Embed Size (px)
Citation preview
12/16/2010
1
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Treatment Advances in Waldenstrom’s Macroglobulinemia
Steve Treon MD, MA, PhD
Director, Bing Center for WM
Associate Professor
Dana Farber Cancer Institute
Harvard Medical School
Advances in the Biology of Waldenstrom’s Macroglobulinemia
6th International Workshop on Waldenström’s Macroglobulinemia
Venice, Italy • October 6-10, 2010www.wmworkshop.org

12/16/2010
2
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Case PresentationThis 63 year old went for a routine physical examand was found to have an elevated total protein.An IgM monoclonal spike was discovered, andhis total serum IgM level was 4,010 mg/dL.Hematocrit was 37.9%. A bone marrow biopsyshowed 30% involvement with LPC. He wass owed 30% vo ve e t w t C. e wasdiagnosed with WM and placed on watch andwait.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Case PresentationOne year later his IgM is 4,820 mg/dL, hematocrit is35 1% H h f ti bl d d i h i35.1%. He has more fatigue, nosebleeds, and is hearing“tree frogs”. He also is experiencing numbness andtingling in his feet. Exam shows “plump retinal vessels”.Neurological exam shows diminished sensation to touchover his soles. Fat pad biopsy with congo red staining isnegative. Anti-MAG IgM antibody screen is positive withtiter >102,400. He undergoes plasmapheresis andreports improvement in his neuropathy, and also stateshis “thinking” has improved.
12/16/2010
3
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Case PresentationWhat is the most appropriate course of action for this patient?pp p p
1. Continue watch and wait2. Gabapentin or Pre-Gabapentin for symptomatic relief3. Continue with periodic plasmapheresis4. Treat with rituximab alone5. Treat with cyclophosphamide based rituximab therapy (CPR or RCD)6. Treat with fludarabine or cladribine based rituximab therapy7. Treat with bortezomib based rituximab therapy (BDR or VR)8 Treat with bendamustine plus rituximab8. Treat with bendamustine plus rituximab
Advances in the Biology of Waldenstrom’s Macroglobulinemia
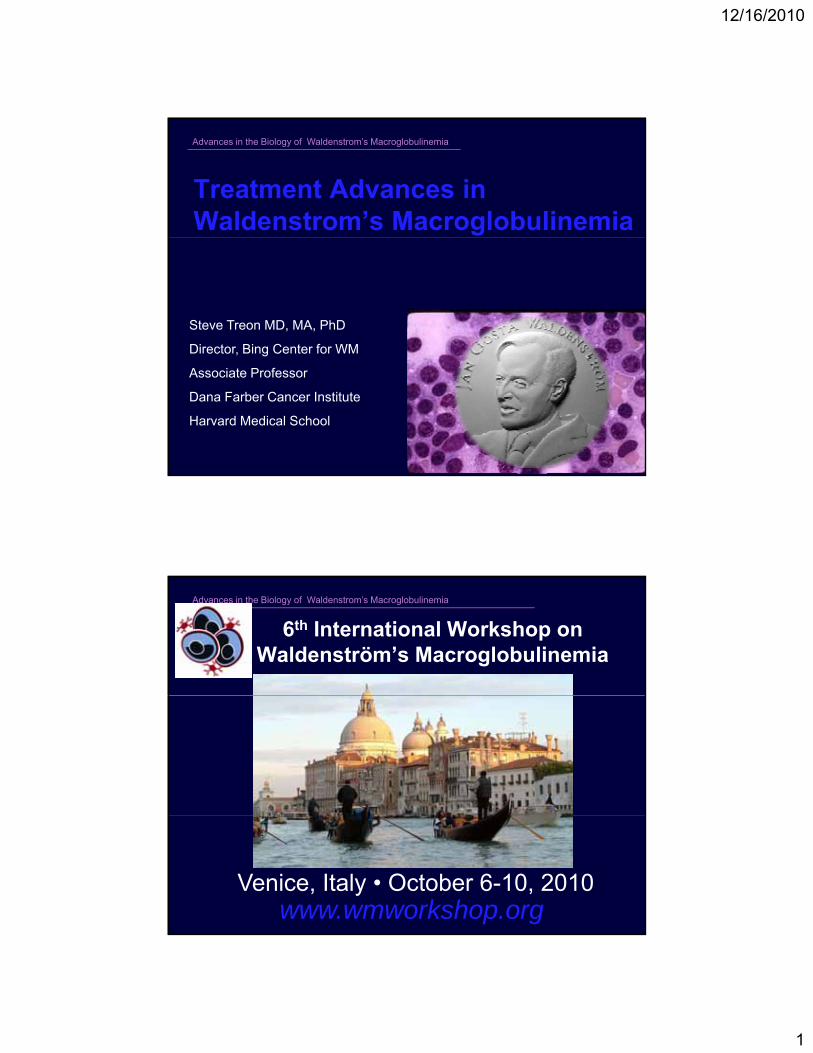
Clinicopathological Manifestations of WM
HCT PLT WBC
Adenopathy, l l
HCT, PLT, WBCHyperviscositySyndrome:Epistaxis, HA,Impaired vision
