
ECONOMIC ANALYSIS
CO-CREATING YOUNG PEOPLE NETWORKS
INDIVIDUALISED CARE PLANS
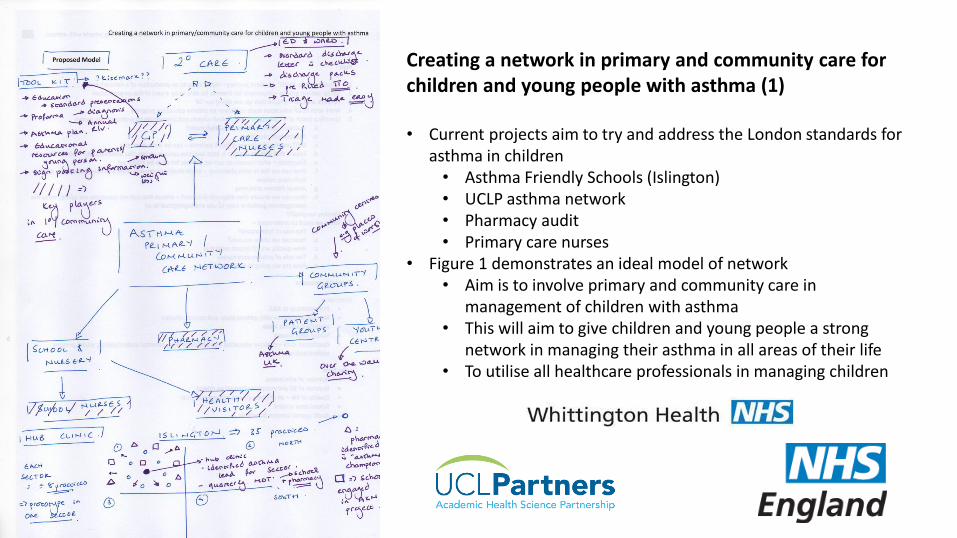
Creating a network in primary and community care for children and young people with asthma (1)
• Current projects aim to try and address the London standards for asthma in children• Asthma Friendly Schools (Islington)• UCLP asthma network • Pharmacy audit• Primary care nurses
• Figure 1 demonstrates an ideal model of network • Aim is to involve primary and community care in
management of children with asthma• This will aim to give children and young people a strong
network in managing their asthma in all areas of their life • To utilise all healthcare professionals in managing children
Cu
rren
t av
enu
es a
nd
p
rop
osa
ls• Improvement to current management in A&E
• Improved proforma• Teaching – using moodle to create a module• Discharge packs that are age appropriate• Discharge summary template and ensuring emailed to Primary care to allow 48hr
review
• Primary care• Creating hubs (7-8 practices) • MDT with clinics to allow teaching and discussions• ‘Upskill’ practice nurses• Education resources via RCGP• Primary care tool kits (emis proforma for annual reviews)
• Regional networks• UCLPartners Asthma Network• Strategic clinical networks
UCLPartners, Creating a network in primary and community care for children and young people with asthma (2)
25
THANK YOUFor more information please contact:
Carol Irish, Health Visitors [email protected]
Chris Owen, Schools Network [email protected]
Suzanne Sweeney, Neonatal ODN [email protected]
Darren Cooper, S.A.F.E., RCPCH [email protected]
Susan Crane, CYM Programmes [email protected]
Rachelle Ferrer, Diabetes Network [email protected]
Dr. Amit Bali, Epilepsy Network [email protected]
Dr. Reena Bhatt, Asthma Network [email protected]
www.uclpartners.com
@uclpartners