Embed Size (px)
Citation preview
ToxicologyPaleerat Jariyakanjana, MD
Faculty of Medicine
Naresuan University
5 Jan 2015

Scope
General Management of Poisoned Patients
Acetaminophen
Organophosphorus and CarbamateInsecticides

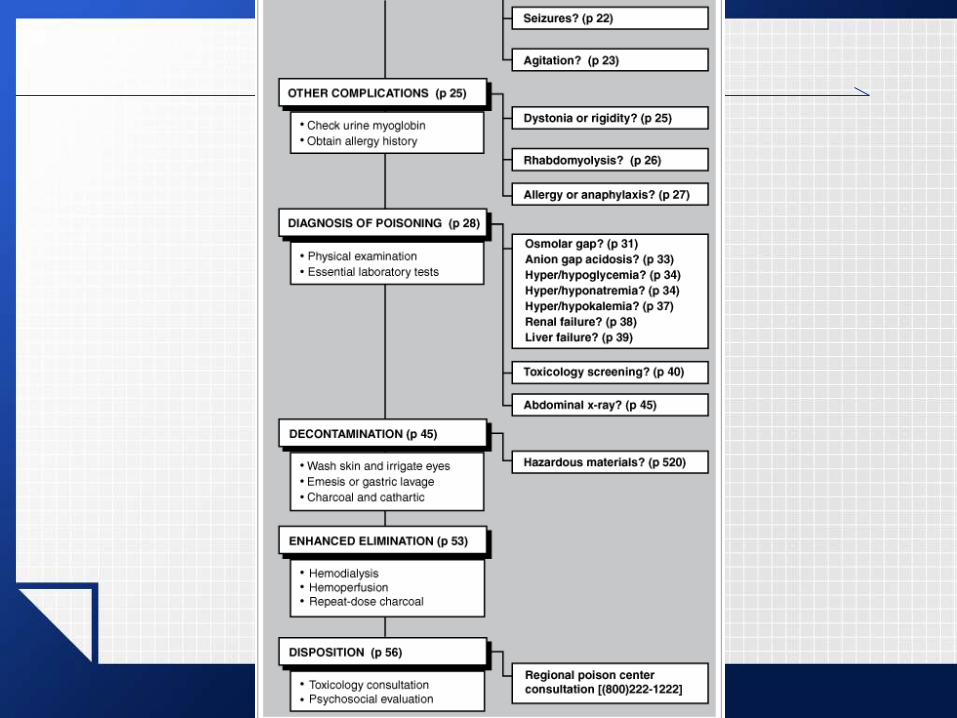

Diagnosis of Poisoning
History
Physical examination
Lab
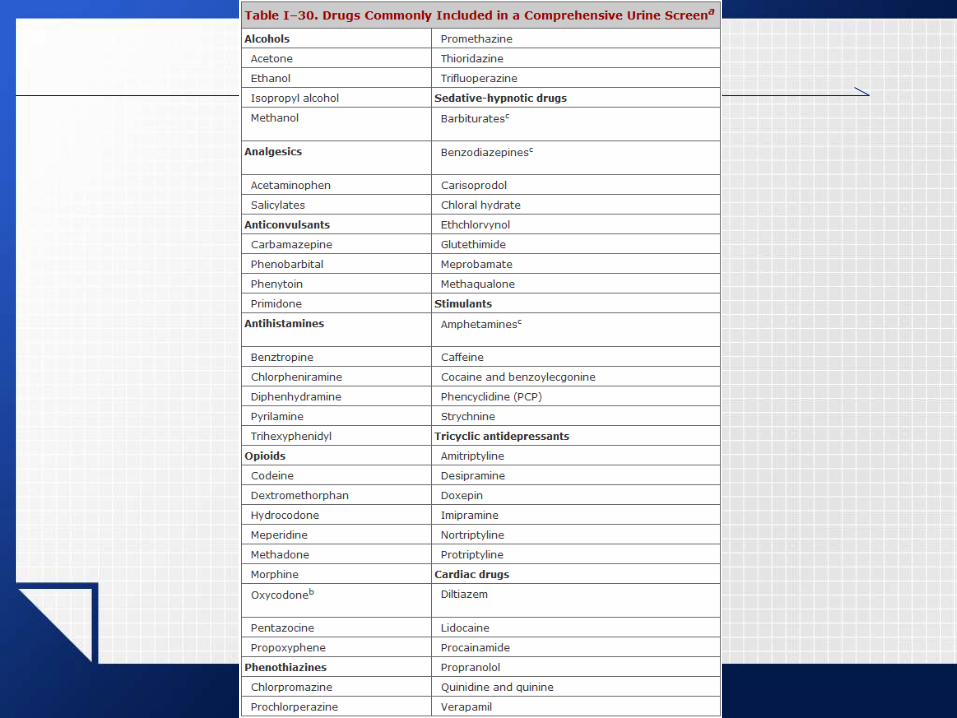
Toxicology screening
Abdominal x-rays

