Embed Size (px)
Citation preview

8787
INTRODUCTION
Hepatic fibrosis has emerged as a highly relevant aspect of liverbiology because of the significant progress in uncovering its mecha-nisms, combined with a growing realization that effective antifibrotictherapies may soon alter the natural history of chronic liver disease.Thus, liver fibrosis can now be viewed as a clinical problem whosediagnosis and treatment will soon have rational, evidence-basedapproaches. This progress is very timely, as the continued ‘aging’ ofthe HCV-infected cohort and the growing prevalence of obesity-related liver diseases are leading to precipitous increases in theprevalence of advanced liver disease.1 With these issues in mind, thischapter will review clinical aspects of hepatic fibrosis, includingnatural history, pathophysiologic mechanisms, current and futuretools for diagnosis, and emerging antifibrotic strategies. In addition,several recent reviews highlight many of these aspects in greaterdetail.2–6
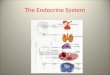
Hepatic fibrosis is the accumulation of extracellular matrix, orscar, in response to acute or chronic liver injury. Fibrogenesis repre-sents a wound healing response to injury (Figure 6-1), and ultimatelyleads to cirrhosis. Cirrhosis is the end-stage consequence of fibrosisof the hepatic parenchyma, resulting in nodule formation that maylead to altered hepatic function and blood flow. Both fibrosis andcirrhosis are the consequences of a sustained wound-healingresponse to chronic liver injury from a range of causes, includingviral, autoimmune, drug induced, cholestatic and metabolic diseases.The clinical manifestations of cirrhosis vary widely, from no symp-
toms at all to liver failure, and are determined by both the natureand severity of the underlying liver disease as well as the extent ofhepatic fibrosis. Up to 40% of patients with cirrhosis are asympto-matic and may remain so for long periods, but progressive deterio-ration leading to death or liver transplantation is typical oncecomplications (such as ascites, variceal hemorrhage or encephalopa-thy) develop. In such patients there is a 50% 5-year mortality, withapproximately 70% of these deaths directly attributable to liverdisease.7 In asymptomatic individuals cirrhosis may be first sug-gested during routine examination, although histologic analysis maybe required to establish the diagnosis.
Cirrhosis affects hundreds of millions of patients worldwide. Theoverall burden of liver disease in the United States – the vast major-ity of which is due to chronic disease with fibrosis – continues toexpand, exacting an increasing economic and social cost.1 Indeed, inthe US cirrhosis is the most common non-neoplastic cause of deathamong hepatobiliary and digestive diseases, accounting for approxi-mately 30000 deaths per year. In addition, 10000 deaths are dueto liver cancer, the majority of which arise in cirrhotic livers, con-sistent with a steadily rising mortality rate from hepatic cancer.8
Notably, hepatocellular carcinoma is the most rapidly increasingneoplasm in the US and western Europe.9
Initial studies of hepatic fibrosis focused on the composition ofextracellular matrix in liver, and continued incremental progress inthis area is still anticipated. However, attention has gradually shiftedtowards exploring the cellular basis of fibrosis and the cellular medi-ators that drive fibrosis progression and regression (see Pathophysi-ology, below). In general, the molecular composition of the scar
Section I: Pathophysiology of the Liver
6HEPATIC FIBROSIS ANDCIRRHOSISDon C. Rockey and Scott L. Friedman
AbbreviationsALT alanine aminotransferaseAST aspartate aminotransferaseAUROC area under the receiver operator
characteristicBMI body mass indexCINC cytokine-induced neutrophil
chemoattractantCTGF connective tissue growth factorDDR discoidin domain receptorsECM extracellular matrixEGF epidermal growth factorELF European liver fibrosisET-1 endothelin-1FGF fibroblast growth factorFPI fibrosis probability indexGGT g-glutamyl transferase
GnT-III N-acetylglucosaminyl transferase IIIHA hyaluronic acidHBV hepatitis B virusHCV hepatitis CHGF hepatocyte growth factorHIV human immunodeficiency virusHOMA-IR insulin resistance by the homeostasis
model assessmentIL-10 interleukin-10JI jejuno-ilealLPS lipopolysaccharideMCP-1 monocyte chemotactic protein-1MEGX monoethylglycinexylidideMELD model for end-stage liver diseaseMMPs matrix metalloproteinasesMMP-2 matrix metalloproteinase 2
