Embed Size (px)
Citation preview
CHAPTER 15
TOXIC RESPONSES OF THERESPIRATORY SYSTEM
Hanspeter R. Witschi and Jerold A. Last
LUNG STRUCTURE AND FUNCTION
Nasal PassagesConducting AirwaysGas-Exchange RegionGas Exchange
VentilationPerfusionDiffusion
GENERAL PRINCIPLES IN THE PATHOGENESIS OF LUNG DAMAGE CAUSED BY CHEMICALS
Oxidative BurdenToxic Inhalants, Gases, and DosimetryParticle Deposition and Clearance
Particle SizeDeposition MechanismsParticle Clearance
ACUTE RESPONSES OF THE LUNG TO INJURY
Airway ReactivityPulmonary EdemaMechanisms of Respiratory Tract InjuryMediators of Lung ToxicityCell Proliferation
CHRONIC RESPONSES OF THE LUNG TO INJURY
Fibrosis EmphysemaAsthmaLung Cancer
AGENTS KNOWN TO PRODUCE LUNG INJURY IN HUMANS
Airborne Agents That Produce Lung Injury in HumansAsbestosSilicaLung Overload Caused by ParticlesNaphthaleneOxygen
Blood-Borne Agents That Cause Pulmonary Toxicity in HumansParaquatMonocrotalineBleomycinCyclophosphamide and 1,3-Bis-(2-Chloroethyl)-1-
Nitrosourea (BCNU)Cationic Amphophilic Drugs
METHODS FOR STUDYING LUNG INJURY
Inhalation Exposure SystemsPulmonary Function StudiesMorphologic TechniquesPulmonary LavageIn Vitro Approaches
Isolated Perfused LungLung Explants and SlicesMicrodissectionOrganotypic Cell Culture SystemsIsolated Lung Cell Populations
Initially, lung injury caused by chemicals was primarily associatedwith certain professions and occupations. In his classic treatise of1713, the Italian physician Bernardino Ramazzini provided detailedand harrowing accounts of the sufferings of miners, whose ailmentshad been known and described since antiquity. Two of Ramazz-ini’s quotations are noteworthy. With regard to miners of metals,he stated that “the lungs and brains of that class of workers arebadly affected, the lungs especially, since they take in with the airmineral spirits and are the first to be keenly aware of injury.” Ra-mazzini also was aware of the important concept of exposure:“They (workers who shovel, melt, and cast and refine mined ma-terial) are liable of the same diseases, though in less acute form,because they perform their tasks in open air.” Thus, exposure tochemicals by inhalation can have two effects: on the lung tissuesand on distant organs that are reached after chemicals enter thebody by means of inhalation. Indeed, the term inhalation toxicol-ogy refers to the route of exposure, whereas respiratory tract tox-
icology refers to target-organ toxicity, in this case abnormalchanges in the respiratory tract produced by airborne (and on oc-casion blood-borne) agents. We now know of numerous lungdiseases prompted by occupational exposures, many crippling andsome fatal. Examples include black lung in coal miners, silicosisand silicotuberculosis in sandblasters and tunnel miners, and as-bestosis in shipyard workers and asbestos miners. Occupational ex-posures to asbestos or metals such as nickel, beryllium, and cad-mium can also cause lung cancer. In the twentieth century, it hasbecome obvious that disease caused by airborne agents may not belimited to certain trades. The ubiquitous presence of airborne chem-icals is a matter of concern, since “air pollution” adversely affectshuman health and may be an important contributor to mortality(Zemp et al., 1999).
To better understand environmental lung disease, we needmore precise knowledge about the doses of toxic inhalants deliv-ered to specific sites in the respiratory tract and an understanding
515
2996R_ch15_515-524 4/12/01 1:32 PM Page 515
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

516 UNIT 4 TARGET ORGAN TOXICITY
of the extent to which repeated and often intermittent low-level ex-posures eventually may initiate and propagate chronic lung disease.Lung tissue can be injured directly or secondarily by metabolicproducts from organic compounds. However, the most importanteffect of many toxic inhalants is to place an undue oxidative bur-den on the lungs. Observations made in humans and animals pro-vide strong evidence that the sequelae of oxidative stress may beinstrumental in initiating and propagating ailments such as chronicbronchitis, emphysema, interstitial disorders (fibrosis), and cancer(Crapo et al., 1992).
Respiratory tract toxicology is a field in which collaborationinvolving epidemiologists, physiologists studying human lungfunction, toxicologists, and cell and molecular biologists has be-come close and fruitful. Epidemiologists now use a variety of pul-monary function tests to assess decrements in lung function inworkers and populations exposed to air pollutants. These tests havebeen adapted for animal studies and are used to examine the mech-anisms responsible for the pulmonary effects of air pollutants.When similar data can be obtained in both experimental animalsand human subjects (for example, studies of mucociliary clearanceof particles or responsiveness to bronchoconstrictive agents), thesedirect comparisons assist in extrapolating from animals to humans.Progress has been made in understanding some of the mechanismsthat underlie the response of the lungs to toxic agents. In responseto toxic insult, pulmonary cells are known to release a variety ofpotent chemical mediators that may critically affect lung function.Biochemical data from the study of cells taken from exposed ani-mals and in vitro exposure of cells in culture are also useful in as-sessing the toxic potential of many agents. Recently, moleculartechniques, such as in situ hybridization and immunostains, havebeen applied to analyze production of chemical mediators and otherimportant macromolecules produced by specific cell types in response to inhaled toxicants. Bronchoalveolar lavage is nowwidely exploited in experimental animals and human subjects toexamine respiratory airways’ contents (cellular and acellular) afterexposure. This chapter discusses how pulmonary toxicologistsprofit from these methods to study the biochemical, structural, andfunctional changes produced by the inhalation of pollutant gasesand particles.
LUNG STRUCTURE AND FUNCTION
Nasal Passages
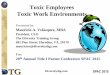
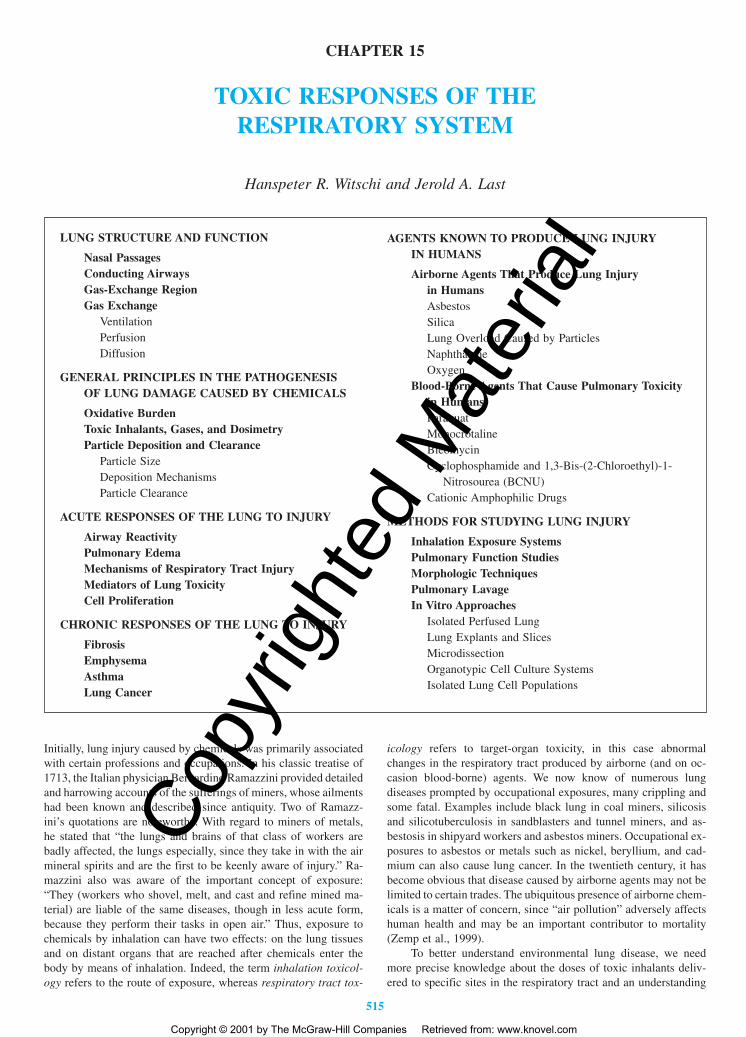
Figure 15-1 shows a schematic overview of the different regionsof the respiratory tract. Air enters the respiratory tract through thenasal and oral regions. Many species, particularly small laboratoryrodents, are obligatory nose breathers, in whom air passes almostexclusively through the nasal passages. Other species, includinghumans, monkeys, and dogs, can inhale air both through the noseand through the mouth (oronasal breathers). Air is warmed and hu-midified while passing through the nose. The nasal passages func-tion as a filter for particles, which may be collected by diffusionor impaction on the nasal mucosa. Highly water-soluble gases areabsorbed efficiently in the nasal passages, which reach from thenostril to the pharynx. The nasal turbinates thus form a first de-fensive barrier against many toxic inhalants.
The nasal passages are lined by distinctive epithelia: stratifiedsquamous epithelium in the vestibule, nonciliated cuboidal/colum-nar epithelium in the anterior chamber, ciliated pseudostratified res-
piratory epithelium, and olfactory epithelium. The greater part ofthe internal nasal passages is covered by respiratory epitheliumcontaining goblet cells, ciliated cells, nonciliated columnar cells,cuboidal cells, brush cells, and basal cells. Located in the superiorpart is the olfactory epithelium, which contains sensory cells. Nerveendings in the nasal passages are associated mostly with the fifthcranial (trigeminal) nerve.
Nasal epithelia are competent to metabolize foreign com-pounds (Fanucchi et al., 1999). Nasal tissue has been found to ac-tivate nitrosamines to mutagenic compounds. P-450 isozymes 1A1,2B1, and 4B1 have been localized in the nose of several speciesby immunohistochemical procedures. The nasal cavity is thus aready target site for metabolite-induced lesions. The olfactory ep-ithelium appears to be particularly vulnerable. Metabolism by theolfactory epithelium may play a role in providing or preventing ac-cess of inhalants directly to the brain; for example, inhaled xylenemay be converted to metabolites that move to the brain by axonaltransport.
Conducting Airways
The proximal airways—the trachea and bronchi—have a pseudo-stratified epithelium containing ciliated cells and two types of non-ciliated cells: mucous and serous cells. Mucous cells (and glandu-lar structures) produce respiratory tract mucus, a family ofhigh-molecular-weight glycoproteins with a sugar content of 80percent or more that coat the epithelium with a viscoelastic stickyprotective layer that traps pollutants and cell debris. Serous cellsproduce a fluid in which mucus may be dissolved. The action ofthe respiratory tract cilia, which beat in synchrony under the con-trol of the central nervous system (CNS), continuously drives themucous layer toward the pharynx, where it is removed from therespiratory system by swallowing or expectoration. The mucouslayer is also thought to have antioxidant, acid-neutralizing, and freeradical–scavenging functions that protect the epithelial cells (Crosset al., 1998).
Conducting airways have a characteristic branched bifurcat-ing structure, with successive airway generations containing ap-proximately twice the number of bronchi with a progressively de-creasing internal diameter. Thus, the conducting airways contain acontinuously increasing total surface area from the trachea to thedistal airways. Bifurcations have flow dividers at branch points thatserve as sites of impaction for particles, and successively narrowerdiameters also favor the collection of gases and particles on airwaywalls. Eventually a transition zone is reached where cartilaginousairways (bronchi) give way to noncartilaginous airways (bronchi-oles), which in turn give way to gas-exchange regions, respiratorybronchioles, and alveoli. Mucus-producing cells and glands giveway to Clara cells in the bronchiolar epithelium. There are impor-tant structural and cellular differences between the conductive air-ways of humans and these of many commonly studied laboratoryanimals, as discussed later in this chapter.
Gas-Exchange Region
Human lungs are divided into five lobes: the superior and inferiorleft lobes and the superior, middle, and inferior right lobes. In smalllaboratory animals such as rats, mice, and hamsters, the left lungconsists of a single lobe, whereas the right lung is divided into fourlobes: cranial, middle, caudal, and ancillary. In the guinea pig and
2996R_ch15_515-524 4/12/01 1:32 PM Page 516
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 517
rabbit, the left lung is divided into two lobes. Dogs have two leftand four right lobes. The lung can be further subdivided at the pe-riphery of the bronchial tree into distinct anatomic bronchopul-monary segments, then into lobules, and finally into acini. An ac-inus includes a terminal bronchiole and all its respiratorybronchioles, alveolar ducts, and alveolar sacs. An acinus may bemade up of two to eight ventilatory units. A ventilatory unit is de-fined as an anatomic region that includes all alveolar ducts andalveoli distal to each bronchiolar-alveolar duct junction (Mercer
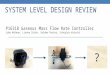
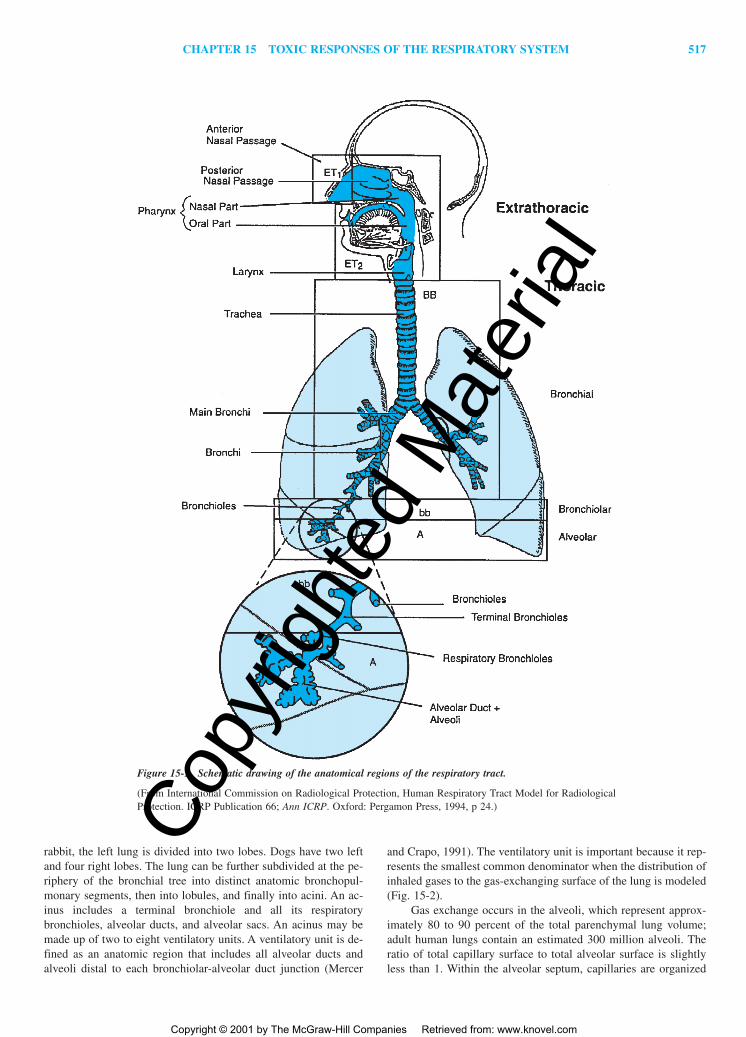
and Crapo, 1991). The ventilatory unit is important because it rep-resents the smallest common denominator when the distribution ofinhaled gases to the gas-exchanging surface of the lung is modeled(Fig. 15-2).
