Embed Size (px)
Citation preview
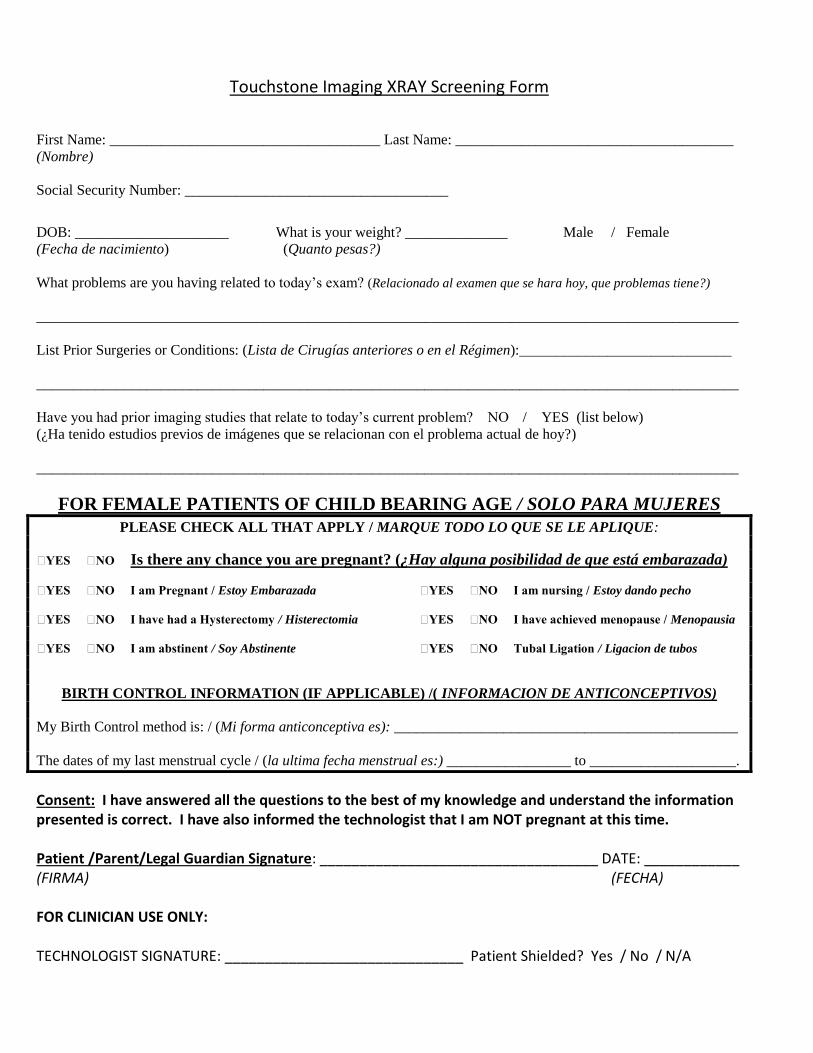
Touchstone Imaging XRAY Screening Form
First Name: _____________________________________ Last Name: ______________________________________
(Nombre)
Social Security Number: ____________________________________
DOB: _____________________ What is your weight? ______________ Male / Female
(Fecha de nacimiento) (Quanto pesas?)
What problems are you having related to today’s exam? (Relacionado al examen que se hara hoy, que problemas tiene?)
________________________________________________________________________________________________
List Prior Surgeries or Conditions: (Lista de Cirugías anteriores o en el Régimen):_____________________________
________________________________________________________________________________________________
Have you had prior imaging studies that relate to today’s current problem? NO / YES (list below)
(¿Ha tenido estudios previos de imágenes que se relacionan con el problema actual de hoy?)
________________________________________________________________________________________________
FOR FEMALE PATIENTS OF CHILD BEARING AGE / SOLO PARA MUJERES
PLEASE CHECK ALL THAT APPLY / MARQUE TODO LO QUE SE LE APLIQUE:
YES NO Is there any chance you are pregnant? (¿Hay alguna posibilidad de que está embarazada)
YES NO I am Pregnant / Estoy Embarazada YES NO I am nursing / Estoy dando pecho
YES NO I have had a Hysterectomy / Histerectomia YES NO I have achieved menopause / Menopausia
YES NO I am abstinent / Soy Abstinente YES NO Tubal Ligation / Ligacion de tubos
BIRTH CONTROL INFORMATION (IF APPLICABLE) /( INFORMACION DE ANTICONCEPTIVOS)
My Birth Control method is: / (Mi forma anticonceptiva es): _______________________________________________
The dates of my last menstrual cycle / (la ultima fecha menstrual es:) _________________ to ____________________.
Consent: I have answered all the questions to the best of my knowledge and understand the information presented is correct. I have also informed the technologist that I am NOT pregnant at this time. Patient /Parent/Legal Guardian Signature: ___________________________________ DATE: ____________ (FIRMA) (FECHA) FOR CLINICIAN USE ONLY: TECHNOLOGIST SIGNATURE: ______________________________ Patient Shielded? Yes / No / N/A