Embed Size (px)
Citation preview
Review
© Future Drugs Ltd. All rights reserved. ISSN 1478-7210 575
CONTENTS
Historical overview
Clinical features
Diagnostic criteria & differential diagnosis
Natural history& susceptibility
Treatment, prognosis& prevention
Microbiology of SSSS
Molecular basis of SSSS
Five-year view: the unanswered questions
Expert opinion
Key issues
References
Affiliation
www.future-drugs.com
Treatment of staphylococcal scalded skin syndromeGirish K Patel
Humans are a natural reservoir for Staphylococcal aureus. Colonization begins soonafter birth and predisposes to infection. S. aureus is one of the most common causes of skin infection, giving rise to folliculitis, furunculosis, carbuncles, ecthyma, impetigo, cellulitis and abscesses. In addition, S. aureus may cause a number of toxin-mediatedlife-threatening diseases, including staphylococcal scalded skin syndrome (SSSS). Epidermolytic toxins released by certain S. aureus strains cause SSSS by cleaving the epidermal cell adhesion molecule, desmogelin-1, resulting in superficial skin erosion. Recent experiments have revealed similarities in the pathophysiology of SSSS and pemphigus foliaceus, an autoimmune disorder that is characterized by antibodies targeting the same epidermal attachment protein. SSSS typically affects neonates and infants but may also occur in predisposed adults. It is painful and distressing for thepatient and parents, although most cases respond to antibiotic treatment.Mortality is low in infants but can be as high as 67% in adults, and is dependent on the extent of skin involvement and the comorbid state. Thus, the management of adults who develop SSSS remains a major therapeutic challenge. The antibody response against the toxins neutralizes their effect and prevents recurrence or limits the effects to the area of infection, which is known as bullous impetigo.
Expert Rev. Anti-infect. Ther. 2(4), 575–587 (2004)
Department of Dermatology, University of Wales College of Medicine, Heath Park, Cardiff CF14 4XN, UKTel.: +44 292 074 7747Fax: +44 292 074 [email protected]
KEYWORDS:blistering disease, dermatitis exfoliativa neonatorum, desmoglein-1, drug therapy, epidermolytic toxin, exfoliative toxin, Gram-positive bacterial infections, Ritter’s disease, staphylococcal scalded skin syndrome, Staphylococcus aureus
Staphylococcus aureus, a member of themicrococcaceae family, is a Gram-positivecoccus that can be distinguished from otherstaphylococci by its ability to form goldencolored colonies and test positive for coagu-lase, mannitol-fermentation and deoxyribo-nuclease [1]. In addition, S. aureus can besubdivided into 11 serotypes based upon thecomposition of the antiphagocytic polysac-charide microcapsule. Serotypes 5 and 8 areresponsible for three-quarters of all humanS. aureus infections [2].
Humans are the natural reservoir forS. aureus, which frequently colonizes the skin,in particular the anterior nares from where itcan invariably be isolated if enrichment tech-niques are used [3]. Using conventional tech-niques and serial nasal sampling of healthynurses, Hutchinson and colleagues found that20% were persistent carriers, 60% intermit-tent carriers and 20% appeared resistant tonasal carriage [4]. Colonization begins soon
after birth; approximately 30% of newbornsare colonized with S. aureus within their firstweek of life and this may rise in to 90% dur-ing S. aureus epidemics [5,6]. S. aureus coloni-zation is associated with a greater risk of infec-tion [7] and is more common amongst atopics[8], diabetics [9], intravenous drug users [10],HIV sufferers [11], and those receiving renaldialysis [12]. The incidence of S. aureus infec-tion is increasing; it is currently amongst themost common causes of skin infection, anddespite the development of antibiotics, it isassociated with morbidity and mortality in allage groups [13–16].
Staphylococci produce various enzymes todestroy tissue and facilitate the spread ofinfection, such as proteases, lipases andhyaluronidase. In addition, staphylococciproduce numerous toxins secreted duringthe stationary phase of bacterial division,which are characterized according to theirmechanism of action. The α-toxin results in
For reprint orders, please contact [email protected]
Patel
576 Expert Rev. Anti-infect. Ther. 2(4), (2004)
cell wall pore formation within the mammalian cell andinduces a proinflammatory response that manifests as septi-cemia [17]. The enterotoxins are superantigenic pyrogenictoxins that induce T-cell proliferation and cytokine releaseby binding to major histocompatibility complex class II pro-teins. They include toxic shock syndrome protein 1, entero-toxin B and C, which manifest as toxic shock syndrome andfood poisoning, respectively [18]. The exfoliative toxinsinclude epidermolytic toxins (ETs)-A and -B, which causeskin separation and erythema and are responsible for bothbullous impetigo and staphylococcal scalded skin syndrome(SSSS) [19].
Historical overviewVon Rittershain was the first to describe SSSS in 1878 as adisease of the newborn that he called dermatitis exfolitivaneonatorum [20]. Later it was referred to as Ritter’s disease andis now known as SSSS. Over a 10-year period in a Prague hos-pital, von Rittershain observed 297 cases [20]. Later in that dec-ade, Almquist established the link between SSSS and S. aureus,which he called micrococcus pemphigi neonatorum [21].Improvements in standards of hygiene have led to a steadydecline in the incidence of SSSS since the initial description.
In 1956, Lyell erroneously grouped SSSS together with anew disease, characterized by epidermal necrosis caused by acirculating toxin, for which he coined the term toxic epider-mal necrolysis (TEN) [22]. The prominence of Lyell within thefield of dermatology at that time perpetuated the confusionand resulted in a number of publications describing SSSS buterroneously called TEN [23–27]. However, the evidence of acausal association between SSSS and S. aureus continued to beapparent, even Lyell in his review of 128 cases described howthe disease in children under 10 years of age was often associ-ated with S. aureus infection [24,28]. Later, Lyell acceptedresponsibility for his error in grouping TEN and SSSStogether in a published historical perspective on SSSS [29].
In 1970, the landmark studies by Melish and Glasgowestablished SSSS as being caused by an ET released byS. aureus [19,30,31]. They showed that passive transfer ofS. aureus cultured supernatant derived from patients withSSSS into neonatal mice caused superficial epidermal blister-ing within the granular layer of the skin, the same as seen inhumans with SSSS. By doing so, they successfully created ananimal model. These findings were reproduced by a number ofother researchers [32,33]. The toxin responsible for SSSS wassubsequently isolated and when injected into newborn miceperitoneum, blistering was observed in a dose-dependent man-ner [34]. Interestingly, mice 5 days or older were not suscepti-ble to blistering and demonstrated suppressed serum levels ofepidermolytic exotoxin [19,31,35].
The first adult case of SSSS was described in 1972 [36]. Adultonset SSSS is a rare disorder, although there are now over50 documented cases, it is almost always observed in individualswho are susceptible to S. aureus infection [37].
A century after the initial clinical description of SSSS, it isonly now understood, at the dawn of a new millennium, howthe S. aureus-derived ETs cause the disease. Through a seriesof elegant experiments, Amagai and colleagues clearly demon-strated how the toxin selectively targets and cleaves desmo-glein (DG)-1, an important epidermal cell–cell attachmentprotein [38–41].
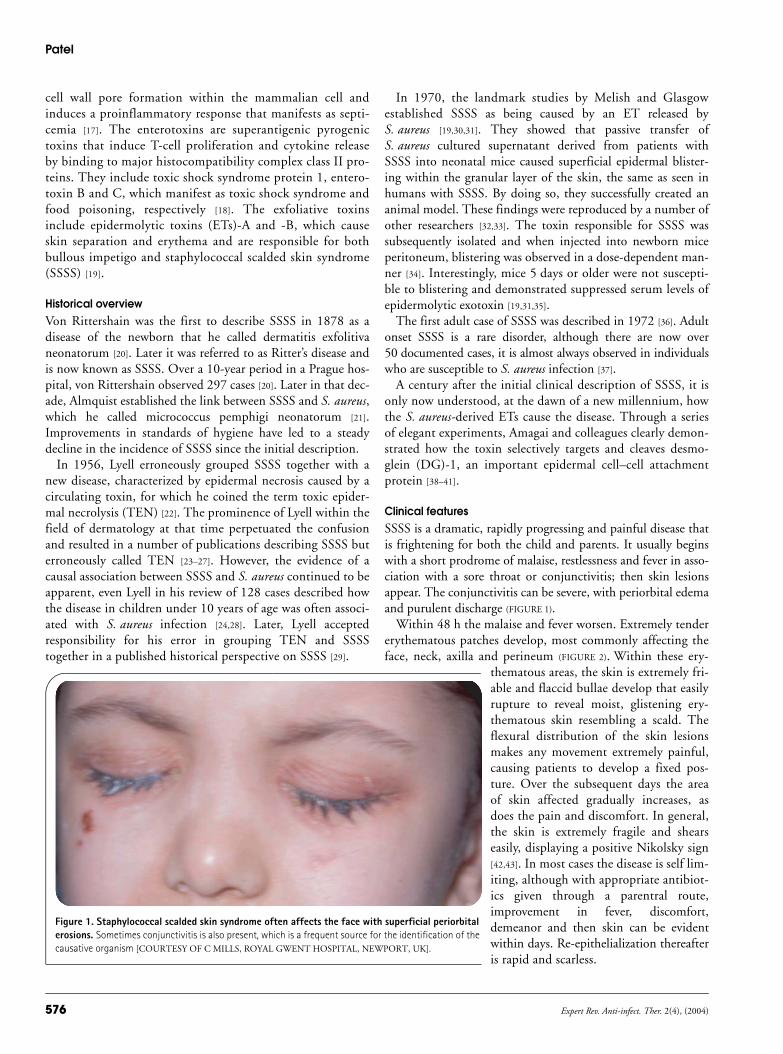
Clinical featuresSSSS is a dramatic, rapidly progressing and painful disease thatis frightening for both the child and parents. It usually beginswith a short prodrome of malaise, restlessness and fever in asso-ciation with a sore throat or conjunctivitis; then skin lesionsappear. The conjunctivitis can be severe, with periorbital edemaand purulent discharge (FIGURE 1).
