Embed Size (px)
Citation preview

TRAUMA INFORMED CARE: TEACHING NOT TREATING.A BRIEF OVERVIEW OF THE TRANSFORMING CARE TRAINING PACKAGE
Sharon Atkin, Diana Boswell, Sue Kitchener, Brenda Boustead & Valerie Picot.
12/5/2008
Thomas Wright Institute
OVERVIEW
12/5/2008Thomas Wright Institute
Goal & objectives of Transforming Care trainingImpact of complex trauma on brain developmentImplicationsRelevance across diagnosesContexts for learningRelevance across culturesSummary
Goal of TC Training
12/5/2008Thomas Wright Institute
Developed through the Thomas Wright InstituteGoal
To positively transform the way care providers understand and respond to the children in their care.
To enhance understanding & promote ways of respondingDevelop practice
Learning objectives of TC Training
12/5/2008Thomas Wright Institute
ObjectivesTo provide information about underpinning theoriesOutline key principles of brain developmentIntroduce concept of pain based behaviour and responsesDescribe the 3 central intervention principles Introduce a sample set of practice skills based on the 3 key principles
Theories
12/5/2008Thomas Wright Institute
The training aims to create a framework that links trauma, developmental, attachment theories and neuroscience
Defining Trauma
12/5/2008Thomas Wright Institute
Trauma as “a psychologically distressing event that is outside the range of usual human experience, often involving a sense of intense fear, terror or helplessness”(Bruce Perry, 2002)
Simple trauma (acute trauma; type 1)- one off event
Complex trauma (relational trauma; developmental trauma; type 2)

Complex Trauma
12/5/2008Thomas Wright Institute
“Complex trauma describes the experience of multiple, chronic and prolonged, developmentally adverse traumatic events, most often of an interpersonal nature (e.g. sexual or physical abuse, war, community violence) and early life onset”(van der Kolk, 2005)
“At the core of traumatic stress is a breakdown in the capacity to regulate internal states like fear, anger, and sexual impulses” Bessel van der Kolk
“The most significant consequence of early relational trauma is the loss of the ability to regulate the intensity and duration of affects” Allan Schore
Trauma and Pain
Trauma leads to the repeated
involuntarytriggering of the stress reaction with feelings of overwhelming
fear and helplessness.
“States of autonomic hyperarousal are subjectively experienced as pain…”
(Schore, 2003, p. 68).
12/5/2008Thomas Wright Institute
The organisation of behaviour
• If young people have learned to be in a constant state of hyperarousal & constantly vigilant for danger or threat?
•What behaviours would we expect to see? •Impulsive responses: Anger; fear; aggression; disorganisede.g. change of plans
Behaviours that make sense given the context

