-
8/9/2019 Toxic Anteror Segment Syndrome
1/40
TASS
DR.PUSHPANJALI
-
8/9/2019 Toxic Anteror Segment Syndrome
2/40
Introduction :
Initially referred to as sterile endophthalmitisor postoperative
uveitis of unknown cause.
Accurately termed TOXIC ANTERIORSEGMENT SYNDROME(TASS)by Monson
etal in 1992.
Toxic endothelial cell destruction (TECD)syndrome : a variant of
TASS with localizedendothelial damage.
-
8/9/2019 Toxic Anteror Segment Syndrome
3/40
Definition :
TOXIC ANTERIOR SEGMENT SYNDROME
Sterile, acute postoperative inflammatoryreaction in which a
noninfectious substanceenters the anterior segment and induces
toxic
damage to the intraocular tissues that mayoccur following any
anterior segment surgery.
-
8/9/2019 Toxic Anteror Segment Syndrome
4/40
Outbreak of toxic anterior segment syndrome
after vitreous surgery
Arch Soc Esp Oftalmol. 2009 Aug;84(8):403-5. Andonegui J,
Jimnez-Lasanta L, Aliseda D, Lameiro F. Servicio de Oftalmologa,
Hospital de Navarra, 31008 Pamplona,
Espaa.( [email protected]) CASE REPORT: An outbreak of Toxic
Anterior Segment Syndrome
after vitreoretinal surgery is reported. Two patients underwent
exclusively vitrectomy while the other
three patients were operated of vitrectomy and some
otheranterior segment procedure.
DISCUSSION: Toxic Anterior Segment Syndrome is a
sterilepostoperative inflammation due to any non infectious
substancethat reaches the anterior segment during surgery. It
occurs inoutbreaks and while most of the cases have been reported
afteranterior segment procedures, this case demonstrates
thatdevelopment after vitreoretinal surgery is also a
possibility.
-
8/9/2019 Toxic Anteror Segment Syndrome
5/40
Severe Intraocular Inflammation after Intravitreal
Injection of Bevacizumab.
Ophthalmology. 2010 Mar;117(3):512-516.e2. Epub 2010 Jan 19.
Sato T, Emi K, Ikeda T, Bando H, Sato S, Morita SI, Oyagi T,
Sawada K.
Department of Ophthalmology, Osaka Rosai Hospital, Sakai,
Japan.
PURPOSE: To report 5 cases of severe intraocular inflammation
that developed after an intravitrealinjection of the same lot of
bevacizumab.
PARTICIPANTS: Patients treated with an intravitreal injection of
bevacizumab (lot B3003B01). METHODS: The clinical charts of 35 eyes
of 35 consecutive patients who were treated with intravitreal
injection of lot B3003B01 bevacizumab from December 18, 2008,
through January 20, 2009, werereviewed.
MAIN OUTCOME MEASURES: Incidence of intraocular inflammation,
results of bacterial cultures, best-corrected visual acuity (BCVA),
and endothelial cell density.
RESULTS: Five (14.3%) of the 35 cases had severe intraocular
inflammation, and the inflammation hadsome characteristics of toxic
anterior segment syndrome (TASS). Five of the 5 cases had a
predominantly
anterior chamber reaction, and 4 of the 5 cases were accompanied
by hypopyon. Undiluted samplescollected from both the aqueous and
vitreous of the 5 cases were culture negative. The BCVA was
0.66+/-0.29 (mean+/-standard deviations) logarithm of the minimum
angle resolution (logMAR) units, and theendothelial cell density
was 2683.6+/-97.3/mm(2) before the intravitreal bevacizumab. At the
final visit,the BCVA was 0.44+/-0.36 logMAR units, and the cell
density was 2679.0+/-217.5/mm(2). Thesedifferences were not
significant (P = 0.171 and 0.964).
CONCLUSIONS: These observations indicate that an intravitreal
injection of bevacizumab can induce sterileendophthalmitis that has
characteristics of TASS.
-
8/9/2019 Toxic Anteror Segment Syndrome
6/40
Pathophysiology :
TASS results from the inadvertent entry of toxicsubstances into
the anterior chamber.
The histopathologic hallmark of TASS is toxic
anterior segment damage. Cellular necrosis and/or apoptosis
and
extracellular damage occur, resulting in thesevere acute
inflammatory response.
The corneal endothelium is often the mostdamaged structure
because of its inability toregenerate and replace dead cells.
Trabecular meshwork damage - IOP
-
8/9/2019 Toxic Anteror Segment Syndrome
7/40
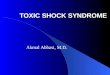
Presentation :
The hallmark of TASS is an inflammatory reaction in theanterior
segment of the eye that starts within 12 to 48 hoursafter
surgery.
