Embed Size (px)
Citation preview

Etiology of Class II malocclusions
Timothy Shaughnessy, DDS, MS, Workshop LeaderLawrence H. Shire, DDS, Workshop Recorder
In reviewing the literature relative to the develop-ment of Class II malocclusions, it can be learned that"not every Class II is a Class II." We must remember thatbehind the soft tissue drape of the patient’s face is atotally dynamic process that can be influenced by ourheritage and altered by our environment. We realizewhen performing an occlusal evaluation of our youngpatients, findings like distal step molar relation or anunusually large overjet may be presenting a false im-pression of what appears to be a true skeletal Class IImalocclusion.
In addition to distal step molar relation, or an unusu-ally large overjet, tooth size discrepancy with or withoutmalrelated mandible and maxilla may also give the firstimpression of a true skeletal Class II malocclusion.
Skeletal Class II malocclusions can be found to havevariants in one or more of the following regions: (1)maxillo-mandibular relationship (mandibularretrognathism, midface protrusion or both); (2) the cra-nial base (increased length of the anterior cranial basewill contribute to the midface protrusion, while length-ening of the posterior cranial base will tend to positionthe temporomandibular articulation more retrusively);(3) vertical dysplasia (anterior upper face height oftengreater than normal); (4) steep occlusal plane (a reflec-tion of vertical skeletal dysplasia).
What role does genetics play in the etiology of ClassII malocclusions? According to the study by Lundstrom(1984), investigations published prior to that articlehave suggested that about 40% of common anomalies intooth position and in the relationship between maxil-lary and mandibular dental arches are due to geneticdifferences between individuals. Corruccini and Potter(1980), in studies of different dental and occlusal vari-ables, found the heritability of dental overjet was re-duced to zero. Several syndromes have Class II maloc-clusions as a major finding. Of these syndromes,Treacher Collins, hemifacial microsomia, achondropla-
sia, and mobius syndrome are a few of the more widelyknown.
Inter-arch problems such as Class II and Class IIImalocclusions are genetic in nature, while intra-archproblems also have an environmental component aswell.
Looking at the importance of environmental vs.inherited factors in the etiology of malocclusions, it wassuggested that urbanization (and evolution) influencemalocclusions, making them more severe. The evolu-tionary factors involved are: a decrease in the size of thejaws, size and number of the teeth. We have no controlover these evolutionary factors (as well as the hereditaryfactors), whereas the environmental factors can often beeliminated through preventive or interceptive treat-ment at the appropriate time.
Mandibular growth deficit following condylar frac-tures or major trauma to the joint complex is highlylikely. Proffit (1980) found between 5 and 10% of allsevere mandibular deficiency or asymmetry problemswere related to previous fracture of the mandibularcondylar process. In this article, Proffit cites Walker andalso Gilhuus-Moe as noting that the younger the patientat the time of the injury, the greater the potential forcomplete regeneration of the condyle, and healing with-out residual deficit. Proffit (1978) states that Lund foundessentially complete recovery in 75% of the childrenwith early condylar fractures. The treatment goals forpatients with condylar fractures include the restorationof joint function, occlusion, and facial symmetry. Thecurrent theory on early treatment of condylar fracture inthe growing child calls for firm fixation for only I week,with physical therapy and mouth opening exercisesbeginning immediately after release of the rigid fixa-tion.
Condylar fractures often go unnoticed and result inClass II malocclusions with asymmetry or severemandibular deficiency. Progressive deformity is associ-ated with mechanical limitations on growth and theresulting condition is referred to as "functional
336 SPECIAL REPORT -- ETIOLOGY OF CLASS II MALOCCLUSIONS: Shaughnessy and Shire

ankylosis." Ankylosis of the mandible can be thought ofas fusion across the TMJ. This fusion restricts motionand inhibits growth. "In order to grow properly, themandible must be able to translate" (Proffit 1980).
Some theories to explain the growth of the craniofa-cial complex include: (1) Sicher’s role of sutural growth;(2) Scott’s role of the cartilage and the knowledge thatbone growth is secondary to cartilage growth; or (3)Moss’s functional matrix hypothesis that cartilage andbone respond secondarily to soft tissue growth. Stillanother theory is that of the influence of mouth breath-ing vs. nasal breathing to which Harvold (1980) eluded.
