-
7/31/2019 Treatment efficiency of conventional vs
selfligaton
1/5
ORIGINAL ARTICLE
Treatment efficiency of conventionalvs self-ligating brackets:
Effects of
archwire size and materialNicholas R. Turnbull and David J.
Birnie
Portsmouth, Hampshire, United Kingdom
Introduction: In this prospective clinical study, we assessed
the relative speed of archwire changes,
comparing self-ligating brackets with conventional elastomeric
ligation methods, and further assessed this
in relation to the stage of orthodontic treatment represented by
different wire sizes and types. Methods: The
time taken to remove and ligate archwires for 131 consecutive
patients treated with either self-ligating or
conventional brackets was prospectively assessed. The study was
carried out in the orthodontic department
of a district general hospital in the United Kingdom. The main
outcome measure was the time to remove or
place elastomeric ligatures or open/close self-ligating brackets
for 2 matched groups of fixed appliance
patients: Damon2 self-ligating bracket (SDS Ormco, Orange,
Calif) and a conventional mini-twin bracket(Orthos, SDS Ormco). The
relative effects of various wire sizes and materials on ligation
times were
investigated. The study was carried out by 1 operator
experienced in the use of self-ligating and conventional
brackets. Results: The Damon2 self-ligating system had a
significantly shorter mean archwire ligation time
for both placing (P .001) and removing (P .01) wires compared
with the conventional elastomeric system.
Ligation of an archwire was approximately twice as quick with
the self-ligating system. Opening a Damon
slide was on average 1 second quicker per bracket than removing
an elastic from the mini-twin brackets, and
closing a slide was 2 seconds faster per bracket. This
difference in ligation time between the Damon2 and
the conventional mini-twin brackets became more marked for
larger wire sizes used in later treatment stages.
Conclusions: The type of bracket and the size of wire used are
statistically significant predictors for speed
of ligation and chairside time. The self-ligating system offered
quicker and arguably more efficient wire
removal and placement for most orthodontic treatment stages. (Am
J Orthod Dentofacial Orthop 2007;131:
395-99)
The reported advantages of self-ligating (SL)
brackets include reduced friction,1-4 full and
secure wire ligation,5 improved oral hygiene,6,7
anchorage conservation,8 chairside time savings and
improved ergonomics,6,9-11 quicker treatment times,
and longer appointment intervals.10,12 The issue of
friction and SL brackets is controversial. Many labora-
tory studies indicated lower friction levels for SL
brackets, but their experimental designs were variable
and might not simulate the dynamics of the oral
environment.
13
However, in this study, we were pri-marily concerned with other
characteristics of SL
brackets. Modest savings in chairside time were re-
ported by Harradine10 using the Damon SL bracket
(SDS Ormco, Orange, Calif). However, Berger and
Byloff 9 found more significant reductions in wire
ligation times with the SPEED SL bracket (Strite
Industries, Cambridge, Ontario, Canada), but they as-
sessed exclusively nonextraction patients and only 1
wire type.
The aim of this study was to assess archwire
ligation times for patients with various archwire sizes
and materials that represented a cross-section of orth-
odontic treatment progress. In this way, the effects of
varying the wire size and material were recorded in 2groups of
patients, allowing comparison of an SL
bracket14 with a conventional mini-twin design.
SUBJECTS AND METHODS
The Damon2 (D2) self-ligating bracket (SDS Ormco)
was compared with a conventional mini-twin bracket
(Orthos, SDS Ormco). The D2 bracket ligates the
archwire with a vertical metal slide that can be opened
or closed to cover or expose the slot (Fig 1). This is a
passive bracket because the wire is not engaged by an
active clip; Harradine15 wrote an excellent summary of
From the Orthodontic Department, Queen Alexandra Hospital,
Portsmouth,
Hampshire, United Kingdom.
Consultant orthodontist.
Reprint requests to: Nicholas R. Turnbull, Orthodontic
Department, Queen
Alexandra Hospital, Portsmouth, Hampshire PO6 3LY, United
Kingdom;
e-mail, [email protected].
Submitted, January 2005; revised and accepted, July 2005.
0889-5406/$32.00
Copyright 2007 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2005.07.018
395
-
7/31/2019 Treatment efficiency of conventional vs
selfligaton
2/5
the advantages and disadvantages of SL brackets with
passive or active clips. A special tool (Damon plier) is
used to open and close the D2 slide mechanism.