Trauma, Attachment & Brain Development
12/5/2008Thomas Wright Institute
AttachmentAttunement (draw upon external (carer) means of regulating emotion whilst learning and developing self regulation)Emotion regulation development
Central challenge is to engage in the world (learn from novel experience) yet maintain a degree of emotional regulation (Shroufe et al, 2005)
Attachment & development
12/5/2008Thomas Wright Institute
Ability to learn and develop compromised when can’t explore the world in the context of responsive care giving (secure attachment base)
Behaviour as organised
12/5/2008Thomas Wright Institute
Infant developing in tandem with carer (relationship with carer)
Infant behaviours as organised to achieve safety – genetically wired to seek care giver to ensure safety.
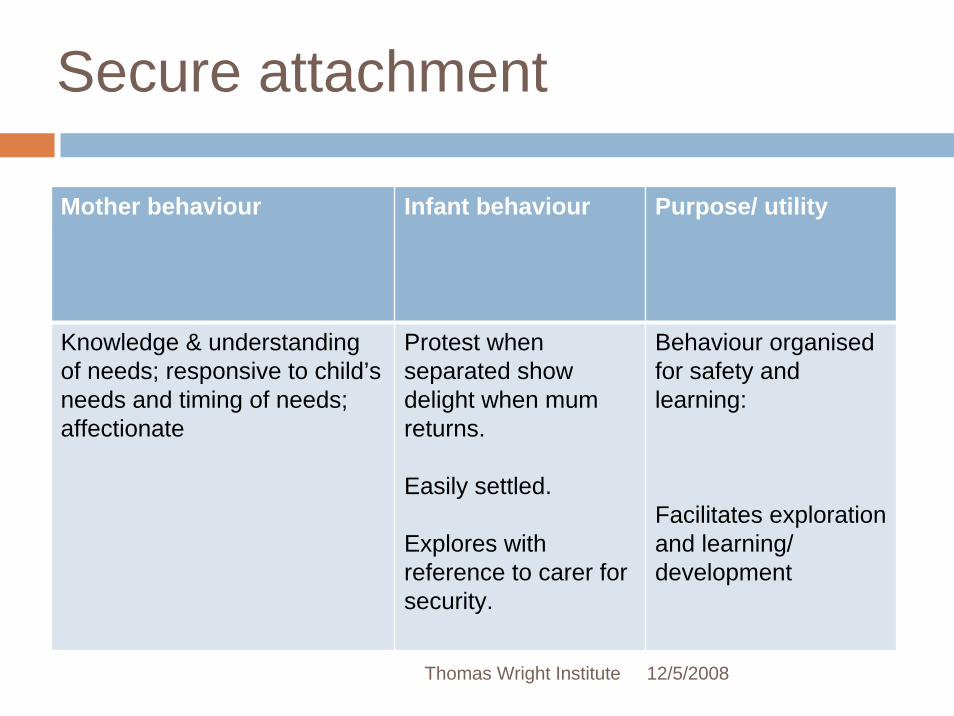
Secure attachment
12/5/2008Thomas Wright Institute
Mother behaviour Infant behaviour Purpose/ utility
Knowledge & understanding of needs; responsive to child’s needs and timing of needs; affectionate
Protest when separated show delight when mum returns.
Easily settled.
Explores with reference to carer for security.