Experiments on transplantation and obvious reac-tions to manipulation of the sutures have, to somedegree, ruled out the sutural growth theory. Cartilagestudies have shown both positive and negative influ-ences on growth when transplantation of cartilage is thevariable factor of the studies. This depends uponwhether the cartilage is primary (from the primordialskeleton) or secondary cartilage. Primary cartilage is growth center where.as secondary cartilage, like that ofthe condyle, is a growth site. It has been shown that thereis a positive correlation between the soft tissue influenceand the growth of the craniofacial complex. For ex-ample, excessive intracranial pressure will cause hydro-cephaly, with a marked increase in the size of the calvar-ium, whereas diminished growth of the brain causesmicrocephaly. When an eye is removed from a child fortreatment of a tumor, the orbit does not continue to growin the normal fashion.
Normally, teeth are balanced between the tongueand the lips. Resting pressure must be considered moreimportant than the pressure created during chewing,swallowing, or speaking, since the time we are at rest faroutweighs the time we are performing these other func-tions. When comparing forces necessary to move teeth,heavy intermittent pressure has less effect than lightcontinuous forces.
How do habits relate to Class II malocclusions? Aswas previously stated, the light continuous forces aremuch more detrimental to the oral complex than areheavy intermittent forces. Habits such as thumb suck-ing, when performed for fewer than 6 hr per day, havenot been shown to be responsible for anterior open bitesor Class II malocclusions. Forward positioning of thetongue (seen during swallowing in patients with ante-rior open bite) is more likely to be an effect than a cause.
What is the mechanism by which nasal impairmentcould alter dentofacial form? Harvold et al. (1981), usingrhesus monkeys, forced them to become mouth breath-ers by mechanical obstruction of their nasal airway. Hewas able to show that previously obligate nose breath-ers forced to breathe 100% of the time through theirmouth, exhibited changes in their soft tissue and skele-
tal components. Changes in head, jaw, and tongueposition could be seen in the experimental group. Sometraits common among the sample were increased faceheight, steeper mandibular plane angle, and largergonial angle. It should be noted that some of the animalsin the experimental group developed other than Class IImalocclusions. Class III malocclusions as well as Class Imalocclusions were also seen. It is not the change inbreathing pattern that caused the malocclusions, butrather it is the change in related functional demands onthe craniofacial musculature and their obligatory re-sponse. Proffit (1978) states that the postural positioningof the head, mandible, and tongue are all at the subcon-scious level. Dentoalveolar morphology can be shownto be related to head posture. The more the head is heldforward, the more likely that the upper dentoalveolarheight will be increased. Also, there will be an increasein the steepness of the occlusal plane related to forwardposturing of the head.
McNamara (1981) reviewed Linder-Aronson’ s workfrom 1975 where it was shown, on a small sample size,that removal of nasal obstruction (adenoidectomy) in children, followed for 5 years postoperatively, had anaverage reduction in the mandibular plane angle of 4°.This was twice the reduction found in the control group(those without nasal airway obstruction and withoutadenoidectomy).
. Are there other environmental factors that causeClass II malocclusions? Early loss of maxillary primarymolars can influence the development of Class II maloc-clusions by allowing the maxillary molar, that may be inan end-on relation with the mandibular molar, to slipforward thus establishing a dental Class II situation. Itwould appear that local environmental factors influ-ence a dental Class II more than they influence a skeletalClass II. Understanding the etiology of the malocclu-sion, should play a role in developing a treatment plan.
The opinions or assertions contained herein are the private views ofthe authors and are not to be construed as official or as reflecting theviews of the Department of the Army or the Department of Defense.
Dr. Shaughnessy is in the private practice of orthodontics in Marietta,Georgia, and Dr. Shire is deputy director, U.S. Army Pediatric Den-tistry Residency Program, Ft. Lewis, Washington. Reprint requestsshould be sent to: Dr. Lawrence H. Shire, QTRS 2338 S. 3rd St., Ft.Lewis, WA 98433.
Corruccini RS, Potter RH: Genetic analysis of occlusal variation intwins. Am I Orthod 78:140-54. 1980.
Harvold EP etal: Primate experiments on oral respiration. Am JOrthod 79:359-72, 1981.
Lundstrom A: Nature versus nurture in dentofacial variation. Eur JOrthod 6:77-91, 1984.
Pediatric Dentistry: December, 1988 - Volume 10, Number 4 337

McNamara JA: Influence of respiratory pattern on craniofacial bances. Am J Orthod 78:1-24, 1980.growth. Angle Orthod 51:269-300, 1981.
Moss ML, Salentijn L: The primary role of the functional matricies infacial growth. Am J Orthod 55:566-77, 1969.
