Embed Size (px)
Citation preview

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 1/10
Ž .International Journal of Gynecology & Obstetrics 72 2001 6170
Review articleTreatment guidelines for depression in pregnancy
S.M. Marcusa,, K.L. Barry b,c, H.A. Flynnb, R. Tandond, J.F. Gredenb,e
aUni ersity of Michigan Department of Psychiatry, Ambulatory Ser ices and Women’s Health Program, Ann Arbor, MI, USA
bUni ersity of Michigan Department of Psychiatry, Ann Arbor, MI, USA
c Department of Veterans Affairs, Serious Mental Illness Treatment Research and E aluation Center, Ann Arbor, MI, USA
d Hospital Ser ices, Uni ersity of Michigan Department of Psychiatry, Ann Arbor, MI, USA
e Mental Health Research Institute, Ann Arbor, MI, USA
Received 24 May 2000; accepted 4 June 2000
Abstract
Depression is a ubiquitous disorder in childbearing women with up to 10% of women experiencing depression inpregnancy. Postpartum depression occurs in 1216% of pregnancies making it a common complication. Moreover,these illnesses are frequently underdiagnosed in obstetric settings, and a recent report of the Surgeon General’sOffice confirms that many women do not access services, or receive treatment of inadequate intensity or duration.This paper provides current treatment guidelines to aid in appropriate diagnosis and treatment of depression inpregnancy and postpartum. Review of current literature on psychotropic medication use in pregnancy is alsoprovided. 2001 International Federation of Gynecology and Obstetrics. All rights reserved.
Keywords: Pregnancy; Postpartum; Depression; Antidepressant medication
1. Introduction
Depression is among the most common of health disorders in women. There are five keyfactors that are important to further characterize
Ž .predictors of Major Depressive Disorder MDDduring pregnancy in order to develop more effec-
Corresponding author. Adult Ambulatory Division andDepression Center, University of Michigan Health Systems, Ann Arbor, MI, USA. Tel.: 1-734-764-0267.
Ž . E-mail address: [email protected] S.M. Marcus .
tive strategies for treatment and prevention. First,almost one woman in four will experience depres-
sion at some point in her life 1 . Second, depres-sive episodes present most often during the child-bearing years, and almost 10% of women will
experience depression during pregnancy 2 . Third,MDD is now recognized as a recurrent disorder, with risks of relapse increasing for those with
prior episodes following antidepressant discontin-uation. Fourth, it is commonplace for physiciansto withdraw antidepressant medications at thetime of conception for women receiving treat-
0020-729201$20.00 2001 International Federation of Gynecology and Obstetrics. All rights reserved.Ž .PII: S 0 0 2 0 - 7 2 9 2 0 0 0 0 3 1 8 - 0

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 2/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 617062
ment for depression. Fifth, there is little informa-tion available about specific risk factors for re-lapse during pregnancy, or strategies for prevent-ing episodes. It is critical for clinicians treatingchildbearing women to have information availableto guide them in treatment decisions as they
negotiate the delicate balance between use of psychotropic medication during pregnancy vs. therisks of undertreating the woman’s depressive ill-ness and risking relapse. The purpose of thispaper is to review the available data on the risksand sequelae of using various psychotropic medi-cations during pregnancy and lactation, and toprovide guidelines for the treatment of majormood disorders through pregnancy and postpar-tum. These guidelines will emphasize pharmaco-logic, psychotherapeutic, and psychosocial man-agement strategies.
