Embed Size (px)
Citation preview

Peter Dreger Dept. Internal Medicine V
University of Heidelberg
Gent 25.01.2013
Transplantation
in CLL

Allogeneic SCT
= initiation of a permanent
immunotherapeutic process!
graft-vs-tumor effect (GVT/GVL)
Autologous SCT
= supportive measure to compensate
hematopoietic toxicity of single-hit
high-dose therapy

Months from randomisation Months from randomisation
TTRT
ASCT observation
PFS

PFS TTRT OS
FCR
auto


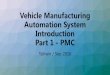
The European Group for Blood and Marrow Transplantation
0
50
100
150
200
250
300
350
400
20002001
20022003
20042005
20062007
20082009
2010
allo auto
EBMT: SCT for CLL 2000-2010 Update January 2012

The European Group for Blood and Marrow Transplantation
0
50
100
150
200
250
300
350
0
50
100
150
200
250
300
350
0
200
400
600
800
1000
1200
1400
1600
1800
Transplant activity for lymphoma
EBMT 2000-2010
auto
allo
Absolute numbers 2010 % increase 2000 -> 2009
CLL HL TCL DLC
L
FL MCL
DLCL HL MCL TCL FL CLL
-100
-50
0
50
100
150
Total lymphoma transplants 2010 (with CLL): allo 1732; auto 5891

The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation
- Do GVL effects exist?
- Therapeutic benefit?
- Indications?
CLL and alloSCT:
Key questions

alloSCT for CLL: MRD response patterns
A: MRD- after CSA taper
CSA taper
GVHD
Ritgen et al, Leukemia 22:1377 (2008)

alloSCT for CLL: MRD response patterns
A: MRD- after CSA taper
CSA taper
GVHD
Dreger et al, Blood 116:2438 (2010)
MRD- immediately
after SCT (16%)
MRD- after CSA
taper (42%)
Other pattern
(42%)
Ritgen et al, Leukemia 22:1377 (2008)
CLL3X (n=52)

alloSCT for CLL: MRD response patterns
Dreger et al, Blood 116:2438 (2010)
MRD- immediately
after SCT (16%)
MRD- after CSA
taper (42%)
Other pattern
(42%)
Hahn et al, EBMT 2013
CLL3X (n=52)
MRD- immediately
after SCT (34%)
MRD- after CSA
taper (35%)
Heidelberg 2005-2012
(n=62)

Are MRD responses durable?
Results from landmark analyses

113
100
90
13 ineligible (no CLL, late
registration, comorbidity etc.)
10 no SCT (Richter‘s, ED,
no donor, refusal)
38 no continuous
MRD sampling
52 13 event <12mo,
CLL3X: Patient flow (MRD)
27 MRD-neg
at +12mo
11 MRD-pos
at +12mo
1 no MRD
at +12mo

CLL3X 6-year follow-up: Relapse
by MRD negativity at +12mo (of 38 patients with MRD monitoring and event-free at mo +12)
12 36 60 84 1080
50
100 +12 MRD+ (10)
+12 MRD- (28)
HR 26.2 (6-115); p 0.0001
Months from SCT
Perc
en
t re
lap
sed
Clinical Relapse MRD or clinical relapse
36 60 84 1080
50
100
16% (95%CI 1-50)
Months from SCT
Perc
en
t M
RD
or
clin
ical re
lap
se
ASH 2012, abstract #966 Dreger et al

ASH 2012, abstract #966 Dreger et al
12 36 60 84 108
0
50
100
16% (95%CI 1-51)
17p-
TP53 mut
NOTCH1 mutSF3B1 mut
no marker
Months from SCT
Pe
rce
nt
no
t in
MR
D-n
eg
ati
ve
clin
ical re
mis
sio
n
CLL3X 6-year follow-up: Relapse
by MRD negativity at +12mo (of 38 patients with MRD monitoring and event-free at mo +12)

53 3 no continuous
MRD sampling
Heidelberg 2005-2012: Patient flow (MRD)
3 MRD-neg
at +12mo
after REL
2 MRD-pos
at +12mo
after REL
9 MRD-pos
and ev.-free
at +12mo
66 13 too early
7 TRM
29 MRD-neg
and ev.-free
at +12mo
58% (29 of 50)
6% 18% 4%
14%
Hahn et al, EBMT 2013
50
43

