Embed Size (px)
Citation preview

Treatment of Treatment of MyopathiesMyopathies
Hanni BoumaHanni Bouma

OverviewOverview
Inflammatory myopathiesInflammatory myopathies– DermatomyositisDermatomyositis– PolymyositisPolymyositis– Inclusion body myositisInclusion body myositis
Clinical featuresClinical features InvestigationsInvestigations Treatment approachTreatment approach

Etiological Etiological Classification of Classification of MyopathiesMyopathies HereditaryHereditary Muscular DystrophiesMuscular Dystrophies
– Duchenne’s Duchenne’s MyotoniasMyotonias ChannelopathiesChannelopathies Congenital Congenital
MyopathiesMyopathies Metabolic MyopathiesMetabolic Myopathies
– Pompe’s diseasePompe’s disease Mitochondrial Mitochondrial
myopathiesmyopathies
AcquiredAcquired Inflammatory Inflammatory
myopathiesmyopathies– PM, DM, IBMPM, DM, IBM
EndocrineEndocrine– thyroidthyroid
Associated with Associated with other systemic other systemic illnessillness
Drug-induced and Drug-induced and toxic myopathiestoxic myopathies– EtOH, steroids, statinsEtOH, steroids, statins

Overview of the IMOverview of the IM

DM: ClinicalDM: Clinical
Slow, progressive, symmetric limb-girdle Slow, progressive, symmetric limb-girdle weaknessweakness
Activity-induced muscle painActivity-induced muscle pain Rash usually accompanies or precedes Rash usually accompanies or precedes
weakness (but not always)weakness (but not always) Associated features:Associated features:
– Adults: Myocarditis, ILD, vasculitis, other CTDs (RA, Adults: Myocarditis, ILD, vasculitis, other CTDs (RA, Scl, CREST)Scl, CREST)
– Children: Contractures, subQ calcinosis, intestinal Children: Contractures, subQ calcinosis, intestinal ulceration ulceration
Cancers: Cancers: adenocarcinomas, ovarian, breast, adenocarcinomas, ovarian, breast, lung, lymphoma/leukemia lung, lymphoma/leukemia


DM: InvestigationsDM: Investigations
CK normal (20-30%) or increased up to 50x CK normal (20-30%) or increased up to 50x – Does not correlate with severity of weaknessDoes not correlate with severity of weakness– Aldolase may be elevated while CK still normalAldolase may be elevated while CK still normal
ANA+ (24-60%) ANA+ (24-60%) Myositis specific antibodies: Myositis specific antibodies:
– Mi-2 (15%) Mi-2 (15%) acute onset, nailfold ulcers & good response to acute onset, nailfold ulcers & good response to
therapytherapy– Anti-Jo-1 (~20%)Anti-Jo-1 (~20%)
ILD, mechanic’s hands, arthritis, Raynaud’sILD, mechanic’s hands, arthritis, Raynaud’s EMGEMG Muscle biopsyMuscle biopsy

Other Investigations: DMOther Investigations: DM
Increased risk of Ca. within first 2-3 yrs of Increased risk of Ca. within first 2-3 yrs of diagnosisdiagnosis– Treatment of malignancy sometimes Treatment of malignancy sometimes
improves muscle strengthimproves muscle strength– Malignancy workup in all patients: Malignancy workup in all patients:
CT CAPCT CAP MammogramMammogram Breast & pelvic examsBreast & pelvic exams ColonoscopyColonoscopy
CXR, High res CT chest (ILD)CXR, High res CT chest (ILD) EKG (myocardial inv’t) or Echo if CHFEKG (myocardial inv’t) or Echo if CHF Swallowing assessment if dysphagiaSwallowing assessment if dysphagia

PolymyositisPolymyositis
““Diagnosis of exclusion” Diagnosis of exclusion” – Often mistaken diagnosis of PM in Often mistaken diagnosis of PM in
cases of DM w/o rash (yet), IBM w/o cases of DM w/o rash (yet), IBM w/o inclusions on biopsyinclusions on biopsy
Prox symmetric weaknessProx symmetric weakness Associated with other autoimmune Associated with other autoimmune
disordersdisorders Myocarditis, arthritis, Raynaud’s, ILDMyocarditis, arthritis, Raynaud’s, ILD

IBMIBM Most common myopathy Most common myopathy
over 50 yoover 50 yo Insidious onset; Dx. Insidious onset; Dx.
usually several yrs after usually several yrs after onsetonset
Early dysphagiaEarly dysphagia Different pattern of Different pattern of
weakness: weakness: – Distal UE, Prox LEDistal UE, Prox LE– Early atrophy & Early atrophy &
weakness of WF, FF & weakness of WF, FF & quadsquads
– Hip girdle, ant. tibial Hip girdle, ant. tibial musclesmuscles

Diagnosis?Diagnosis?