MMP-9 matrix metalloproteinase 9NASH non-alcoholic steatohepatitisNGFR nerve growth factor receptorNO nitric oxidePDGF platelet-derived growth factorPELD pediatric end-stage liver diseasePIIINP propeptide of type III collagenPPAR peroxisomal proliferator-activated receptorQTL quantitative trait lociROC receiver operating characteristicTGF-b1 transforming growth factor beta 1TIMPs tissue inhibitors of metalloproteinasesULN upper limit of normalVEGF vascular endothelial growth factor
Ch006-X2998.qxd 3/15/06 5:21 PM Page 87

Section I. Pathophysiology of the Liver
tissue in cirrhosis is similar regardless of etiology, and resembles thatof other parenchymal scarring (e.g. kidney), consisting of the extra-cellular matrix constituents, collagen types I and III (i.e. ‘fibrillar’collagens), sulfated proteoglycans, and glycoproteins.10 However,some isoforms of extracellular matrix constituents, for examplefibronectin11 and proteoglycans,12 may be relatively enriched duringprogressive injury. These scar constituents accumulate from a netincrease in their deposition in liver and not simply from the collapseof existing stroma.
CLINICAL ASPECTS OF HEPATICFIBROSISNATURAL HISTORY AND RISK FACTORSFibrosis leading to cirrhosis can accompany virtually any chronic liverdisease that is characterized by the presence of architectural dis-ruption and/or inflammation. The vast majority of patients with liverdisease worldwide have chronic viral hepatitis, or steatohepatitisassociated with either alcohol or obesity; other etiologies of liverdisease include parasitic infestation (e.g. schistosomiasis), auto-immune attack on hepatocytes or biliary epithelium, neonatal liver disease, metabolic disorders including Wilson’s disease,
hemochromatosis and a variety of storage diseases, chronic inflam-matory conditions (e.g. sarcoidosis), drug toxicity (e.g. metho-trexate or hypervitaminosis A), and vascular derangements, eithercongenital or acquired.
Of the many causes of chronic liver disease, our understanding ofnatural history of fibrosis is most complete in HCV, with some infor-mation about HBV and steatohepatitic diseases, including alcoholicliver disease and NASH. Information about fibrosis progression inother diseases is largely anecdotal, but the development of cirrhosistypically requires many years to decades. There are, however, somenotable exceptions in which the development of cirrhosis can begreatly accelerated, possibly occurring within months rather thanyears: (1) neonatal liver disease – infants with biliary atresia maypresent at birth with severe fibrosis and marked parenchymal dis-tortion; (2) HCV-infected patients after liver transplantation – asubset of patients who undergo liver transplantation for HCV cir-rhosis may develop rapidly progressive cholestasis and recurrent cir-rhosis within months, requiring retransplantation;13 (3) patients withHIV/HCV co-infection – these patients have relatively rapid fibro-sis compared to those with HCV alone,14 especially if the HIV isuntreated (see below); (4) severe delta hepatitis;15 and (5) somecases of drug-induced liver disease. These examples of ‘fulminantfibrosis’ probably reflect dysregulation of several pathways, includ-ing defective immunity, massive inflammation and necrosis, and/or
88
Normal liver Liver injury
Quiescentstellate cell
Endothelial cell
Hepatocytes
Hepatic sinusoid
Kup�er cell
Activatedstellate cell
Depositionof scar matrix
Loss offenestrae
Kup�er cellactivation
Space of Disse
Loss of Hepatocyte microvilli
Figure 6-1. Hepatic liver cells and the hepatic sinusoid in normal and injured liver. On the left panel is shown the multiple key liver-specific cellular elements inthe normal liver, including hepatocytes, endothelial cells, Kupffer cells, and stellate cells. Stellate cells are located within the subendothelial space of Disse (i.e.between the sinusoidal endothelium and hepatocytes). The figure emphasizes the close physical relationships between the various cellular elements in the liver.After liver injury, changes in numerous cells occur; for example, stellate and Kupffer cells become activated (see Figure 6-3), hepatocytes lose their microvilli, andendothelial cells lose their characteristic fenestrae. All of these features contribute to continued cell activation and injury, as well as dysfunction at the wholeorgan level.
