Embed Size (px)
Citation preview
Streptococcal & Staphylococcal Toxic Shock Syndrome (TSS)
David A Wininger, MDInternal Medicine Residency Program Director Associate Professor, Clinical Internal Medicine Division of Infectious DiseasesThe Ohio State University Wexner Medical Center614-293-3989 [email protected]
Learning Objectives
Describe the nature and mechanisms of action of streptococcal and staphylococcal virulence factors as it related to Toxic Shock Syndrome (TSS)
Describe the role of molecular signals and cytokines involved in the pathophysiology of Toxic Shock Syndrome (TSS)
Compare and contrast the epidemiology, clinical manifestations, diagnosis, management and prognosis of streptococcal and staphylococcal Toxic Shock Syndrome (TSS)
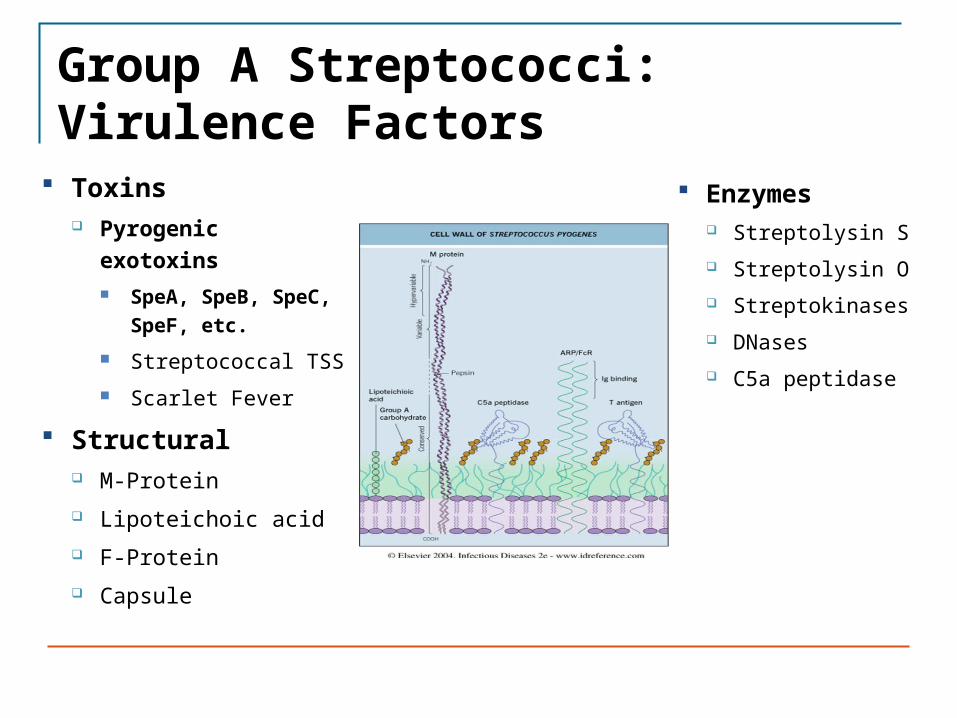
Group A Streptococci: Virulence Factors
Toxins Pyrogenic exotoxins
SpeA, SpeB, SpeC, SpeF, etc.