Proffit WR, Vig KW, Turvey TA: Early fracture of the mandibularcondyles: frequently an unsuspected cause of growth distur-
Proffit WR: Equilibrium theory revisited: factors influencing posi-tion of the teeth. Angle Orthod 48:175-86, 1978.
Solow B, Tallgren A: Head posture and craniofacial morphology.Am J Phys Anthropol 44:417-35, 1976.
PEDIATRIC DENTISTRY/Copyright © 1988 byThe American Academy of Pediatric Dentistry
Volume 10, Number 4
Supervision of Class II discrepanciesGerald S. Samson, DDS, Workshop LeaderMichael J. Hechtkopf, DDS, MSD, Workshop Recorder
Literature Review
Early orthodontic treatment continues to be contro-versial and the subject of arguments among dentists,especially pediatric dentists and orthodontists.
Clearly, there are psychological and sociologicalreasons for accepting the concept of early treatment.Attractiveness does have an effect on one’s life. In 1978,Kalick noted that cosmetic facial alterations improve apatient’s appearance and thereby directly enhance hisor her social value. The way in which others perceive theindividual is also based on attractiveness; physicallyattractive persons are preferred to the unattractive andthus receive preferential treatment (Bersheid andWalster 1974; Adams and Crossman 1978; Bersheid1981).
Bersheid (1981) noted that physical appearancemakes a difference in one’s life -- in education andcareers. Allen (1978) showed that social choices werebased on appearance, which one would expect, but alsonoted that attractive persons were perceived to be morehonest and independent. Of special importance is an-other of Bersheid’s comments describing how behavioris affected by our physical attractiveness, and how thatbehavior in turn affects another person’s behavior. Self-esteem also is impacted by attractiveness, and has psy-chological importance associated with a variety of be-haviors (Aronson and Mettee 1968).
Adams (1981) reported evidence exists to suggestthat attractiveness has an impact upon the social expe-
rience for both children and adults. He revealed datathat suggested that children as young as 3 and 4 years ofage are potentially influenced by physical attractive-ness. He also noted that appearance creates certainstereotypes, which stimulates expectations of specificattributes, and that this process may actually emergeshortly after birth and continue throughout life. Othershave suggested that as early as infancy, physical attrac-tiveness may have profound influences upon parentalattitudes, expectations, and behavior with their infants(Hildebrant 1976; Boukydis 1977). Adams (1981) made a most profound observation in noting that teach-ers, like parents, are influenced by attractiveness; teach-ers were more attentive and positive to attractive chil-dren.
Graber (1981) relates a surge in orthodontic care foryounger children under early orthodontic guidance fordentofacial esthetic purposes. Graber further notes thatmost children present for care due to parental motiva-tion, seeking dental and facial form alteration for per-sonal and social gain rather than biologic or physiologicimprovement.
There are, of course, other reasons for early ortho-dontic treatment, especially for the Class II patient. Bass(1983) raises the possibility of the risk of trauma unprotected incisors in active children. Approximately10% of children with severe overjet will fracture oravulse one or more maxillary incisors before attainingage 12 (Eichenbaum 1963; McEwen et al. 1967).
Another consideration is whether changes can be
338 SPECIAL REPORT -- SUPERVISION OF CLASS II DISCREPANCIES: Samson and Hechtkopf

effective in early treatment of Class II malocclusions.Enlow (1982) relates that the face grows and developsrapidly throughout the childhood period, as it "catchesup" with the earlier maturing brain and brain case. Bass(1983) describes a first phase of orthodontics as orthopedic phase to establish normal relationships ofthe skeletal components supporting the dentition. This,in turn, improves adverse soft tissue patterns.
As discussed by Krieg (1987), there are growth spurtsbetween the ages of 5 and 12, which he describes asperiods of growth in the craniofacial dimensions inwhich one period exceeds the growth velocity of aprevious period by twice. He notes that spurts are foundthroughout this age range, with highest peaks of growthvelocities in the younger age groups. He relates that dueto the active growth that characterizes the childhoodand juvenile growth periods, early treatment can bequite advantageous for certain orthodontic problems.Krieg adds that these younger patients are significantlymore cooperative than older groups. There is then agood possibility that the dentist’s efforts may be helpedby these growth spurts.