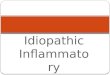
PMPM
Endomysial mononuclear inflammatory cell infiltrate invading and surrounding non-necrotic muscle fibres
Mediated by CD8+ T-cells which attack Mediated by CD8+ T-cells which attack muscle fibresmuscle fibres


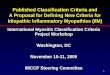
DMDM Humorally-mediated Humorally-mediated
microangiopathymicroangiopathy
1) Perifascicular necrosis/atrophy (late finding)2) Perivascular & perimysial inflammation: macrophages, B cells, CD4+ cells

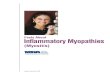
IBMIBM
Similar to PM: CD8+ T cells & macrophagesSimilar to PM: CD8+ T cells & macrophages
Same features as PM + rimmed vacuoles + amyloid depositsModified Gomori trichrome stain

Is it possible to have IBM without Is it possible to have IBM without inclusions on biopsy?inclusions on biopsy?
QuestionQuestion

TreatmentTreatment
Overall lack of “EBM” to guide Overall lack of “EBM” to guide treatment; we don’t know:treatment; we don’t know:– Which second lineWhich second line therapies are most therapies are most
beneficialbeneficial– The doses required to see an effectThe doses required to see an effect– The best time to initiate 2The best time to initiate 2ndnd or 3 or 3rdrd line line
agentsagents– If some agents are more effective in If some agents are more effective in
certain types of myositiscertain types of myositis

Treatment: Step 1Treatment: Step 1Initiate corticosteroidsInitiate corticosteroids
Treatment of choice in DM & PM:Treatment of choice in DM & PM:– Majority of patients will improve with Majority of patients will improve with
pred, but response may be pred, but response may be incompleteincomplete
Start prednisone at ~1 mg/kg/day up Start prednisone at ~1 mg/kg/day up to 100 mg qd to 100 mg qd
In severe weakness, treatment often In severe weakness, treatment often initiated w/ short course of IV initiated w/ short course of IV Solumedrol 1 g x 3 days prior to predSolumedrol 1 g x 3 days prior to pred

Treatment: Step 1Treatment: Step 1Post-initiation of steroidsPost-initiation of steroids
Close clinical F/U q2-4 weeks initiallyClose clinical F/U q2-4 weeks initially Maintain dose until muscle strength Maintain dose until muscle strength
normalizes, improvement plateaus, or normalizes, improvement plateaus, or CK normalizes (at least 4-6 wks)CK normalizes (at least 4-6 wks)
Then Then slowslow taper: by taper: by 5 mg q2-3 5 mg q2-3 weeksweeks, below 20 mg by 2.5 q2wks, below 20 mg by 2.5 q2wks
*Most will need to stay on a small dose *Most will need to stay on a small dose of pred (10 mg qd) or need a 2of pred (10 mg qd) or need a 2ndnd line line agent to stay in remissionagent to stay in remission

Step 1: SteroidsStep 1: SteroidsSide effect considerationsSide effect considerations
Monitor fasting glucose, K+ levelsMonitor fasting glucose, K+ levels Septra for PCP prophylaxisSeptra for PCP prophylaxis
– If concurrent ILD or pred + other If concurrent ILD or pred + other immunosuppressantimmunosuppressant
Bone density scan at baseline & qyearlyBone density scan at baseline & qyearly Calcium 1 g/day + Vit D 1000 IU/dayCalcium 1 g/day + Vit D 1000 IU/day Bisphosphonate used if postmenopausalBisphosphonate used if postmenopausal Record BP at each visit (accelerated HTN & Record BP at each visit (accelerated HTN &
renal failure is a risk) renal failure is a risk) – Coexistence of scleroderma & other MCTDsCoexistence of scleroderma & other MCTDs
Periodic eye exams for glaucoma & cataractsPeriodic eye exams for glaucoma & cataracts

QuestionQuestion
What should I do if there is no What should I do if there is no response after an adequate trial response after an adequate trial of high dose prednisone?of high dose prednisone?

QuestionQuestion
How can I tell if the patient is How can I tell if the patient is weaker because of refractory weaker because of refractory disease or because of chronic disease or because of chronic steroid use?steroid use?