Gas exchange occurs in the alveoli, which represent approx-imately 80 to 90 percent of the total parenchymal lung volume;adult human lungs contain an estimated 300 million alveoli. Theratio of total capillary surface to total alveolar surface is slightlyless than 1. Within the alveolar septum, capillaries are organized
Figure 15-1. Schematic drawing of the anatomical regions of the respiratory tract.
(From International Commission on Radiological Protection, Human Respiratory Tract Model for RadiologicalProtection. ICRP Publication 66; Ann ICRP. Oxford: Pergamon Press, 1994, p 24.)
2996R_ch15_515-524 4/12/01 1:32 PM Page 517
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
518 UNIT 4 TARGET ORGAN TOXICITY
in a single sheet. Capillaries, blood plasma, and formed blood el-ements are separated from the air space by a thin layer of tissueformed by epithelial, interstitial, and endothelial components(Pinkerton et al., 1991).
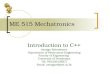
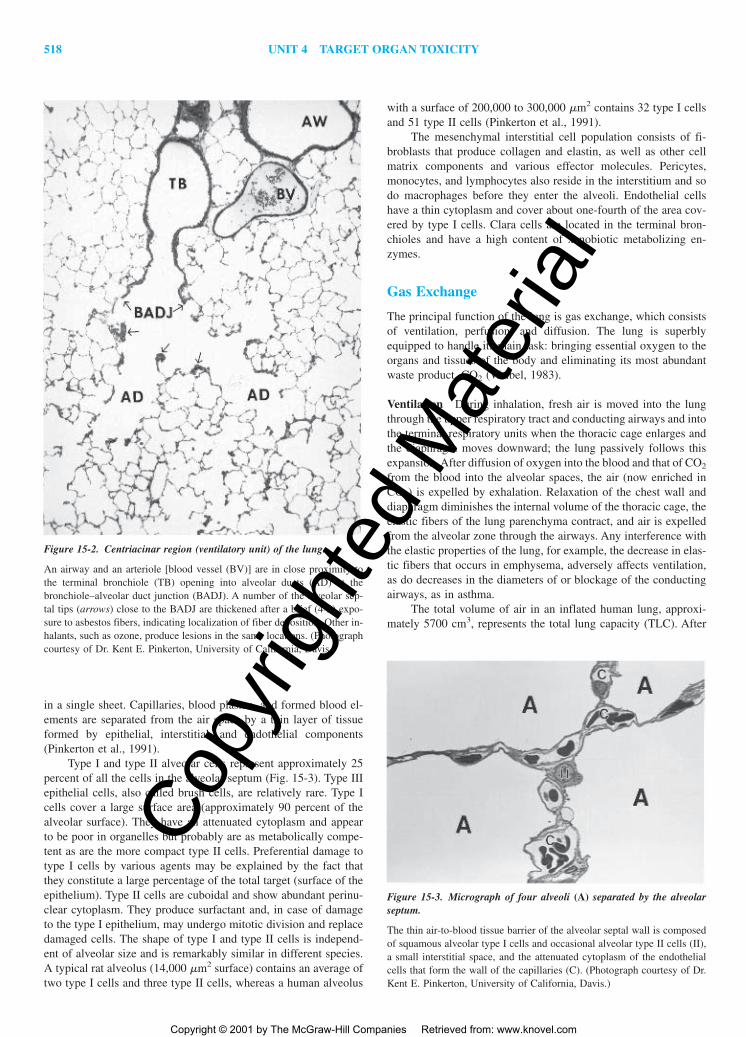
Type I and type II alveolar cells represent approximately 25percent of all the cells in the alveolar septum (Fig. 15-3). Type IIIepithelial cells, also called brush cells, are relatively rare. Type Icells cover a large surface area (approximately 90 percent of thealveolar surface). They have an attenuated cytoplasm and appearto be poor in organelles but probably are as metabolically compe-tent as are the more compact type II cells. Preferential damage totype I cells by various agents may be explained by the fact thatthey constitute a large percentage of the total target (surface of theepithelium). Type II cells are cuboidal and show abundant perinu-clear cytoplasm. They produce surfactant and, in case of damageto the type I epithelium, may undergo mitotic division and replacedamaged cells. The shape of type I and type II cells is independ-ent of alveolar size and is remarkably similar in different species.A typical rat alveolus (14,000 �m2 surface) contains an average oftwo type I cells and three type II cells, whereas a human alveolus
with a surface of 200,000 to 300,000 �m2 contains 32 type I cellsand 51 type II cells (Pinkerton et al., 1991).
The mesenchymal interstitial cell population consists of fi-broblasts that produce collagen and elastin, as well as other cellmatrix components and various effector molecules. Pericytes,monocytes, and lymphocytes also reside in the interstitium and sodo macrophages before they enter the alveoli. Endothelial cellshave a thin cytoplasm and cover about one-fourth of the area cov-ered by type I cells. Clara cells are located in the terminal bron-chioles and have a high content of xenobiotic metabolizing en-zymes.
Gas Exchange
The principal function of the lung is gas exchange, which consistsof ventilation, perfusion, and diffusion. The lung is superblyequipped to handle its main task: bringing essential oxygen to theorgans and tissues of the body and eliminating its most abundantwaste product, CO2 (Weibel, 1983).
Ventilation During inhalation, fresh air is moved into the lungthrough the upper respiratory tract and conducting airways and intothe terminal respiratory units when the thoracic cage enlarges andthe diaphragm moves downward; the lung passively follows thisexpansion. After diffusion of oxygen into the blood and that of CO2
from the blood into the alveolar spaces, the air (now enriched inCO2) is expelled by exhalation. Relaxation of the chest wall anddiaphragm diminishes the internal volume of the thoracic cage, theelastic fibers of the lung parenchyma contract, and air is expelledfrom the alveolar zone through the airways. Any interference withthe elastic properties of the lung, for example, the decrease in elas-tic fibers that occurs in emphysema, adversely affects ventilation,as do decreases in the diameters of or blockage of the conductingairways, as in asthma.
The total volume of air in an inflated human lung, approxi-mately 5700 cm3, represents the total lung capacity (TLC). After
Figure 15-2. Centriacinar region (ventilatory unit) of the lung.
An airway and an arteriole [blood vessel (BV)] are in close proximity tothe terminal bronchiole (TB) opening into alveolar ducts (AD) at thebronchiole–alveolar duct junction (BADJ). A number of the alveolar sep-tal tips (arrows) close to the BADJ are thickened after a brief (4-h) expo-sure to asbestos fibers, indicating localization of fiber deposition. Other in-halants, such as ozone, produce lesions in the same locations. (Photographcourtesy of Dr. Kent E. Pinkerton, University of California, Davis.)
Figure 15-3. Micrograph of four alveoli (A) separated by the alveolarseptum.
The thin air-to-blood tissue barrier of the alveolar septal wall is composedof squamous alveolar type I cells and occasional alveolar type II cells (II),a small interstitial space, and the attenuated cytoplasm of the endothelialcells that form the wall of the capillaries (C). (Photograph courtesy of Dr.Kent E. Pinkerton, University of California, Davis.)
2996R_ch15_515-524 4/12/01 1:32 PM Page 518
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 519
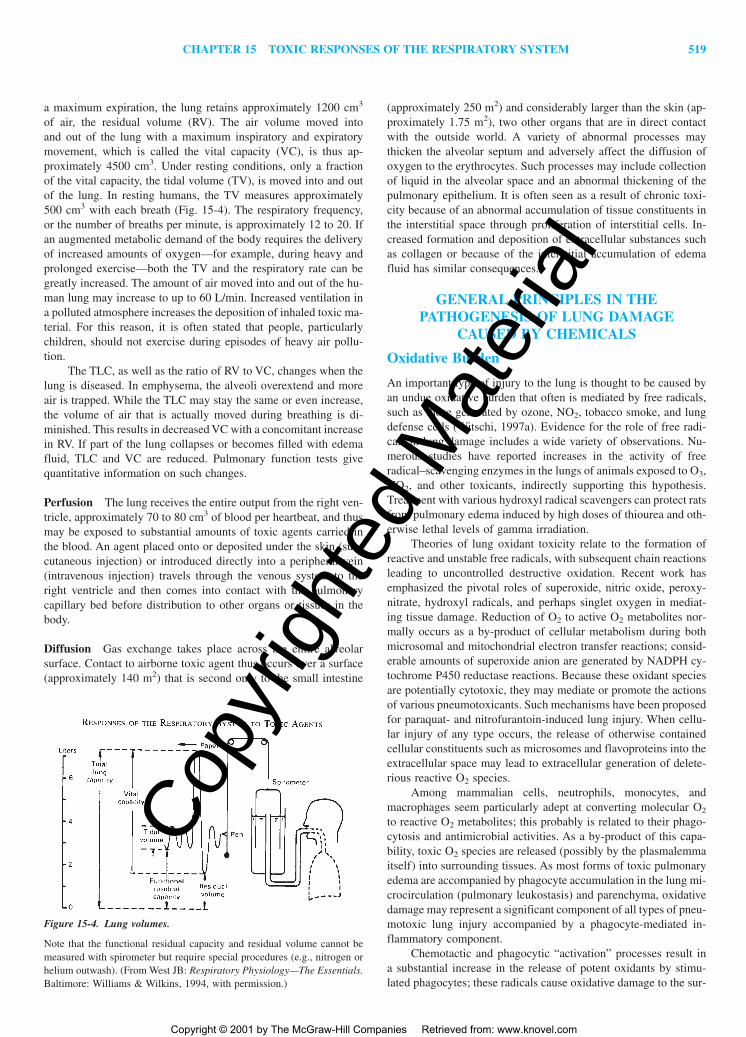
a maximum expiration, the lung retains approximately 1200 cm3
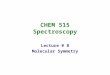
of air, the residual volume (RV). The air volume moved into and out of the lung with a maximum inspiratory and expiratorymovement, which is called the vital capacity (VC), is thus ap-proximately 4500 cm3. Under resting conditions, only a fractionof the vital capacity, the tidal volume (TV), is moved into and outof the lung. In resting humans, the TV measures approximately500 cm3 with each breath (Fig. 15-4). The respiratory frequency,or the number of breaths per minute, is approximately 12 to 20. Ifan augmented metabolic demand of the body requires the deliveryof increased amounts of oxygen—for example, during heavy andprolonged exercise—both the TV and the respiratory rate can begreatly increased. The amount of air moved into and out of the hu-man lung may increase to up to 60 L/min. Increased ventilation ina polluted atmosphere increases the deposition of inhaled toxic ma-terial. For this reason, it is often stated that people, particularlychildren, should not exercise during episodes of heavy air pollu-tion.
The TLC, as well as the ratio of RV to VC, changes when thelung is diseased. In emphysema, the alveoli overextend and moreair is trapped. While the TLC may stay the same or even increase,the volume of air that is actually moved during breathing is di-minished. This results in decreased VC with a concomitant increasein RV. If part of the lung collapses or becomes filled with edemafluid, TLC and VC are reduced. Pulmonary function tests givequantitative information on such changes.
Perfusion The lung receives the entire output from the right ven-tricle, approximately 70 to 80 cm3 of blood per heartbeat, and thusmay be exposed to substantial amounts of toxic agents carried inthe blood. An agent placed onto or deposited under the skin (sub-cutaneous injection) or introduced directly into a peripheral vein(intravenous injection) travels through the venous system to theright ventricle and then comes into contact with the pulmonary capillary bed before distribution to other organs or tissues in thebody.
Diffusion Gas exchange takes place across the entire alveolarsurface. Contact to airborne toxic agent thus occurs over a surface(approximately 140 m2) that is second only to the small intestine
(approximately 250 m2) and considerably larger than the skin (ap-proximately 1.75 m2), two other organs that are in direct contactwith the outside world. A variety of abnormal processes maythicken the alveolar septum and adversely affect the diffusion ofoxygen to the erythrocytes. Such processes may include collectionof liquid in the alveolar space and an abnormal thickening of thepulmonary epithelium. It is often seen as a result of chronic toxi-city because of an abnormal accumulation of tissue constituents inthe interstitial space through proliferation of interstitial cells. In-creased formation and deposition of extracellular substances suchas collagen or because of the interstitial accumulation of edemafluid has similar consequences.
GENERAL PRINCIPLES IN THEPATHOGENESIS OF LUNG DAMAGE
CAUSED BY CHEMICALS
Oxidative Burden
An important type of injury to the lung is thought to be caused byan undue oxidative burden that often is mediated by free radicals,such as those generated by ozone, NO2, tobacco smoke, and lungdefense cells (Witschi, 1997a). Evidence for the role of free radi-cals in lung damage includes a wide variety of observations. Nu-merous studies have reported increases in the activity of freeradical–scavenging enzymes in the lungs of animals exposed to O3,NO2, and other toxicants, indirectly supporting this hypothesis.Treatment with various hydroxyl radical scavengers can protect ratsfrom pulmonary edema induced by high doses of thiourea and oth-erwise lethal levels of gamma irradiation.
Theories of lung oxidant toxicity relate to the formation ofreactive and unstable free radicals, with subsequent chain reactionsleading to uncontrolled destructive oxidation. Recent work hasemphasized the pivotal roles of superoxide, nitric oxide, peroxy-nitrate, hydroxyl radicals, and perhaps singlet oxygen in mediat-ing tissue damage. Reduction of O2 to active O2 metabolites nor-mally occurs as a by-product of cellular metabolism during bothmicrosomal and mitochondrial electron transfer reactions; consid-erable amounts of superoxide anion are generated by NADPH cy-tochrome P450 reductase reactions. Because these oxidant speciesare potentially cytotoxic, they may mediate or promote the actionsof various pneumotoxicants. Such mechanisms have been proposedfor paraquat- and nitrofurantoin-induced lung injury. When cellu-lar injury of any type occurs, the release of otherwise containedcellular constituents such as microsomes and flavoproteins into theextracellular space may lead to extracellular generation of delete-rious reactive O2 species.
Among mammalian cells, neutrophils, monocytes, andmacrophages seem particularly adept at converting molecular O2
to reactive O2 metabolites; this probably is related to their phago-cytosis and antimicrobial activities. As a by-product of this capa-bility, toxic O2 species are released (possibly by the plasmalemmaitself) into surrounding tissues. As most forms of toxic pulmonaryedema are accompanied by phagocyte accumulation in the lung mi-crocirculation (pulmonary leukostasis) and parenchyma, oxidativedamage may represent a significant component of all types of pneu-motoxic lung injury accompanied by a phagocyte-mediated in-flammatory component.
Chemotactic and phagocytic “activation” processes result ina substantial increase in the release of potent oxidants by stimu-lated phagocytes; these radicals cause oxidative damage to the sur-
Figure 15-4. Lung volumes.
Note that the functional residual capacity and residual volume cannot bemeasured with spirometer but require special procedures (e.g., nitrogen orhelium outwash). (From West JB: Respiratory Physiology—The Essentials.Baltimore: Williams & Wilkins, 1994, with permission.)
