Embed Size (px)
Citation preview

TRAUMA IN ORLTRAUMA IN ORLTRAUMA IN ORLTRAUMA IN ORL
DR. SAAD AL-MUHAYAWI, M.D., FRCSCAssociate Professor & ConsultantAssociate Professor & Consultant
ORL Head & Neck Surgery

TYPES OF TRAUMATYPES OF TRAUMA
EAR & TEMPORAL BONE TRAUMANOSE & FACIAL BONES TRAUMALARYNGEAL TRAUMALARYNGEAL TRAUMANECK TRAUMACAUSTIC INGESTION

PRIORITIES IN TRAUMAPRIORITIES IN TRAUMA
A – AirwayB – Breathing C CirculationC – Circulation
Priorities according to life threatening situation

AURICULAR HEMATOMAAURICULAR HEMATOMA
Blunt trauma – Shear injury – Contact sports / child abuseContact sports / child abuse
Hematoma – Between cartilage and perichondrium
Fluctuant anterior swelling g

TreatmentTreatment – Needle aspiration: inadequate – Incision & drainage: recommended – Compressive dressing p g– Antistaph antibiotics
Complications – Infection / abscess – Cauliflower earCauliflower ear

AURICULAR HEMATOMAAURICULAR HEMATOMA


AURICULAR HEMATOMAAURICULAR HEMATOMA

TEMPORAL BONE FRACTURETEMPORAL BONE FRACTURE
Blunt > penetrating – MVA, fall and assault– Associated with life threatening conditions
EvaluationEvaluation – Trauma protocol / clear c – spine – Assess facial nerve function early
Immediate vs. delayed
– Ear examination: hemotympanum, csf leak, TM perforation. p

EvaluationEvaluation – Assess function: tunning forks, audiogram
di lRadiology– Head CT scan: evaluate for head injury j y
HRCT of temporal bone with bony windowE l t t t f th f t– Evaluate extent of the fracture

TEMPORAL BONE FRACTURETEMPORAL BONE FRACTURE
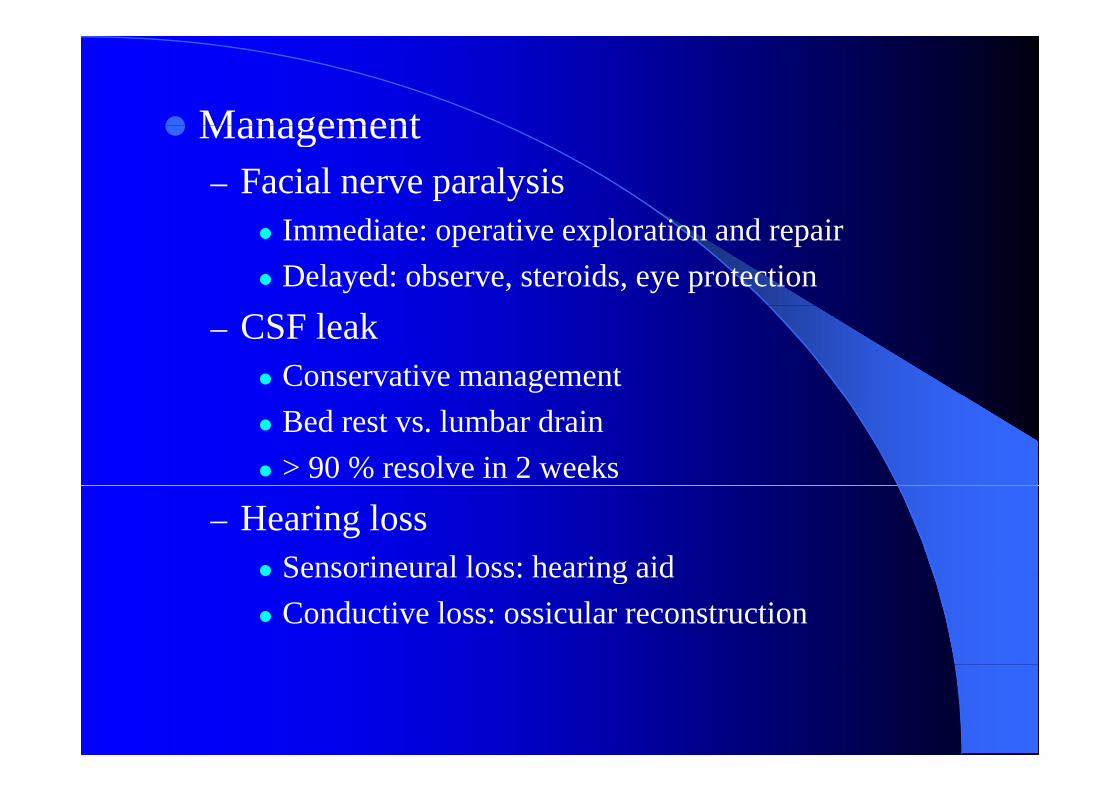
ManagementManagement – Facial nerve paralysis
Immediate: operative exploration and repairDelayed: observe, steroids, eye protection
– CSF leak Conservative management Bed rest vs. lumbar drain> 90 % resolve in 2 weeks
– Hearing lossSensorineural loss: hearing aidSensorineural loss: hearing aidConductive loss: ossicular reconstruction

