Embed Size (px)
Citation preview

Centro Oncologico
Tossicità epatica da farmaci antiblastici
Roma, 3 dicembre 2010
Michele BassoOncologia Medica

Liver toxicity in patients with HBV resolved infection(anti HBc+)
Liver damage and risk of liver failure in patientsreceiving neo-adjuvant chemotherapy for colorectal cancer liver metastases

Patients with cancer and chronic HBV infection have an high risk of viral reactivation on
chemotherapy, with two different outcomes:
Acute hepatitis:the spectrum of HBV reactivation ranges
from asymptomatic hepatitis to fatal liver failure.
Disruption in treatment protocols:may worsen the prognosis of cancer
because of delays or withdrawals of chemotherapeutic agents

BackgroundHBV in cancer patients
HBsAg+ Anti-HBc+
Europe China Europe China
Range 5.3-12.230-40%
40% 80%Taiwan
Italy 8.8%° 41.7%°
HBV reactivation 15-40% (Onc) 21-67% (Em) 12-50% (HSCT)
Mortality 20%
Linfomain portatori
0R 2.6 (Cina)-2.8 (USA) in B-NHL
Wang F et al, Cancer 2007; Ulcickas YM et al, Hepatology 2007
• °Marcucci et al ,Haematologica 2006
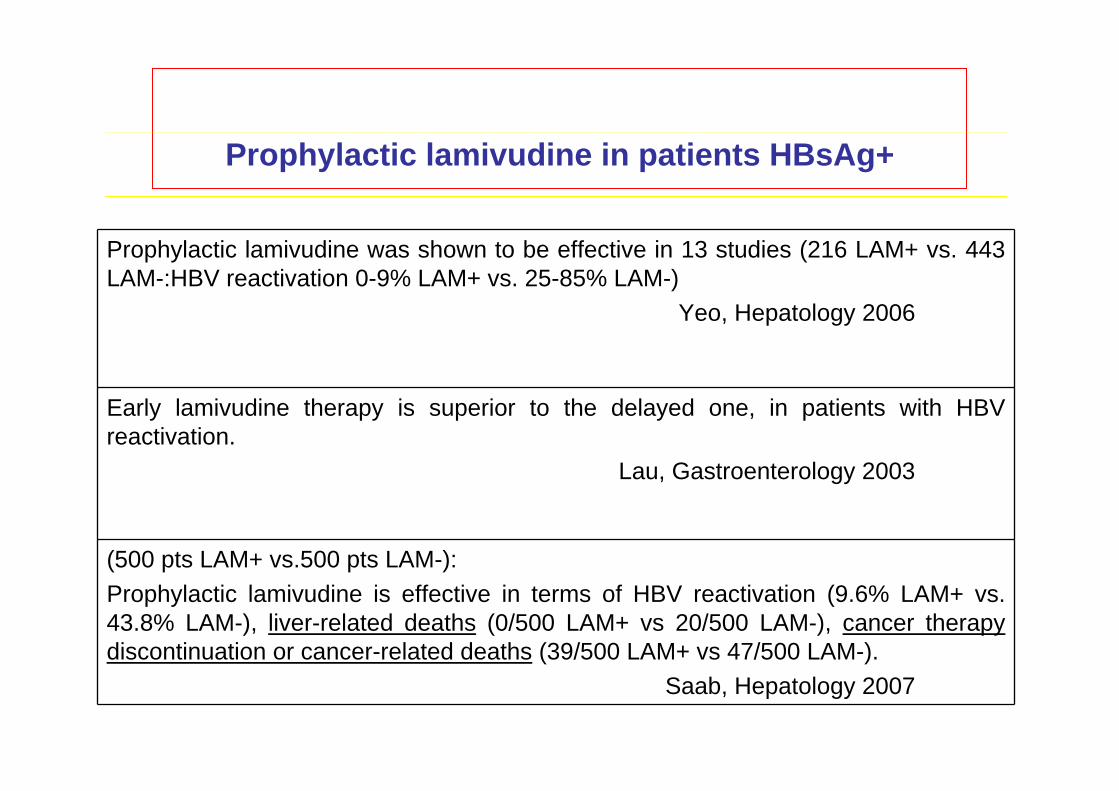
Prophylactic lamivudine in patients HBsAg+
Prophylactic lamivudine was shown to be effective in 13 studies (216 LAM+ vs. 443 LAM-:HBV reactivation 0-9% LAM+ vs. 25-85% LAM-)
Yeo, Hepatology 2006
Early lamivudine therapy is superior to the delayed one, in patients with HBV reactivation.
Lau, Gastroenterology 2003
(500 pts LAM+ vs.500 pts LAM-): Prophylactic lamivudine is effective in terms of HBV reactivation (9.6% LAM+ vs. 43.8% LAM-), liver-related deaths (0/500 LAM+ vs 20/500 LAM-), cancer therapy discontinuation or cancer-related deaths (39/500 LAM+ vs 47/500 LAM-).
Saab, Hepatology 2007