>4.0 CP
splenomegaly ≤15% IgM Neuropathy (~20%)
Cryoglobulinemia (<5%)Cold Agglutinemia (<10%)Fatigue, Constitutional Sxs
Cytokinemia?
Treon SP et al. Cancer Treat Res. 2008;142:211-242.
12/16/2010
4
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Anemia in Waldenstrom’s macroglobulinemia
Bone marrow replacementBone marrow replacement
Hemodilution (high IgM levels)
Hemolysis (cold agglutinin; warm antibody)
Therapeutic injury (nucleoside analogue mediated hemolysis; MDS)hemolysis; MDS)
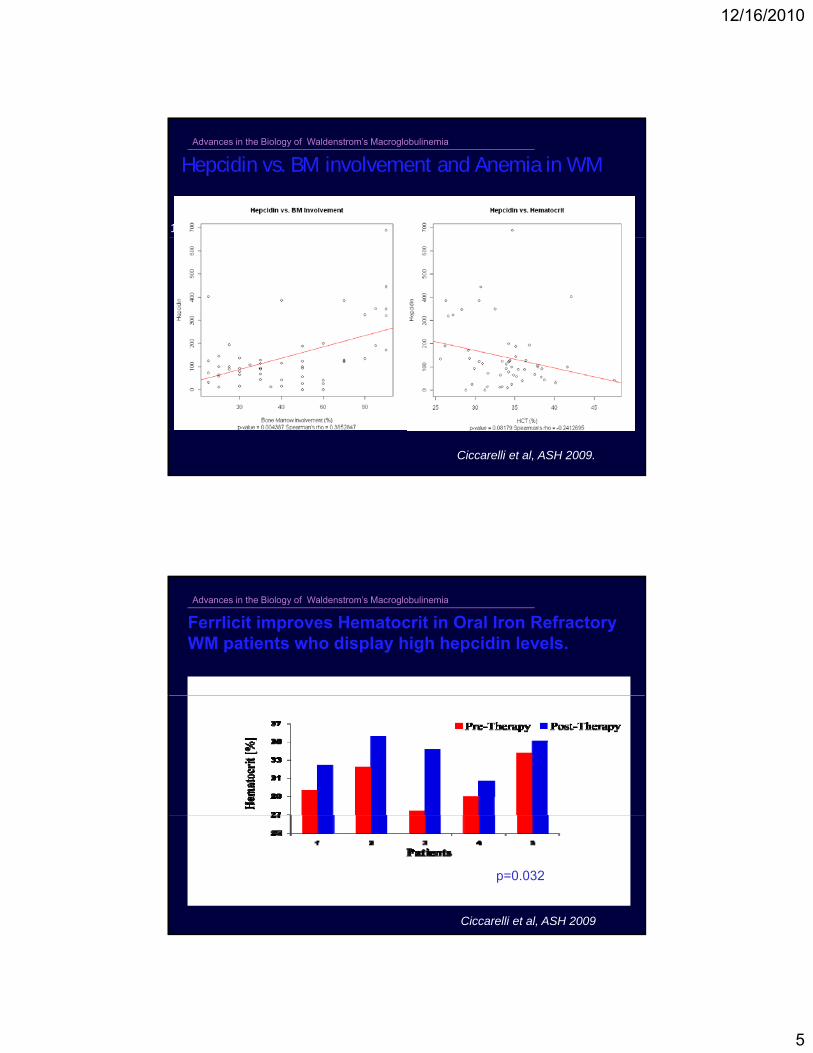
Iron deficiency (Hepcidin)
Advances in the Biology of Waldenstrom’s Macroglobulinemia
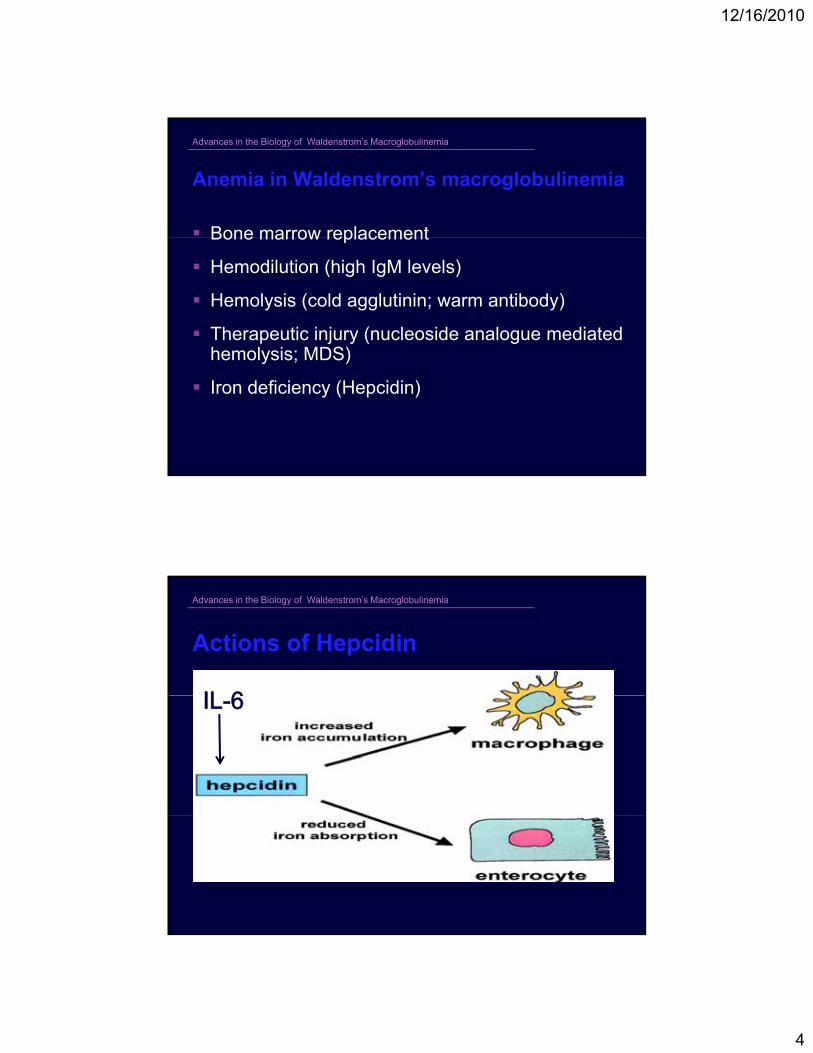
Actions of Hepcidin
12/16/2010
5
Advances in the Biology of Waldenstrom’s Macroglobulinemia
1. 2.
Hepcidin vs. BM involvement and Anemia in WM
Ciccarelli et al, ASH 2009.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Ferrlicit improves Hematocrit in Oral Iron Refractory WM patients who display high hepcidin levels.
p=0.032
Ciccarelli et al, ASH 2009

12/16/2010
6
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Consensus Panel Recommendations for Initiation of Therapy in WM Hb ≤ 10 g/dL on basis of diseaseHb ≤ 10 g/dL on basis of disease
PLT < 100,000 mm3 on basis of disease
Symptomatic hyperviscosity (> 4.0 cp)
Moderate to severe peripheral neuropathy
Symptomatic cryoglobulinemia, cold agglutinemia, y p y g , gg ,amyloidosis, or symptomatic autoimmune related events on the basis of disease
Kyle RA, et al. Semin Oncol. 2003;30:116-120.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
First published report of response to rituximab in WM
Semin Oncol. 1999; 26:97-106.
12/16/2010
7
Advances in the Biology of Waldenstrom’s Macroglobulinemia
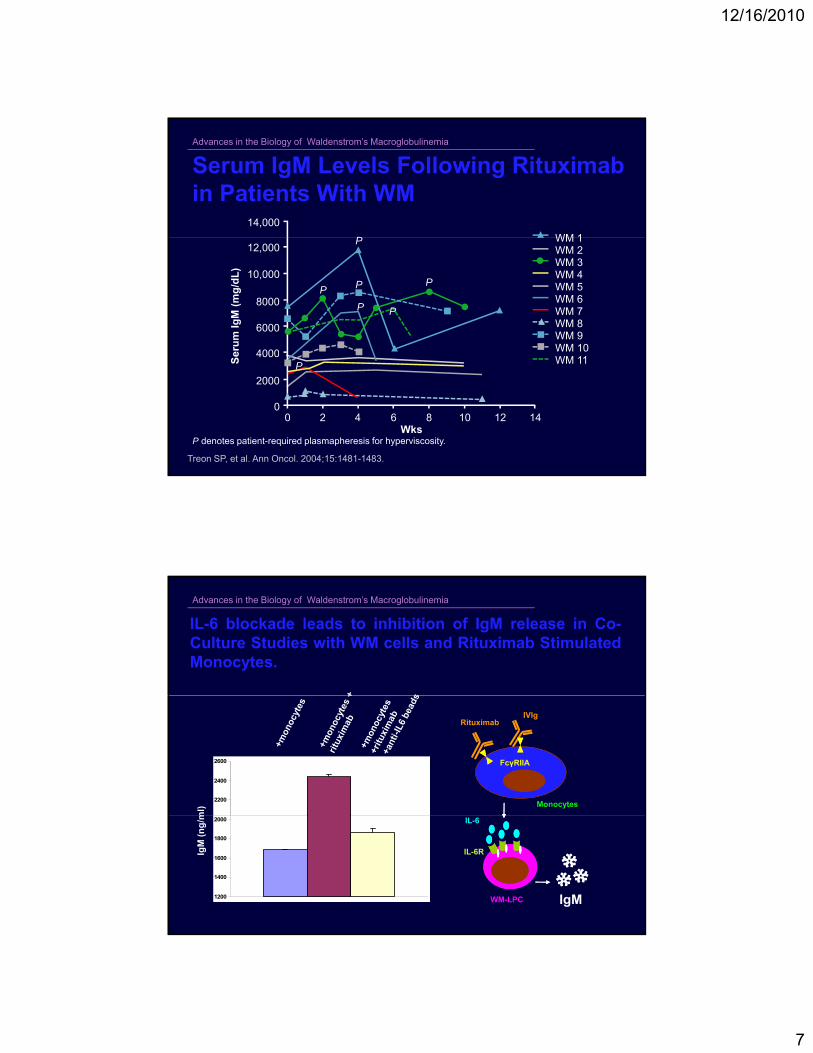
Serum IgM Levels Following Rituximabin Patients With WM
14,000
WM 1P12,000
eru
m Ig
M (
mg
/dL
)
10,000
8000
6000
4000
WM 1WM 2WM 3WM 4WM 5WM 6WM 7WM 8WM 9WM 10WM 11
P
P
P
PP
P
Treon SP, et al. Ann Oncol. 2004;15:1481-1483.
P denotes patient-required plasmapheresis for hyperviscosity.
00 2 4 6 8 10
Wks
S
4000
2000
12 14
WM 11P
Advances in the Biology of Waldenstrom’s Macroglobulinemia
IL-6 blockade leads to inhibition of IgM release in Co-Culture Studies with WM cells and Rituximab StimulatedMonocytes.
