Embed Size (px)
Citation preview
![Page 1: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/1.jpg)
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8
ª 2 0 1 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
FOCUS ON TRENDS IN SURGICAL ANDTRANSCATHETER AORTIC VALVE REPLACEMENT
Trends in Isolated Surgical Aortic
Valve Replacement According toHospital-Based TranscatheterAortic Valve Replacement Volumes Harun Kundi, MD,a Jordan B. Strom, MD, MSC,a Linda R. Valsdottir, MS,a Sammy Elmariah, MD,bJeffrey J. Popma, MD,a Changyu Shen, PHD,a Robert W. Yeh, MD, MSCa
JACC: CARDIOVASCULAR INTERVENTIONS CME/MOC/ECME
This article has been selected as this issue’s CME/MOC/ECME activity,
available online at http://www.acc.org/jacc-journals-cme by selecting the
JACC Journals CME/MOC/ECME tab.
Accreditation and Designation Statement
The American College of Cardiology Foundation (ACCF) is accredited by
the Accreditation Council for Continuing Medical Education to provide
continuing medical education for physicians.
The ACCF designates this Journal-based CME activity for a maximum of
1 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit
commensurate with the extent of their participation in the activity.
Successful completion of this CME activity, which includes participation in
the evaluation component, enables the participant to earn up to 1 Medical
KnowledgeMOC point in the American Board of Internal Medicine’s (ABIM)
Maintenance of Certification (MOC) program. Participants will earn MOC
points equivalent to the amount of CME credits claimed for the activity. It is
the CME activity provider’s responsibility to submit participant completion
information to ACCME for the purpose of granting ABIM MOC credit.
Trends in Isolated Surgical Aortic Valve Replacement According to
Hospital-Based Transcatheter Aortic Valve Replacement Volumes will be
accredited by the European Board for Accreditation in Cardiology (EBAC)
for 1 hour of External CME credits. Each participant should claim only
those hours of credit that have actually been spent in the educational ac-
tivity. The Accreditation Council for Continuing Medical Education
(ACCME) and the European Board for Accreditation in Cardiology (EBAC)
have recognized each other’s accreditation systems as substantially
equivalent. Apply for credit through the post-course evaluation. While
offering the credits noted above, this program is not intended to provide
extensive training or certification in the field.
Method of Participation and Receipt of CME/MOC/ECME Certificate
To obtain credit for this CME/MOC/ECME, you must:
1. Be an ACC member or JACC: Cardiovascular Interventions subscriber.
2. Carefully read the CME/MOC/ECME-designated article available on-
line and in this issue of the journal.
ISSN 1936-8798/$36.00
From the aRichard A. and Susan F. Smith Center for Outcomes Research in C
Israel Deaconess Medical Center, Boston, Massachusetts; and the bCardiology
School, Massachusetts General Hospital, Boston, Massachusetts. Members o
3. Answer the post-test questions. A passing score of at least 70%must be
achieved to obtain credit.
4. Complete a brief evaluation.
5. Claim your CME/MOC/ECME credit and receive your certificate electron-
ically by following the instructions given at the conclusion of the activity.
CME/MOC/ECME Objective for This Article: Uponcompletionof this activity,
the learner should be able to: recognize the impact of hospital transcatheter
aortic valve replacement (TAVR) volume on: 1) isolated surgical aortic valve
replacement (SAVR) volume; 2) SAVR patient characteristics; and 3)
short- and long-term mortality of patients undergoing isolated SAVR.
CME/MOC/ECME Editor Disclosure: JACC: Cardiovascular Interventions
CME/MOC/ECME Editor Bill D. Gogas, MD, PhD, has reported that he has
no disclosures.
Author Disclosures: Members of the study team are supported by funding
from the National Heart, Lung, and Blood Institute (1F32HL1407-11
[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-
01 [Robert W. Yeh]). Dr. Elmariah is funded by the American Heart
Association (14 FTF20440012). The funding organizations had no role in
the final edits or submission of this manuscript. Dr. Elmariah has received
institutional research support from Siemens and Boehringer Ingelheim
Pharmaceuticals, Inc.; and consulting fees from Medtronic and Edwards
Lifesciences. Dr. Popma has received grants from Boston Scientific,
Medtronic, Abbott Vascular, Edwards Lifesciences, and Direct Flow
Medical; is on the Advisory Board of Edwards Lifesciences; and received
personal fees from Boston Scientific, Cordis, and Direct Flow Medical,
outside the submitted work. Dr. Yeh has received investigator-initiated
grant funding from Abiomed; grant support from Boston Scientific; and
consulting fees from Abbott, Medtronic, Boston Scientific, and Teleflex,
outside the submitted work. All other authors have reported that they
have no relationships relevant to the contents of this paper to disclose.