Heidelberg CLL 2005-2012:
Relapse by MRD negativity at +12mo (of 38 patients with MRD monitoring and event-free at mo +12)
12 36 60 84
0
25
50
75
100 +12 MRD+ (9)
+12 MRD- (29)
p<0.0001
Months from SCT
Perc
en
t re
lap
sed
Clinical Relapse MRD relapse of patients MRD- at 12months
12 36 60 84
0
50
100
7% (95%CI 0-68)
Months from SCT
Perc
en
t M
RD
rela
pse
Hahn et al, EBMT 2013

Clinical impact of MRD negativity at the
+6mo landmark (Milan data)
Farina et al, Haematologica 94:654 (2009)

The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation
- Do GVL effects exist?
yes. Even in poor-risk disease.
- Therapeutic benefit?
- Indications?
CLL and alloSCT:
Key questions

PFS after RIC alloSCT for CLL
Study GCLLSG Seattle Boston FCGCLL Houston
n 90 82 76 40 86
PFS 38% (6y) 39% (5y) 43% (5y) 46% (3y) 36% (5y)
OS 58% (6y) 50% (5y) 63% (5y) 55% (3y) 51% (5y)
NRM 23% (6y) 23% (5y) 16% (5y) 27% (3y) 17% (1y)
Ext. cGVHD 55% 49-53% 64% 42% 56%
F/U mo 72 (7-129) 11-87 61 28 (3-71) 37(11-131)
0 24 48 72 96 1200
50
100
6-y EFS 38% (27, 48)
Months from SCT
Perc
en
t E
FS
GCLLSG ASH 2012; Sorror JCO 2008; Brown Leukemia 2012;
Michallet Exp Hematol 2012; Khouri Cancer 2011

What does that mean in
real life?

I Herth, U Hegenbart, S Dietrich, M Rieger, P Stadtherr, A Bondong, H
Tran, T Zenz, AD Ho, P Dreger
Dept Medicine V, University of Heidelberg, Germany
First evidence that alloSCT can improve the natural
course of poor-risk CLL as defined by the EBMT
consensus criteria:
A retrospective donor vs no donor comparison.

Department of Internal Medicine V
• Design:
Single center retrospective analysis
• Patient eligibility:
All consecutive patients referred
for alloSCT for CLL between June
2005 and July 2011
to the University of Heidelberg
Study design and patients

Department of Internal Medicine V
Eligibility for donor search was either
one of the three EBMT consensus criteria
or
Richter‘s transformation.
• symptomatic 17p-
• fludarabine refractoriness (non-response or relapse within 6 months after the last cycle)
• early relapse after intensive pretreatment (relapse after intensive treatment like FR, FCR, BR, R-CHOP or similar later
than 6 months but within 2 years)

Department of Internal Medicine V
Study population:
patients for whom a 9/10 or 10/10
matched related or unrelated donor could
be found within 3 months
Control population:
patients without 9/10 or 10/10 matched
donor found within 3 months

Department of Internal Medicine V
Overall survival (OS),
measured from the 3-month
landmark after donor search
initiation
(to eliminate the early relapse-
mortality favoring the donor group).
Primary endpoint

Department of Internal Medicine V
Donor
search
indication
(=EBMT risk
or Richter’s)
?
B
Observe OS
yes
Observe OS
8 lost w/i
3 months (6 dead PD, 1
refusal, 1 lost
to f/u)
Heidelberg donor vs no-donor CLL study Patient flow
134 113
3
105 SEARCH
8 No
search 5 refusal,
1 comorbidity,
2 lost to f/u R
E
F
E
R
R
A
L
no
21
MCL 2,
MZL 1
donor 9/10
within 3 Mo
83
no donor 9/10
within 3 Mo
14
Herth et al, EBMT 2012

0 12 24 36 48 60 720
25
50
75
100
p 0.011 ; HR 3.85 (1.36-10.8)
donor yes (83)
donor no (14)
55% (33-85)
78% (65-86)
Months from 3 month after start of search
Perc
en
t alive
Overall survival from 3 months after start of donor
search by donor availability (all patients with donor search completed, n = 97)
Follow-up 25 (0.5-80) months
Medizinische Klinik V
Herth et al, EBMT 2012