Behaviour organised for safety and learning:
Facilitates exploration and learning/ development
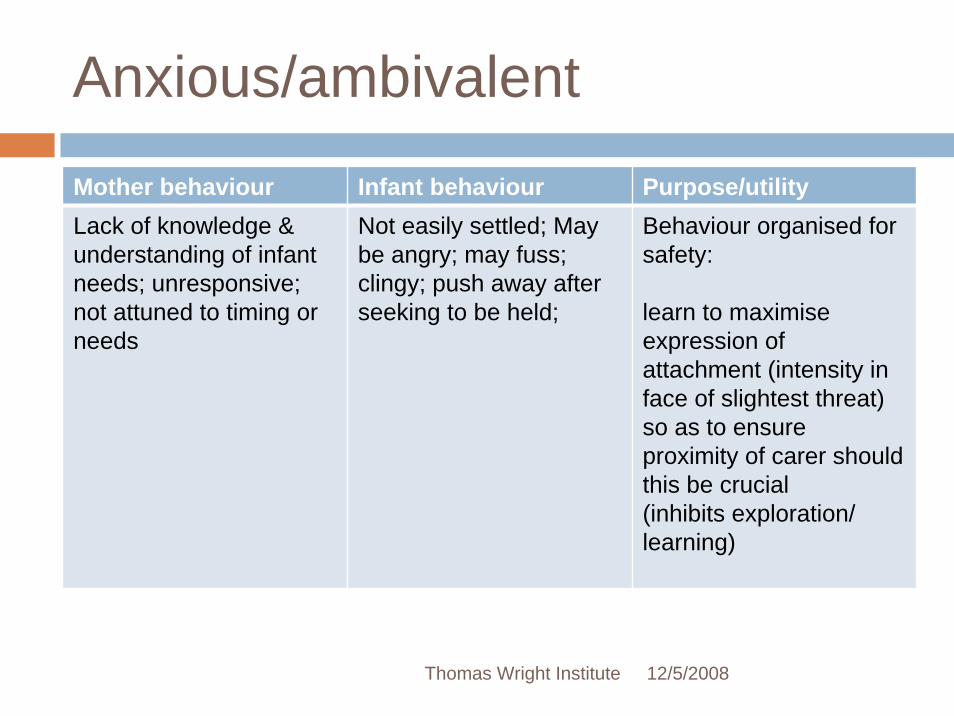
Anxious/ambivalent
12/5/2008Thomas Wright Institute
Mother behaviour Infant behaviour Purpose/utilityLack of knowledge & understanding of infant needs; unresponsive; not attuned to timing or needs
Not easily settled; May be angry; may fuss; clingy; push away after seeking to be held;
Behaviour organised for safety:
learn to maximise expression of attachment (intensity in face of slightest threat) so as to ensure proximity of carer should this be crucial(inhibits exploration/ learning)
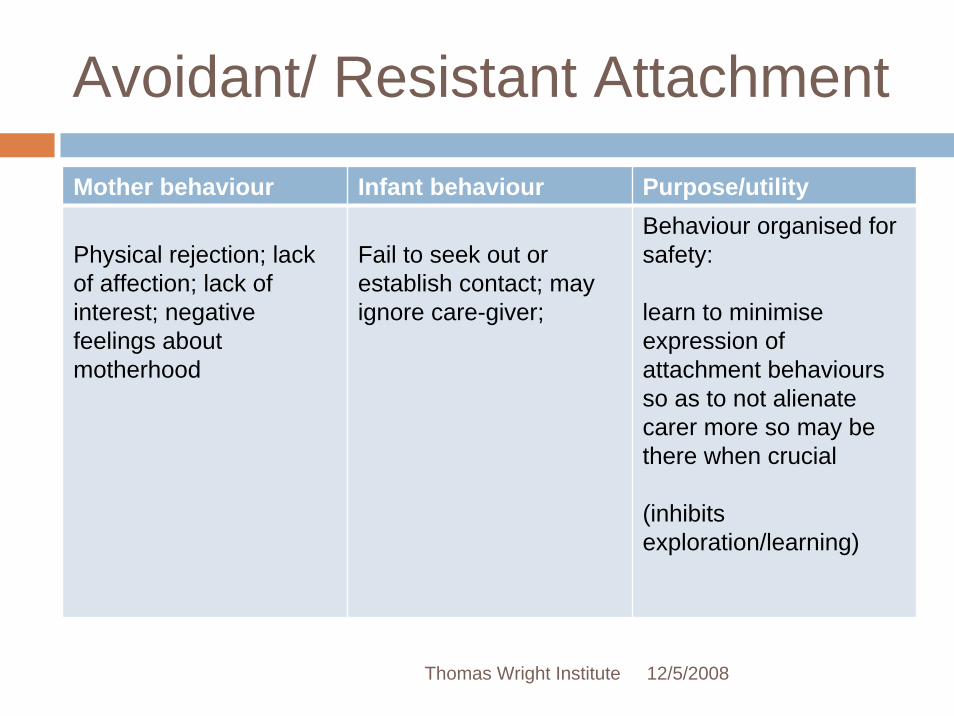
Avoidant/ Resistant Attachment
12/5/2008Thomas Wright Institute
Mother behaviour Infant behaviour Purpose/utility
Physical rejection; lack of affection; lack of interest; negative feelings about motherhood
Fail to seek out or establish contact; may ignore care-giver;
Behaviour organised for safety:
learn to minimise expression of attachment behaviours so as to not alienate carer more so may be there when crucial
(inhibits exploration/learning)