2200
2400
2600
ml) Monocytes
FcγRIIA
RituximabIVIg
1200
1400
1600
1800
2000
IgM
(n
g/m IL-6
WM-LPC
IL-6R
IgM
12/16/2010
8
Advances in the Biology of Waldenstrom’s Macroglobulinemia
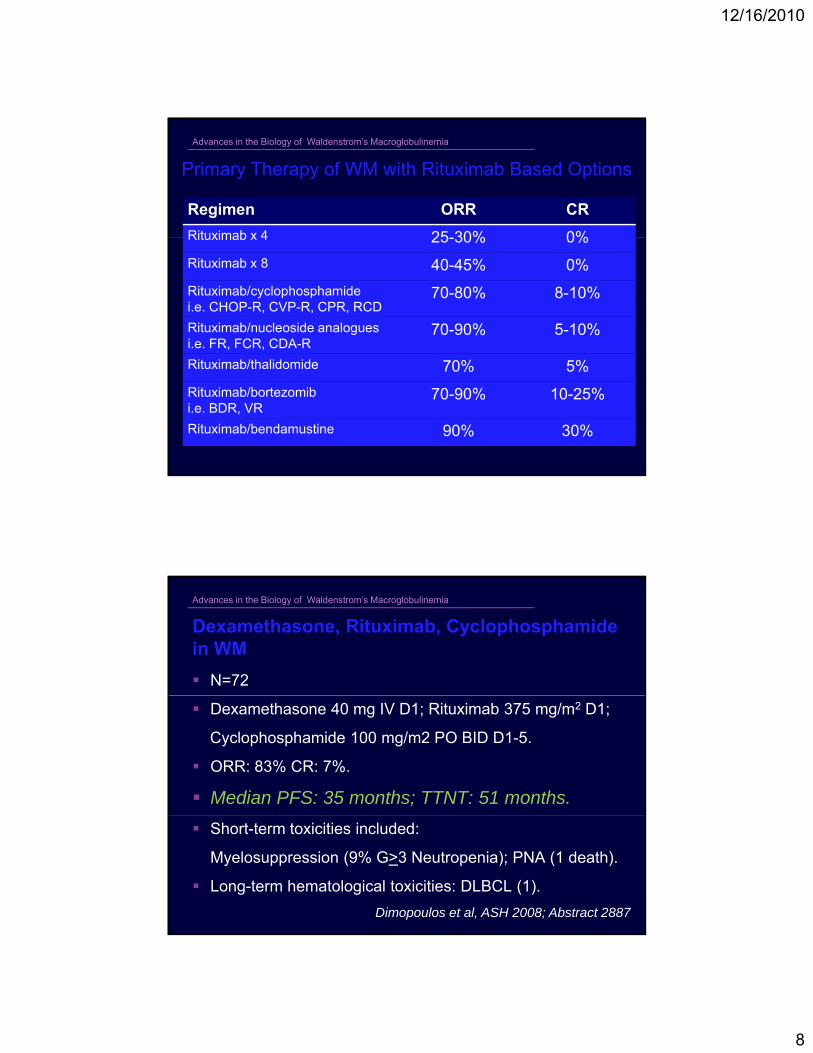
Primary Therapy of WM with Rituximab Based Options
Regimen ORR CR
Rituximab x 4 25 30% 0%Rituximab x 4 25-30% 0%
Rituximab x 8 40-45% 0%
Rituximab/cyclophosphamidei.e. CHOP-R, CVP-R, CPR, RCD
70-80% 8-10%
Rituximab/nucleoside analoguesi.e. FR, FCR, CDA-R
70-90% 5-10%
Rituximab/thalidomide 70% 5%
Rituximab/bortezomibi.e. BDR, VR
70-90% 10-25%
Rituximab/bendamustine 90% 30%
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Dexamethasone, Rituximab, Cyclophosphamidein WM
N=72
Dexamethasone 40 mg IV D1; Rituximab 375 mg/m2 D1;
Cyclophosphamide 100 mg/m2 PO BID D1-5.
ORR: 83% CR: 7%.
Median PFS: 35 months; TTNT: 51 months.
Short-term toxicities included:
Myelosuppression (9% G>3 Neutropenia); PNA (1 death).
Long-term hematological toxicities: DLBCL (1).
Dimopoulos et al, ASH 2008; Abstract 2887
12/16/2010
9
Advances in the Biology of Waldenstrom’s Macroglobulinemia
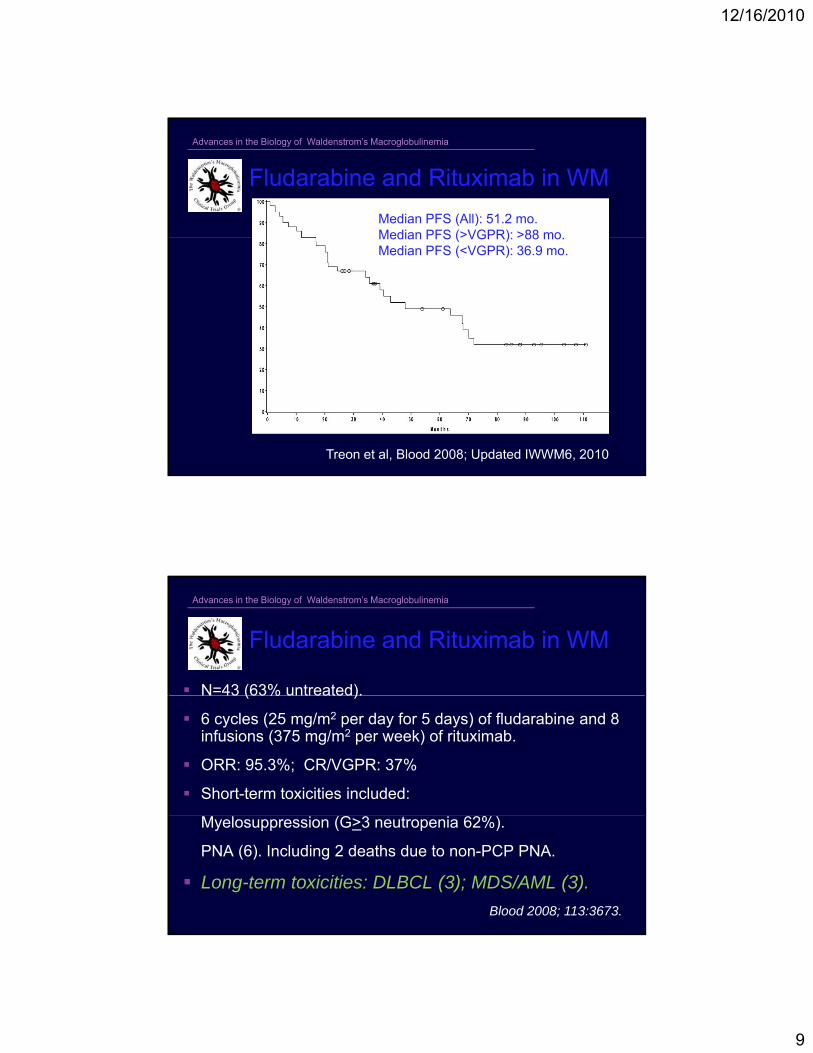
Fludarabine and Rituximab in WM
Median PFS (All): 51.2 mo.Median PFS (>VGPR): >88 moMedian PFS (>VGPR): >88 mo.Median PFS (<VGPR): 36.9 mo.
Median Follow-up: 50.6 months
Treon et al, Blood 2008; Updated IWWM6, 2010
Advances in the Biology of Waldenstrom’s Macroglobulinemia
N=43 (63% untreated).
Fludarabine and Rituximab in WM
N 43 (63% untreated).
6 cycles (25 mg/m2 per day for 5 days) of fludarabine and 8 infusions (375 mg/m2 per week) of rituximab.
ORR: 95.3%; CR/VGPR: 37%
Short-term toxicities included:
Myelosuppression (G>3 neutropenia 62%).
PNA (6). Including 2 deaths due to non-PCP PNA.
Long-term toxicities: DLBCL (3); MDS/AML (3).
Blood 2008; 113:3673.
