Embed Size (px)
DESCRIPTION
lpopp
Citation preview

Treatment of Class III Malocclusions UsingMiniplate and Mini-Implant AnchorageSeung-Hak Baek, Il-Hyung Yang, Keun-Woo Kim, and Hyo-Won Ahn
Orthodontic miniplates and mini-implants have become essential tools for
anchorage management. This article presents the treatment of growing Class
III patients with the use of the facemask in conjunction with the mini-plate
(FM/MP), and also the treatment of postadolescent Class III patients camou-
flaged by the use of mini-implants as skeletal anchorage. For FM/MP therapy,
an orthopedic force of more than 500 g per side with a vector of 30° downward
and forward from the occlusal plane was applied 12-14 hours per day after
placement of the curvilinear type surgical miniplates in the zygomatic buttress
areas of the maxilla. After 16 months of maxillary protraction, significant for-
ward displacement of the maxilla (point A) was found. Side effects of maxillary
protraction, such as labial tipping of the upper incisors, extrusion of the upper
molars, clockwise rotations of the mandibular plane, and bite opening, which
are usually observed using tooth-borne anchorage, were minimized. Therefore,
FM/MP can be an effective alternative treatment modality for maxillary hyp-
oplasia with minimal unwanted side effects. Class III patients in the postado-
lescent period can be camouflaged with fixed appliance by the use of mini-
implants as skeletal anchorage. The authors prefer to install the mini-implants in
the buccal attached gingiva between the upper second premolar and the first
molar. Class I intraarch elastics can be used to decompensate the already labially
inclined upper incisors. Class III interarch elastics can be used for distal en masse
movement of the lower dentition. Vertical elastics can be used to correct an open
bite problem if present. Extrusion or intrusion of the lower molars can be con-
trolled with strategic positioning of the mini-implants in the lower arch. With an
understanding of biomechanics, the careful use of miniplates and mini-implants
can expand the boundaries and scope of conventional fixed appliance therapy.
(Semin Orthod 2011;17:98-107.) © 2011 Elsevier Inc. All rights reserved.
desitp
Associate Professor, Department of Orthodontics, School of Den-tistry, Dental Research Institute, Seoul National University, Seoul,South Korea; Fellow Doctor and Graduate Student (PhD), Depart-ment of Orthodontics, School of Dentistry, Seoul National Univer-sity, Seoul, South Korea; Fellow Doctor and Graduate Student(PhD), Department of Orthodontics, School of Dentistry, Seoul Na-tional University, Seoul, South Korea; Resident and Graduate Stu-dent (PhD), Department of Orthodontics, School of Dentistry, SeoulNational University, Seoul, South Korea.
Address correspondence to Seung-Hak Baek, DDS, MSD, PhD,Associate Professor, Department of Oral and Maxillofacial Surgery,School of Dentistry, Dental Research Institute, Seoul National Uni-versity, Yeonkun-dong 28, Jongro-ku, Seoul, South Korea. E-mail:[email protected]
© 2011 Elsevier Inc. All rights reserved.1073-8746/11/1702-0$30.00/0
mdoi:10.1053/j.sodo.2010.12.003
98 Seminars in Orthodontics, Vol 17, N
Facemask in Conjunction withMiniplate as Skeletal Anchorage(FM/MP) Therapy for GrowingClass III Patients
The protraction facemask has been used tostimulate sutural growth at the circum-maxillary suture sites in growing Class III pa-tients with mild-to-moderate maxillary hyp-oplasia.1-3 However, the use of tooth-borne
evices as an anchor, such as palatal arches orxpansion appliances, can lead to unwantedide effects, such as labioversion of the upperncisors, extrusion of the upper molars, coun-erclockwise rotation of the upper occlusallane, and eventual clockwise rotation of the
andible.3-6o 2 (June), 2011: pp 98-107
piFutb
psmszb
Ta
99Class III Malocclusion and Miniplate/Mini-Implant
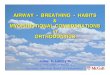
Placement of miniplates in the zygomatic but-tress area or other areas in the maxilla can trans-mit the orthopedic force to the maxilla directlyand minimize the rotational effect.7-11 Growing
atients with a Class III malocclusion and max-llary hypoplasia can be successfully treated withM/MP. The protocols of FM/MP are as follows:nder local anesthesia, a 1�2-cm horizontal ves-
ibular incision is made just below the zygomaticuttress area and the zygomatic buttress is ex-
Figure 1. Schematic drawing of installation and forcevector of the miniplate. (Courtesy of Professors BKCha and SM Kim.)