Disorganised Attachment
12/5/2008Thomas Wright Institute
Mother behaviour Infant behaviour Purpose/ utilityMay be incoherent; confusing or frightening (addiction; mental health; own prior trauma)
Intrusive/ interfering
May be abusive (carer as a source of threat)
Crucial to survival that infant be able to depend on care-giver when under threat
Contradictory behaviours
Negative & overwhelmed reactions
May consist of trance like behaviour; stereotypic motions e.g. rocking; head banging
Behaviour not organised
Irresolvable paradox (Shroufe et. al, 2005)
Can’t minimise and maximise attachment behaviours at the same time
Serious compromise to infants ability to organise behaviour; to explore, learn, develop
Principles of Brain Development
12/5/2008Thomas Wright Institute
The brain develops in an experience dependent manner
Neurons that fire together wire together
Use it or lose it
The brain develops from back to front

12/5/2008Thomas Wright Institute
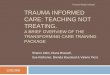
The triune brain (McLean, 1990)
Survival Brain
Emotional Brain
Logical Brain
The Primary Function
“The primary function of parents can be thought of as helping children modulate their own arousal by …teaching them skills that will gradually help them modulate their own arousal” van der Kolk, 2005
What then is the primary function of teachers, & care workers in programs for troubled kids?
Outcomes
12/5/2008Thomas Wright Institute
Pervasive impact across contextsParticular concern re integration of brain functionsCompromises child’s ability to make sense of the world- connections between stimulus or event & emotional reactions strong whilst connections between emotion and reasoning & logic weakStress response & cortisol level; noise & focus (hyperactivity)Dissociation or tuning out (attention deficit)
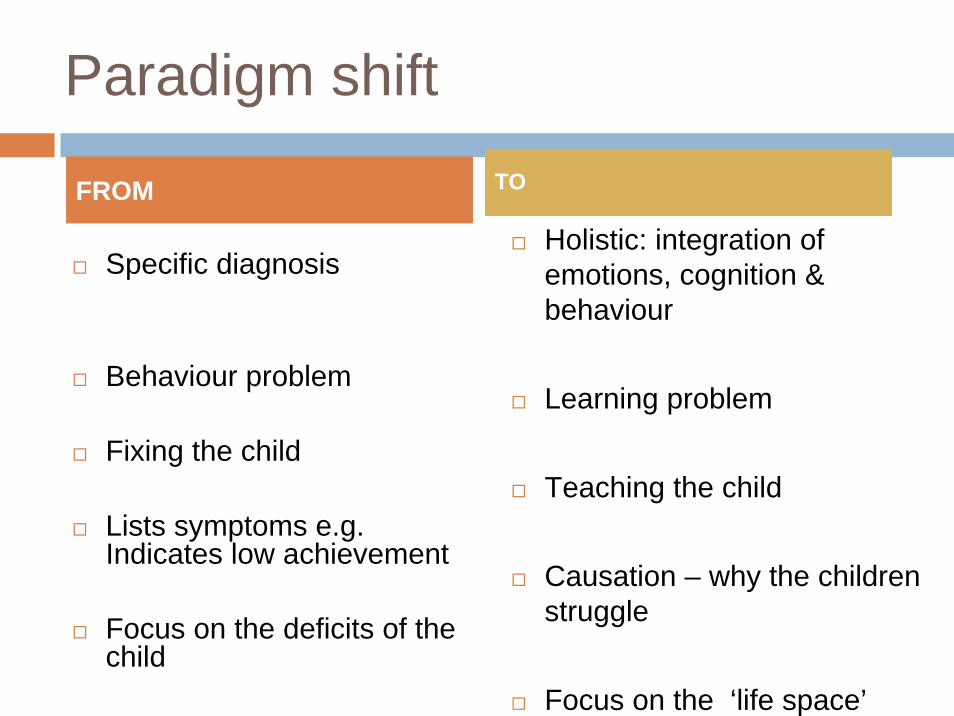
Paradigm shift
Specific diagnosis
Behaviour problem
Fixing the child
Lists symptoms e.g. Indicates low achievement
Focus on the deficits of the child
Holistic: integration of emotions, cognition & behaviour
Learning problem
Teaching the child
Causation – why the children struggle
Focus on the ‘life space’
FROM TO
The question is not “What is wrong with you?” …but“What has
happened to you?”
Sandra Bloom
The ‘life space’ of the childHow do we help not harm?
12/5/2008Thomas Wright Institute
“dealing with…primary pain without unnecessarily inflicting secondary pain experiences on the residents through punitive or controlling reactions”
(Anglin, 2002, p. 55)