12/16/2010
10
Advances in the Biology of Waldenstrom’s Macroglobulinemia
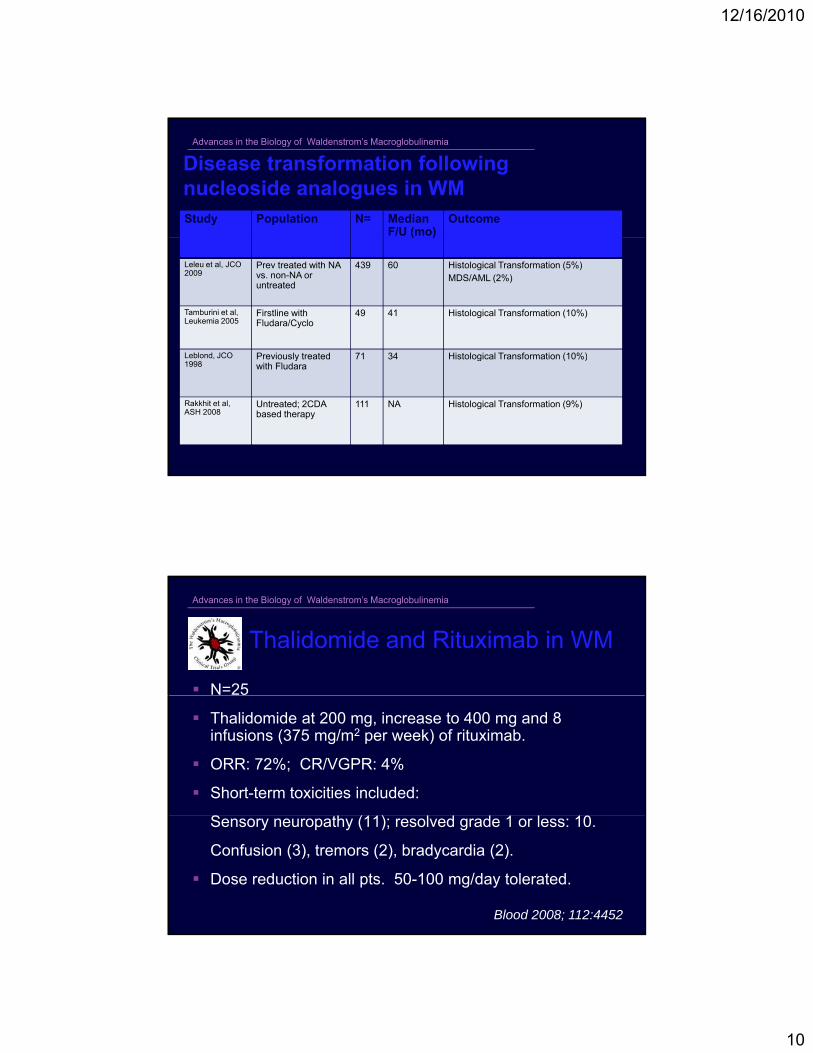
Disease transformation following nucleoside analogues in WMStudy Population N= Median
F/U (mo)Outcome
( )
Leleu et al, JCO 2009
Prev treated with NA vs. non-NA or untreated
439 60 Histological Transformation (5%)MDS/AML (2%)
Tamburini et al, Leukemia 2005
Firstline with Fludara/Cyclo
49 41 Histological Transformation (10%)
Leblond JCO Previously treated 71 34 Histological Transformation (10%)Leblond, JCO 1998
Previously treated with Fludara
71 34 Histological Transformation (10%)
Rakkhit et al, ASH 2008
Untreated; 2CDA based therapy
111 NA Histological Transformation (9%)
Advances in the Biology of Waldenstrom’s Macroglobulinemia
N=25
Thalidomide and Rituximab in WM
Thalidomide at 200 mg, increase to 400 mg and 8 infusions (375 mg/m2 per week) of rituximab.
ORR: 72%; CR/VGPR: 4%
Short-term toxicities included:
Sensory neuropathy (11); resolved grade 1 or less: 10.
Confusion (3), tremors (2), bradycardia (2).
Dose reduction in all pts. 50-100 mg/day tolerated.
Blood 2008; 112:4452
12/16/2010
11
Advances in the Biology of Waldenstrom’s Macroglobulinemia
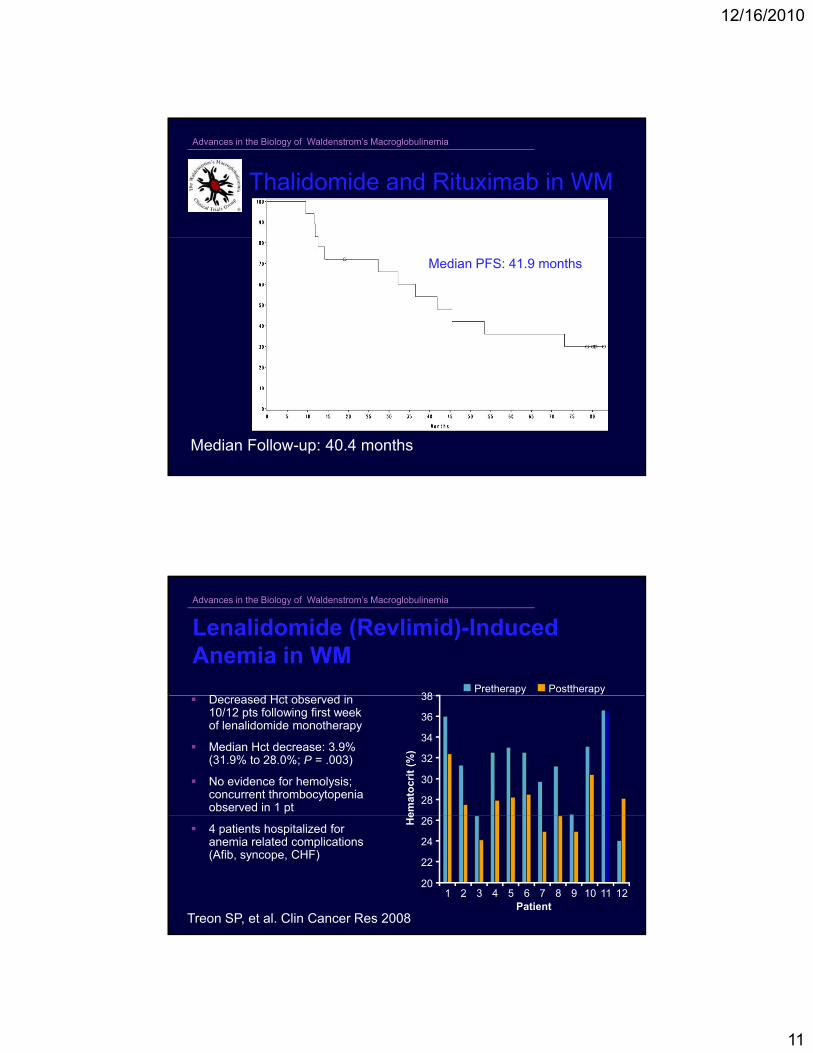
Thalidomide and Rituximab in WM
Median PFS: 41.9 months
Median Follow-up: 40.4 months
Advances in the Biology of Waldenstrom’s Macroglobulinemia
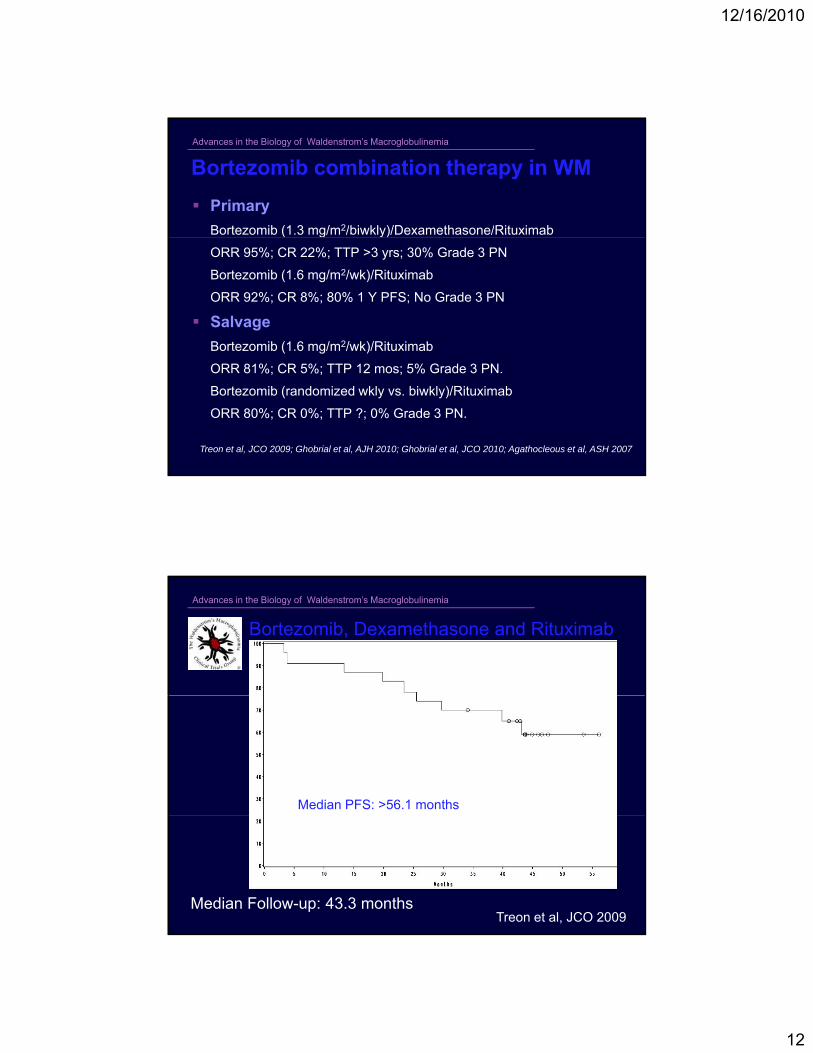
Lenalidomide (Revlimid)-Induced Anemia in WM
D d H t b d i 38Pretherapy Posttherapy
Decreased Hct observed in 10/12 pts following first week of lenalidomide monotherapy
Median Hct decrease: 3.9% (31.9% to 28.0%; P = .003)
No evidence for hemolysis; concurrent thrombocytopenia observed in 1 pt
28
30
32
34
36
38
emat
ocr
it (
%)
4 patients hospitalized for anemia related complications (Afib, syncope, CHF)
Treon SP, et al. Clin Cancer Res 2008
20
22
24
26
1 2 3 4 5 6 7 8 9 10 11 12
He
Patient
12/16/2010
12
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Bortezomib combination therapy in WM
Primary
Bortezomib (1.3 mg/m2/biwkly)/Dexamethasone/Rituximab( g y)
ORR 95%; CR 22%; TTP >3 yrs; 30% Grade 3 PN
Bortezomib (1.6 mg/m2/wk)/Rituximab
ORR 92%; CR 8%; 80% 1 Y PFS; No Grade 3 PN
Salvage
Bortezomib (1.6 mg/m2/wk)/Rituximab
ORR 81%; CR 5%; TTP 12 mos; 5% Grade 3 PN.