As early as 1960, Ricketts treated a sample of 8-year-old Class II patients, and showed that the maxilla wasnot an immutable structure. He showed that forcestransmitted to the sutures of the maxilla did affect thegrowth of the maxilla, changed teeth dramatically, andrelieved lip strain. Also, incisors were intruded andmolars distalized. The distal movement of the maxillaryfirst molar was most evident during the transition be-tween the primary and mixed dentitions. For this rea-son, Ricketts concluded, early treatment seemed advis-able for maximum orthodontic orthopedic correctioneven at the primary dentition level. Even earlier, Hahn(1954) reported that treatment of extreme Class II, Divi-sion 1 malocclusions and maxillary protrusions in theprimary dentition is valuable in that it retards the prog-ress of the malocclusions and gives a better opportunityfor success in the second period of treatment. Kloehn(1954) agreed that treatment should be directed andcorrelated with growth and not against it. He concludedthat this philosophy demands that treatment be startedas early as any factors and forces are recognized whichwill inhibit growth and development. Terry (1954) alsoadvocated early treatment of Class II malocclusionso In1962, Hahn, Cheney, and Tweed all supported the the-ory of early treatment of Class II, Division 1 malocclu-sions, in the mixed dentition stage.
It is clear from this brief review that there are socio-psychological reasons for early treatment of Class IImalocclusions, and at least moderate psychological andmechanical evidence to support the effectiveness of thistreatment.
The workshop concerning Supervision of Class IIdiscrepancies was divided by moderator Dr. Gerald
Samson into four major categories: (1) treatment timing;(2) records and analysis; (3) treatment objectives; and selection of clinician. Each of these were presented withone or more subheadings in question form to stimulatediscussion. The workshop then focused on each cate-gory and discussed it.
Treatment TimingAge for Evaluation
The workshop participants were interested in theage that a practitioner, regardless of specialty, shouldevaluate the developing dental and facial structures andadvise the parents regarding the need for detailedorthodontic records and analysis. There is presently nodefinitive literature available on the recommended agefor a first orthodontic exam, so the workshop tried toestablish some guidelines.
There was little disagreement among the workshopparticipants that for any craniofacial anomaly includingcleft palate, an orthodontic evaluation should occur atbirth, although this does not always mean a need forimmediate treatment. Such evaluation should by doneby a team, and the dentist on the team, although usuallya pediatric dentist, can be any dental practitioner (pedi-atric dentist, orthodontist, or general dentist) who canmake a critical evaluation of the pati,ent.
Other patients who present to the dentist at birth orshortly thereafter do not need a team evaluation. Suchpatients are those who present due to parental concernsor physician referral, or where there is potential ofmalocclusion due to a family history or hereditary prob-lem. Also included in this category are asymmetries ofthe skull or face. Again, the workshop participantsagreed that usually a pediatric dentist was the practitio-ner who should evaluate this patient, but that the evalu-ation could be performed by an orthodontist or generalpractitioner qualified to do a critical exam of the patient.
The practitioner should be familiar with normal vs.abnormal skeletal and facial structures, growth anddevelopment, and the temporomandibular joint com-plex. The College of Diplomates made the recommen-dation that some type of documentation is needed forthese patients, including photographs.
One of four dual-trained pediatric dentist/ortho-dontists attending the workshop noted how little ortho-dontic residency programs teach students concerningnormal pediatric developmental changes. It was agreedthat more information needs to be taught and shared inboth pediatric dental and orthodontic residency pro-grams concerning early growth of the skull, face, anddentition. It also was stated that orthodontists and otherpractitioners must realize that it is in the best interests ofchildren to allow more dissemination of information on
Pediatric Dentistry: December, 1988 - Volume 10, Number 4 339

this subject, so that dentists evaluating children do sowith expertise, or refers to another dentists as indicated.The participants further suggested that the AmericanAcademy of Pediatric Dentistry provide more knowl-edge for its members regarding the anatomy of theinfant face and skull, and that neonatologists and otherphysicians, as well as dentists, be called upon for thisinformation. Only in this manner can criteria be set fora functional history and dentofacial exam, which shouldbe a part of every routine exam.
Although the above criteria were agreed upon forany child’s evaluation, there was far less agreement onthe age that a child with a routine Class II malocclusionshould be evaluated. It was decided that these patientsshould certainly be seen not later than the eruption ofthe full complement of primary teeth and possibly ear-lier. Some of these patients may be too young for actualtreatment, but appropriate information should be re-lated to parents; habits that contribute to the problemcould be eliminated and nasal airways evaluated. It alsowas pointed out that there is a need for age-appropriateexam forms relating to patient development instead ofthe standard universal form for all ages of children usedin most offices.