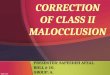
Figure 2. Initial records. (A) Facial photographs; (B)
version of figure is available online.)osed with a subperiosteal flap. Curvilinear typeurgical miniplates (Martin, Tuttlinger, Ger-any) are bent to conform to the anatomical
hape of the zygomatic buttress. The bone of theygomatic buttress has sufficient thickness andone quality for attachment of the miniplates.12
Placement of miniplates in this area is close tothe center of resistance of the nasomaxillarycomplex so the force vector can be placed closeto the center of rotation of the nasomaxillarycomplex.7,13,14 The mesial end hole of the mini-plate was modified to the shape of a hook forattachment of elastics. After the miniplates are
aoral photographs; (C) Lateral cephalograms. (Color
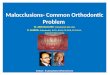
able 1. Skeletal and Dental Measurements Beforend After Treatment
Initial Debonding
SNA 76.0 80.6SNB 81.4 77.7ANB �5.4 2.9A-N perp �3.4 2.2Pog-N perp 4.7 0.6FMA 32.7 37.0U1 to FH 123.14 119.48IMPA 88.2 76.3Interincisal angle 121.48 135.5
Intr
shed
100 Baek et al
placed into the zygomatic buttress areas, 3 self-tapping type screws per side are used to fix theminiplates. The mesial end of the miniplateshould be exposed through the attached gingivabetween the upper canine and the first premolar
Figure 3. Treatment progress. (A) After 15 months,placed. (C) Normal overbite and overjet were establi
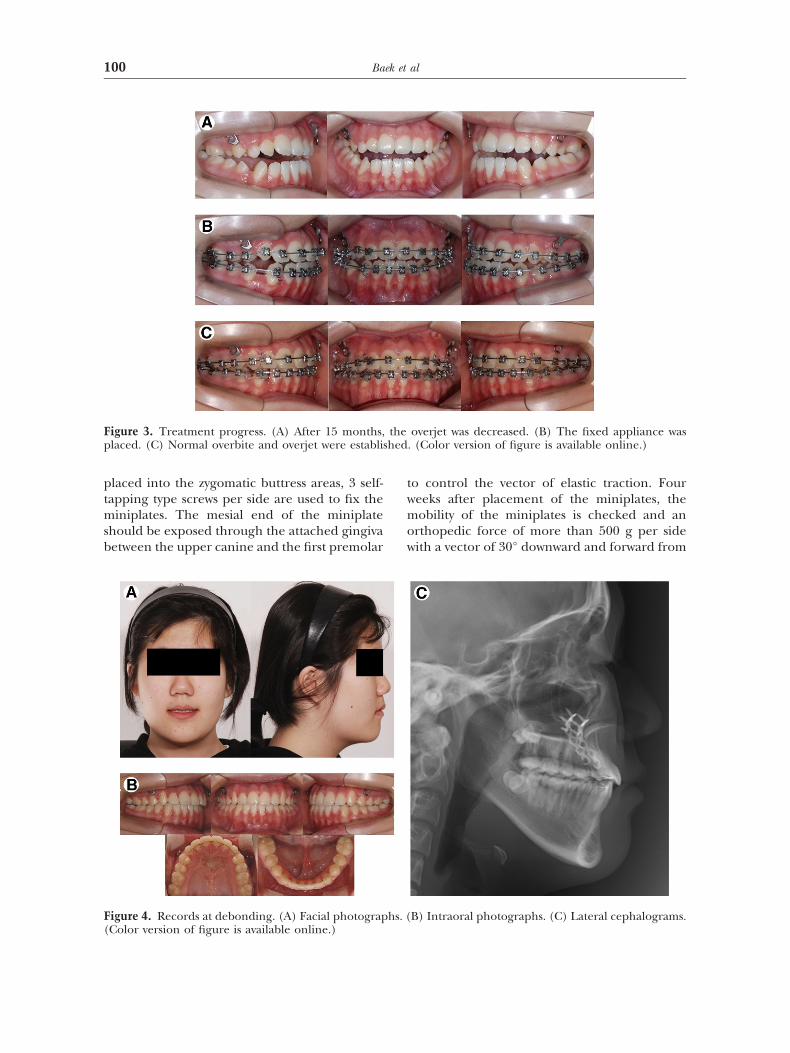
Figure 4. Records at debonding. (A) Facial photograp
(Color version of figure is available online.)to control the vector of elastic traction. Fourweeks after placement of the miniplates, themobility of the miniplates is checked and anorthopedic force of more than 500 g per sidewith a vector of 30° downward and forward from
overjet was decreased. (B) The fixed appliance was. (Color version of figure is available online.)
B) Intraoral photographs. (C) Lateral cephalograms.
the
hs. (

la le o
101Class III Malocclusion and Miniplate/Mini-Implant
the occlusal plane is applied for 12-14 hours perday (Fig 1). It is recommended to overcorrectthe malocclusion into a positive overjet andslight Class II canine and molar relationship.