Variable Hazard
ratio Lower CL Upper CL p
Donor yes 0.29 0.15 0.65 0.003
Previous therapies >2 2.88 1.33 6.26 0.008
Age per decade 0.55 0.32 0.94 0.03
Donor availibility and overall survival:
Multivariate analysis Patients with completed search (3-months landmark), n=97
Variables not remaining in the model:
Search indication (EBMT criterion), Binet stage
Herth et al, EBMT 2012

0 12 24 36 48 60 720
25
50
75
100
p 0.011 ; HR 3.85 (1.36-10.8)
donor yes (83)
donor no (14)
55% (33-85)
78% (65-86)
Months from 3 month after start of search
Perc
en
t alive
Long-term survivors in no-donor group Medizinische Klinik V
m, 55y, early relapse,
5th-line treatment
m, 51y, fludara-refr.,
SCT (late donor),
a&w 55+ months
m, 57y, 17p-,
SCT (2mm donor),
a&w 75+ months
Herth et al, EBMT 2012

The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation
- Do GVL effects exist?
yes.
- Therapeutic benefit?
Yes! Even in poor-risk disease.
-> …but at what price?
- Indications?
CLL and alloSCT:
Key questions

Study GCLLSG Seattle Boston FCGCLL Houston
n 90 82 76 40 86
Mucositis 3-4 6% 12% na <5% na
Infection 3-4 55% 60% na 48% na
Early death (< d +100)
<3% <10% <3% 0% 3%
NRM 23% (6y) 23% (5y) 16% (5y) 27% (3y) 17% (1y)
Ext. cGVHD 55% 49-53% 48% 42% 56%
F/U mo 72 (7-129) 11-87 61 28 (3-71) 37(11-131)
Toxicity of RIC alloSCT for CLL
GCLLSG ASH 2012; Sorror JCO 2008; Brown Leukemia 2012;
Michallet Exp Hematol 2012; Khouri Cancer 2011

The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation
NRM (%) by age groups
0%
10%
20%
30%
40%
50%
60%
100d 6 m 12 m
18-50 yo 51-60 yo 61-70 yo
Lymphoma Registry: Allo-SCT ’06-’10

25% of allografted patients
will suffer from QOL-relevant
chronic GVHD,
but…

0 120 240 360 480 600 720
0
20
40
60
80
100
cGVHD cum. incidence:67% at 12months
cGVHD prevalence:52% at 12months
on immunosuppression:39% at 12months
Days from SCT
Perc
en
t w
ith
cG
VH
D
his
tory
Heidelberg CLL 2005-2012:
Chronic GVHD over time (n=66)
Hahn et al, EBMT 2013

Seattle CLL trial: OS and chronic
GVHD by donor (n=82)
Sorror et al, JCO 26:4912 (2008)
After 5 years, 76% of living patients are off immunosuppression

The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation The European Group for Blood and Marrow Transplantation
- Do GVL effects exist?
yes.
- Therapeutic benefit?
Cure! Even in poor-risk disease.
But 15-25% 2y-NRM.
- Indications?
CLL and alloSCT:
Key questions

EBMT CLL transplant consensus
allo-SCT is a reasonable treatmentoption in poor-risk CLL:– .Relapse <24 mo after intensive treatment
(purine analogue combinations or auto-SCT)
– .p53 mutation with treatment indication
– .Non-response or early relapse (<12 mo) afterpurine analogue-based therapy(= fludarabine resistance)
VERY
HI
GH
HI
GH
RISK
Leukemia 21:12-17 (2007)
Still valid in 2013?

EBMT CLL Transplant Consensus 2013
- Is poor-risk CLL still poor risk?
- Can alloSCT improve the outcome of
poor-risk CLL?