The most common clinical findings in patients are
(1) diffuse, limbus-to-limbus corneal edema,
(2) increased inflammation in the anterior chamber withhypopyon
formation, and the deposition of fibrin.
(3) a dilated pupil with an irregularity of the iris and(4)
potential damage to the trabecular meshwork with
subsequent secondary glaucoma.
(5) Cystoid macular edema in few cases.
(6) rapidly improves after topical steroids.
-
8/9/2019 Toxic Anteror Segment Syndrome
8/40
Clinical course :
Mild presentation : rapid clearing of the cornealedema with no
long-term corneal or trabeculardamage and normal or near normal
visual acuity.
Moderate presentation : persistent corneal edemathat will take
several weeks to clear, intraocularpressure that is difficult to
control, and a moderateeffect on visual acuity.
Severe presentation of TASS: marked corneal edema
that does not clear, iris and trabecular meshworkdamage with
resultant glaucoma, and possible cystoidmacular edema. Visual
outcome is usually poordespite medical or surgical
intervention.
-
8/9/2019 Toxic Anteror Segment Syndrome
9/40
TASS VERSUS ENDOPHTHALMITIS
-
8/9/2019 Toxic Anteror Segment Syndrome
10/40
TASS Vs ENDOPHTHALMITIS
1. TIMING OF THE DISEASE 2. PAIN
-
8/9/2019 Toxic Anteror Segment Syndrome
11/40
TASS Vs ENDOPHTHALMITIS
3. CONJUCTIVAL & LID REACTION 4. CORNEAL EDEMA
-
8/9/2019 Toxic Anteror Segment Syndrome
12/40
TASS Vs ENDOPHTHALMITIS
5.IRIS FINDINGS 6. IOP
-
8/9/2019 Toxic Anteror Segment Syndrome
13/40
TASS Vs ENDOPHTHALMITIS
7. THERAPEUTIC RESPONSE
-
8/9/2019 Toxic Anteror Segment Syndrome
14/40
TASS ENDOPHTHALMITISCAUSE Noninfectious reaction to toxic
agent present in:BSS solution
Antibiotic injectionEndotoxinResidue
Bacterial, fungal, or viralInfection
ONSET 12-24 hours 4-7 days
SIGNS/SYMPTOMS
*distinguishingfeature
Blurry visionPain: none, or mild to moderateCorneal edema:
diffuse, limbus to
limbus*Pupil: dilated, irregular, nonreactive*
Increased IOP*
Anterior chamber: mild to severereaction with cells,
flare,hypopyon, fibrinSigns and symptoms are limited to
anterior chamber*
Gram stain and culture negative
Decreased VA
Pain (25% have no pain)Lid swelling with edema
Conjunctival injectionHyperemiaAnterior chamber:
markedinflammatory response withhypopyonVitreous involvement
Inflammation in entire
ocular cavity*
TREATMENT Rule out infectionCulture anterior chamberIntensive
corticosteroids
Monitor IOP closely for signs ofdamage to trabecular meshworkand
side effects of steroidsWatch closely over next few hours
for signs of bacterial infection
Culture anterior chamberand vitreousIntravitreal and topical
antibiotics
Vitrectomy
-
8/9/2019 Toxic Anteror Segment Syndrome
15/40
Causes :
1. Substances that accidentally enter the eye during or
after
surgery:
Topical antiseptic
Topical lidocaine jelly, anesthetic agents
Powder from gloves
Particles from tray, lint from drapes
Air contaminants
Plain water on instruments
Preservatives in solutions/ medications used
Topical ointment (an eye patch that is too tight may cause the
wound tosuck the antibiotic back inside the eye)
-
8/9/2019 Toxic Anteror Segment Syndrome
16/40
Causes :
2. Substances that are introduced as part of the OR procedure:
Improper irrigation solutions (BSS) Inappropriate pH (< 6.5 -
> 8.5), chemical composition or osmolality Addition of
medications/ antibiotics (the use of vancomycin is still
controversial)
Toxic preservatives in BSS (benzalkonium chloride - 1000 corneas
damaged inIndia)
Contaminated BSS: During manufacturing process During addition
of epinephrine (e.g. sulfites) or antibiotics Out-dated BSS
(contamination with glue that leeches inside the bag)
Mitomycin-C
Contaminants on IOL Manufacturer debris Residual polishing
compounds (e.g. Memorylens ) During manipulation: powder from
gloves
-
8/9/2019 Toxic Anteror Segment Syndrome
17/40
Causes :
3. Irritants from surgical instruments due to improper
cleaning/sterilization: Dry blood and debris left on
instruments
Tissue and dry visco-elastics found in re-used phaco tips,
irrigation/aspiration tips andcannulated instruments - flushed into
the next patients eye
Irritants from deterioration of instruments due to
re-processing: re-usable equipment and re-used single use device
(SUD)
Residue of detergent on instruments not properly rinsed
Coliforms and metals left on/in instruments (tap water used
instead of distilled, sterile water)
Endotoxins: gram-negative bacteria lodged inside the improperly
irrigated cannulated
instruments die during sterilization but release endotoxins that
are flushed into the nextpatients eye (e.g. contaminated ultrasonic
cleaning solution with Klebsiella pneumoniaebacteria )
Oxidized metal deposits/residues on instruments from Plasma Gas
Sterilization System
Ethylene oxide gas residue on instruments from using E.O.
