Embed Size (px)
Citation preview
TOPICS OF INTEREST
Maximizing Mandibular Prosthesis StabilityUtilizing Linear Occlusion, Occlusal PlaneSelection, and Centric RecordingRichard A. Williamson) DDS) MS/ Anne E. Williamson) DDS/John Bowley) DDS) MS/ and Randy Toothaker) DDS4
The stability of mandibular complete dentures may be improved by reducing the transverse forceson the denture base through linear (noninterceptive) occlusion, selecting an occlusal plane thatreduces horizontal vectors of force at occlusal contact, and utilizing a central bearing intraoral gothicarch tracing to record jaw relations. This article is intended to acquaint the reader with one techniquefor providing stable complete denture prostheses using the aforementioned materials, devices, andprocedures.
] Prosthodont 2004; 13:55-61. Copyright © 2004 by The American College of Prosthodontists.
OBTAINING CONSISTENT mandibulardenture stability has long been a challenge
for dental professionals. The dynamic contactof teeth has an effect on the stability of denturebases, the forces transmitted to denture bearingtissues, and the comfort and function experiencedby patients.l Literature has supported the use oflinear (also known as lineal) occlusion to enhancethe stability of complete denture prostheses.2,3~oninterceptive occlusion (linear occlusion) re-quires that there should be no interference orinterception with mandibular movement in pro-trusive or lateral excursions.
It has been reported that linear occlusion mini-mizes horizontal force vectors that act to dislodge
1Assistant Prqftssor, The University if Iowa College if Dentistry,Iowa City, IA.
2Clinical Faculty, Department q/Endodontics, University q/ IowaCollege if Dentistry, Iowa City, IA.
3Post-Doctoral Prosthodontics, Boston University School q/DentalMedicine.
4AssociatePrqftssorandDirector, Graduate Prosthodontics, UNMG.Accepted May 5, 2003Presented as a table clinic in the 1999 American College if
Prosthodontists annual meeting, New York, NY.Correspondence to: Dr. Richard Williamson, University q/ Iowa
College q/ Dentistry, Department q/ Prosthodontics, 424 Dental Sci-ence South, Iowa City, Iowa 52242. E-mail: [email protected]
Copyright © 2004 by The American Collegeq/Prosthodontists1059-941X/04doi: 10.1111/j.1532-849X2004.04001.x
prostheses.2,3 It has been the experience of theauthors that the use of linear occlusion, in con-junction with a steeper than conventional occlusalplane, assists in stabilizing mandibular denturebases. This is particularly helpful for patientsexhibiting advanced mandibular residual ridgeresorption. The additional use of intraoral centralbearing gothic arch-tracing devices aids in pro-ducing repeatable centric relation measurementscontributing to more stable mandibular denturebases.