Medium of Participation: Print (article only); online (article and quiz).
CME/MOC/ECME Term of Approval
Issue Date: November 12, 2018
Expiration Date: November 11, 2019
https://doi.org/10.1016/j.jcin.2018.07.002
ardiology, Division of Cardiovascular Medicine, Beth
Division, Department of Medicine, Harvard Medical
f the study team are supported by funding from the
![Page 2: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/2.jpg)
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8 Kundi et al.N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6 Trends in Isolated SAVR
2149
Trends in Isolated Surgical
Aortic Valve ReplacementAccording to Hospital-Based TranscatheterAortic Valve Replacement VolumesHarun Kundi, MD,a Jordan B. Strom, MD, MSC,a Linda R. Valsdottir, MS,a Sammy Elmariah, MD,b
Jeffrey J. Popma, MD,a Changyu Shen, PHD,a Robert W. Yeh, MD, MSCa
ABSTRACT
Na
1R
org
su
sci
Flo
Dir
su
wo
Ma
OBJECTIVES This study sought to evaluate the trends in isolated surgical aortic valve replacement (SAVR)
procedures across hospitals with different transcatheter aortic valve replacement (TAVR) volumes among Medicare
beneficiaries.
BACKGROUND The volume of TAVR has increased in the United States since its approval, now exceeding that of
isolated SAVR.
METHODS Hospitalizations of adults ($18 years of age) with International Classification of Diseases-9th Revision-Clinical
Modification procedure codes for SAVR (35.21 or 35.22) or TAVR (35.05 or 35.06) who were included in the Medicare
Provider Analysis and Review database between January 1, 2011, and December 31, 2014, were included. Trends in isolated
SAVR patient characteristics, procedural volumes, and outcomes by quartile (Q) of hospital-level TAVR use were assessed
over the study period.
RESULTS A total of 37,705 isolated SAVR procedures were analyzed for the study. The annual volume of isolated
SAVR procedures decreased in hospitals performing the largest number of TAVR procedures (Q3: 1,557 in 2011 to 1,391 in
2014; and Q4: 2,607 in 2011 to 1,791 in 2014). Thirty-day and 1-year mortality after SAVR also declined over the study
period in hospitals with the largest TAVR volume (annual change rate in mortality for Q3: �16.4%; p < 0.001;
Q4: �20.8%; p < 0.001).
CONCLUSIONS The advent of TAVR was associated with a reduction in isolated SAVR volumes, a decrease in
comorbidities among patients undergoing SAVR, and corresponding reductions in observed short- and long-term
SAVR mortality among hospitals performing the greatest number of TAVRs. (J Am Coll Cardiol Intv 2018;11:2148–56)
© 2018 by the American College of Cardiology Foundation.
S ymptomatic severe aortic stenosis is the mostcommon indication for aortic valve replace-ment (AVR) in the elderly population in the
United States (1). Whereas surgical aortic valvereplacement (SAVR) has been the traditional treat-ment option for decades (2,3), more recently trans-catheter aortic valve replacement (TAVR) has
tional Heart, Lung, and Blood Institute (1F32HL1407-11 [Jordan B.
01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the America
anizations had no role in the final edits or submission of this manuscri
pport from Siemens and Boehringer Ingelheim Pharmaceuticals, Inc.; and
ences. Dr. Popma has received grants from Boston Scientific, Medtronic
w Medical; is on the Advisory Board of Edwards Lifesciences; and receiv
ect Flow Medical, outside the submitted work. Dr. Yeh has received inve
pport from Boston Scientific; and consulting fees from Abbott, Medtronic, B
rk. All other authors have reported that they have no relationships relev
nuscript received April 4, 2018; revised manuscript received June 21, 201
become a widely used alternative to surgery basedon clinical trials suggesting comparable efficacy andsafety profiles among patients at intermediate orhigh surgical risk (4–8). The volume of TAVR hasincreased rapidly since its approval and now exceedsthat of isolated SAVR in the United States (9). Despitethis, SAVR volume has not decreased after the advent
Strom], R01HS024520-01 [Changyu Shen], and
n Heart Association (14 FTF20440012). The funding
pt. Dr. Elmariah has received institutional research
consulting fees from Medtronic and Edwards Life-
, Abbott Vascular, Edwards Lifesciences, and Direct
ed personal fees from Boston Scientific, Cordis, and
stigator-initiated grant funding from Abiomed; grant
oston Scientific, and Teleflex, outside the submitted
ant to the contents of this paper to disclose.
8, accepted July 3, 2018.