The time taken to open or close the D2 slides or
remove or replace ligatures on the Orthos bracket was
measured for 140 D2 bonded arches compared with 122
mini-twin bonded arches. This was performed by 1
operator (N.R.T.) with significant experience with both
the D2 bracket and the Orthos (current practice, 60%
D2 and 40% Orthos). Consecutive patients who ful-
filled the following criteria were included in the study:
scheduled for maxillary and mandibular fixed appli-
ances, agreed to take part in the study, age between 11
and 18 years, and due for archwire changes at the
assessment visit. Patients with cleft lip and palate,severe
skeletal dysgnathia, and ectopic canines were
excluded because they were to likely represent unusual
outliers in time taken to manipulate archwires.
Times were recorded with a stopwatch, with the
clinician working at a normal rate. A specially designed
proforma recorded sex, age, extraction or nonextrac-
tion, time taken to remove or place archwire, arch
(maxillary or mandibular), number of brackets en-
gaged, number of tubes or bands engaged, and wire size
and material.
The patients represented a balance in terms of
extraction and nonextraction in each group. In mostpatients, the
second molars had already been bonded.
Because the clinician had a wide spread of patients in
treatment, it was possible to record ligation times at
various stages of treatment progress so that the full
range of wire sizes was assessed. For statistical analy-
sis, the archwires used were divided into 4 main groups
based on wire size and material (Table I).
To standardize the study as much as possible, a
careful protocol was followed. The time required to
remove or place auxiliaries such as power chain was
not included in the total time recorded. Figure-eight
elastics and metal tie ligatures were not used. All slides
for the D2 brackets were opened to site the archwire
(the wires were not pushed through the closed premolar
brackets as is occasionally possible with the system).
Statistical analysis
The statistical evaluation of the data included anal-
ysis of variance (ANOVA), ttest, and 95% confidence
intervals (CI) for difference of the means. The statisti-
cal software package used was Stats Direct Ltd (Sale,
Cheshire, United Kingdom).
RESULTS
The 2 patient groups (D2 and Orthos) demonstrated
good demographic matching; girls represented 56% of
D2 group and 59% of the Orthos group. The mean ages
were 13.7 years for the D2 group and 14.4 years for the
Orthos group. The ratios of extraction to nonextraction
patients were 39% extraction for the D2 group and 43%extraction
for the Orthos group.
The time taken for ligating or removing wires was
expressed as mean units of time (seconds) per bonded
arch and per bracket. Overall, it was quicker to remove
wires than to replace them. This was evident with both
bracket types, but much more significant in the Orthos
patients; the mean wire removal time for the Orthos
brackets was 64.5 seconds per bonded arch (SD 18),
compared with 98.4 seconds (SD 24) for wire
placement. A smaller difference was observed for the
D2 brackets (Table II).
When the different wire sizes were combined, themean time to
open slides for the D2 patients per bracket
was 3.7 seconds compared with 4.7 seconds for elastic
ligature removal with the Orthos brackets (Table II).
This difference of 1 second per bracket was statistically
significant when comparing the 2 groups as a whole
(P .01). The 95% CI for the difference between the
per-bracket means was 0.28-1.77. Assessment of the
effect of the 4 wire subgroups also showed significant
differences in time taken for archwire removal between
the D2 and Orthos brackets. The greatest difference
was found for larger wire sizes; it took a mean time of
Fig 1. D2 SL brackets.
Table I. Four archwire groups used in study, based on
wire size and material
Wire
group Wire type
Wire sizes
( 1100 in)
1 Round nickel-titanium 14, 16, 18
2 Small rectangular nickel-titanium 14 25, 16 25,
16 22
3 Large rectangular nickel-titanium 18 25, 19 25
4 Rectangular stainless steel 18 25, 19 25
American Journal of Orthodontics and Dentofacial Orthopedics
March 2007
396 Turnbull and Birnie
-
7/31/2019 Treatment efficiency of conventional vs
selfligaton
3/5
1.6 seconds longer per bracket to remove elastic liga-
tures compared with opening the D2 slides for wire
group 4 (Table III). T h e smallest nickel-titanium
wires (group 1) had a small difference in wire
removal time between the 2 bracket types, but this
was not statistically significant. There was no differ-
ence in time taken for removing maxillary vs man-dibular
archwires for either the D2 or the Orthos
patients.