Sterilization Method
-
8/9/2019 Toxic Anteror Segment Syndrome
18/40
Postoperative sterile endophthalmitis
(TASS) associated with the memorylens.
Faisal S. Jehan MD, Nick Mamalis MD, Terrence S. Spencer MD,
Luther L. Fry MD, Richard S. Kerstine
MD and Randall J. Olson MD
John A. Moran Eye Center, Univeristy of Utah, Salt Lake City,
Utah, USA
Journal of Cataract & Refractive Surgery, Volume 26, Issue
12, December 2000, Page 1777
Purpose : To report 10 cases of delayed-onset acute intraocular
inflammation following cataract extractionand posterior chamber
implantation of the MemoryLens intraocular lens (IOL).
Methods : This retrospective study evaluated 10 cases of
postoperative inflammation that occurred aftercataract extraction
with placement of the posterior chamber MemoryLens IOL. Protocols
of theIntermountain Ocular Research Center used to analyze
outbreaks of unexplained postoperativeinflammation as well as
medical records were reviewed.
Results : Nine patients had uneventful cataract extraction and 1
had a small anterior capsule tear withplacement of the MemoryLens
IOL. All 10 patients presented with increased anterior
segmentinflammation a mean of 7.8 days (range 1 to 21 days) after
surgery. Three cases were tapped and wereculture negative, and 7
were presumed noninfectious. The anterior segment inflammation
improved in all
patients. Treatment of the 7 patients included intensive topical
steroids. Careful analysis of theinflammation has not revealed an
obvious etiology; however, the MemoryLens was associated with all
thecases.
Conclusions :We postulate that these cases of noninfectious
postoperative endophthalmitis may beassociated with the
MemoryLens.
-
8/9/2019 Toxic Anteror Segment Syndrome
19/40
Outbreak of toxic anterior segment syndromeassociated with
glutaraldehyde after cataract surgery
nal M, Ycel I, Akar Y;J Cataract Refract Surg vol. 32, 1696 -
1701, 2006
Purpose: To present clinical findings of a cluster of cases of
toxic anterior segmentsyndrome (TASS) after uneventful
phacoemulsification cataract surgery.
Setting: Department of Ophthalmology, Akdeniz University,
Antalya, Turkey.
Methods: Six eyes of 6 patients developed TASS after
uneventfulphacoemulsification cataract surgery with implantation of
a 3-piece acrylic IOLperformed by 2 ophthalmologists on the same
day. Clinical findings includedcorneal edema, Descemet's membrane
folds, anterior chamber reaction, fibrinformation, and irregular,
dilated, and unreactive pupils.
Results: Glutaraldehyde 2% solution was used inadvertently by
the operatingroom staff who cleaned and sterilized reusable ocular
instruments beforeautoclaving. None of the affected corneas
improved. Additional surgicalprocedures were required and included
penetrating keratoplasty, trabeculectomy,and glaucoma tube
implantation.
Conclusions: Glutaraldehyde in concentrations generally used for
cold sterilizationis highly toxic to the corneal endothelium. The
operating room staff involved insterilizing instruments should be
well educated about and careful to follow the
protocols to properly clean and sterilize reusable ocular
instruments.
-
8/9/2019 Toxic Anteror Segment Syndrome
20/40
Outbreak of toxic anterior segment syndrome following cataract
surgery
associated with impurities in autoclave steam moisture.
Infect Control Hosp Epidemiol. 2006 Mar;27(3):294-8. Epub 2006
Feb 22.
Hellinger WC, Hasan SA, Bacalis LP, Thornblom DM, Beckmann SC,
Blackmore C, Forster TS, Tirey JF, RossMJ, Nilson CD, Mamalis N,
Crook JE, Bendel RE, Shetty R,Stewart MW, Bolling JP, Edelhauser
HF.