![Page 3: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/3.jpg)
ABBR EV I A T I ON S
AND ACRONYMS
AVR = aortic valve
replacement
Q = quartile
SAVR = surgical aortic valve
replacement
TAVR = transcatheter aortic
valve replacement
Kundi et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8
Trends in Isolated SAVR N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6
2150
of TAVR in the United States and Europe,suggesting that TAVR has broadened eligi-bility for AVR rather than displacing SAVRas an alternative treatment (10,11). It is un-known, however, whether this trend is uni-form across all hospitals, and whether thereis an impact of hospital TAVR volume onthe patient characteristics, procedural vol-umes, and outcomes of isolated SAVR.
SEE PAGE 2157
We therefore sought to evaluate the trends in iso-lated SAVR procedures across hospitals with differentTAVR volumes among Medicare beneficiaries toevaluate the impact of hospital TAVR volume on:1) isolated SAVR volume; 2) SAVR patient character-istics; and 3) outcomes of patients undergoing iso-lated SAVR.
METHODS
STUDY POPULATION. Hospitalizations of adultpatients ($18 years of age) with International Classi-fication of Diseases-9th Revision-Clinical Modifica-tion procedure codes for SAVR (35.21 or 35.22) orTAVR (35.05 or 35.06) were identified within theCenters for Medicare & Medicaid Services MedicareProvider Analysis and Review database betweenJanuary 1, 2011, and December 31, 2014, and includedin the analysis. The Medicare Provider Analysis andReview database contains inpatient billing claims for100% of Medicare fee-for-service beneficiaries andhas been used extensively to study national patternsof procedure use in the United States (12,13).
TAVR-performing hospitals were defined as thosebilling for at least 1 TAVR procedure annually duringthe study period. Quartiles of hospital-level TAVRvolume were defined according to the total volume ofTAVR procedures. During the same time period,SAVR-only hospitals were defined as those perform-ing <1 TAVR procedure annually while performing atleast 1 isolated SAVR annually. To identify a popula-tion of patients with severe aortic valve disease andexclude those patients who might have undergoneAVR for more moderate disease in conjunction withother procedures, patients who underwent concomi-tant valve or coronary artery bypass graft surgerieswere excluded from the study (Online Table 1).
COVARIATES AND OUTCOMES. Possible risk factorsfor mortality were defined based on prior studies(14–16) and clinical knowledge, and correspondingInternational Classification of Diseases-9th Revision-Clinical Modification diagnosis codes were used to
identify surrogates for these variables in the dataset(Online Table 1). All covariates were ascertained fromsecondary diagnosis codes that were coded as “pre-sent on admission” during the index hospitalizationas well as from principal and secondary diagnosiscodes from all hospitalizations for up to 1 year beforethe hospitalization for AVR (Online Table 1). TheCharlson comorbidity index as defined in OnlineTable 2 was also calculated for each patient toestimate 10-year survival rates (14).
The primary outcome was 30-day all-cause mor-tality among isolated SAVR patients, identifiedthrough linkage to the Medicare Denominator File.The rate of 1-year all-cause mortality among patientswith SAVR was evaluated as a secondary endpoint.
STATISTICAL ANALYSIS. Continuous variables arepresented as mean � SD and categorical variables asfrequencies with percentages. Covariates in patientsundergoing isolated SAVR were assessed for changesover time using 1-way analysis of variance forcontinuous variables and the Pearson chi-square testfor categorical variables.
Isolated SAVR volume trends in non-TAVR andTAVR-performing hospitals by quartile of TAVR usewere plotted over the study period. For each TAVRquartile, means of isolated SAVR, TAVR, and combinedvolume trends were plotted. Within each year, 30-dayand 1-year all-cause mortality rates were comparedbetween non-TAVR hospitals and the 4 quartiles (Q1,Q2, Q3, Q4) of TAVR-performing hospitals using chi-squared statistics. A trend test was used to evaluatefor changes in unadjusted within-hospital mortalityrates of patients undergoing isolated SAVR over timeby quartile of TAVR volume. All statistical analyseswere performed in STATA version 15.0 (STATA Cor-poration, College Station, Texas), using a 2-tailed pvalue <0.05 to define significance.
RESULTS
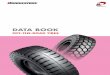
OVERALL RESULTS. A total of 1,165 U.S. hospitalsperformed at least 1 isolated SAVR during the studyperiod, of which 639 (54.8%) did not perform asingle TAVR. One hundred of these SAVR-onlyhospitals (15.6%) were excluded from analysisbecause they did not perform at least 1 case annu-ally, resulting in a final analytic sample of 539SAVR-only hospitals. There were 526 hospitals(45.2%) that performed at least 1 TAVR during thestudy period. A total of 441 of these TAVR hospitals(83.8%) were excluded from analysis because theydid not perform at least 1 TAVR case annually,resulting in a final analytic sample of 85 TAVR-performing hospitals (Figure 1).