When closing the D2 slides, the mean time per
bracket was 5.7 seconds, compared with 7.6 seconds
for Orthos ligation (P .001). The mean ligation
times were 46.3 seconds (SD 22) for a fully
bonded arch for D2 and 98.4 seconds (SD 24) for
the Orthos brackets. Unpaired t tests showed these
differences to be highly statistically significant (t
3.55; P .001) when comparing the 2 bracket types
as a whole (Table II). The 95% CI for the difference
between the means was 20.3 to 5.8. The CI value
does not include zero, which indicates a true differ-
ence in the mean ligation times between the 2 bracket
systems. For closing slides/religating elastics (ligat-
ing wires), the type of archwire had a significant
effect. The D2 brackets had shorter ligation times for
all wire groups and were statistically significant for
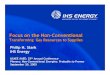
wire groups 2, 3, and 4 (Table III). This is clearly
illustrated inFigure 2by the separation of the plotted
lines for the 2 bracket systems. It also shows that the
relative differences in ligation times are more
marked for the larger wire sizes in both nickel-titanium and
stainless steel.
Comparison of the maxillary arch with the mandib-
ular arch showed no difference in wire ligation times
for the Orthos brackets for any wire size. However, in
the D2 group, the ligation time (placing wires) was
significantly slower in the manidbular arch for wire
group 1 (small round nickel-titanium). The mean times
to ligate a round nickel-titanium wire per bracket were
9.1 seconds in the mandibular arch and 6.5 seconds in
the maxillary arch. However, this was only marginally
statistically significant (P .041).
Fig 2. Interaction plot of 4 wire groups for time taken to
close slides/replace ligatures (mean time per bracket in
seconds); note clear separation of 2 time lines for
Orthos and D2 brackets, showing relatively greater
difference as wire size increases (see Table I for wire
group details).
Table II. Mean wire removal and ligation times in seconds (SD)
per bonded arch and per bracket for all wire size
groups combined for D2 vs Orthos brackets. Wire removal
represents opening D2 slides or removal of elastomeric
rings, wire ligation represents closing D2 slides or replacing
new elastic rings
D2 Orthos
Arch
Bracket
Arch
Bracket Difference Significance(n 140) (n 122)
Wire removal 39.8 (13) 3.7 (1.1) 64.5 (18) 4.7 (0.9) 24.7 *
Wire ligation 46.3 (22) 5.7 (2.3) 98.4 (24) 7.6 (1.2) 52.1
*Means different at P .01; means different at P .001.
Table III. Mean times (seconds) for wire removal or
ligation per bracket for different wire sizes (see Table I
for wire sizes), wire removal represents opening D2
slides or removal of elastomeric rings, wire ligation
represents closing D2 slides or replacing new elasticrings
D2 Orthos
Wire group
Mean time
per bracket
Mean time
per bracket Difference Significance
Wire removal
1 3.8 (n 38) 4.2 (n 31) 0.4 NS
2 3.9 (n 31) 4.9 (n 33) 1.0 *
3 3.6 (n 39) 4.8 (n 30) 1.2
4 3.6 (n 32) 5.2 (n 28) 1.6
Wire ligation
1 7.8 (n 38) 8.7 (n 31) 0.9 NS
2 6.5 (n
31) 8.2 (n
33) 1.7
3 4.4 (n 39) 7.1 (n 30) 2.7
4 4.1 (n 32) 6.4 (n 28) 2.3
NS, no significant difference; *means different at P .05;
means
different at P .01; means different at P .001.
American Journal of Orthodontics and Dentofacial Orthopedics
Volume 131, Number3
Turnbull and Birnie 397
-
7/31/2019 Treatment efficiency of conventional vs
selfligaton
4/5
DISCUSSION
The time taken to remove or ligate orthodontic
wires is of interest but is a less significant
characteristic
of SL systems when compared with secure ligation and
the possibility of lower friction/force generation.
Nev-ertheless, the ergonomics of archwire manipulation in a
busy clinical environment is important.