Division of Infectious Diseases, Mayo Clinic, Jacksonville, FL
32224, USA.
METHODS: Medical records of patients who underwent cataract
surgery during the outbreak werereviewed, and surgical team members
who participated in the operations were interviewed. Potential
causes of TASS were identified and eliminated. Feedwater from
autoclave steam generators and steamcondensates were analyzed by
use of spectroscopy and ion chromatography.
RESULTS: During the outbreak, 8 (38%) of 21 cataract operations
were complicated by TASS, comparedwith 2 (0.07%) of 2,713
operations performed from January 1996 through November 2002.
Results of aninitial investigation suggested that cataract surgical
equipment may have been contaminated bysuboptimal equipment
reprocessing or as a result of personnel changes. The frequency of
TASS decreased(1 of 44 cataract operations) after reassignment of
personnel and revision of equipment reprocessingprocedures. Further
investigation identified the presence of impurities (eg, sulfates,
copper, zinc, nickel,
and silica) in autoclave steam moisture, which was attributed to
improper maintenance of the autoclavesteam generator in the
outpatient surgical center. When impurities in autoclave steam
moisture wereeliminated, no cases of TASS were observed after more
than 1,000 cataract operations.
CONCLUSION: Suboptimal reprocessing of cataract surgical
equipment may evolve over time in busy,multidisciplinary surgical
centers. Clinically significant contamination of surgical equipment
may resultfrom inappropriate maintenance of steam sterilization
systems. Standardization of protocols forreprocessing of cataract
surgical equipment may prevent outbreaks of TASS and may be of
assistanceduring outbreak investigations.
-
8/9/2019 Toxic Anteror Segment Syndrome
21/40
Toxic anterior segment syndrome and possible association
with
ointment in the anterior chamber following cataract surgery.
J Cataract Refract Surg. 2006 Feb;32(2):227-35.
Werner L, Sher JH, Taylor JR, Mamalis N, NashWA, Csordas JE,
Green G, Maziarz EP, Liu XM.
John A. Moran Eye Center, University of Utah, Salt Lake City,
Utah 84132, USA.
PURPOSE: To report clinical and laboratory findings of 8 cases
of TASS related to an oily
substance in the anterior chamber of patients foll. cataract
surgery with intraocular lens (IOL)implantation.
METHODS: 8 patients had uneventful phacoemulsification by the
same surgeon via clearcorneal incisions with implantation of the
same 3-piece silicone IOL design. Postopmedications included
antibiotic/steroid ointment and pilocarpine gel; each eye was
firmlypatched at the end of the procedure. On 1st POD, some
patients presented with diffusecorneal edema, increased IOP, and an
oily film-like material within the anterior chamber
coating the corneal endothelium. The others presented with an
oily bubble floating inside theanterior chamber, which was later
seen coating the IOL. Additional surgical proceduresrequired
included penetrating keratoplasty, IOL explantation, and
trabeculectomy. 2 cornealbuttons were analyzed histopathologically.
2 explanted IOLs had gross and light microscopicanalyses (as well
as surface analyses of 1 of them), and 4 other explanted IOLs had
gaschromatography-mass spectrometry.
-
8/9/2019 Toxic Anteror Segment Syndrome
22/40
RESULTS: Pathological examination of the corneas showed
variablethinning of the epithelium with edema. The stroma was
diffuselythickened and the endothelial cell layer was absent.
Evaluation of theexplanted IOLs confirmed the presence of an oily
substance coating largeareas of their anterior and posterior optic
surfaces. Gas chromatography-mass spectrometry of the lens extracts
identified a mixed chainhydrocarbon compound that was also found in
the gas chromatography-mass spectrometry analyses of the ointment
used postoperatively.
CONCLUSIONS: The results indicate that the ointment gained
access to theeye, causing the postoperative complications
described. These caseshighlight the importance of appropriate wound
construction and integrity,as well as the risks of tight eye
patching following placement of ointment.
-
8/9/2019 Toxic Anteror Segment Syndrome
23/40
Update on toxic anterior segment syndrome.
Current opinion in ophthalmology Volume: 18 ISSN: 1040-8738
ISO
Publication Date: 2007 Feb
PURPOSE OF REVIEW: To review, summarize and update our present
understanding of toxicanterior segment syndrome.
RECENT FINDINGS: Toxic anterior segment syndrome has emerged
within the last 2 years as acomplication of increasing frequency
following uneventful cataract surgery. Over 100 NorthAmerican
clinics reported toxic anterior segment syndrome cases to a
specially constitutedtask force over a 4-month period in 2006.