Concept of Linear OcclusionThe Glossary of Prosthodontic Terms Qanuary1999, 7th edition) credits William H. Goddard, ofLouisville, Kentucky with the founding of linearocclusion. In 1966J.P. Frush described occlusion ingeometric terms as one-dimensional (linear), two-dimensional (flat plane), and three-dimensional(cusped). This geometric classification of occlu-sion specifically classified the dimensional contactbetween occluding posterior teeth. Linear occlu-sion was promoted as an occlusal scheme that ledto increased stability of denture bases by minimiz-ing the lateral forces applied to those bases.2
Gronas and Stout explained how both anatomicand nonanatomic occlusal schemes transmit sig-nificant lateral forces to the denture bases, andthey suggested that linear occlusion had thepotential for creating the smallest lateral force
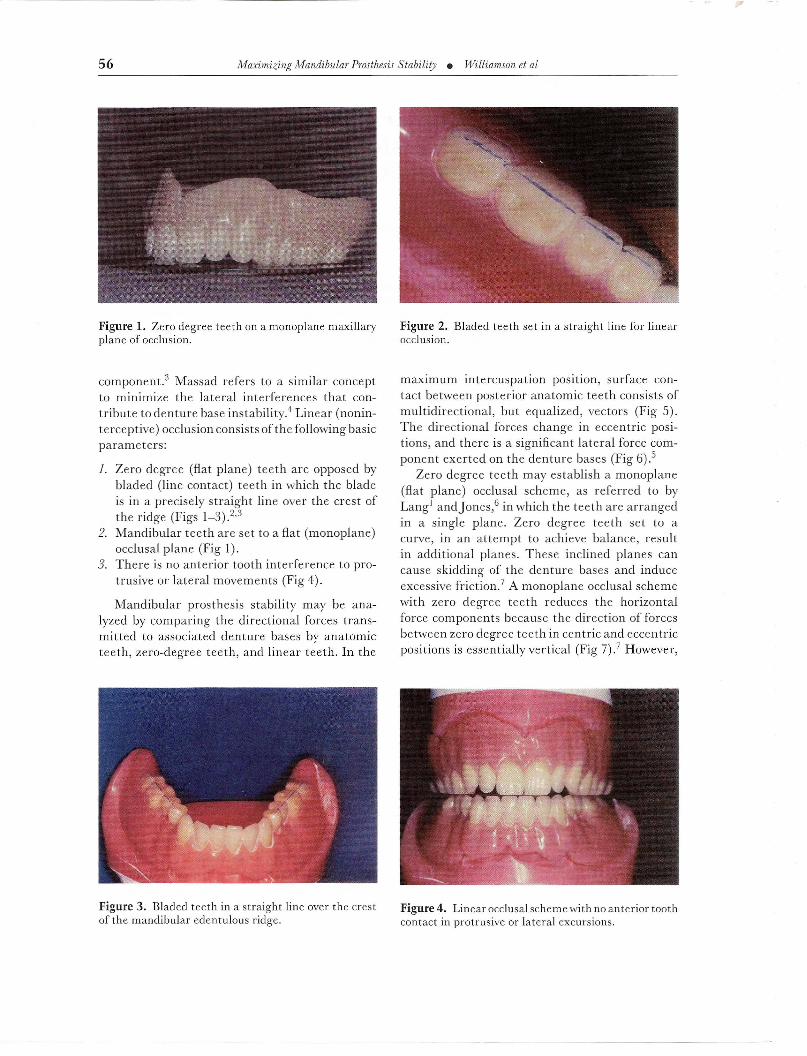
Figure 1. Zero degree teeth on a monoplane maxillaryplane of occlusion.
component.3 Massad refers to a similar conceptto minimize the lateral interferences that con-tribute to denture base instability.4 Linear (nonin-terceptive) occlusion consists of the following basicparameters:
1. Zero degree (flat plane) teeth are opposed bybladed (line contact) teeth in which the bladeis in a precisely straight line over the crest ofthe ridge (Figs 1_3).2,3
2. Mandibular teeth are set to a flat (monoplane)occlusal plane (Fig I).
3. There is no anterior tooth interference to pro-trusive or lateral movements (Fig 4).
Mandibular prosthesis stability may be ana-lyzed by comparing the directional forces trans-mitted to associated denture bases by anatomicteeth, zero-degree teeth, and linear teeth. In the
Figure 3. Bladed teeth in a straight line over the crestof the mandibular edentulous ridge.
Figure 2. Bladed teeth set in a straight line for linearocclusion.
maXImum intercuspation posItIOn, surface con-tact between posterior anatomic teeth consists ofmultidirectional, but equalized, vectors (Fig 5).The directional forces change in eccentric posi-tions, and there is a significant lateral force com-ponent exerted on the denture bases (Fig 6).5
Zero degree teeth may establish a monoplane(flat plane) occlusal scheme, as referred to byLang! andJones,6 in which the teeth are arrangedin a single plane. Zero degree teeth set to acurve, in an attempt to achieve balance, resultin additional planes. These inclined planes cancause skidding of the denture bases and induceexcessive friction.7 A monoplane occlusal schemewith zero degree teeth reduces the horizontalforce components because the direction of forcesbetween zero degree teeth in centric and eccentricpositions is essentially vertical (Fig 7).7 However,
Figure 4. Linear occlusalschemewith noanterior toothcontact in protrusive or lateral excursions.