1.1. Background
Although there have been advances in psy-chopharmacologic treatment for depression, a re-cent report of the United States Surgeon Gen-eral’s Office confirms that many women do notseek treatment. Many who do seek treatment fordepression do so in the primary care setting where50% go unrecognized and many more are under-
treated 3 . At the University of Michigan HealthSystem, pilot data suggests that a diagnosis of depression is made in only 0.8% of childbearing
women 4 , however, national data suggests1020% prevalence of the disorder in medical
surgical settings 5 . Of those who are diagnosed,most receive inadequate treatments. In addition,medical adherence is extremely problematic; half of antidepressants prescribed are not filled after
the first month 6 . The under-detection and un-der-treatment of depression in women of child-bearing age leads to substantial maternal andinfant morbidity, and medical costs. Psychiatricillness has adverse consequences in pregnancyincluding inadequate nutrition, poor compliance
with prenatal care, poor pregnancy outcomes,substance abuse, and dangerous risk-taking be- havior 7 . The more dramatic outcomes such as
risk taking, fetal abuse, or maternal suicide maybe the disastrous consequences of untreated
depression in pregnancy 8 . In women withbipolar illness, the risk of postpartum relapse is well established and estimated between 30 and50% particularly when mood stabilizers are dis-
continued 9 .Due to the prevalence of psychiatric disorders
in childbearing women, many women are usingpsychotropic medications at the time of concep-tion. As all psychoactive medications cross theplacental barrier, the woman’s health and diseasemanagement must be balanced against the risk of infant exposure during pregnancy. Many timesthe risk of medication is outweighed by the sub-stantial morbidity of the undertreated illness.
2. Research on adverse effects of psychotropic
medications in pregnancy
Psychotropic medications potentially can haveŽ .three types of adverse effects on the fetus: 1
teratogenic effects increase risk of congenitalmalformation usually during the first trimester;Ž .2 neonatal toxicity and withdrawal syndromesare usually related to ongoing third trimester
Ž .exposure; 3 behavioral effects are more difficultto characterize and are manifest by later behav-ioral and developmental difficulties in the child.
The FDA has assigned risk categories B, C, D,and X to different psychotropic medications. Cat-egory A indicates no risk. The risk categories are
useful even though estimates of the teratogeniceffects of various psychotropic medications areimprecise. Bupropion, clozapine, and buspironehave received the B designation, which indicatesan absence of human risk with the caveat of
Žlimited data. SSRIs fluoxetine, sertraline, paroxe-.tine , desipramine, venlafaxine, mirtazapine, nefa-
zodone, clonazepam, and most conventional andatypical antipsychotics have received the C desig-nation. This denotes that human risk cannot beentirely eliminated because of inadequate humanclinical trials and either no animal studies or, in
some, evidence of risk in animals. The D designa-tion has been assigned to lithium, carbamazepine,sodium valproate, most tricyclic antidepressants,
Žand other benzodiazepines other than clo-.nazepam , indicating evidence of fetal risk but not

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 3/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 6170 63
an across the board contraindication during preg-nancy. Benzodiazepines, including triazolam,temazepam, flurazepam, and quazepam have re-
Ž .ceived the X completely contraindicated desig-nation.
3. Antidepressant and mood stabilizing agents
There are significant methodological issues inthe study of antidepressant medications in preg-nancy. Factors including the use of other medica-tions, the impact of other comorbid illnesses anduse of alcohol and nicotine, genetic factors, ma-ternal age, and time of gestation can confound
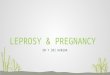
the results of studies in this area 10 . Table 1includes the teratogenicity, neonatal toxicity, andbehavioral risks associated with antidepressantand mood stabilizing agents during pregnancy andlactation. This section briefly summarizes the mostsalient studies for each type of agent.
3.1. Selecti e serotonin reuptake inhibitors
3.1.1. PregnancyŽRecent research on the use of SSRIs fluoxe-
.tine, sertraline, paroxetine, fluvoxamine suggeststhat they are relatively safe for both the motherand fetus during pregnancy. Studies with fluvox-
amine, paroxetine and sertraline have failed to show an increased risk of fetal anomalies 11,12 .
There have been no maternal reports of adverse sequelae in the infants exposed to sertraline 13 .
Moreover, longer term studies assessing infantdevelopment reveal that infants exposed to a vari-ety of tricyclic agents as well as fluoxetine weredevelopmentally normal and similar to siblingcontrols on measures of IQ and learning at the
age of 5 years 14 . In another European study, noincrease in congenital abnormalities was found inthe perinatal period in 969 infants whose mothers
used SSRIs andor tricyclic antidepressants 15 .The study was unique in that it included 375infants exposed to citalopram, a newly approvedSSRI in the United States. These findings did notsupport two adverse reaction reports linking
citalopram during early pregnancy with opticnerve hypoplasia and septum pellucidum defects.