For both the D2 and Orthos brackets, it was quicker
to remove wires than to replace them. However, Maijer
and Smith11 found the opposite using the Activa SL
bracket (A Company, San Diego, Calif), which had a
slightly quicker ligation time. A common initial finding
with the D2 bracket is difficulty in opening the
slidesa time-consuming wire removal process
whereas closing slides is relatively simple. It is possible
that the Activa bracket also had similar time-consuming
opening characteristics. However, our study suggeststhat wire
removal is slightly quicker than placement
for both bracket types. This is most likely due to the
experience and comfort zone of the operator in D2
slide manipulation. Use of 1 operator removed the
potential interoperator variability in experience lev-
els with the 2 bracket systems. To compare like with
like, the operator needed to be at least as comfortable
with the D2 bracket as the Orthos bracket. This
allowed isolation of bracket type as the determinant
of outcome rather than variation in clinical experi-
ence. A follow-up study will assess effects of the
clinical experience on ligation time by comparingdental
students, postgraduate trainees, and estab-
lished specialists.
The ligation times show mean savings of 2 seconds
per bracket for closing slides with the D2 system, and
1 second per bracket for opening slides when compared
with the Orthos elastics. These time savings are more
significant than those reported by Harradine.10 The
mean time for wire placement in a fully bonded arch
with the D2 system was 46 seconds compared with 98
seconds for the Orthos brackets. The difference be-
tween the 2 bracket types was statistically significant
for both placing and removing wires, but is thisclinically
significant?
It took approximately twice as long to ligate a wire
by using the elastics and Orthos brackets compared
with the D2 system. The average time saved with the
D2 was about 1.3 minutes per visit. This is approxi-
mately a 10% time saving in an average wire adjust-
ment appointment. In the United Kingdoms National
Health Service, a 10 to 15 minute archwire change
appointment is commonly allocated as standard. If the
time is extended to a full day, a 10% saving could free
up an extra 45 to 60 minutes of clinical time. This could
be used to reinforce oral hygiene measures, discuss
treatment progress, or generally enhance patient or
parent relationships through improved communication.
The D2 brackets offer relatively greater time sav-
ings for larger wire sizes. This can be seen clearly inFigure 2,
which represents the mean ligation times of
the 4 wire-size groups. The 2 lines plotted on the chart
diverge as wire sizes increase, indicating less time to
ligate wires with both bracket types, but proportionally
a greater drop in ligation time for the D2 system.
Therefore, time-saving efficiencies appear to be rela-
tively greater for the D2 brackets at later treatment
stages, associated with larger wires when alignment of
the teeth has progressed. This is explained by the
Damon treatment philosophy16 that stresses full en-
gagement of all teeth at the earliest stage. Therefore, it
will take relatively more time to fully engage light
nickel-titanium archwires in all teeth with the D2
system compared with bypassing selected teeth with a
conventional elastomeric appliance. Similarly, the dif-
ference in ligation time for the maxillary vs the man-
dibular arch was found to be significant only in the D2
group and only for small round nickel-titanium wires
(initial alignment). It was statistically significantly
quicker to ligate a wire in the maxillary arch in this
group. This is most likely due to the generally more
severe crowding in the mandibular arch, smaller inter-
bracket distances in the mandibular incisor region, and
attempts to initially fully ligate all teeth with the D2
system.The decreased reliance on assistant support with SL
brackets produces hidden efficiency savings, which are
potentially greater for orthodontic therapists who gen-
erally do not have chairside support from dental assis-
tants; this is required for speedy and efficient elastic
ligation. Chairside time savings are welcome, but other
advantages of SL systems, such as decreased treatment
duration10,12 and absence of bio-hostable elastic mod-
ules5,7 are probably more important. However, an
understated advantage is the absence of the need for
passing, placing, and removing elastomeric ringsa
labor-intensive, tedious, and ergonomically unsatisfac-tory
process.
SL brackets are more expensive than most conven-
tional brackets, but this cost can be offset by the
reductions in chairside time9,11 and treatment dura-
tion.10,12 There is also the small financial saving related
to elastomeric rings that are obviously not required.