Cook 2005 – Pervasive effect on adaptation
Attachment – tend not to ‘belong’ to school, to class, to peer group, not to relate to teacher -Biological – often sleep deprived and stress related illnesses – low tolerance for stress -behaviourAffect regulation – explosive, overreact -suspension Dissociation – attention, focus – academic failure/suspensionBehaviour – disruptive - suspensionCognition – language, logic – academic failureSelf concept
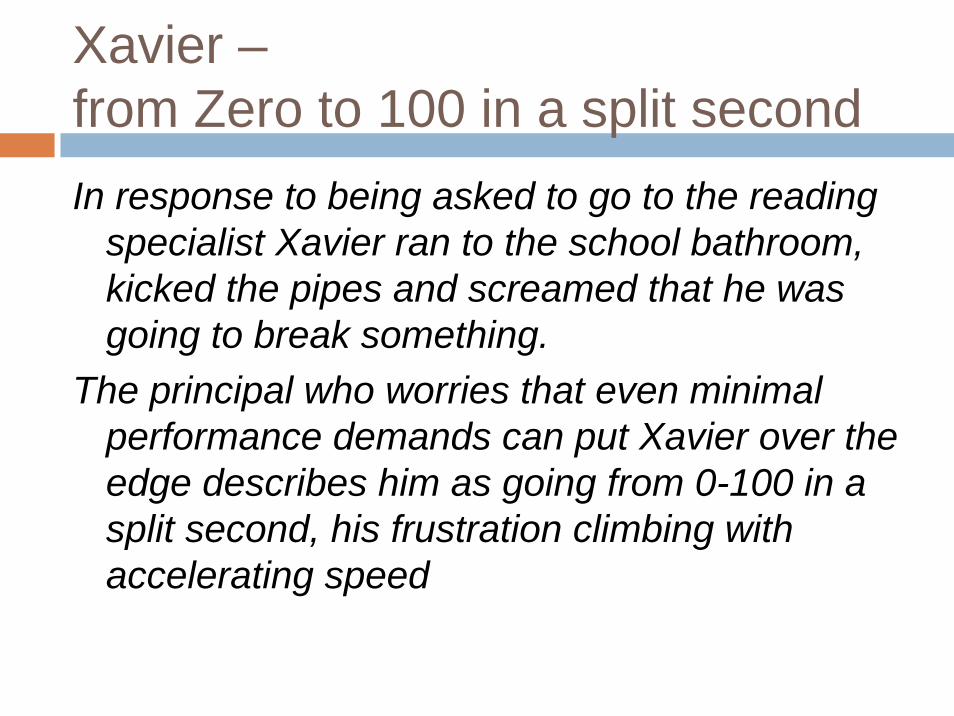
Xavier –from Zero to 100 in a split secondIn response to being asked to go to the reading
specialist Xavier ran to the school bathroom, kicked the pipes and screamed that he was going to break something.
The principal who worries that even minimal performance demands can put Xavier over the edge describes him as going from 0-100 in a split second, his frustration climbing with accelerating speed
Sticky kid
Xaviers parents describe him as a sticky kid who gets fixated on an activity and consequently has a hard time changing gears.
According to his parents and teachers Xavier’s aggressive behaviours especially punching and kicking are typically precipitated by his being asked to end a favourite activity or engage in an activity that he dislikes. He is often remorseful and feels bad after he has hit another child or family member. Nevertheless his parents and teachers agree that their attempts to use rewards and punishments to modify these behaviour have been,
Most Frequent DSM diagnoses
given to chronically abused children
1. Separation Anxiety2. Oppositional Defiant
Disorder3. Phobic Disorders 4. Post Traumatic
Stress Disorder5. Attention Deficit
Hyperactivity Disorder Ackerman and colleagues