Patients with cleft lip and or palate oftenpresent with a Class III malocclusions with max-illary hypoplasia. Scar tissue that develops aftercleft lip and palate surgery can disturb normalmaxillary growth. Because of hypoplasia of themaxillary and relative prognathism of the man-dible, treatment with conventional facemasktherapy might not achieve satisfactory results.15
The following Case 1 illustrates the treatment ofa cleft palate patient diagnosed with skeletal
Figure 5. Evaluation of the treatment changes. (A) Sateral cephalogram tracings (red in the online versionnd post-treatment. (Color version of figure is availab
Figure 6. Class III treatment mechanics using distalelastics and eventual counterclockwise rotation (flatt
available online.)Class III malocclusion and an anterior open biteusing FM/MP.
Case 1
Diagnosis and Treatment Plan
Figure 2 shows a 12-year-old girl who presentedwith a history of a repaired cleft palate and askeletal Class III malocclusion. The patient pre-sented with a concave facial profile, an anteriorcrossbite, and an anterior open bite. The cervi-cal vertebrae maturation index showed a stage 4skeletal maturation, indicating that her skeletal
rimposition between pre- (black) and post-treatment) Comparison of soft tissue profile between pre-, mid-
nline.)
asse movement of the lower dentition with Class IIIg) of the occlusal plane. (Color version of figure is
upe). (B
en menin
tmastottsirtit
102 Baek et al
age was beyond her pubertal growth spurt.16
The cephalometric analysis showed a skeletalClass III open-bite tendency with a steep man-dibular plane angle. This hyperdivergent growthpattern contraindicated conventional facemasktherapy (Table 1). Although growth observationfor 2 years and then reassessment was proposedto the patient, the patient’s parents elected toreceive the FM/MP therapy.
Treatment Progress
FM/MP therapy was started 4 weeks after place-ment of the miniplates according to the proto-col advocated by the authors (Fig 3A). Duringprotraction, fixed appliances were placed toalign the dentition (Fig 3B, C).
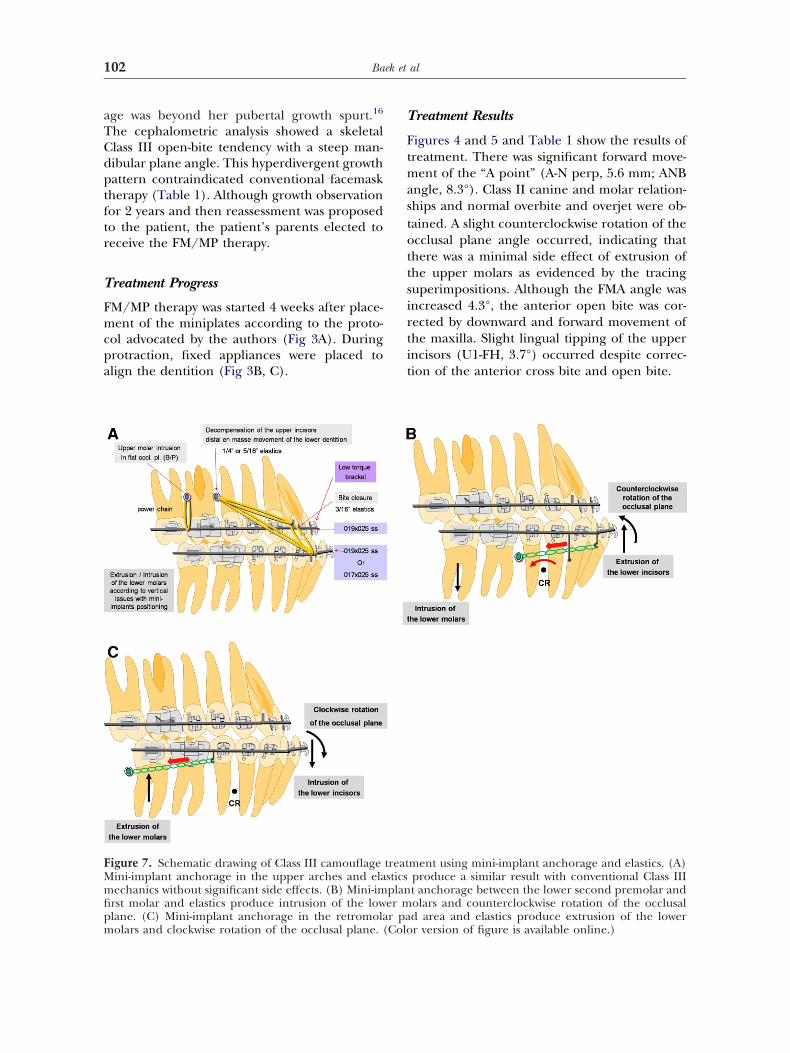
Figure 7. Schematic drawing of Class III camouflageMini-implant anchorage in the upper arches and elamechanics without significant side effects. (B) Mini-imfirst molar and elastics produce intrusion of the lowplane. (C) Mini-implant anchorage in the retromola
molars and clockwise rotation of the occlusal plane. (ColoTreatment Results
Figures 4 and 5 and Table 1 show the results ofreatment. There was significant forward move-
ent of the “A point” (A-N perp, 5.6 mm; ANBngle, 8.3°). Class II canine and molar relation-hips and normal overbite and overjet were ob-ained. A slight counterclockwise rotation of thecclusal plane angle occurred, indicating thathere was a minimal side effect of extrusion ofhe upper molars as evidenced by the tracinguperimpositions. Although the FMA angle wasncreased 4.3°, the anterior open bite was cor-ected by downward and forward movement ofhe maxilla. Slight lingual tipping of the upperncisors (U1-FH, 3.7°) occurred despite correc-ion of the anterior cross bite and open bite.