2996R_ch15_515-524 4/12/01 1:32 PM Page 519
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
520 UNIT 4 TARGET ORGAN TOXICITY
rounding tissues. A key role of hydrogen peroxide as the mediatorof the extracellular cytotoxic mechanism of “activated” phagocyteshas been well documented. Phenomena occurring at the phagocytesurface, such as those which may occur in endogenous lung phago-cytes after exposure to dusts and toxic gases, or in circulatingphagocytes before their accumulation in the lung or after their at-tachment to normal or damaged lung endothelium seem to be im-portant in determining their degree of enhanced oxidative activity,which is otherwise at a much lower basal level in the unstimulatedcell. It also has been long appreciated that phagocytes may causelysosomal enzyme release and tissue damage.
The fact that oxidative processes are complex is suggested bythe finding that phagocytic production of active oxygen speciescauses inactivation of proteinase inhibitors and degranulation ofmast cells. The production of oxygen radicals by phagocytes is en-hanced not only by interactions of cell surface membranes withvarious appropriate stimuli but also by hyperoxia. Platelets (andplatelet microthrombi) also have the ability to generate activatedO2 species.
The lung can respond with specific defense mechanisms thatmay be acquired over time and may be stimulated by constant ex-posure to numerous species of airborne microorganisms as well asby a variety of low- and high-molecular-weight antigenic materi-als. The immune system can mount either cellular or humorallymediated responses to these inhaled antigens. Direct immunologiceffects occur when inhaled foreign material sensitizes the respira-tory system to further exposure to the same material. The mam-malian lung has a well-developed immune system. Lymphocytesreside in the hilar or mediastinal lymph nodes, lymphoid aggre-gates, and lymphoepithelial nodules as well as in aggregates or assingle cells throughout the airways. Bronchoconstriction andchronic pulmonary disease can result from the inhalation of mate-rials that appear to act wholly or partly through an allergic re-sponse. In some instances, these reactions are caused by spores ofmolds or bacterial contaminants. Frequently, chemical componentsof the sensitizing dusts or gases are responsible for the allergic re-sponse. Low-molecular-weight compounds can act as haptens thatcombine with native proteins to form a complex that is recognizedas an antigen by the immune system. Further exposure to the sen-sitizing compound can result in an allergic reaction that is charac-terized by the release of various inflammatory mediators that pro-duce an early and/or a late bronchoconstrictor response. Such aresponse is observed in sensitized workers exposed to toluene di-isocyanate (TDI), a chemical widely used in the manufacture ofpolyurethane plastics (Karol et al., 1994).
Indirect immune effects occur when exposure to air pollutantseither suppresses or enhances the immune response to other mate-rials. Both sulfur dioxide (SO2) and ozone can boost the responseof the respiratory system to inhaled foreign material, at least in ex-perimental animals (guinea pigs). It is not known whether these ef-fects occur in humans, but they form the bases for concerns aboutincreased susceptibility of asthmatic individuals to air pollutantssuch as ozone and sulfur dioxide.
Toxic Inhalants, Gases, and Dosimetry
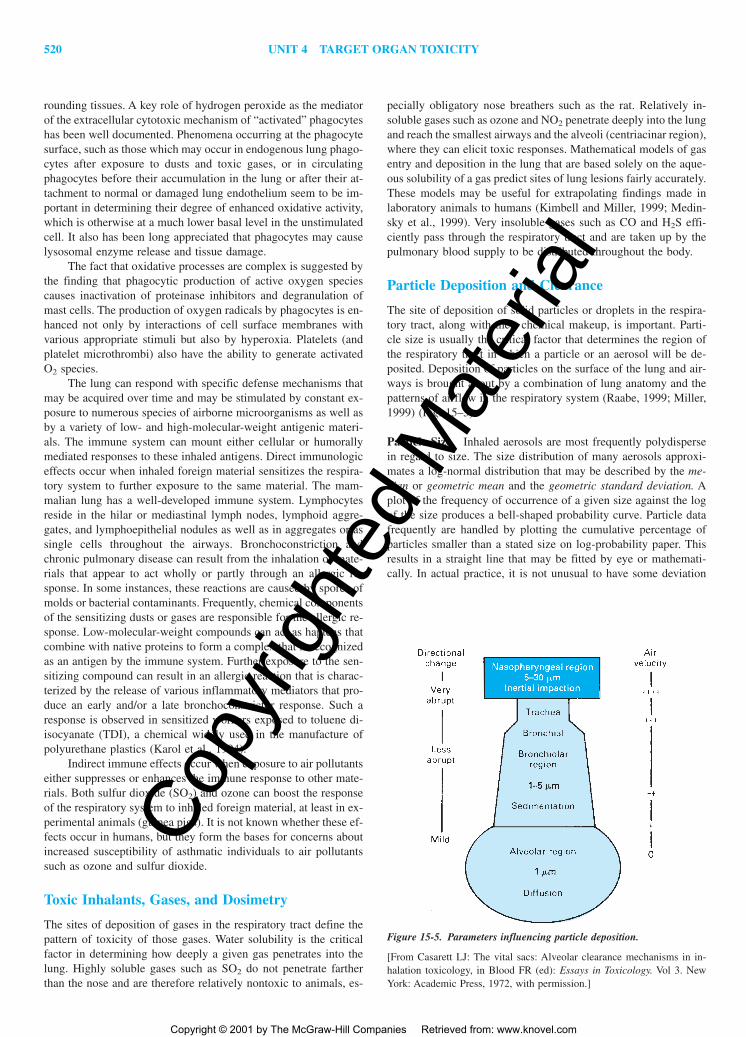
The sites of deposition of gases in the respiratory tract define thepattern of toxicity of those gases. Water solubility is the criticalfactor in determining how deeply a given gas penetrates into thelung. Highly soluble gases such as SO2 do not penetrate fartherthan the nose and are therefore relatively nontoxic to animals, es-
pecially obligatory nose breathers such as the rat. Relatively in-soluble gases such as ozone and NO2 penetrate deeply into the lungand reach the smallest airways and the alveoli (centriacinar region),where they can elicit toxic responses. Mathematical models of gasentry and deposition in the lung that are based solely on the aque-ous solubility of a gas predict sites of lung lesions fairly accurately.These models may be useful for extrapolating findings made inlaboratory animals to humans (Kimbell and Miller, 1999; Medin-sky et al., 1999). Very insoluble gases such as CO and H2S effi-ciently pass through the respiratory tract and are taken up by thepulmonary blood supply to be distributed throughout the body.
Particle Deposition and Clearance
The site of deposition of solid particles or droplets in the respira-tory tract, along with their chemical makeup, is important. Parti-cle size is usually the critical factor that determines the region ofthe respiratory tract in which a particle or an aerosol will be de-posited. Deposition of particles on the surface of the lung and air-ways is brought about by a combination of lung anatomy and thepatterns of airflow in the respiratory system (Raabe, 1999; Miller,1999) (Fig. 15–5).
Particle Size Inhaled aerosols are most frequently polydispersein regard to size. The size distribution of many aerosols approxi-mates a log-normal distribution that may be described by the me-dian or geometric mean and the geometric standard deviation. Aplot of the frequency of occurrence of a given size against the logof the size produces a bell-shaped probability curve. Particle datafrequently are handled by plotting the cumulative percentage ofparticles smaller than a stated size on log-probability paper. Thisresults in a straight line that may be fitted by eye or mathemati-cally. In actual practice, it is not unusual to have some deviation
Figure 15-5. Parameters influencing particle deposition.
[From Casarett LJ: The vital sacs: Alveolar clearance mechanisms in in-halation toxicology, in Blood FR (ed): Essays in Toxicology. Vol 3. NewYork: Academic Press, 1972, with permission.]
2996R_ch15_515-524 4/12/01 1:32 PM Page 520
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 521
from a straight line at the largest or smallest particle sizes meas-ured. The geometric mean is the 50 percent size as the mean bi-sects the curve. The geometric standard deviation (�g) is calcu-lated as
�g � 84.1% size�50% size
The �g of the particle size distribution is a measure of the poly-dispersity of the aerosol. In the laboratory, values for �g of 1.8 to3.0 are encountered frequently. In the field, values for �g may rangeup to 4.5. An aerosol with a �g below 1.2 may be consideredmonodisperse.
The median diameter that is determined may reflect the num-ber of particles, as in the count median diameter (CMD), or reflectmass, as in the mass median aerodynamic diameter (MMAD). Thelarger the number and mass of particles capable of penetrating thelung, the greater the probability of a toxic effect. The size distri-bution in relation to other factors, such as particle shape and sur-face area, also may be of interest. Surface area is of special im-portance when toxic materials are adsorbed on the surfaces ofparticles and thus are carried to the lung.
Particles that are nonspherical in shape are frequently char-acterized in terms of equivalent spheres on the basis of equal mass,volume, or aerodynamic drag. The MMAD takes into account boththe density of the particle and aerodynamic drag. It represents thediameter of a unit density sphere with the same terminal settlingvelocity as the particle, regardless of its size, shape, and density.Aerodynamic diameter is the proper measurement for particles thatare deposited by impaction and sedimentation. For very small par-ticles, which are deposited primarily by diffusion, the critical fac-tor is particle size, not density. It must be kept in mind that the sizeof a particle may change before its deposition in the respiratorytract. Materials that are hygroscopic, such as sodium chloride, sul-furic acid, and glycerol, take on water and grow in size in the warm,saturated atmosphere of the lower respiratory tract.
Deposition Mechanisms Deposition of particles occurs prima-rily by interception, impaction, sedimentation, and diffusion(Brownian movement). Interception occurs only when the trajec-tory of a particle brings it near enough to a surface so that an edgeof the particle contacts the airway surface. Interception is impor-tant for the deposition of fibers. Whereas fiber diameter determinesthe probability of deposition by impaction and sedimentation, in-terception is dependent on fiber length. Thus, a fiber with a diam-eter of 1 �m and a length of 200 �m will be deposited in thebronchial tree primarily by interception rather than impaction.
As a result of inertia, particles suspended in air tend to con-tinue to travel along their original path. In a bending airstream,such as at an airway bifurcation, a particle may be impacted on thesurface. At relatively symmetrical bifurcations, which typically oc-cur in the human lung, the deposition rate is likely to be high forparticles that move in the center of the airway. Generalizations re-garding the site of deposition of particles of a given size are prob-lematic. However, in the average adult, most particles larger than10 �m in aerodynamic diameter are deposited in the nose or oralpharynx and cannot penetrate to tissues distal to the larynx. Re-cent data have shown that very fine particles (0.01 �m and smaller)are also trapped relatively efficiently in the upper airways bydiffusion. Particles that penetrate beyond the upper airways areavailable to be deposited in the bronchial region and the deeper-lying airways. Therefore, the alveolar region has significant depo-
sition efficiencies for particles smaller than 5 �m and larger than0.003 �m.
Sedimentation brings about deposition in the smaller bronchi,the bronchioles, and the alveolar spaces, where the airways aresmall and the velocity of airflow is low. As a particle moves down-ward through air, buoyancy and the resistance of air act on the par-ticle in an upward direction while gravitational force acts on theparticle in a downward direction. Eventually, the gravitational forceequilibrates with the sum of the buoyancy and the air resistance,and the particle continues to settle with a constant velocity knownas the terminal settling velocity. Sedimentation is not a significantroute of particle deposition when the aerodynamic diameter is be-low 0.5 �m.
Diffusion is an important factor in the deposition of submi-crometer particles. A random motion is imparted to these particlesby the impact of gas molecules. This brownian motion increaseswith decreasing particle size, and so diffusion is an important de-position mechanism in the nose and in other airways and alveolifor particles smaller than about 0.5 �m.
An important factor in particle deposition is the pattern ofbreathing. During quiet breathing, in which the TV is only two tothree times the volume of the anatomic dead space (i.e, the vol-ume of the conducting airways where gas exchange does not oc-cur), a large proportion of the inhaled particles may be exhaled.During exercise, when larger volumes are inhaled at higher veloc-ities, impaction in the large airways and sedimentation and diffu-sion in the smaller airways and alveoli increase. Breath holdingalso increases deposition from sedimentation and diffusion. Fac-tors that modify the diameter of the conducting airways can alterparticle deposition. In patients with chronic bronchitis, the mucouslayer is greatly thickened and extended peripherally and may par-tially block the airways in some areas. Jets formed by air flowingthrough such partially occluded airways have the potential to in-crease the deposition of particles by impaction and diffusion in thesmall airways. Irritant materials that produce bronchoconstrictiontend to increase the tracheobronchial deposition of particles. Cig-arette smoking has been shown experimentally to produce such aneffect.
Particle Clearance The clearance of deposited particles is an im-portant aspect of lung defense. Rapid removal lessens the timeavailable to cause damage to the pulmonary tissues or permit lo-cal absorption. The specific mechanisms available for the removalof particles from the respiratory tract vary with the site of the dep-osition. It is important to emphasize that clearance of particles fromthe respiratory tract is not synonymous with clearance from thebody. Depending on the specific clearance mechanism used, par-ticles are cleared to (1) the stomach and gastrointestinal (GI) tract;(2) the lymphatics and lymph nodes, where they may be dissolvedand enter the venous circulation; or (3) the pulmonary vasculature.The only mechanisms by which the respiratory system can trulyremove deposited particles from the body are coughing and blow-ing the nose.Nasal Clearance Particles deposited in the nose are cleared byvarious mechanisms, depending on their site of deposition and sol-ubility in mucus. The anterior portion of the nose is lined with rel-atively dry squamous epithelium, and so particles deposited thereare removed by extrinsic actions such as wiping and blowing. Theother regions of the nose are largely covered by a mucociliary ep-ithelium that propels mucus toward the glottis, where it is swal-lowed. Insoluble particles generally are cleared from this region in
2996R_ch15_521 5/22/01 9:31 AM Page 521
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

522 UNIT 4 TARGET ORGAN TOXICITY
healthy adults and swallowed within an hour of deposition. Parti-cles that are soluble in mucus may dissolve and enter the epithe-lium and/or blood before they can be mechanically removed. Un-certainties still remain about the clearance of particles that aredeposited on olfactory regions or areas that are damaged by acuteinfection, chronic illnesses, or toxic injury.Tracheobronchial Clearance The mucous layer covering the tra-cheobronchial tree is moved upward by the beating of the under-lying cilia. This mucociliary escalator transports deposited parti-cles and particle-laden macrophages upward to the oropharynx,where they are swallowed and pass through the GI tract. Mucocil-iary clearance is relatively rapid in healthy individuals and is com-pleted within 24 to 48 h for particles deposited in the lower air-ways. Infection and other injuries can greatly impair clearance.Pulmonary Clearance There are several primary ways by whichparticulate material is removed from the lower respiratory tractonce it has been deposited:
1. Particles may be directly trapped on the fluid layer of the con-ducting airways by impaction and cleared upward, in the tra-cheobronchial tree via the mucociliary escalator.
