Embed Size (px)
Citation preview

1
1 Kristin Martin-Cook M.S. and Myron F. Weiner M.D. Alzheimer's Disease Center UT Southwestern Medical Center at Dallas
1
2

DEMENTIA OVERVIEW
The term dementia means a person has impaired ability to think, reason, or remember to the point that it affects their ability to function in activities of daily living. Persons with dementia and their families often have a high quality of life for many years, depending how they deal with the problems and changes that occur within each person and the relationship between family members. It is a process of dealing with increasing impairment and need for help.
The most common cause of dementia is Alzheimer disease (AD), one of the most common chronic illnesses of late life. By age 80, between 20% and 40% of Americans develop the disease, and it is the 80-year-plus portion of our population that is growing most rapidly. Based on these facts, it seems reasonable to expect that most of us will live with AD one way or another; by developing the disease or by caring for someone who is affected.
A less common form of dementia is so-called frontotemporal dementia; a collection of diseases (including Pick disease) that primarily damage the front part of the brain (AD affects the sides of the brain). In contrast to AD, in which the initial problems are related to memory, the problem in most persons with frontotemporal dementia is loss of judgment, with memory difficulty developing later. Some individuals with frontotemporal dementia have their first difficulties related to either expressing or understanding words. The other common cause of dementia is due to a condition that resembles Parkinson disease, and is called dementia with Lewy bodies because of the characteristic small, round bodies that develop in brain cells. In this disease, Parkinson-like symptoms such as problems with balance occur, as well as, sleep and mood disturbances.
Caring for a person with dementia is said to be more stressful than caring for persons with many other chronic illnesses. The following suggestions may help those coping with dementia.
Families are interested in helping their loved ones maintain a high quality of life and to retain their ability to function as long as possible.
3
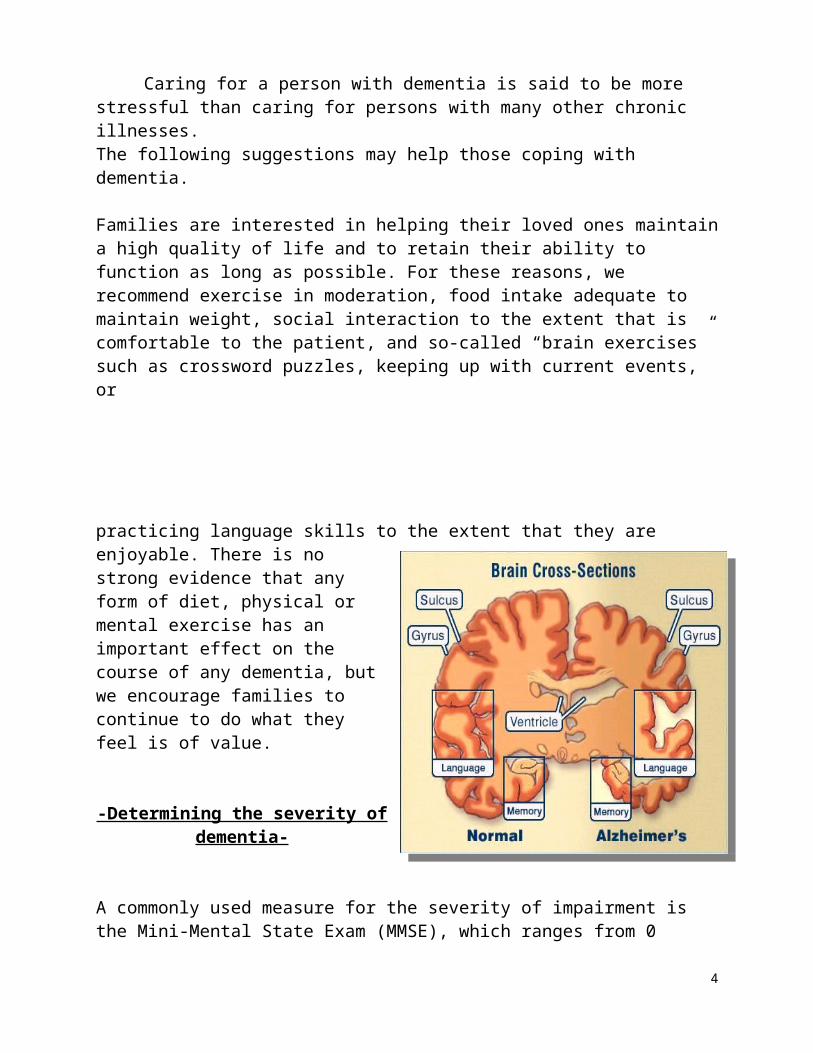
For these reasons, we recommend exercise in moderation, food intake adequate to maintain weight, social interaction to the extent that is comfortable to the patient, and so-called “brain exercises” such as crossword puzzles, keeping up with current events, or
practicing language skills to the extent that they are enjoyable. There is no strong evidence that any form of diet, physical or mental exercise has an important effect on the course of any dementia, but we encourage families to continue to do what they feel is of value.
