Embed Size (px)
Citation preview
Translational research
Catherine Gallagher andThe Cochrane Collaboration College for Policy
GMU

Definition of knowledge translation:
CIHR (2000) “the exchange, synthesis and ethically sound application of knowledge – within a complex system of interactions among researchers and users – to accelerate the capture of the benefits of research for the public through improved health, more effective services and products, and a strengthened health care system”

Definition of knowledge translation:
“process of moving what we learned through research to the actual applications…
….in a variety of practice settings and circumstances…...the interest in KT appears to coincide with the growing
engagement in the EBP approach, in which practitioners make practice decisions based on the integration of the research evidence with clinical expertise and the patient’s unique values and circumstances.
Straus, Richardson, Glasziou, & Haynes, 2005

Knowledge translation in a word
Goal of translational efforts:
Minimize the gap between the “bench and the bedside” Ensure the use of the best evidence for the best practice

Coinciding with knowledge translation movement
Increased:• rigor and standardization of all elements of the scientific process• burden of proof of utility of investigation• investigation into communication methods (dissemination sciences)• open access tools to summarize knowledge base, manage references • efforts to make available publicly funded research to the public• stakeholder involvement• joint decision making
It is impossible to separate it from Evidence-based Practice Movement

Why do we need it?
1. To make sense of knowledge proliferation10,000 new trials each year in MEDLINE350,000 new trials each year in Cochrane

Why do we need it?2. Public is not benefiting from evidence
30-40% of patients do not receive care according to present scientific evidence20-25% of care provided is not needed or potentially harmful
Grol & Grimshaw (2003) Lancet
3. Current publication practices do not speak language or format of decision makers (both societal and individual)

Why do we need it?
4. Ease some tensions, strike some balance:
Investigator interest : Social utilityTimeliness : ExhaustivenessSimplicity of design : Complexity of social worldGeneralizability : Local acceptabilityAcademic freedom : Costs to publicIncreases in standardization : Loss of natural variationQuantity of publications : Quality of reconciliation

What does it look like?
There are many models of the KT processCommonalities across models include:
1. Early and consistent stakeholder engagement2. Standardization of reporting requirements to maximize benefits of research efforts3. Concern with content delivery to public4. Iterative processes

What does it look like: Key themes
• Evidence-based• Implementation• Dissemination• Scaling-up• Evidence uptake• Importation
– Tools for assessing applicability and transferability of evidence

Figure 1. CIHR research cycle superimposed by the six opportunities to facilitate KT
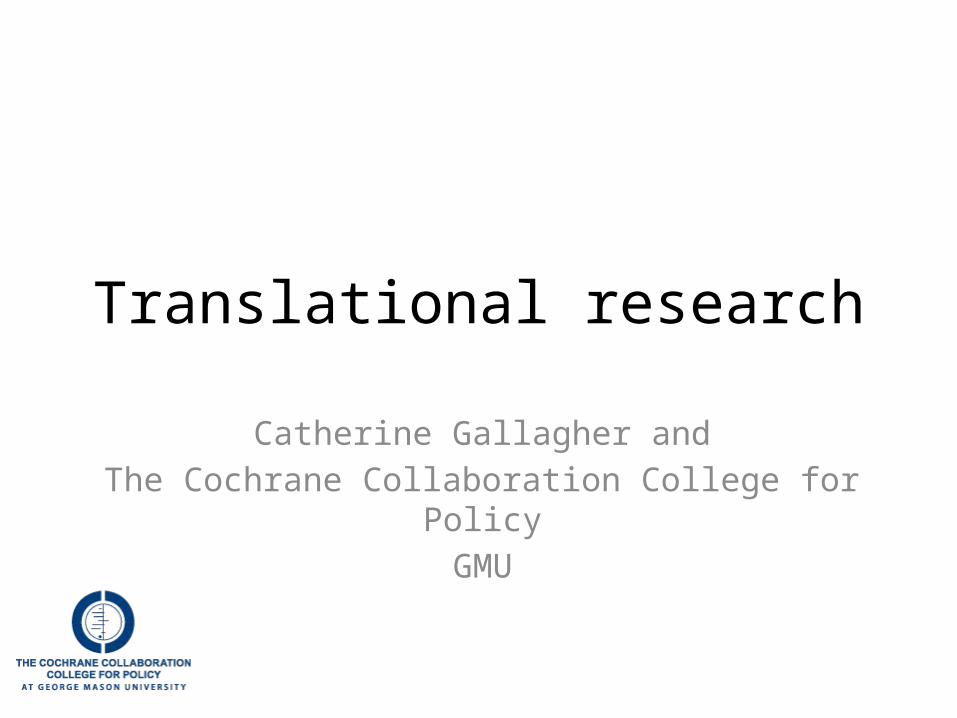
EDITORIALTranslational research
BMJ 2008; 337 doi: 10.1136/bmj.a863 (Published 28 August 2008)Cite this as: BMJ 2008;337:a863 M E J Lean et al