Not all studies have supported the safety of the SSRIs in pregnancy and one group 16 concluded
from a prospective cohort study that the infantsof women who take fluoxetine in the first trimester
are at increased risk for minor anomalies, such aslarger for their gestational age with 55% fallinginto the 90th percentile and above for birthweightindicating a teratogenic effect. They also reportedthat those exposed during the third trimester areat increased risk for premature delivery, poorneonatal adaptation, cyanosis on feeding, and jit-teriness. The findings of this study have beencriticized for confounding factors of severity of depressive illness in the mother and increased
maternal age 17 .
3.1.2. LactationFluoxetine and sertraline are secreted in breast
milk and there is one report of infant irritability with exposure to fluoxetine through lactation,though no reports of neonatal difficulties in lac-
tating infants who’s mothers used sertraline 12 .Paroxetine was not found in measurable quanti-ties in breast milk, and there were not reports of infant difficulties when this agent was used.
3.1.3. General information
SSRIs are excellent first line agents and canalso be used with panic disorder or obsessivecompulsive disorder. Potential side effects fluox-etine can include agitation, insomnia, gastroin-testinal distress such as nausea or diarrhea, facialtension or headaches, sexual side effects, or weightgain.
3.2. Tricyclic antidepressants
3.2.1. Pregnancy
There are many studies exploring the risk of fetal exposure to the tricyclic agents during preg-nancy. A comprehensive review of the literaturefrom 1966 to 1995 did not reveal an associationbetween fetal exposure to tricyclic antidepres-

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 4/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 617064
T a b l e 1
S u m m a r y o f t e r a t o g e n i c i t y , n e o n a t a l t o x i c i t y , a n d b e h a v i o r a l r
i s k s a s s o c i a t e d w i t h a n t i d e p r e s s a n t a n d m o o d
s t a b i l i z i n g a g e n t s d u r i n g p r e g n a n c y a n d l a c t a
t i o n
D r u g
T e r a t o g e n i c i t y
N e
o n a t a l t o x i c i t y
B e h a
v i o r a l r i s k
L a c t a t i o n
S S R I s
F o u n d t o b e s a f e f o r b o t h
A n
e c d o t a l r e p o r t s o f p o s s i b l e c o l i c ,
O n e
s t u d y f o u n d n o a d v e r s e
B o t h fl u o x e t i n e a n d s e r t r a l i n
Ž
m o t h e r a n d f e t u s n o i n c r e a s e
i r r i t a b i l i t y a n d i n c r e a s e d r e s p i r a t o r y
n e u r
o p s y c h i a t r i c e f f e c t s o n
a r e s e c r e t e d i n
t o b r e a s t m i l k ;
Ž
.
i n s p e c i fi c m a l f o r m a t i o n s i n
r a t e p a r o x e t i n e o n l y
l a n g u a g e ,
I Q , o r b e h a v i o r
d u e t o l o n g h a
l f - l i f e o f fl u o x e t i n e ,
Ž
s t u d i e s t o d a t e
i n c h i l d r e n u p t o
e x p o s u r e t h r o u
g h b r e a s t m i l k
.
Ž
.
5 y e a
r s
fl u o x e t i n e o n l y
m a y l e a d t o d e
t e c t a b l e l e v e l s
i n b r e a s t m i l k ;
m o r e s t u d y
n e e d e d
B u p r o p i o n
N o a d e q u a t e w e l l - c o n t r o l l e d
N o
i n f o r m a t i o n o n n e o n a t a l t o x i c i t y
N o s t u d i e s o f b e h a v i o r a l r i s k
P h a r m a c o k i n e
t i c s t u d i e s h a v e
s t u d i e s . R e p r o d u c t i v e s t u d i e s i n
r e v e a l e d t h a t b
u p r o p i o n a n d
a n i m a l s i n d o s e 7 1 2 t i m e s
i t s m e t a b o l i t e s
a r e s e c r e t e d
h u m a n d o s e r e v e a l e d n o e v i d e n c e
i n b r e a s t m i l k
o f t e r a t o g e n i c i t y . P r e g n a n c y
r e g i s t r y f a i l e d t o d e m o n s t r a t e
r i s k o f s p e c i fi c a n o m a l i e s
T r i c y c l i c s
N o c o n g e n i t a l d e f e c t s f o u n d
A
n u m b e r o f p e r i n a t a l s y n d r o m e s
V e r y
l i m i t e d d a t a o n h u m a n s ;
T r i c y c l i c a g e n t s a r e s e c r e t e d i n t o
w i t h f e t a l e x p o s u r e
a s s
o c i a t e d w i t h w i t h d r a w a l
o n e s t u d y ; f o u n d n o a d v e r s e
b r e a s t m i l k ; i n
f a n t s f o u n d t o b e a t
h a v e b e e n f o u n d
n e u r
o p s y c h i a t r i c e f f e c t s o n
l o w r i s k f o r a d
v e r s e e f f e c t s ;
l a n g u a g e , I Q , o r b e h a v i o r
m o r e s t u d y n e e d e d
Ž
.