Treatment: Step 2Treatment: Step 2Add immunosuppressantAdd immunosuppressant
Indications:Indications:– Moderate or severe weaknessModerate or severe weakness– Other organ system inv’t (ILD, myocarditis)Other organ system inv’t (ILD, myocarditis)– Increased risk of steroid complications Increased risk of steroid complications
(diabetic, OP, postmenopausal women)(diabetic, OP, postmenopausal women)– Failure to significantly improve after 2-4 Failure to significantly improve after 2-4
months of steroidsmonths of steroids– Any pt expected to need steroids for 10-12 Any pt expected to need steroids for 10-12
mos or moremos or more* Must weigh risks of immunosuppression vs. * Must weigh risks of immunosuppression vs.
possible benefits (faster improvement, possible benefits (faster improvement, steroid-sparing)steroid-sparing)

Treatment: Step 2Treatment: Step 2ImmunosuppressionImmunosuppression
Options:Options:– Azathioprine Azathioprine – MethotrexateMethotrexate– IVIG IVIG – CellceptCellcept– CyclophosphamidCyclophosphamid
ee
Generally used Generally used as 3as 3rdrd line, if line, if refractory to refractory to other Rx.:other Rx.:– Rituximab Rituximab – PLEX PLEX – CiclosporineCiclosporine– TacrolimusTacrolimus

AzathioprineAzathioprine
Effective in DM/PM (retrospective Effective in DM/PM (retrospective studies), but takes 6-18 mos to studies), but takes 6-18 mos to workwork
Prior to starting, can screen for Prior to starting, can screen for TPMT deficiency (BM toxicity in TPMT deficiency (BM toxicity in homozygotes) or just monitor CBChomozygotes) or just monitor CBC
Begin at 50 mg/d, increase by 50 Begin at 50 mg/d, increase by 50 mg q2wks up to 2-3 mg/kg/dmg q2wks up to 2-3 mg/kg/d

AzathioprineAzathioprineMonitoring & SEsMonitoring & SEs
Major SEs:Major SEs: 12% develop systemic rxn (fever, 12% develop systemic rxn (fever, abdo pain, N/V) w/i first few wks requiring abdo pain, N/V) w/i first few wks requiring discontinuation of drug; BM & liver toxicity discontinuation of drug; BM & liver toxicity (avoid allopurinol), pancreatitis, (avoid allopurinol), pancreatitis, teratogenicity, oncogenicity, infectionteratogenicity, oncogenicity, infection
Monitor CBC, LFTs closely; D/C if LFTs double Monitor CBC, LFTs closely; D/C if LFTs double (esp. GGT)(esp. GGT)
Leukopenia:Leukopenia: can develop at 1 wk to as late as can develop at 1 wk to as late as 2 yrs post-initiation; decrease dose if WBCs 2 yrs post-initiation; decrease dose if WBCs fall to <4, D/C altogether if <2.5 or ANC <1; fall to <4, D/C altogether if <2.5 or ANC <1; usually reverses w/i 1 mo., can then usually reverses w/i 1 mo., can then rechallengerechallenge

MethotrexateMethotrexate
Most DM & PM respond to MTX Most DM & PM respond to MTX (retrospective studies only)(retrospective studies only)
Begin at 7.5 mg/wk po, increase Begin at 7.5 mg/wk po, increase gradually by 2.5 mg each week gradually by 2.5 mg each week up to 25 mg/wkup to 25 mg/wk
If no improvement after 1 month If no improvement after 1 month on 25 mg, switch to weekly subQ on 25 mg, switch to weekly subQ & increase dose by 5 mg qwk up & increase dose by 5 mg qwk up to 60 mg/wkto 60 mg/wk

MethotrexateMethotrexateMonitoring & SEsMonitoring & SEs
Major SEs:Major SEs: alopecia, stomatitis, alopecia, stomatitis, pulmonary pulmonary fibrosis, fibrosis, teratogenicity, oncogenicity, teratogenicity, oncogenicity, infection; renal, liver & BM toxicityinfection; renal, liver & BM toxicity
Avoid MTX in pts with ILD or anti-Jo-1+Avoid MTX in pts with ILD or anti-Jo-1+ Avoid MTX in heavy drinkersAvoid MTX in heavy drinkers Treat all pts with folate 5 mg qwkTreat all pts with folate 5 mg qwk Monitor LFTs, CBC q2wks until on stable Monitor LFTs, CBC q2wks until on stable
dose, then q1-3 mosdose, then q1-3 mos Check GGT because AST/ALT can be Check GGT because AST/ALT can be
elevated from muscle inv’t; consider liver elevated from muscle inv’t; consider liver Bx. if cumulative dose exceeds 2 gBx. if cumulative dose exceeds 2 g
Monitor PFTs periodicallyMonitor PFTs periodically