Streptococcal TSS Scarlet Fever
Structural M-Protein Lipoteichoic acid F-Protein Capsule
Enzymes Streptolysin S Streptolysin O Streptokinases DNases C5a peptidase
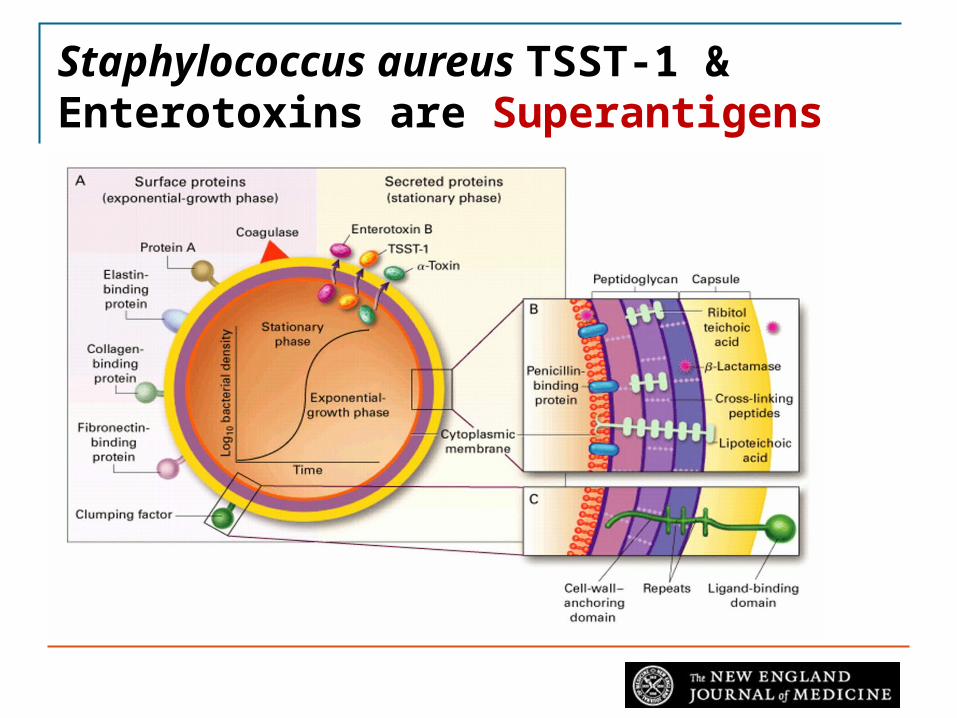
Staphylococcus aureus TSST-1 & Enterotoxins are Superantigens
Or 2 separate slides
Superantigens in Staph and Strep
Staphylococcal
Toxic Shock Syndrome Toxin -1 (TSST-1)
Staphylococcal enterotoxins
At least 15 types
Staphylococcal exotoxins
Homologous to the enterotoxins
Streptococcal
SPE-A, SPE-C (Scarlet Fever- coded by bacteriophage)
SPE-B, SPE-E, SPE-G, etc.
SSA (Streptococcal Superantigen)
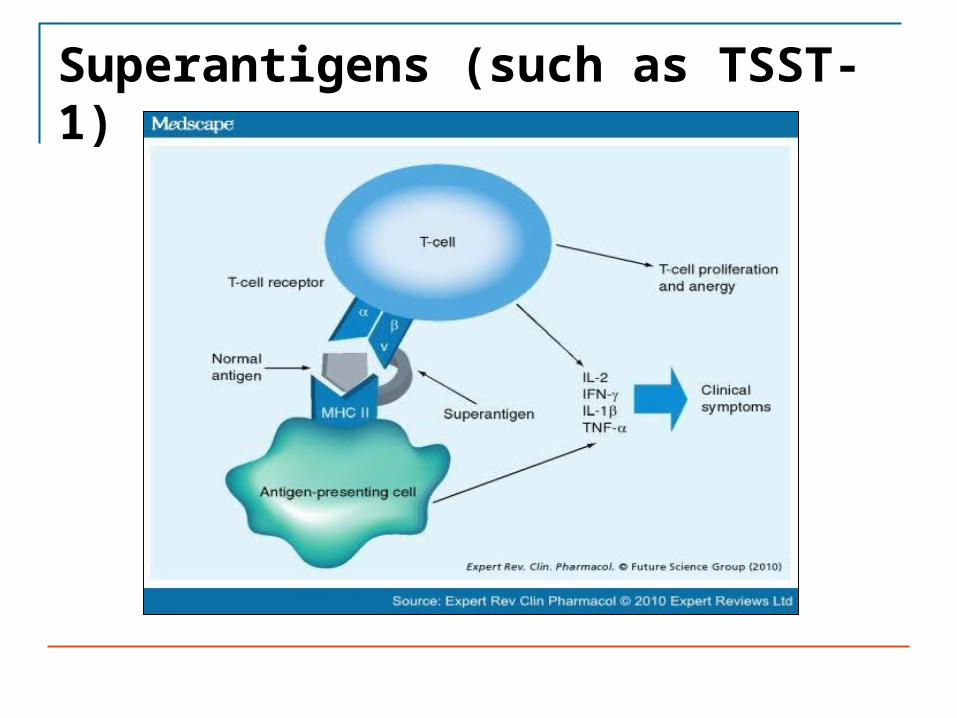
Superantigens (such as TSST-1)
Cytokine Release after Nonspecific Superantigen Stimulation of T-cells
Primarily CD4+ T cell response is triggered by superantigen
T-helper Th1 response IL-2, IFN-γ, IL-1β and TNF-α
Immune Response
Given lack of Th2 response, antibody expression is decreased during response to superantigens
Lack of protective antibody to TSST-1 after first episode leaves ~50% patients vulnerable to recurrence
Toxic Shock Syndrome Epidemiology
Staphylococcus aureus TSST-1 producing strains
Menstruating women Hyper absorbent tampons
Non-menstrual disease results from colonization of any site: Surgical wounds (may not look hot)
Post-influenza lung
Other skin/soft tissue
Contraceptive diaphragms
5% mortality now that condition is routinely recognized
Toxic Shock Syndrome Epidemiology
Streptococcus pyogenes (Group A) M-serotypes 1 or 3
