-
7/30/2019 Toxic Responses to the Liver
1/18
TOXIC RESPONSES TO THE LIVER
-
7/30/2019 Toxic Responses to the Liver
2/18
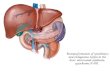
Liver Anatomy and Physiology
Liver- main organ where exogenous compounds
are metabolized and eventually secreted.
- Has multiple cell types and numerous
functions which can respond in many different
ways to acute and chronic insults.
-
7/30/2019 Toxic Responses to the Liver
3/18
-
7/30/2019 Toxic Responses to the Liver
4/18
-
7/30/2019 Toxic Responses to the Liver
5/18
Major functions of liver and consequences
of impaired hepatic function
Type of function Examples Consequences of
impaired function
Nutrient homeostasis Glucose storage and
synthesis
Cholesterol uptake
Hypoglycemia and
confusion
Hypercholesterolemia
Filtration of
particulates
Products of intestinal
bacteria (e.g.
Endotoxin)
Endotoxemia
Protein Synthesis Clotting factors
Albumin
Transport proteins
(e.g. VLDL)
Excess bleeding
Hypoalbuminemia
Fatty liver
-
7/30/2019 Toxic Responses to the Liver
6/18
Type of
function
Examples Consequences of
Impaired functions
Bioactivation
anddetoxification
Bilirubin and
ammonia
Steroid hormones
Xenobiotics
Jaundice,
hyperammonemia-relatedcoma
Loss of sec. Male sex
characteritics
Diminished drug
metabolism
Inadequate detoxification
Formation of
bile and
biliaryseretion
Bile acid-dependent
uptake of dietary
lipid and vitaminsBilirubin and
cholesterol
Metals (e.g. Cu and
Mn) Xenobiotics
Fatty diarrhea,
malnutrition, Vitamin E
deficiency jaundice,gallstones,hypercholester
olemia,
Mn-induced neurotoxicity
Delayed drug clearance
-
7/30/2019 Toxic Responses to the Liver
7/18
Types of hepatobiliary injury
Types of injury with damage Representative Toxin
Fatty liver,- build up of lipids in
the hepatocyte
Amiodarone, CCl4, ethanol,
fialurudine, tamoxifen, valproic
acid
Hepatotocyte death/necrosis Acetaminophen, allyl alcohol,
Cu,
dimethylformamide, ethanol
Immune-mediated response Diclofenal, ethanol, halothane,
tieniilic acidCanalicular cholestasis-decrease
in the volume of the bile formed
or an impaired secretion of
solutes into bile
Cyclosporin A, 1,1-
dichloroethylene, estrogens, Mn,
phalloidin
-
7/30/2019 Toxic Responses to the Liver
8/18
Bile duct damage Alpha-napthylisothiocyanate,
amoxicillin, methylene dianiline,
sporidesmin
Sinusoidal disorders Anabolic steroids,
cyclophosphamide, microcystin,
pyrrolizidine alkaloids
Fibrosis and cirrhosis CCl4, ethanol, thioacetamide,
vitamin A, vinyl chloride
Tumors Aflatoxin, androgens, arsenic,
thorium dioxide, vinyl chloride
-
7/30/2019 Toxic Responses to the Liver
9/18
-
7/30/2019 Toxic Responses to the Liver
10/18
-
7/30/2019 Toxic Responses to the Liver
11/18
Mechanisms of toxin induced injury to liver cells
include lipid peroxidation, binding to cell
macromolecules, mitochondrial damage,
disruption of the cytoskeleton and massive
calcium influx.
-
7/30/2019 Toxic Responses to the Liver
12/18
Canicular Cholestasis
Decrease in the volume of bile formed or an
impaired secretion of specific solutes into bile
Characterized by elevated serum levels of
compounds normally concentrated in bile,
particularly bile salts and bilirubin
-
7/30/2019 Toxic Responses to the Liver
13/18
Bile Duct damage
Cholandiodestructive cholestasis- damage into
the intrahepatic bile ducts which carry bile
from the liver to the GI tract
-indicator is increase levels of serum alkaline
phosphatase, bile slats and bilirubin
-
7/30/2019 Toxic Responses to the Liver
14/18
Sinusoidal disorders
sinusoids- are the channels between cords ofhepatocytes where
blood percolates on its way tothe terminal hepatic vein. The
sinusoids are madeup of tissues namely endothelial cells,
Kupffer
cells and stellate.Sinusoidal disorders due to Xenobiotic may
be
manifested as:
a. Blockade of its lumen
b. Dilation of lumen
c. Progressive destruction of its endothelial lining
-
7/30/2019 Toxic Responses to the Liver
15/18
Factors in the site-specific injury of
representative hepatotoxicantsSite Representative Toxicants
Potential Explanation for Site
Specificity
Zone 1 hepatocytes Fe Preferential uptake and high
oxygen levels
Zone 3 hepatocytes CCl4 More P450 isozyme for
bioactivation and less GSH for
detoxification
Acetaminophen More P450 isozyme for
bioactivation and less GSH for
detoxification
Alcohol More hypoxic and gresterimbalance in
bioactivation/detoxification
reaction
-
7/30/2019 Toxic Responses to the Liver
16/18
Bile duct cells Methylene dianiline,
sporidesmin
Exposure to the high
concentration of
reactive metabolites inbile
Sinusoidal
endothelium
Cyclophosphamide,
monocrotaline
Greater vulnerability to
toxic metabolites and
less ability to maintainglutathione levels.
Kupflerr cells Endotoxins Preferential site for
storage and then
engorgementStellate cells Vitamin A Preferential site
-
7/30/2019 Toxic Responses to the Liver
17/18
Examples of drugs with known
idiosyncratic hepatotoxicity
A. Immune mediated (allergic) idiosyncratic
hepatotoxicity
Diclofenac (analgesic)
Halothane (anesthetic)
Nitrofurantoin (antibiotic)
Phenytoin ( anticonvulsant) Tienilic acid (diuretic)
-
7/30/2019 Toxic Responses to the Liver
18/18
B. Non-immune mediated (non-allergic)idiosyncratic toxicity
Amiodarone (antiarrythmic) Bromfenac (analgesic)-withdrawn from
market
Diclofenac- (analgesic)
Disulfiram (alcoholism)
Isoniazid (antituberculosis)
Ketoconazole(antifungal)
Rifampicin( antimicrobial) Troglitazone( antidiabetic)
Valproate(anticonvulsant)