-Determining the severity of dementia-
A commonly used measure for the severity of impairment is the Mini-Mental State Exam (MMSE), which ranges from 0 (severely impaired) to 30 (little to no impairment). Your physician may refer to this number.
AD is a unique disease in that no two cases are the same- symptoms can present with much fluctuation and individuality; however, certain symptoms can be loosely grouped into the following stages:
Early/Mild – average length is 1-3 years; memory loss primarily, with some changes in complex brain function (multi-tasking, learning new things, integrating a lot of information); some difficulty with complex activities of daily living like balancing checkbook, driving may become an issue, desire to socialize in smaller groups
Middle/Moderately impaired – average length is 5-7 years; increased language difficulties (word finding, writing, comprehension); difficulty with abstracting (time), increased repetitiveness, may lack awareness of problems, may need prompts to care for oneself (wears same thing over and over, not as attentive to hygiene); behavioral and personality changes are most common during this stage (irritability, frustration, agitation)
Late/Severely impaired – average length of time is 2-3 years, but is highly dependent on the quality of physical care provided;
4

gradual inability to care for basic needs without assistance, disorientation to people and places, finally motor losses (falling, trouble walking); speech and language are impaired (trouble understanding words, and difficulty putting together words in a meaningful way).
Like all of us, people who have a dementing illness will have strengths and weaknesses which do not decline in a uniform manner. A person may have severely impaired new learning and short term memory, while remaining able to reason and discuss things in detail. It is often possible to maximize use of preserved skills in order to compensate for deficits in cognition.
-Treatments -
Cholinesterase inhibitors (Aricept, Cognex, Exelon, Razadyne)-not a cure, but do help most patients function better for longer, slow down the progression of symptoms by increasing the availability of acetylcholine, an important neurotransmitter, in the brain.
Memantine / Namenda – This drug regulates levels of glutamate, an important chemical affecting the function of the cellular system and may reduce excitotoxicity in the brain. This drug is generally used in conjunction with the standard of care, Cholinesterace inhibitor whenever possible.
Vaccine ??? – some initial trials discontinued due side effects; however, several different forms of vaccine are in development with numerous studies in patients underway and recruiting new patients.
5

Antidepressants: Activating or sedating; chosen based on symptoms/purpose. These drugs are helpful for reducing frustration and irritability and may help people concentrate and function better.
Antipsychotic medications/anti-anxiety medications: for agitation, delusions, hallucinations or sleep problems
Be careful about using over the counter medications for sleep - many medications make people more confused
LONG-TERM PLANNING
It is difficult to plan for the future by making financial and legal arrangements, but now is the time, as soon as there is a diagnosis and while the person with dementia is able to personally and legally engage in the decision making process.