http://sketchymedicine.com/2012/01/toxidromes/

Essential clinical laboratory tests
1. Serum osmolality and calculation of the osmolar gap
2. e’: Na, K & AG
3. Serum glucose
4. BUN/Cr
5. LFT
6. CBC
7. UA: crystalluria, hemoglobinuria, or myoglobinuria
8. ECG
9. Stat serum acetaminophen level and serum ethanol level
10.UPT

Tintinalli's Emergency Medicine, 7e

Tintinalli's Emergency Medicine, 7e

Decontamination
Surface decontamination
Skin
Eyes
Inhalation
GI decontamination
Emesis
Gastric lavage
Activated charcoal
Cathartics
Whole-bowel irrigation
Other oral binding
agents
Surgical removal
Gastric lavage
not necessary for small-moderate ingestions of most substances if activated charcoal can be given promptly

Gastric lavage
Indications
massive overdose or particularly toxic substance + within 30–60 minutes
several hours after ingestion of agents that slow
gastric emptying (eg, salicylates or anticholinergic
drugs)
Contraindications
A. Obtunded, comatose, or convulsing patients
B. Ingestion of sustained-release or enteric-coated tablets
C. Use of gastric lavage after ingestion of a corrosive substance

Activated charcoal
Indications
≤4 hr
Drugs and Toxins Poorly Adsorbed by Activated Charcoal
AlkaliCyanideEthanol and other alcoholsEthylene glycolFluorideHeavy metals
Inorganic saltsIronLithiumMineral acidsPotassium
Activated charcoal
Contraindications
drowsy patient
Technique
60–100 g (1 g/kg), orally or by gastric tube
Whole-bowel irrigation
Indications
A. iron, lithium, or other drugs poorly adsorbed to activated charcoal
B. sustained-release or enteric-coated tablets
C. foreign bodies or drug-filled packets or condoms

Whole-bowel irrigation
Contraindications
A. Ileus or intestinal obstruction.
B. Obtunded, comatose, or convulsing patient unless the airway is protected.

Whole-bowel irrigation
Technique
bowel preparation solution (polyethylene glycol)
2 L/h by gastric tube (children: 500 mL/h or 35 mL/kg/h), until rectal effluent is clear

