Embed Size (px)
Citation preview

00226347/97/1576-2252$03.00/0 THE JOURNAL OF U~LOGY copyright Q 1997 by AMERICAN UROLOGICAL. Assocu~~oN, INC.
Vol. 157,2252-2253. June 1997 Printed in U.S.A.
TRANSITIONAL CELL CARCINOMA ARISING FROM A FIBROEPITHELIAL URETERAL POLYP IN A PATIENT WITH
DUPLICATED UPPER URINARY TRACT ANASTASIOS ZERVAS, GEORGE RASSIDAKIS, LYDIA NAKOPOULOU, DIONISIOS MITROPOULOS
AND CONSTANTINOS DIMOPOULOS From the Departments of Urology and Pathology, University of Athens, Laiko General Hospital, Athens, Greece
KEY WORDS: ureter; polyps; carcinoma, transitional cell
The fibroepithelial polyp is a rare but the most frequently described benign neoplasm of the ureter.' Although its patho- genesis remains unclear, most investigators agree that it arises from elements of mesodermal origin within the ure- teral wall.' The association of the fibroepithelial polyp with a ureteral carcinoma is extremely rare.1.2 To our knowledge this is the second report of a transitional cell carcinoma arising from the epithelium covering a ureteral fibroepithe- lial polyp and the first with coexisting congenital abnormal- ities of the genitourinary tract.
CASE REPORT
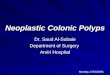
A 38-year-old man presented to our hospital because of asymptomatic unilateral hydronephrosis discovered ultra- sonographically during a routine examination. There was no history of gross hematuria or urinary tract infection. Physi- cal examination, urinalysis and routine blood studies were normal. Excretory urography showed a unilateral duplicated upper urinary tract as well as a large filling defect in the distal third of the left ureter, which expanded to the bladder in the left ureteral orifice area (fig. 1). At cystoscopy a pap- illary tumor protruded from the left ureteral orifice. Total
Accepted for publication November 15, 1996.
nephroureterectomy with excision of a bladder cuff was per- formed. Gross pathological analysis revealed a 4 cm. in max- imum diameter polypoid mass attached by a narrow stalk to the ureteral wall. Histological examination showed a super- ficial noninfiltrating low grade transitional cell carcinoma arising from the epithelium of a large benign fibroepithelial polyp (fig. 2). In addition, the mucosa from the left renal pelves, ureters and bladder revealed different degrees of papillary epithelial hyperplasia with foci of mild or moderate dysplasia.
DISCUSSION
Ureteral fibroepithelial polyps are rare neoplasms. Bolton et al reviewed 116 cases and recognized 2 distinct groups, adult and pediatric, suggesting a different pathogenesis for each group.' These lesions can occur at any age, and the majority of cases present with hematuria and/or flank pain.13 Chronic irritation and inflammation due to extrinsic agents (urinary crystals, calculi and so forth) have been sug- gested as possible causes, while only 5% of the reported cases had bacteriological evidence of a urinary tract infection.'. 3 Except for the acquired pathogenesis, a congenital origin of these polyps has also been proposed, which is supported by the fact that the lesions have been described in children, even in a neonate, and in the absence of inflammatory changes or other predisposing factors.'-3 According to a hypothesis the polyp might be an attempt to abort the duplication of the ureter,3 which is strongly supported by our case in which additional multiple congenital defects of the urinary tract were detected. The potential for malignant transformation of a fibroepithelial polyp is extremely rare.' To our knowledge this is the second report of a transitional cell carcinoma
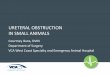
FIG. 2. Histological study of olyp demonstrates abundant fibrous strorna covered by transitionay epithelium from which superficial noninfiltrating low grade transitional cell carcinoma arises. Arrows show most prominent foci of latter neoplasm. H & E, reduced from x30.
FIG. 1. Excretory urography reveals large well-defined filling de- fect in distal third of inner left ureter expanding to bladder at left ureteral orifice area. Multiple papillary projections arise from lesion.
2252

TRANSITIONAL CELL CARCINOMA ON URETERAL FIBROEPITHELIAL POLYP 2253
arising from the epithelium of a benign ureteral polyp. The extensive papillary epithelial hyperplasia with dysplastic foci found at histological examination could indicate a malignant potential of the epithelium along the entire urinary tract. These microscopic findings do not allow speculation that the fibroepithelial polyp by itself could predispose to carcinoma- tous transformation. Although benign ureteral polyps are best treated by local excision, total nephroureterectomy was necessary in this case because of coexisting malignancy.
REFERENCES
1. Bolton, D., Stoller, M. L. and Irby, P.: Fibroepithelial ureteral polyps and urolithiasis. Urology, 44. 582, 1994.
2. Davides, K. C. and King, L. M.: Fibrous polyps of the ureter. J. Urol., 115: 651, 1976.
3. Van Poppel, H., Nuttin, B., Oyen, R., Stessens, R., Van Damme. B. and Verduyn, H.: Fibroepithelial polyps of the ureter. Eti- ology, diagnosis, treatment and pathology. Eur. Urol., 12: 174, 1986.