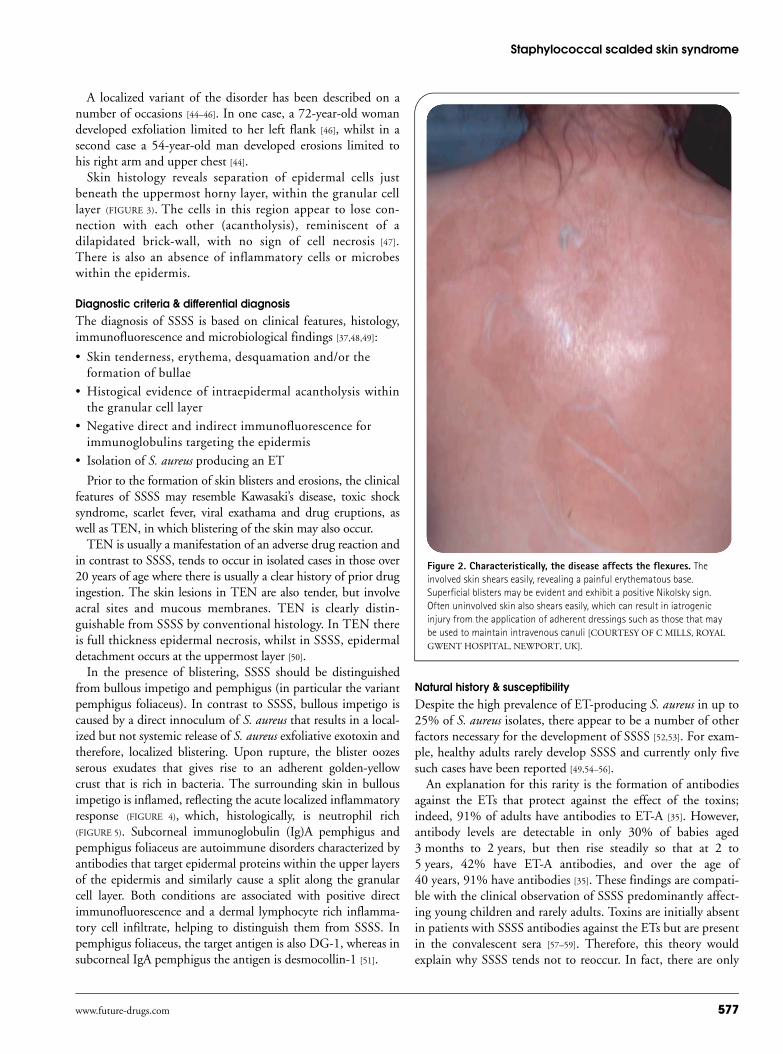
Within 48 h the malaise and fever worsen. Extremely tendererythematous patches develop, most commonly affecting theface, neck, axilla and perineum (FIGURE 2). Within these ery-
thematous areas, the skin is extremely fri-able and flaccid bullae develop that easilyrupture to reveal moist, glistening ery-thematous skin resembling a scald. Theflexural distribution of the skin lesionsmakes any movement extremely painful,causing patients to develop a fixed pos-ture. Over the subsequent days the areaof skin affected gradually increases, asdoes the pain and discomfort. In general,the skin is extremely fragile and shearseasily, displaying a positive Nikolsky sign[42,43]. In most cases the disease is self lim-iting, although with appropriate antibiot-ics given through a parentral route,improvement in fever, discomfort,demeanor and then skin can be evidentwithin days. Re-epithelialization thereafteris rapid and scarless.
Figure 1. Staphylococcal scalded skin syndrome often affects the face with superficial periorbital erosions. Sometimes conjunctivitis is also present, which is a frequent source for the identification of the causative organism [COURTESY OF C MILLS, ROYAL GWENT HOSPITAL, NEWPORT, UK].
Staphylococcal scalded skin syndrome
www.future-drugs.com 577
A localized variant of the disorder has been described on anumber of occasions [44–46]. In one case, a 72-year-old womandeveloped exfoliation limited to her left flank [46], whilst in asecond case a 54-year-old man developed erosions limited tohis right arm and upper chest [44].
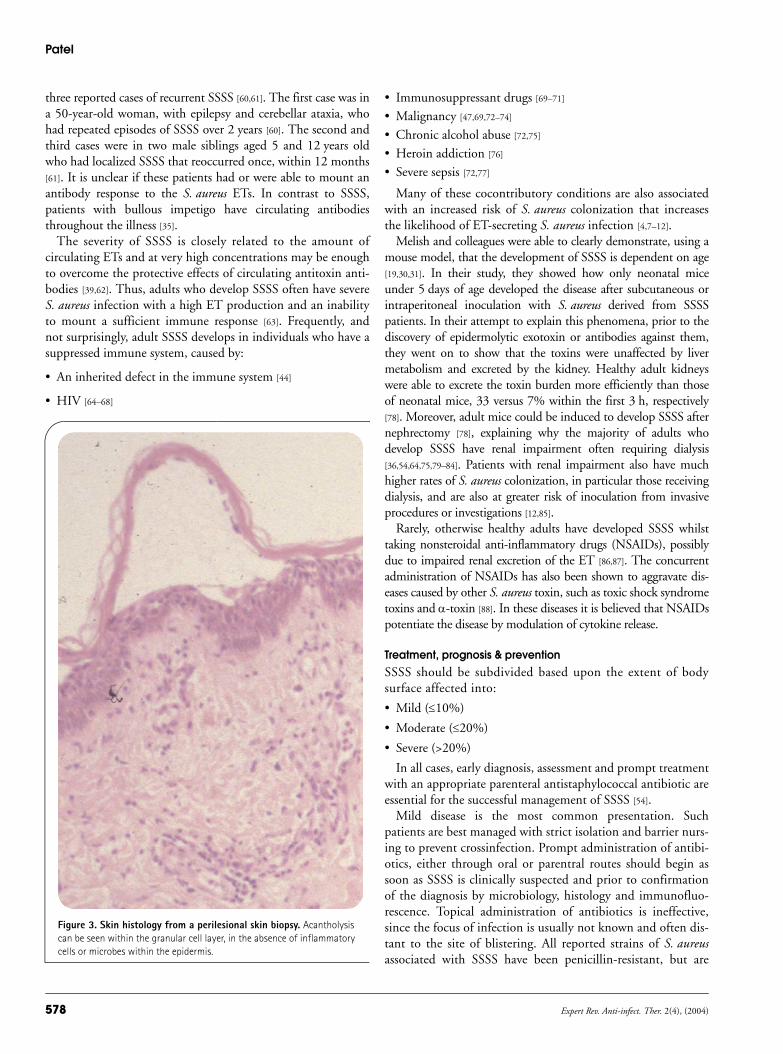
Skin histology reveals separation of epidermal cells justbeneath the uppermost horny layer, within the granular celllayer (FIGURE 3). The cells in this region appear to lose con-nection with each other (acantholysis), reminiscent of adilapidated brick-wall, with no sign of cell necrosis [47].There is also an absence of inflammatory cells or microbeswithin the epidermis.
Diagnostic criteria & differential diagnosisThe diagnosis of SSSS is based on clinical features, histology,immunofluorescence and microbiological findings [37,48,49]:
• Skin tenderness, erythema, desquamation and/or theformation of bullae
• Histogical evidence of intraepidermal acantholysis withinthe granular cell layer
• Negative direct and indirect immunofluorescence forimmunoglobulins targeting the epidermis
• Isolation of S. aureus producing an ET
Prior to the formation of skin blisters and erosions, the clinicalfeatures of SSSS may resemble Kawasaki’s disease, toxic shocksyndrome, scarlet fever, viral exathama and drug eruptions, aswell as TEN, in which blistering of the skin may also occur.
TEN is usually a manifestation of an adverse drug reaction andin contrast to SSSS, tends to occur in isolated cases in those over20 years of age where there is usually a clear history of prior drugingestion. The skin lesions in TEN are also tender, but involveacral sites and mucous membranes. TEN is clearly distin-guishable from SSSS by conventional histology. In TEN thereis full thickness epidermal necrosis, whilst in SSSS, epidermaldetachment occurs at the uppermost layer [50].