Toxic anterior segment syndrome is nowrecognized as a specific,
noninfectious condition presenting as anterior segmentinflammation
that occurs within days of surgery and is responsive to topical
steroids. Specificcauses have been identified such as endotoxin
contamination of balanced salt solutions andantibiotic ointment
accessing the anterior chamber, although most cases appear to
resultfrom inadequate instrument sterilization and preparation.
Outcomes are usually excellent,but delayed treatment and severe
cases may result in glaucoma and persisting cornealedema requiring
penetrating keratoplasty.
SUMMARY: Toxic anterior segment syndrome has become a
significant complication ofcataract surgery. Rapidly increasing
knowledge made possible by ophthalmic organizationsand the prompt
dissemination of research findings, however, appear to have
provided theinformation necessary to help prevent and resolve this
condition.
-
8/9/2019 Toxic Anteror Segment Syndrome
24/40
Toxic anterior segment syndrome after cataract
surgery--Maine, 2006.
MMWR (Morb MortalWkly Rep.) 2007 Jun 29;56(25):629-30.
Centers for Disease Control and Prevention (CDC).
Toxic anterior segment syndrome (TASS), an acute, noninfectious
inflammation of theanterior segment of the eye, is a complication
of anterior segment eye surgery; cataractextraction is the most
common form of this type of surgery. Various contaminants,
usually
from surgical equipment or supplies, have been implicated as
causes of TASS. The syndrometypically develops within 24 hours
after surgery and is characterized by corneal edema andaccumulation
of white cells in the anterior chamber of the eye. Although most
cases of TASScan be treated successfully with topical steroids,
topical nonsteroidal antiinflammatoryagents, or both, the
inflammatory response associated with TASS can cause serious
damageto intraocular tissues, resulting in vision loss. In October
2006, the Maine Department ofHealth and Human Services (MDHHS)
received a report of a cluster of TASS cases among
outpatients who had undergone cataract surgery at a hospital in
Maine. MDHHS and CDCinvestigated the cluster and worked with the
treating ophthalmologist and the hospital toprevent additional
cases. This report describes the results of that investigation and
thesubsequent prevention measures implemented. Although the
specific cause of the outbreakwas not identified, no additional
cases were reported after two series of changes were madeto the
materials and equipment used for surgery. Prevention of TASS
requires carefulattention to solutions, medications, and ophthalmic
devices and to cleaning and sterilization
of surgical equipment because of the numerous potential causes
of the condition.
-
8/9/2019 Toxic Anteror Segment Syndrome
25/40
Multistate outbreak of toxic anterior segment
syndrome, 2005.
J Cataract Refract Surg. 2008 Apr;34(4):585-90.
Kutty PK, Forster TS,Wood-Koob C, Thayer N, Nelson RB, Berke SJ,
Pontacolone L, Beardsley TL, EdelhauserHF, Arduino MJ, Mamalis N,
Srinivasan A.
PURPOSE: To present the findings of an outbreak of toxic
anterior segment syndrome (TASS).
SETTING: Six states, 7 ophthalmology surgical centers, United
States.
METHODS: Cases were identified through electronic communication
networks and via reports to anational TASS referral center.
Information on the procedure, details of instrument reprocessing,
andproducts used during cataract surgery were also collected.
Medications used during the procedures weretested for endotoxin
using a kinetic assay.
RESULTS: The search identified 112 case patients (median age 74
years) from 7 centers from July 19, 2005,through November 28, 2005.
Common presenting clinical features included blurred vision (60%),
anteriorsegment inflammation (49%), and cell deposition (56%). Of
the patients, 100 (89%) had been exposed to asingle brand of
balanced salt solution manufactured by Cytosol Laboratories and
distributed by AdvancedMedical Optics as AMO Endosol. Two patients
continued to have residual symptoms. There were no
reports of significant breaches in sterile technique or
instrument reprocessing. Of 14 balanced saltsolution lots, 5 (35%)
had levels exceeding the endotoxin limit (0.5 EU/mL). Based on
these findings, thebalanced salt solution product was withdrawn,
resulting in a termination of the outbreak.
CONCLUSIONS: This is the first known report of an outbreak of
TASS caused by intrinsic contamination of aproduct with endotoxin.
Ophthalmologists and epidemiologists should be aware of TASS and
its commoncauses. To facilitate investigations of adverse outcomes
such as TASS, those performing cataract surgeriesshould document
the type and lot numbers of products used intraoperatively.
-
8/9/2019 Toxic Anteror Segment Syndrome
26/40
Development of toxic anterior segment syndrome
immediately after uneventful phaco surgery.
Korean J Ophthalmol. 2008 Dec;22(4):220-7.