Mucoid strains – prominent capsules
Produce SPE’s
Can occur in patients of any age
Patients at risk: HIV infection, Diabetes mellitus, Cancer, Heart or Lung disease, Chicken-pox/Shingles, Injection drug use, Ethanol abuse
Mortality almost 50%
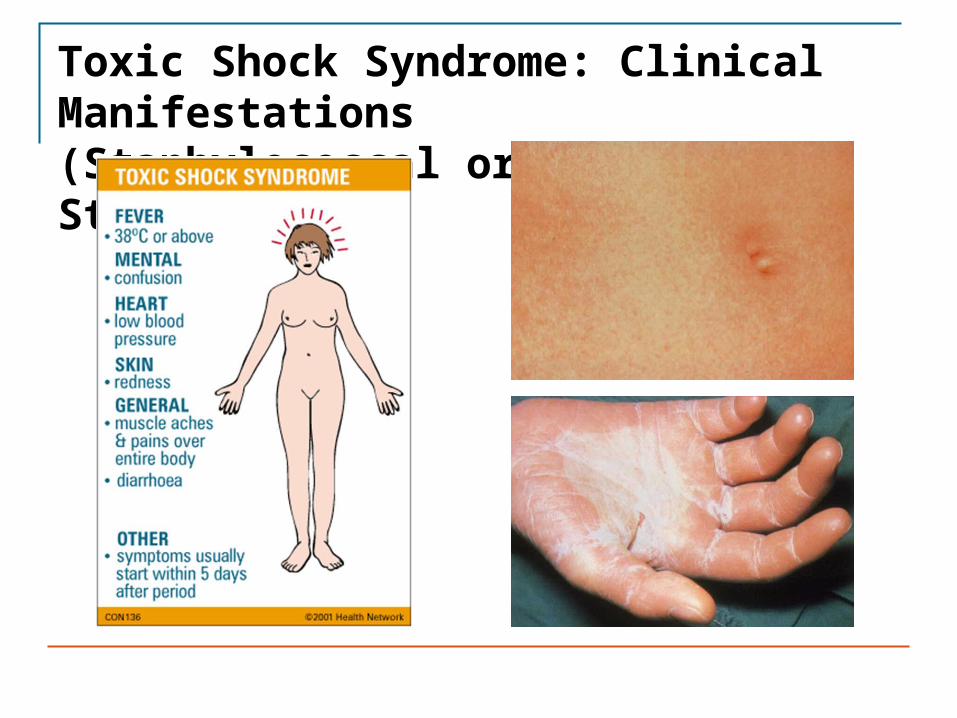
Toxic Shock Syndrome: Clinical Manifestations(Staphylococcal or Streptococcal)
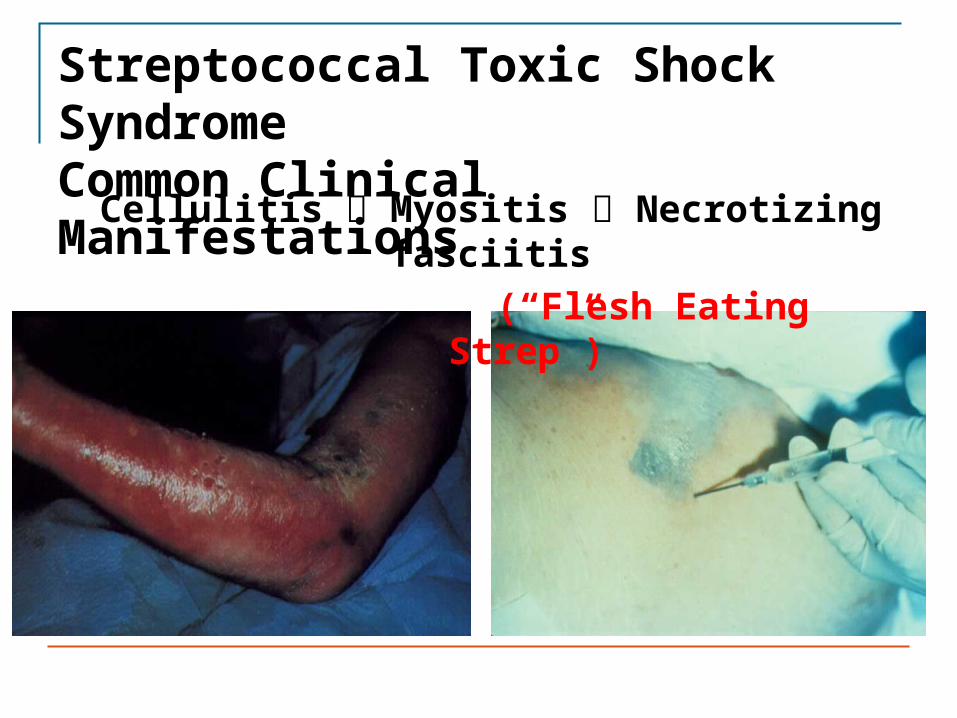
Streptococcal Toxic Shock SyndromeCommon Clinical Manifestations
Cellulitis Myositis Necrotizing fasciitis (“Flesh Eating Strep”)
Toxic Shock Syndrome (TSS): Diagnosis
Staphylococcal TSS
Usually a clinical diagnosis
Diagnostic criteria have been developed
Often lack positive cultures for staph
Staph can be cultured from colonized sites (mucosal surfaces)
Lack of anti-TSST1 antibodies during acute syndrome is expected.
Toxic Shock Syndrome (TSS): Diagnosis
Streptococcal TSS
Cultures from involved sites are usually positive
Positive growth from sterile site (blood, deep tissue) is more definitive than positive culture from non-sterile site like superficial skin
Clinical diagnostic criteria are similar to those for Staph TSS
Toxic Shock Syndrome (TSS): Management
Staphylococcal TSS
Supportive care
IV fluids, other blood pressure support, intensive care as needed (ventilator, renal dialysis, etc.)
Removal of potential focus
Anti-staphylococcal antibiotics even if cultures are negative.
Consider IVIG for more severe cases but usually not necessary
Toxic Shock Syndrome (TSS): Management