ment using mini-implant anchorage and elastics. (A)produce a similar result with conventional Class IIIt anchorage between the lower second premolar andolars and counterclockwise rotation of the occlusald area and elastics produce extrusion of the lower
treatsticsplaner mr pa
r version of figure is available online.)
hua
ctftlbcclc
Eciiape
Ta
103Class III Malocclusion and Miniplate/Mini-Implant
Treatment of Postadolescent Class IIIPatients by the Use of Fixed Appliancesin Conjunction with Mini-Implants asSkeletal Anchorage
Class III patients with mild-to-moderate skeletaldiscrepancies can be camouflaged by orthodontictooth movement. A half-step Class III molar rela-tionship could be corrected into a Class I molarrelationship by the use of distal en masse move-ment of the lower dentition with Class III elastics,counterclockwise rotation (flattening) of theocclusal plane, and dentoalveolar compensation(Fig 6).17-25 However, this treatment mechanics
as side effects, including labioversion of thepper incisors, extrusion of the upper molars,nd clockwise rotation of the mandible.
With recent development of mini-implant an-horage, the side effects of Class III camouflagereatment can be minimized.26,27 The authors pre-er to insert the mini-implants in the buccal at-ached gingiva between the upper second premo-ar and the first molar. Class I intraarch elastics cane used to decompensate the already labially in-lined upper incisors. Class III interarch elasticsan be used for distal en masse movement of theower dentition. Vertical elastics can be used to
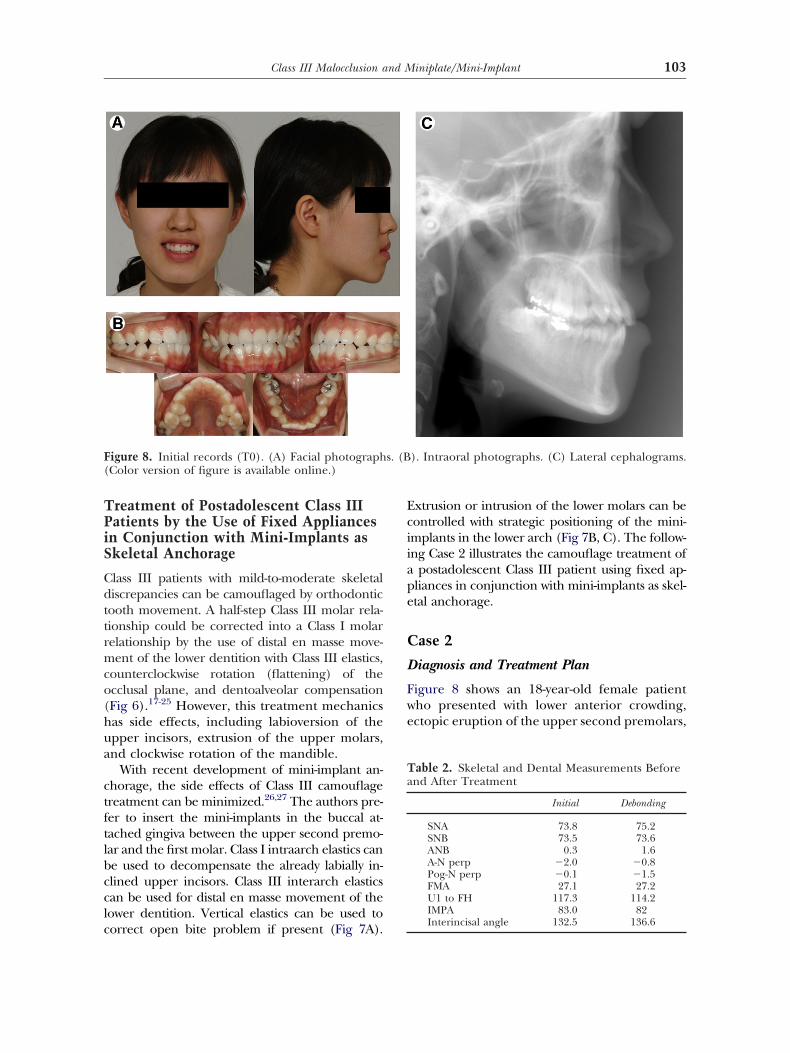
Figure 8. Initial records (T0). (A) Facial photograph(Color version of figure is available online.)
orrect open bite problem if present (Fig 7A).
xtrusion or intrusion of the lower molars can beontrolled with strategic positioning of the mini-mplants in the lower arch (Fig 7B, C). The follow-ng Case 2 illustrates the camouflage treatment of
postadolescent Class III patient using fixed ap-liances in conjunction with mini-implants as skel-tal anchorage.