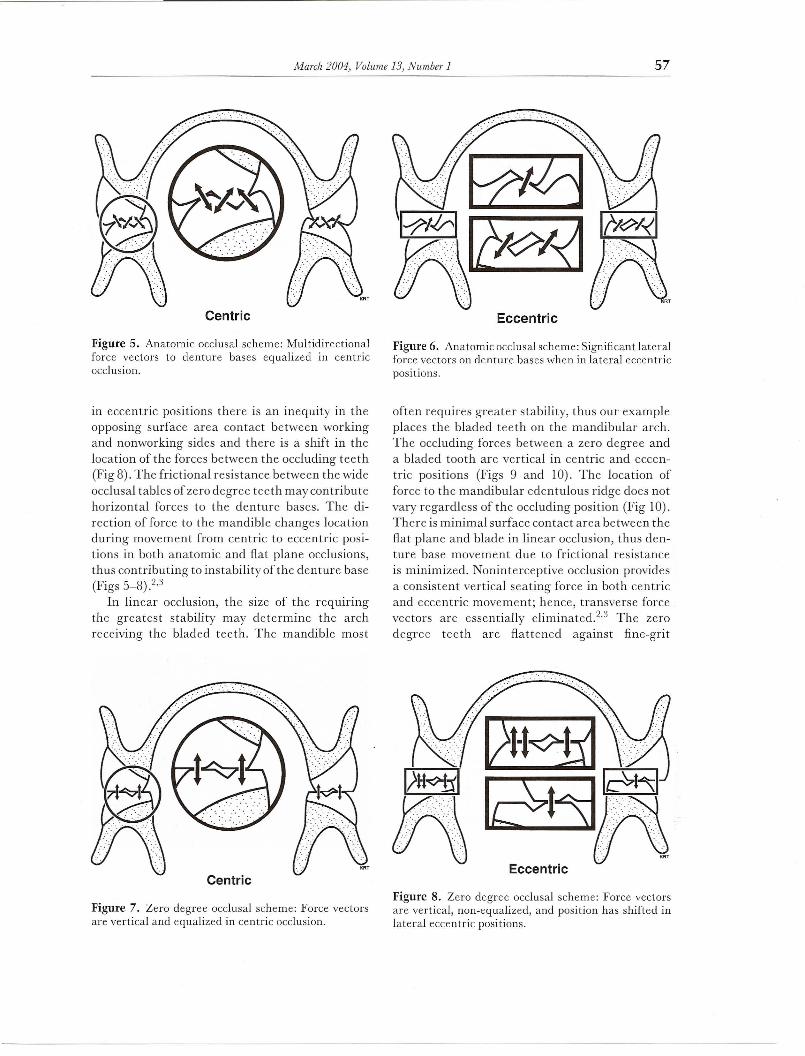
Figure 5. Anatomic occlusal scheme: Multidirectionalforce vectors to denture bases equalized in centricocclusion.
in eccentric positions there is an inequity in theopposing surface area contact between workingand nonworking sides and there is a shift in thelocation of the forces between the occluding teeth(Fig 8). The frictional resistance between the wideocclusal tables of zero degree teeth may contributehorizontal forces to the denture bases. The di-rection of force to the mandible changes locationduring movement from centric to eccentric posi-tions in both anatomic and flat plane occlusions,thus contributing to instability of the denture base(Figs 5_8).2,3
In linear occlusion, the size of the requiringthe greatest stability may determine the archreceiving the bladed teeth. The mandible most
Figure 7. Zero degree occlusal scheme: Force vectorsare vertical and equalized in centric occlusion.
tilE~LY~/~R
", . ". .. RT
Figure 6. Anatomic occlusalscheme: Significant lateralforce vectors on denture bases when in lateral eccentricpositions.
often requires greater stability, thus our exampleplaces the bladed teeth on the mandibular arch.The occluding forces between a zero degree anda bladed tooth are vertical in centric and eccen-tric positions (Figs 9 and 10). The location offorce to the mandibular edentulous ridge does notvary regardless of the occluding position (Fig 10).There is minimal surface contact area between theflat plane and blade in linear occlusion, thus den-ture base movement due to frictional resistanceis minimized. Noninterceptive occlusion providesa consistent vertical seating force in both centricand eccentric movement; hence, transverse forcevectors are essentially eliminated.2.3 The zerodegree teeth are flattened against fine-grit
Figure 8. Zero degree occlusal scheme: Force vectorsare vertical, non-equalized, and position has shifted inlateral eccentric positions.