Bortezomib (randomized wkly vs. biwkly)/Rituximab
ORR 80%; CR 0%; TTP ?; 0% Grade 3 PN.
Treon et al, JCO 2009; Ghobrial et al, AJH 2010; Ghobrial et al, JCO 2010; Agathocleous et al, ASH 2007
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Bortezomib, Dexamethasone and Rituximab
in WM
Median PFS: >56.1 months
Median Follow-up: 43.3 monthsTreon et al, JCO 2009
12/16/2010
13
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Advances in the Biology of Waldenstrom’s Macroglobulinemia
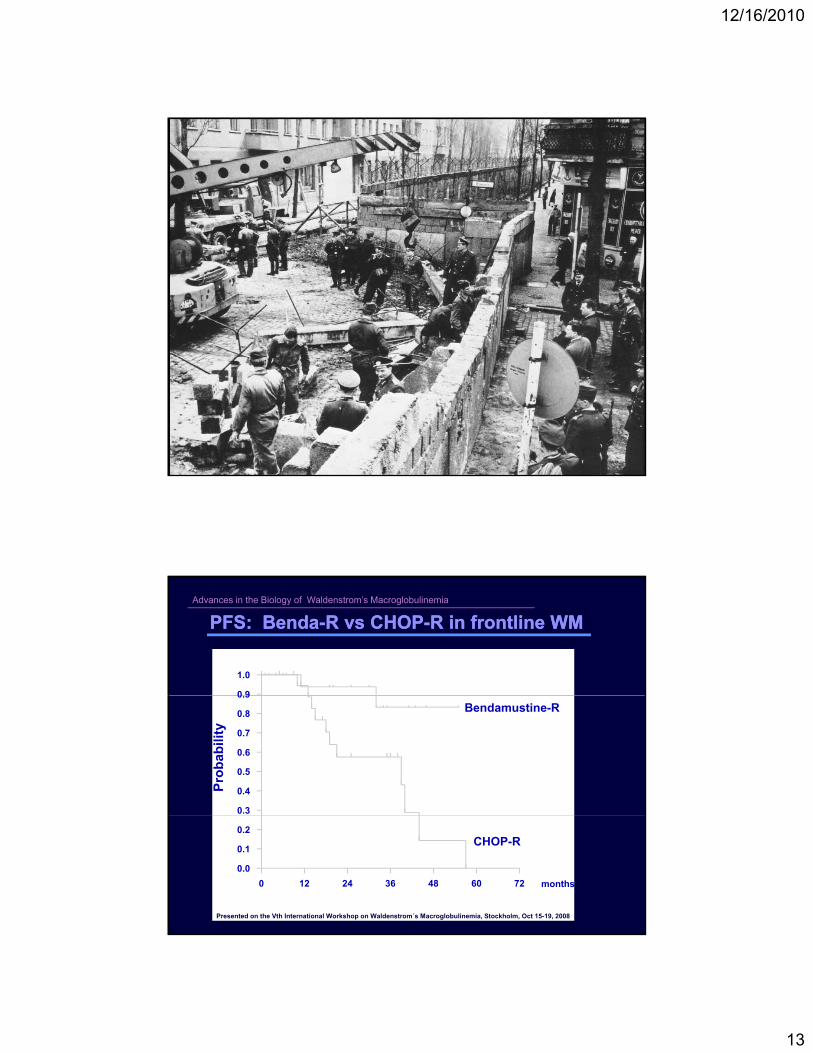
PFS: BendaPFS: Benda--R vs CHOPR vs CHOP--R in frontline WMR in frontline WM
0 9
1.0
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Pro
bab
ility
Bendamustine-R
0 12 24 36 48 60 72
0.0
0.1
0.2
months
CHOP-R
Presented on the Vth International Workshop on Waldenstrom´s Macroglobulinemia, Stockholm, Oct 15-19, 2008
12/16/2010
14
Advances in the Biology of Waldenstrom’s Macroglobulinemia
CR >90 mos.
CR
VGPR
PR
MR
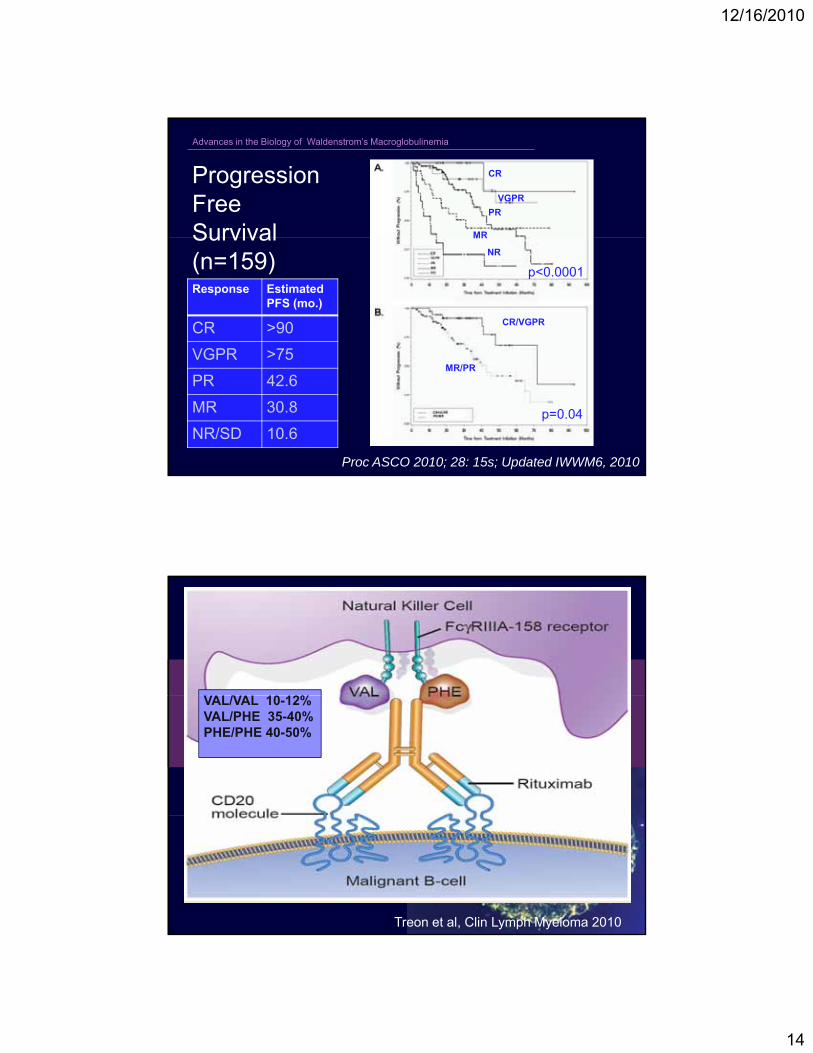
Progression Free Survival
VGPR >75 mos.
PR 42.8 mos.
MR 30.8 mos.
MR
NR
CR/VGPR
Survival (n=159) p<0.0001Response Estimated
PFS (mo.)
CR >90
VGPR >75
P<0.0001
NR 10.1 mos.