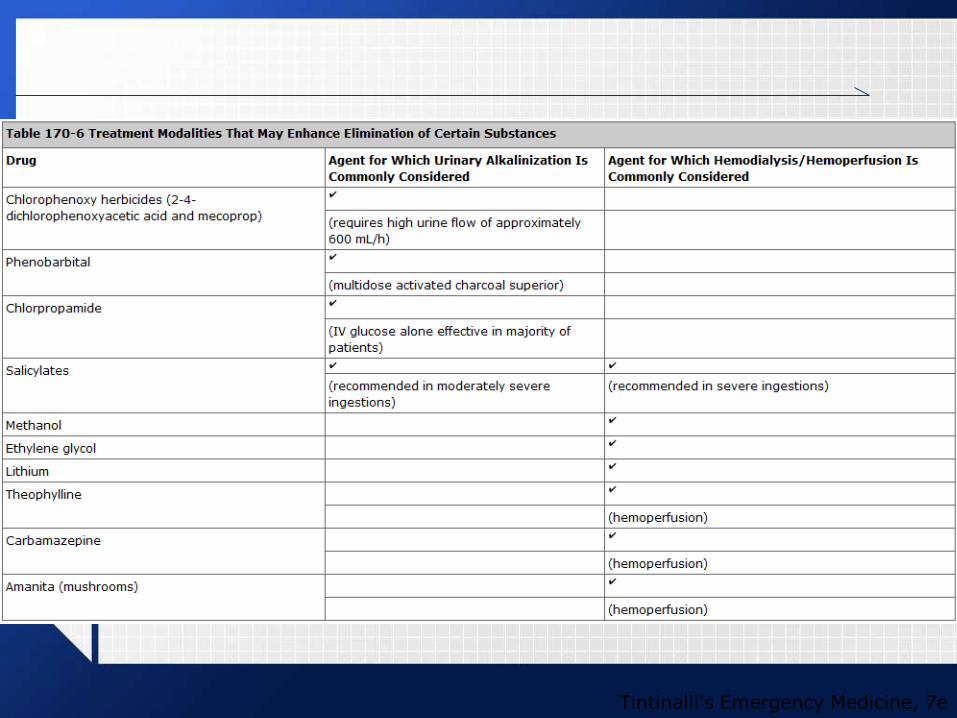
Enhanced Elimination
Urinary manipulation
Hemodialysis
Hemoperfusion
Peritoneal dialysis
Continuous renal replacement therapy
Repeat-dose activated charcoal
Urinary manipulation
Forced diuresis
Alkalinization
sodium bicarbonate: 1-2 mEq/kg IV bolus or
3-4 mEq/kg IV infusion over 1 hour
Keep urine pH 7.5-8.5
Tintinalli's Emergency Medicine, 7e

Repeat-dose activated charcoal
20–30 g or 0.5–1 g/kg every 2–3 hours
interrupting enterohepatic or enteroenteric recirculation of the drug or toxin

Disposition of the Patient
Emergency department discharge or intensive care unit admission?
Psychosocial evaluation

Acetaminophen


Toxic dose
Acute ingestion
>200 mg/kg in children or 6-7 g in
adults
Chronic toxicity
>200 mg/kg within 24-hr period
>150 mg/kg/d (or 6 g/d) x ≥2 d
>100 mg/kg/d (or 6 g/d) x ≥3 d
Diagnosis
many clinicians routinely order acetaminophen levels in all overdose patients regardless of the history of substances ingested
Diagnosis
Specific levels
1. acute overdose: 4-hour postingestionacetaminophen level
Obtain a second level at 8 hours if the 4-hour
value is borderline or if delayed absorption is
anticipated.
2. The nomogram should not be used to assess chronic or repeated ingestions.
Diagnosis
Other useful laboratory studies
electrolytes
glucose
BUN, creatinine
liver transaminases, bilirubin
PT/INR

Treatment
Emergency and supportive measures
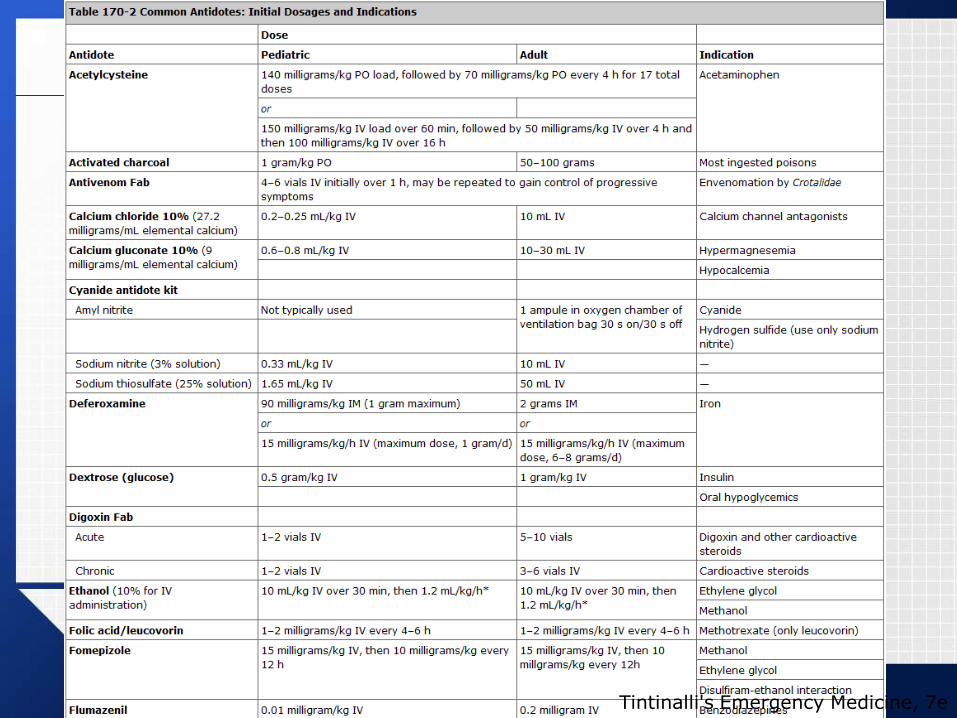
Specific drugs and antidotes