i n c h i l d r e n u p t o 5 y e a r s
Ž
.
t r i c y c l i c a g e n t s o n l y
M o n o a m i n e
C o n t r a i n d i c a t e d i n p r e g n a n c y
C o n t r a i n d i c a t e d i n p r e g n a n c y
C o n t r a i n d i c a t e d i n p r e g n a n c y
C o n t r a i n d i c a t e
d i n l a c t a t i o n
o x i d a s e
i n h i b i t o r s
B e n z o d i a z e p i n e s
P o s s i b l e c a u s e o f c l e f t p a l a t e
M u
l t i p l e s e q u e l a a s s o c i a t e d w i t h
S o m e e v i d e n c e o f
S e c r e t e d i n t o b r e a s t m i l k ; m a y
p r e
n a t a l e x p o s u r e ,
i n c l u d i n g
d e v e l o p m e n t a l d e l a y
c o n t r i b u t e t o l e t h a r g y , w e i g h t
w i t
h d r a w a l s y n d r o m e w i t h
l o s s , a n d k e r n i
c t e r u s i n i n f a n t s
s u s
t a i n e d u s e i n t h i r d
e x p o s e d
t r i m
e s t e r
L i t h i u m
I n c r e a s e d r i s k o f m a t e r n a l
A s s o c i a t e d w i t h n e o n a t a l m o r b i d i t y ;
N o d
e v e l o p m e n t a l r i s k s
S h o u l d n o t b e
u s e d d u r i n g
c a r d i a c c o n g e n i t a l a n o m o l i e s
n e o n a t a l t o x i c i t y m a y r e s u l t w h e n
n o t e d i n h u m a n s
b r e a s t f e e d i n g d u e t o t o x i c i t y
m a
t e r n a l b l o o d l e v e l s a r e n o t c l o s e l y
m o
n i t o r e d i n t h i r d t r i m e s t e r a n d
i m m e d i a t e l y p o s t p a r t u m
C a r b a m a z e p i n e
I n c r e a s e d r i s k o f c o n g e n i t a l
L i m
i t e d d a t a
D i f fi c u l t t o d e t e r m i n e d u e
M a y b e s a f e r t
h a n l i t h i u m f o r
a n t i c o n v u l -
m a l f o r m a t i o n s
t o c o
n f o u n d i n g e f f e c t s o f
b r e a s t f e e d i n g w o m e n w h o r e q u i r e
s a n t
m a t e
r n a l e p i l e p s y
m o o d s t a b i l i z e
r s ; g e n e r a l l y
c o n t r a i n d i c a t e d

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 5/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 6170 65
sants and rates or clustering of congenital malfor- mation in 414 cases of first trimester exposure 9 .
3.2.2. LactationLong-term follow-up studies on developmental
outcomes of infants exposed to tricyclics through
lactation are limited. These agents are secreted inbreast milk, with a serum to milk ratio approxi-mately equal to 1. Levels in infant serum are variable and sometimes undetectable. Despite alimited database, most reviews support the use of
Žsecondary amine tricyclics nortriptyline and de-.sipramine as first line agents for treatment of
depression in nursing women 12 .
3.2.3. General informationTricyclics are good agents for patients with
proven response but they have more side effectsthan SSRIs. Side effects include dry mouth,blurred vision, constipation, dizziness, cardiacsymptoms, sedation or agitation, and weight gain.These agents can be lethal in an overdose.