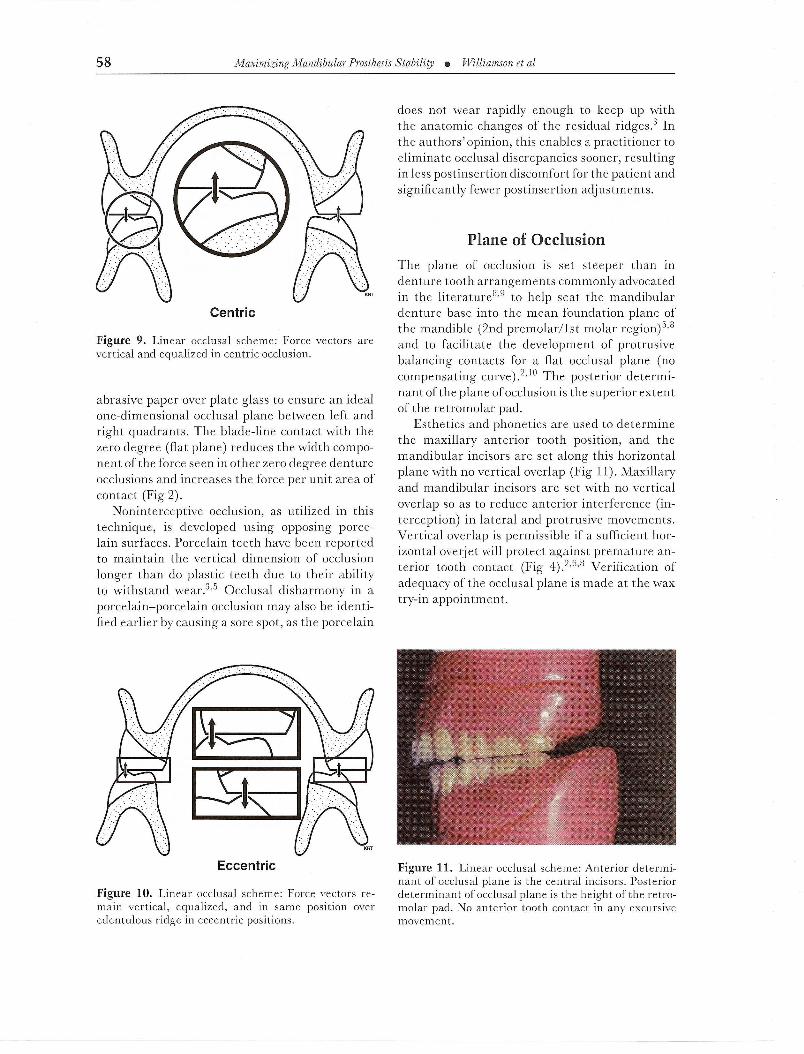
Figure 9. Linear occlusal scheme: Force vectors arevertical and equalized in centric occlusion.
abrasive paper over plate glass to ensure an idealone-dimensional occlusal plane between left andright quadrants. The blade-line contact with thezero degree (flat plane) reduces the width compo-nent of the force seen in other zero degree dentureocclusions and increases the force per unit area ofcontact (Fig 2).
Noninterceptive occlusion, as utilized in thistechnique, is developed using opposing porce-lain surfaces. Porcelain teeth have been reportedto maintain the vertical dimension of occlusionlonger than do plastic teeth due to their abilityto withstand wear.3,5 Occlusal disharmony in aporcelain-porcelain occlusion may also be identi-fied earlier by causing a sore spot, as the porcelain
Figure 10. Linear occlusal scheme: Force vectors re-main vertical, equalized, and in same position overedentulous ridge in eccentric positions.
does not wear rapidly enough to keep up withthe anatomic changes of the residual ridges.3 Inthe authors' opinion, this enables a practitioner toeliminate occlusal discrepancies sooner, resultingin less postinsertion discomfort for the patient andsignificantly fewer postinsertion adjustments.
The plane of occlusion is set steeper than indenture tooth arrangements commonly advocatedin the literature8,9 to help seat the mandibulardenture base into the mean foundation plane ofthe mandible (2nd premolar/1st molar region)5,8and to facilitate the development of protrusivebalancing contacts for a flat occlusal plane (nocompensating curve) .2,]0 The posterior determi-nant of the plane of occlusion is the superior extentof the retromolar pad.