Hodgepodge of labels
In the absence of a diagnosis that accurately captures the pervasive nature of disturbances
related to early childhood trauma, children tend to receive a hodgepodge of labels for any number of symptoms that are treated as separate conditions
Approaching any of these problems piecemeal rather than as expressions of a vast system of internal disorganisation, runs the risk of losing sight of the forest in favor of one tree
van der Kolk
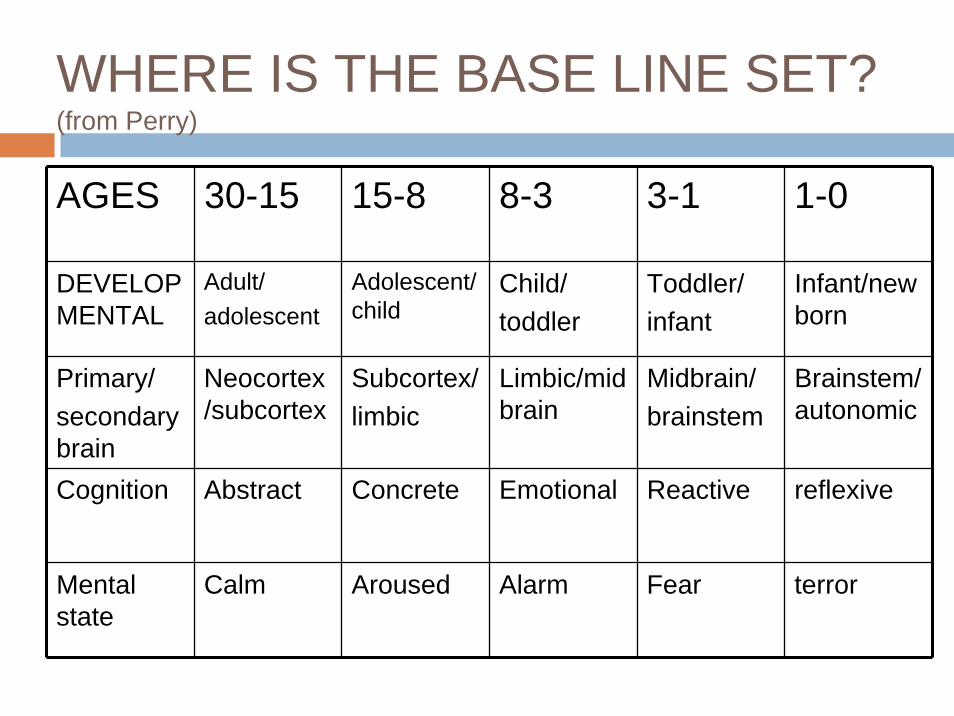
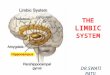
WHERE IS THE BASE LINE SET?(from Perry)
AGES 30-15 15-8 8-3 3-1 1-0
DEVELOPMENTAL
Adult/adolescent
Adolescent/child
Child/toddler
Toddler/infant
Infant/newborn
Primary/secondary brain
Neocortex/subcortex
Subcortex/limbic
Limbic/midbrain
Midbrain/brainstem
Brainstem/autonomic
Cognition Abstract Concrete Emotional Reactive reflexive
Mental state
Calm Aroused Alarm Fear terror
Brainstem drivenbehaviour
During school, if any emotionally charged content is present the child’s state will shift.If this shift is dramatic enough the person will essentially be so anxious and regressed that ‘brainstem driven’
Don’t behave like a baby!It’s like he’s fighting for his life!He’s OK on 1:1
BRAINSTEM DRIVEN BEHAVIOUR
his or her functioning will be


Turn to the person next to you and discuss a child you know
Look at the list of thinking difficulties associated with éxplosive’ childrenDo you recognise any as relating to a child you know who is experiencing difficulty being included at school?What does the child’s BEHAVIOUR MANAGEMENT plan look like?

Characteristics of students from a trauma background
Characteristics of traditional classroom environments
Difficulty organising time, tasks, materials Students expected to start, complete and turn in work with appropriate independence
Concrete black and white thinker Emphasis on conceptual themes
“lost” in class, class clown, ME ME ME Group learning activities, group rules
Impaired understanding of other’s non verbal
Teacher/peer intentions communicated through emotional expression, tone of voice, gestures
Impairment in complex auditory comprehension
Emphasis on teaching through talk
Reduced control over outbursts Outbursts seen as intentionally disruptive and punished
Limited understanding of own and other’s emotional responses
Teacher uses social-emotional reasoning “how would you feel?”
Difficulty considering likely outcomes of actions
Impulsive behaviour interpreted as deliberate rule breaking because he ‘knows’
Difficulty considering a range of solutions Language of “choice” – you have made a bad choice