Legal things to consider: - take care of legal issues now while the person with AD can participate in the process rather than waiting until a legal issue comes up; it may be too late for the person to execute a legal document if you wait. Wills - designate how a persons assets will be distributed at the
time of their death Living wills – how you want to be cared for at certain critical points
near the end of life (life-prolonging treatment) Medical and Durable power of attorney (MUST HAVE) - allows
you to select the person you want to make legal, financial or medical decisions on your behalf when you are no longer able to do so. Can be broad or specific in stating what the appointed person can do or not do.
Living Trust - an individual is given the right to manage some or all of another person’s assets which are held in a trust with certain guidelines attached regarding how the money or assets should be used.
Guardianship - legal action taken if the person with dementia is no longer able to make legal decisions (execute legal documents) and needs someone appointed to make decisions for them.
Dallas Volunteer Attorney Program -In addition to sponsoring Debt Counseling Clinic, Legal Clinic for the Elderly, and Mental Health Law Clinic, the Dallas Volunteer Attorney program provides telephone referral of low-income Dallas County residents to volunteer attorneys
6
who provide free legal services. Voice: (214) 742-5768 www.dallasbar.org/dvap
The Area Agency on Aging (AAA) provides legal assistance through a contract with an attorney for individuals identified and referred by AAA staff. Call the AAA at 214-871-5065www.nctcog.org/cs/aging/older_adults_info.asp
Financial things to consider:
Insurance policies - who knows about them and where info is kept
Stock and bonds - who knows about them and where info is kept Medicare-covers hospital, doctors bills, rehab, hospice but NOT ASSISTANCE WITH DAILY CARE OR SUPERVISION Medicaid-income/need based, provides some financial assistance
with day care, home health, nursing home Spousal impoverishment - means that the spouse of a patient
needing care is allowed to keep their home, certain assets and moneys to support their own needs despite the patient needing to spend down other assets in order to qualify for federal and state financial programs like Medicaid and Community Based Alternatives.
Community resources:You are not alone. There are many services available to you to aid in coping with caregiving.
Alzheimer Association Dallas (214) 827-0062/ www.alz.org Adult Day Programs/Centers - place for cognitively impaired elders
who need supervision and structured activities
In home help - companions/sitters on average cost approximately $17.00 per hour through many home health agencies in community
7
-Friends Place – independent, private pay program in Richardson 972-437-2940 -Casa de Vida – activity and respite program at Northpark Presbyterian Church 972-783-8780 -Treasured Times – activity and respite program at Custer Rd.United

In-patient respite - many long term care facilities will take a patient temporarily (for days to a couple weeks to give the caregiver a break or allow them to travel)
Hospice – offers many services such as medications, in home health care visits and equipment all for maximizing a persons comfort near the end of life
Veterans benefits - low-cost medication program, home health, nursing home care
For help finding specific companies, services and facilities you can go online to www.newlifestyles.com
Questions when evaluating a facility:1. What type of payment is accepted? (do they have Medicaid beds, accept VA benefits)2. Do they have specialty/Alzheimer's care?Locked unit, appropriate dementia training, relatively stable long-term staff3. Are care plan meetings held at a time that family can attend?4. Are they flexible - ask how they will deal with situations that you have experienced with your loved one (trouble with using fork, wanting to go home…)5. How much staff and what type (nurses, aides) are there at different times of day?6. Visit without making an appointment. Note whether the patients look kept, content, and seem comfortable talking with the staff. Do the patients seem to want to be around the staff?7. Activities are great if you can engage in them and enjoy them, but are not universally of benefit to or appreciated by everyone, especially persons with dementia.8. What is the basic care routine? Where is bathing done, is it a comfortable, warm place? 9. You can compare nursing homes and obtain inspection results at:
www.medicare.gov and other online resources www.elderhope.com
8

BEHAVIOR MANAGEMENT
Behavioral changes are not uncommon but very individual. Some behaviors that are common are: wandering, pacing, making up stories (people are stealing…), over-reacting, irritability, impatience, shadowing the caregiver
***The key to understanding and managing behaviors is to identify and adjust the factors that trigger and maintain the behavior. It is always easier to anticipate and prevent a problem than to fix while it is occurring***:
1. Define the behavior – be specific about what behavior is really a problem
2. Identify what is happening before or what triggers the behavior (ask yourself who, what, when, where does this happen…)Interactive factors - how are the too of you interactingWhat are you asking of the person (too many steps involved, task appropriate to abilities, feelings about that task); how are you asking (tone of voice, touch, language); when are you asking (already agitated, time of day)Environmental factors - what is happening around the
personIs there too much noise; not enough light; are the surroundings unfamiliar; is there too much clutter
3. By identifying behaviors, triggers and consequences you can understand, anticipate, plan for, and decrease the occurrence of problem before they occur.