Choi JS, Shyn KH.
Department of Ophthalmology, Seoul National University College
of Medicine, Seoul, Korea.
PURPOSE:We report on 15 cases of suspected toxic anterior
segment syndrome after uneventful phacosurgery.
METHODS: We retrospectively reviewed the charts of patients who
had developed toxic anterior segmentsyndrome (TASS) after
uneventful phacoemulsification for senile cataracts between April
and December of2005. Clinical features and all possible causes were
investigated including irrigating solutions or drugs,surgical
instruments or intraocular lenses, sterilization techniques for
instruments, or any otheraccompanying disease.
RESULTS: The patients consisted of 2 males and 13 females with
an average age of 64.7+/-10.9 years. Fivedifferent surgeons had
performed their phaco surgeries. No abnormal preoperative or
operative findingswere reported. Nevertheless, all 15 patients
developed a moderate degree of corneal edema. Ordinarytreatments
were not helpful. We suspect that lack of sterilization resulted in
the development of the
syndrome, because after ethylene oxide gas sterilization was
replaced with autoclaving, no such incidentshave occurred.
CONCLUSIONS: Toxic anterior segment syndrome requires special
attention and thorough management,including sterilization of reused
surgical instruments.
-
8/9/2019 Toxic Anteror Segment Syndrome
27/40
Identification of unknown intraocular material after
cataract
surgery: evaluation of a potential cause of toxic anterior
segment syndrome.
J Cataract Refract Surg. 2008 Mar;34(3):465-9.
Mathys KC, Cohen KL, Bagnell CR.
Department of Ophthalmology, Microscopy Services Laboratory,
University of North Carolina at ChapelHill, School of Medicine,
University of North Carolina Hospitals, Chapel Hill, North Carolina
27599-7040,USA.
PURPOSE: To describe and identify unknown opaque material
between the optic of an AR40 intraocular
lens (IOL) injected with the Emerald Series implantation system
(both AMO, Inc.) and the posterior capsuleat the conclusion of
routine phacoemulsification to prevent an outbreak of toxic
anterior segmentsyndrome (TASS).
METHODS: After coaxial phacoemulsification in multiple patients,
opaque material was present betweenthe optic of a posterior chamber
IOL and the posterior capsule. Although there was no TASS, the
materialwas removed from 2 eyes and analyzed with scanning electron
microscopy (SEM) and x-ray microanalysis(XRM). Similarly,
crystalline lens, Klenzyme (Steris Corp.), Viscoat (sodium
hyaluronate 3.0%-chondroitinsulfate 4.0%), and Provisc (sodium
hyaluronate 1.0%) were analyzed.
RESULTS: On SEM, the material had an irregular undulating
surface similar to that of Provisc. Viscoat andthe crystalline lens
had smoother surfaces. On XRM, the material contained sodium,
chlorine, and calcium,like Viscoat and Provisc, and phosphorous and
sulfur, like Viscoat. The material also contained
silicone,magnesium, aluminum, titanium, iron, and zinc. Klenzyme
had smaller peaks of sodium, chlorine, andcalcium and a higher
carbon background than the unknown material.
CONCLUSIONS: The material was likely ophthalmic viscosurgical
device that was chemically andstructurally altered by the cleaning
and sterilization process. The silicone and metallic elements
wereprobably from the Emerald Series implantation system as the
disposable cartridge is coated with silicone
and the reusable injector is metal.
-
8/9/2019 Toxic Anteror Segment Syndrome
28/40
Toxic Anterior Segment Syndrome (TASS): studying an
outbreak
Farm Hosp. 2008 Nov-Dec;32(6):339-43. Sarobe Carricas M,
Segrelles Bellmunt G, Jimnez Lasanta L, Iruin Sanz A. Servicio de
Farmacia, Hospital de Navarra, Pamplona, Espaa.
[email protected] INTRODUCTION: An effect associated with
cataract surgery known as Toxic Anterior Segment
Syndrome (TASS) has been reported in recent years. It is an
inflammatory non-infectious processwhich appears within the first
few hours after surgery and generally resolves well with
topical
steroids if the course of treatment is started promptly. In this
paper we describe the syndrome and analyze the possible causes for
the TASS outbreak that
occurred in our hospital and affected 5 patients. METHODS: As
the syndrome may be due to multiple causes, the members of a
research team
created at the hospital reviewed all the procedures involved.
The washing and sterilization methodsapplied to the materials were
analyzed, as well as the drugs and substances used which might
havecaused the outbreak.We verified the substances prepared by the
Pharmacy Department, speciallythe irrigating solution which was
used in all the cases.