EBMT CLL Transplant Consensus 2013
- Is poor-risk CLL still poor risk? - 17p-

1st-line treatment results in 17p- CLL
Overall response Median PFS (mo)
CLL
HL
DLCL
FL
MCL
Hallek 2010, Wierda 2011, Hillmen 2007, Stilgenbauer 2012, Badoux 2011, Fischer 2012
0
20
40
60
80
100
R-
FC
O-
FC
CD52 Lena CD52-
Dexa
0 12 24 36 48
R-FC
O-FC
CD52
Lena
CD52-D
R-B
R-Benda
*
* 27% of patients received alloSCT consolidation

EBMT CLL Transplant Consensus 2013
- Is poor-risk CLL still poor risk? - 17p-
- PA refractory

Treatment results in PA-ref CLL
Overall response Median PFS (mo)
CLL
HL
DLCL
FL
MCL
Badoux 2011a, Fischer 2011, Wierda 2010, Stilgenbauer 2012, Badoux 2011b; Lanasa 2010
0
20
40
60
80
100
R-
FC
R-
Ben
da
Ofa Flavo CFAR 0 12 24 36
R-Benda
CD52-D
Ofa
Flavo
CFAR
CD52
R-FC

EBMT CLL Transplant Consensus 2013
- Is poor-risk CLL still poor risk? - 17p-
- PA refractory
- Relapse within 2 years after intensive therapy

Overall survival after 1st salvage after
FC/FCR 1st-line failure: CLL8 data
PFS >24 months
Zenz et al, ASH 2010
OS from 2nd-line therapy (months)
PFS <6 months
PFS 12-24 months
PFS 6-12 months

EBMT CLL Transplant Consensus 2012
- Is poor-risk CLL still poor risk?
yes, but

BCR kinase inhibitors:
Is the Gleevec of CLL
approaching?

CLL: B cell receptor signaling downstream
kinase targets and inhibitors
Wiestner et al, Blood Dec 6, 2012

Risk group n Response rate
All patients 61 67% (CR 2%)
PA-refractory 28 61%
17p- 20 65%
Bruton’s tyrosine kinase inhibitor Ibrutinib:
Phase Ib/II study in rel./ref. CLL (O’Brien et al, ASH 2011)
17p Del No (n=36)
17p Del Yes (n=20)
Median follow-up 9-12mo

PCYC-1102-CA
Progression-free Survival
Data cut-off of 19OCT2012
R/R + High-Risk R/R (n=85)
Est. PFS at 26 mo is 75%
Months on Study
+ Censored
Logrank p=0.0256
0 5 10 15 20 25
1.0
0.8
0.6
0.4
0.2
0.0
PF
S P
robabili
ty
50
Relapsed/Refractory patients
(n=85; 24 of them relapsed <24mo after immunohemotherapy)
ASH 2012, abstract #188 Byrd et al

PCYC-1102-CA
Patient Characteristics
TN ≥65 yrs (N=31)
R/R + HR (N=85)
Age, years Median (Range)
71 (65 – 84)
66 (37 – 82)
Fludarabine refractory - 48%
Prognostic Markers, % IgVH unmutated del(17p13.1) del(11q22.3)
55% 7% 3%
85% 35% 39%
51
ASH 2012, abstract #188 Byrd et al

PCYC-1102-CA
Progression-free Survival
del(17p13.1)/del(11q22.3) Status
Months on Study
Data cut-off of 19OCT2012
del17p (n=28)
Est. PFS at 26 mo is 57%
del11q (n=23)
Est. PFS at 26 mo is 73%
No del17p or del11q (n=29)
Est. PFS at 26 mo is 93%
1.0
0.8
0.6
0.4
0.2
0.0
PF
S P
rob
ab
ility
0 5 10 15 20 25
52
Relapsed/Refractory including High-Risk R/R
+ Censored
Logrank p=0.0437
ASH 2012, abstract #188 Byrd et al

PCYC-1102-CA
Progression-free Survival
del(17p13.1)/del(11q22.3) Status
Months on Study
Data cut-off of 19OCT2012
del17p (n=28)
Est. PFS at 26 mo is 57%
del11q (n=23)
Est. PFS at 26 mo is 73%
No del17p or del11q (n=29)
Est. PFS at 26 mo is 93%
1.0
0.8
0.6
0.4
0.2
0.0
PF
S P
rob
ab
ility
0 5 10 15 20 25
53
Relapsed/Refractory including High-Risk R/R
+ Censored
Logrank p=0.0437
Months0 6 12 18 24 30 36 42 48 54
0.0
0.2
0.4
0.6
0.8
1.0
CLL2O: Progression free survival
F-refr.: n = 61
17p- relapse: n = 28
17p- 1st-line: n = 42
ASH 2012, abstract #188 Byrd et al
ASH 2012, abstract #716 Stilgenbauer et al

• Superior disease control in poor-risk
CLL
• Low tox
• Virtually no CRs/mCRs, continuous
progressions in 17p- CLL
• Do they make SCT unnecessary - or
do they help getting patients to
transplant?
BCR kinase inhibitors (Ibrutinib):
The Gleevec of CLL?
↑
↓
↑
?