2. Particles may be phagocytized by macrophages and clearedvia the mucociliary escalator.
3. Particles may be phagocytized by alveolar macrophages andremoved via the lymphatic drainage.
4. Material may dissolve from the surfaces of particles and be re-moved via the bloodstream or lymphatics.
5. Small particles may directly penetrate epithelial membranes.
Minutes after particles are inhaled, they may be found in alve-olar macrophages. Many alveolar macrophages are ultimatelytransported to the mucociliary escalator. It is possible thatmacrophages are carried to the bronchioles with the alveolar fluidthat contributes to the fluid layer in the airways. Other particlesmay be sequestered in the lung for very long periods, often inmacrophages located in the interstitium.
ACUTE RESPONSES OF THE LUNGTO INJURY
Airway Reactivity
Large airways are surrounded by bronchial smooth muscles, whichhelp maintain airway tone and diameter during expansion and con-traction of the lung. Bronchial smooth muscle tone is normally reg-ulated by the autonomic nervous system. Reflex contraction occurswhen receptors in the trachea and large bronchi are stimulated byirritants such as cigarette smoke and air pollutants. Bronchocon-striction can be provoked by cholinergic drugs such as acetyl-choline, a phenomenon that serves as the basis for a sensitive meas-ure of whether a toxicant can cause bronchoconstriction in animalsor humans primed by a prior dose of an acetylcholinelike agent(bronchoprovocation testing) . These agents bind to cell surface re-ceptors (cholinergic receptors) and trigger an increase in the in-tracellular concentration of cyclic guanosine monophosphate(cGMP), which in turn facilitates smooth muscle contraction. Theactions of cGMP can be antagonized by cyclic adenosinemonophospate (cAMP), which has bronchodilatory activity, andcan be increased by agents that bind to beta-adrenergic receptorson the cell surface. Other important mediators of airway smoothmuscle tone include histamine, various prostaglandins and
leukotrienes, substance P, and nitric oxide. The bronchial smoothmuscles of individuals with asthma contract with much less provo-cation than do those of normal subjects. Bronchoconstrictioncauses a decrease in airway diameter and a corresponding increasein resistance to airflow. Characteristic associated symptoms includewheezing, coughing, a sensation of chest tightness, and dyspnea.Exercise potentiates these problems. A major cause of concernabout ambient air pollution is whether asthmatic individuals rep-resent a population that is particularly susceptible to the adversehealth effects of sulfur dioxide, ozone, nitrogen dioxide, other res-piratory irritant gases, and respirable particles. Since the majorcomponent of airway resistance usually is contributed by largebronchi, inhaled agents that cause reflex bronchoconstriction aregenerally irritant gases with moderate solubility. Demonstrationsof the bronchoconstrictive effects of gases in laboratory animalsoften are performed in guinea pigs, which seem to represent a nat-ural animal model of asthmatic humans with respect to innate air-way reactivity.
Pulmonary Edema
Toxic pulmonary edema represents an acute, exudative phase oflung injury that generally produces a thickening of the alveolar-capillary barrier. Edema fluid, when present, alters ventilation-perfusion relationships and limits diffusive transfer of O2 and CO2
even in otherwise structurally normal alveoli. Edema is often a signof acute lung injury.
The biological consequences of toxic pulmonary edema notonly induce acute compromise of lung structure and function butalso may include abnormalities that remain after resolution of theedematous process. After exposure to some toxic agents in whichthe alveolar-capillary surface is denuded (such as alloxan), recov-ery is unlikely, whereas in situations of more modest injury (suchas histamine administration), full recovery is readily achievable.Between these two extremes there are forms of severe lung injuryaccompanied by amplified inflammatory damage and/or exagger-ated restorative-reparative processes (e.g., after paraquat ingestion).In these severe forms, the extensive interstitial and intraalveolar in-flammatory exudate resolves via fibrogenesis, an outcome that maybe beneficial or damaging to the lung. Accumulation and turnoverof inflammatory cells and related immune responses in an edema-tous lung probably play a role in eliciting both mitogenic activityand fibrogenic responses.
Pulmonary edema is customarily quantified in experimentalanimals by some form of gravimetric measurement of lung watercontent. Very commonly, the wet (undesiccated) weight of thewhole lung or that of a single lung lobe is determined. This valueis often normalized to the weight of the animal from which thelung was taken. Alternatively, some investigators determine lungwater content by weighing whole lungs or lung slices before andafter complete drying in an oven or desiccator. Commonly usedmethods for expressing such data include (1) percentage water con-tent [100 � (wet weight � dry weight)�(wet weight)], (2) percent-age dry weight [100 � (dry weight)�(wet weight)], and (3) watercontent [(milliliters of water)�(dry weight)].
Mechanisms of Respiratory Tract Injury
Airborne agents can contact cells lining the respiratory tract fromthe nostrils to the gas-exchanging region. The sites of interaction
2996R_ch15_515-524 4/12/01 1:32 PM Page 522
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 523
of toxicants in the respiratory tract have important implications forevaluation of the risk to humans posed by inhalants. For example,rats have much more nasal surface on a per body weight basis thando humans. Measurement of DNA-protein cross-links formed innasal tissue by the highly reactive gas formaldehyde has demon-strated that rats, which readily develop nasal tumors, have manymore DNA cross-links per unit of exposure (concentration offormaldehyde � duration of exposure) than do monkeys. Becausethe breathing pattern of humans resembles that of monkeys morethan that of rats, it was concluded that extrapolation of tumor datafrom rats to humans on the basis of formaldehyde concentrationmay overestimate doses of formaldehyde to humans. Patterns ofanimal activity can affect dose to the lung; nocturnally active ani-mals such as rats receive a greater dose per unit of exposure atnight than during the day, whereas humans show the opposite di-urnal relationships of exposure concentration to dose.
Certain gases and vapors stimulate nerve endings in the nose,particularly those of the trigeminal nerve (Alarie et al., 1998). Theresult is holding of the breath or changes in breathing patterns, toavoid or reduce further exposure. If continued exposure cannot beavoided, many acidic or alkaline irritants produce cell necrosis andincreased permeability of the alveolar walls. Other inhaled agentscan be more insidious; inhalation of HCl, NO2, NH3, or phosgenemay at first produce very little apparent damage in the respiratorytract. The epithelial barrier in the alveolar zone, after a latency pe-riod of several hours, begins to leak, flooding the alveoli and pro-ducing a delayed pulmonary edema that is often fatal.
A different pathogenetic mechanism is typical of highly re-active molecules such as ozone. It is unlikely that ozone as suchcan penetrate beyond the layer of fluid covering the cells of thelung. Instead, ozone lesions are propagated by a cascade of sec-ondary reaction products, such as aldehydes and hydroxyperoxidesproduced by ozonolysis of fatty acids and other substrates in thelung’s lining fluid, and by reactive oxygen species arising fromfree radical reactions. Reactive oxygen species also have been im-plicated in pulmonary bleomycin toxicity, pulmonary oxygen tox-icity, paraquat toxicity, and the development of chronic lesions suchas the fibrogenic and carcinogenic effects of asbestos fibers.
Metabolism of foreign compounds can be involved in thepathogenesis of lung injury. The balance of activation and detoxi-fication plays a key role in determining whether a given chemicalultimately will cause damage. The lung contains most of the en-zymes involved in xenobiotic metabolism that have been identifiedin other tissues, such as the liver (Buckpitt et al., 1997). While theoverall levels of these enzymes tend to be lower in lung than inliver, they often are highly concentrated in specific cell populationsof the respiratory tract. Moreover, their specific content of partic-ular cytochrome P450 isozymes may be much higher in lung. Thus,the turnover of a substrate for a lung P450 may be far more rapidthan occurs in liver. Many isozymes of the cytochrome P450 com-plex have been identified in and isolated from the lungs of rabbits,rats, hamsters and humans. Cytochrome P450 1A1 is present inlow amounts in normal rat and rabbit lungs but is highly inducibleby polycyclic aromatic hydrocarbons, flavones, and mixtures ofpolyhalogenated biphenyls. This isozyme also is present in humanlungs and is thought to be involved in the metabolic activation ofthe polycyclic aromatic hydrocarbons that are present in cigarettesmoke. By inference, this P450 isozyme may play a role in thepathogenesis of lung cancer. Attempts have been made to use theexpression of cytochrome P450 1A1 as a biomarker of exposureand sensitivity to cigarette smoke in humans, although the precise
relationships remain unclear. Cytochrome P450 2B1, which is read-ily inducible in rat liver by phenobarbital, is not inducible in lungtissue. Other isozymes identified in human lung are cytochromeP450 2F1, 4B1, and 3A4. Further microsomal enzymes found inthe lung include NADPH cytochrome P450 reductase, epoxide hy-drolase, and flavin-containing monoxygenases. Finally, two im-portant cytosolic enzymes involved in lung xenobiotic metabolismare glutathione-S-transferase and glutathione peroxidase. Adulthuman lungs appear to contain several forms of glutathione-S-transferase.
Mediators of Lung Toxicity
Advances in cell culture techniques (Leikauf and Driscoll, 1993)have allowed investigators to examine the role of specific signalmolecules in toxicant-induced lung damage; this is a very activearea of research. Such studies are often guided by results obtainedby analysis of cytokines and other mediators in lung lavage fluidfrom animals or human volunteers exposed to inhaled toxic agents.
For example, interleukin 1 beta (IL-1�), transforming growthfactor beta (TGF-�), and tumor necrosis factor alpha (TNF-�) haveall been implicated in the cascade of reactions that is thought tobe responsible for the pathogenesis of pulmonary fibrosis (Zhangand Phan, 1999). Similarly, several of the nine described membersof the interleukin family, especially IL-1, IL-2, IL-5 and IL-8, arethought to be essential components of the lung’s response to ep-ithelial cell injury. Various specific prostaglandins, especiallyPGE2, and leukotrienes have been implicated in intracellular sig-naling pathways in the lung. The roles of cell surface adhesion mol-ecules and their interaction with cell matrix components and withcontrol of inflammatory cell migration (particularly neutrophil in-flux to the lung) have been studied intensively.
Analysis of normal lung homogenates suggests that the lungcontains large amounts of endogenous cytokines and inflammatorymediators, far more than enough for these potent compounds toelicit effects. Thus, these agents must be compartmentalized in ahealthy lung to control their potent bioactivity. How these processesare regulated normally, what exactly goes wrong with homeosta-sis in a damaged lung, the temporal and geographic relationship ofdifferent cytokines in the amplification of an initial injurious event,and detailed mechanisms of resolution of lung injury are not wellunderstood and represent the current focus of much research onmechanisms of lung injury by toxic agents. The reader is referredto reviews of these topics (Massague, 1998; Barnes et al., 1998)for more details on specific mediators and toxic agents in this rap-idly changing research area.
Cell Proliferation
The effects of toxicants on the lung may be reversible or irre-versible. Postexposure progression of lung fibrosis has beendemonstrated in rats exposed to ozone, mice exposed to cy-clophosphamide, and hamsters exposed to bleomycin or bleomycinplus oxygen. The mechanisms for exacerbating lung damage or re-pairing such damage during a postexposure period in which fil-tered air alone is inhaled are not obvious. Examination of the timecourse and cellular components of reepithelialization of the alve-olar ducts and walls during the postexposure period would be especially important in this regard. Research on the postexpo-sure effects of inhaled toxicants is an important area for furtherstudy.
2996R_ch15_515-524 4/12/01 1:32 PM Page 523
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

524 UNIT 4 TARGET ORGAN TOXICITY
The normal adult lung is an organ for which under normalcircumstances very few cells appear to die and to be replaced. Whendamaged by a toxic insult, the lung parenchyma is capable to re-pair itself in an efficient manner. Type I cell damage is followedby proliferation of type II epithelial cells which eventually trans-form into new type I cells; in the airways, the Clara cells prolifer-ate and divide following injury. The migration of mobile blood cellssuch as leukocytes across the pulmonary capillaries into the alve-olar lumen may also trigger a mitotic response. Other cells in thealveolar zone, such as capillary endothelial cells, interstitial cells,and alveolar macrophages, also proliferate. The result is a normallooking organ again although on occasion excessive proliferationof fibroblasts may result in lung disease. In general, however, thelung appears to have a high capacity to repair itself and thus todeal with the many toxic insults presented by the environment(Witschi, 1997b).
CHRONIC RESPONSES OF THELUNG TO INJURY
Fibrosis
Defined clinically, lung fibrosis refers to the type of interstitialfibrosis that is seen in the later stages of idiopathic pulmonary fi-brosis (also called cryptogenic fibrosing alveolitis in the UnitedKingdom). In this disease, the hallmark of pulmonary fibrosis seenby the pathologist is increased focal staining of collagen fibers inthe alveolar interstitium. Fibrotic lungs from humans with acute orchronic pulmonary fibrosis contain increased amounts of collagenas evaluated biochemically, in agreement with the histological find-ings.
In lungs damaged by toxicants, the response resembles adultor infant respiratory distress syndrome more closely than it re-sembles chronic interstitial fibrosis. Excess lung collagen is usu-ally observed not only in the alveolar interstitium but also through-out the centriacinar region, including the alveolar ducts andrespiratory bronchioles. The relationship between increased colla-gen deposition around small airways and lung mechanics is not un-derstood either theoretically or empirically.
At least 19 genetically distinct collagen types are known tooccur in all mammals, most of which have been found in normallungs or to be synthesized by isolated lung cells. Two types pre-dominate in the lung, representing about 90 percent or more of thetotal lung collagen. Type I and type III collagen are major inter-stitial components and are found in the normal lungs of all mam-mals in an approximate ratio of 2:1. Type I collagen is the mate-rial that stains histologically as “collagen,” whereas type IIIcollagen is appreciated histologically as reticulin. Some types oftoxicant-induced pulmonary fibrosis, including that induced by O3,involve abnormalities in the type of collagen made. For example,there is an increase in type I collagen relative to type III collagenin patients with idiopathic pulmonary fibrosis. Similar shifts havebeen demonstrated in the lungs of adults and infants dying of acuterespiratory distress syndrome. It is not known whether shifts in col-lagen types, compared with absolute increases in collagen content,account for the increased stiffness of fibrotic lungs. Type III col-lagen is much more compliant than is type I; thus, an increasingproportion of type I relative to type III collagen may result in astiffer lung, as is observed in pulmonary fibrosis. Changes in col-lagen cross-linking in fibrotic lungs also may contribute to the in-creased stiffness. It is unclear whether the observed increase in
stainable collagen is due solely to the increase in the collagen con-tent of the lungs observed biochemically or whether altered colla-gen types or cross-linking might also contribute to the histologicalchanges.
Increased collagen type I:type III ratios also have been ob-served in newly synthesized collagen in several animal models ofacute pulmonary fibrosis. Although the mechanism for this shift incollagen types is unknown, there are many possible explanations.Clones of fibroblasts responsive to recruitment and/or proliferationfactors may preferentially synthesize type I collagen compared withthe action of the fibroblasts normally present. Alterations in the ex-tracellular matrix resulting from inflammatory mediators secretedby various effector cells also may cause the fibroblasts to switchthe collagen phenotype that is synthesized.
Collagen associated with fibrosis also may be abnormal withrespect to cross-linking. Alterations in cross-links in experimentalsilicosis and bleomycin-induced fibrosis have been described. Asin the case of alterations in collagen type ratios, it is unclearwhether the mechanisms can be ascribed to changes in the clonesof fibroblasts that actively synthesize collagen or to changes in themilieu that secondarily affect the nature of the collagen made bya given population of lung fibroblasts.