General Guidelines
9
Don’t expect the person with dementia to learn or to remember.
Fill for memory deficit; don’t point it out or try to improve it.
Help in word-finding by suggesting the word being sought.
Keep decision-making at a level that fits the person’s ability to function.
Ask persons with dementia to do only one thing at a time, and repeat.
Augment verbal requests or instructions with physical guidance and demonstration.
When persons with dementia are frustrated, take a break rather than explaining.
Allow persons with dementia to do as much of what they wish to do as they can
Avoid contest of wills. Don’t leave things in sight that you don’t want to be
picked up and lost When something is lost, look for it; don’t ask where it
is. Develop a predictable daily routine, including pleasant
activities and exercise. Keep explanations short and be willing to repeat. Focus on use of the person’s over-learned skills and
routines. Avoid unfamiliar activities, situations and places.
HOME SAFETY AND ENVIRONMENT
Three Principles of Home Safety
1. Prevention - we can not predict the future but we can anticipate possibilities. Even with careful planning, accidents can happen. However, checking the safety of the home helps the families take control of some of the potential problems that may create hazardous situations.
2. It is more effective to change the environment than it is to attempt to change the behavior of the person with cognitive problems. When
10

someone's memory is impaired, so is their ability to learn and reason through multiple steps.
3. By minimizing danger you can maximize independence. A safe environment is a less restrictive environment. The person with dementia can experience increased security and more mobility. It also lessens the caregiver's need for constant close supervision, thus reducing time, attention and stress in the caregiving task.
Examples:
A. Prevention--for example, if we think ahead, we can prevent falls by removing unanchored rugs, unsturdy furniture, and clutter in walkways. We can also prevent problems sometimes by providing assistive devices like, walkers, canes, bath rails...safe return program (a program of registering people who might become lost so they can be helped back home.)
B. Changing the environment rather than the person.-- for example, remove mirrors if they cause confusion. Don’t argue that pills have already been taken just remove pills from sight once taken. Establish routines and systems that compensate for memory problems.
C. Minimizing danger can maximize independence. -- for example, removing potentially dangerous things from the kitchen like the knobs from the stove, putting away dangerous chemicals and medications, picking up unanchored rugs, and taking weapons out of the home, make it more safe for the person with AD to access the house independently without family members feeling a need to provide constant supervision.
Environmental Variables to Maximize Awareness, and Orientation/using cues to increase functioning
1) Use memory aids/prompts. For example, large simple calender with dailyroutine or written reminders on it, label drawers to identify the location of clothing items and doors to direct a persons attention to important places like the bathroom. Provide a list
11

(simple and organized) of important or frequently used telephone numbers near the phone.
2) Use multiple cues that relate to different abilities and senses. For example, pictures, colors, and words to identify the bathroom and differentiate it from other rooms/doors.
3) Desired activities and/or locations should be easy to access and obvious.For a person with AD things that are out of sight are often out of mind. The person with AD is frequently unable to initiate, without cues, an activity and subsequently go look for the materials. For example, putting out old pictures or coins on the tablemay prompt a usually apathetic person to focus on sorting or
reminiscing.
Back to safety. PROVIDE FOR SAFE but FREE environment. Unrestricted access to the environment encourages autonomy and independence. A secured and safe outside area is important also--research has shown a decrease in agitation when doors to the outside are left unlocked with access to an outside area.