3.3. Other antidepressant agents
Monoamine oxidase inhibitors have been asso-ciated with growth retardation, congenitalanomalies and fetal death in animal and humanstudies and are contraindicated in pregnancy. Ad-ditionally, there are no published controlled clini-cal trials involving bupropion, venlafaxine, trazo-
done, or mirtazapine during pregnancy or lac-tation. Animal studies with bupropion haverevealed no evidence of impaired fertility or fetalharm and retrospective analysis in the bupropionpregnancy registry did not show increased fetal
anomalies 18 .
3.4. Alternati e therapies and the nutraceuticals
European double blind placebo controlledŽstudies involving St John’s Wort Hypericum per -
. foratum have demonstrated efficacy in treating
mild-moderate depression but the potency of thepsychoactive substance and contaminants in the various preparations confound these studies.More research is needed in this area. Becausesome women self-medicate with herbal remedies,
assuming them to be ‘natural’ and fail to considerpotential toxicity in pregnancy or lactation, it isimportant for clinicians to inquire about herbalremedies when obtaining clinical histories inchildbearing women.
3.5. Benzodiazepines
The early literature on benzodiazepines sug-gests that they contribute to cleft palate duringfirst trimester exposure though the degree of riskis difficult to determine. The risk of cleft palate inthe general population is approximately 0.064%.In women using benzodiazepines during the firsttrimester, the risk appears to be increased, butstill less than 1% in infants of women who are
exposed 9 . There is evidence for adverse neona-tal syndromes associated with consistent late third
trimester exposure to benzodiazepines, including‘floppy infant syndrome’ with hypotonia, lethargy,and poor temperature regulation.
3.6. Mood stabilizers
Lithium has been well studied in pregnancyand general cardiac anomalies occur in approxi-mately 7% of bipolar women taking lithium. Thedegree of risk of the most common cardiacanomaly, Epstein’s Anomaly, is estimated at 0.1%or 1020 times the rate in the general population.This is much lower than initial estimates from the
International Register of Lithium Babies 19 .Lithium is associated with neonatal morbidity andtoxicity in the neonate and may result from non-toxic maternal levels. Clinical manifestations in-clude hypotonia, hypothyroidism, cyanosis,lethargy, poor sucking, and abnormal reflexes.
Prenatal exposure to valproic acid has beenassociated with a 15% risk of neural tube de-fects. The incidence of neural tube anomalies incarbamazepine exposed children is 0.5% and otheranomalies such as hypoplastic nails and craniofa-
cial anomalies have also been identified 9 . Risk
may be increased with the use of multiple anti-convulsant drugs or higher maternal plasma lev-els. The data on behavioral teratogenicity relatedto anticonvulsant exposure is difficult to interpretbecause the results are complicated by factors

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 6/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 617066
such as parental IQ, impact of seizure disordersin pregnancy, maternal blood levels of anticonvul-
sants, and timing of exposure 9 . A prospectivecontrolled trial demonstrated no adverse neu-robehavioral outcome in exposed children as indi-
cated by IQ and language development 20 . Car-
bamazepine is metabolized more rapidly neona-tally than lithium and may be a safer agent fornursing mothers.
4. Management of depression in pregnancy
Depression that is left untreated or not properlytreated has been shown to negatively impact thehealth and overall functioning of women duringpregnancy and in the postpartum. The followingtreatment guidelines are provided to assist with
proper treatment in this population.
4.1. Step 1 making a diagnosis
Establishing a diagnosis of depression is a criti-cal first step in its treatment. Frequent tearful-ness, irritability or complaints of insomnia areclues that depression screening is necessary.Patients who present with features of depressionfor a period of two weeks or greater and whohave impaired psychosocial functioning warrant a
Ždiagnosis of major depressive disorder see Table.2 . Many women are not forthcoming about their
symptoms and may present with somatic manifes-tations of their illness. Sleep problems, headache,fatigue, gastrointestinal distress, or anxiety arecommon complaints. A comprehensive evaluation
should include thyroid screening, as well as as-sessment for alcohol abuse. Many women who aredepressed may use alcohol to self-medicate theirsymptoms. Other medications including proges-terone containing compounds, cardiac medica-tions, steroids, antihistamines, analgesics, andanticholingergics may induce depressive symp-toms.