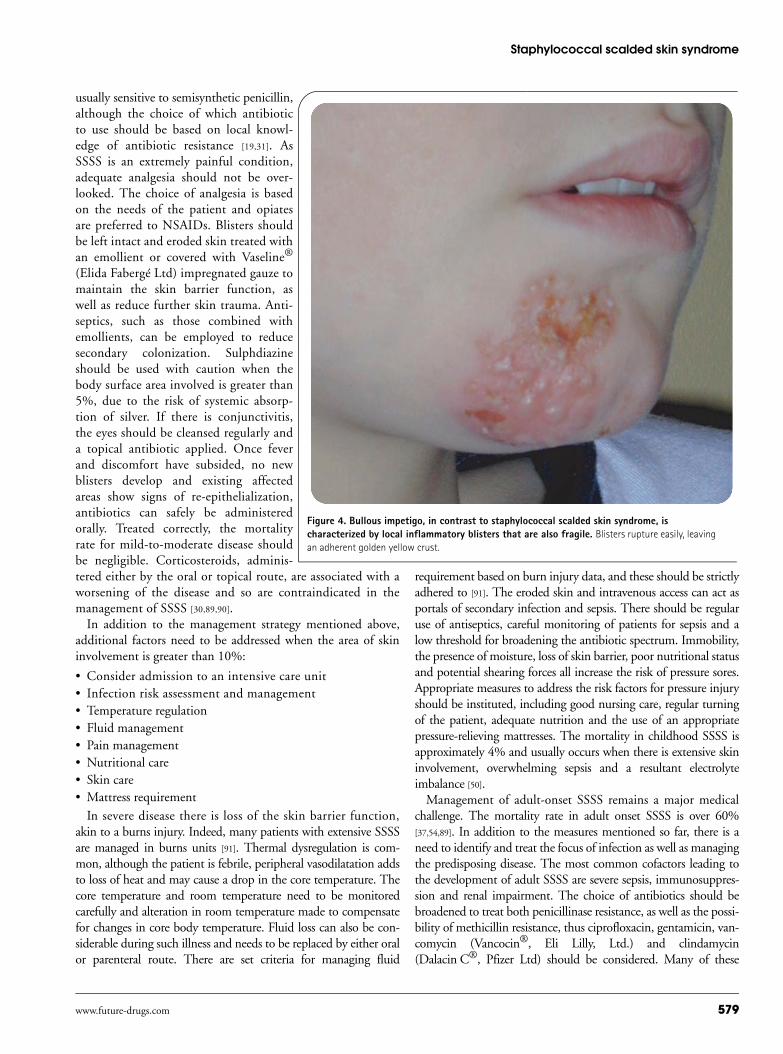
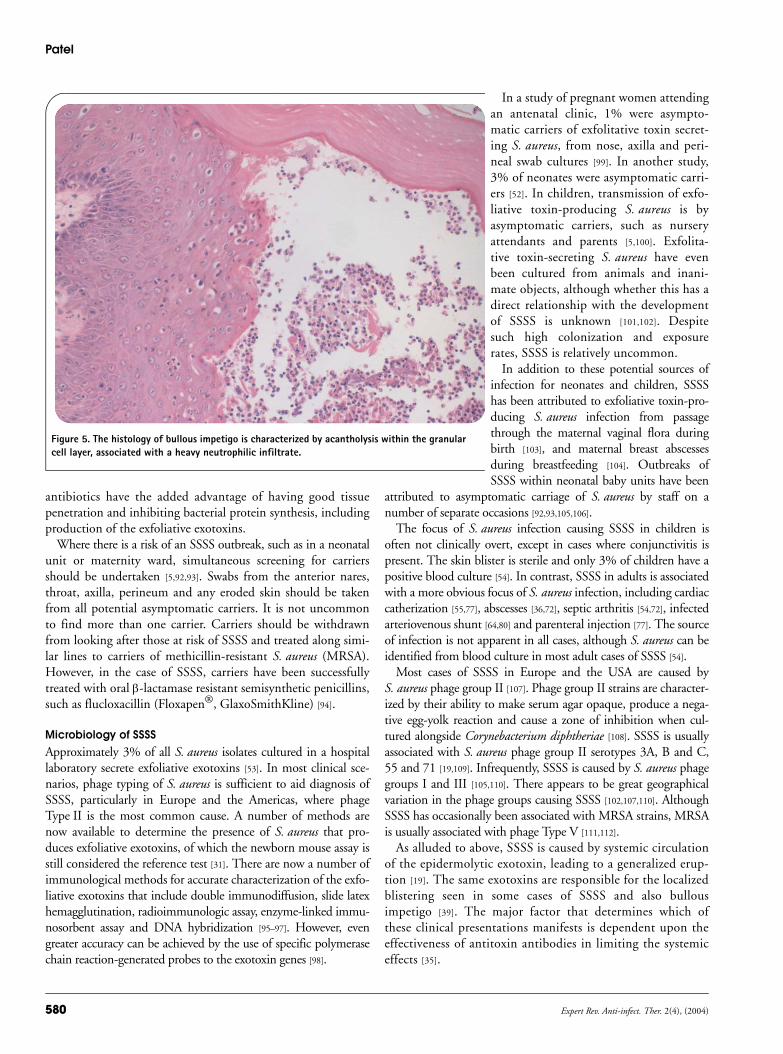
In the presence of blistering, SSSS should be distinguishedfrom bullous impetigo and pemphigus (in particular the variantpemphigus foliaceus). In contrast to SSSS, bullous impetigo iscaused by a direct innoculum of S. aureus that results in a local-ized but not systemic release of S. aureus exfoliative exotoxin andtherefore, localized blistering. Upon rupture, the blister oozesserous exudates that gives rise to an adherent golden-yellowcrust that is rich in bacteria. The surrounding skin in bullousimpetigo is inflamed, reflecting the acute localized inflammatoryresponse (FIGURE 4), which, histologically, is neutrophil rich(FIGURE 5). Subcorneal immunoglobulin (Ig)A pemphigus andpemphigus foliaceus are autoimmune disorders characterized byantibodies that target epidermal proteins within the upper layersof the epidermis and similarly cause a split along the granularcell layer. Both conditions are associated with positive directimmunofluorescence and a dermal lymphocyte rich inflamma-tory cell infiltrate, helping to distinguish them from SSSS. Inpemphigus foliaceus, the target antigen is also DG-1, whereas insubcorneal IgA pemphigus the antigen is desmocollin-1 [51].
Natural history & susceptibilityDespite the high prevalence of ET-producing S. aureus in up to25% of S. aureus isolates, there appear to be a number of otherfactors necessary for the development of SSSS [52,53]. For exam-ple, healthy adults rarely develop SSSS and currently only fivesuch cases have been reported [49,54–56].
An explanation for this rarity is the formation of antibodiesagainst the ETs that protect against the effect of the toxins;indeed, 91% of adults have antibodies to ET-A [35]. However,antibody levels are detectable in only 30% of babies aged3 months to 2 years, but then rise steadily so that at 2 to5 years, 42% have ET-A antibodies, and over the age of40 years, 91% have antibodies [35]. These findings are compati-ble with the clinical observation of SSSS predominantly affect-ing young children and rarely adults. Toxins are initially absentin patients with SSSS antibodies against the ETs but are presentin the convalescent sera [57–59]. Therefore, this theory wouldexplain why SSSS tends not to reoccur. In fact, there are only
Figure 2. Characteristically, the disease affects the flexures. The involved skin shears easily, revealing a painful erythematous base. Superficial blisters may be evident and exhibit a positive Nikolsky sign. Often uninvolved skin also shears easily, which can result in iatrogenic injury from the application of adherent dressings such as those that may be used to maintain intravenous canuli [COURTESY OF C MILLS, ROYAL
GWENT HOSPITAL, NEWPORT, UK].
Patel
578 Expert Rev. Anti-infect. Ther. 2(4), (2004)
three reported cases of recurrent SSSS [60,61]. The first case was ina 50-year-old woman, with epilepsy and cerebellar ataxia, whohad repeated episodes of SSSS over 2 years [60]. The second andthird cases were in two male siblings aged 5 and 12 years oldwho had localized SSSS that reoccurred once, within 12 months[61]. It is unclear if these patients had or were able to mount anantibody response to the S. aureus ETs. In contrast to SSSS,patients with bullous impetigo have circulating antibodiesthroughout the illness [35].
The severity of SSSS is closely related to the amount ofcirculating ETs and at very high concentrations may be enoughto overcome the protective effects of circulating antitoxin anti-bodies [39,62]. Thus, adults who develop SSSS often have severeS. aureus infection with a high ET production and an inabilityto mount a sufficient immune response [63]. Frequently, andnot surprisingly, adult SSSS develops in individuals who have asuppressed immune system, caused by:
• An inherited defect in the immune system [44]
• HIV [64–68]
• Immunosuppressant drugs [69–71]
• Malignancy [47,69,72–74]
• Chronic alcohol abuse [72,75]
• Heroin addiction [76]
• Severe sepsis [72,77]
Many of these cocontributory conditions are also associatedwith an increased risk of S. aureus colonization that increasesthe likelihood of ET-secreting S. aureus infection [4,7–12].
Melish and colleagues were able to clearly demonstrate, using amouse model, that the development of SSSS is dependent on age[19,30,31]. In their study, they showed how only neonatal miceunder 5 days of age developed the disease after subcutaneous orintraperitoneal inoculation with S. aureus derived from SSSSpatients. In their attempt to explain this phenomena, prior to thediscovery of epidermolytic exotoxin or antibodies against them,they went on to show that the toxins were unaffected by livermetabolism and excreted by the kidney. Healthy adult kidneyswere able to excrete the toxin burden more efficiently than thoseof neonatal mice, 33 versus 7% within the first 3 h, respectively[78]. Moreover, adult mice could be induced to develop SSSS afternephrectomy [78], explaining why the majority of adults whodevelop SSSS have renal impairment often requiring dialysis[36,54,64,75,79–84]. Patients with renal impairment also have muchhigher rates of S. aureus colonization, in particular those receivingdialysis, and are also at greater risk of inoculation from invasiveprocedures or investigations [12,85].
Rarely, otherwise healthy adults have developed SSSS whilsttaking nonsteroidal anti-inflammatory drugs (NSAIDs), possiblydue to impaired renal excretion of the ET [86,87]. The concurrentadministration of NSAIDs has also been shown to aggravate dis-eases caused by other S. aureus toxin, such as toxic shock syndrometoxins and α-toxin [88]. In these diseases it is believed that NSAIDspotentiate the disease by modulation of cytokine release.
Treatment, prognosis & preventionSSSS should be subdivided based upon the extent of bodysurface affected into:
• Mild (≤10%)
• Moderate (≤20%)
• Severe (>20%)
In all cases, early diagnosis, assessment and prompt treatmentwith an appropriate parenteral antistaphylococcal antibiotic areessential for the successful management of SSSS [54].
Mild disease is the most common presentation. Suchpatients are best managed with strict isolation and barrier nurs-ing to prevent crossinfection. Prompt administration of antibi-otics, either through oral or parentral routes should begin assoon as SSSS is clinically suspected and prior to confirmationof the diagnosis by microbiology, histology and immunofluo-rescence. Topical administration of antibiotics is ineffective,since the focus of infection is usually not known and often dis-tant to the site of blistering. All reported strains of S. aureusassociated with SSSS have been penicillin-resistant, but are
Figure 3. Skin histology from a perilesional skin biopsy. Acantholysis can be seen within the granular cell layer, in the absence of inflammatory cells or microbes within the epidermis.
Staphylococcal scalded skin syndrome
www.future-drugs.com 579
usually sensitive to semisynthetic penicillin,although the choice of which antibioticto use should be based on local knowl-edge of antibiotic resistance [19,31]. AsSSSS is an extremely painful condition,adequate analgesia should not be over-looked. The choice of analgesia is basedon the needs of the patient and opiatesare preferred to NSAIDs. Blisters shouldbe left intact and eroded skin treated withan emollient or covered with Vaseline®
(Elida Fabergé Ltd) impregnated gauze tomaintain the skin barrier function, aswell as reduce further skin trauma. Anti-septics, such as those combined withemollients, can be employed to reducesecondary colonization. Sulphdiazineshould be used with caution when thebody surface area involved is greater than5%, due to the risk of systemic absorp-tion of silver. If there is conjunctivitis,the eyes should be cleansed regularly anda topical antibiotic applied. Once feverand discomfort have subsided, no newblisters develop and existing affectedareas show signs of re-epithelialization,antibiotics can safely be administeredorally. Treated correctly, the mortalityrate for mild-to-moderate disease shouldbe negligible. Corticosteroids, adminis-tered either by the oral or topical route, are associated with aworsening of the disease and so are contraindicated in themanagement of SSSS [30,89,90].