Emphysema
In many ways emphysema can be viewed as the opposite of fi-brosis in terms of the response of the lungs to an insult: the lungsbecome larger and too compliant rather than becoming smaller andstiffer. Destruction of the gas-exchanging surface area results in adistended, hyperinflated lung that no longer effectively exchangesoxygen and carbon dioxide as a result of both loss of tissue andair trapping. The currently accepted pathological definition of em-physema is “a condition of the lung characterized by abnormal en-largement of the airspaces distal to the terminal bronchiole, ac-companied by destruction of the walls, without obvious fibrosis”(Snider et al., 1985). The major cause of human emphysema is, byfar, cigarette smoke inhalation, although other toxicants also canelicit this response. A feature of toxicant-induced emphysema issevere or recurrent inflammation, especially alveolitis with releaseof proteolytic enzymes by participating leukocytes.
A unifying hypothesis that explains the pathogenesis of em-physema has emerged from studies by several investigators. Earlyclinical research on screening blood protein phenotypes identifieda rare mutation giving rise to a hereditary deficiency of the serumglobulin alpha1-antitrypsin. Homozygotes for this mutation had nocirculating levels of this protein, which can prevent the proteolyticactivity of serine proteases such as trypsin. Thus, alpha1-antitrypsin(now called alpha1-antiprotease) is one of the body’s main defensesagainst uncontrolled proteolytic digestion by this class of enzymes,which includes elastase. There is a clinical association between thegenetic lack of this important inhibitor of elastase and the devel-opment of emphysema at an extraordinarily young age. Furtherstudies in smokers led to the hypothesis that neutrophil (and per-haps alveolar macrophage) elastases can break down lung elastinand thus cause emphysema; these elastases usually are kept incheck by alpha1-antiprotease that diffuses into the lung from theblood. As the individual ages, an accumulation of random elas-tolytic events can cause the emphysematous changes in the lungsthat are normally associated with aging. Toxicants that cause in-flammatory cell influx and thus increase the burden of neutrophilelastase can accelerate this process. In accordance with this hy-
2996R_ch15_515-524 4/12/01 1:32 PM Page 524
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 525
pothesis are a large number of experimental studies in animals in-stilled intratracheally with pancreatic or neutrophil elastase or withother proteolytic enzymes that can digest elastin in which a patho-logical condition develops that has some of the characteristics ofemphysema, including destruction of alveolar walls and airspaceenlargement in the lung parenchyma.
An additional clue to the pathogenesis of emphysema is pro-vided by the observation that mice with defects in genes that codefor elastin and collagen modifying enzymes develop emphysema(O’Byrne and Postma, 1999). These observations suggest that prob-lems with elastin synthesis may play an important role in the patho-genesis of emphysema, and that in its simplest form the elastase-antiprotease model alone cannot fully explain the detailedbiochemical mechanisms that underlie the etiology of emphysema.
Asthma
Asthma is becoming increasingly prevalent in the United Statesand Europe, especially in crowded urban areas. This disease is char-acterized clinically by attacks of shortness of breath, which maybe mild or severe. It is caused by narrowing of the large conduct-ing airways (bronchi) either upon inhalation of provoking agentsor for unknown causes. There are well-established links betweenoccupational and environmental exposure to antigens or to chem-icals that can act as haptens and in the pathogenesis of asthma.There are histopathologic components that are common betweenasthma and pulmonary fibrosis, but in this case the disease is cen-tered in and around the large conducting airways rather than thecentriacinar region of the lung parenchyma. There may be com-mon mechanisms, especially with regard to the role of inflamma-tory cells and the cytokines and growth factors they secrete (Barneset al., 1998). The clinical hallmark of asthma is increased airwayreactivity: the smooth muscle around the large airways contract inresponse to exposure to irritants. The extreme sensitivity of guineapigs (as opposed to rats or mice) to inhaled irritants such as ozoneor SO2 may be an example of an animal model of the human asth-matic subject (Barnes et al., 1998).
Lung Cancer
Lung cancer, an extremely rare disease around the turn of the cen-tury, is now the leading cause of death from cancer among menand women. Retrospective and, more conclusively, prospective epi-demiologic studies unequivocally show an association between to-bacco smoking and lung cancer. It has been estimated that ap-proximately 80 to 90 percent of lung cancers (and several othercancers, such as cancer of the bladder, esophagus, oral cavity, andpancreas) are caused by cigarette smoking. Average smokers havea 10-fold and heavy smokers a 20-fold increased risk of develop-ing lung cancer compared with nonsmokers. Quitting the habit willreduce the risk (Wingo et al., 1999).
Inhalation of asbestos fibers and metallic dusts or fumes—such as arsenic, beryllium, cadmium, chromium, and nickel, en-countered in smelting and manufacturing operations— has beenassociated with cancer of the respiratory tract. Workers who man-ufacture chloromethyl ether or mustard gas also have an increasedrisk of developing lung cancers, as do workers exposed to effluentgases from coke ovens. Radon gas is a known human lung car-cinogen. Formaldehyde is a probable human respiratory carcino-gen. Silica, human-made fibers, and welding fumes are suspectedcarcinogens (International Agency for Research on Cancer, 1987,
1993). Smokers who inhale radon or asbestos fibers increase theirrisk of developing lung cancer severalfold, suggesting a synergis-tic interaction between the carcinogens. To what extent commonair pollutants such as ozone, nitrogen dioxide, sulfur dioxide, andfumes emanating from power plants, oil refineries, and Dieselfuel–powered trucks and cars contribute to the development of lungcancer in the general population remains an open question. Someevidence suggests that respirable particulates suspended in pollutedair are a risk factor (Beeson et al., 1998). Indoor air pollution, in-cluding environmental tobacco smoke, increases the risk of devel-oping lung cancer in nonsmokers (National Cancer Institute, 1999).
Human lung cancers may have a latency period of 20 to 40years, making the relationship to specific exposures difficult to es-tablish. Many lung cancers in humans originate from the cells lin-ing the airways (lung cancer originating from such sites is oftenreferred to as bronchogenic carcinoma), but during the last twodecades a significant increase in peripheral adenocarcinomas hasoccurred. Compared with cancer in the lung, cancer in the upperrespiratory tract is less common. Malignant lesions of the nasalpassages, which are seen frequently in experimental animals, arecomparatively rare in humans. They are associated with certainoccupations, including work with chromate, nickel, mustard gas,isopropyl alcohol, the manufacture of wooden furniture, and bootand shoe manufacture. Possible carcinogens include hexavalentchromium compounds, metallic nickel and nickel subsulfide, nickeloxide, formaldehyde, and certain wood and leather dusts.
The potential mechanisms of lung carcinogenesis have beenstudied extensively by means of analysis of tumor material and instudies of human bronchial cells maintained in culture. Damage toDNA is thought to be a key mechanism. An activated carcinogenor its metabolic product, such as alkyldiazonium ions derived fromN-nitrosamines, may interact with DNA. Persistence of O6-alkyldeoxyguanosine in DNA appears to correlate with carcino-genicity (Hecht, 1999). However, tumors do not always developwhen adducts are present, and adduct formation may be a neces-sary but not sufficient condition for carcinogenesis. DNA damagecaused by active oxygen species is another potentially importantmechanism. Ionizing radiation leads to the formation of superox-ide, which is converted through the action of superoxide dismutaseto hydrogen peroxide. In the presence of Fe and other transitionmetals, hydroxyl radicals may be formed which then cause DNAstrand breaks. Cigarette smoke contains high quantities of activeoxygen species and other free radicals. Additional oxidative stressmay be placed on the lung tissue of smokers by the release of su-peroxide anions and hydrogen peroxide by activated macrophages,metabolism of carcinogens, and lipid peroxidation caused by re-active aldehydes.
In laboratory animals, spontaneously occurring malignantlung tumors are uncommon unless the animals reach a very ad-vanced age. Exposure to carcinogens by the inhalation route or byintratracheal instillation or systemic administration readily pro-duces lung tumors in many laboratory species, such as mice, rats,hamsters, and dogs. There are several differences between lung tu-mors in animals and bronchogenic cancer in humans. In animals,particularly rodents, most tumors are in the periphery rather thanarising from the bronchi. The incidence of benign lung tumors suchas adenomas is often very high, and carcinomas seem to requiremore time to develop. Lung tumors in animals do not metastasizeas aggressively, if they do so at all, as do human lung cancers(Hahn, 1997). Cancer of the nasal passages is readily induced inexperimental animals in inhalation studies.
2996R_ch15_525-534 4/12/01 1:32 PM Page 525
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

526 UNIT 4 TARGET ORGAN TOXICITY
Because lung tumors in mice and rats are often seen in car-cinogenesis bioassays, they deserve special mention. Murine lungtumors are mostly benign-appearing adenomas originating fromalveolar type II cells or bronchiolar Clara cells. They can progressto adenocarcinomas and invade lymphatics and blood vessels. Cer-tain mouse strains, such as strain A and the Swiss-Webster mouse,have a high incidence of spontaneously occurring lung tumors.These animals respond with increased numbers of tumors to theinhalation or injection of many carcinogens. Other strains are muchmore resistant. Lung tumors in strain A mice have become valu-able tools for studing the genetic factors that determine suscepti-bility (Malkinson, 1998). They contain frequent mutations in theK-ras gene, a mutation also found frequently in human lung can-cers (Graziano et al., 1999). Methylating nitrosamines (NNK andDMN) produce mutations consistent with the formation of O6-methylguanine and ethylating nitrosamines (ENU and DEN) andmutations consistent with the formation of O4-ethylthymidine. Instrains less susceptible than the A/J mouse, chemicals such astetranitromethane, 1,3-butadiene, DMN, and NNK generate tumorswith mutations consistent with the result of DNA adduct forma-tion, whereas other chemicals (acetylaminofluorene, methylenechloride) do not produce tumors with carcinogen-specific muta-tions.
Lung tumors in rats exposed to airborne carcinogens consistmostly of peripheral adenocarcinomas and squamous cell carcino-mas. In addition, rat lungs on occasion contain lesions that are char-acterized by an epithelium surrounding a space filled with keratin.The mass may compress the adjacent lung parenchyma and occa-sionally invades it. These lesions are classified by some patholo-gists as bona fide tumors, whereas other pathologists characterizethis type of lesion as a cyst filled with keratin. Classification ofsuch a lesion as a tumor is important because these lesions oftenare found in long-term tests in animals that have been exposed toagents that are not considered carcinogens, such as carbon black,titanium dioxide, and certain human-made fibers (ILSI, 2000).
AGENTS KNOWN TO PRODUCELUNG INJURY IN HUMANS
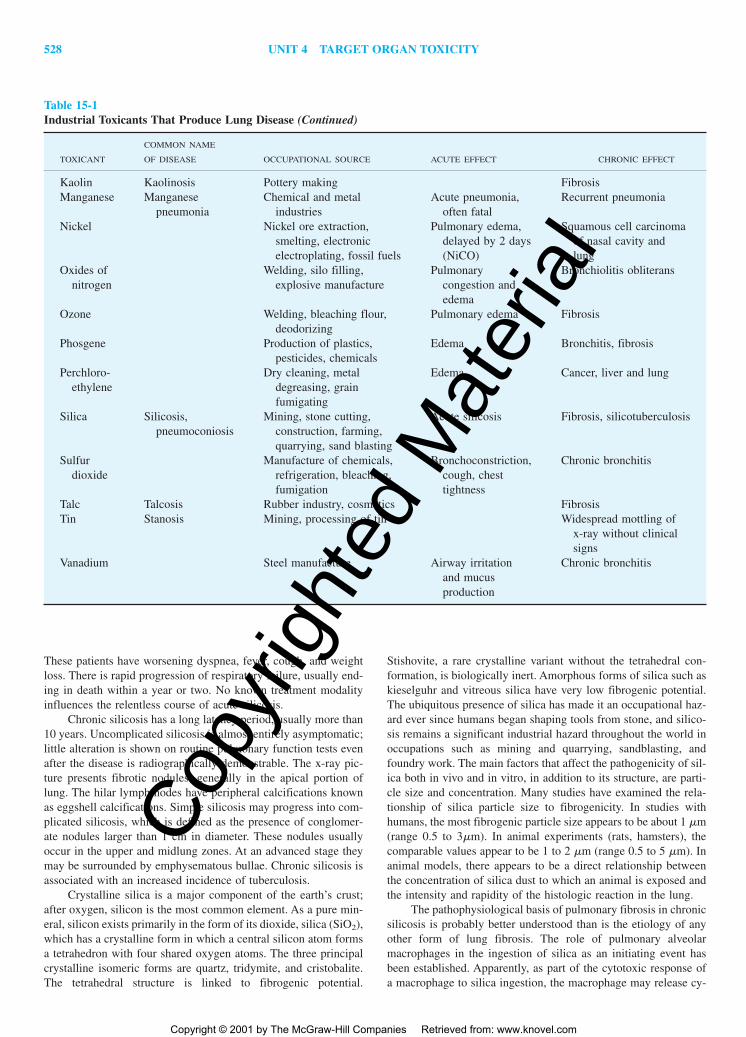
The prevention and treatment of acute and chronic lung diseasewill eventually be based on a knowledge of the cellular and mo-lecular events that determine lung injury and repair. During the past20 years, a large body of evidence has accumulated. Table 15-1lists common toxicants that are known to produce acute and chroniclung injury in humans. In the following sections, a few examplesof our current understanding of lung injury at the mechanistic levelare discussed, with emphasis on agents directly responsible for hu-man lung disease.
Airborne Agents That Produce LungInjury in Humans
Asbestos The term “asbestos” describes silicate minerals in fiberform. The most commonly mined and commercially used asbestosfibers include the serpentine chrysotile asbestos and the amphi-boles crocidolite, anthophyllite, amosite, actinolite, and tremolite.Exposure to asbestos fibers occurs in mining operations and in theconstruction and shipbuilding industries, where asbestos was at onetime widely used for its highly desirable insulating and fireproof-ing properties. During the last few years, concern about asbestos
in older buildings has led to the removal of asbestos-based insu-lating material; abatement workers may now represent an addi-tional population at risk.
Asbestos causes three forms of lung disease in humans: as-bestosis, lung cancer, and malignant mesothelioma. Asbestosis ischaracterized by a diffuse increase of collagen in the alveolar walls(fibrosis) and the presence of asbestos fibers, either free or coatedwith a proteinaceous material (asbestos bodies). Malignantmesothelioma (a tumor of the cells covering the surface of the vis-ceral and parietal pleura), a tumor that otherwise occurs only ex-tremely rarely in the general population, is unequivocally associ-ated with asbestos exposure. There is some discrepancy betweenhuman observations and animal data. In animal experiments,chrysotile produces mesothelioma much more readily than do theamphibole fibers. In humans, amphibole fibers are implicated moreoften even when the predominant exposure is to chrysotile asbestos.Chrysotile breaks down much more readily than do the amphiboles.It is possible that in small laboratory animals chrysotile fibers, evenif broken down, are retained longer relative to the life span of theanimal than they are in humans, thus explaining the higher rate ofmesothelioma development.