![Page 4: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/4.jpg)
FIGURE 1 Study Flow Diagram
SAVR ¼ surgical aortic valve replacement; TAVR ¼ transcatheter aortic valve replacement.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8 Kundi et al.N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6 Trends in Isolated SAVR
2151
Among those undergoing SAVR in non-TAVR hos-pitals, 7 covariates including age, chronic heart fail-ure, coronary artery disease, coronary artery bypasssurgery, peripheral vascular disease, chronic kidneydisease, and chronic obstructive pulmonary diseaseconsistently and significantly declined over the studyperiod (Table 1). In addition to those 7 covariates, 5more covariates including diabetes mellitus, priormyocardial infarction, prior percutaneous coronaryintervention, cerebrovascular disease, and home ox-ygen use also consistently and significantly declinedin TAVR-performing hospitals over the study periodamong patients undergoing SAVR (Table 2).
Trends in rates of comorbidities for isolated SAVRpatients by quartile of TAVR performance are notedin Online Tables 3 to 6. With the exception of pe-ripheral vascular disease and coronary artery disease,there was no change in rates of comorbidities overtime in hospitals performing the lowest numbers ofTAVR (Q1). With increasing hospital TAVR volume, agreater percentage of comorbidities in patients un-dergoing SAVR were observed to decline over thestudy period, without an observed threshold effect.Although there was no difference in estimated 10-year survival rates based on the Charlson comorbid-ity index in Q1 hospitals (annual change rate ¼ 0.99%;p ¼ 0.47), it improved most in hospitals with the
highest TAVR volume over the study period (Q3:annual change rate ¼ 6.9%; p < 0.001; Q4: annualchange rate ¼ 10.1%; p < 0.001).
VOLUME TRENDS. The volume of isolated SAVR pro-cedures decreased only in hospitals performing thelargest number of TAVR procedures (Q3: 1,557 to 1,391SAVRhospitalizations per year; Q4: 2,607 to 1,791 SAVRhospitalizations per year) (Figure 2). Individual hospi-tal trends according to quartiles of TAVR volumedemonstrated wide interhospital variation in the vol-ume of SAVR procedures performed annually (OnlineFigure 1). The mean TAVR volume exceeded that ofSAVR in all hospitals except those in the lowest quar-tile of TAVR performance, with the crossover pointoccurring as early as 2012 in the highest-volumeTAVR-performing hospitals (Online Figure 2).
OUTCOMES. There were no significant changes in 30-day all-cause mortality of isolated SAVR patients overthe study period for hospitals in the lowest quartilesof TAVR volume (annual change in mortality, non-TAVR: �4.6%; p ¼ 0.06; Q1: 10.7%; p ¼ 0.08;Q2: �7.2%; p ¼ 0.33) (Table 3). By contrast, 30-day all-cause mortality significantly declined for hospitals inthe highest TAVR volume quartiles (annual change inmortality Q3: �16.4%; p < 0.001; Q4: �20.8;p < 0.001) with the largest annual rate of decline seen
![Page 5: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/5.jpg)
TABLE 1 Characteristics of Isolated SAVR Patients in Non-TAVR Hospitals Over the Study Period
2011(n ¼ 3,708)
2012(n ¼ 3,932)
2013(n ¼ 4,207)
2014(n ¼ 4,286) p Value
Age, yrs 76.30 � 6.52 76.02 � 6.51 75.73 � 6.47 75.50 � 6.30 <0.001
Men 1,936 (52.2) 2,098 (53.4) 2,329 (55.4) 2,300 (53.7) 0.043
Chronic heart failure 1,393 (37.6) 1,451 (36.9) 1,447 (34.4) 1,464 (34.2) 0.001
Diabetes mellitus 921 (24.8) 1,006 (25.6) 1,070 (25.4) 1,132 (26.4) 0.44
Smoker 532 (14.3) 569 (14.5) 615 (14.6) 666 (15.5) 0.41
Coronary artery disease 1,442 (38.9) 1,574 (40.0) 1,562 (37.1) 1,496 (34.9) <0.001
Prior myocardial infarction 272 (7.3) 274 (7.0) 299 (7.1) 264 (6.2) 0.17
Prior PCI 172 (4.6) 188 (4.8) 196 (4.7) 184 (4.3) 0.74
Prior valvular surgery 32 (0.9) 35 (0.9) 33 (0.8) 25 (0.6) 0.38
Prior aortic surgery 3 (0.1) 7 (0.2) 2 (<1) 1 (<1) 0.073
Prior CABG 326 (8.8) 344 (8.7) 305 (7.2) 250 (5.8) <0.001
Peripheral vascular disease 151 (4.1) 150 (3.8) 142 (3.4) 128 (3.0) 0.043
Atrial fibrillation 1,648 (44.4) 1,713 (43.6) 1,799 (42.8) 1,854 (43.3) 0.50
Cerebrovascular disease 339 (9.1) 351 (8.9) 379 (9.0) 348 (8.1) 0.34
CKD without dialysis 559 (15.1) 621 (15.8) 562 (13.4) 507 (11.8) <0.001
Renal dialysis 17 (0.5) 22 (0.6) 31 (0.7) 22 (0.5) 0.37
Liver disease 115 (3.1) 115 (2.9) 125 (3.0) 108 (2.5) 0.42
COPD 903 (24.4) 907 (23.1) 934 (22.2) 871 (20.3) <0.001
Home O2 14 (0.4) 41 (1.0) 49 (1.2) 49 (1.1) <0.001
Charlson Comorbidity index,estimated 10-yr survival, %
32.1 � 29.5 31.8 � 29.2 33.3 � 29.5 34.2 � 29.3 <0.001
Values are mean � SD or n (%).