Emergency and supportive measures
ABC
Observe 4-6 hour

Specific drugs and antidotes
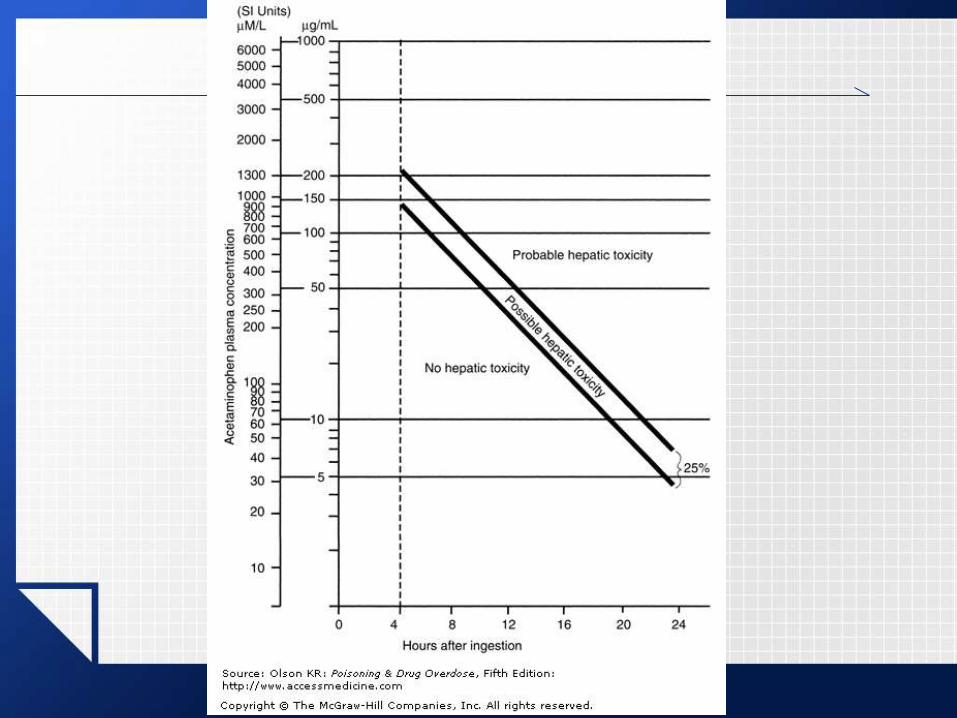
Acute single ingestion
Above the “possible toxicity” line
NAC
Maximum benefit if start within 8-10 hr
Extended-release tablets
Repeat the serum acetaminophen level at 8 &
12 hr
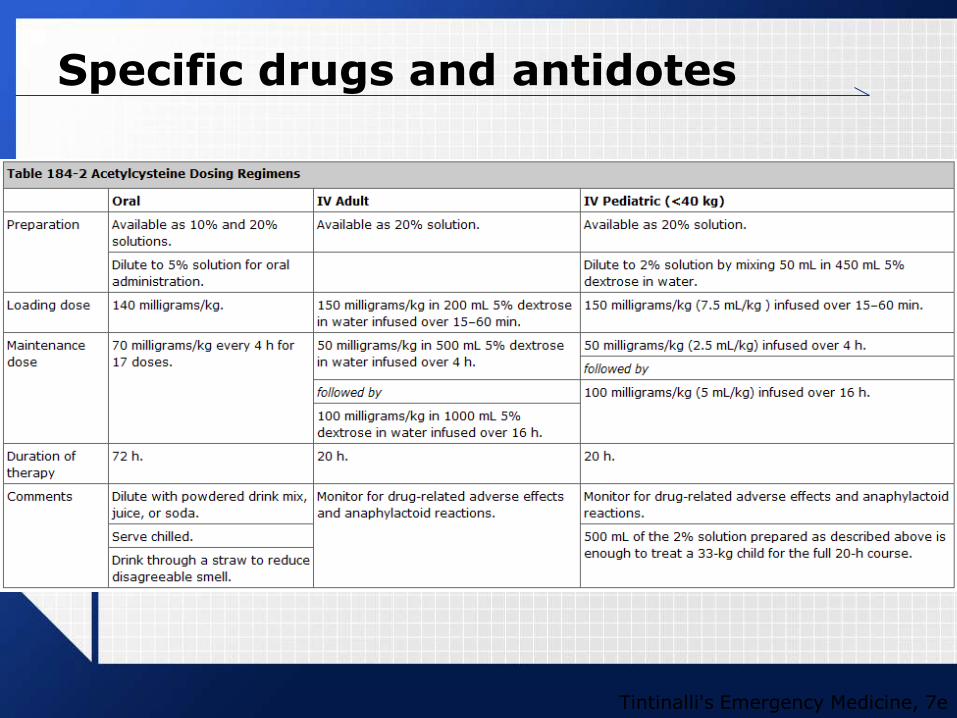
Specific drugs and antidotes
Tintinalli's Emergency Medicine, 7e