In addition to the management strategy mentioned above,additional factors need to be addressed when the area of skininvolvement is greater than 10%:
• Consider admission to an intensive care unit• Infection risk assessment and management• Temperature regulation• Fluid management• Pain management• Nutritional care• Skin care• Mattress requirement
In severe disease there is loss of the skin barrier function,akin to a burns injury. Indeed, many patients with extensive SSSSare managed in burns units [91]. Thermal dysregulation is com-mon, although the patient is febrile, peripheral vasodilatation addsto loss of heat and may cause a drop in the core temperature. Thecore temperature and room temperature need to be monitoredcarefully and alteration in room temperature made to compensatefor changes in core body temperature. Fluid loss can also be con-siderable during such illness and needs to be replaced by either oralor parenteral route. There are set criteria for managing fluid
requirement based on burn injury data, and these should be strictlyadhered to [91]. The eroded skin and intravenous access can act asportals of secondary infection and sepsis. There should be regularuse of antiseptics, careful monitoring of patients for sepsis and alow threshold for broadening the antibiotic spectrum. Immobility,the presence of moisture, loss of skin barrier, poor nutritional statusand potential shearing forces all increase the risk of pressure sores.Appropriate measures to address the risk factors for pressure injuryshould be instituted, including good nursing care, regular turningof the patient, adequate nutrition and the use of an appropriatepressure-relieving mattresses. The mortality in childhood SSSS isapproximately 4% and usually occurs when there is extensive skininvolvement, overwhelming sepsis and a resultant electrolyteimbalance [50].
Management of adult-onset SSSS remains a major medicalchallenge. The mortality rate in adult onset SSSS is over 60%[37,54,89]. In addition to the measures mentioned so far, there is aneed to identify and treat the focus of infection as well as managingthe predisposing disease. The most common cofactors leading tothe development of adult SSSS are severe sepsis, immunosuppres-sion and renal impairment. The choice of antibiotics should bebroadened to treat both penicillinase resistance, as well as the possi-bility of methicillin resistance, thus ciprofloxacin, gentamicin, van-comycin (Vancocin®, Eli Lilly, Ltd.) and clindamycin(Dalacin C®, Pfizer Ltd) should be considered. Many of these
Figure 4. Bullous impetigo, in contrast to staphylococcal scalded skin syndrome, is characterized by local inflammatory blisters that are also fragile. Blisters rupture easily, leaving an adherent golden yellow crust.
Patel
580 Expert Rev. Anti-infect. Ther. 2(4), (2004)
antibiotics have the added advantage of having good tissuepenetration and inhibiting bacterial protein synthesis, includingproduction of the exfoliative exotoxins.
Where there is a risk of an SSSS outbreak, such as in a neonatalunit or maternity ward, simultaneous screening for carriersshould be undertaken [5,92,93]. Swabs from the anterior nares,throat, axilla, perineum and any eroded skin should be takenfrom all potential asymptomatic carriers. It is not uncommonto find more than one carrier. Carriers should be withdrawnfrom looking after those at risk of SSSS and treated along simi-lar lines to carriers of methicillin-resistant S. aureus (MRSA).However, in the case of SSSS, carriers have been successfullytreated with oral β-lactamase resistant semisynthetic penicillins,such as flucloxacillin (Floxapen®, GlaxoSmithKline) [94].
Microbiology of SSSSApproximately 3% of all S. aureus isolates cultured in a hospitallaboratory secrete exfoliative exotoxins [53]. In most clinical sce-narios, phage typing of S. aureus is sufficient to aid diagnosis ofSSSS, particularly in Europe and the Americas, where phageType II is the most common cause. A number of methods arenow available to determine the presence of S. aureus that pro-duces exfoliative exotoxins, of which the newborn mouse assay isstill considered the reference test [31]. There are now a number ofimmunological methods for accurate characterization of the exfo-liative exotoxins that include double immunodiffusion, slide latexhemagglutination, radioimmunologic assay, enzyme-linked immu-nosorbent assay and DNA hybridization [95–97]. However, evengreater accuracy can be achieved by the use of specific polymerasechain reaction-generated probes to the exotoxin genes [98].
In a study of pregnant women attendingan antenatal clinic, 1% were asympto-matic carriers of exfolitative toxin secret-ing S. aureus, from nose, axilla and peri-neal swab cultures [99]. In another study,3% of neonates were asymptomatic carri-ers [52]. In children, transmission of exfo-liative toxin-producing S. aureus is byasymptomatic carriers, such as nurseryattendants and parents [5,100]. Exfolita-tive toxin-secreting S. aureus have evenbeen cultured from animals and inani-mate objects, although whether this has adirect relationship with the developmentof SSSS is unknown [101,102]. Despitesuch high colonization and exposurerates, SSSS is relatively uncommon.
In addition to these potential sources ofinfection for neonates and children, SSSShas been attributed to exfoliative toxin-pro-ducing S. aureus infection from passagethrough the maternal vaginal flora duringbirth [103], and maternal breast abscessesduring breastfeeding [104]. Outbreaks ofSSSS within neonatal baby units have been
attributed to asymptomatic carriage of S. aureus by staff on anumber of separate occasions [92,93,105,106].
The focus of S. aureus infection causing SSSS in children isoften not clinically overt, except in cases where conjunctivitis ispresent. The skin blister is sterile and only 3% of children have apositive blood culture [54]. In contrast, SSSS in adults is associatedwith a more obvious focus of S. aureus infection, including cardiaccatherization [55,77], abscesses [36,72], septic arthritis [54,72], infectedarteriovenous shunt [64,80] and parenteral injection [77]. The sourceof infection is not apparent in all cases, although S. aureus can beidentified from blood culture in most adult cases of SSSS [54].
Most cases of SSSS in Europe and the USA are caused byS. aureus phage group II [107]. Phage group II strains are character-ized by their ability to make serum agar opaque, produce a nega-tive egg-yolk reaction and cause a zone of inhibition when cul-tured alongside Corynebacterium diphtheriae [108]. SSSS is usuallyassociated with S. aureus phage group II serotypes 3A, B and C,55 and 71 [19,109]. Infrequently, SSSS is caused by S. aureus phagegroups I and III [105,110]. There appears to be great geographicalvariation in the phage groups causing SSSS [102,107,110]. AlthoughSSSS has occasionally been associated with MRSA strains, MRSAis usually associated with phage Type V [111,112].
As alluded to above, SSSS is caused by systemic circulationof the epidermolytic exotoxin, leading to a generalized erup-tion [19]. The same exotoxins are responsible for the localizedblistering seen in some cases of SSSS and also bullousimpetigo [39]. The major factor that determines which ofthese clinical presentations manifests is dependent upon theeffectiveness of antitoxin antibodies in limiting the systemiceffects [35].
Figure 5. The histology of bullous impetigo is characterized by acantholysis within the granular cell layer, associated with a heavy neutrophilic infiltrate.

Staphylococcal scalded skin syndrome
www.future-drugs.com 581
Currently, five different ETs have been identified (TABLE 1,
FIGURE 6): ET-A, -B, -C and -D and Staphylococcus hyicus(Sh)ET [105,105,110,113–117]. Of the ETs mentioned, only ET-Aand -B are known to cause SSSS and bullous impetigo inhumans. The nucleotide sequences of both ET-A and -B havebeen established [110,118,119], their respective genes have beensequenced [119–121] and the ET-A gene has been cloned inEscherichia coli [122]. ET-A is the most commonly secretedtoxin, is a heat stable protein, is encoded on the bacterial chro-mosome and is produced by 89% of isolates [113]. ET-B is aplasmid-derived heat labile protein, which is produced by 4%of isolates [113]. In approximately 17% of S. aureus frompatients with SSSS, ET-A and -B are cosecreted [113]. There aregeographic differences in the incidence of the different strainsof S. aureus. In Japan, S. aureus appears to secrete ET-B ratherthan ET-A. Furthermore, the prevalence of ET-B secretingS. aureus appears to be increasing [95,105,123].
Molecular basis of SSSSRecently, the target antigen for ET-A, -B and -D has beenidentified as the epidermal cell attachment protein DG-1[38,41,116]. DG-1 has been suspected to be the target antigenfor the exfoliative exotoxins due to the histological and clini-cal similarities between SSSS and pemphigus foliaceus[38,124]. Although DG-1 is expressed throughout the epider-mis, in the lower epidermis DG-3 is coexpressed and is ableto compensate for the loss of DG-1 function (FIGURE 1) [125].In a series of experiments, Amagai and colleagues showedDG-1 to be the target antigen for ET-A [38]. Through theinjection of ET-A into neonatal skin, followed by directimmunofluorescence on skin epidermis using antibodies thattarget DG-1 and -3, the authors observed reduced, disruptedand cytoplasmic staining of DG-1 instead of the normalmembrane staining. In contrast, the DG-3 staining patternremained normal. Human keratinocytes adult skin epider-mis, calcium reduced level, temperature elevated (HaCaT)cells were then transfected with cDNA encoding mouse DG-1 and -3, containing a flagellar antigen (FLAG) octapeptideepitope on its carboxyl termini. The transfected cells were
then incubated with ET-A and western blot analysis withantibodies against the FLA G peptide revealed degradationof DG-1, but not the closely related DG-3. Subsequently,neonatal mice were injected with ET-A and western blotanalysis was used for DG-1, -3 and other epidermal cadher-ins on the skin extracts of superficial blisters. This showeddegradation of DG-1 only, revealing a cleaved 113 kDa frag-ment instead of the normal 160 kDa. ET-B and -D havebeen shown to similarly cleave DG-1, with an identicalcleavage product [116,126].
It has been believed for some time that ETs are proteolyticenzymes that cause epidermal separation through cleavage ofattachment molecules. Indeed, early studies demonstratedstructural similarities to the staphylococcal V8 serine pro-tease, a trypsin-like serine protease, with sequence homologyto the active site a serine–aspartic acid–histidine catalytictriad [134]. Mutational analysis of the ET showed that substi-tution of any one of the three central amino acids resulted incomplete loss of their biological activity, when injected intonewborn mice [127]. Later, computer modelling [128] and crys-tallography [129] of the three dimensional structure revealed ahigh degree of similarity with known glutamate specifictrypsin-like serine proteases. After Amagai and colleagues hadidentified DG-1 as the target of the ETs, they went on toshow that the cleavage site of DG-1, as determined by protein
Table 1. There are at least five ETs identified thus far. Of these, ET-A and -B are known to cause SSSS and bullous impetigo in humans.