EBMT CLL Transplant Consensus 2013
- Is poor-risk CLL still poor risk?
yes - but might be re-shaped once the
therapeutic value of BCR kinase
inhibitors has been defined
- Can alloSCT improve the outcome of
poor-risk CLL?

EBMT CLL Transplant Consensus 2013
Can alloSCT improve the outcome of
poor-risk CLL? - 17p-

Allo-SCT in CLL: Effect of del 17p-
EBMT (retrospective; n=44)
Schetelig et al, JCO 26:5094-5100 (2008)

Allo-SCT in CLL: Effect of del 17p-
EBMT (retrospective; n=44) CLL3X (prospective;
17p- + TP53mut; n=24)
12 MRD-negative at 12mo landmark
MRD-negative at last f/u
Schetelig et al, JCO 26:5094-5100 (2008) Update June 2012
0 24 48 72 96 1200
50
100
TP53 del and/or mut (24)
TP53 normal (49)
1212
*
12
*1212
*12
12
*12
*12
*1212
Months from SCT
Perc
en
t even
t-fr
ee
*

EBMT CLL Transplant Consensus 2013
Can alloSCT improve the outcome of
poor-risk CLL? - 17p-
- PA refractory

Study GCLLSG Seattle Boston FCGCLL Houston
n 90 82 76 40 86
Higher age ++ (>55) - ++ (>65) - -
HCT-CI na ++ ++ (>0) na -
Unrelated
donor - - - na -
PA ref - - - na na
Active / bulky
CLL at SCT ++ ++ ++ - -
17p- - - - na na
Prognostic factors for PFS in RIC alloSCT for
CLL: Focus on purine analogue refractoriness
GCLLSG ASH 2012; Sorror JCO 2008; Brown Leukemia 2012;
Michallet Exp Hematol 2012; Khouri Cancer 2011

EBMT CLL Transplant Consensus 2013
Can alloSCT improve the outcome of
poor-risk CLL? - 17p-
- PA refractory
- Relapse within 2 years after intensive therapy

Outcome of RIC alloSCT for CLL (by EBMT indication; Heidelberg 2005-2012, n=64)
0 12 24 36 48 60 72 840
20
40
60
80
100
p53 (22)
F-ref (26)
early rel (13)
Richter (3)
Months from Start of Seach
% P
FS
PFS OS
0 12 24 36 48 60 72 840
20
40
60
80
100
Months from Start of Search
% S
urv
ival
Hahn et al, EBMT 2013

EBMT CLL transplant consensus
allo-SCT is a reasonable treatmentoption in poor-risk CLL:– .Relapse <24 mo after intensive treatment
(purine analogue combinations or auto-SCT)
– .p53 mutation with treatment indication
– .Non-response or early relapse (<12 mo) afterpurine analogue-based therapy(= fludarabine resistance)
VERY
HI
GH
HI
GH
RISK
Leukemia 21:12-17 (2007)
Still valid in 2013 !

Conclusions:
- AlloSCT seems to have the potential to
improve the natural course of poor-risk
CLL
- The 2007 EBMT/ERIC CLL transplant
consensus is still valid in 2013
- New agents will hopefully improve but
probably not replace alloSCT

Many Thanks for Invitation and…
Med V
Heidelberg
M Rieger
F McClanahan
U Hegenbart
S Dietrich
M Hahn
I Herth
T Zenz
AD Ho
E Kimby
P Ghia
E Montserrat
C Moreno
EBMT
A van Biezen
H Finel
R Brand
K Cwynarski
D Niederwieser
M Michallet
D Milligan
T de Witte
J Schetelig
DCLLSG
M Ritgen
R Busch
T Zenz
M Hallek
S Böttcher
M Kneba
H Döhner
S Stilgenbauer