4.2. Step 2 determine se erity of illness period of interepisode wellbeing
Many women prefer to remain medication freeduring their pregnancy if their symptoms are notsevere. Patients with only mild impairment of mood, in whom sleep and appetite are unim-paired, and who have reasonable daytimefunctioning and no suicidal ideation would becandidates for non-pharmacologic managementstrategies. Likewise, childbearing women takingantidepressant agents at the time of conceptionmay discontinue them, assuming they are asymp-tomatic, have a long period of inter-episode well-
Table 2 Diagnostic and Statistical Manual of Mental Disorders IV Diagnostic 21 criteria for Major Depressive Episode
[ Fi e or more of the following symptoms that ha e been present for the same 2-week period or longer at least one( ) ( ) ] symptoms is either: 1 depressed mood or 2 loss of interest or pleasure :
Depressed mood most of the day nearly every dayDiminished interest or pleasure in almost all activities most of the day nearly every day
Ž .Significant weight loss more than 5% body wt. when not dieting or significant change in appetite nearly every dayInsomnia or hypersomnia nearly every dayPsychomotor agitation or retardation nearly every dayFatigue or loss of energy nearly every dayFeelings of worthlessness or excessive or inappropriate guilt nearly every dayDiminished ability to think or concentrate or indecisiveness nearly every dayRecurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or specific plan
for committing suicide
The symptoms cause clinically significant distress or impairment in social, occupational or otherimportant areas of functioning
The symptoms are not due to the direct physiological effects of a substance or medical conditionThe symptoms are not better accounted for by bereavement

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 7/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 6170 67
being, and a history of mild illness. Prepregnancyplanning is important in this population so thatdecisions can be made regarding pharmacother-apy. Medications should be weaned, as precipi-tous discontinuation may predispose to relapse.Women who are medication free should be care-
fully followed for recurrence or exacerbation of symptoms during their antenatal visits.
4.3. Step 3 initiating pre ention strategies for women with mild illness
Many therapeutic prevention strategies may beemployed to prevent the exacerbation of minorsymptoms, including a healthy diet free of al-cohol, nicotine, and caffeine. Emphasizing propersleep hygiene, stress management, and exercise
are helpful measures. Mobilizing support systemsmay also be helpful in preventing relapse in women who are single or geographically distantfrom extended family. Individual or conjointtreatment is a very helpful adjunctive strategyespecially when psychosocial stressors exist. Re-ferral for cognitive behavioral therapy, or inter-personal therapy also reduces relapse risk in vul-nerable populations of women with past history of major depression. Close monitoring during ante-natal checks is important, and clinicians shouldproceed with pharmacotherapy, if symptoms be-
come more severe.
4.4. Step 4 pharmacological treatments of major depression
The psychosocial management strategies de-scribed above should always be used as adjunctivestrategies even in women with more severe ill-ness. Women who have moderate to severe illnessimpeding their ability to care for themselvesnutritionally or medically, or who are predisposed
to significant anxiety, insomnia, risk-taking, orsuicidal thinking, are candidates for pharma-cotherapy in pregnancy. Women who have hadsevere episodes of depression that have recurred with medication discontinuation should also con-
tinue pharmacotherapy. Consulting psychiatristsmay be helpful in reassuring women about medi-cations choices and providing or referring foradjunctive services. Full discussion of availableresearch, treatment options, risks of undertreat-ing depression, and benefits of medication are
paramount in pregnancy. Medications should beused at the lowest dose necessary to improvesymptoms, however, increased metabolism inpregnancy may necessitate higher doses relativeto pre-pregnancy.
As stated, the selective serotonin reuptake in-hibitors and the secondary amine tricyclic antide-pressants are preferred agents in pregnancy andappear safe even in the first trimester. Personalor family history of response to a given agentfrequently guides the first choice. Additionally,many women prefer to avoid the side effects of
the tricyclic agents. The selective serotonin reup-take inhibitor fluoxetine has been best studied inpregnancy. Preliminary studies on sertraline,paroxetine, and citalopram are similarly encour-aging without evidence of teratogenicity. Theseshould be considered for women who have previ-ously had good outcomes. The tricyclic antide-pressants nortriptyline and desipramine are goodcandidates for use in pregnancy because theytend to cause less orthostatic hypotension, drymouth and constipation. They should be con-sidered in women who have failed trials with the
SSRIs or with previous good response. Cautionshould be employed in women with severe suici-dal ideation because of the risk of cardiac ar-rhythmias when tricyclics are used in overdose.Weaning tricylic antidepressants prior to the timeof delivery is contraindicated because fetal with-drawal syndromes pose greater risk to the fetusthan extrauterine withdrawal and places the woman at risk for relapse. MAOIs are contraindi-cated in pregnancy. There is limited informationabout pregnancy risks of bupropion, nefazodone,and venlafaxine. Generally patients should be
seen by a physician or contacted by a member of the nursing staff every few weeks until symptomsbegin to remit. Medications should be continuedfor 6 months following delivery to prevent exac-cerbation during the postpartum.