Case 2
Diagnosis and Treatment Plan
Figure 8 shows an 18-year-old female patientwho presented with lower anterior crowding,ectopic eruption of the upper second premolars,
). Intraoral photographs. (C) Lateral cephalograms.
able 2. Skeletal and Dental Measurements Beforend After Treatment
Initial Debonding
SNA 73.8 75.2SNB 73.5 73.6ANB 0.3 1.6A-N perp �2.0 �0.8Pog-N perp �0.1 �1.5FMA 27.1 27.2U1 to FH 117.3 114.2IMPA 83.0 82
s. (B
Interincisal angle 132.5 136.6
mag o
aaraoesaloCaty
104 Baek et al
protrusive lower lip, and mild skeletal Class IIIalocclusion. The cephalometric analysis showedskeletal Class III open bite tendency with lin-
ually inclined lower incisors (Table 2). Becausethe patient elected to receive a nonsurgical treat-ment option, the treatment plan was extractionof the upper second premolar teeth and Class IIIcamouflage treatment with fixed appliances us-ing mini-implants as skeletal anchorage.
Treatment Progress
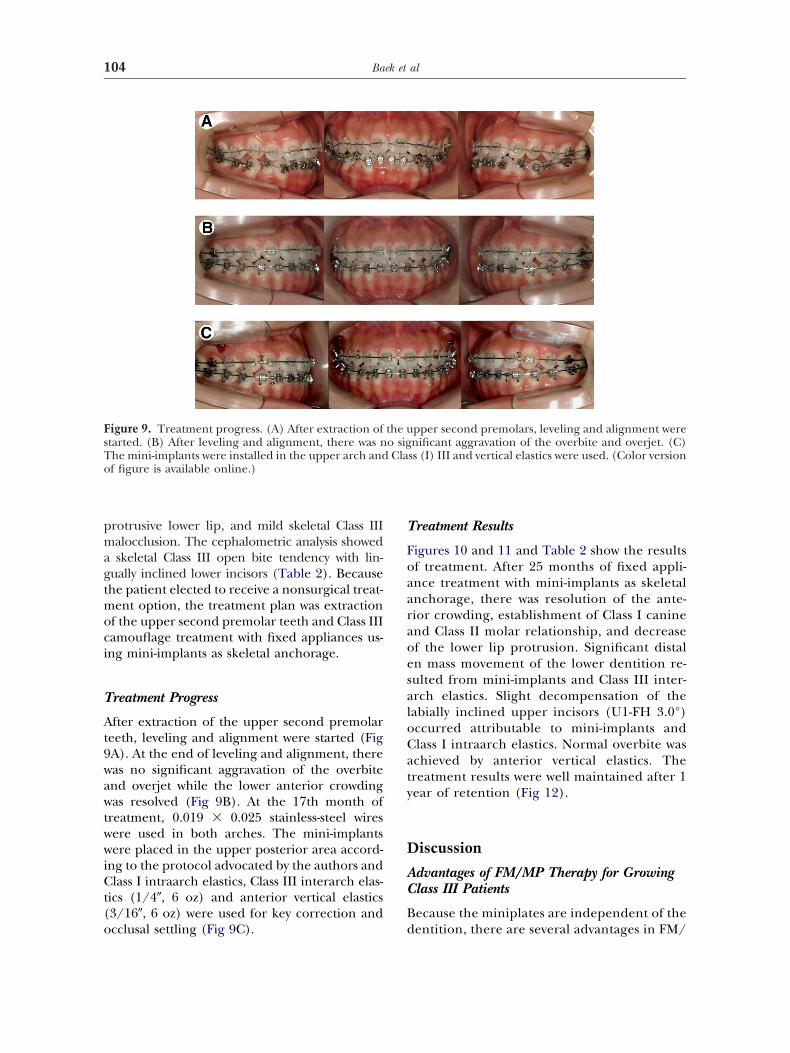
After extraction of the upper second premolarteeth, leveling and alignment were started (Fig9A). At the end of leveling and alignment, therewas no significant aggravation of the overbiteand overjet while the lower anterior crowdingwas resolved (Fig 9B). At the 17th month oftreatment, 0.019 � 0.025 stainless-steel wireswere used in both arches. The mini-implantswere placed in the upper posterior area accord-ing to the protocol advocated by the authors andClass I intraarch elastics, Class III interarch elas-tics (1/4�, 6 oz) and anterior vertical elastics(3/16�, 6 oz) were used for key correction and
Figure 9. Treatment progress. (A) After extraction ofstarted. (B) After leveling and alignment, there was nThe mini-implants were installed in the upper arch andof figure is available online.)
occlusal settling (Fig 9C).
