Embed Size (px)
Citation preview

Treatment of Treatment of Mild to moderate Mild to moderate
Extensive Extensive Ulcerative ColitisUlcerative Colitis
Philippe Marteau, Paris, FrancePhilippe Marteau, Paris, France

Mild to moderate Extensive UCMild to moderate Extensive UC
Oral ASA are needed as local treatments cannot cover all lesions
Recommendation : 1st line : oral 5-ASA 4 g/dObtaining endoscopic remission or frank improvement
usually takes more than 4 weeks
2nd line : if severe or resistant : consider oral steroids
Marteau P et al. Gastroenterol Clin Biol. 2004 Oct;28(10 Pt 2):955-60.

UC Consensus 2006UC Consensus 2006Treatment of Active DiseaseTreatment of Active Disease
Simon Travis, Eduard Stange, Simon Travis, Eduard Stange, Yehuda Chowers, Philippe Yehuda Chowers, Philippe MarteauMarteau

Active disease Active disease ECCO Statement: Extensive colitisECCO Statement: Extensive colitis
● Extensive ulcerative colitis of mild-moderate severity should initially be treated with mesalazine >2g/day [EL1a, RG A], combined with topical mesalazine[EL1b, RG A]
● Oral aminosalicylates alone induce remission only in a minority of patients [EL1a, RG A]….

Optimise the first line treatment of extensive UC ?
– Many symptoms originate form the distal colon
(blood in stools, tenesmus…)
– Is association of local and oral salicylates better than
oral treatment alone ?

PatientsPatients
● 116 patients
● Mild to moderate exacerbation of extensive UC (UCDAI ≥3 and ≤8)
● Exclusion criteria: ● maintenance treatt with aminosalicylates > 3 g/d● corticosteroids● immunosuppressive agents
Marteau et al. Gut 2005;54:960-5

MethodsMethods
● Double-blind, parallel-group, placebo-controlled RCT
● For 8 weeks, each patient received 4 g/d pentasa orally
● During the initial 4 weeks, each patient additionally applied daily a 100 mL enema at bedtime, either containing 1 g Pentasa or placebo
● Evaluation ● at inclusion, 4 weeks and 8 weeks ● UCDAI score (clinical signs and endoscopic evaluation of
the distal colon)
Marteau et al. Gut 2005;54:960-5

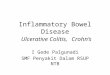
0102030405060708090
100
Rem. Imp. Rem. Imp.
week 4 week 8
%
P=0.308
P=0.0008
P=0.030
P=0.026
Pentasa orally + pentasa enema
Pentasa orally + placebo enema
Marteau et al. Gut 2005;54:960-5

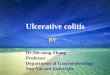
Time to cessation of rectal bleeding Time to cessation of rectal bleeding Patients with frank bleeding at baselinePatients with frank bleeding at baseline
Marteau et al. Gut 2005;54:960-5

Active disease Active disease ECCO Statement: Extensive colitis (cont)ECCO Statement: Extensive colitis (cont)
Systemic corticosteroids are appropriate if symptoms of active colitis do not respond rapidly to mesalazine [EL1b, RG C],
or for patients who are already taking appropriate maintenance therapy

Active disease Active disease ECCO Statement: ECCO Statement: Oral steroidOral steroid--refractory UCrefractory UC
● Patients with persistently active, steroid-refractory disease should be treated with azathioprine / mercaptopurine [EL1b, RG B], – Although surgical options should also be discussed – intravenous steroids, – infliximab [EL1b, RG B] – or calcineurin inhibitors [EL3, RG C]
should also be considered

Active disease Active disease ECCO Statement: ECCO Statement: ThiopurineThiopurine--intolerant or intolerant or --refractory ulcerative colitisrefractory ulcerative colitis
● Infliximab [EL1b, RG B] or surgical options should be considered
● Continued medical therapy that does not achieve steroid-free remission is not recommended [EL5, RG D]