V tiVertigo:– Treat symptomatically– Meclizine, physical therapy

Physical examination Physical examination

CT findings CT findings

TEMPORAL BONE FRACTURETEMPORAL BONE FRACTURE

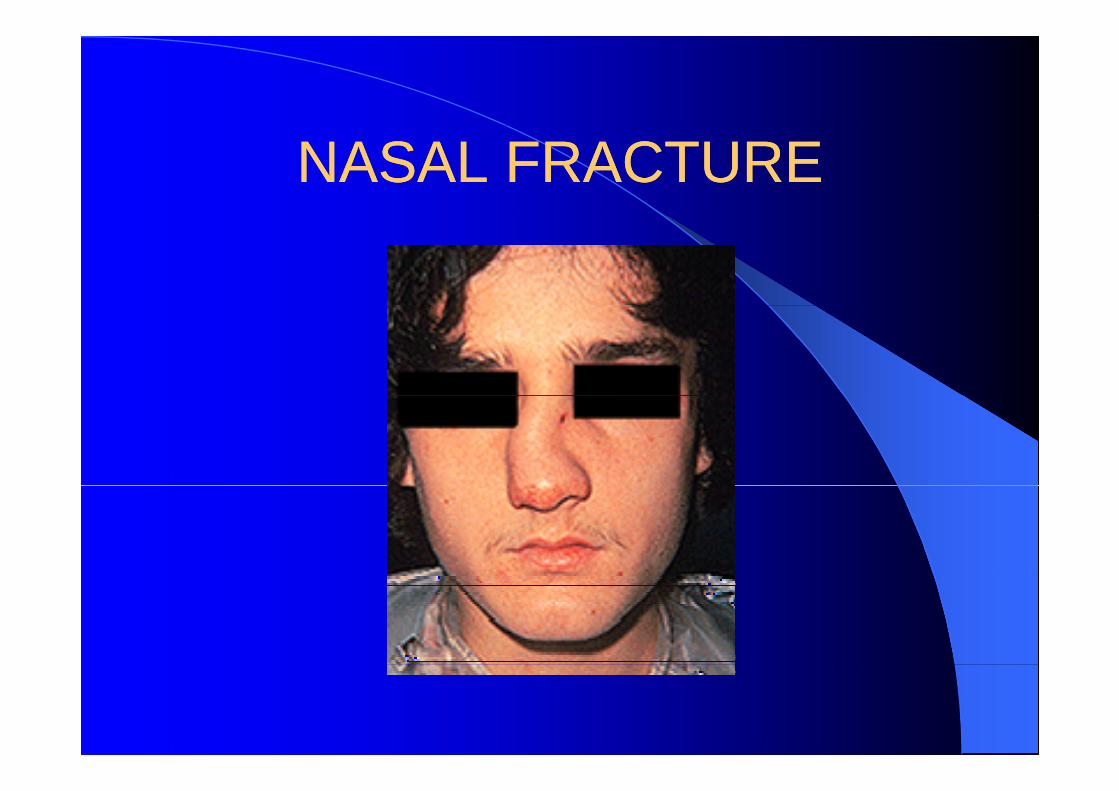
NASAL FRACTURENASAL FRACTURE
Very commonM t f i l f t– Most common facial fracture
– 3rd most fractured boneHi h i d f i i f f tHigh index of suspicion for fracture– Mechanism, change in appearance
Epistaxis nasal obstruction– Epistaxis, nasal obstruction Examine and palpate nose carefully
I t bilit bilit it ti– Instability, mobility, crepitation – Fracture, septal hematoma
NASAL FRACTURENASAL FRACTURE

NASAL FRACTURENASAL FRACTURE
Management

NASAL FRACTURENASAL FRACTURE

ZYGOMA FRACTURE ZYGOMA FRACTURE
Signs and symptoms – Subconjunctival hemorrhage – Infraorbital hypesthesiaInfraorbital hypesthesia – Depressed malar eminence
T i / b t ff– Trismus / bony step off

E l iEvaluation – Facial CT – coronal cuts – Ophthalmology evaluation
Evaluate for ocular injuryEvaluate for ocular injury
Management– Open reduction / internal fixation ( ORIF)

ZYGOMA FRACTUREZYGOMA FRACTURE

ZYGOMA FRACTUREZYGOMA FRACTUREZYGOMA FRACTURE ZYGOMA FRACTURE

ZYGOMA FRACTUREZYGOMA FRACTURE

ORBITAL FLOOR FRACTURE ORBITAL FLOOR FRACTURE

ORBITAL FLOOR FRACTUREORBITAL FLOOR FRACTURE

ORBITAL FLOOR FRACTUREORBITAL FLOOR FRACTURE

MANDIBLE FRACTURE MANDIBLE FRACTURE
1/3– ½ facial fractures Signs and symptoms
Malocclusion step off– Malocclusion, step off– Floor of mouth hematoma – Chin ( V3) hypoesthesia

Evaluation– Secure airway – as neededSecure airway as needed – Rule out associated injury
Closed head injuryClosed head injury C – spine, facial fractureTooth aspirationTooth aspiration
– ( panarox, mandible series) plain x – ray– CT – scan
MANDIBLE FRACTUREMANDIBLE FRACTURE

MANDIBLE FRACTUREMANDIBLE FRACTURE

ManagementManagement – Soft diet, severe fractures
P di i l l iPediatric, normal occlusion Non – displaced
Ramus subcondylar– Ramus, subcondylarClosed reduction
– Minimally displaced y pOpen reduction
Complications – Infection / non unionInfection / non union– Malocclusion

MIDFACE FRACTURES MIDFACE FRACTURES
Diagnosis– Malocclusion, depressed midface, open bite– Assess midface mobilityAssess midface mobility– CT scan – axial, coronal cuts
MManagement – Secure airway ( oral intubation if possible )
C – spine injury or laryngeal fracture: surgical airway

– Avoid nasal instrumentation , cranial penetrationp
– Recognize and treat closed head injury Brisk epistaxis common posterior nasal– Brisk epistaxis common – posterior nasal packing S t CSF l k– Suspect CSF leak
– Open reduction and internal fixation


MIDFACE FRACTURESMIDFACE FRACTURES

MIDFACE FRACTUREMIDFACE FRACTURE

MIDFACE FRACTUREMIDFACE FRACTURE

MIDFACE FRACTUREMIDFACE FRACTURE

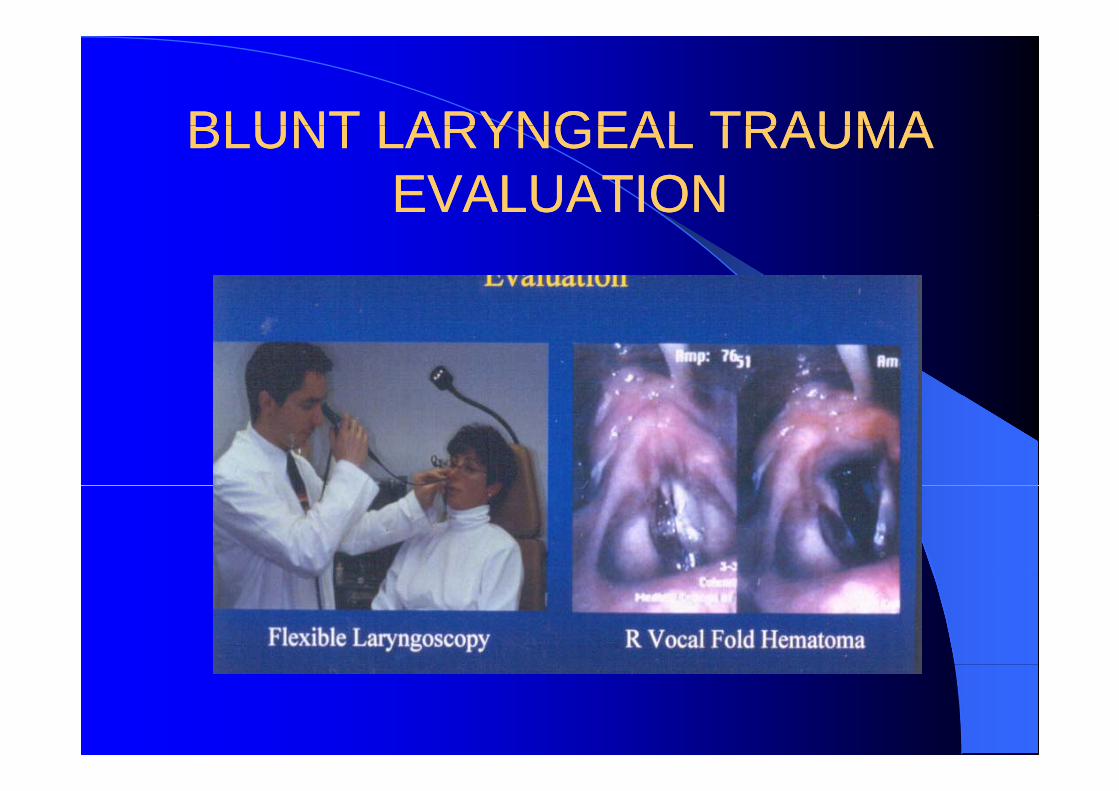
BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMA
Mechanism: MVA,Sport,AssaultSigns and Symptoms
Hoarseness Voice change StridorHoarseness, Voice change, StridorSub-Q emphysema, Hemoptysis
Secure AirwayOral Intubation-problematicO pTracheotomy(not cricothyrotomy)

BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMA
Flexible Fiberoptic Laryngoscopy
CT Scan- evaluate C Sca eva uateskeletal derangement
SurgicalSurgical Explporation/
iRepair

BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMAEVALUATIONEVALUATION
BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMAEVALUATIONEVALUATION

BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMA
Indications for CT scan Significant voice alteration Edema or hematoma on endoscopyEdema or hematoma on endoscopy Laceration or blood on endoscopy V l f ld l iVocal fold paralysis Palpation suspicious of fracture After tracheotomy- before definitive treatment

BLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMABLUNT LARYNGEAL TRAUMAMANAGEMENTMANAGEMENT

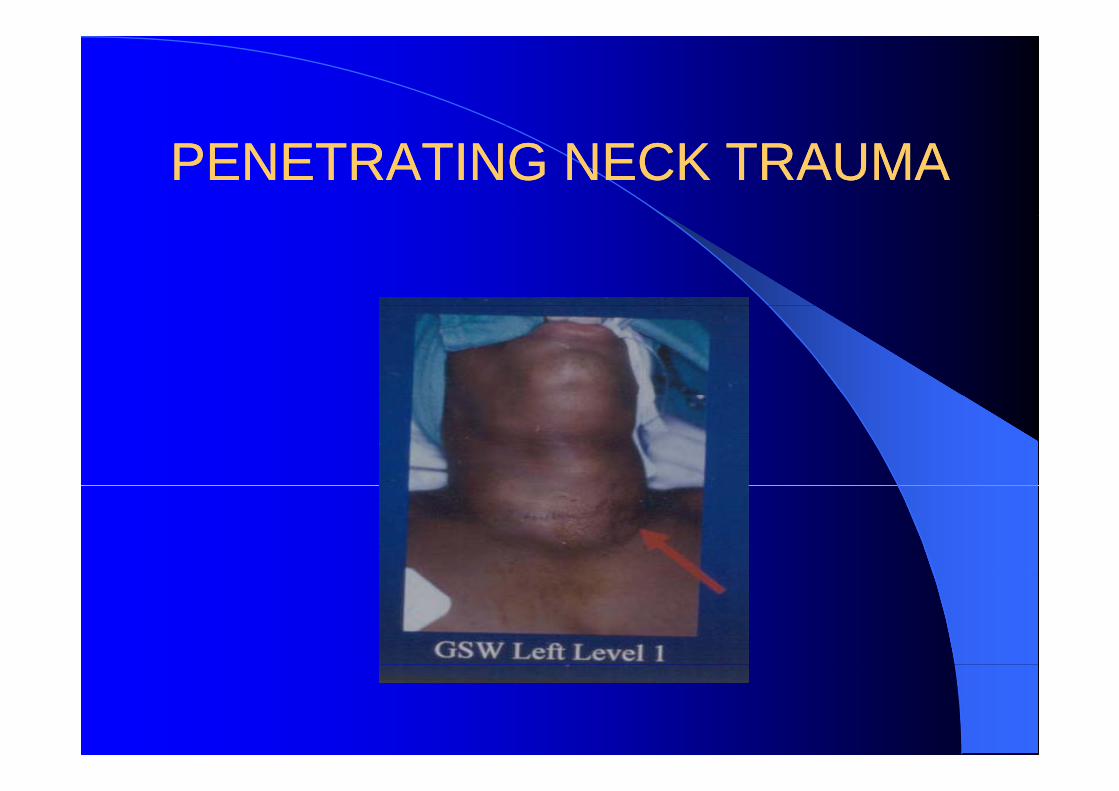
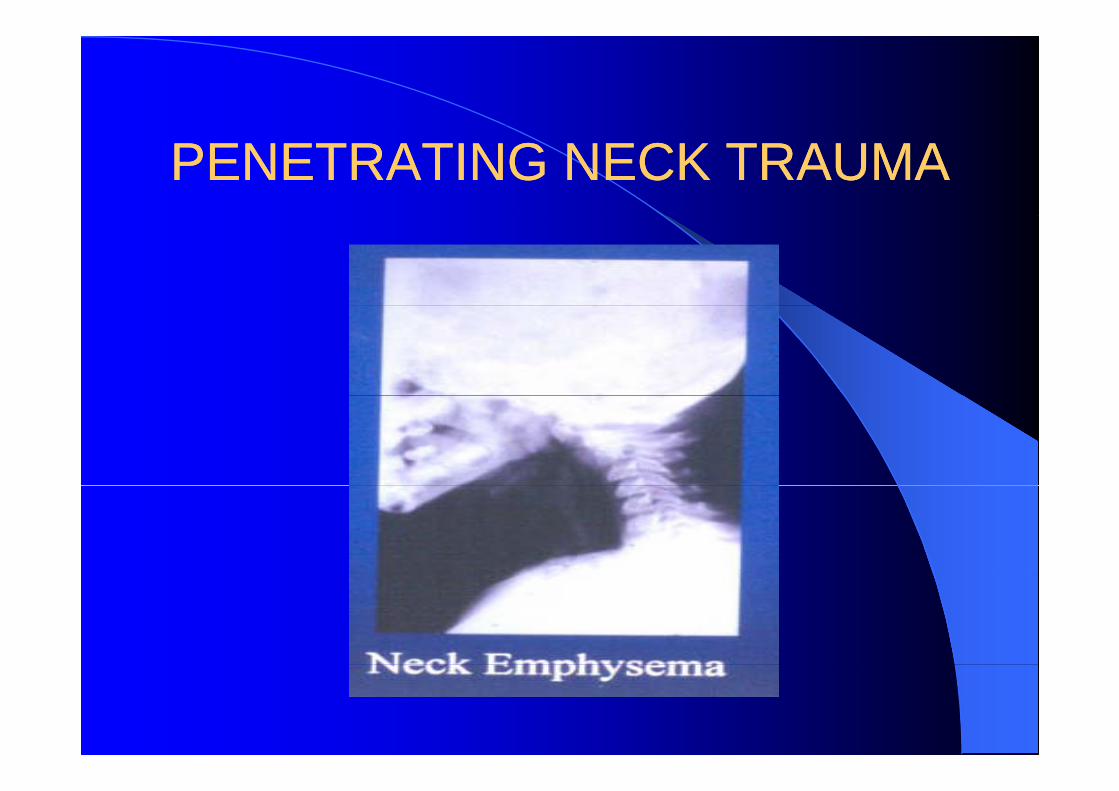
PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA
Secure Airway, Clear C-spineAssume Multiple InjuriesX rays Neck and ChestX-rays Neck and Chest
Foreign bodies, PneumothoraxBony trauma