Treatment Results
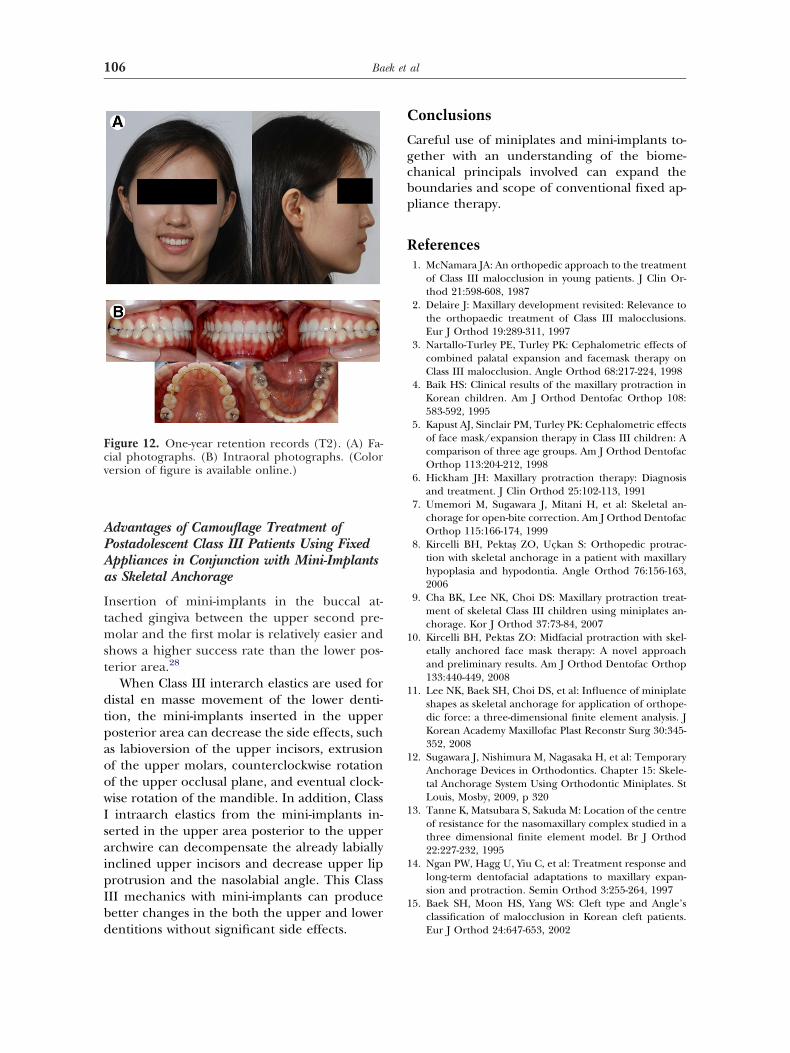
Figures 10 and 11 and Table 2 show the resultsf treatment. After 25 months of fixed appli-nce treatment with mini-implants as skeletalnchorage, there was resolution of the ante-ior crowding, establishment of Class I caninend Class II molar relationship, and decreasef the lower lip protrusion. Significant distaln mass movement of the lower dentition re-ulted from mini-implants and Class III inter-rch elastics. Slight decompensation of theabially inclined upper incisors (U1-FH 3.0°)ccurred attributable to mini-implants andlass I intraarch elastics. Normal overbite waschieved by anterior vertical elastics. Thereatment results were well maintained after 1ear of retention (Fig 12).