The hazards associated with asbestos exposure depend onfiber length. Fibers 2 �m in length may produce asbestosis;mesothelioma is associated with fibers 5 �m long, and lung can-cer with fibers larger than 10 �m. Fiber diameter is another criti-cal feature. Fibers with diameters larger than approximately 3 �mdo not readily penetrate into the peripheral lung. For the develop-ment of mesothelioma, fiber diameter must be less than 0.5 �m,since thinner fibers may be translocated from their site of deposi-tion via the lymphatics to other organs, including the pleural surface.
Once asbestos fibers have been deposited in the lung, theymay become phagocytized by alveolar macrophages. Short fibersare completely ingested and subsequently removed via the mu-cociliary escalator. Longer fibers are incompletely ingested, andthe macrophages become unable to leave the alveoli. Activated bythe fibers, macrophages release mediators such as lymphokines andgrowth factors, which in turn attract immunocompetent cells orstimulate collagen production. Asbestos-related lung disease thusmay be mediated through the triggering of an inflammatory se-quence of events or the production of changes that eventually leadto the initiation (DNA damage caused by reactive molecularspecies) or promotion (increased rate of cell turnover in the lung)of the carcinogenic process.
The surface properties of asbestos fibers appear to be an im-portant mechanistic element in toxicity. The protection afforded bysuperoxide dismutase or free radical scavengers in asbestos-relatedcell injury in vitro suggests that the generation of active oxygenspecies and concomitant lipid peroxidation are important mecha-nisms in asbestos toxicity. The interaction of iron on the surfaceof asbestos fibers with oxygen may lead to the production of hy-drogen peroxide and the highly reactive hydroxyl radical, eventsthat have been associated with asbestos toxicity (Timblin et al.,1999).
Silica Silicosis in humans may be acute or chronic; this distinc-tion is important conceptually because the pathological conse-quences are manifested quite differently. Acute silicosis occurs onlyin subjects exposed to a very high level of aerosol containing par-ticles small enough to be respirable (usually less than 5 �m) overa relatively short period, generally a few months to a few years.
2996R_ch15_525-534 4/12/01 1:32 PM Page 526
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 527
Table 15-1Industrial Toxicants That Produce Lung Disease
COMMON NAME
TOXICANT OF DISEASE OCCUPATIONAL SOURCE ACUTE EFFECT CHRONIC EFFECT
Asbestos Asbestosis Mining, construction, Fibrosis, pleuralshipbuilding, manufacture calcification, lungof asbestos-containing cancer, pleuralmaterial mesothelioma
Aluminum Aluminosis Manufacture of aluminum Cough, shortness Interstitial fibrosisdust products, fireworks, of breath
ceramics, paints, electricalgoods, abrasives
Aluminum Shaver’s disease, Manufacture of abrasives, Alveolar edema Interstitial fibrosis,abrasives corundum smelter’s smelting emphysema
lung, bauxite lungAmmonia Ammonia production, Upper and lower Chronic bronchitis
manufacture of fertilizers, respiratory tractchemical production, irritation, edemaexplosives
Arsenic Manufacture of pesticides, Bronchitis Lung cancer, bronchitis,pigments, glass, alloys laryngitis
Beryllium Berylliosis Ore extraction, manufacture Severe pulmonary Fibrosis, progressiveof alloys, ceramics edema, dyspnea, interstitial
pneumonia granulomatosis, lung cancer,cor pulmonale
Cadmium Welding, manufacture of Cough, pneumonia Emphysema, coroxide electrical equipment, pulmonale
alloys, pigments, smeltingCarbides of Hard metal disease Manufacture of cutting Hyperplasia and Peribronchial and
tungsten, edges on tools metaplasia of perivascular fibrosistitanium, bronchialtantalum epithelium
Chlorine Manufacture of pulp Cough, hemoptysis,and paper, plastics, dyspnea,chlorinated chemicals tracheobronchitis,
bronchopneumoniaChromium Production of Cr Nasal irritation, Lung cancer, fibrosis
(VI) compounds, paint bronchitispigments, reductionof chromite ore
Coal dust Pneumoconiosis Coal mining FibrosisCotton dust Byssinosis Manufacture of textiles Chest tightness, Reduced pulmonary
wheezing, dyspnea function, chronicbronchitis
Hydrogen Manufacture of chemicals, Respiratory irritation,fluoride photographic film, hemorrhagic
solvents, plastics pulmonary edemaIron oxides Siderotic lung Welding, foundry work, Cough Silver finisher’s lung:
disease; silver steel manufacture, subpleural andfinisher’s lung, hematite mining, jewelry perivascularhematite miner’s making aggregations oflung, arc welder’s macrophages;lung hematite miner’s lung:
diffuse fibrosislikepneumoconiosis; arcwelder’s lung: bronchitis
Isocyanates Manufacture of plastics, Airway irritation, Asthma, reducedchemical industry cough, dyspnea pulmonary function
2996R_ch15_525-534 4/12/01 1:32 PM Page 527
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com
528 UNIT 4 TARGET ORGAN TOXICITY
These patients have worsening dyspnea, fever, cough, and weightloss. There is rapid progression of respiratory failure, usually end-ing in death within a year or two. No known treatment modalityinfluences the relentless course of acute silicosis.
Chronic silicosis has a long latency period, usually more than10 years. Uncomplicated silicosis is almost entirely asymptomatic;little alteration is shown on routine pulmonary function tests evenafter the disease is radiographically demonstrable. The x-ray pic-ture presents fibrotic nodules, generally in the apical portion oflung. The hilar lymph nodes have peripheral calcifications knownas eggshell calcifications. Simple silicosis may progress into com-plicated silicosis, which is defined as the presence of conglomer-ate nodules larger than 1 cm in diameter. These nodules usuallyoccur in the upper and midlung zones. At an advanced stage theymay be surrounded by emphysematous bullae. Chronic silicosis isassociated with an increased incidence of tuberculosis.
Crystalline silica is a major component of the earth’s crust;after oxygen, silicon is the most common element. As a pure min-eral, silicon exists primarily in the form of its dioxide, silica (SiO2),which has a crystalline form in which a central silicon atom formsa tetrahedron with four shared oxygen atoms. The three principalcrystalline isomeric forms are quartz, tridymite, and cristobalite.The tetrahedral structure is linked to fibrogenic potential.
Stishovite, a rare crystalline variant without the tetrahedral con-formation, is biologically inert. Amorphous forms of silica such askieselguhr and vitreous silica have very low fibrogenic potential.The ubiquitous presence of silica has made it an occupational haz-ard ever since humans began shaping tools from stone, and silico-sis remains a significant industrial hazard throughout the world inoccupations such as mining and quarrying, sandblasting, andfoundry work. The main factors that affect the pathogenicity of sil-ica both in vivo and in vitro, in addition to its structure, are parti-cle size and concentration. Many studies have examined the rela-tionship of silica particle size to fibrogenicity. In studies withhumans, the most fibrogenic particle size appears to be about 1 �m(range 0.5 to 3�m). In animal experiments (rats, hamsters), thecomparable values appear to be 1 to 2 �m (range 0.5 to 5 �m). Inanimal models, there appears to be a direct relationship betweenthe concentration of silica dust to which an animal is exposed andthe intensity and rapidity of the histologic reaction in the lung.
The pathophysiological basis of pulmonary fibrosis in chronicsilicosis is probably better understood than is the etiology of anyother form of lung fibrosis. The role of pulmonary alveolarmacrophages in the ingestion of silica as an initiating event hasbeen established. Apparently, as part of the cytotoxic response ofa macrophage to silica ingestion, the macrophage may release cy-
Table 15-1Industrial Toxicants That Produce Lung Disease (Continued)
COMMON NAME
TOXICANT OF DISEASE OCCUPATIONAL SOURCE ACUTE EFFECT CHRONIC EFFECT
Kaolin Kaolinosis Pottery making FibrosisManganese Manganese Chemical and metal Acute pneumonia, Recurrent pneumonia
pneumonia industries often fatalNickel Nickel ore extraction, Pulmonary edema, Squamous cell carcinoma
smelting, electronic delayed by 2 days of nasal cavity andelectroplating, fossil fuels (NiCO) lung
Oxides of Welding, silo filling, Pulmonary Bronchiolitis obliteransnitrogen explosive manufacture congestion and
edemaOzone Welding, bleaching flour, Pulmonary edema Fibrosis
deodorizingPhosgene Production of plastics, Edema Bronchitis, fibrosis
pesticides, chemicalsPerchloro- Dry cleaning, metal Edema Cancer, liver and lung
ethylene degreasing, grainfumigating
Silica Silicosis, Mining, stone cutting, Acute silicosis Fibrosis, silicotuberculosispneumoconiosis construction, farming,
quarrying, sand blastingSulfur Manufacture of chemicals, Bronchoconstriction, Chronic bronchitis
dioxide refrigeration, bleaching, cough, chestfumigation tightness
Talc Talcosis Rubber industry, cosmetics FibrosisTin Stanosis Mining, processing of tin Widespread mottling of
x-ray without clinicalsigns
Vanadium Steel manufacture Airway irritation Chronic bronchitisand mucusproduction
2996R_ch15_525-534 4/12/01 1:32 PM Page 528
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 529
tokines and other substances that cause fibroblasts to replicateand/or increase their rate of collagen biosynthesis. The role of in-flammatory cells other than alveolar macrophages in this processis unknown. Also not understood is the role of the host’s immuneresponse and the roles of lymphocyte factors in stimulating fi-broblast proliferation and/or collagen synthesis by fibroblasts inlung fibrogenesis (Varani and Ward, 1997).
Lung Overload Caused by Particles Investigators studying thekinetics of the pulmonary clearance of particles have observed aslowing of the rate of alveolar clearance when deposited lung bur-dens are high. At about the same time, investigators evaluating in-haled particles in carcinogenesis bioassays observed excess tumorsin animals that inhaled very high concentrations of apparently in-ert so-called nuisance dusts, which were included in such experi-ments as negative controls. From these observations came a uni-fying hypothesis (Morrow, 1992) that clearance mechanisms in thedeep lung depending predominantly if not completely on phago-cytosis and migration of pulmonary alveolar macrophages can beoverwhelmed by quantities of respirable dusts far in excess of phys-iologic loads. As a consequence, lung burdens of these dusts per-sist for months or years, and completely unphysiologic mechanismsof disease pathogenesis may come into play. In rats, lung tumorshave been produced by particles such as Diesel exhaust that carrymutagens and carcinogens on their surface, but also by inert car-bon black particles. The issue of whether particle overloading de-fines a threshold in such experiments remains unresolved.
Naphthalene Naphthalene occurs in tars and petroleum and is awidely used precursor chemical for synthetic tanning agents,phthalic acid anhydride, carbaryl, and 2-naphthol. It is present inambient air. Smokers inhale substantial amounts of naphthalene incigarette smoke. In experimental animals, inhaled or parenterallyadministered naphthalene has shown remarkable species and tis-sue specificity: it produces extensive and selective necrosis in thebronchiolar epithelium of the mouse but much less necrosis in ratsand hamsters.
Animals treated with small doses of naphthalene or inhibitorsof microsomal oxidases show little or no tissue damage, implicat-ing metabolism in the toxicity of this chemical. Metabolism to theoxide is mediated through cytochrome P450 1A1 and 2F2. Naph-thalene epoxides may subsequently be conjugated with glutathioneand form adducts that presumably are not toxic. It is also possiblethat the epoxides undergo rearrangement to 1-naphthol with sub-sequent metabolism to quinones, which are potentially toxic com-pounds. In rats and other species, probably including humans, con-version of naphthalene is less stereospecific and rates of formationof the epoxide are much slower than in mice. This may explain thespecies differences that were noted previously (Franklin et al.,1993).
Oxygen Oxygen toxicity is mediated though increased produc-tion of partially reduced oxygen products such as superoxide an-ion, perhydroperoxy and hydroxyl radicals, peroxynitrite and pos-sibly singlet molecular oxygen. In infants who are given oxygentherapy after birth, a syndrome known as bronchopulmonary dys-plasia may develop. Lung pathology is characterized by necrotiz-ing bronchiolitis, fibroblast proliferation, squamous metaplasia ofthe bronchial lining, and destruction of alveolar ducts. In animalsexposed to 95 to 100% oxygen, diffuse pulmonary damage devel-ops and is usually fatal after 3 to 4 days. There is extensive dam-
age to the cells of the alveolar-capillary septum. Type I epithelialcells and capillary endothelial cells develop necrotic changes. Cap-illary damage leads to leakage of proteinaceous fluid and formedblood elements into the alveolar space. Hyaline membranes formedby cellular debris and proteinaceous exudate are a characteristicsign of pulmonary oxygen toxicity. In animals returned to air af-ter the development of acute oxygen toxicity, there is active cellproliferation (Frank, 1997).
Blood-Borne Agents That CausePulmonary Toxicity in Humans
Paraquat The bipyridylium compound paraquat, a widely usedherbicide, produces extensive lung injury when ingested by hu-mans. In patients who survive the first few days of acute paraquatpoisoning, progressive and eventually fatal lung lesions can de-velop. Paraquat lung disease is characterized by diffuse interstitialand intraalveolar fibrosis. The initial damage consists of wide-spread necrosis of both type I and type II epithelial cells of thealveolar region. Extensive proliferation of fibroblasts in the alveo-lar interstitium and the largely collapsed alveoli follows. Paraquataccumulates in the cells of the lung through the polyamine uptakesystem. Once inside the cells, paraquat continuously cycles fromits oxidized form to the reduced form, with the concomitant for-mation of active oxygen species. A mechanistic hypothesis to ex-plain paraquat toxicity involves oxidation of cellular NADPH andeventual depletion of the NADPH content of pulmonary cells(Smith, 1997).
Monocrotaline Monocrotaline (MCT) is a pyrrolizidine alkaloid,one of many structurally related naturally occurring products ofplants that have been identified in grains, honey and herbal teas.These compounds produce liver toxicity (hepatocellular necrosisand veno-occlusive disease). Although the hepatic metabolism ofthe pyrrolidine alkaloids is usually completed by 24 h, the ad-ministration of a single dose of monocrotaline is known to initiatea delayed lung injury. This pulmonary lesion is characterized by aremodeling of the vascular bed with hyperplasia of capillary en-dothelial cells, thickening of the arterial media, formation of mi-crothrombi, and eventually capillary occlusion with resulting hy-pertension of the pulmonary arterial system and hypertrophy of theright side of the heart.