Age of DiagnosisThe next discussion centered on the appropriate age
for diagnosis, that is, actual orthodontic records. Mostagreed that for very young children, the severity of thecase, the eruption of the second primary molars, andpatient management had to be taken into account. Inorder to observe whether the malocclusion is naturallyimproving or worsening, it was noted that some recordshad to be taken, for comparison of later findings. Thiswould be appropriate for those cases where treatment isnot immediately indicated for any reason. These rec-ords might be what are termed "mini-records," whichwould consist of a detailed clinical description andphotographs. Optional data for these abbreviated rec-ords might include study models and cephalometricanalysis. The workshop participants all agreed that thedetailed clinical description should include a functionaltemporomandibular joint exam and test for hypermo-bility of the mandible.
Records and AnalysisRecords would include a detailed clinical exam, a
functional exam, and description of discrepancy, photo-graphs, a lateral cephalometric radiograph, traced andanalyzed, a panoramic radiograph, and trimmed studymodels. Optional data to be included should be frontalradiograph, traced and analyzed, and a hand/wrist
radiograph for determination of skeletal age. In addi-tion, a panoramic radiograph should be repeated once ayear while treatment continues to check for any possibleindication of root resorption or ectopic eruption of teeth.
Attention should be given to condylar position,contour, and space on panoramic radiographs. Thisradiograph gives a screening of normality to the anat-omy of the condyles. If suspicious areas are noted, thenmore detailed tomogram-type radiographs should beordered.
In recommending a cephalometric analysis, certainkey factors should be required. Most Diplomates feltthat any analysis used for treatment on children shouldbe able to be related to age, race, facial type, facial softtissue and profile, possibly sex, and aimed at the grow-ing patient and aging of the face.
Discussion then centered on which methods avail-able could provide the desired information. It was notedthat the Steiner analysis was not age or race related andwas based on the sample analysis of one white femalepatient, and that Tweed’s analysis did not have a knownsample of patients, although the University of Michiganhad age related Tweed’s analysis.
It was generally accepted that the Rickett’s cepha-lometric analysis provided most of the relating informa-tion needed for diagnosis, although a few persons pres-ent felt it might be less accurate for very young childrenthan it is for those aged eight years and older.
Treatment Objectives
Although there was not complete agreement con-cerning objectives of early treatment, the followingstatement was adopted: "The objective of early Class IItreatment should be to obtain maximally achievableresults toward a Class I skeletal and dental relationship,and as closely as possible functional and esthetic nor-mality."
It was agreed that the overall objective was to attainoptimal facial and dental development, including facialharmony and balance, TMJ function, Class I skeletal anddental relationships, periodontal health, and enoughspace for eruption of the remaining permanent teeth.
In determining whether early treatment for Class IIcases can avoid extractions or orthognathic surgerylater; ~here was less discussion by the Diplomates. Mostfelt that preventing extractions in any subsequent treat-ment by early intervention was highly variable, butcertainly more likely. The workshop participants alsowere in agreement that early treatment would mostlikely prevent the need for surgery at a later date. Therewas concensus that early treatment did not necessarilypreclude the need for orthodontics at a later age, butsurely makes a case less difficult and complicated, andas stated, with less need for extractions or surgery. In
340 SPECIAL REPORT -- SUPERVISION OF CLASS II DISCREPANCIES: Samson and Hechtkopf

essence, phase I treatment is not complete until phase IItreatment begins.
Selection of ClinicianThe final discussion by the College of Diplomates
concerned who is best qualified to care and treat theClass II pediatric dental patient. The workshop con-cluded that any dental practitioner, whether a pediatricdentist, orthodontist, or general dentist, should treatthese patients provided the clinician meets the follow-ing criteria: (1) understands how to modify growth anddevelopment of the face; (2) is adequately trained; (3) able to enlist the compliance of the child patient; (4) "experienced" in providing the services; (5) has stayedabreast of the current literature; (6) has adequate knowl-edge on adjusting and manipulating the appliancesused; and (7) has provided the appropriate informationto the parent, including proper informed consent anddeposition of the case to completion or maturity, notingthe likelihood of a second phase of treatment.
Dr. Samson is in the full-time private practice of orthodontics anddentofacial orthopedics in Marietta, Georgia, and Dr. Hechtkopf is inthe private practice of pediatric dentistry in Virginia Beach, Virginia.Reprint requests should be sent to: Dr. Michael J. Hechtkopf, RoseHall Professional Centre, 3145 Virginia Beach Blvd., Virginia Beach,VA 23452.
Adams GR, Crossman, SM: Physical Attractiveness: A CulturalImperative. Roslyn Heights, New York; Libra Publishing, 1978.