Discussion
Advantages of FM/MP Therapy for GrowingClass III Patients
Because the miniplates are independent of the
pper second premolars, leveling and alignment werenificant aggravation of the overbite and overjet. (C)
ss (I) III and vertical elastics were used. (Color version
the uo sigCla
dentition, there are several advantages in FM/
line
cT
105Class III Malocclusion and Miniplate/Mini-Implant
MP. Firstly, simultaneous orthodontic treat-ment and maxillary protraction using FM/MPis possible. Secondly, FM/MP can be used forrelatively longer periods than conventionalfacemask therapy and result in uniform ad-
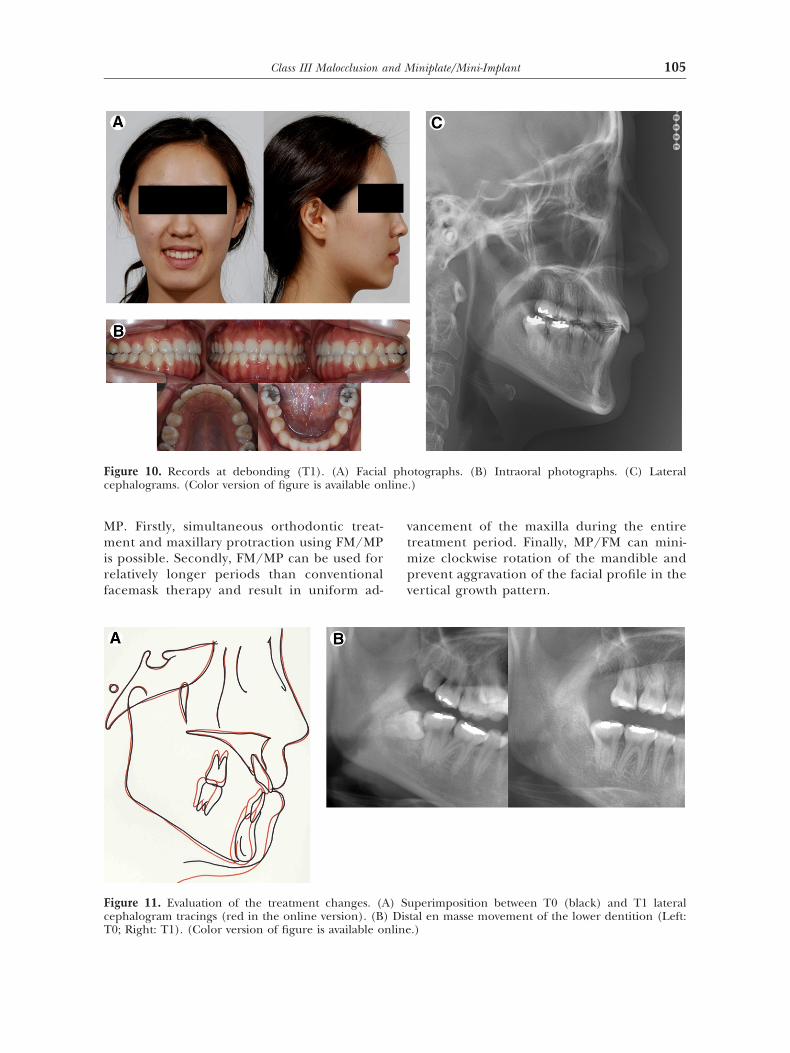
Figure 10. Records at debonding (T1). (A) Faciacephalograms. (Color version of figure is available on
Figure 11. Evaluation of the treatment changes. (Aephalogram tracings (red in the online version). (B
0; Right: T1). (Color version of figure is available onlinevancement of the maxilla during the entiretreatment period. Finally, MP/FM can mini-mize clockwise rotation of the mandible andprevent aggravation of the facial profile in thevertical growth pattern.
otographs. (B) Intraoral photographs. (C) Lateral.)
uperimposition between T0 (black) and T1 lateraltal en masse movement of the lower dentition (Left:
l ph
) S) Dis
.)
106 Baek et al
Advantages of Camouflage Treatment ofPostadolescent Class III Patients Using FixedAppliances in Conjunction with Mini-Implantsas Skeletal Anchorage
Insertion of mini-implants in the buccal at-tached gingiva between the upper second pre-molar and the first molar is relatively easier andshows a higher success rate than the lower pos-terior area.28
When Class III interarch elastics are used fordistal en masse movement of the lower denti-tion, the mini-implants inserted in the upperposterior area can decrease the side effects, suchas labioversion of the upper incisors, extrusionof the upper molars, counterclockwise rotationof the upper occlusal plane, and eventual clock-wise rotation of the mandible. In addition, ClassI intraarch elastics from the mini-implants in-serted in the upper area posterior to the upperarchwire can decompensate the already labiallyinclined upper incisors and decrease upper lipprotrusion and the nasolabial angle. This ClassIII mechanics with mini-implants can producebetter changes in the both the upper and lower
Figure 12. One-year retention records (T2). (A) Fa-cial photographs. (B) Intraoral photographs. (Colorversion of figure is available online.)
dentitions without significant side effects.
Conclusions
Careful use of miniplates and mini-implants to-gether with an understanding of the biome-chanical principals involved can expand theboundaries and scope of conventional fixed ap-pliance therapy.