Esthetics and phonetics are used to determinethe maxillary anterior tooth position, and themandibular incisors are set along this horizontalplane with no vertical overlap (Fig 11). Maxillaryand mandibular incisors are set with no verticaloverlap so as to reduce anterior interference (in-terception) in lateral and protrusive movements.Vertical overlap is permissible if a sufficient hor-izontal overjet will protect against premature an-terior tooth contact (Fig 4).2,6,8 Verification ofadequacy of the occlusal plane is made at the waxtry-in appointment.
Figure 11. Linear occlusal scheme: Anterior determi-nant of occlusal plane is the central incisors. Posteriordeterminant of occlusal plane is the height of the retro-molar pad. No anterior tooth contact in any excursivemovement.
Figure 12. Intraoral central-bearing gothic arch-tracing device.
For extremely resorbed ridges, a consistent, re-peatable, and easily verified centric relationrecording may be achieved through using an in-tram'al gothic arch-tracing device (Geneva Dental,Beverly Hills, CA).11-14 The work of Kapur andYurkstas confirmed the findings of Trapozzanoand Kingery that the central bearing assemblywill provide equalization of occlusal pressure andincrease base stability when mucosal resiliency ismodest. I 1-13 Although the wax method of record-ing centric relation is accurate, it requires consid-erable experience to produce repeatability. Thegothic tracing method is a highly reliable tech-nique for even the inexperienced operator (Figs 12and 13).12,13Centric relation records can be read-ily verified at the wax try-in stage.
Figure 13. Intraoral central-bearing gothic arch-tracing device.
Clinical Technique1. Irreversible hydrocolloid (Accu-Gel, Ivoclar
North America, Inc., Amherst, l\TY)and stockedentulous trays (Accu-Dent, Ivoclar NorthAmerica, Inc.) are used to make overextendedmaxillary and mandibular impressions. Max-illary and mandibular impressions are pouredand casts trimmed. Muscle tonicity and frenumextensions are determined intraorally andnoted for both the maxillary and mandibu-lar denture arches. Following location of themylohyoid ridges, external oblique ridges, andretromolar pads intraorally, a myostatic outlineform is scribed on the mandibular cast.
2. Anterior tooth position, maxillary incisorlength, and lip support were determined withthe wax rim after which the anterior 6 teethwere set.
3. Vertical dimension of occlusion is determinedby evaluating the patient's interocclusal restspace, profile, tactile sense, and comfort, andcentric relation recordings were obtained withthe intraoral gothic arch tracing.9
4. The casts are mounted and occlusal plane de-termined using the heights of the retromolarpads and positions of the incisal edge of thecentral incisors.2 A metal template was setat the level of the incisal edge of the centralincisors and made level with the height ofthe highest retromolar pad and secured to themandibular cast. The template then serves asthe flat surface to which the maxillary zerodegree teeth are set (Fig I). After the maxillaryteeth are set, the mandibular anterior teethare arranged ensuring no anterior or lateralprotrusive contacts (Figs 4 and II). The cor-responding mandibular posterior bladed teethare set in a straight line over the edentulousridge.2
5. Centric relation, vertical dimension of occlu-sion, esthetic and phonetic relationships, oc-clusal plane angulation, and denture base sta-bility are verified at a wax try-in appointment.After receiving patient approval, the denturesare processed and delivered.