MR/PR
p=0.04
VGPR >75
PR 42.6
MR 30.8
NR/SD 10.6
Proc ASCO 2010; 28: 15s; Updated IWWM6, 2010
/ 10 12%VAL/VAL 10-12%VAL/PHE 35-40%PHE/PHE 40-50%
Treon et al, Clin Lymph Myeloma 2010
12/16/2010
15
Advances in the Biology of Waldenstrom’s Macroglobulinemia
80%
90%
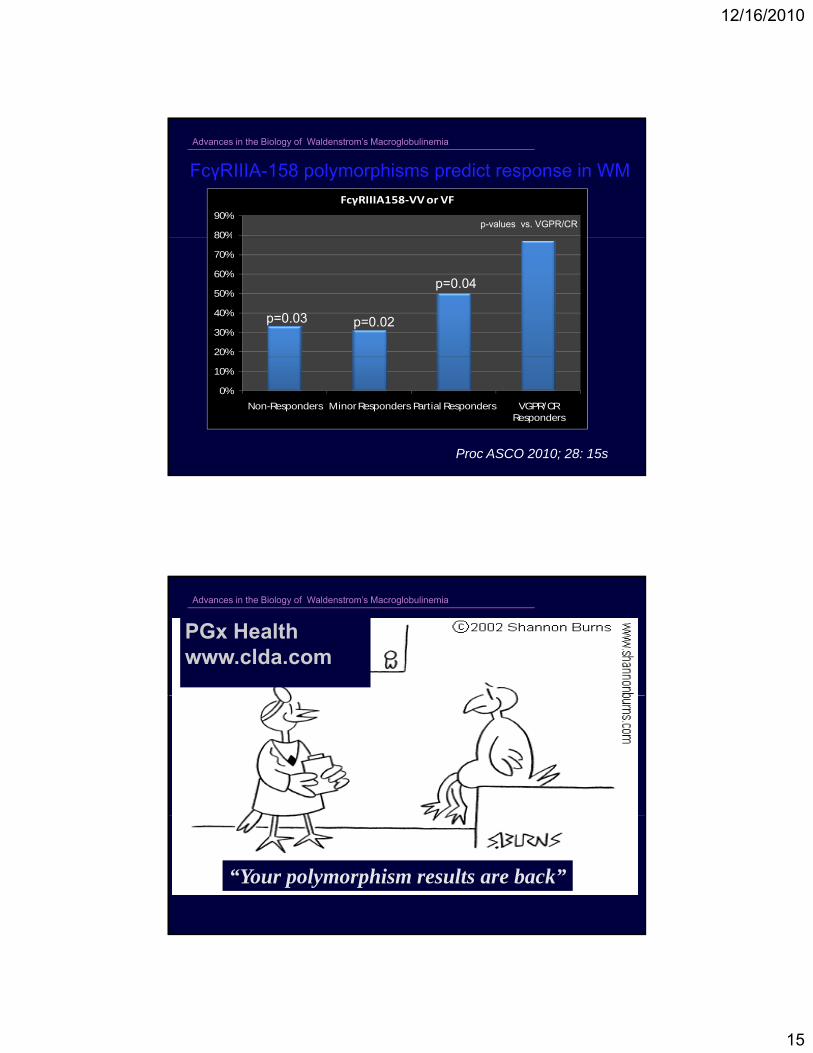
FcγRIIIA158-VV or VF
FcγRIIIA-158 polymorphisms predict response in WM
p-values vs. VGPR/CR
20%
30%
40%
50%
60%
70%
80%
p=0.03 p=0.02
p=0.04
0%
10%
Non-Responders Minor Responders Partial Responders VGPR/CR Responders
Proc ASCO 2010; 28: 15s
Advances in the Biology of Waldenstrom’s Macroglobulinemia
PGx Healthwww.clda.com
“Your polymorphism results are back”
12/16/2010
16
Advances in the Biology of Waldenstrom’s Macroglobulinemia
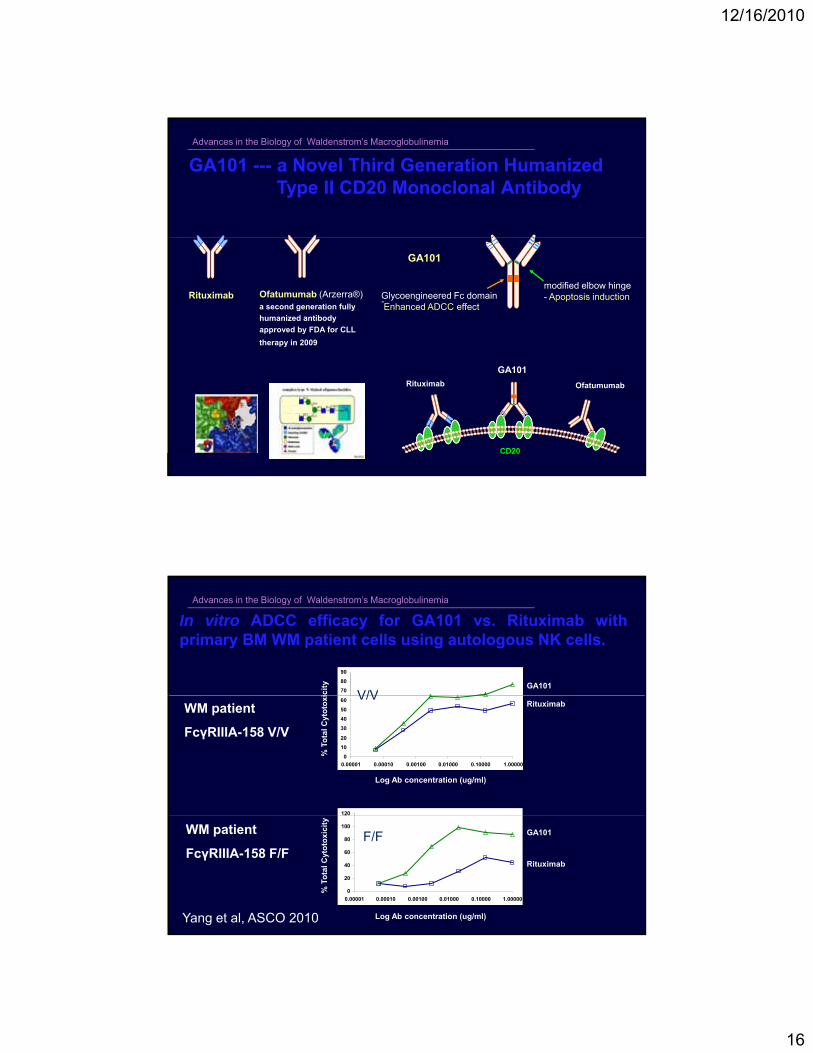
GA101 --- a Novel Third Generation HumanizedType II CD20 Monoclonal Antibody
Ofatumumab (Arzerra®) a second generation fully
humanized antibody
approved by FDA for CLL
therapy in 2009
Rituximab Glycoengineered Fc domain-Enhanced ADCC effect
modified elbow hinge- Apoptosis induction
GA101
Rituximab Ofatumumab
GA101
CD20
Advances in the Biology of Waldenstrom’s Macroglobulinemia
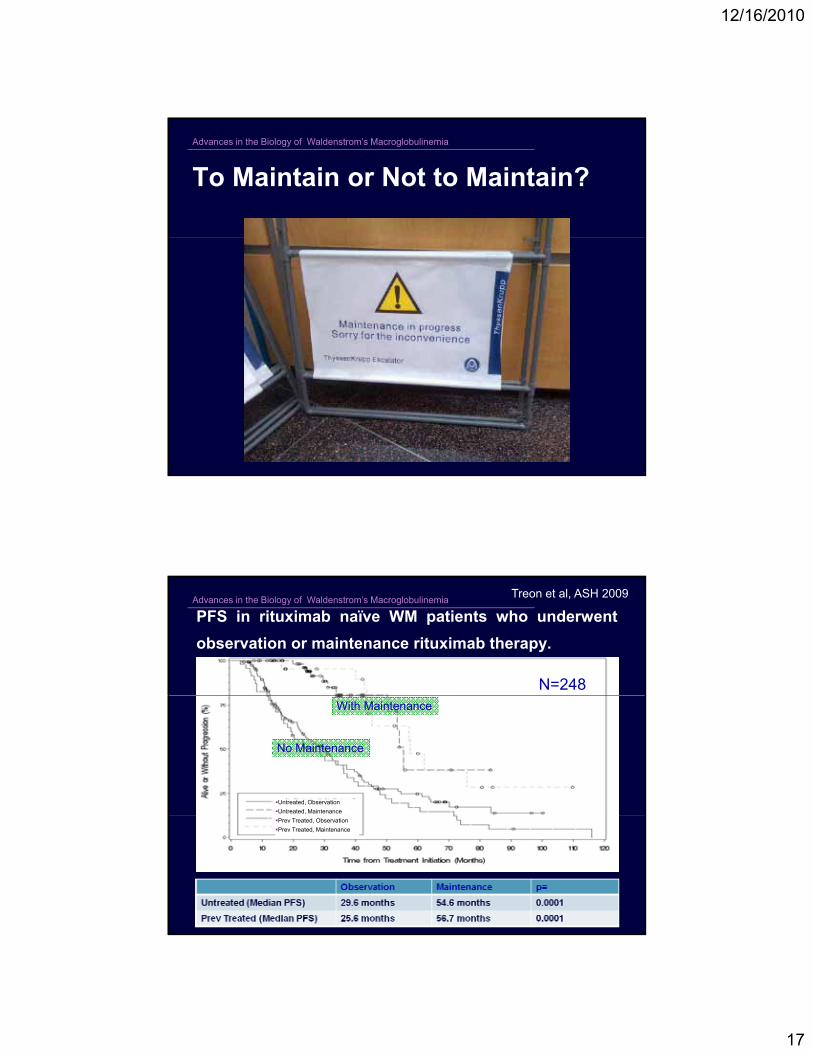
In vitro ADCC efficacy for GA101 vs. Rituximab withprimary BM WM patient cells using autologous NK cells.