Calmer Classrooms. A guide to working with traumatised children
Teachers who understand the effects of trauma on children’s education, who are able to develop teaching practices to help them, and who are able to participate actively and collaboratively (with carers) ..will not only improve their educational outcomes but will assist in their healing and recovery.
Child Safety Commissioner, Victoria
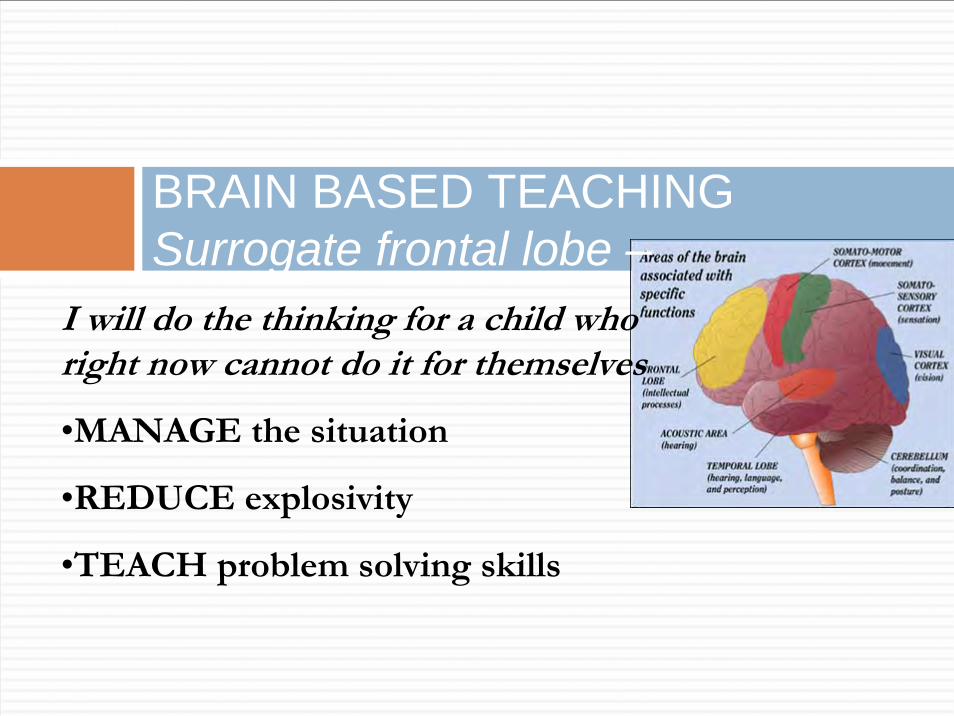
BRAIN BASED TEACHINGSurrogate frontal lobe –
I will do the thinking for a child who right now cannot do it for themselves
•MANAGE the situation
•REDUCE explosivity
•TEACH problem solving skills

Ritchie
12/5/2008Thomas Wright Institute
Were Richie’s developmental needs for SAFETY being met?What was he saying that he needed?Did the adults at home/school LISTEN? Why not?Did his mother CO-REGULATE his emotional arousal? Why not?Were Richie and his mother CONNECTED? Is love enough?
Questions to ask ourselves
12/5/2008Thomas Wright Institute
Help teach carers HOW to LISTENHelp teach carers HOW to SELF REGULATE
HOW to CO-REGULATEHelp teach carers HOW to help the child USE
FRONTAL LOBE thinking skills to meet normal
developmental goals for INDEPENDENCE and
Transforming Care – skills base
12/5/2008Thomas Wright Institute