Ch006-X2998.qxd 3/15/06 5:21 PM Page 88

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
altered matrix resorption. Together, they highlight the highlydynamic nature of scar accumulation and degradation. Moreover,when matrix accumulation is unopposed because degradation is inef-fective, more rapid fibrosis may ensue.
Once cirrhosis and its complications develop the prognosis is pre-dicted by widely used systems, including Child–Pugh, PELD16 andMELD,17 which are predictive independent of the etiology of liverdisease.
Hepatitis C VirusThe risk and natural history of fibrosis associated with HCV havebeen greatly clarified as a result of several large clinical studies incor-porating standardized assessments of fibrosis that combine detailedhistorical and clinical information.18 The disease can run a remark-ably variable course, from decades of viremia with little fibrosis toa rapid onset of cirrhosis within 10–15 years. It appears to be hostfactors rather than viral factors that correlate with fibrosis progres-sion in HCV. The data supporting this conclusion include the fol-lowing: (1) there is no relationship between viral load or genotypeand severity of fibrosis even though these former factors affect theresponse to antiviral therapy; (2) human promoter polymorphisms(e.g. TGF-b1 and angiotensin) appear to correlate with fibrosisrisk,19 with large-scale efforts currently under way to identify addi-tional genetic markers of fibrosis risk;20 (3) host immune phenotypemay be critical, as there is more rapid progression in immunosup-pressed patients, whether due to HIV or to immunosuppressivedrugs.14 In mice, a Th2 phenotype strongly correlates with fibrogenicpotential,21 which has led to successful efforts to use quantitativetrait loci (QTL) mapping to identify specific fibrosis risk genes inthese animals.22
Other identified host risk factors for more rapid progression ofHCV include: (1) older age at the time of infection; (2) concurrentliver disease due to HBV or alcohol (>50g/day); it is uncertain,however, whether lesser amounts of alcohol intake are additivetowards fibrosis progression: recent studies suggest that less than50g/day of alcohol results in a neglible increased risk of hepaticfibrosis;23 (3) male gender; (4) increased body mass index (BMI),associated with hepatic steatosis;24 (5) HIV infection or immuno-suppression following liver transplantation.
Because standard clinical indices cannot distinguish betweenminimal and even advanced fibrosis, knowledge about these riskfactors and duration of infection can greatly inform clinical man-agement. Thus, for chronic HCV, if the time of infection is knownand a biopsy obtained at any time thereafter, the rate of progressionper year based on either Ishak or METAVIR scoring can be esti-mated.25 Although initial analyses of this type suggested that fibro-sis progression is truly linear, it is now increasingly clear that theprogression rate accelerates as the disease advances,26 such that ittakes less time to progress between Metavir stages 3 and 4, thanfrom stage 1 to 2, for example.
Assessment of fibrosis stage and rate of fibrosis progression can be valuable for at least three reasons: (1) the actual stage of fibro-sis will indicate the likelihood of response to a-interferon or a-interferon/ribavirin, as the advanced stages of fibrosis (F3 or F4)generally have a lower response rate to antiviral therapy;27,28 (2) iflittle fibrosis progression has occurred over a long interval, thentreatment with antiviral therapy may be deemed to be less urgent
and it may be safe to await more effective and/or better-toleratedtherapy; (3) the approximate time to the development of cirrhosiscan be estimated. This would not, however, indicate if or when clin-ical liver failure would occur, as the complications of liver disease may be delayed for up to a decade or more after the establishmentof cirrhosis. As genetic risk markers that predict a rapid fibrosis progression rate are developed, this information, combined with the absolute stage of fibrosis, may enable more accurate identifica-tion of patients at risk for disease and thus in need of antifibrotictherapy.