GA101
icit
y
70
80
90
V/V
120
WM patient
FcγRIIIA-158 V/V
Rituximab
Log Ab concentration (ug/ml)
% T
ota
l C
yto
tox
i
0
10
20
30
40
50
60
0.00001 0.00010 0.00100 0.01000 0.10000 1.00000
V/V
0
20
40
60
80
100
120
0.00001 0.00010 0.00100 0.01000 0.10000 1.00000
GA101
Rituximab
Log Ab concentration (ug/ml)
% T
ota
l C
yto
tox
icit
y
WM patient
FcγRIIIA-158 F/FF/F
Yang et al, ASCO 2010
12/16/2010
17
Advances in the Biology of Waldenstrom’s Macroglobulinemia
To Maintain or Not to Maintain?
Advances in the Biology of Waldenstrom’s Macroglobulinemia
PFS in rituximab naïve WM patients who underwent
observation or maintenance rituximab therapy.
Treon et al, ASH 2009
N=248
Untreated, Observation
Untreated, Maintenance
With Maintenance
No Maintenance
Prev Treated, Observation
Prev Treated, Maintenance
12/16/2010
18
Advances in the Biology of Waldenstrom’s Macroglobulinemia
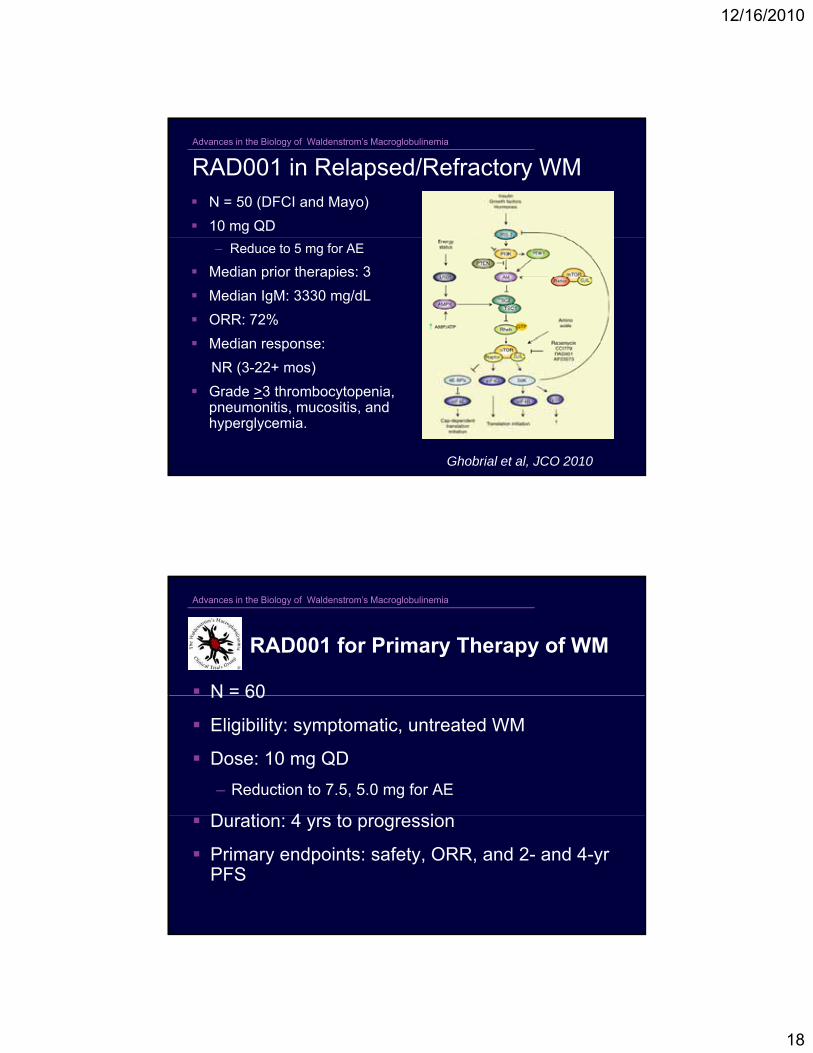
N = 50 (DFCI and Mayo)
10 mg QD
RAD001 in Relapsed/Refractory WM
– Reduce to 5 mg for AE
Median prior therapies: 3
Median IgM: 3330 mg/dL
ORR: 72%
Median response:
NR (3-22+ mos)
Grade >3 thrombocytopenia, pneumonitis, mucositis, and hyperglycemia.
Ghobrial et al, JCO 2010
Advances in the Biology of Waldenstrom’s Macroglobulinemia
RAD001 for Primary Therapy of WM
N = 60N 60
Eligibility: symptomatic, untreated WM
Dose: 10 mg QD
– Reduction to 7.5, 5.0 mg for AE
D ti 4 t i Duration: 4 yrs to progression
Primary endpoints: safety, ORR, and 2- and 4-yr PFS
12/16/2010
19
Advances in the Biology of Waldenstrom’s Macroglobulinemia
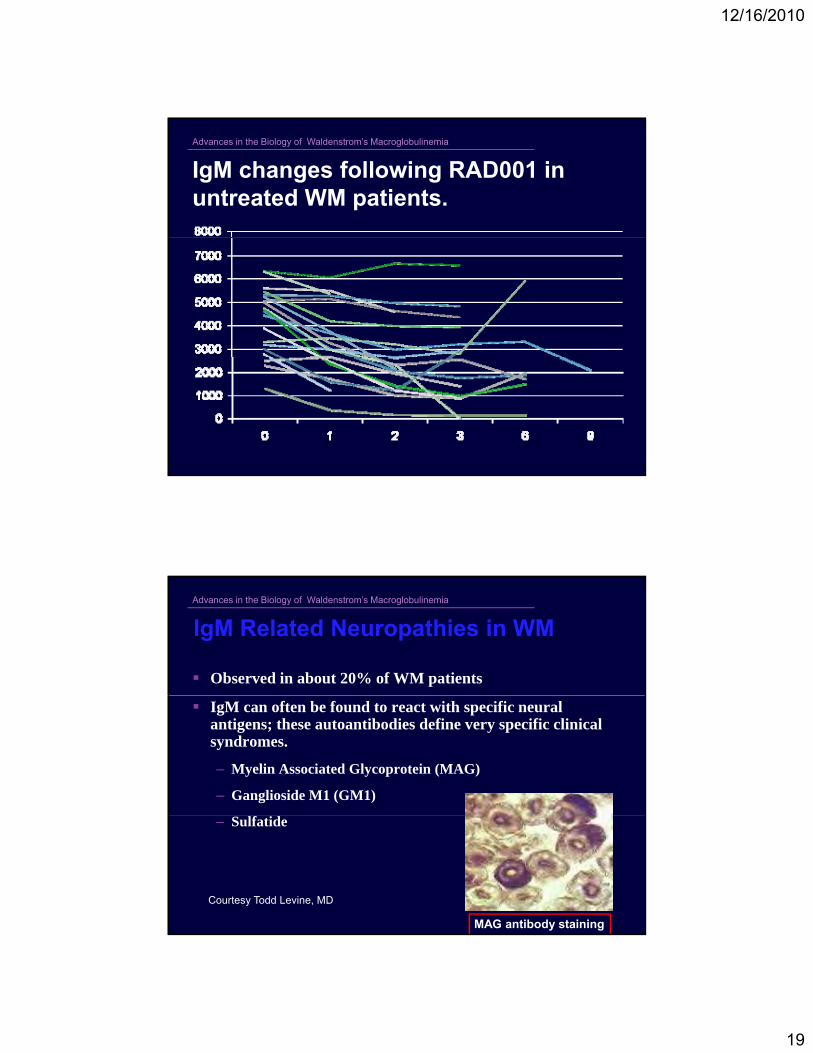
IgM changes following RAD001 in untreated WM patients.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
IgM Related Neuropathies in WM
Observed in about 20% of WM patients
IgM can often be found to react with specific neural antigens; these autoantibodies define very specific clinical syndromes.