CABG ¼ coronary artery bypass graft; CKD ¼ chronic kidney disease; COPD ¼ chronic obstructive pulmonary disease; PCI ¼ percutaneous coronary intervention; SAVR ¼surgical aortic valve replacement; TAVR ¼ transcatheter aortic valve replacement.
Kundi et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8
Trends in Isolated SAVR N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6
2152
in Q4 (Figure 3). With the exception of Q1, the 1-yearall-cause mortality rates for SAVR patients signifi-cantly declined in all quartiles over the study period(annual change in 1-year mortality Q2: �16.4%;Q3: �15.4%; Q4: �16.3%, p < 0.001 for each).
SENSITIVITY ANALYSIS. Because we excluded 83.8%of TAVR-performing hospitals in our primary anal-ysis, we performed a sensitivity analysis withoutexcluding hospitals that performed <1 TAVR proced-ure annually, but that performed at least 1 such pro-cedure during the study period. In this analysis, therewere 488 TAVR-performing hospitals that performeda total of 54,603 SAVR procedures. As shown inOnline Tables 7 to 9 and Online Figures 3 and 4, theresults of this analysis were consistent with our pri-mary findings.
DISCUSSION
Although TAVR has now eclipsed SAVR worldwideas the predominant treatment for severe symptomaticaortic stenosis, knowledge about how the establish-ment and growth of TAVR programs have influencedthe volumes and outcomes of patients undergoingSAVR at hospitals is limited. The current study
demonstrates that SAVR volume declined from 2011 to2014 only in hospitals performing the highest volumeof TAVR procedures. Additionally, rates of comorbid-ities and 30-day and 1-year all-cause mortality alldeclined during the study period in patients under-going SAVR, with the largest decline seen in hospitalsperforming the highest volume of TAVR procedures.
Prior studies from the United States and Europehave suggested that isolated SAVR volume was notaffected by the advent of TAVR (11,12). By contrast,the current study indicates that this conclusion maynot apply to the highest volume TAVR-performinghospitals. In fact, we demonstrate that hospitalsperforming the highest number of TAVR procedureshad the greatest observed decline in SAVR volume,with TAVR volume exceeding that of SAVR nationallyin the highest volume TAVR-performing hospitalsearlier than previously reported (9). These data sug-gest that the degree of displacement of SAVR by TAVRcorrelates directly with the number of TAVR proced-ures performed at a given hospital.