Collaborative Problem-Solving
The Three ‘Plans
Plan A – When the adults will must prevailPlan B – A format for negotiating issues that canbe negotiatedPlan C – Issues that can be deferred
Worker/carer perspective of the training – Val Picot
12/5/2008Thomas Wright Institute
Transforming Care training beneficial for me as a worker
Training is primarily in relation to children and young people in careUnderstanding the impact trauma has on a child/yp in careparticularly ‘the brain and it development’section, how its functions and explains why children/yp have difficulty in learning and many other challenges they faceThe second part of TC module, a lot more interaction with other participants which made training interesting but also gives a realistic experience of how a child/yp is feeling
Worker/carer perspective
12/5/2008Thomas Wright Institute
Cultural perspectiveModule 2 beings with the three pillars of intervention: Safety, Connection and Emotion ManagementFirst Piller of Intervention: SafetyIf children are anxious and fearful most of the time they cannot focus on other areas of development
Builds resilience, short story
Worker/carer perspective
12/5/2008Thomas Wright Institute
Carer perspectiveTC training beneficial as a carer to understand what trauma is and how it affects children/yp in care
Behaviour management, behaviour strategiesAs carer helps me to respond positively to behaviourAble to recognise behaviors’ linked to trauma
Indigenous perspective
12/5/2008Thomas Wright Institute
Bargumar & KIPA- Sue KitchenerIFACSS- Brenda Boustead
–Recognised Entities
The of the REEnsuring child placement principles are upheld; provided cultural & family advice throughout the decision making processes
KIPA
12/5/2008Thomas Wright Institute
Funding from Department of Child SafetyCaboolture AreaRedcliffe AreaPine Rivers Area
KIPA
12/5/2008Thomas Wright Institute
Foster & kinship care team leader
Provide responsive, diverse care environments
Culturally appropriate
Safe
Indigenous Family And Child Support Service
12/5/2008Thomas Wright Institute
IFACSS
12/5/2008Thomas Wright Institute
Alternative CareRecruitment
Working with Carers:Training and AssessmentCarer Support Approvals and RenewalsLocating culturally appropriate placements (S83)Attend relevant meetingsPlacement Referrals/RespiteCultural SupportAdvocacy ReferralsPlacement AgreementsCarer Agreements
Recognised EntitySCAN CoordinatorS6 Child Protection Act 1999S83 Child Placement PrincipleCourt and Court ReportsSCANI & A’sFGMCultural SupportLiaisonReferralsCase Discussions and ReviewsPlacement Support
Indigenous perspective
12/5/2008Thomas Wright Institute
Trauma of Indigenous childrenHistoricalContextual (reasons came into care)Non-indigenous placement
Many Aboriginal and/or Torres Strait Islander children do not like to express/share their feelings to the non-Indigenous or wider community.Assuming body language and facial expressions can often be mistaken for sadness, disrespect, lack of understanding
Indigenous perspective
12/5/2008Thomas Wright Institute
Relevance of Transforming Care Training
Provides greater awareness of how children suffer traumaProvides opportunity to develop greater flexibilityTeaching not trying to manage behaviours
Mirroring is common with Aboriginal and/or Torres Strait Islander children as this is traditionally the way of learning/teaching e.g. through Dance, Art/drawings/symbols, Storytelling and Music/Song.
Practicing the skills from the Transforming Care Course will especially benefit Aboriginal and/or Torres Strait Islander children and young people to become more confident about themselves and in control of their own decisions and choices.
Usefulness of the training from an Indigenous perspective
12/5/2008Thomas Wright Institute
Carers know first hand the struggles with children when we don’t understand the behaviourSkills
ListeningLearning about co-regulationConcrete ideas about collaborative problem solving which encourages working with rather on children

Usefulness of the training from an Indigenous perspective
12/5/2008Thomas Wright Institute
Fit with Indigenous culturePromotes notion of needing multiple carers/ significant adults input
Develops resilience
Promotion of positive self esteem through cultural awareness and pride

Implications
12/5/2008Thomas Wright Institute
Expectations of children don’t necessarily fit with child’s skills.They can at times intellectually reason out good responses; however their ability to connect with this reasoning in times of stress is compromised.Adults response can lead to more confusion & shame; child does not know why they react the way they do at times

Delivery
12/5/2008Thomas Wright Institute
Broken down into smaller trainings of about 3 hoursEach section to be presented with a skill or practice tool e.g. When training refers to how putting words to feelings can assist traumatised young people include straight after listening skills training & practiceLots of poster around to reinforceFollow up learning by support person

Learning through role plays
12/5/2008Thomas Wright Institute
Skills practice- collaborative problem solving as one approachCreative delivery Special thanks to Shirlene Boyd, Judy Scorinis, Tracy Gray & Amanda Schroder from Cairns & Atherton Alt care teams for the clips of role playsScenario What might the adults expectation be
Why e.g. consistent; following through
Plan A- adult’s will prevails
12/5/2008Thomas Wright Institute

Plan B; negotiation
12/5/2008Thomas Wright Institute
What’s happened?
12/5/2008Thomas Wright Institute
Engaged by Policy & Practice Development Branch; Policy & Programs Division to present train the trainer programs across a number of regions
North Brisbane - NudgeeSouth Brisbane – Beenleigh; RuncornToowoomba/Ipswich - ToowoombaTownsville Cairns
Train the trainer participants
12/5/2008Thomas Wright Institute
96 participants across a number of organisations
Department of Child SafetyKIPAIFACSSLife Without BarriersTRACCMercy Family ServicesIntegrated Family & Youth ServicePartners in Foster CarePathways
Feedback
12/5/2008Thomas Wright Institute
94 of the 96 train the trainer participants provided feedback
Of those 94 – 96% indicated a belief that the training would be very useful for those interacting with children & young people in the care system; 4% indicated the training as useful

Summary
12/5/2008Thomas Wright Institute
Transforming care training aims to provide information for direct care providers that links knowledge and provides a climate in which the paradigm shift from fixing behaviour to teaching skills can occurTo provide the basis of necessary tools to address the skills deficits