Although complete denture occlusion may be equi-librated with the Coble Intra-Oral Balancer TNI
(Coble Denture Research Co. Inc, Greensboro,

NC)4 or utilizing a clinical remount, in the authors'experience, a more simplified approach does ex-ist for linear occlusion.3 Following postprocessingequilibration on the articulator, occlusion is eval-uated intraorally via a three-step clinical process.While somewhat subjective, the first step is to lis-ten for a clear, distinctive single-click upon closing,which is indicative of uniform centric contact.15 Adouble-click indicates one side is occluding pre-maturely. Secondly, a close intraoral observationof centric relation closure will frequently enablea practitioner to determine which side is occlud-ing prematurely. Finally, the offending contact isverified with thin articulating film before adjust-ment.3,5,15
Mandibular denture base stability has been re-ported to be increased through linear occlusion.3
It is the authors' opinion that the mandibulardenture base stability is improved via linear oc-clusion, a steeper-than-conventional plane of oc-clusion, and an accurate centric relation recordingby a central bearing intraoral gothic arch tracing.Linear occlusion has been reported to significantlyreduce transverse force vectors and to provide aconsistent vertical seating force in both centricand eccentric mandibular movement, thus im-proving stability.2,3,5,11-14
Although linear occlusal schemes can beachieved using acrylic opposing acrylic or porce-lain opposing acrylic, the use of porcelain-porcelain occlusion is most resistant to wear.Porcelain-porcelain occlusion is distasteful tosome practitioners. First, the increased clickingsound during mastication may be disturbing to thepatient and second, some believe it is more diffi-cult to adapt to porcelain teeth.1,3,5Some believeplastic, as opposed to porcelain, will more easilyaccommodate an occlusal disharmony. It seems alogical deduction that this could potentially elim-inate some postoperative discomfort.3 Some prac-titioners prefer the hardness of composite resinteeth as well as the ease of occlusal adjustment. 1
Porcelain teeth will always wear less than acrylicteeth, and it would stand to reason that this canhelp preserve the vertical dimension of occlusionover time.4.5 Linear occlusion can occasionallycause an esthetic concern for the patient whenflat plane teeth are set on the maxillary arch. Thisproblem can be easily rectified by using either an
anatomic first premolar or by esthetically reshap-ing the buccal aspect of the flat plane tooth.3
Although there are many acceptable tech-niques, the intraoral gothic arch tracing has beenproven to be repeatable and consistent even in in-experienced hands. It also increases maxillary andmandibular base stability by providing a centralbearing area during the recording process. This isespecially evident in severely resorbed mandibularridges.11-13
The purpose of this article was to present a less fa-miliar concept for providing improved mandibularprosthesis stability with the use oflinear occlusionand steeper occlusal plane selection. In this clin-ical technique, a gothic arch tracing device wasutilized to record centric relation. In the authors'experience with linear occlusion and the tech-niques presented here, exceptional mandibularprosthesis stability and patient satisfaction due tolack of movement of the denture bases, lack of sorespots, and fewer postoperative visits have been theresult.
The authors thank Palmer Meyer and ProfessionalDental Arts Laboratory, Lincoln, Nebraska, for theirpreparation of the dentures and casts. Special thanksto Dr.John Frush for his personal communication.
l. Lang BR: Complete denture occlusion. Dent Clin NorthAm 1996;40;85-10 I
2. FrushJP; Linear occlusion. III DentJ 1966;35;788-7943. Gronas DG, Stout CJ Lineal occlusion concepts for com-
plete dentures.J Prosthet Dent 1974;32;122-1294. MassadlJ; A metal-based denture with soft liner to accom-
modate the severely resorbed mandibular alveolar ridge.J Prosthet Dent 1987;57;707-711
5. Winkler S; Essentials of Complete Denture Prosthodontics,ed 2. Philadelphia, PA, WB Saunders, 1996
6. Jones PM; The monoplane occlusion for complete dentures.J Am Dent Assoc 1972;85;94-100
7. International Prosthodontic Workshop on CompleteDenture Occlusion; Paper presented at InternationalProsthodontic Workshop on Complete Denture Occlusion,1972, Ann Arbor, MI
8. Friedman S; Principles of setups in complete dentures.J Prosthet Dent 1969;22; 111-130
9. Zarb GA, Bolender, CL, Carlsson GE, et al: Boucher'sprosthodontic treatment for edentulous patients, ed II.St. Louis, MO, Mosby, 1997

10. Levin B: A reevaluation of Hanau's Laws of Articula-tion and the Hanau Quint. J Prosthet Dent 1978;39:254-258
II. Kingery RH: A review of some of the problems associ-ated with centric relation. J Prosthet Dent 1952;2:307-319
12. Trapozzano V: Occlusal records. J Prosthet Dent1955;5:325-332
13. Kapur KK, Yurkstas A: An evaluation of centric relationrecords obtained by various techniques. J Prosthet Dent1957;7: 770-786
14. Porter C: Simplicity versus complexity. J Prosthet Dent1954;2: 723-729
15. Bauman R: Minimizing post insertion problems. A proce-dure for removable partial denture placement. J ProsthetDent 1979;42:381-385