IVIGIVIG
One prospective, double-blind, One prospective, double-blind, placebo-controlled study in 15 pts placebo-controlled study in 15 pts w/ DM showed significant w/ DM showed significant improvementimprovement
Little RCTLittle RCT evidence of benefit as evidence of benefit as monotherapy but plenty of monotherapy but plenty of anecdotal evidence that IVIG is anecdotal evidence that IVIG is effective, even aloneeffective, even alone

IVIGIVIG
2 g/kg over 2-5 days, repeated at 2 g/kg over 2-5 days, repeated at monthly intervals for at least 3 mosmonthly intervals for at least 3 mos
Then decrease or spread out dose Then decrease or spread out dose ((40 g q2wks40 g q2wks))
SEs:SEs:– Renal failure (esp. diabetics), flu-like Renal failure (esp. diabetics), flu-like
Sx., rash, aseptic meningitis, MI, Sx., rash, aseptic meningitis, MI, stroke, CHFstroke, CHF

CyclophosphamideCyclophosphamide
Used often if ILDUsed often if ILD SEs: infections, secondary SEs: infections, secondary
malignancies, hemorrhagic malignancies, hemorrhagic cystitis, sterilization, BM toxicity, cystitis, sterilization, BM toxicity, GI upset, alopeciaGI upset, alopecia– Usually given pulsed (0.5-1 g/ Usually given pulsed (0.5-1 g/
IV/m2/mo. for 6-12 mos), higher risk IV/m2/mo. for 6-12 mos), higher risk of cystitis poof cystitis po

Mycophenolate mofetilMycophenolate mofetil
Blocks purine synthesis in lymphsBlocks purine synthesis in lymphs Actual benefit unknownActual benefit unknown Main advantage: Main advantage: lack of renal or liver lack of renal or liver
toxicitytoxicity Starting dose 1.0 g bid, increased to Starting dose 1.0 g bid, increased to
1.5 bid if needed1.5 bid if needed Limit 1 g/d if renal insufficiencyLimit 1 g/d if renal insufficiency Side effects: N/V, diarrhea, fever, Side effects: N/V, diarrhea, fever,
leukopenia, severe infections possibleleukopenia, severe infections possible

Treatment: Step 3Treatment: Step 3If refractory to other modalities…If refractory to other modalities…
RituximabRituximab -> monoclonal Ab -> monoclonal Ab against CD20, depletes B cellsagainst CD20, depletes B cells– Dose 750 mg/m2 (up to 1 g) x 1, Dose 750 mg/m2 (up to 1 g) x 1,
repeat in 2 wks & then q6-9mosrepeat in 2 wks & then q6-9mos– Warnings re: PML risk…Warnings re: PML risk…

Treatment: Step 3Treatment: Step 3If refractory to other If refractory to other
modalities…modalities… Ciclosporine & tacrolimusCiclosporine & tacrolimus -> renal -> renal
toxicity, HTN, electrolyte imbalance, toxicity, HTN, electrolyte imbalance, GI upset, hypertrichosis, gingival GI upset, hypertrichosis, gingival hyperplasia, cancers, tremor, hyperplasia, cancers, tremor, infectioninfection
PLEXPLEX -> few small open label series -> few small open label series suggested benefit in DM, PM & IBMsuggested benefit in DM, PM & IBM– Controlled trial of 36 pts w/ DM & PM Controlled trial of 36 pts w/ DM & PM
comparing PLEX, leukopheresis & sham comparing PLEX, leukopheresis & sham apheresis showed no improvementapheresis showed no improvement

SISide Effects & Side Effects & MonitoringMonitoring

Non-medical therapiesNon-medical therapies
PT & OTPT & OT Dietician consult if on steroidsDietician consult if on steroids Aerobic exercise programsAerobic exercise programs
– Prevents contracturesPrevents contractures– May help w/ steroid SEs (weight May help w/ steroid SEs (weight
gain, OP, type 2 fibre atrophy)gain, OP, type 2 fibre atrophy) Speech therapySpeech therapy
– Esp if concomitant dysphagiaEsp if concomitant dysphagia

QuestionQuestion
What is the value of monitoring What is the value of monitoring serum CK levels in the treatment serum CK levels in the treatment of DM & PM?of DM & PM?