ET Host Frequency Origin Molecular mass(kDa)
Heat sensitivity
Genetic control
Mouse model
ET-A Human Common S. aureus 30,000 Heat stable Chromosome Causes intraepidermal split
ET-B Human Common S. aureus 29,500 Heat labile Plasmid Causes intraepidermal split
ET-C Horse ? S. aureus 27,000 Heat labile Chromosome Causes intraepidermal split
ET-D Human Unlikely, as yet not identified in SSSS or bullous impetigo
S. aureus 27,000 Heat stable? Chromosome Causes intraepidermal split
ShET Piglets ? S. hyicus 27,000 Heat labile ? Does not cause intraepidermal split
ET: Epidermolytic toxin; S. aureus: Staphylococcus aureus; ShET: S. hyicus ET; S. hyicus: Staphylococcal hyicus; SSSS: Staphylococcal scalded skin syndrome.
0.423
0.158
0.171
0.202
0.291
0.134
0.476
0.087
ShET-A
ShET-B
ORF1
ET-B
ET-AET-C
Figure 6. Phylogenetic tree. Using pair-wise analysis to calculate a distance matrix, Yamaguchi and colleagues have proposed a phylogenetic tree illustrating the relationships between the different ETs. The distance is equal to the number of exact matches divided by the overall nucleotide sequence length, using a conventional 0.05 scale [116].ET: Epidermolytic toxin; ORF: Open reading frame; ShET: Staphylococcus hyicus ET.

Patel
582 Expert Rev. Anti-infect. Ther. 2(4), (2004)
sequencing of the resultant cleaved products, was consistent withspecific cleavage at glutamic acid residue 381 [38,39]. This cleavagesite is located between the third and forth extracellular domains,and mutation of the predicted site completely inhibited cleavage[39]. Furthermore, the group went on to demonstrate dose-dependent cleavage of the extracellular domain of mouse andhuman DG-1 [38,39]. The proteolytic activity of ET-A is depend-ent upon a calcium binding mechanism that can be inhibited byethylenediaminetetra-acetic acid (EDTA) [130]. Based upon struc-tural studies of the DG cadherin protein family, calcium binding,which stabilizes the rigidity and orientation of the protein, hasbeen shown to be critical [131]. Therefore, it can be assumed thatthe presence of calcium within the DG complex facilitates prote-olysis. Also, if proteolysis was to impair the ability of DG to bindcalcium, this would lead to the functional loss of DG-1 andtherefore cell separation would occur. However, it remainsunclear why in vitro and in vivo studies using protease inhibitorshave failed to prevent epidermolysis [50].
Five-year view: the unanswered questionsThe comparison between pemphigus foliaceus and SSSS hasmany virtues and clearly there are important overlaps, includ-ing sharing the same antigenic target, DG-1. However, furtherexperimentation is needed to elucidate the obvious differencesthat exist between SSSS and pemphigus foliaceus (TABLE 2).
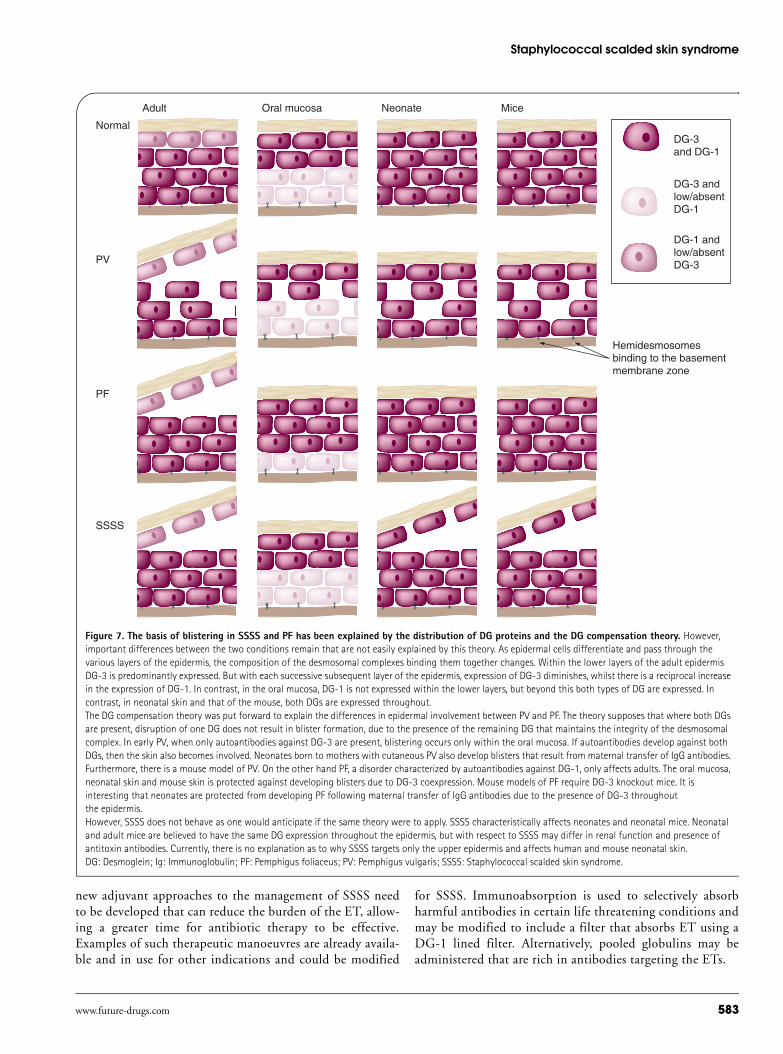
One central question that remains to be addressed is howSSSS targets neonates, when our current understanding of thepathophysiology would suggest that two independent proc-esses protect neonates. Firstly, in approximately 90% of new-borns, cord blood samples contain effective antitoxin anti-bodies, as part of the maternal transfer of immunoglobulinprotection [132]. Maternal antibodies are usually present for upto 6 months, yet SSSS is still able to occur within this period.The second factor is based upon the DG compensation the-ory, derived from our understanding of pemphigus, which sug-gests that the presence of DG-3 protects the lower epidermis
and mucosa from also undergoing epidermal cell detachment(FIGURE 7). This theory is used to explain why maternal anti-body transfer containing the pemphigus vulgaris autoanti-body (targeting DG-3) can cause neonatal pemphigus vul-garis, but that maternal transfer of the pemphigus foliaceusautoantibody (targeting DG-1) is unable to cause neonatalpemphigus foliaceus (FIGURE 3). Wu and colleagues found thatneonatal skin expresses DG-3 throughout the epidermis,which would protect against the development of neonatalpemphigus foliaceus [133]. Yet it appears that neonates are notprotected against the development of SSSS.
It also remains to be determined how and why NSAIDSand corticosteroids, administered either by the topical ororal route, are detrimental in SSSS and not in pemphigusfoliaceus. It is hoped that over the next 5 years the answersto these questions will greatly enhance our knowledge of thepathogenesis of SSSS.
Expert opinionIn conclusion, a century after von Rittershain described SSSS,our understanding of the cause and management of this devas-tating condition has come a long way. However, over and abovethe theory, SSSS remains a dramatic, painful experience forpatients and parents. Appropriate management with antibioticsand supportive care, including analgesia, is essential, whilst tak-ing care to avoid cross infection. When the affected body sur-face area of skin exceeds 25%, supportive care needs to considerfluid loss, temperature dysregulation and nutritional needs. Inall cases, good nursing care is needed to minimize the discom-fort associated with this condition. Corticosteroids should notbe used, as they clearly have a detrimental effect.
The advent of improved hygiene and effective antibiotictherapy has dramatically altered the prognosis for childrensuffering with SSSS. However, there remain individuals forwhom antibiotics alone are not effective, in particular adultswith SSSS where the prognosis remains grim. For this group,
Table 2. PF autoantibodies and SSSS ETs disrupt the desmosomal cell–cell attachment complex by binding to DG-1. Both result in superficial blistering disease in humans and when injected into mice. Important differences remain despite the obvious overlap in pathogenesis, some of which can be explained by the presence of antibodies against ETs that prevent SSSS from developing.
PF, caused by autoantibodies SSSS, caused by ETs
NeonateMouse Blistering, due to adult pattern DG expression Blistering
Human No blistering, due to epidermal DG-3 expression Blistering, despite epidermal expression of DG-3 and maternal transfer of antitoxin antibodies
Child or adultMouse Blistering No blistering
Human Blistering No blistering, believed to be due to presence of antitoxin antibodies
DG: Desmoglein; ET: Epidermolytic toxin; PF: Pemphigus foliaceus; SSSS: Staphylococcal scalded skin syndrome.
Staphylococcal scalded skin syndrome
www.future-drugs.com 583
new adjuvant approaches to the management of SSSS needto be developed that can reduce the burden of the ET, allow-ing a greater time for antibiotic therapy to be effective.Examples of such therapeutic manoeuvres are already availa-ble and in use for other indications and could be modified
for SSSS. Immunoabsorption is used to selectively absorbharmful antibodies in certain life threatening conditions andmay be modified to include a filter that absorbs ET using aDG-1 lined filter. Alternatively, pooled globulins may beadministered that are rich in antibodies targeting the ETs.