Infliximab in Ulcerative colitis ACT1 & ACT2 Rutgeerts et al. N Engl J Med 2005;353:2462-76
●● 2 RCTs 364 patients in each
● Patients with active UC (extensive 40% - 46%):– Mayo score of 6 to 12 points - Endoscopic subscore ≥2
●Either– Concurrent treatment with ≥ 1 of the following:
– Steroids, azathioprine, 6-MP, or aminosalicylates (ACT 2 only)– Failure to tolerate or respond to ≥ 1 of:
– Steroids, azathioprine, 6-MP, or aminosalicylates (ACT 2 only)
● Infliximab 5mg/kg vs 10mg/kg vs placeboAt weeks. 0,2,6 then every 8 weeks. 46 weeks

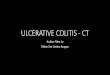
ACT 1 ACT 1 Rutgeerts et al. N Engl J Med 2005;353:2462-76
38,8
33,932
36,9
14,9 15,7
05
1015202530354045
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
IFX 5 mg/kgIFX 10 mg/kgPlacebo
‡
††
† 62
50,4
59
49,2
33,9
24,8
0
10
20
30
40
50
60
70
8 Weeks 30 Weeks
Perc
ent o
f Pat
ient
s
IFX 5 mg/kgIFX 10 mg/kgPlacebo
††
† †
21,7
10,1
0
5
10
15
20
25
CorticosteroidDiscontinued (Week 30)
Perc
ent o
f Pat
ient
s
IFX (combined)Placebo
†
Clinical RemissionClinical Remission EndoscopicEndoscopic RemissionRemission
Steroid discontinuationSteroid discontinuation

Infliximab (keep thiopurines) or calcineurine inhib.
AlgorithmAlgorithmOral 5-ASA (4g/d)
Oral 5-ASA (4g/d) + 5-ASA enema (or suppos?)
Oral steroids (40-60mg/d) (keep 5-ASA ?)
Tapering ... consider thiopurines (keep 5-ASA !)
Surgery

Infliximab (keep thiopurines) or calcineurine inhib.
AlgorithmAlgorithmOral 5-ASA (4g/d)
Oral 5-ASA (4g/d) + 5-ASA enema (or suppos?)
Oral steroids (40-60mg/d) (keep 5-ASA ?)
Tapering ... consider thiopurines (keep 5-ASA !)
Surgery
What happened before ?How many episodes ?Resistance to treatments ?
Severity ?Patient preferences ?Personal view on the risk/benefit

Infliximab (keep thiopurines) or calcineurine inhib.
AlgorithmAlgorithmOral 5-ASA (4g/d)
Oral 5-ASA (4g/d) + 5-ASA enema (or suppos?)
Oral steroids (40-60mg/d) (keep 5-ASA ?)
Tapering ... consider thiopurines (keep 5-ASA !)
Surgery
What happened before ?How many episodes ?Resistance to treatments ?
Severity ?Patient preferences ?Personal view on the risk/benefit
Directly ? No improvement
after 2 weeks

Infliximab (keep thiopurines) or calcineurine inhib.
AlgorithmAlgorithmOral 5-ASA (4g/d)
Oral 5-ASA (4g/d) + 5-ASA enema (or suppos?)
Oral steroids (40-60mg/d) (keep 5-ASA ?)
Tapering ... consider thiopurines (keep 5-ASA !)
Surgery
What happened before ?How many episodes ?Resistance to treatments ?
Severity ?Patient preferences ?Personal view on the risk/benefit
Directly ?
If previous failure to 5-ASA
If « rapid remissionneeded » ?
If nocturnal stools ?
No improvementafter 2 weeks
4-8 weeks

Infliximab (keep thiopurines) or calcineurine inhib.
AlgorithmAlgorithmOral 5-ASA (4g/d)
Oral 5-ASA (4g/d) + 5-ASA enema (or suppos?)
Oral steroids (40-60mg/d) (keep 5-ASA ?)
Tapering ... consider thiopurines (keep 5-ASA !)
Surgery
What happened before ?How many episodes ?Resistance to treatments ?
Severity ?Patient preferences ?Personal view on the risk/benefit
Directly ?
If previous failure to 5-ASA
If « rapid remissionneeded » ?
If nocturnal stools ?
If steroid dependencyor contra-indication
& thiopurine resistance
No improvementafter 2 weeks
4-8 weeks
4 weeks
4 - **** weeks