Adams GR: The effects of physical attractiveness on the socializationprocess, in Psychological Aspects of Facial Form, Lucker GW etal., eds, monograph 11, Craniofacial Growth Series. Ann Arbor,Michigan; Center for Human Growth and Development 1980.
Allen BP: Social Behavior: Fact and Falsehood. Chicago; NelsonHall, 1978.
Aronson E, Mettee DR: Dishonest behavior as a function of differen-tial levels of induced self-esteem. J Personal Doc Psych 9:121-27,1968.
Bass NM: Dentofacial orthopedics in the correction of the skeletalClass II malocclusion, in Clinical Alterations of the Growing Face,McNamara JA Jr et al., eds, monograph 14, Craniofacial GrowthSeries. Ann Arbor, Michigan; Center for Human Growth andDevelopment 1983.
Bersheid E, Walster E: Physical attractiveness, in Advances in Experi-mental Social Psychology, vol 7, Berkowitz L, ed. New York;Academic Press, 1974.
Bersheid E: An overview of the psychological effects of physicalattractiveness, in Psychological Aspects of Facial Form, LuckerGW et al., eds, monograph 11, Craniofacial Growth Series. AnnArbor, Michigan; Center for Human Growth and Development1980.
Boukydis ZC: Infant attractiveness and the infant-caretaker relation-ship, paper presented to the International Conference on Loveand Attraction. Wales, United Kingdom; University of Swansea,September 1977.
Cheney EA: Treatment planning and therapy in the mixed dentition,presented at the 1962 annual meeting of the American Associa-tion of Orthodontists as part of a panel discussion by Hahn G,Cheney E, Tweed C, Terry H, Murray R. Am J Orthod 49:568-80,1963.
Eichenbaum IW: A correlation of traumatized anterior teeth toocclusion. ASDC J Dent Child 30:229-36, 1963.
Enlow DH: Handbook of Facial Growth, 2nd ed. Philadelphia; WBSaunders Co, 1982.
Graber LW: Psychological considerations of orthodontic treatment,in Psychological Aspects of Facial Form, Lucker GW et al., eds,monograph 11, Craniofacial Growth Series. Ann Arbor, Michi-gan; Center for Human Growth and Development 1980.
Hahn GW: Treatment in the deciduous dentition, read as part of apanel discussion before the American Association of Orthodon-tists, May 20, 1954. Am J Orthod 41:255-61, 1955.
Hahn GW: Treatment planning and therapy in the mixed dentition,presented at the 1962 annual meeting of the American Associa-tion of Orthodontists as part of a panel discussion by Hahn G,Cheney E, Tweed C, Terry H, Murray R. Am J Orthod 49:563-67,1963.
Hildebrant KA: Adult responses to infant cuteness (unpublishedmaster’s thesis). East Lansing, Michigan; Michigan State Univer-sity, 1976.
Kalick SM: Toward an interdisciplinary psychology of appearances.Psychiatry 41:243-53, 1978.
Kloehn SJ: At what age should treatment be started?, read as part ofa panel discussion before the American Association of Orthodon-tists, May 20, 1954. Am J Orthod 41:262-78, 1955.
Krieg WL: Early facial growth accelerations -- a longitudinal study.Angle Orthod 57:50-62, 1987.
McEwen JD, McHugh WD, Hitchin AD: Fractured maxillary centralincisors and incisal relationships. J Dent Res 46:1290, 1967.
Ricketts RM: The influence of orthodontic treatment on facial growthand development. Angle Orthod 30:103-31, 1960.
Terry HK: Cases indicating early treatment, read as part of a paneldiscussion before the American Association of Orthodontists,May 20, 1954. Am J Orthod 41:279-90, 1955.
Tweed CH: Treatment planning and therapy in the mixed dentition,presented at the 1962 annual meeting of the American Associa-tion of Orthodontists as part of a panel discussion by Hahn G,Cheney E, Tweed C, Terry H, Murray R. Am J Orthod 49:881-906,1963.
Pediatric Dentistry: December, 1988 ~ Volume 10, Number 4 341

PEDIATRIC DENTISTRY/Copyright © 1988 byThe American Academy of Pediatric Dentistry
Volume 10~ Number 4
Corrective methods for Class II patients]ames R. Long, DMD, Workshop LeaderPaul S. Casarnassimo, DDS, MS, Workshop Recorder
The Class II malocclusions represent a treatmentchallenge for which various appliances can be used,based on patient characteristics. This workshop ad-dressed the following questions.