RESULTS: According to the results obtained in the biochemical,
micro-biological, pH, osmolarity and
endotoxins assays, the solutions prepared by the Pharmacy
Department were all correct. DISCUSSION: Since the results obtained
in the analyses of the substances used were correct and no
adverse effect was observed after the re-administration of the
substances, we may conclude thatthe outbreak would be related to
the washing process performed previously to the sterilization ofthe
instrumentation used in the surgery, mainly because the
recommendation to use distilled andsterile water for this purpose
was not followed and, on the contrary, tap water continued to
beused.
-
8/9/2019 Toxic Anteror Segment Syndrome
29/40
Toxic Anterior Segment Syndrome Following
Penetrating Keratoplasty
Philip Maier, MD; Florian Birnbaum, MD; Daniel Bhringer, MD;
Thomas Reinhard, MD .
Arch Ophthalmol. 2008;126(12):1677-1681.
Objectives To describe an outbreak of toxic anterior segment
syndrome (TASS) followingpenetrating keratoplasty (PK) and to
examine its possible causes.
Methods Owing to a series of TASS following PK between June 6,
2007, and October 2, 2007,
we reviewed the records of all patients who had undergone PK
during that time. Inadditionto routine microbial tests on organ
culture media, we looked for specific pathogensand endotoxins in
all of the materials used for organ culture or PK. Furthermore, we
analyzedall of the perioperative products and instrument
processing.
Results Of the 94 patients who underwent PK, we observed 24
cases of postoperative sterilekeratitis. Causal research revealed
that the accumulation of cleaning substances or
heat-stableendotoxins on the surface of the routinely used guided
trephine system was most likely
responsible for the TASS. Conclusions To our knowledge, this is
the first report on TASS following PK. Suboptimal
reprocessing of surgical instrumentsmay be an important cause of
TASS as in this series theTASS-likesymptoms resolved after modified
instrument-cleaning procedures. Thestandardization of protocols for
processing reusable trephine systems might preventoutbreaks of TASS
following PK.
-
8/9/2019 Toxic Anteror Segment Syndrome
30/40
-
8/9/2019 Toxic Anteror Segment Syndrome
31/40
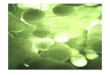
Retrospective analysis of clinical characteristics
of toxic anterior segment syndrome
Zhonghua Yan Ke Za Zhi. 2009 Mar;45(3):225-8. Yang SL, Yan XM.
Department of Ophthalmology, Peking University First Hospital,
Beijing 100034, China. OBJECTIVE: To investigate the etiology,
clinical features, treatment and prognosis of toxic anterior
segment
syndrome (TASS). METHODS: It was a retrospective series case
study. The clinical data of eight definite diagnosed TASS cases
were retrospectively analyzed. RESULTS: Among eight TASS cases,
seven were post cataract surgery cases and one was post
corneapenetrating injury. Three cases were caused by residual
povidone iodine on instruments, 2 cases resultedfrom the misuse of
distilled water as intraocular irrigating liquid during cataract
surgery, 2 cases wereproduced by the countercurrent of antibiotic
solution via the cornea-scleral incision into anterior
chamberduring subconjunctival injection at the end of the surgery,
and 1 case was induced by the injection of thedistilled water into
the anterior chamber at the end of the surgery. Three TASS cases
occurred duringoperation and 5 cases occurred at 1 day after
operation. All eight cases suffered from the painless
blurredvision. Three cases occurred during operation presented with
decrease of corneal transparence anddepigmentation of iris. On the
first day after operation, all cases had diffuse corneal stroma
edema and
severe anterior uveitis. Dexamethasone 0.1% or prednisolone
acetate 1% eye drops, three times per dayor one time per hour was
used in all cases. Carteolol 2% eye drop, two times per day, was
used for thecases with ocular hypertension. The cornea was clear in
6 cases, but corneal endothelial decompensationin 2 cases after
therapy.
CONCLUSION: Various toxic agents injected into anterior chamber
by misuse can result in TASS. All thesemisuse can be avoided. Early
diagnosis and proper management may be important to improve
theprognosis of TASS.
-
8/9/2019 Toxic Anteror Segment Syndrome
32/40
-
8/9/2019 Toxic Anteror Segment Syndrome
33/40
Toxic Anterior Segment Syndrome - A Reality
First Independent Ophthalmic Journal Published from Islamabad,
Pakistan; Vol. 7,No. 4 Oct-Dec-2009
Dr. Mahfooz Hussain Director & Senior Consultant
Ophthalmologist,Dr. Tariq Farooq Babar, AssociateProfessor &
Visiting Eye Surgeon,Dr. Mir Zaman, Senior Registrar,Dr. Mohammad
Younas Khan, ConsultantOphthalmologist,Dr. Anwar Iqbal & Dr.