Adult Oral mucosa Neonate Mice
Normal
PF
PV
SSSS
DG-3and DG-1
DG-1 andlow/absentDG-3
DG-3 andlow/absentDG-1
Hemidesmosomesbinding to the basementmembrane zone
Figure 7. The basis of blistering in SSSS and PF has been explained by the distribution of DG proteins and the DG compensation theory. However, important differences between the two conditions remain that are not easily explained by this theory. As epidermal cells differentiate and pass through the various layers of the epidermis, the composition of the desmosomal complexes binding them together changes. Within the lower layers of the adult epidermis DG-3 is predominantly expressed. But with each successive subsequent layer of the epidermis, expression of DG-3 diminishes, whilst there is a reciprocal increase in the expression of DG-1. In contrast, in the oral mucosa, DG-1 is not expressed within the lower layers, but beyond this both types of DG are expressed. In contrast, in neonatal skin and that of the mouse, both DGs are expressed throughout.The DG compensation theory was put forward to explain the differences in epidermal involvement between PV and PF. The theory supposes that where both DGs are present, disruption of one DG does not result in blister formation, due to the presence of the remaining DG that maintains the integrity of the desmosomal complex. In early PV, when only autoantibodies against DG-3 are present, blistering occurs only within the oral mucosa. If autoantibodies develop against both DGs, then the skin also becomes involved. Neonates born to mothers with cutaneous PV also develop blisters that result from maternal transfer of IgG antibodies. Furthermore, there is a mouse model of PV. On the other hand PF, a disorder characterized by autoantibodies against DG-1, only affects adults. The oral mucosa, neonatal skin and mouse skin is protected against developing blisters due to DG-3 coexpression. Mouse models of PF require DG-3 knockout mice. It is interesting that neonates are protected from developing PF following maternal transfer of IgG antibodies due to the presence of DG-3 throughout the epidermis. However, SSSS does not behave as one would anticipate if the same theory were to apply. SSSS characteristically affects neonates and neonatal mice. Neonatal and adult mice are believed to have the same DG expression throughout the epidermis, but with respect to SSSS may differ in renal function and presence of antitoxin antibodies. Currently, there is no explanation as to why SSSS targets only the upper epidermis and affects human and mouse neonatal skin.DG: Desmoglein; Ig: Immunoglobulin; PF: Pemphigus foliaceus; PV: Pemphigus vulgaris; SSSS: Staphylococcal scalded skin syndrome.
Patel
584 Expert Rev. Anti-infect. Ther. 2(4), (2004)
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Wilkinson BJ. The staphylococci in human disease. In: Biology. Crossley KB, Archer GL (Eds), Churchill Livingstone, NY, USA (1997).
2 Lee JC. The prospects for developing a vaccine against Staphylococcus aureus. Trends Microbiol. 4, 162–166 (1996).
3 Hay RJ, Adriaans BM. Bacterial infections. In: Textbook of Dermatology, Sixth Edition. Champion RH, Burton JL, Burns DA, Breathnach SM (Eds), Blackwell Sciences Ltd, Oxford, UK (1998).
4 Hutchison JG, Green CA, Grimson TA. Nasal carriage of Staphylococcus aureus in nurses. J. Clin. Pathol. 195, 10, 92–95 (1957).
5 Dancer SJ, Simmons NA, Poston SM, Noble WC. Outbreak of staphylococcal scalded skin syndrome among neonates.J. Infect. 16, 87–103 (1988).
6 Hargiss C, Larson E. The epidemiology of Staphylococcus aureus in a newborn nursery from 1970 through 1976. Pediatrics 61, 348–353 (1978).
7 Wenzel RP, Perl TM. The significance of nasal carriage of Staphylococcus aureus and the incidence of postoperative wound infection. J. Hosp. Infect. 31, 13–24 (1995).
8 Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesion of atopic dermatitis. Br. J. Dermatol. 90, 525–530 (1974).
9 Tuazon CU, Perez A, Kishaba T, Sheagren JN. Staphylococcus aureus among insulin-injecting diabetic patients: an increased carrier rate. J. Am. Med. Assoc. 231, 1272 (1975).
10 Tuazon CU, Sheagren JN. Increased rate of carriage of Staphylococcus aureus among narcotic addicts. J. Infect. Dis. 129, 725–727 (1974).
11 Weinke T, Schiller R, Fehrenbach FJ, Pohle HD. Association between Staphylococcus aureus nasopharyngeal colonization and septicemia in patients infected with the human immunodeficiency virus. Eur. J. Clin. Microbiol. Infect. Dis. 11, 985–989 (1992).
12 Yu VL, Goetz A, Wagener M et al. Staphylococcus aureus nasal carriage and infection in patients on hemodialysis: efficacy of antibiotic prophylaxis. N. Engl. J. Med. 315, 91–96 (1986).
13 Pittet D, Wenzel RP. Nosocomial bloodstream infections: secular trends in rates, mortality, and contribution to total hospital deaths. Arch. Intern. Med. 155, 1177–1184 (1995).
14 Ayliffe GA. The progressive intercontinental spread of methicillin-resitant Staphylococcus aureus. Clin. Infect. Dis. 24(Suppl. 1), S74–S79 (1997).
15 Kallman JE, Kihlstrom J, Joberg L, Schollin J. Increase in staphylococci in neonatal septicaemia: a 14-year study. Acta Paediatr. 86, 533–538 (1997).
16 Mehtar S. The continuing problem of ‘hospital staphylococci’: why?J. Chemother. 6(Suppl. 4), 25–40 (1994).
17 Bhakdi S, Tranum-Jensen J. α-toxin of Staphylococcus aureus. Microbiol. Rev. 55, 733–751 (1991).
18 Marrack P, Kappler J. The staphylococcal enterotoxins and their relatives. Science 248, 705–711 (1990).
19 Melish ME, Glasgow LA. The staphylococcal scalded-skin syndrome.N. Engl. J. Med. 282, 1114–1119 (1970).
•• Eestablishes that the cause of staphylococcal scalded skin syndrome is a Staphylococcus aureus exotoxin.
20 Ritter von Rittershain G. Die exfoliativa dermatitis jüngerer Säulinge. Centralz Kinderheilk 2, 3–23 (1878).
21 Almquist E. Pemphigus neonatorum, backteriologisch und epidemiologisch beleuchtet. Z. Hyg. Infec. 10, 253 (1891).
22 Lyell A. Toxic epidermal necrolysis: an eruption resembling scalding of the skin. Br. J. Dermatol. 68, 355–361 (1956).
23 Lyell A, Dick HM, Alexander JO. Outbreak of toxic epidermal necrolysis associated with staphylococci. Lancet 1, 787–789 (1969).
24 Lyell A. A review of toxic epidermal necrolysis in Britain. Br. J. Dermatol. 79, 662–671 (1967).
25 Jefferson J. Lyell’s toxic epidermal necrolysis: a staphylococcal etiology? Br. Med. J. 555, 802–804 (1967).
26 Tyson RG, Ushinski SC, Kisilevsky R. Toxic epidermal necrolysis (the scalded skin syndrome). Its association in two cases with pathogenic staphylococci and its similarity in infancy to Ritter’s disease. Am. J. Dis. Child. 111, 386–392 (1966).
27 Messaritakis J. Toxic epidermal necrolysis in children (description of 4 cases). Ann. Paediatr. 207, 236–246 (1966).
28 Lowney ED, Baublis JV, Kreye GM et al. The scalded skin syndrome in small children. Arch. Dermatol. 95, 359–369 (1967).
29 Lyell A. The staphylococcal scalded skin syndrome in historical perspective: emergence of dermopathic strains of Staphylococcus aureus and discovery of the epidermolytic toxin. A review of events up to 1970. J. Am. Acad. Dermatol. 9, 285–294 (1983).
30 Melish ME, Glasgow LA, Turner MD. The staphylococcal scalded-skin syndrome: isolation and partial characterization of the exfoliative toxin. J. Infect. Dis. 125, 129–140 (1972).
31 Melish ME, Glasgow LA. Staphylococcal scalded skin syndrome: the expanded clinical syndrome. J. Pediatr. 78, 958–967 (1971).
32 Kapral FA, Miller MM. Product of Staphylococcus aureus responsible for the scalded skin syndrome. Infect. Immun. 4, 541–545 (1971).
Key issues
• The prevalence of Staphylococcus aureus is high and is thought to be associated with high population densities within cities.
• Certain strains of S. aureus release epidermolytic toxins that can cause bullous impetigo or staphylococcal scalded skin syndrome (SSSS), depending upon the host immune response and predisposition.
• Epidermolytic toxins target and cleave the epidermal cell attachment protein desmoglein-1.
• SSSS is a disorder that mainly affects neonates and young children, but may rarely occur in susceptible adults.
• SSSS is a very painful condition, and the overall morbidity relates to the extent of skin involved.
• Mortality due to SSSS is now low in neonates and children, but remains very high in adults.
Staphylococcal scalded skin syndrome
www.future-drugs.com 585
33 Elias PM, Fritsch P, Mittermayer H et al. Experimental staphylococcal toxic epidermal necrolysis (TEN) in adult humans and mice. J. Lab. Clin. Med. 84, 414–424 (1974).
34 Arbuthnott JP, Kent J, Lyell A. Studies of staphylococcal toxins in relation to toxic epidermal necrolysis: the scalded skin syndrome. Br. J. Dermatol. 86(Suppl.), S35–S39 (1972).
35 Melish ME, Chen FS, Sprouse S et al. Epidermolytic toxin in staphylococcal infection: toxin levels and host response. Zentralbl. Bakteriol. 10(Suppl.), 287–298 (1981).
• Important study of age and presence of antibodies against exfoliative toxin A.
36 Levine G, Norden CW. Staphylococcal scalded-skin syndrome in an adult. N. Engl. J. Med. 287, 1339–1340 (1972).
•• First report of adult-onset staphylococcal scalded skin syndrome.
37 Patel GK, Finlay AY. Staphylococcal scalded skin syndrome: diagnosis and management. Am. J. Clin. Dermatol. 4, 165–175 (2003).
•• Clearly outlines the diagnostic criteria for staphylococcal scalded skin syndrome.
38 Amagai M, Matsuyoshi N, Wang ZH, Andl C, Stanley JR. Toxin in bullous impetigo and staphylococcal scalded skin syndrome targets desmoglein-1. Nature Med. 6, 1275–1277 (2000).
•• Key paper, showing that desmoglein-1 is the target for the exfoliative toxin.
39 Hanakawa Y, Schechter NM, Lin C et al. Molecular mechanisms of blister formation in bullous impetigo and staphylococcal scalded skin syndrome. J. Clin. Invest. 110, 53–60 (2002).
•• Key paper, outlining the cleavage site on desmoglein-1 in staphylococcal scalded skin syndrome.
40 Amagai M. Desmoglein as a target in autoimmunity and infection. J. Am. Acad. Dermatol. 48, 244–252 (2003).
41 Amagai M, Yamaguchi T, Hanakawa Y, Nishifuji K, Sugai M, Stanley JR. Staphylococcal exfoliative toxin B specifically cleaves desmoglein-1. J. Invest. Dermatol. 118, 845–850 (2002).