1. Can the mandible be "grown?"2. What is a functional appliance?3. What criteria should be considered in Class II correc-
tion?4. What types of appliances are appropriate for Class II
correction?5. Does each treatment affect the growing face in the
same way?6. Which characteristics of a Class II malocclusion favor
the selection of a functional appliance?’7. What are the treatment effects of various appliances
according to the resource readings provided?
DiscussionCan the Mandible be Grown?
It appears that with timely treatment and using anappropriate appliance, the mandible can be stimulatedto grow and improve the malocclusion to some degree.The many variables affecting growth and its inherentunpredictability make it difficult to use growth stimula-tion reliably.
What is a Functional Appliance?The variety of functional appliances complicates a
definition. Each appliance reflects the philosophy, ob-jectives, and experience of its originator. An encompass-ing definition of the functional appliance is:
A functional appliance works on the malocclusion byemploying the activation of neuromuscular reflexes to guidethe developing jaws and erupting teeth of children into moreacceptable relationships.
Each appliance design -- the Frankel, Bionator, and
others -- emphasizes that particular aspect of the neu-romuscular physiology of the stomatognathic systemwhich its originator considered important. These vari-ations are reflected in differences in the constructionand use of the appliance.
Any appliance which alters growth is a functionalappliance. Headgear, for example, might be considereda functional appliance. A functional appliance ad-dresses; (1) mandibular position; (2) mandibular toothposition; and (3) the neuromuscular component of oro-facial complex.
What Criteria Should be Consideredin Class II Correction?
The following elements should be considered in theuse of any appliance in Class II correction:
Cephalometric appraisal -- Chin position/relation-ships; maxillary position/relationships; mandibularposition/relationships; tooth position/relationshipsClinical appraisal -- Habits; breathing; posture; intelli-gence; age of patient; temporomandibular joint statusCompliance appraisal -- Goal-orientedi persistence;adaptability to alternative appliance types to help pa-tient comply.
What types of appliances are appropriatefor Class II correction?
In a general sense, the following types of appliancesseem appropriate for Class II correction: (1) those aimedat orthodontic change; (2) those aimed at orthopedicchange; and (3) those aimed at alleviating parafunc-tional habits.
Ideally, an appliance should combine all 3 aspects oftreatment so as to address the individual patient’sneeds. In most cases, the functional appliance is ortho-dontic, orthopedic, and corrects parafunctional prob-lems.
342 SPECIAL REPORT -- CORRECTIVE METHODS FOR CI_ASS II PATIENTS; Long and Casamassimo

Does Each Treatment Affect the GrowingFace in the Same Way?
The workshop consensus was that all patients do notrespond in the same fashion, nor do all appliances workin the same way. Treatment outcomes may be similar,but the mechanisms and pathways may differ. TheTable shows the varying treatment effects of functionalappliances.
Which Factors of a Class II Malocclusion Favor theSelection of a Functional Appliance?
The following characteristics were identified as fa-vorable to the choice of a functional appliance: deepoverbite; lower arch crowding; greater than normaloverjet; Class II permanent molar relationship; protru-sive maxillary incisors; retruded mandibular incisors;
short corpus length; less-than-normal lower face height.
What are the Treatment Effects of VariousAppliances According to the ResourceReadings Provided?
The Table depicts the anticipated treatment effectsfor the following structures: maxillary first permanentmolar; mandibular first permanent molar; upper lip;chin; mandible; maxilla; maxillary incisor; and mandi-bular incisor.
The appliances described in the resource readingsand compared in discussion include the following fixedand removable appliances: Bionator; activator; head-gear (cervical, occipital, and hook-on); combined head-gear-activator; edgewise appliance; edgewise withClass II elastics; and Frankel II.
TA.LE. Class II Treatment Effect
Upper Lower Upper Lip Chin Mandible Maxilla Max. Mand.Molar Molar Incisor Incisor
Bionator Same as Same as . No No No No Tipped Intrudedgrowth growth change change change change lingual with
growth
Activator Same as Upward No No Slight Held Tipped Nogrowth change change change back lingual change
from fromgrowth growth
Headgear Distal Distal Flatter Down- No Held No Slight1. Cervical direc- intruded ward change back change lingual
tional from from move-growth growth/ ment
distal-ized
2. Occipital Distal Same as Same as No Auto- Distal- No Nodirec- growth growth change rotation ized change changetional from
growth
3. Hook-on Direc- Same as Flatter/ No Auto- Distal- Tipped Notional growth fuller change rotation ized lingual change
directional fromgrowth
Combined HG- Distal Vertical Same as Forward Auto- Distal- Direc- TippedActivator growth rotation ized tional labial
Edgewise No No No No Slight No Direc- Direc-change change change change change change tional tional
Edgewise with No Upward Flatter Forward Slight Distal- Direc- TippedClass II change vertical change ized tional labial
fromgrowth
Frankel II Vertical Vertical More No No No Tipped Tippedfull change change change lingual labial
from fromgrowth growth
Pediatric Dentistry: December, 1988 - Volume 10, Number 4 343

ConclusionsThe treatment of Class II malocclusions can involve
a variety of appliance designs, many of which act tostimulate mandibular growth. The functional applianceaffects neuromuscular reflexes to help correct the mal-occlusion. Selection of appropriate appliances is basedon patient characteristics as well as diagnosis. CertainClass II malocclusion characteristics seem more suitedto the functional appliance. The correction of the maloc-clusion by different appliances can be linked to differingeffects on various parts of the stomatognathic system.