References1. McNamara JA: An orthopedic approach to the treatment
of Class III malocclusion in young patients. J Clin Or-thod 21:598-608, 1987
2. Delaire J: Maxillary development revisited: Relevance tothe orthopaedic treatment of Class III malocclusions.Eur J Orthod 19:289-311, 1997
3. Nartallo-Turley PE, Turley PK: Cephalometric effects ofcombined palatal expansion and facemask therapy onClass III malocclusion. Angle Orthod 68:217-224, 1998
4. Baik HS: Clinical results of the maxillary protraction inKorean children. Am J Orthod Dentofac Orthop 108:583-592, 1995
5. Kapust AJ, Sinclair PM, Turley PK: Cephalometric effectsof face mask/expansion therapy in Class III children: Acomparison of three age groups. Am J Orthod DentofacOrthop 113:204-212, 1998
6. Hickham JH: Maxillary protraction therapy: Diagnosisand treatment. J Clin Orthod 25:102-113, 1991
7. Umemori M, Sugawara J, Mitani H, et al: Skeletal an-chorage for open-bite correction. Am J Orthod DentofacOrthop 115:166-174, 1999
8. Kircelli BH, Pektas ZO, Uçkan S: Orthopedic protrac-tion with skeletal anchorage in a patient with maxillaryhypoplasia and hypodontia. Angle Orthod 76:156-163,2006
9. Cha BK, Lee NK, Choi DS: Maxillary protraction treat-ment of skeletal Class III children using miniplates an-chorage. Kor J Orthod 37:73-84, 2007
10. Kircelli BH, Pektas ZO: Midfacial protraction with skel-etally anchored face mask therapy: A novel approachand preliminary results. Am J Orthod Dentofac Orthop133:440-449, 2008
11. Lee NK, Baek SH, Choi DS, et al: Influence of miniplateshapes as skeletal anchorage for application of orthope-dic force: a three-dimensional finite element analysis. JKorean Academy Maxillofac Plast Reconstr Surg 30:345-352, 2008
12. Sugawara J, Nishimura M, Nagasaka H, et al: TemporaryAnchorage Devices in Orthodontics. Chapter 15: Skele-tal Anchorage System Using Orthodontic Miniplates. StLouis, Mosby, 2009, p 320
13. Tanne K, Matsubara S, Sakuda M: Location of the centreof resistance for the nasomaxillary complex studied in athree dimensional finite element model. Br J Orthod22:227-232, 1995
14. Ngan PW, Hagg U, Yiu C, et al: Treatment response andlong-term dentofacial adaptations to maxillary expan-sion and protraction. Semin Orthod 3:255-264, 1997
15. Baek SH, Moon HS, Yang WS: Cleft type and Angle’sclassification of malocclusion in Korean cleft patients.
Eur J Orthod 24:647-653, 2002
107Class III Malocclusion and Miniplate/Mini-Implant
16. Hassel B, Farman AG: Skeletal maturation evaluationusing cervical vertebrae. Am J Orthod Dentofac Orthop107:58-66, 1995
17. Jacobson A: The “Wits” appraisal of jaw disharmony.Am J Orthod 67:125-138, 1975
18. Bibby RE: Incisor relationships in different skeletal pat-terns. Angle Orthod 50:41-44, 1980
19. Casko JS, Sheperd WB: Dental and skeletal variationwithin the range of normal. Angle Orthod 54:5-17, 1984
20. Ishikawa H, Nakamura S, Iwasaki H, et al: Dentoalveolarcompensation in negative overjet cases. Angle Orthod70:145-148, 2000
21. Costa-Pinho TM, Ustrell-Torrent JM, Correia-Pinto JG:Orthodontic camouflage in the case of a skeletal class IIImalocclusion. World J Orthod 5:213-223, 2004
22. Kim JY, Lee SJ, Kim TW, et al: Classification of the skeletalvariation in normal occlusion. Angle Orthod 75:311-319, 2005
23. Janson G, de Souza JE, Alves-Fde A, et al: Extreme den-
toalveolar compensation in the treatment of Class IIImalocclusion. Am J Orthod Dentofac Orthop 128:787-794, 2005
24. Baek SH: Treatment mechanics of Fixed Appliance forClass III malocclusion. J Korean Dental Association 44:229-238, 2006
25. Baek SH, Shin SJ, Ahn SJ, et al: Initial effect of multiloopedgewise archwire on the mandibular dentition in ClassIII malocclusion subjects. A three-dimensional finite el-ement study. Eur J Orthod 30:10-15, 2008
26. Sung JH, Kyung HM, Bae SM, et al: Microimplants inOrthodontics. Daegu, Korea, Dentos, 2006, pp 63-82
27. Baek SH, Moon CH, Sung SJ, et al: Orthodontic Mini-Implant: Treatment Strategy and Clinical Application.Seoul, Korea, Jeesung Publishing Co, 2007, pp 76-90,347-390
28. Moon CH, Lee DG, Lee HS, et al: Factors associated withthe success rate of orthodontic miniscrews placed in theupper and lower posterior buccal region. Angle Orthod
78:101-106, 2008