Additionally, the patient case mix changed overtime, with patients undergoing SAVR exhibiting thegreatest reduction in rates of comorbidities in highTAVR volume hospitals. This finding may suggest a
![Page 6: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/6.jpg)
TABLE 2 Characteristics of Isolated SAVR Patients in TAVR-Performing Hospitals Over the Study Period
2011(n ¼ 5,762)
2012(n ¼ 5,324)
2013(n ¼ 5,485)
2014(n ¼ 5,001) p Value
Age, yrs 78.10 � 7.39 76.91 � 6.92 76.43 � 6.73 75.55 � 6.42 <0.001
Men 3,089 (53.6) 2,917 (54.8) 3,173 (57.8) 2,911 (58.2) <0.001
Chronic heart failure 2,833 (49.2) 2,378 (44.7) 2,466 (45.0) 2,093 (41.9) <0.001
Diabetes mellitus 1,410 (24.5) 1,287 (24.2) 1,279 (23.3) 1,115 (22.3) 0.039
Smoker 681 (11.8) 691 (13.0) 727 (13.3) 626 (12.5) 0.11
Coronary artery disease 2,676 (46.4) 2,251 (42.3) 2,130 (38.8) 1,763 (35.3) <0.001
Prior myocardial infarction 624 (10.8) 504 (9.5) 408 (7.4) 355 (7.1) <0.001
Prior PCI 426 (7.4) 318 (6.0) 271 (4.9) 223 (4.5) <0.001
Prior valvular surgery 87 (1.5) 78 (1.5) 76 (1.4) 59 (1.2) 0.49
Prior aortic surgery 12 (0.2) 13 (0.2) 12 (0.2) 12 (0.2) 0.98
Prior CABG 681 (11.8) 499 (9.4) 419 (7.6) 240 (4.8) <0.001
Peripheral vascular disease 283 (4.9) 216 (4.1) 173 (3.2) 132 (2.6) <0.001
Atrial fibrillation 2,733 (47.4) 2,446 (45.9) 2,642 (48.2) 2,356 (47.1) 0.13
Cerebrovascular disease 638 (11.1) 520 (9.8) 512 (9.3) 397 (7.9) <0.001
CKD without dialysis 1,201 (20.8) 996 (18.7) 769 (14.0) 673 (13.5) <0.001
Renal dialysis 28 (0.5) 33 (0.6) 22 (0.4) 26 (0.5) 0.45
Liver disease 180 (3.1) 164 (3.1) 169 (3.1) 164 (3.3) 0.93
COPD 1,478 (25.7) 1,162 (21.8) 1,080 (19.7) 844 (16.9) <0.001
Home O2 106 (1.8) 60 (1.1) 60 (1.1) 55 (1.1) <0.001
Charlson Comorbidity index,estimated 10-yr survival, %
26.0 � 28.8 28.6 � 28.9 31.1 � 29.0 34.3 � 29.5 <0.001
Values are mean � SD or n (%).
Abbreviations as in Table 1.
FIGURE 2 Unweighted Annual Isolated SAVR Volumes in Each Hospital Group
Q ¼ quartile; other abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8 Kundi et al.N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6 Trends in Isolated SAVR
2153
![Page 7: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/7.jpg)
TABLE 3 30-Day and 1-Year Isolated SAVR Mortality Rates According to Year and Hospital-Level Quartile of TAVR Volume
2011(n ¼ 9,470)
2012(n ¼ 9,256)
2013(n ¼ 9,692)
2014(n ¼ 9,287)
Trendp Value (Slope)
Non-TAVR hospitals30-day mortality 151/3,708 (4.1) 164/3,932 (4.2) 135/4,207 (3.2) 147/4,286 (3.4) 0.06 (�0.0024)1-yr mortality 388/3,708 (10.5) 380/3,932 (9.7) 356/4,207 (8.5) 352/4,286 (8.2) <0.001 (�0.0079)
Quartile-1 hospitals30-day mortality 18/652 (2.8) 15/746 (2.0) 28/792 (3.5) 36/853 (4.2) 0.08 (0.0062)1-yr mortality 77/652 (11.8) 66/746 (8.1) 64/792 (8.1) 82/853 (9.6) 0.17 (�0.0065)
Quartile-2 hospitals30-day mortality 33/946 (3.5) 22/1,027 (2.1) 29/1,034 (2.8) 25/966 (2.6) 0.33 (�0.0019)1-yr mortality 116/946 (12.3) 83/1,027 (8.1) 77/1,034 (7.4) 58/966 (6.0) <0.001 (�0.0192)
Quartile-3 hospitals30-day mortality 70/1,557 (4.5) 41/1,439 (2.8) 32/1,454 (2.2) 30/1,391 (2.2) <0.001 (�0.0078)1-yr mortality 191/1,557 (12.3) 136/1,439 (9.5) 104/1,454 (7.2) 86/1,391 (6.2) <0.001 (�0.0207)
Quartile-4 hospitals30-day mortality 87/2,607 (3.3) 55/2,112 (2.6) 38/2,205 (1.7) 24/1,791 (1.3) <0.001 (�0.0069)1-yr mortality 292/2,607 (11.2) 168/2,112 (8.0) 146/2,205 (6.6) 98/1,791 (5.5) <0.001 (�0.0191)
Values are n/N (%).
Abbreviations as in Table 1.
