Embed Size (px)
Citation preview

For information about the strategies above orany of the developments discussed on thispage, contact your Sibson consultant, or sendan e-mail to [email protected]
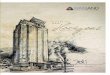
TREND AND CPI
Medical Rx CPI-Urban
0
2
-2
4
6
8
10
12%
Medical PPO
Health Plan Cost Trend, 2008-2010 Actual and 2011-2012 Projected
Consumer Price Index (CPI) through May 2012Rx Dental DPO
For 2012, medical and prescription drug plan cost trend rates are projected to decline from levels forecast for 2011.
Sources: 2012 Sibson Health Plan Cost Trend Survey(http://www.sibson.com/publications/surveysandstudies/2012trendsurvey.pdf) and Bureau of Labor Statistics for CPI(http://www.bls.gov/cpi/)
Trend is the forecasted change in claims cost determined by insurance carriers, managed careorganizations (MCOs), pharmacy benefits managers(PBMs) and third party administrators (TPAs). Trendcan be influenced by a variety of factors includingprice inflation, the leveraging effect of copayments,cost shifting and utilization. The CPI is a measure ofthe average change over time in the prices paid byurban consumers for a market basket of consumergoods and services. The CPI is often used as aneconomic indicator.
THE AFFORDABLE CARE ACT (ACA) AND COMPLIANCE NEWS
Enhance prescription drug coverage while manag-ing plan costs. Several new strategies can aid plansponsors in overseeing their plan’s prescription drugbenefit. One strategy is reviewing retail pharmacy network access and the potential savings associated with adopting a more narrow retail drug distribution network. Another is maximizing the utilization and costeffectiveness of generic medications by reviewing PBMcontracts for pricing applicable to the generic versions of brand-name drugs coming off patent. Drug manufac-turers are increasing plan sponsor costs by usingdirect-to-consumer “couponing” efforts to extend abrand-name medication’s lifespan. Plan sponsors cancounter these efforts by instituting plan design changesthat block or restrict coverage for couponed drugs andmotivate participants to select available and appropriategeneric and therapeutic alternatives.Address the implementation steps needed to produce SBC drafts and templates. Plan sponsorsshould determine whether their plans must provide anSBC, and for which benefit packages. They shouldalso address SBC production when there are multipleservice providers, such as a self-insured medical planadministered by a TPA and a separate PBM. Plansponsors will also need to create coverage examplesto simulate how the plan would process the claims for two specific benefits scenarios: maternity and Type 2 diabetes.Refine competing provider networks. Sibson has foundthat as many as 10 percent of listed network providers arenot valid for some networks in some locations. Whilesome change due to providers closing locations or clos-ing practices to new patients is expected, plan sponsorscan utilize the competitive bidding process to assure vendors are more accountable for their responses to network provider questions. Plan sponsors can introducemechanisms to make vendors responsible for the net-works they are quoting. Such ideas include requiring that only open network provider locations are included inproposals, defining performance standards and monetaryguarantees that ensure proposed network providercounts match member’s actual experience, and creatingaudit protocols during the bid process that can be usedto enforce the standard.
THE VENDOR MARKETPLACE
WHAT EMPLOYERS ARE DOING TO MANAGECOSTS: SELECTED STRATEGIES
THIRD QUARTER 2012 TRENDS Noteworthy Developments of Interest to Employers that Provide Health Coverage
1 See Sibson’s Stat! Health Reform News webpage: http://www.sibson.com/publications-and-resources/stat/?id=18732 See Sisbon’s Capital Checkup, “Plan Sponsors Working Diligently and in Good Faith on the Summary of Benefits and Coverage Will Not Face Penalties During the First Year”:
: http://www.sibson.com/publications-and-resources/capital-checkup/archives/?id=18443 See Sibson’s Capital Checkup, “Proposed Rule on the Affordable Care Act's Comparative Effectiveness Research Fees”: http://www.sibson.com/publications-and-resources/
capital-checkup/archives/?id=18284 See Sibson’s Capital Checkup, “2013 Minimums and Maximums for Health Savings Accounts and High-Deductible Health Plans”: http://www.sibson.com/publications-and-resources/
capital-checkup/archives/?id=1837Copyright © 2012 by The Segal Group, Inc., the parent of The Segal Company. All rights reserved.
Large PBMs continue to combine, with Express Scripts and Medco HealthSolutions, now merged with government approval into the Express Scripts Holding Company (ESHC). SXC Health Solutions, parent company of informedRx, merged with CatalystRx and will operate under the name Catamaran.ESHC and Walgreens, a prescription drug store chain, have entered into amulti-year pharmacy network agreement that will allow ESHC members thatutilize ESHC’s “National Plus” pharmacy network to fill their prescriptions atWalgreens stores.The private health care Exchange market continues to develop, with benefits administrator BenefitFocus announcing its intent to enter this spaceand Extend Health being purchased by a large benefits outsourcer.
The U.S. Supreme Court has announced its opinion concerning theconstitutionality of the ACA. Specifically, it held: The ACA’s requirement that individuals either purchase health insurance or
pay a financial penalty (the law’s “individual mandate” or “minimum coverageprovision”) is constitutional.
The law’s expansion of Medicaid to a broader group of low-income individuals is constitutional, but the federal government does not have the power to terminate all Medicaid funding for a state government thatdoes not accept the ACA expansion.
All provisions of the ACA relevant to employers and health plan sponsors wereupheld. Consequently, there will be no changes to the ACA, and implemen-tation of the law must continue. Existing regulations and programs enactedby the ACA are unch anged, as are the obligations of plan sponsors.1
Answers to Frequently Asked Questions (FAQs) about the implementa-tion and electronic distribution of the Summary of Benefits andCoverage (SBC), required by the ACA, were issued by the Departments of Labor, Health and Human Services and Treasury. The FAQs provideenforcement relief during the first year of applicability for plans andissuers that are working diligently and in good faith to comply.2
The ACA imposes a new comparative effectiveness research fee onspons ors of self-insured group health plans and health insuranceissuers for seven years starting in 2012 for calendar-year plans. The Treasury Department and the Internal Revenue Service (IRS) issued a proposed rule that would implement the fees. However, no guidance onthe payment process has been published.3
The Health Care Reform Guide web page on the Sibson site links to allresources related to the ACA: http://www.sibson.com/health-care-reform/The IRS released the inflation-adjusted minimums and maximums for HealthSavings Accounts and High-Deductible Health Plans for 2013. The IRS calcu-lates the annual adjustments using the 12-month period ending March 31.4