176 pts HBsAg-/anti-HBc+ :
seroreversion in 21 (12%)
Acute Hepatitis B:
4-30% during chemotherapy
14-50% during or after HSCT
Yeo W, Hepatology 2006
BackgroundRisk of HBV reactivation in patients with
HBsAg-/anti-HBc+ (anti-core)


Chemotherapeutic Agents That Have Been Associated with Development of HBV Reaction
Yeo & Johnson, Hepatology 2006; 43:209

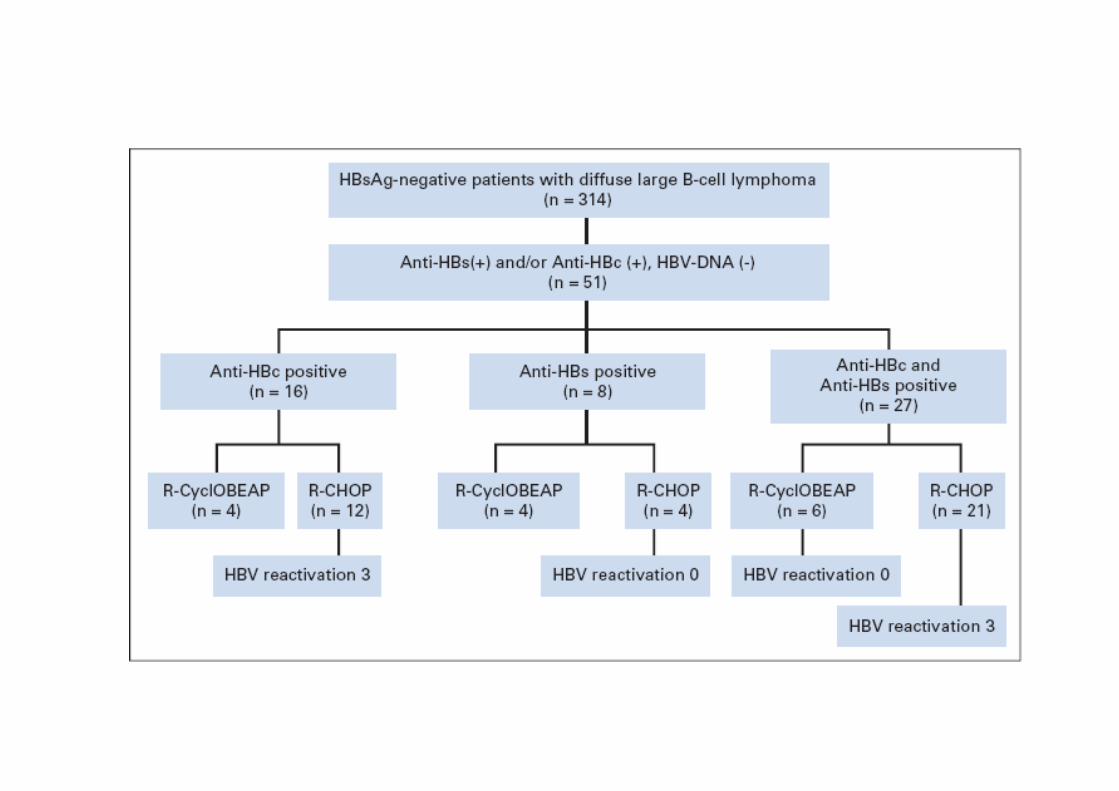
Jan 2003-Dec 2006
All patients diagnosedwith DLBCL were testedfor anti HBc (anti HBS -)