Naz Jehangir Postgraduate Trainees Pakistan Institute ofCommunity
Ophthalmology, Khyber Institute of Medical Sciences, Hayatabad
Medical Complex,Peshawar,Dr. Patricia D. Wade, Consultant
Ophthalmology JOS University Teaching Hospital, Nigeria.
PURPOSE: The purpose is to report two outbreaks of toxic
anterior segment syndrome (TASS) and toemphasize importance of its
early diagnosis, appropriative treatment and prevention which is
all the moreimportant.
PATIETS and MATERIALS: We had two outbreaks of TASS at two
different occasions in 2007-08 afterroutine cataract extraction
with posterior chamber implant. We retrieved clinical records of
all patientsand collected information on a specially designed
performa. Details of postoperative signs and symptomsand treatment
were recorded. All the patients were followed up for at least 3
months. We also looked atmethods of instrument cleaning and
sterilization in detail.
RESULTS:We diagnosed 11 patients with TASS at two different
occasions as two clusters. All the patients
were correctly diagnosed and no patient turned out to be
infective, which is usually the main concern. Allthe patients were
successfully treated. Final visual acuity was 6/6 in 7 patients,
6/9 in 3 patients and 6/18in one patient. Increased IOP in 4
patients returned to normal at 3 months.
CONCLUSIONS: It is important to differentiate TASS patients from
infective endophthalmitis. Timing ofonset and sparing of posterior
segment are important factors for diagnosis along with other
clinicalfeatures. Early and intensive treatment with topical
steroids, cycloplegics and oral anti-inflammatory drugscan resolve
the condition and visual acuity can improve to preoperatively
expected levels.
-
8/9/2019 Toxic Anteror Segment Syndrome
34/40
PREVENTION
-
8/9/2019 Toxic Anteror Segment Syndrome
35/40
Task Force
When reports of toxic anterior segment syndrome (TASS) inNorth
America suddenly began to escalate to five times their normal level
early in 2006, theAmerican Society of Cataract and Refractive
Surgery (ASCRS)provided support for a task
force convened to investigate the reasons why and develop
recommendations for reducingits incidence.
Analysis of the data the task force assembled failed to reveal
any single cause of the outbreakand, instead, suggested that a
number of etiologic factors could have been involved.
The analysis also provided support for the belief that the
cleaning and sterilization of theinstruments used in cataract
surgery appears to be a critical factor in reducing the risk
ofTASS.
The team came up with this Special ASCRS/ASORN Report:
Recommended Practices forCleaning and Sterilizing Intraocular
Surgical Instruments.
Guidelines : Establish written protocols for instrument cleaning
and reprocessing, certifycompetency of responsible personnel, and
monitor compliance
Use only medications and solutions that are free of
preservatives, bisulfites, or metasulfites.
-
8/9/2019 Toxic Anteror Segment Syndrome
36/40
Treatment :
Medical Care
Once TASS is confirmed,
patients should be startedon topical steroids.
Careful assessment andtreatment of elevated IOP.
Nonsteroidal anti-inflammatory drops.
Close follow-up.
RULE OUT ENDOPHTHALMITIS
-
8/9/2019 Toxic Anteror Segment Syndrome
37/40
Treatment :
Surgical Care
Intraocular lens exchange.
Corneal transplantation. Trabeculectomy (seton valve
procedures).
-
8/9/2019 Toxic Anteror Segment Syndrome
38/40
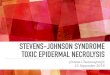
TASS TIMELINE
1980 1992 2000 2002 2005 2006 2006 2006
Sporadicreports ofsevere
anteriorsegmentinflammationfollowingcataract
surgery
ConditiontermedToxic
AnteriorSegmentSyndrome(TASS)Monsonet al. JCRS
1992
Delayed-onsetTASS
associated withMemoryLens
softenedcity waterthat
suppliedthe auto-clavesteamgenerator(sulphate
impurity)
OctoberIncreasingreports of
sterileInflammation linkedtoBSS(Endosol)
TASS atCommunity
Hospitalin Maine
Numerous eyecenters
in NorthAmericareportedanincreaseincidence
of TASSfollowingOutpatient cataractsurgery
ASCRScreated aTASS Task
Force toinvestigateoutbreaksof TASSand
identifycausativeagents
-
8/9/2019 Toxic Anteror Segment Syndrome
39/40
Just because something is sterile,
it does not mean its not toxic!
-
8/9/2019 Toxic Anteror Segment Syndrome
40/40
THANK YOU!