Kundi et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8
Trends in Isolated SAVR N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6
2154
shift from SAVR to TAVR use in the highest surgicalrisk patients. Accordingly, there was a reduction overtime in 30-day and 1-year all-cause mortality rates forSAVR patients, with the greatest declines observed inhigh-volume TAVR-performing hospitals. In 2014, wefound that 30-day and 1-year mortality rates in non-TAVR hospitals were 3.4% and 8.2%, respectively. Incomparison, 30-day and 1-year mortality rates inhigh-volume TAVR hospitals were lower, at 1.3% and
FIGURE 3 Trends of Isolated SAVR 30-Day Mortality Rates in Each H
Error bars represent the SEMs. Abbreviations as in Figures 1 and 2.
5.5%, respectively. The estimated 10-year survivalrates also differed between hospitals, with the rate ofchange in 10-year survival progressively increasing inTAVR-performing hospitals but not in non-TAVRhospitals. These findings suggest that TAVR avail-ability may have led to the selective use of SAVR inlower risk patients. It may also partially reflectsecular trends in mortality for AVR patients, becauseSAVR mortality declined even in hospitals not
ospital Group
![Page 8: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/8.jpg)
PERSPECTIVES
WHAT IS KNOWN? Isolated SAVR volume has not decreased
after the advent of TAVR worldwide.
WHAT IS NEW? The current study demonstrates that the
degree of displacement of SAVR by TAVR correlates directly with
the number of TAVR procedures performed at a given hospital. In
addition, SAVR mortality rates declined the most at hospitals
with the highest TAVR volumes, likely representing declining risk
of the SAVR case mix.
WHAT IS NEXT? The continued rapid growth and dissemination
of TAVR may promote a shift from SAVR to TAVR. Whether this
shift toward less complex surgical patients may mitigate the
adverse effects of declining surgeon volumes for SAVR is
unknown.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8 Kundi et al.N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6 Trends in Isolated SAVR
2155
performing TAVR. We also found that the prevalenceof chronic heart failure was higher in TAVR hospitalsthan non-TAVR hospitals. This may be caused bydifferences in case mix of AVR patients at TAVR-performing versus nonperforming hospitals. Howev-er, it may also be possible that these differences arecaused by discrepancies in coding practices.
Although TAVR is a novel and expanding treatmentchoice for severe aortic stenosis, most U.S. hospitalsperform a relatively small number of TAVR casesannually. Our study suggests that in low TAVRvolume facilities, the number of transcatheter pro-cedures was not large enough to displace surgicalvolumes. As TAVR use continues to expand world-wide, these results suggest that the volume of SAVRmay continue to decline. Our sensitivity analysis forTAVR-performing hospitals found consistent results.The results have significant implications for trainingand experience of SAVR centers. We found that theaverage number of isolated SAVRs performed perhospital was 60.4 over the study period. Prior studieshave suggested a negative relationship betweenvolume and outcomes after cardiac surgery (15).However, the continued rapid growth and dissemi-nation of TAVR promote a shift from SAVR to TAVR.Whether this shift toward less complex surgical pa-tients may mitigate the adverse effects of decliningsurgeon volumes for SAVR is unknown.
STUDY LIMITATIONS. First, the study is retrospec-tive and based on administrative data, and istherefore subject to residual confounding becauseof unmeasured variables and inaccuracies in coding.Second, the patterns observed may in part becaused by changes in secular trends over the studyperiod. Third, because claims represent billingdiagnoses, they may not accurately reflect thepresence and severity of clinical conditions. Fourth,because of limited granularity in the administrativedataset, traditional surgical risk scores, such as theSociety for Thoracic Surgery Predicted Risk of Mor-tality (16,17) or logistic EuroSCORE (18), could notbe determined for each patient. The data also donot allow us to see how many patients were
transferred from non-TAVR hospitals to have theprocedure elsewhere. Because TAVR patients duringthis time period were restricted to those at extremeor high surgical risk, we purposefully did notcompare outcomes between TAVR and SAVRpatients due to the potential for unmeasured con-founding. Finally, the observed patterns may notreflect overall trends in countries outside the UnitedStates and in non-Medicare beneficiaries.
CONCLUSIONS
In Medicare beneficiaries from 2011 to 2014, theadvent of TAVR was associated with a reduction inSAVR volumes, the selection of lower risk patients forSAVR, and corresponding declines in short- and long-term mortality in hospitals performing the most TAVRprocedures.
ADDRESS FOR CORRESPONDENCE: Dr. Robert W.Yeh, Richard A. and Susan F. Smith Center for Out-comes Research in Cardiology, Beth Israel DeaconessMedical Center, 375 Longwood Avenue, Fourth Floor,Boston, Massachusetts 02215. E-mail: [email protected].