Figure 2. The Ottawa Model of Research Use


Moving from medicine to social science
1. Knowledge translation has better support structure in medical field

Clearer research stages and types
What are the different types of clinical trials?
Treatment trials test experimental treatments, new combinations of drugs, or new approaches to surgery or radiation therapy.
Prevention trials look for better ways to prevent disease in people who have never had the disease or to prevent a disease from returning. These approaches may include medicines, vaccines, vitamins, minerals, or lifestyle changes.
Diagnostic trials are conducted to find better tests or procedures for diagnosing a particular disease or condition.
Screening trials test the best way to detect certain diseases or health conditions.
Quality of Life trials (or Supportive Care trials) explore ways to improve comfort and the quality of life for individuals with a chronic illness.
Phases of clinical trials?
Clinical trials are conducted in phases. The trials at each phase have a different purpose and help scientists answer different questions:
In Phase I trials, researchers test an experimental drug or treatment in a small group of people (20-80) for the first time to evaluate its safety, determine a safe dosage range, and identify side effects.
In Phase II trials, the experimental study drug or treatment is given to a larger group of people (100-300) to see if it is effective and to further evaluate its safety.
In Phase III trials, the experimental study drug or treatment is given to large groups of people (1,000-3,000) to confirm its effectiveness, monitor side effects, compare it to commonly used treatments, and collect information that will allow the experimental drug or treatment to be used safely.
In Phase IV trials, post marketing studies delineate additional information including the drug's risks, benefits, and optimal use.
From: http://clinicaltrials.gov/ct2/info/understand

Question formulation tends to be standardized
For interventions, for example PICO (TS)
Population (participants)InterventionComparatorOutcome
Time (duration)Study design (experimental / observational, N)

Infrastructure
• Clinical trials registry (clinicaltrials.gov)• Registry of RCTs (Cochrane registry of studies)• Registry of studies (Embase, Medline)• Meta thesasarus (Medical Subject Headings
(MeSH®)
Allows for standardization and natural variationRequires greater organization of individual research
programs

Medical field has greater standardization on research
reporting CONSORT: Consolidated Standards of Reporting Trials
GRADE: Grading of Recommendations Assessment, Development and Evaluation
AMSTAR: Assessment of multiple systematic reviews
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses

Cochrane Collaboration “Summary of findings table”Uses GRADE scale for quality of evidence (in addition to confidence interval)

Importation tools:Assessment of Applicability & Transferability
PUBLIC INVOLVEMENT
Applicability/feasibility of importing practice– Political acceptability– Social acceptability– Available essential resources– Organizational expertise
Transferability/generalizability of practice– Absolute magnitude of problem (baseline prevalence)– Reach to target population– How great are the differences in culture, health, system's between studied populations and practice
population in question
– See Buffet, C., Ciliska, D., & Thomas, H. (2011). It worked there. Will it work here? Tool for Assessing Applicability and Transferability of Evidence (A: When considering starting a new program). Hamilton, ON: National Collaborating Centre for Methods and Tools.
National Collaborating Centre for Methods and Tools, McMaster University

Medical networks for incorporating evidence into decision making
DEcIDE Network Developing Evidence to Inform Decisions about Effectiveness Network
From AHRQ: These centers gather new knowledge and information on specific treatments. The DEcIDE Network conducts studies on the outcomes, effectiveness, safety, and usefulness of medical treatments and services.

Concern with display of findings
From David Speigelhalter

Drug facts box




‘risk balance’

But what about the medicalisation of
1000 people?

Concern with how to reach audiences
WHO Alliance for Healthcare InformationLancet series on Research into Practice,
Grimshaw and Grol:


Concern with how to reach audiences
WHO Alliance for Healthcare InformationLancet series on Research into Practice,
Grimshaw and Grol:

CONCLUSIONS
For criminology….

Translational approaches create new environment
1. Allow for more business-like view
– Specify all steps in the processes • tacit or explicit
– Adopt incrementally • discrete program area versus global take over
– Reduce redundancies, unnecessary steps– Document and share processes, eliminate excess– Use protocols for operations– Extract and share expertise– Create Internal competency banks
HBR: Lean business principles in knowledge work

Translational approaches create new environment
2. Considers outcomes in social utility and return on investment before the start of the study
Evidence 2011, Patrick MM Bossuyt
Question Feature
Is it true? Analytical Validity
Is it meaningful? Clinical Validity
Is it useful? Clinical Utility

Translational approaches create new environment
3. Emphasizes how to communicate findings
• Accurately depicts benefits, harms, costs• Tailored to consumer• True aid in decision-making

Translational approaches create new environment
4. Changes innovation balance
• Investigator initiated and• Field demand
– Democratized methods– Stakeholder input
Less tolerance for bench science without clear social utility and with incongruent findings

Conclusions about our field
As methodology improves, so does:Narrative about discrepant findingsQuantitative synthesis of findings
Standards settingCommon language and measurementWithout crushing natural variation