QuestionQuestion
How does the treatment of IBM How does the treatment of IBM differ from that of PM & DM?differ from that of PM & DM?

IBMIBM
Glucocorticoids have limited roleGlucocorticoids have limited role– In largest published series, muscle strength In largest published series, muscle strength
continued to deteriorate in all of 25 pred-continued to deteriorate in all of 25 pred-treated patients followed for at least 2 yrstreated patients followed for at least 2 yrs
– CK levels often normalize, but this doesn’t CK levels often normalize, but this doesn’t correlate with clinical benefitcorrelate with clinical benefit
– Exception:Exception: Cases of IBM ass’d w/ other CTDs Cases of IBM ass’d w/ other CTDs (Sjogren’s, SLE, cutaneous DM) may have (Sjogren’s, SLE, cutaneous DM) may have clinically important benefit from steroidsclinically important benefit from steroids
MTX, Imuran: minor benefit at bestMTX, Imuran: minor benefit at best

IBM: suggested IBM: suggested approachapproach If ++inflammation seen on Bx., If ++inflammation seen on Bx.,
consider trial of steroids +/- consider trial of steroids +/- Imuran (3 mos) early in diseaseImuran (3 mos) early in disease
Discontinue all therapy if Discontinue all therapy if continued decline in strengthcontinued decline in strength
For most patients, no treatmentFor most patients, no treatment Cricopharyngeal myotomy may Cricopharyngeal myotomy may
be helpful if severe dysphagiabe helpful if severe dysphagia

ReferencesReferences
Dr. Erin O’Ferrall!Dr. Erin O’Ferrall! Amato & Barohn. Evaluation and Amato & Barohn. Evaluation and
treatment of inflammatory treatment of inflammatory myopathies. myopathies. Journal of Neurology, Journal of Neurology, Neurosurgery & Psychiatry. Neurosurgery & Psychiatry. 2009; 2009; 80: 1060-1068.80: 1060-1068.
UptoDateUptoDate

Lambert-Eaton Lambert-Eaton Myasthenic Myasthenic SyndromeSyndrome
Hanni BoumaHanni Bouma

SymptomsSymptoms
Slowly progressive proximal muscle Slowly progressive proximal muscle weakness (legs>>arms)weakness (legs>>arms)
Muscle fatigability or cramping after exerciseMuscle fatigability or cramping after exercise Autonomic dysfunction: Autonomic dysfunction:
– Dry mouth**Dry mouth**– EDED– Blurred vision, constipationBlurred vision, constipation
CN dysfunction (less prominent than in MG & CN dysfunction (less prominent than in MG & rarely the presenting symptom) rarely the presenting symptom) – Ptosis most commonPtosis most common– Diplopia, dysarthria, dysphagia, difficulty chewingDiplopia, dysarthria, dysphagia, difficulty chewing
Respiratory failure late in courseRespiratory failure late in course

SignsSigns Proximal muscle weakness without Proximal muscle weakness without
atrophyatrophy– Functional difficulties often worse than Functional difficulties often worse than
exam findingsexam findings Depressed or absent reflexesDepressed or absent reflexes
– Isometric contraction of relevant muscle Isometric contraction of relevant muscle can temporarily bring out reflexes or can temporarily bring out reflexes or improve muscle weakness improve muscle weakness ((postactivation postactivation facilitation)facilitation)
– More sustained physical exercise More sustained physical exercise muscle fatigabilitymuscle fatigability
Paradoxical eyelid elevation with Paradoxical eyelid elevation with sustained upgazesustained upgaze
Symmetric, sluggish pupillary Symmetric, sluggish pupillary responsesresponses
Reduced salivationReduced salivation

PathophysiologyPathophysiology
VGCC VGCC antibodies:antibodies: interfere interfere with normal with normal calcium calcium influx influx required for required for Ach release Ach release reduced reduced Ach release Ach release from from presynaptic presynaptic nerve nerve terminalsterminals

EpidemiologyEpidemiology
Annual incidence & prevalence 0.48 & Annual incidence & prevalence 0.48 & 2.32 per million2.32 per million
½ ½ of cases associated w/ malignancyof cases associated w/ malignancy– Usually starts after age 50Usually starts after age 50– SCLC most commonly (84%), Hodgkin’s SCLC most commonly (84%), Hodgkin’s
lymphomalymphoma– Presence of LEMS implies better prognosis Presence of LEMS implies better prognosis
in SCLC ptsin SCLC pts In non-paraneoplastic forms, younger In non-paraneoplastic forms, younger
age of onsetage of onset