12
We have some general suggestions for caregivers’ self management:
Accept the person with dementia for who he is instead of trying to restore him to who he was.
You have as much right to a life as does the person you are caring for.
To the extent that you feel the need and are able to do so, take time for yourself.
To the extent compatible with your values and the needs of the person with AD, develop a separate life of your own.
Begin thinking of ways to have others share the caregiving with you, such as becoming a part of a group that is supportive of you, whether it be an Alzheimer’s Association support group or an informal group of caregivers.
Include your children; they don’t need to be protected and usually want to know how they can be involved.
If you feel depressed, seek treatment. You’ll feel better and you’ll do a better job or providing care.
Try not to endanger your own health. Remember that if you fail to take care of yourself, there may be
no one else left to care for your loved one.
13
CAREGIVER ISSUES
Common/Normal caregiver emotions: Grief and/or Depression about losses in the person
and life expectations Guilt about everything, not being patient enough,
not knowing how to handle things or about being well when my loved one is struggling
Resentment and/or anger about the disease and even the person with AD
What makes you feel bad? Anticipation – live a day or problem at a time. It sounds “corny” but aside
from taking care of some basic legal and financial decisions and problems as they arise, trying to anticipate what life or your loved one will be like in months or years may not be accurate and will lead to nothing productive. Worrying excessively about next year will rob you of the time you have now with each other. Live the moments you have.
Pick your battles – if it really doesn’t matter then don’t sweat it. Often we get caught up in the performance of a task, or the way things “should” be and end up arguing, getting upset or missing an opportunity over something that didn’t really matter.
Developing a coping plan to use when feeling overwhelmed : Coping thoughts - say to yourself:
“Been there done that!; What do I need to take care of this - make a plan of action;
What is the worst thing that could happen?; What would I say to a friend in this Situation?; Does it really matter? Have a support system in place so you know who and where to turn when
you need a break Realistic Expectations (of you and the patient) / Know your limits Pleasant Events - with and without the person with dementia
Try to build in events that you can enjoy together without being the "caregiver."
Prioritize and relax - in the end do what is important and let the rest slide for now.
Stress relievers – talk to someone, physical exercise, get away for a while, massage, take a nap, listen to music, imagery-sit quietly and think of a happy memory and view the memory in detail, use other methods of stress reduction that you can learn more about in books or internet
Join a support group near you www.alz.org/greater dallas
14
ACTIVITIES
Everyone can do something and everyone enjoys doing something. Activities serve many purposes but generally they should:
Empower - be an opportunity to express oneself in some way, give responsibility and a sense of control and contribution
Maintain - use intact or maintained cognitive, social or physical skills
Structure - provide a comfortable amount of stimulation, promote success, and give an opportunity to relate to others.
Almost any activity can be modified into doable tasks for a person at any level of skill or impairment.
List of Activities (everyday activities)
Clip coupons Cards/games Organize or rummage through
drawers Exercise Plant seeds (window boxes)
Water plants Weed the garden
Sweep Rake leaves
Cut and arrange flowers
Vacuum
Fold clothes Dust
Roll or sort coins Feed animals (even just a fish)
Sort, test, sharpen pens/pencils Groom pets
Baking (or at least stirring) Roll yarn into a ball Sewing buttons or on material
15
Sand wood(for frustrated workers)
Sort bottles, papers for recycling
And many, many more…
Help in the kitchen (wash veggies, peel and cut fruit, mix, fill salt and pepper shakers)
Painting (not masterpieces maybe but appropriate craft items like blocks of wood)
Think simplicity and repetitive - any activity that involves doing only 1 or 2 steps over and over and over.
Successful use of activities means focusing on the doing rather than the completion or end product.
HELPFUL HINTS
Following is a list of some common problems and basic care ideas, excerpted from a handout published by the Alzheimer’s Disease and Related Disorders Association Greater Philadelphia Chapter, Inc.