Streptococcal TSS
Supportive care as with staph
Aggressive surgical debridement or other removal of infected source (site is usually overt)
Anti-streptococcal antibiotics (penicillin + clindamycin)
Clindamycin blocks protein synthesis (↓ toxin production)
IVIG more likely to be used, since cases are often more severe
Summary
Toxic Shock Syndrome (TSS) is mediated by superantigen toxins produced by Staphylococcus aureus and Group A Streptococcus.
Staphylococcal TSS is more likely to be a culture negative presentation of septic shock, while Streptococcal TSS is likely to manifest with a severe overt localizable infection of soft tissue or another body site.
Both aggressive supportive care and antimicrobial coverage of the causative organism are critical for successful management of TSS.
Intravenous immunoglobulin is a consideration for the management of severe TSS, since one hallmark of the acute condition is absence of antibodies against the superantigen toxin.
Quiz
Thank you for completing this module
If you have any questions, write to me at [email protected] or try my office at 614-293-3989.
David Wininger, MD
References
Medical Microbiology, 7th Ed. Murray, Rosenthal & Pfaller; Chapter 18 & 19, selected pages.
Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, Seventh Edition Chapter 195 and Chapter 198 selected pages (available electronically in Prior Health Sciences Library among the Core 25 Textbooks)
Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey