Embed Size (px)
Citation preview

Transplantation of Three Adult Patients With OneCadaveric Graft: Wait or Innovate
Daniel Azoulay, Denis Castaing, Rene Adam, Olivier Mimoz, and Henri Bismuth
Graft shortage continues to prolong waiting times foradults requiring liver transplantation. Living related donortransplantation is possible for only a small minority of adults.The techniques for in situ splitting of the liver used for rightand left hepatectomies in living donors were adapted to acombined split-liver–domino procedure to obtain right andleft hemiliver grafts from a patient undergoing total hepatec-tomy with liver transplantation for a metabolic disorder. Thetwo grafts were adequate in size and function for transplanta-tion to two adults with low priority for regular cadaver grafts.More frequent use of split-liver techniques in cadaverdonors could considerably reduce the graft shortage andwaiting time for adult liver recipients.Copyright r 2000 by the American Association for theStudy of Liver Diseases
F or pediatric patients, the shortage of donor organsis partly offset by reduced-size, split-liver, and living
related–donor transplantation. For adults, reduced-sizepediatric grafts increase the shortage, and there arelimits to the safe resectable volume of grafts for adultsfrom living donors. To overcome the shortage and toreduce the waiting time, techniques for in situ splittingused in living related donors to develop should beadapted to the harvesting of cadaver donor livers andused, whenever possible, to obtain two hemiliver graftsof adequate size and function for transplantation toadults. We successfully adapted split-liver techniques ina patient undergoing total hepatectomy and livertransplantation for familial amyloidotic polyneuropa-thy (FAP) to obtain two hemiliver grafts whose size andfunction were suitable for adult recipients.
Case Report
On September 15, 1999, we performed transplantation on 3adults, starting with 1 cadaver donor liver. This was proposedfor an adult with FAP, a slow-onset congenital metabolicdisorder now treated by liver transplantation. An explantedFAP liver can be transplanted to recipients not eligible forcadaver organs in so-called domino transplantation proce-dures. In this case, we used an in situ split to produce graftsfor 2 adults with cirrhosis and hepatocellular carcinoma.
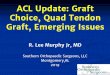
The 3 patients underwent simultaneous operations. Theprocedure is outlined in Figure 1. The right liver wasseparated from the vena cava, in continuity with the righthepatic vein and the right portal pedicle.1 The remaining leftliver was removed en bloc with the inferior vena cava and theleft portal pedicle.
The in situ division results in short ischemia times,2 inthis case, less than 90 minutes for both recipients. The recipientof the left hemiliver had transient jaundice, but otherwise all3 patients had a smooth postoperative course and were discharged20, 25, and 30 days posttransplantation. All are currently athome leading a normal life at 85 days after transplantation.
In a previous report of using 1 liver for 3 patients, acadaveric liver was split ex situ for 1 adult and 1 child, whichis the usual case in that type of procedure. The adult recipientwas a patient with FAP whose liver was transplanted into athird patient.3 In this procedure, an in situ split was safelyperformed in a living patient with FAP without detriment tothe subsequent cadaver graft, transplanting the right and lefthemilivers to 2 adults.
In situ splitting in a living donor adds dimensions ofrapidity and risk to the technical challenge that are notpresent with a cadaver donor. In situ splitting in cadaverdonors can also be performed potentially for 2 adults,4 but inour case, marginal donor liver function precluded theprocedure. Nonetheless, the ultimate message of this report isthat the cadaver donor has the potential to yield 2 livers.When the transplant world routinely understands that theliver is a paired organ, then we can also compensate for theshortage of donors for adults.
References
1. Yamaoka Y, Washida M, Honda K, Tanaka K, Mori K,Shimahara Y, et al. Liver transplantation using a right lobe graftfrom a living related donor. Transplantation 1994;57:1127-1130.
2. Rogiers X, Malago M, Gawad K, Jauch KW, Olausson M, KnoefelWT, et al. In situ splitting of cadaveric livers. The ultimate expansionof a limited donor pool. Ann Surg 1996;224:331-341.
3. Furtado L, Oliveira F, Furtado E, Geraldes B, Reis A, Viana J,et al. Maximum sharing of cadaver liver grafts: Composite splitand domino liver transplants. Liver Transpl Surg 1999;5:157-158.
4. Colledan M, Andomo E, Valente U, Gridelli B. A new splittingtechnique for liver grafts [letter]. Lancet 1999;353:1763.
From the Centre Hepatobiliaire, Hopital Paul Brousse, Universite deParis Sud and Assistance Publique-Hopitaux de Paris, Villejuif, France.
Address reprint requests to Henri Bismuth, MD, FACS (Hon), CentreHepatobiliaire, Hopital Paul Brousse, 12 ave Paul Vaillant Couturier,Villejuif F-94804, France.
Copyright r 2000 by the American Association for the Study ofLiver Diseases
1527-6465/00/0602-0027$3.00/0
Liver Transplantation, Vol 6, No 2 (March), 2000: pp 239-240 239

Figure 1. ‘‘One liver for three’’ using domino transplantation and in situ splitting.
Azoulay et al240