The D2 bracket is not difficult to open and close,
but it requires a sustained learning period to become
comfortable and skilled in manipulation of the bracket
slide. There are more new brackets on the market with
modified and novel SL mechanisms. Some of these will
American Journal of Orthodontics and Dentofacial Orthopedics
March 2007
398 Turnbull and Birnie
-
7/31/2019 Treatment efficiency of conventional vs
selfligaton
5/5
probably be more efficient than others. In this study, we
compared the D2 bracket with the Orthos design. The
Orthos was used because it approximates the size of the
D2 bracket and because larger size standard/regular
twin brackets are less commonly used in the UnitedKingdom. It is
theoretically possible that wing size
could affect elastomeric ligation time, with smaller
wings more difficult to ligate. Therefore, the time
savings found in this study relate to a comparison with
mini-twin brackets.
CONCLUSIONS
The D2 SL brackets had significantly quicker mean
archwire ligation times for both placing and removing
wires compared with the conventional Orthos system.
Ligation of wires was twice as quick with the D2
system. The average time savings was almost 1.5
minutes of clinical activity per patient contact. In terms
of clinical time, SL brackets are more efficient for most
wire sizes and therefore at most stages of orthodontic
treatment. However, the improvement in ligation time
became more marked and statistically significant for the
larger archwire sizes used later in treatment. Therefore,
both the type of bracket and the size of the wire appear to
be significant predictors for speed of ligation andchairside
time.
We thank Bernie Higgins, Portsmouth Institute of
Medicine, Health and Social Care, University of Ports-
mouth, for help with statistics.
REFERENCES
1. Read-Ward GE, Jones SP, Davies EH. A comparison of self-
ligating and conventional orthodontic bracket systems. Br J
Orthod 1997;24:309-17.
2. Henao SP, Kusy RP. Evaluation of the frictional resistance
of
conventional and self-ligating bracket designs using
standardized
archwires and dental typodonts. Angle Orthod 2004;74:202-11.
3. Khambay B, Millett D, McHugh S. Evaluation of methods of
archwire ligation on frictional resistance. Eur J Orthod
2004;26:
327-32.4. Thorstenson BS, Kusy RP. Comparison of resistance to
sliding
between different self-ligating brackets with second-order
angu-
lation in the dry and saliva states. Am J Orthod Dentofacial
Orthop 2002;121:472-82.
5. Taloumis LJ, Smith TM, Hondrum SO, Lorton L. Force decay
and deformation of orthodontic elastomeric ligatures. Am J
Orthod Dentofacial Orthop 1997;111:1-11.
6. Shivapuja PK, Berger J. A comparative study of
conventional
ligation and self-ligation bracket systems. Am J Orthod
Dento-
facial Orthop 1994;106:472-80.
7. Forsberg CM, Brattstrom V, Malmberg E, Nord CE. Ligature
wires and elastomeric rings: two methods of ligation, and
their
association with microbial colonization of Streptococcus
mutans
and lactobacilli. Eur J Orthod 1991;13:416-20.
8. Pilon JGM, Kuijpers-Jagtman AM, Maltha JC. Magnitude
oforthodontic forces and rate of bodily tooth movement. An
experimental study. Am J Orthod Dentofacial Orthop 1996;110:
16-23.
9. Berger J, Byloff FK. The clinical efficiency of
self-ligated
brackets. J Clin Orthod 2001;35:304-8.
10. Harradine NWT. Self-ligating brackets and treatment
efficiency.
Clin Orthod Res 2001;4:220-7.
11. Maijer R, Smith DC. Time savings with self-ligating
brackets.
J Clin Orthod 1990;24:29-31.
12. Eberting JJ, Straja SR, Tuncay OC. Treatment time,
outcome,
and patient satisfaction comparisons of Damon and
conventional
brackets. Clin Orthod Res 2001;4:228-34.
13. Braun S, Bluestein M, Moore BK, Benson G. Friction in
perspective. Am J Orthod Dentofacial Orthop 1999;115:619-27.
14. Damon DH. The Damon low-friction bracket: a biologically
compatible straight-wire system. J Clin Orthod
1998;32:670-80.
15. Harradine NW. Self-ligating brackets: where are we now?
J Orthod 2003;30:262-73.
16. Damon DH. The rationale, evolution and clinical application
of
the self-ligating bracket. Clin Orthod Res 1998;1:52-61.
American Journal of Orthodontics and Dentofacial Orthopedics
Volume 131, Number3
Turnbull and Birnie 399