Wandering
1. Establish regular times for daily activities: meals, chores, bed
2. Gauge activity level to patients’ tolerance.
3. Always make sure that patients have in their possession a card containing their home address and phone number. They should wear a medic-alert bracelet identifying them as “memory impaired.”
4. Use a simple sound system (bells, for example) so that you
will know patients have gone out the door.
5. Ask neighbors to call you if they see patients on the street unaccompanied.
6. If possible, give patients time to walk around, to go into the yard, and so forth. Give in, to some degree, to their desire to wander.
7. Divert patients into their activities such as dusting, folding laundry, or yard work.
Memory Problems16

Establish a system that supports a reality orientation.
These include:1. A clock with large numbers.2. An easy-read appointment
calendar with large letters and numbers.
3. A chalkboard or bulletin board for recording the daily schedule.
4. A place for frequency used items such as keys, hearing aids, and eyeglasses.
Insomnia
1. Restrict nap time.2. Provide adequate exercise
during the day.3. Have a simple, consistent
bedtime routine.4. Use a night light.5. Consider sleep medications or
small amounts of beer, wine, or sherry at bedtime. (Talk with your physician about this.)
6. Limit fluids after dinner.
Difficulty in Communication
1. If unable to understand patients’ behavior, attempt to understand the emotion behind it.
2. Ask patients to stop, relax, and speak slowly.
3. Do not criticize the speech itself.
4. Speak distinctly in short, simple sentences when talking with patients.
5. Be calm and reassuring.6. Do not speak in a loud voice.
7. Maintain eye contact and use touch.
Catastrophic Reactions (Strong Emotional Response)
1. Respond to the emotion expressed.
2. Be calm and use a quiet tone of voice.
3. Redirect patients to another activity or another room.
4. Avoid similar situations that may cause this reaction.
5. Remember that the reaction is time limited.
6. Remember that restraining patients will probably make matters worse.
Worsening in the Evening
1. Leave lights on.2. Tell patients where they are and
what is happening.3. Plan the day so that fewer
things are expected of patients on the evening.
4. Provide a calm environment.5. Plan your day so that you are
reasonably rested and not too pressed for time.
Nervousness and Restlessness
1. Respond calmly and gently.2. Attempt to determine the cause
of restlessness, for example, pain or the need to urinate. Simplify what is going on around the patients.
3. Respond with an appropriate substitute activity. For
17

example, take patients for a walk or provide a simple task.
4. Avoid beverages with caffeine.5. Consult your doctor about the
use of medication.
Suspiciousness
1. Keep in mind that accusations of stealing are common.
2. Remember, patients cannot control this behavior.
3. Do not argue or confront patients; be reassuring.
4. Together, make a list of where things are.
5. Offer to help patients find the lost article.
Anger
1. Respond calmly2. Remove patients from the
situation or remove the upsetting stimulus.
3. Look for the event that precipitated the reaction so you can prevent or minimize a recurrence.
EMERGENCY MEDICAL INFORMATION
Name: ________________________________________ Date of Birth: _____________________
Address: ________________________________________ SS #: ____________________________18
________________________________________ Male _______ Female______
Phone: ________________________________________
Family/EMERGENCY Contacts:
(name,phone,relationship)______________________________________________________________________
______________________________________________________________________
Medical history or diagnoses: (check and add details if appropriate)
____Memory or cognitive problems ____________ ____Blood Pressure____Seizures ____HIV____Heart condition ________________________ ____Anemia____Cancer _______________________________ ____Diabetes____Asthma ____Stroke: __________________________________Delirium ____Other: ______________________________
Current medication/vitamins Use Dose / frequency Location kept in house
Name of Primary doctor: _____________________________ address: _____________________________________
Name of other treating doctor: ____________________________ address: ___________________________________
Allergies: ________________________ ____________________________
________________________ ____________________________
Medical Insurance Coverage information: _______________________________________________
_______________________________________________
PLACE ON REFRIGERATOR, WALLET AND GLOVE COMPARTMENT OF CAR
19





