Metastatic CRC
The Shift of the Paradigm
FromPalliation
ToCureto
The Aim is
TO CURE

Overall survival in advanced CRCin 2007: were might we be in 2017?
0 1 2 3 4
100
50
0
% s
urvi
ving
Years after diagnosis of colorectal metastases
2007 chemotherapy aloneMedian survival >24 months5-yr survival 9%
2007 overall with addition of surgeryMedian survival ~36 months5 year survival 20 %
20%
Poston GJ. EJSO 2005; 31: 325-30
9%1927 1997
3%
2007
?50%2017

Karoui, Nordlinger et al. Annals Surgery 2006
Postoperative morbidity was correlated with no. cyclesbut not with the type of chemotherapy
Extended chemotherapy
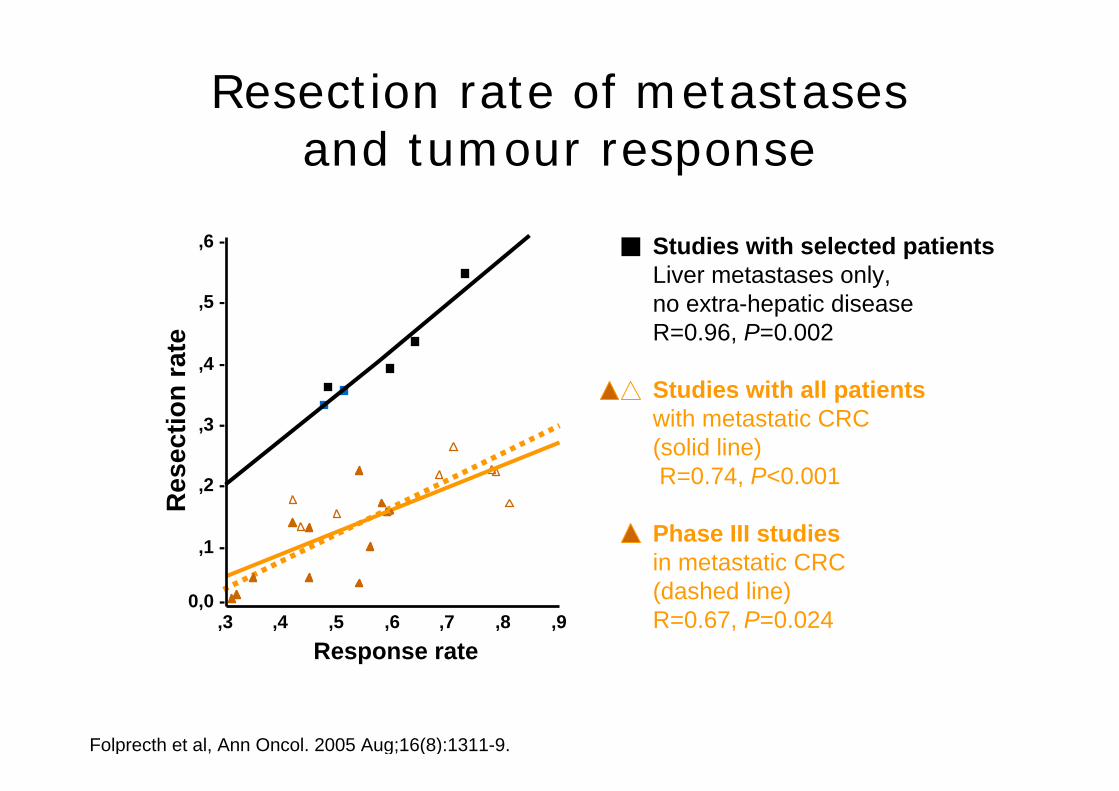
Resection rate of metastasesand tumour response
Studies with all patientswith metastatic CRC (solid line) R=0.74, P<0.001
Phase III studiesin metastatic CRC(dashed line)R=0.67, P=0.024
Studies with selected patientsLiver metastases only, no extra-hepatic diseaseR=0.96, P=0.002
Folprecth et al, Ann Oncol. 2005 Aug;16(8):1311-9.
Response rate,9,8,7,6,5,4,3
Res
ectio
n ra
te
,6 -
,5 -
,4 -
,3 -
,2 -
,1 -
0,0 -