Monocrotaline propagates changes in the contractile responseof arterial smooth muscle, changes in smooth muscle Na/K-ATP-ase activity, release of platelet factors, and decreased serotonintransport by vascular endothelial cells (Wilson et al., 1992).Monocrotaline is metabolized in the liver by cytochrome P450 3Ato a highly reactive pyrrole, a bifunctional alkylating agent, wheresome of the reactive pyrrole forms nontoxic conjugates with eitherglutathione or cysteine. A percentage of the remaining pyrrole isreleased from the liver and travels to other organs, such as the lungand possibly the kidney, via red blood cells (RBCs), where it ini-tiates endothelial injury. It had been previously shown that RBCscirculated through an isolated perfused buffer containing[14C]MCT, subsequently washed and recirculated through an iso-lated lung preparation could transfer electrophiles to pulmonarytissues. Recent evidence has indicated that the pyrrole is conju-gated to the RBCs, mainly to the bb-chains of hemoglobin (Lamééet al., 1997) . These pyrrole adducts may be particularly suscepti-ble to removal from globin chains following either enzymatic
2996R_ch15_525-534 4/12/01 1:32 PM Page 529
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

530 UNIT 4 TARGET ORGAN TOXICITY
combine with phospholipids and form indigestible complexes.Degradation of pulmonary surfactant is impaired, and the materialaccumulates in phagocytic cells. In humans, amiodarone may causedyspnea and cough. In animals and humans, the condition is fullyreversible on drug withdrawal (Reasor, 1997).
METHODS FOR STUDYING LUNG INJURY
Inhalation Exposure Systems
The generation of a gas available in high purity as a compressed“tank gas,” for example, SO2, O2, or NO2, is relatively straight-forward, and metering and dilution produce appropriate concen-trations for exposure. Monitoring and quantifying gaseous pollu-tants require either expensive detectors that need frequentcalibration (and usually a computer to process the tremendousamount of data generated) or very labor intensive wet chemicalanalysis procedures after sampled gases from the chambers are bub-bled through traps. Particle generation is difficult, and specializedreferences must be consulted (Wong, 1999).
Exposure chambers must allow for the rapid attainment of thedesired concentrations of toxicants, maintenance of desired levelshomogeneously throughout the chamber, adequate capacity for ex-perimental animals, and minimal accumulation of undesired prod-ucts associated with animal occupancy (usually ammonia, dander,heat, and carbon dioxide). Modern chambers tend to be fabricatedfrom inert materials (usually glass, stainless steel, and Teflon) andhave flow patterns that are designed to promote mixing and ho-mogeneity of the chamber atmosphere and prevent a buildup of un-desirable contaminants. A major concern with regard to exposureto acid aerosols has been the putative buildup of ammonia in cham-bers because of microbial action on animal excreta. Thus, maxi-mal loading factors and sanitation also must be considered in cham-ber usage. As a general rule, the total body volume of the animalsshould not exceed 5 percent of the chamber volume. Nose-only ex-posure chambers avoid some of these problems. Finally, concernfor the environment and the safety of facility personnel suggestprudence in how chambers are exhausted.
In inhalation studies, selection of animals with a respiratorysystem similar to that of humans is particularly desirable. The res-piratory system of monkeys most closely resembles that of humans.However, the availability and cost of animals and the necessity forspecial facilities for housing monkeys and performing long-termexposures, along with ethical considerations, including the con-finement of primates in small exposure chambers for prolonged pe-riods, severely limit the use of primates. Rats are widely used,although fundamental differences in respiratory anatomy (for ex-ample, lack of respiratory bronchioles) and function (rats are ob-ligate nose breathers) can complicate the extrapolation of effectsto humans. Guinea pigs and rabbits have been used to predict theresponse of humans to sulfuric acid (Amdur, 1989).
Pulmonary Function Studies
Numerous tests are available with which to study pulmonary func-tion and gas exchange in humans and experimental animals.Commonly used tests include measurement of VC, TLC, functionalresidual volume, TV, airway resistance, and maximum flow(Fig. 15-6). Additional tests evaluate the distribution of ventilation,
degradation or environmental changes observed during circulationthrough hepatic and pulmonary tissues and consequently interactwith key target proteins.
Bleomycin Bleomycin, a mixture of several structurally similarcompounds, is a widely used cancer chemotherapeutic agent. Pul-monary fibrosis, often fatal, represents the most serious form oftoxicity. The sequence of damage includes necrosis of capillary en-dothelial and type I alveolar cells, edema formation and hemor-rhage, delayed (after 1 to 2 weeks) proliferation of type II epithe-lial cells, and eventually thickening of the alveolar walls by fibroticchanges.
In many tissues, the cytosolic enzyme bleomycin hydrolaseinactivates bleomycin. In lung and skin, two target organs forbleomycin toxicity, the activity of this enzyme is low comparedwith that in other organs. Bleomycin stimulates the production ofcollagen in the lung. Before increased collagen biosynthesis,steady-state levels of mRNA coding for fibronectin and procolla-gens are increased, presumably subsequent to a bleomycin-mediated release of cytokines such as TGF-� and TNF. Bleomycinalso combines with Fe(II) and molecular oxygen; when it com-bines with DNA, single- and double-strand breaks are produced bya free radical reaction (Hoyt and Lazo, 1997).
Cyclophosphamide and 1,3-Bis-(2-Chloroethyl)-1-Nitrosourea(BCNU) Cyclophosphamide is widely used as an anticancer andimmunosuppressive agent. The undesirable side effects include hemorrhagic cystitis and pulmonary fibrosis. Cyclophosphamide ismetabolized by the cytochrome P450 system to two highly reac-tive metabolites: acrolein and phosphoramide mustard. In the lung,cooxidation with the prostaglandin-H synthase system, which hashigh activity in the lung, is a possibility. Although the exact mech-anism of action for causing lung damage has not been established,studies with isolated lung microsomes have shown that cy-clophosphamide and its metabolite acrolein initiate lipid peroxi-dation. Carmustine (BCNU) is an effective chemotherapeutic agentthat exerts its antitumor properties by reacting with cellular macro-molecules and forms inter- and intrastrand cross-links with DNA.In humans, a dose-related pulmonary toxicity is often noticed firstby a decrease in diffusion capacity. Pulmonary fibrosis caused bythis drug can be fatal. The mechanism of action is not entirely clear.It is possible that BCNU inhibits pulmonary glutathione disulfidereductase, an event that may lead to a disturbed GSH/GSSG statein pulmonary cells. Eventually, this state leaves the cell unable tocope with oxidant stress. High concentrations of oxygen in the in-spired air may enhance the pulmonary toxicity of BCNU and alsothat of the other anticancer drugs known to affect lung tissue: cy-clophosphamide and bleomycin. Several other chemotherapeuticagents can produce lung damage and pulmonary toxicity in patientstreated with these drugs can be a significant problem (Ramu andKehrer, 1997).
Cationic Amphophilic Drugs Several drugs with similar struc-tural characteristics that are called cationic amphophilic drugs(CADs) produce pulmonary lipidosis. The antiarrhythmic amio-darone and the anorexic chlorphentermine elicit such changes inhumans. Pulmonary lipidosis is characterized by the intracellularpresence, particularly in macrophages, of large concentric mem-branous structures now known to be secondary lysosomes. CADsinhibit phospholipases A and B, presumably because these drugs
2996R_ch15_525-534 4/12/01 1:32 PM Page 530
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 531
lung and chest wall compliance, diffusion capacity, and the oxy-gen and carbon dioxide content of the arterial and venous blood(Costa et al., 1991).
Many pulmonary function tests require active collaborationby the subject examined, for example, the so-called FEV1 (forcedexpiratory volume) during the first second of an active exhalation.This is an easy test to administer to humans, does not require so-phisticated equipment or a hospital setting, and is completely non-invasive. The subject is asked first to inhale deeply and then to ex-hale the air as quickly as possible. The test is often used inepidemiological studies or controlled clinical studies designed toassess the potential adverse effects of air pollutants. A reductionin FEV1 is usually indicative of impaired ventilation such as thatfound in restrictive (increased lung stiffness) or obstructive (ob-structed airflow) lung disease. Experimental animals, by contrast,cannot be made to maximally inhale or exhale at the investigator’swill. In experimental animals, FEV1 can be obtained, but the testis done under anesthesia. Expiration is forced by applying exter-nal pressure to the thorax or negative pressure to the airways.
Analysis of breathing patterns has been widely used to assessthe effects of irritants. This technique allows one to differentiatebetween sensory or upper airway irritants and “pulmonary” irri-tants. Highly water soluble irritants such as ammonia, chlorine, andformaldehyde produce upper respiratory tract irritation, whereasless soluble gases such as nitrogen dioxide and ozone generate pul-monary irritation. The sensory irritant pattern has been describedas slowing down respiratory frequency while increasing TV. Pul-monary irritants usually increase respiratory frequency and de-crease minute volume. The result is rapid, shallow breathing.
Analysis of volume-pressure curves of the lung provides someindication of lung compliance. Compliance (volume/ pressure) ismeasured as the slope of the volume-pressure curve; it gives someindication of the intrinsic elastic properties of the lung parenchymaand, when measured in vivo, the thoracic cage. This is a compar-atively easy test to perform in animals, requiring little specializedapparatus. Cannulation of the excised lungs and attachment to asyringe and manometer to measure volume and pressure are all thatis needed. Volume-pressure curves can be obtained from lungs
filled with air or physiological saline. The latter test is much moresensitive to structural changes in lung parenchyma, as the effectsof surfactant are eliminated in a saline-filled lung.
To accomplish proper oxygenation of venous blood and elim-ination of CO2, the gases have to diffuse across the air-blood bar-rier. Gas exchange may be hindered by the accumulation of fluidsor cellular elements in the alveoli (edema, pneumonic infiltrates),thickening of the alveolar wall (fibrosis), insufficient ventilation ofthe alveolar region (emphysema), or insufficient presence of oxy-gen transport elements (reduced alveolar blood volume or reducedamount of hemoglobin in the blood). Gas exchange can be evalu-ated by measuring the arterial partial pressure of both oxygen andCO2. In experimental animals, the collection of arterial blood mayrequire the presence of indwelling catheters.
In general, blood gas analysis is a comparatively insensitiveassay for disturbed ventilation because of the organism’s bufferingand reserve capacities. While it is a useful tool in clinical medi-cine, only the most severe obstructive or restrictive pulmonary alterations cause signs of impaired gas exchange in animals. Measurement of diffusion capacity with CO, a gas that binds with250 times higher affinity to hemoglobin than does oxygen, is moresensitive. The test is comparatively easy to perform in both hu-mans and laboratory animals and is widely used in toxicology studies.
Morphologic Techniques
The pathology of acute and chronic injury may be described afterexamination of the respiratory tract by gross inspection and underthe microscope. Morphologic evaluation should not be limited tothe peripheral lung; nasal passages, the larynx, and major airwaysmust be examined as carefully as is the lung parenchyma. For ex-ample, formaldehyde produces nasal tumors but not deep lung tu-mors in the rat. In hamsters exposed to cigarette smoke, cancerouschanges are found in the larynx but not in the more distal airways.
Careful consideration must be given to tissue fixation andpreparation. Nasal passages must be flushed with fixative. Afterdecalcification, cross sections should be cut at multiple levels; theregional distribution of lesions may vary from agent to agent.Proper fixation of the lung is done by vascular perfusion with fix-ative through the pulmonary artery or by instillation of fixativethrough the trachea. Perfusion fixation does not dislodge material(lining fluid, deposited particles) or cells in the lumen of the air-ways or the alveoli from their original position. Fixation by instil-lation does this, but it also keeps the alveoli open. It is done un-der controlled pressure, usually 30 cm H2O, and is required ifsemiquantitative or quantitative measurements will be made. Thechoice of fixative depends on how the lung will be further ana-lyzed. Formalin-based fixatives are satisfactory for routinehistopathology, whereas the use of more sophisticated techniquessuch as electron microscopy, immunohistochemistry, and in situhybridization require careful selection of the fixative.
Ordinary paraffin sections of respiratory tract tissue are suit-able for routine histopathologic analysis; gross pathologicalchanges such as inflammation and the presence of cancerous tis-sue can be detected easily. Plastic or epon sections about 1 �mthick are required for proper identification of different cell typeslining the airways or alveoli and for recognition of cytoplasmicchanges in damaged Clara cells. Other structural alterations, suchas degenerative changes or necrosis of type I epithelial cells or cap-
Figure 15-6. Typical lung volume measurements from individuals withnormal lung function, obstructive airways disease, or restrictive lungdisease.
Note that there is (1) a slowing of forced expiration in addition to gas trap-ping (an increase in residual volume) in obstructive disease and (2) a gen-eral decrease in lung volumes in restrictive disease. Note that the meas-urements read from left to right.
2996R_ch15_525-534 4/12/01 1:32 PM Page 531
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

532 UNIT 4 TARGET ORGAN TOXICITY
illary endothelial cells, usually are detected by transmission elec-tron microscopy (TEM). TEM is essential for an unequivocal iden-tification of cells in the alveolar interstitium and is used mainly inmorphometric analysis of the lung. Scanning electron microscopyallows visualization of the surface of interior lung structures, re-veals alterations in the tissue surface, and detects rearrangement ofthe overall cell population. Confocal microscopy, consisting of alaser microscope coupled to a computer, allows examination ofthick sections and discovery of specific cell types deep within thetissue; it is an ideal tool for three-dimensional reconstruction ofnormal and damaged lung.
Morphometry, the quantitative description of structure, refersto a quantitative analysis of tissue (Gehr et al., 1993). Measure-ments made in two dimensions on photographs taken under the mi-croscope allow one to measure areas, the thickness of a structure,and numerical density. With the help of appropriate formulas, val-ues such as the volume occupied by a specific cell population inthe entire lung parenchyma can be calculated. The method is par-ticulalry useful for the detection of subtle toxic effects in the lungparenchyma (Witschi et al., 1999).
Additional tools for the study of toxic lung injury include im-munohistochemistry, in situ hybridization, and analysis of cell ki-netics. Antibodies to a variety of enzymes, mediators, and otherproteins are available. It is possible to identify cell types that carrycertain enzymes and their anatomic locations. This information isimportant for mechanistic studies. In situ hybridization allows oneto visualize anatomic sites where a specific gene product is ex-pressed, for example, collagen production in a fibrotic lung. Thistechnique is especially important in an organ such as the lung wherethere are more than 40 morphologically distinct cell types present.Ascribing a given metabolic capability to a specific cell type requires evaluation of gene expression and/or protein produc-tion in specific cells in situ. Flow cytometry is valuable in the study of cell populations prepared from the lung. The techniquerequires dissociation of the lung parenchyma into its individual cellpopulations. Different lung cells then can be identified and iso-lated.
Pulmonary Lavage
Pulmonary edema and/or pulmonary inflammation appear to beobligatory early events in acute and chronic lung injury. Markersof these processes generally are chosen to reflect lung edema orcellular changes in the lung. The most popular of these types ofassays have quantified various parameters in lung lavage fluid fromanimals exposed to pneumotoxic substances. Generally, the lungsof exposed and control animals are washed with multiple smallvolumes of isotonic saline This technique has the further advan-tage of allowing direct comparisons with data accessible from nor-mal human volunteers or patients undergoing bronchopulmonarylavage for therapeutic purposes. Current emphasis seems to be onthe measurement of polymorphonuclear leukocytes, macrophages,and monocytes (and their phagocytotic capabilities) in the cellularfraction and the measurement of lactate dehydrogenase (and itssubstituent isoenzymes), N-acetylglucosaminidase, acid or alkalinephosphatase, other lysosomal hydrolases, lavageable total proteinand/or albumin, and sialic acid. Although such measurements haveoften formed the basis of mechanistic interpretations, we really donot have a rigorous theoretical understanding of the exact sourceof any of these parameters.