TreatmentTreatment
1) 1) Treatment of underlying malignancyTreatment of underlying malignancy– causes remission of LEMS in many but not causes remission of LEMS in many but not
all paraneoplastic forms; may be only all paraneoplastic forms; may be only intervention necessary intervention necessary
2) 2) Symptomatic therapiesSymptomatic therapies – increase amt. of Ach available at increase amt. of Ach available at
postsynaptic membranepostsynaptic membrane 3) 3) Immunologic therapiesImmunologic therapies
– reduce aberrant immune response causing reduce aberrant immune response causing formation of VGCC antibodiesformation of VGCC antibodies
– Regimens similar to those used in MGRegimens similar to those used in MG

AminopyridineAminopyridiness
MoA: significant prolongation of nerve MoA: significant prolongation of nerve terminal membrane depolarization terminal membrane depolarization calcium channels kept open longer, calcium channels kept open longer, which improves release of Achwhich improves release of Ach
3,4-Diaminopyridine:3,4-Diaminopyridine: limited CNS limited CNS penetration, few SEs (perioral & penetration, few SEs (perioral & extremity paresthesias, extremity paresthesias, seizuresseizures at at higher doses)higher doses)

GuanidineGuanidine
MoA: inhibits VGKC & enhances release MoA: inhibits VGKC & enhances release of Achof Ach
First beneficial agent for symptomatic First beneficial agent for symptomatic treatment of LEMStreatment of LEMS
Significant bone marrow, liver & renal Significant bone marrow, liver & renal toxicity at higher dosestoxicity at higher doses
Max dose 1000 mg/d.Max dose 1000 mg/d.

AChEIAChEI
MoA: reduce metabolism of Ach, MoA: reduce metabolism of Ach, thereby increasing amt. available thereby increasing amt. available for AchR bindingfor AchR binding
Pyridostigmine:Pyridostigmine: best-tolerated best-tolerated Only marginally effective used in Only marginally effective used in
isolationisolation

ImmunologicImmunologic therapiestherapies
Indications:Indications:– Significant weaknessSignificant weakness– Limited response to symptomatic Rx.Limited response to symptomatic Rx.
Options: the usual suspects…Options: the usual suspects…– IVIGIVIG– SteroidsSteroids– Azathioprine, myocophenolate, Azathioprine, myocophenolate,
cyclophoscyclophos– PLEX, RituximabPLEX, Rituximab

Treatment ApproachTreatment Approach
If mild persistent weakness, with If mild persistent weakness, with or without malignancyor without malignancy– Trial of pyridostigmine 30-120 mg Trial of pyridostigmine 30-120 mg
q3-6hrsq3-6hrs– If response inadequate, 3,4-DAP can If response inadequate, 3,4-DAP can
be added (10-25 mg tid to qid)be added (10-25 mg tid to qid)– OR add low-dose guanidine (5-10 OR add low-dose guanidine (5-10
mg/kg/d given in 3-4 divided doses)mg/kg/d given in 3-4 divided doses) Not used much anymoreNot used much anymore

ApproachApproach
If significant weakness refractory to If significant weakness refractory to symptomatic therapies, with treated symptomatic therapies, with treated malignancy or without malignancymalignancy or without malignancy
Two options:Two options:1) 1) Course of IVIG (2 g/kg over 2-5 days) Course of IVIG (2 g/kg over 2-5 days) – Temporary improvement (4-8 weeks)Temporary improvement (4-8 weeks)– Requires maintenance w/ repeat infusions Requires maintenance w/ repeat infusions
at 4-12 week intervals at 4-12 week intervals – used if good response to initial IVIG courseused if good response to initial IVIG course

ApproachApproach
2) 2) Prednisone (1 mg/kg/day) and Prednisone (1 mg/kg/day) and azathioprine (starting at 50 mg azathioprine (starting at 50 mg bid, increasing by 50 mg qweek up bid, increasing by 50 mg qweek up to 2-3 mg/kg/d)to 2-3 mg/kg/d)– May take several months for clinically May take several months for clinically
significant improvement (remission)significant improvement (remission)– Then attempt to taper or discontinue Then attempt to taper or discontinue
prednisoneprednisone

ApproachApproach
PLEX not as effective for LEMS as PLEX not as effective for LEMS as MGMG
Slower response, short-term Slower response, short-term benefitbenefit
Can be used if IVIG intolerance or Can be used if IVIG intolerance or refractory disease with severe refractory disease with severe clinical courseclinical course