Extended chemotherapy
Kishi et al; Ann Surg Oncol 2010

Resectable liver mtsCT vs Surg alone
CT + S (n=45) S alone (n=22) pSinusoidal dilation 22 (49%) 3 (14%) 0.05Steatosis
<20%20-50%>50%
25 (56%)6 (13%)9 (20%)
10 (22%)
14 (64%)6 (27%)5 (23%)3 (14%)
NS
FibrosisF0-F1F2
25 (56%)19 (42%)
15 (68%)7 (32%)
NS
Karoui, Nordlinger et al. Annals Surgery 2006
Postoperative morbidity was correlated with no. cyclesbut not with the type of chemotherapy
Appropriateness of medical treatments
BenefitsRisks
Primary ChemotherapyNeoadjuvant Chemoterapy
Adjuvant Chemotherapy
Appropriateness of medicaltreatments
DownsizingResectability
Survival
Pathologic damageSurgical risk
Late complications
Primary ChemotherapyNeoadjuvant Chemoterapy
Adjuvant Chemotherapy
A difficult balance

Risk Assessment Liver after CT
« congestive liver? » « blue liver? » « chemo’s liver? » « steatosis? » « cirrhosis? »
normal liver
Liver after chemotherapy

Risk assessment: Pathology
Vauthey et al. JCO 2006
Steatohepatitis (Irinotecan)
Sinusoidal distention and obstruction
(oxaliplatin)

Normal liver Liver after chemotherapy
Centrilobular vein
sinusoïds
Centrilobular vein
Centrilobularvein
sinusoïds
Similar to VOD, more appropriately named “Sinusoïdal Obstruction Syndrome (SOS)”
(De Leve et al. 2002)
Rubbia-Brandt L. et al Ann Oncol 2004

The integrity of the sinusoidal wall is interrupted
Liver after chemotherapyNormal liver

Type of Chemotherapy
No. Patients
Pathologic liver histology
n (%) No chemotherapy 66 0 (0)With chemotherapy 87 44 (51)5-FU 27 6 (22)5-FU / Irinotecan 17 4 (23)5-FU / Oxaliplatin 27 20 (74)5-FU / Oxali + Irinotecan 16 14 (88)
Rubbia-Brandt, Ann Oncol 2004
Risk assessment CT prior to resection
• 44/87 pts (51%) who received CT exhibited centrolobular lesions

Incidence of steatohepatitis with modern CT regimens
Treatment N Evidence of fatty changes
5-FU/FA 25 6 (24%)
Iri/5-FU/FA 25 12 (48%)Oxali/5-FU/FA 25 7 (28%)
Leonard et al ASCO 2005

Type of Chemotherapy
No.pts
Sinusoidaldilation
n=22
Steatosis>30%n=36
Steatohepatitis
n=34
No CT 158 3 (2%) 9% 4%5-FU 63 0 17% 5%
5-FU / IRI 94 4 (4%) 11% 20%
5-FU / Oxa 79 15 (19%) 4% 6%
90-day mortality 1% 1% 15%
Vauthey et al. JCO 2006
Hepatoxicity of preoperative CT