– Myelin Associated Glycoprotein (MAG)
– Ganglioside M1 (GM1)
– Sulfatide
Courtesy Todd Levine, MD
MAG antibody staining
12/16/2010
20
Advances in the Biology of Waldenstrom’s Macroglobulinemia
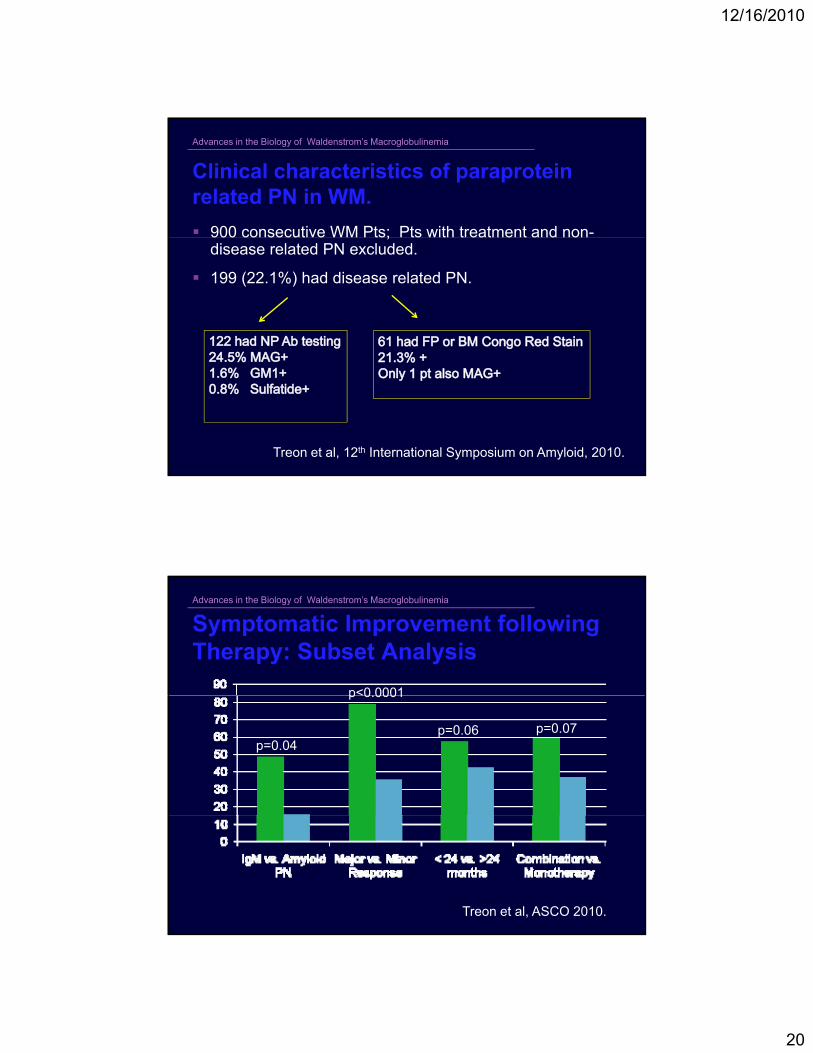
Clinical characteristics of paraproteinrelated PN in WM.
900 consecutive WM Pts; Pts with treatment and non-900 consecutive WM Pts; Pts with treatment and nondisease related PN excluded.
199 (22.1%) had disease related PN.
Treon et al, 12th International Symposium on Amyloid, 2010.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Symptomatic Improvement following Therapy: Subset Analysis
p<0 0001
p=0.04
p<0.0001
p=0.06 p=0.07
Treon et al, ASCO 2010.
12/16/2010
21
Advances in the Biology of Waldenstrom’s Macroglobulinemia
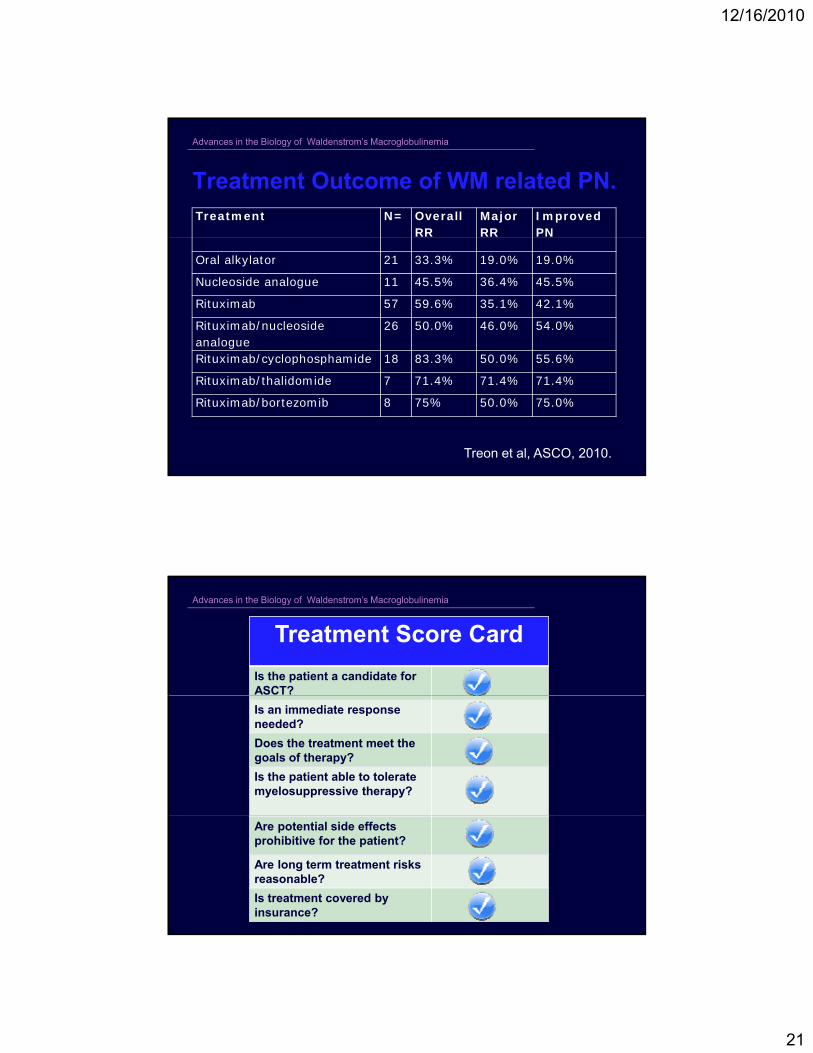
Treatment Outcome of WM related PN.Treatment N= Overall
RRMajorRR
ImprovedPN
Oral alkylator 21 33.3% 19.0% 19.0%
Nucleoside analogue 11 45.5% 36.4% 45.5%
Rituximab 57 59.6% 35.1% 42.1%
Rituximab/nucleosideanalogue
26 50.0% 46.0% 54.0%
Rituximab/cyclophosphamide 18 83 3% 50 0% 55 6%Rituximab/cyclophosphamide 18 83.3% 50.0% 55.6%
Rituximab/thalidomide 7 71.4% 71.4% 71.4%
Rituximab/bortezomib 8 75% 50.0% 75.0%
Treon et al, ASCO, 2010.
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Treatment Score Card
Is the patient a candidate for ASCT?
Is an immediate response needed?
Does the treatment meet the goals of therapy?
Is the patient able to tolerate myelosuppressive therapy?
Are potential side effects prohibitive for the patient?
Are long term treatment risks reasonable?
Is treatment covered by insurance?

12/16/2010
22
Advances in the Biology of Waldenstrom’s Macroglobulinemia
Summary
Watch and wait is appropriate for asymptomatic patients.
Bendamustine Bortezomib Cyclophosphamide and Bendamustine, Bortezomib Cyclophosphamide, andThalidomide based rituximab therapies are active and canbe considered in the upfront treatment of WM.
Use of nucleoside analogues should be carefullyconsidered due to potential long-term consequences.
Better categorical responses are associated with improvedPFS in rituximab naïve WM patients receiving rituximabbased therapy, and may reflect underlying FcγRIIIA-158polymorphisms.
Patients with IgM related PN benefit with earlier treatmentwith rituximab combination therapy.