Specific drugs and antidotes
Specific drugs and antidotes
Duration of NAC treatment
If evidence of liver injury develops, NAC is
continued until liver function tests are
improving.

Decontamination
Activated charcoal
Gastric lavage

Enhanced elimination
Hemodialysis
effectively removes acetaminophen from the
blood
not generally indicated because antidotal
therapy is so effective
considered for massive ingestions with very
high levels (eg, >1000 mg/L) complicated by
coma and/or hypotension
Organophosphorus and Carbamate Insecticides

Clinical presentation
Tintinalli's Emergency Medicine, 7e

Clinical presentation
Nicotinic effects
muscle weakness and tremors/fasciculations
Central nervous system manifestations
agitation, seizures, and coma

Diagnosis
Specific levels
RBC AChE (red blood cell acetylcholinesterase)
PChE (plasma pseudocholinesterase)
blood, urine, gastric lavage fluid, and excretion for specific agents and their metabolites

Diagnosis
Other useful laboratory studies to consider
ABG
pulse oximetry
ECG
electrolytes, glucose, BUN, creatinine, lactic acid, CK, lipase and LFT
CXR
Treatment
Emergency and supportive measures
Specific drugs and antidotes
Emergency and supportive measures
ABC
Observe asymptomatic patients for ≥8–12 hours

Specific drugs and antidotes
atropine
2-5 mg IV initially, and double the dose administered every 5 minutes until respiratory secretions have cleared

Specific drugs and antidotes
Pralidoxime
Loading dose (30-50 mg/kg, total of 1–2 g in adults) over 30 minutes, followed by a continuous infusion of 8-20 mg/kg/h
continue 2-PAM for 24 h after the patient becomes asymptomatic, or at least as long as atropine infusion is required
not recommended for carbamateintoxication
if the exact agent is not identified and the patient has significant toxicity, pralidoxime should be given empirically
Decontamination
Skin and mucous membranes
Ingestion
activated charcoal
gastric lavage

Enhanced elimination
not indicated

Take home message
A: airway
B: breathing
C: circulation
D: decontamination
E: enhance elimination
Reference

ANY QUESTIONS?








![TOXICOLOGY CENTRE SELF-ASSESSMENT DOCUMENT Assessment_Report... · toxicopathology, inorganic biogeochemistry [later changed to analytical toxicology], and contaminant fate ... Toxicology](https://img.pdfslide.us/doc/110x75/5b42ffd97f8b9ab15f8b94bd/toxicology-centre-self-assessment-document-assessmentreport-toxicopathology.jpg)






![[Toxicology] toxicology introduction](https://img.pdfslide.us/doc/110x75/55c46616bb61ebb3478b4643/toxicology-toxicology-introduction.jpg)