Relation between type of liver damage and clinical outcome
• Steatosis associated with higher infection rate (Kooby et al. 2003)
• Steatohepatitis associated with higher mortality rate due to liver failure after surgery (Vauthey et al.,2006)
• Vascular injury associated with higher rate of operative bleeding and transfusion requirement (Vauthey et al. 2006; Adam et al. 2005)
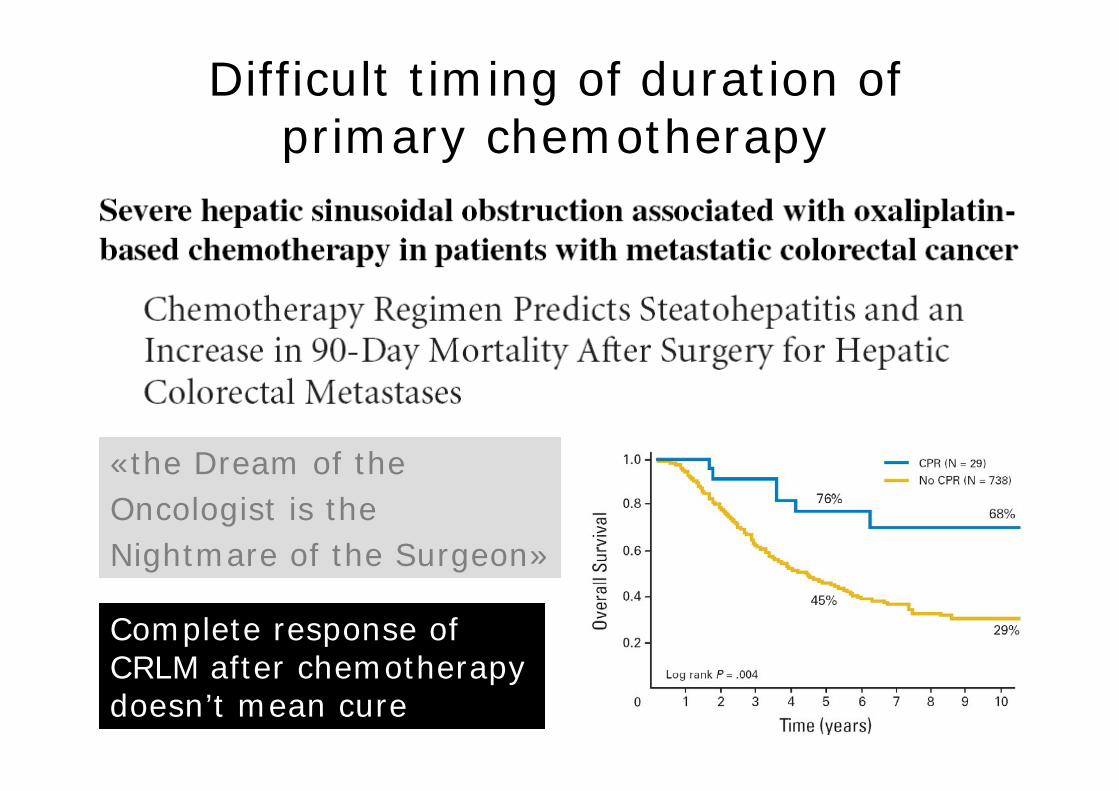
Difficult timing of duration of primary chemotherapy
«the Dream of the Oncologist is theNightmare of the Surgeon»
Complete response ofCRLM after chemotherapy doesn’t mean cure

CONCLUSION
Neadjuvant chemotherapy can increase the possibility of cure for patients withliver metastases of colorectal cancer
Response rate is strictly related with resection rate
Extended chemotherapy does not increase response but increase the risk ofmorbidity and mortality after surgery (risk of liver failure).
A multidisciplinary approach (oncologist, surgeon, pathologist) is warranted















![28 Novembre Aviano.ppt [modalità compatibilità] 28/07 Dott. Abu Rumeileh.pdf · di tossicità tardiva del retto, sono emersi infatti i seguenti vincoli dose-volume: dose massima](https://img.pdfslide.us/doc/110x75/5c69169609d3f2e4258c5f12/28-novembre-modalita-compatibilita-2807-dott-abu-rumeilehpdf-di-tossicita.jpg)