42 Salopek TG. Nikolsky’s sign: is it ‘dry’ or is it ‘wet’? Br. J. Dermatol. 136, 762–767 (1997).
43 Holme SA, Davies JH, Mills CM. Iatrogenic injury in childhood staphylococcal scalded skin syndrome. J. Paediatr. Child Health 39, 73–74 (2003).
44 Reid LH, Weston WL, Humbert JR. Staphylococcal scalded skin syndrome. Adult onset in a patient with deficient cell-mediated immunity. Arch Dermatol 109, 239–241 (1974).
45 Norden CW, Mendelow H. Letter: staphylococcal scalded skin syndrome in adults. N. Engl. J. Med. 290, 577 (1974).
46 Fine JD, Harrist TJ, Radford MJ. Adult scalded skin syndrome fatally complicated by mixed Gram-negative sepsis and cellulitis. Cutis 27, 162–167 (1981).
47 Amon RB, Dimond RL. Toxic epidermal necrolysis: rapid differentiation between staphylococcal- and drug-induced disease. Arch. Dermatol. 111, 1433–1437 (1975).
48 Falk DK, King LEJ. Criteria for the diagnosis of staphylococcal scalded skin syndrome in adults. Cutis 31, 421–424 (1983).
49 Patel GK, Varma S, Finlay AY. Staphyloccocal scalded skin syndrome in healthy adults. Br. J. Dermatol. 142, 1253–1255 (2000).
50 Elias PM, Fritsch P, Epstein EH. Staphylococcal scalded skin syndrome. Clinical features, pathogenesis, and recent microbiological and biochemical developments. Arch Dermatol 113, 207–219 (1977).
51 Robinson ND, Hashimoto T, Amagai M, Chan LS. The new pemphigus variants.J. Am. Acad. Dermatol. 40, 649–671 (1999).
• Good review of pemphigus and variants.
52 Elsner P, Hartmann AA. Epidemiology of ET-A- and ET-B-producing staphylococci in dermatological patients. Zentrlbl. Bakteriol. Mikrobiol. Hyg. (A) 268, 534 (1988).
53 Dancer SJ, Noble WC. Nasal, axillary, and perineal carriage of Staphylococcus aureus among women: identification of strains producing epidermolytic toxin. J. Clin. Pathol. 44, 681–684 (1991).
54 Cribier B, Piemont Y, Grosshans E. Staphylococcal scalded skin syndrome in adults. A clinical review illustrated with a new case. J. Am. Acad. Dermatol. 30, 319–324 (1994).
• Clinical review of staphylococcal scalded skin syndrome.
55 Opal SM, Johnson-Winegar AD, Cross AS. Staphylococcal scalded skin syndrome in two immunocompetent adults caused by exfoliatin B-producing Staphylococcus aureus. J. Clin. Microbiol. 26, 1283–1286 (1988).
56 Oyake S, Oh-i T, Koga M. Staphylococcal scalded skin syndrome in a healthy adult.J. Dermatol. 28, 145–148 (2001).
57 Wiley B, Glasgow L, Rogolsky M. Studies on staphylococcal scalded skin syndrome (SSSS): isolation and purification of toxin and development of a radio-immunobinding
assay for antibodies to exfoliative toxin (ET). In: Staphylococci and Staphylococcal Diseases. Proceedings of the III International Conference on Staphylococci and Staphylococcal Infections.Warszawa. Jeljaszewicz J (Ed.), Gustav Fischer, Struttgart, Germany (1976).
58 Haas Baker D, Wuepper KD, Rasmussen JE. Staphylococcal scalded skin syndrome: detection of antibody to epidermolytic toxin by a primary binding assay. Clin. Exp. Dermatol. 3, 17–24 (1978).
59 Wiley BB, Glasgow LA, Rogolsky M. Staphylococcal scalded-skin syndrome: development of a primary binding assay for human antibody to the exfoliative toxin. Infect. Immun. 13, 513–520 (1976).
60 Shelley ED, Shelley WB, Talanin NY. Chronic staphylococcal scalded skin syndrome. Br. J. Dermatol. 139, 319–324 (1998).
• Case of recurrent staphylococcal scalded skin syndrome.
61 Machang’u RS, Mgode G, Gisakanyi N. Recurrent staphylococcal scalded skin syndrome in children: report of two cases. East Afr. Med. J. 74, 603–604 (1997).
• Two cases of recurrent staphylococcal scalded skin syndrome.
62 Plano LR, Adkins B, Woischnik M, Ewing R, Collins CM. Toxin levels in serum correlate with the development of staphylococcal scalded skin syndrome in a murine model. Infect. Immun. 69, 5193–5197 (2001).
63 Lina G, Gillet Y, Vandenesch F, Jones ME, Floret D, Etienne J. Toxin involvement in staphylococcal scalded skin syndrome. Clin. Infect. Dis. 25, 1369–1373 (1997).
64 Donohue D, Robinson B, Goldberg NS. Staphylococcal scalded skin syndrome in a woman with chronic renal failure exposed to human immunodeficiency virus. Cutis 47, 317–318 (1991).
65 Strumia R, Bedetti A, Cavazzini L. Staphylococcal scalded-skin syndrome in AIDS. G. Ital. Dermatol. Venereol. 125, 461–464 (1990).
66 Farrell AM, Ross JS, Umasankar S, Bunker CB. Staphylococcal scalded skin syndrome in an HIV-1 seropositive man. Br. J. Dermatol. 134, 962–965 (1996).
67 Callahan EF, Adal KA, Tomecki KJ. Cutaneous non-HIV infections. Dermatol. Clin. 18, 497–508 (2000).
68 Richard M, Mathieu-Serra A. Staphylococcal scalded skin syndrome in a homosexual adult. J. Am. Acad. Dermatol. 15, 385–389 (1986).
Patel
586 Expert Rev. Anti-infect. Ther. 2(4), (2004)
69 O’Keefe R, Dagg JH, MacKie RM. The staphylococcal scalded skin syndrome in two elderly immunocompromised patients. Br. Med. J. (Clin. Res. Ed.) 295, 179–180 (1987).
70 Roeb E, Schonfelder T, Matern S et al. Staphylococcal scalded skin syndrome in an immunocompromised adult. Eur. J. Clin. Microbiol. Infect. Dis. 15, 499–503 (1996).
71 Strauss G, Mogensen AM, Rasmussen A, Kirkegaard P. Staphylococcal scalded skin syndrome in a liver transplant patient. Liver Transpl. Surg. 3, 435–436 (1997).
72 Rothenberg R, Renna FS, Drew TM, Feingold DS. Staphylococcal scalded skin syndrome in an adult. Arch. Dermatol. 108, 408–410 (1973).
73 Ridgway HB, Lowe NJ. Staphylococcal scalded skin syndrome in an adult with Hodgkin’s disease. Arch. Dermatol. 115, 589–590 (1979).
74 Goldberg NS, Ahmed T, Robinson B, Ascensao J, Horowitz H. Staphylococcal scalded skin syndrome mimicking acute graft versus host disease in a bone marrow transplant recipient. Arch. Dermatol. 125, 85–87 (1989).
75 Beers B, Wilson B. Adult staphylococcal scalded skin syndrome. Int. J. Dermatol. 29, 428–429 (1990).
76 Neefe LI, Tuazon CU, Cardella TA, Sheagren JN. Staphylococcal scalded skin syndrome in adults: case report and review of the literature. Am. J. Med. Sci. 277, 99–110 (1979).
77 Diem E, Konrad K, Graninger W. Staphylococcal scalded skin syndrome in an adult with fatal disseminated staphylococcal sepsis. Acta. Derm. Venereol. 62, 295–299 (1982).
78 Fritsch P, Elias P, Varga J. The fate of staphylococcal exfoliatin in newborn and adult mice. Br. J. Dermatol. 95, 275–284 (1976).
•• Key study outlining the relationship between age, renal function and staphylococcal scalded skin syndrome.
79 Petzelbauer P, Konrad K, Wolff K. Staphylococcal scalded skin syndrome in two adults with acute kidney failure. Hautarzt. 40, 90–93 (1989).
80 Borchers SL, Gomez EC, Isseroff RR. Generalized staphylococcal scalded skin syndrome in an anephric boy undergoing hemodialysis. Arch. Dermatol. 120, 912–918 (1984).
81 Herzog JL, Sexton FM. Desquamative rash in an immunocompromised adult. Staphylococcal scalded skin syndrome (SSSS). Arch Dermatol. 126, 815–819 (1990).
82 Saiag P, Caumes E, Roujeau JC, Wechsler J, Touraine R. Staphylococcal scalded skin syndrome (staphylococcal Lyell’s syndrome) in adults: two cases. Ann. Dermatol. Venereol. 115, 1164–1166 (1988).
83 Suzuki R, Iwasaki S, Ito Y et al. Adult staphylococcus scalded skin syndrome in a peritoneal dialysis patient. Clin. Exp. Nephrol 7, 77–80 (2003).
84 Sharkey MP, Muir JB. Staphylococcal scalded skin syndrome complicating acute generalized pustular psoriasis. Australas. J. Dermatol. 43, 199–201 (2002).
85 Kirmani N, Tauzon CU, Murray HW et al. Staphylococcus aureus carriage rate of patients receiving long-term hemodialyisis. Arch. Intern. Med. 138, 467–475 (1978).
86 Khuong MA, Chosidow O, el Solh N et al. Staphylococcal scaled skin syndrome in an adult: possible influence of nonsteroidal anti-inflammatory drugs. Dermatology 186, 153–154 (1993).
• First report of the importance of nonsteroidal anti-inflammatory drugs in staphylococcal scalded skin syndrome.
87 Hardwick N, Parry CM, Sharpe GR. Staphylococcal scalded skin syndrome in an adult. Influence of immune and renal factors. Br. J. Dermatol. 132, 468–471 (1995).
88 Stevens DL. Could nonsteroidal anti-inflammatory drugs (NSAIDs) enhance the progression of bacterial infections to toxic shock syndrome? Clin. Infect. Dis. 21, 977–980 (1995).
89 Wiley BB, Allman S, Rogolsky M, Norden CW, Glasgow LA. Staphylococcal scalded skin syndrome: potentiation by immunosuppression in mice; toxin-mediated exfoliation in a healthy adult. Infect. Immun. 9, 636–640 (1974).
90 Rudolph RL, Schwartz W, Leyden JJ. Treatment of staphylococcal toxic epidermal necrolysis. Arch. Dermatol. 111, 1135–1139 (1974).