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 8/10

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 9/10
( )S.M. Marcus et al. International Journal of Gynecology & Obstetrics 72 2001 6170 69
ferred in the first trimester because its risk forŽ .Ebstein’s anomaly is relatively remote 0.1% . Ul-
trasound with full fetal survey should be obtainedat 1618 weeks to assess for congenital anomalies when any of the mood stabilizers are used. FolateŽ .4 mgday is also recommended for all women 4
weeks prior to conception and throughout thefirst trimester when the anticonvulsants are used,pediatric teams should be arranged at the time of delivery to optimize neonatal outcomes. Lithiumshould be prescribed in multiple daily dosings toavoid exposing the infant to large variations inblood levels with close monitoring in the thirdtrimester and postpartum due to variations inblood levels. It should generally be continued for612 months following delivery to avoid postpar-tum exacerbation of illness.
5.4. Step 4 treatment resistance and treatment of psychosis
ECT is indicated if rapid reconstitution is es-sential. Psychosis with delusions and commandhallucinations present a psychiatric emergency,and it is this clinical situation which may be apredisposing factor in the disastrous consequenceof suicide or fetal abuse. Hospitalization and theaddition of neuroleptics are always required if the woman and her fetus are at risk.
5.5. Step 5 treatment of bipolar illness in
postpartum
All patients who have bipolar illness need to bemonitored quite closely during the postpartumperiod. For patients who have had previous exac-erbations of bipolar illness during the puer-perium, it is prudent to re-institute the moodstablizer at the time of delivery, as this signifi-cantly reduces the risk of relapse from 50 to 70%to a more modest 1020%. Lithium levels shouldbe closely monitored shortly after delivery be-cause of the risk of toxicity. Breastfeeding is
relatively contraindicated with use of lithium dueto its concentration within the neonate. Carba-mazepine, with its rapid metabolism is slightlypreferred for nursing mothers, although theseinfants should be very closely monitored. Any
evidence of suicidal thinking, hallucinations, voiced concern about harming the infant or disor-ganized thinking about the infant’s health shouldbe viewed as psychiatric emergencies. Hospital-ization, aggressive pharmacotherapy and ECT aretreatments of choice.
6. Referral considerations
Many obstetricians are quite comfortablemanaging uncomplicated major depression. Pri-mary care is the ‘de facto’ mental health systemin the country. Patients who respond well to SS-RIs and tricyclic agents can usually be managedin primary care. Such patients should be moni-tored by physicians and nursing staff every few
Ž weeks until their acute phase symptoms sleep,.
appetite, mood have resolved. Compliance withmedication is also important to monitor as over50% of patients discontinue medication withinthe first month. Refractory illness or complex bipolar disorder may require psychiatric consulta-tion. In women who have active suicidality, ahistory of psychosis, emerging symptoms of disor-ganized thinking, or hallucinations or delusions,referral for psychiatric management is recom-mended and hospitalization is often required.
ŽOther co-morbid problems eating disorders, sub-.stance abuse, panic disorder with agoraphobia or
persistent psychosocial problems also frequently
require more formalized mental health treat-ments.
7. Conclusions
All psychotropic agents freely cross the placen-tal barrier and expose the fetus to those medica-tions; therefore, the risks of untreated psychiatricillness must always be balanced with the risk of fetal or infant exposure. While some moodstabilizers may increase the absolute risk for ter-
atogenicity, that risk should be considered in theentire context of the woman’s illness and theadverse consequences of untreated depression.
Further study is essential to elucidate risk fac-tors that predispose women to relapse with dis-

8/12/2019 Treatment Guidelines for Depression in Pregnancy
http://slidepdf.com/reader/full/treatment-guidelines-for-depression-in-pregnancy 10/10