Dr. Long is in the full-time private practice of orthodontics in Atlanta,Georgia, and Dr. Casamassimo is chief of dentistry and director,Pediatric Dentistry Residency Program, Children's Hospital, Colum-bus, Ohio. Reprint requests should be sent to: Dr. Paul S. Casamas-simo, Columbus Children's Hospital, Dept, of Pediatric Dentistry,700 Children's Dr., Columbus, OH 43205.
Armstrong MM: Controlling the magnitude, direction, and durationof extraoral force. Am J Orthod 59:217-43, 1971.
Gianelly A et al: A comparison of Class II treatment changes notedwith the light wire, edgewise, and Frankel appliances. Am JOrthod 86:269-76,1984.
Harvold EP, Vargervik K: Morphogenetic response to activatortreatment. Am J Orthod 60:478-90,1971.
Klein PL: An evaluation of cervical traction on the maxilla and theupper first permanent molar. Angle Orthod 27:61-68, 1957.
McNamara JA et al: Skeletal and dental changes following functionalregulator therapy on Class II patients. Am J Orthod 88:91-110,1985.
Odom WO: Mixed dentition treatment with cervical traction andlower lingual arch. Angle Orthod 53:329-42, 1983.
Owen AH: Mandibular incisolabial responses in Class II, division 1treatment with Frankel and edgewise. Angle Orthod 56:56-87,1986.
Ricketts RM: The influence of orthodontic treatment on facial growthand development. Angle Orthod 30:103-31, 1960.
Schmuth GPF: Milestones in the development and practical applica-tion of functional appliances. Am J Orthod 84:48-53, 1983.
Schulhof R], Engle GA: Results of Class II functional appliancetreatment. J Clin Orthod 16:587-99, 1982.
PEDIATRIC DENTISTRY/Copyright 6 1988 byThe American Academy of Pediatric Dentistry
Volume 10, Number 4
Pioneer in Pediatric Dentistry: James J. Leib
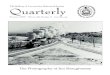
Dr. James J. Leib was born on Decem-ber 21,1945, in Los Angeles, California.He attended the local elementaryschools, and was graduated from Bev-erly Hills High School in 1942.
After attending the University ofSouthern California from 1942 to 1944,he enlisted in the U.S. Navy and servedfrom 1943 to 1946, and again from 1948 to1949 and 1952 to 1954. In 1948 Dr. Leibreceived the DDS degree from the Col-lege of Physicians and Surgeons, Univer-sity of the Pacific School of Dentistry.
Dr. Leib was clinical instructor inpediatric dentistry at the University ofSouthern California from 1957 to 1958 and from 1970 to1972. His hospital affiliations included Children's Hos-pital of Los Angeles, Tarzana Hospital, and EncinoHospital where he is chairman of the dental and oralsurgery staff.
He is a past-president of the San Fernando Valley
Dental Society and the Southern Cali-fornia Society of Pediatric Dentistry. Dr.Leib served the American Academy ofPediatric Dentistry as president in 1972,and as a member of the Board of Trus-tees.
He was a member of the Dental CareCommittee of the California DentalAssociation (1960-65), the LegislationCouncil (1961 -71), and the University ofthe Pacific Dental Alumni Board of Di-rectors (1948). Dr. Leib is a Fellow of theAmerican and International College ofDentists and the American Academy ofPediatric Dentistry.
Dr. Leib, his wife Marian, and their two children,Geoffrey and Denise, reside in Pasadena, California.
Ralph L. Ireland, DDSHistorian Emeritis
344 SPECIAL REPORT — CORRECTIVE METHODS FOR CLASS II PATIENTS: Long and Casamassimo