91 Greenwood JE, Dunn KW, Davenport PJ. Experience with severe extensive blistering skin disease in a pediatric burns unit. Burns 26, 82–87 (2000).
• Role of burns units in the management of staphylococcal scalded skin syndrome.
92 Curran JP, Al-Salihi FL. Neonatal staphylococcal scalded skin syndrome: massive outbreak due to an unusual phage type. Pediatrics 66, 285–290 (1980).
• Report of an outbreak of staphylococcal scalded skin syndrome.
93 Dave J, Reith S, Nash JQ, Marples RR, Dulake C. A double outbreak of exfoliative toxin-producing strains of Staphylococcus aureus in a maternity unit. Epidemiol. Infect. 112, 103–114 (1994).
94 Mackenzie A, Johnson W, Heyes B et al. A prolonged outbreak of exfoliative toxin A-producing Staphylococcus aureus in a newborn nursery. Diagn. Microbiol. Infect. Dis. 21, 69–75 (1995).
95 Kawabata A, Ichiyama S, Iinuma Y, Hasegawa Y, Ohta M, Shimokata K. Exfoliative toxin detection using reversed passive latex agglutination: clinical and epidemiologic applications. J. Clin. Microbiol. 35, 1984–1987 (1997).
96 de Azavedo JCS, Arbuthnott JP. Assays for epidermolytic toxin of Staphylococcus aureus. Meth. Enzymol 165, 333–338 (1988).
97 Murono K, Fujita K, Yoshioka H. Detection of staphylococcal exfoliative toxin by slide latex agglutination. J. Clin. Microbiol. 26, 271–274 (1988).
98 Rifai S, Barbancon V, Prevost G et al. Synthetic exfoliative toxin A and B DNA probes for detection of toxigenic Staphylococcus aureus strains. J. Clin. Microbiol. 27, 504–506 (1989).
99 Arbuthnott JP. Characterisation of the epidermolytic toxins of Staphylococcus aureus. In: The Staphylococci: proceedings of the Alexander Ogston Centennial Conference. Macdonald A, Smith G (Eds), Aberdeen University Press, Aberdeen, UK (1981).
100 Hoeger PH, Elsner P. Staphylococcal scalded skin syndrome: transmission of exfoliatin-producing Staphylococcus aureus by an asymptomatic carrier. Pediatr. Infect. Dis. J. 7, 340–342 (1988).
101 Kaplan MH, Chmel H, Hsieh HC, Stephens A, Brinsko V. Importance of exfoliative toxin A producing Staphylococcus aureus strains isolated from clustered epidemics of neonatal pustulosis. J. Clin. Microbiol. 23, 83–91 (1986).
102 Adesiyun AA, Lenz W, Schaal KP. Exfoliative toxin-production by Staphylococcus aureus strains isolated from animals and human beings in Nigeria. Microbiologica 14, 357–362 (1991).
103 Loughead JL. Congenital staphylococcal scaled skin syndrome: report of a case. Pediatr. Infect. Dis. J. 11, 413–414 (1992).
104 Raymond J, Bingen E, Brahimi N et al. Staphylococcal scalded skin syndrome in a neonate. Eur. J. Clin. Microbiol. Infect. Dis. 16, 453–454 (1997).
Staphylococcal scalded skin syndrome
www.future-drugs.com 587
105 Murono K, Fujita K, Yoshioka H. Microbiologic characteristics of exfoliative toxin-producing Staphylococcus aureus. Pediatr. Infect. Dis. J. 7, 313–315 (1988).
106 Bell FG, Fenton PA. Early hospital discharge and cross-infection. Lancet 342, 120 (1993).
107 Gemmell CG. Staphylococcal scalded skin syndrome. J. Med. Microbiol. 43, 318–327 (1995).
108 Parker MT. Some cultural characteristics of Staphylococcus aureus strains from superficial skin infections. J. Hyg. (London) 56, 238–253 (1958).
109 Dajani AS. The scalded skin syndrome: relation to phage group II staphylococci.J. Infect. Dis. 125, 548 (1972).
110 Kondo I, Sakurai S, Sarai Y. New type of exfoliatin obtained from staphylococcal strains belonging to phage groups other than group II, isolated from patients with impetigo and Ritter’s disease. Infect. Immun. 10, 851–861 (1974).
111 Acland KM, Darvay A, Griffin C, Aali SA, Russell-Jones R. Staphylococcal scalded skin syndrome in an adult associated with methicillin-resistant Staphylococcus aureus. Br. J. Dermatol. 140, 518–520 (1999).
• Rare occurrence of staphylococcal scalded skin syndrome with methicillin resistant Staphylococcal aureus.
112 Yokota S, Imagawa T, Katakura S, Mitsuda T, Arai K. Staphylococcal scalded skin syndrome caused by exfoliative toxin B-producing methicillin-resistant Staphylococcus aureus. Eur. J. Pediatr. 155, 722 (1996).
113 Oono T, Kanzaki H, Yoshioka T, Arata J. Staphylococcal scalded skin syndrome in an adult. Identification of exfoliative toxin A and B genes by polymerase chain reaction. Dermatology 195, 268–270 (1997).
114 Sato H, Tanabe T, Kuramoto M et al. Isolation of exfolitive toxin from Staphylococcus hyicus subspecies hyicus and its exfoliative activity in piglet. Vet Microbiol. 27, 263–275 (1991).
115 Sato H, Matsumori Y, Tanabe T et al. A new type of staphylococcal exfolitative toxin isolated from a Staphylococcus aureus strain isolated from a horse with phlegmon. Infect. Immun. 62, 3780–3785 (1994).
116 Yamaguchi T, Nishifuji K, Sasaki M et al. Identification of the Staphylococcus aureus ETD pathogenicity island that encodes a novel exfoliative toxin, ETD and EDIN-B. Infect. Immun. 70, 5835–5845 (2002).
117 Prevost G, Couppie P, Monteil H. Staphylococcal epidermolysins. Curr. Opin. Infect. Dis. 16, 71–76 (2003).
118 Bailey CJ, de Azavedo J, Arbuthnott JP. A comparitive study of two serotypes of epidermolytic toxin from Staphylococcus aureus. Biochem. Biophys. Acta 624, 111–120 (1980).
119 Sakurai S, Suzuki H, Kondo I. DNA sequencing of the eta gene encoding for staphylococcal exfoliative toxin serotype A. J. Get. Microbiol. 134, 711–717 (1988).
120 Lee CY, Schmidt JJ, Johnson-Winegar AD et al. Sequence determination and comparison of exfoliative toxin A and B genes from Staphylococcus aureus.J. Bacteriol. 169, 3904–3909 (1987).
121 O’Toole PW, Foster TJ. Nucleotide sequence of the epidermolytic toxin A gene of Staphylococcus aureus. J. Bacteriol. 169, 3910–3915 (1987).
122 Sakurai S, Suzuki H, Kondo I. Cloning of the gene coding for staphylococcal exfoliative toxin A and its expression in Escherichia coli. FEMS Microbiol. Lett. 42, 63–67 (1987).
123 Sakurai S, Suzuki H, Machida K. Rapid identification by polymerase chain reaction of staphylococcal exfoliative toxin serotype A and B genes. Microbiol. Immunol. 39, 379–386 (1995).
124 Lillibridge CB, Melish ME, Glasgow LA. Site of action of exfoliative toxin in the staphylococcal scalded skin syndrome. Pediatrics 50, 728–738 (1972).
125 Mahoney MG, Wang Z, Rothenberger K et al. Explanation for the clinical and microscopic localisation of lesions in pemphigus foliaceus and vulgaris. J. Clin. Invest. 103, 461–468 (1999).
126 Amagai M, Yamaguchi T, Hanakawa Y, Nishifuji K, Sugai M, Stanley JR. Staphylococcal exfoliative toxin B specifically cleaves desmoglein-1. J. Invest. Dermatol. 118, 845–850 (2002).
127 Prevost G, Rifai S, Chaix ML, Piemont Y. Functional evidence that the Ser-195 residue of staphylococcal exfoliative toxin A is essential for biological activity. Infect. Immun. 59, 3337–3339 (1991).
128 Barbosa JA, Saldanha JW, Garratt RC. Novel features of serine protease active sites and specificity pockets: sequence analysis and modelling studies of glutamate-specific endopeptidases and epidermolytic toxins. Protein Engl. 9, 591–601 (1996).
129 Vath GM, Earhart CA, Monie DD, Iandolo JJ, Schlievert PM, Ohlendorf DH. The crystal structure of exfoliative toxin B: a superantigen with enzymatic activity. Biochemistry 38, 10239–10246 (1999).
130 Smith TP, Bailey CJ. Activity requirements of epidermolytic toxin from Staphylococcus aureus studied by an in vitro assay. Toxicon 28, 675–683 (1990).
• Demonstrates that the activity of the epidermolytic toxin is calcium dependent.
131 Nagar B, Overduin M, Ikura M, Rini JM. Structural basis of calcium-induced E-cadherin rigidification and dimerization. Nature 380, 360–364 (1996).
132 Machida K. Immunological investigations on pathogenesis of staphylococcal scalded skin syndrome. Rinsho Byori 43, 547–556 (1995).
133 Wu H, Wang ZH, Yan A et al. Protection against pemphigus foliaceus by desmoglein-three in neonates. N. Engl. J. Med. 343, 31–35 (2000).
134 Dancer SJ, Garratt R, Saldanha J, Jhoti H, Evans R. The epidermolytic toxins are serine proteases. FEBS Lett. 268, 129–132 (1990).
•• Key reference showing that the exfoliative toxin has proteolytic properties.
Affiliation• Girish K Patel, PhD
Dermatology Specialist Registrar, Department of Dermatology, University of Wales College of Medicine, Heath Park, Cardiff CF14 4XN, UKTel.: +44 292 074 7747Fax: +44 292 074 [email protected]




![Division of Public Health Services...Syndrome [Treponema pallidum] Tetanus [Clostridium tetani] Toxic-Shock Syndrome (TSS) [streptococcal or staphylococcal] Trichinosis [Trichinella](https://img.pdfslide.us/doc/110x75/600aad0a71e3742d46221fb0/division-of-public-health-services-syndrome-treponema-pallidum-tetanus-clostridium.jpg)