RE F E RENCE S
1. Nkomo VT, Gardin JM, Skelton TN,Gottdiener JS, Scott CG, Enriquez-Sarano M.Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11.
2. Manning WJ. Asymptomatic aortic stenosis inthe elderly: a clinical review. JAMA 2013;310:1490–7.
3. Harken DE. Partial and complete prostheses inaortic insufficiency. J Thorac Cardiovasc Surg1960;40:744–62.
4. Leon MB, Smith CR, Mack M, et al. Trans-catheter aortic-valve implantation for aortic ste-nosis in patients who cannot undergo surgery.N Engl J Med 2010;363:1597–07.
5. Reardon MJ, Van Mieghem NM, Popma JJ, et al.Surgical or transcatheter aortic-valve replacementin intermediate-risk patients. N Engl J Med 2017;376:1321–31.
6. Mack MJ, Leon MB, Smith CR, et al. 5-yearoutcomes of transcatheter aortic valve replace-ment or surgical aortic valve replacement for high
![Page 9: Trends in Isolated Surgical Aortic Valve Replacement ...[Jordan B. Strom], R01HS024520-01 [Changyu Shen], and 1R01HL136708-01 [Robert W. Yeh]). Dr. Elmariah is funded by the American](https://reader033.pdfslide.us/reader033/viewer/2022042909/5f3c4de735eda8087f06f5d7/html5/thumbnails/9.jpg)
Kundi et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 1 , N O . 2 1 , 2 0 1 8
Trends in Isolated SAVR N O V E M B E R 1 2 , 2 0 1 8 : 2 1 4 8 – 5 6
2156
surgical risk patients with aortic stenosis (PART-NER 1): a randomised controlled trial. Lancet 2015;385:2477–84.
7. Thourani VH, Kodali S, Makkar RR, et al.Transcatheter aortic valve replacement versussurgical valve replacement in intermediate-riskpatients: a propensity score analysis. Lancet2016;387:2218–25.
8. Baron SJ, Arnold SV, Wang K, et al. Healthstatus benefits of transcatheter vs surgical aorticvalve replacement in patients with severe aorticstenosis at intermediate surgical risk: results fromthe PARTNER 2 randomized clinical trial. JAMACardiol 2017;2:837–45.
9. Grover FL, Vemulapalli S, Carroll JD, et al. 2016annual report of the Society of Thoracic Surgeons/American College of Cardiology transcathetervalve therapy registry. Ann Thorac Surg 2017;103:1021–35.
10. Culler SD, Cohen DJ, Brown PP, et al. Trends inaortic valve replacement procedures between2009 and 2015: has transcatheter aortic valvereplacement made a difference? Ann Thorac Surg2018;105:1137–43.
11. Reinöhl J, Kaier K, Reinecke H, et al. Effect ofavailability of transcatheter aortic-valve replace-ment on clinical practice. N Engl J Med 2015;373:2438–47.
12. Krumholz HM, Nuti SV, Downing NS,NormandSL,WangY.Mortality,hospitalizations, andexpenditures for the Medicare population aged 65years or older, 1999-2013. JAMA 2015;314:355–65.
13. Schermerhorn ML, Buck DB, O’Malley AJ, et al.Long-term outcomes of abdominal aortic aneu-rysm in the Medicare population. N Engl J Med2015;373:328–38.
14. CharlsonME, Pompei P, Ales KL, MacKenzie CR.A new method of classifying prognostic comor-bidity in longitudinal studies: development andvalidation. J Chronic Dis 1987;40:373–83.
15. Birkmeyer JD, Siewers AE, Finlayson EV, et al.Hospital volume and surgical mortality in theUnited States. N Engl J Med 2002;346:1128–37.
16. O’brien SM, Shahian DM, Filardo G, et al. TheSociety of Thoracic Surgeons 2008 cardiac surgeryrisk models: part 2—isolated valve surgery. AnnThorac Surg 2009;88:23–42.
17. Edwards FH, Cohen DJ, O’Brien SM, et al. Devel-opment and validation of a risk prediction model forin-hospital mortality after transcatheter aortic valvereplacement. JAMA Cardiol 2016;1:46–52.
18. Nashef SA, Roques F, Michel P, Gauducheau E,Lemeshow S, Salamon R. European system forcardiac operative risk evaluation (Euro SCORE).Eur J Cardiothorac Surg 1999;16:9–13.
KEY WORDS isolated surgical aortic valvereplacement, Medicare, transcatheter aorticvalve replacement
APPENDIX For supplemental tables andfigures, please see the online version ofthis paper.
Go to http://www.acc.org/jacc-journals-cme to takethe CME/MOC/ECME quizfor this article.