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA
Weapons- Knife, GunDetermine Zone
1 below cricoid(16%)1- below cricoid(16%)2- cricoid to angle of mandible(78%)3- above angle of mandible(6%)

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA
PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMAMANAGEMENTMANAGEMENTMANAGEMENTMANAGEMENT

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPATTERNS OF INJURYPATTERNS OF INJURY
Vascular InjuryC tid i jCarotid injurySigns & Symptoms
Neurologic Deficit- ¼Neurologic Deficit- ¼Expanding Hematoma- 2/3Clinically silent- 15%
Arteriogram- 97% sensitiveEmbolization Possible-zone 1,3& vertebral artery
C li tiComplicationsStroke, ExsanguinationPseudoaneurysm, AV fistulay ,

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPENETRATING NECK TRAUMAPATTERNS OF INJURYPATTERNS OF INJURY
Pharynx& esophagus- 10%P i D h i H t iPain, Dysphagia, HematemesisBarium Swallow/ EsophagoscopyComplicationsComplications
Mediastinitis, Sepsis, Fistula
Larynx& Trachea-9%Larynx& Trachea 9%Hoarseness, Stridor, HemoptysisLaryngoscopy, BronchoscopyLaryngoscopy, BronchoscopyComplications
Laryngeal Dysfunction, Stenosis

PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA
PENETRATING NECK TRAUMAPENETRATING NECK TRAUMA

CAUSTIC INGESTIONCAUSTIC INGESTION
Esophagus, pharynx, larynxBases
Drain cleanersDrain cleanersElectric dishwasher soapHair relaxant
AcidsBleaches

CAUSTIC INGESTIONCAUSTIC INGESTION
Alkalis – pH > 7Liquefaction necrosis
Acids – pH < 7Acids pH < 7Coagulation necrosis
Bleaches – pH = 7Irritants a

CAUSTIC INGESTIONCAUSTIC INGESTION
Children- most common, accidental
Adults- suicide attempt
Do not induce vomitingDo not induce vomitingDetermine- brand name, quantity ingested
Call poison control centerAlkali worse than acidsAlkali worse than acids

CAUSTIC INGESTIONCAUSTIC INGESTION
Examination not predictive of severityMost without oral lesions
Urgent speciality consultationUrgent speciality consultationFlexible LaryngoscopyEsophagogramEsophagoscopy- early

CAUSTIC INGESTIONCAUSTIC INGESTION