Measurement of apparent changes in the permeability of theair-blood barrier by quantification of intravenously injected tracerin lung lavage fluid is another useful index of lung damage. Themovement of low-molecular-weight tracers such as [51Cr] EDTAacross the blood-air barrier occurs rapidly (within 10 min of IV in-jection). High-molecular-weight tracers such as radiolabeled albu-min also have been used for this purpose.
In Vitro Approaches
In vitro systems are particularly suited for the study of mechanismsthat cause lung injury. The following systems are widely used(Postlethwait and Bidani, 1997).
Isolated Perfused Lung The isolated perfused lung method isapplicable to lungs from many laboratory animal species (rabbit,rat, mouse, guinea pig). The lung, in situ or excised, is perfusedwith blood or a blood substitute through the pulmonary arterialbed. At the same time, the lung is actively (through rhythmicinflation-deflation cycles with positive pressure) or passively (bycreating negative pressure with an “artificial thorax” in which thelung is suspended) ventilated. Toxic agents can be introduced intothe perfusate or the inspired air. Repeated sampling of the perfusateallows one to determine the rate of metabolism of drugs and themetabolic activity of the lung.
Lung Explants and Slices Slices and explants from the con-ducting airways or the lung parenchyma allow one to examine bio-chemical and morphologic changes in the lung parenchyma with-out intervening complications from cells migrating into the tissue(e.g., leukocytes). If the lung is first inflated with agar, the alveo-lar spaces remain open in the explant. Slices prepared in this waycan be kept viable for several weeks, and the mechanisms of de-velopment of chronic lesions can be studied.
Microdissection Many inhalants act in circumscribed regions ofthe respiratory tract, such as the terminal bronchioles, a region es-pecially rich in metabolically highly competent Clara cells. Mi-crodissection of the airways consists of the stripping of smallbronchi and terminal bronchioli from the surrounding parenchymaand maintenance of the isolated airways in culture. Specific bio-chemical reactions predominantly located in the cells of the smallairways can then be studied with biochemical or morphologic tech-niques.
Organotypic Cell Culture Systems Tissue culture systems havebeen developed in which epithelial cells maintain their polarity,differentiation, and normal function similar to what is observed invivo. Epithelial cell surfaces are exposed to air (or a gas phase con-taining an airborne toxic agent), while the basal portion is bathedby a tissue culture medium. Epithelial cells may be seeded on topof a suitable supporting material (e.g., collagen or nitrocellulosemembranes) with mesenchymal cells seeded on the other side toobserve epithelial cell–fibroblast interactions.
Isolated Lung Cell Populations Many specific lung cell typeshave been isolated and maintained as primary cultures in vitro.Alveolar macrophages are easily obtained from human and animallungs by lavage. Their function can be examined in vitro with orwithout exposure to appropriate toxic stimuli. Type II alveolar ep-
2996R_ch15_525-534 4/12/01 1:32 PM Page 532
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

CHAPTER 15 TOXIC RESPONSES OF THE RESPIRATORY SYSTEM 533
ithelial cells are isolated after digestion of the lung. Direct isola-tion of type I epithelial cells has also been successful. Systems forthe isolation and culture of Clara cells and neuroepithelial cells areavailable. Lung fibroblasts are easily grown and have been studiedin coculture with epithelial cells. Multiple primary cell cultures and
cell lines have been established from lung tumors found in exper-imental animals and humans. Isolated cell techniques suffer frompossible enzymatic digestion of critical cellular components. Cau-tion should be exercised in the final interpretation of experimentsutilizing this approach.
REFERENCES
Alarie Y, Nielsen GD, Abraham MD: A theoretical approach to the Fergu-son principle and its use with nonreactive and reactive airborne chem-icals. Pharmacol Toxicol 83:270–279, 1998.
Amdur MO: Sulfuric acid: The animals tried to tell us. 1989 HerbertStokinger Lecture. Appl Ind Hyg 4:189–197, 1989.
Barnes PJ, Chung KF, Page CP: Inflammatory mediators of asthma: An up-date. Pharmaco. Rev 50:575–596, 1998.
Beeson WL, Abbey DE, Knutsen SF: Long-term concentrations of ambientair pollutants and incident lung cancer in California adults: Resultsfrom the ASHMOG study. Environ Health Perspect 106:813–823,1998.
Buckpitt AR, Cruikshank MK: Biochemical function of the respiratory tract:Metabolism of xenobiotics, in Sipes IG, McQueen CA, Gandolfi JA(eds): Comprehensive Toxicology. Vol 8. Roth RA (ed): Toxicology ofthe Respiratory System. Oxford, England: Elsevier, 1997, pp 159–186.
Costa DL, Tepper JS, Raub JA: Interpretations and limitations of pulmonaryfunction testing in small laboratory animals, in Parent RA (ed): Com-parative Biology of the Normal Lung. Vol 1. Treatise on PulmonaryToxicology. Boca Raton, FL: CRC Press, 1991, pp 367–399.
Crapo J, Miller FJ, Mossman B, et al: Relationship between acute inflam-matory responses to air pollution and chronic lung disease. Am RevRespir Dis 145:1506–1512, 1992.
Cross DE, van der Vliet A, Louie S, et al: Oxidative stress and antioxidantsat biosurfaces: Plants, skin, and respiratory tract surfaces. EnvironHealth Perspect 106(suppl 5):1241–1251, 1998.
Fanucchi MV, Harkema JR, Plopper CG, Hotchkiss JA: In vitro culture ofmicrodissected rat nasal airway tissues. Am J Respir Cell Mol Biol20:1274–1285, 1999.
Frank L: Oxygen toxicity, in Sipes IG, McQueen CA, Gandolfi JA (eds):Comprehensive Toxicology.Vol 8. Roth RA (ed): Toxicology of the Res-piratory System. Oxford, England: Elsevier, 1997, pp 275–302.
Franklin RB, Plopper CG, Buckpitt AR: Naphthalene and 2-methylnaph-thalene-induced pulmonary bronchiolar epithelial cell necrosis: Me-tabolism and relationship to toxicity, in Gram TE (ed): InternationalEncyclopedia of Pharmacology and Therapeutics. Sec 138: MetabolicActivation of Toxicity of Chemical Agents to Lung Tissue and Cells.New York: Pergamon Press, 1993, pp 123–144.
Gehr P, Geiser M, Stone KC, Crapo JD: Morphometric analysis of the gasexchange region of the lung, in: Gardner DE, Crapo JD, McClellanRO (eds): Toxicology of the Lung, 2d ed. New York: Raven Press, 1993,pp 111–154.
Graziano SL, Gamble GP, Newman NB, et al: Prognostic significance ofK-ras codon 12 mutations in patients with resected stage I and II non-small-cell lung cancer. J Cli Oncol 17:668–675, 1999.
Hahn FF: Carcinogenic responses of the respiratory tract, in Sipes IG, Mc-Queen CA, Gandolfi JA (eds): Comprehensive Toxicology. Vol 8. RothRA (ed): Toxicology of the Respiratory System. Oxford, England:Elsevier, 1997, pp 187–202.
Hecht SS: Tobacco smoke carcinogens and lung cancer. J Natl Cancer Inst91:1194–1210, 1999.
Hoyt DG, Lazo JS: Bleomycin-induced pulmonary fibrosis, in Sipes IG,McQueen CA, Gandolfi JA (eds): Comprehensive Toxicology. Vol 8.Roth RA (ed): Toxicology of the Respiratory System. Oxford, Eng-land: Elsevier, 1997, pp 543–554.
ILSI Risk Science Institute Workshop: The relevance of the rat lung re-
sponse to particle overload for human risk assessment. Inhalat Toxi-col 12:1–148, 2000.
International Agency for Research on Cancer: Overall evaluations of car-cinogenicity. An updating of IARC monograph vols 1–47, suppl 7.Lyons, France: IARC, 1987.
International Agency for Research on Cancer: Iarc Monographs on theEvaluation of Carcinogenic Risks to Humans: Beryllium, Cadmium,Mercury and Exposures in the Glass Manufacturing Industry. Vol 58.Lyons, France: IARC, 1993.
Karol MH, Tollerud DJ, Campbell TP, et al: Predictive value of airwayshyperresponsiveness and circulating IgE for identifying types of re-sponses to toluene diisocyanate inhalation challenge. Am J Respir CritCare Med 149:611–615, 1994.
Kimball JS, Miller F: Regional respiratory-tract absorption of inhaled re-active gases: A modeling approach, in Gardner DE, Crapo JD, Mc-Clellan RO (eds): Toxicology of the Lung, 3d ed. Philadelphia: Taylor& Francis, 1999, pp 557–597.
Laméé MW, Jones AD, Morin DW, et al: Association of dehydro-monocrotaline with rat red blood cells. Chem Res Toxicol 10:694–701, 1997.
Leikauf G, Driscoll K: Cellular approaches in respiratory tract toxicology,in Gardner DE, Crapo JD, McClellan RO (eds): Toxicology of the Lung,2d ed. New York: Raven Press, 1993, pp 335–370.
Malkinson AM: Molecular comparison of human and mouse pulmonaryadenocarcinomas. Exp Lung Res 24:541–555, 1998.
Massague J. TGF-� signal transduction. Annu Rev Biochem 67:753–791,1998.
Medinsky MA, Bond JA, Schlosser PM, Morris JB: Mechanisms and mod-els for respiratory-tract uptake of volatile organic chemicals, in Gard-ner DE, Crapo JD, McClellan RO (eds): Toxicology of the Lung, 3ded. Philadelphia: Taylor & Francis, 1999, pp 483–512.
Mercer RR, Crapo JD: Architecture of the acinus, in Parent RA (ed): Trea-tise on Pulmonary Toxicology: Comparative Biology of the NormalLung. Boca Raton, FL: CRC Press, 1991, pp 109–120.
Miller F: Dosimetry of particles in laboratory animals and humans, in Gard-ner DE, Crapo JD, McClellan RO (eds): Toxicology of the Lung, 3ded. Philadelphia: Taylor & Francis, 1999, pp 513–555.
Morrow PE: Dust overloading in the lungs: Update and appraisal. ToxicolAppl Pharmacol 113:1–12, 1992.
National Cancer Institute: Health Effects of Exposure to Environmental To-bacco Smoke: The Report of the California Environmental ProtectionAgency. Smoking and Tobacco Control Monograph No. 10. NIH Pub.No. 99-4645. Bethesda, MD: U.S. Department of Health and HumanServices, National Institutes of Health, National Cancer Institute,1999.
O’Byrne PM, Postma DS: The many faces of airway inflammation. AmRespir Crit Care Med 159:541–566, 1999.
Pinkerton KE, Gehr P, Crapo JD: Architecture and cellular composition ofthe air-blood barrier, in Parent RA (ed): Treatise on Pulmonary Toxi-cology: Comparative Biology of the Normal Lung. Boca Raton, FL:CRC Press, 1991, pp 121–128.
Postlethwait EM, Bidani A: In vitro systems for studying respiratory sys-tem toxicology, in Sipes IG, McQueen CA Gandolfi JA (eds): Com-prehensive Toxicology. Vol 8. Roth RA (ed): Toxicology of the Respi-ratory System. Oxford England: Elsevier, 1997, pp 249–264.
2996R_ch15_525-534 4/12/01 1:32 PM Page 533
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com

534 UNIT 4 TARGET ORGAN TOXICITY
Raabe OG: Respiratory exposure to air pollutants, in Swift DL, Foster WM(eds): Air Pollutants and the Respiratory Tract. New York: MarcelDekker 1999, pp 39–73.
Ramazzini B: Disease of Workers. Translated from the Latin text De Mor-bis Artificum by Wright WC. New York and London: Hafner, 1964.
Ramu K, Kehrer JP: The pulmonary toxicity of chemotherapeutic agents,in Sipes IG, McQueen CA, Gandolfi JA (eds): Comprehensive Toxi-cology. Vol 8. Roth RA (ed): Toxicology of the Respiratory System.Oxford, England: Elsevier, 1997, pp 521–541.
Reasor M: Cationic amphophilic drugs, in Sipes IG, McQueen CA, Gan-dolfi JA (eds): Comprehensive Toxicology. Vol 8. Roth RA (ed): Tox-icology of the Respiratory System. Oxford, England: Elsevier, 1997,pp 555–566.
Smith LL: Paraquat, in Sipes IG, McQueen CA, Gandolfi JA (eds): Com-prehensive Toxicology. Vol 8. Roth RA (ed): Toxicology of the Respi-ratory System. Oxford, England: Elsevier, 1997, pp 581–590.
Snider GL, Kleinerman J, Thurlbeck WM, Bengali ZH: The definition em-physema: Report of a National Heart, Lung, and Blood Institute Work-shop. Am Rev Respir Dis 132:182–185, 1985.
Timblin C, Janssen-Heininger Y, Mossmann BT: Pulmonary reactions andmechanisms of toxicity of inhaled fibers, in Gardner DE, Crapo JD,McClellan RO (eds): Toxicology of the Lung, 3d ed. Philadelphia: Tay-lor & Francis, 1999, pp 221–240.
Varani J, Ward PA: Activation of the inflammatory response by asbestosand silicate mineral dusts, in Wallace KB (ed): Free Radical Toxicol-ogy. New York: Taylor & Francis 1997, pp 295–322.
Weibel ER: Is the lung built reasonably? The 1983 J. Burns Anderson lec-ture. Am Rev Respir Dis 128:752–760, 1983.
Wilson DW, Segall HJ, Pan LC, et al: Mechanism and pathology ofmonocrotaline pulmonary toxicity. CRC Crit Rev Toxicol 22:307–325,1992.
Wingo PA, Ries LA, Giovino GA, et al: Annual report to the nation on thestatus of cancer, 1973–1996, with a special section lung cancer andtobacco smoking. J Natl Cancer Inst 91:675–690, 1999.
Witschi HP: Selected examples of free-radical-mediated lung injury, in Wallace KB (ed): Free Radical Toxicology. New York: Taylor & Francis, 1997a, pp 279–294.
Witschi HP: Cell damage and cell renewal in the lung, in Sipes IG, Mc-Queen CA, Gandolfi JA (eds): Comprehensive Toxicology. Vol 8. RothRA (ed): Toxicology of the Respiratory System. Oxford, England:Elsevier, 1997b, pp 231–248.
Witschi HP, Espiritu I, Pinkerton KE, et al: Ozone carcinogenesis revisited.Toxicol Sci 52:62–167, 1999.
Wong BA: Inhalation exposure systems design, methods, and operation, inGardner DE, Crapo JD, McClellan RO (eds): Toxicology of the Lung,3d ed. Philadelphia:Taylor & Francis 1999, pp 1–53.
Zemp E, Elsasser S, Schindler C, et al: Long-term ambient air pollutionand respiratory symptoms in adults (SAPALDIA study). The SAPAL-DIA Team. Am J Respir Crit Care Med 159:1257–1266, 1999.
Zhang HY, Phan S: Inhibition of myofibroblast apoptosis by transform-ing growth factor �1. Am J Respir Cell Mol Biol 21:658 – 665,1999.
2996R_ch15_525-534 4/12/01 1:32 PM Page 534
Copy
right
ed M
ater
ial
Copyright © 2001 by The McGraw-Hill Companies Retrieved from: www.knovel.com