Hepatitis B VirusVery few studies have assessed the progression rate of fibrosis inchronic HBV infection. In general, inflammatory activity, as influ-enced by viral factors, including e Ag status, that indicate active viralreplication, correlates with fibrosis.29,30 Fibrosis progression has beencorrelated with HBV genotype in at least one study.31 In a subset ofpatients a rapidly progressive ‘fibrosing cholestatic hepatitis’ mayoccur,32 but there are neither definitive risk factors for this condi-tion nor unique etiologic, cellular or molecular determinants identi-fied. In addition, delta hepatitis superinfection or co-infection maygreatly accelerate the risk of advanced fibrosis and cirrhosis.15 Whatis striking, however, is that virologic suppression in response topotent antiviral regimens can effect remarkable improvement not only in serum alanine aminotransferase (ALT) levels and histologic inflammation, but also in fibrosis.15,33–35 Indeed, dramaticresolution of cirrhosis in a 10-year follow-up has been reported in patients with delta hepatitis who were successfully treated witha-interferon.15
Alcoholic Liver DiseaseThe clearest clinical determinant of fibrosis is continued alcoholabuse: patients with fibrosis who continue to drink are virtuallyassured of progression. In addition, two clinical features commonlyseen in steatohepatitis, elevated BMI and serum glucose, also conferan increased risk of fibrosis in alcoholic liver disease.36 Pathologically,the presence of pericentral fibrosis (central hyaline sclerosis) carriesa high risk of eventual panlobular cirrhosis, which is almost certainif alcohol intake continues.
Non-Alcoholic SteatohepatitisThere is a critical need for better data about natural history, riskfactors for fibrosis, and rate of fibrosis progression in NASH, issuesnow being addressed in several multicenter studies. Patients withonly steatosis and no inflammation appear to have a benign coursewhen followed for up to 19 years;37 however, it is unclear whetherthis lesion is completely distinct from steatohepatitis, or instead represents a precursor of NASH. It is instructive to remember thatHCV fibrosis progression rates were underestimated shortly afterthe virus was first identified, as many patients had a relatively earlyfibrosis stage. With continued infection, however, a sizeable fractioneventually have progressed to more advanced stages. In a parallel situation, the obesity epidemic in the US and the developed worldis only now being fully appreciated, and a threshold level of obesitymay have only begun to confer a risk of liver disease that will becomeclinically significant in the next decade. In patients with sustained
89
Ch006-X2998.qxd 3/15/06 5:21 PM Page 89

Section I. Pathophysiology of the Liver
NASH spontaneous histologic improvement is very uncommon, butbetter longitudinal data are needed to understand the natural historyof this disease; for example, data examining the evolution of NASHin patients undergoing bariatric surgery who have extensive weightloss and improvement in their metabolic syndrome are awaited. Inthree combined studies of 26 patients followed with sequentialbiopsies for up to 9 years, 27% had progression of fibrosis and 19%advanced to cirrhosis, but none had reversal of fibrosis.37 Of interest is the recurrence of NASH following liver transplantationin some patients with cryptogenic cirrhosis, implicating an underly-ing metabolic defect that may account for liver disease in both thenative and the transplanted organs.
Risk of fibrosis and rate of progression are critical issues that willinfluence risk stratification and patient selection for clinical trials, asprogression to cirrhosis is the most important clinical consequenceof NASH. Recently developed systems to grade and stage liverdisease in NASH38 should allow for improved, prospective collec-tion of standardized data that can further address these vital questions.
In general, increasing obesity (BMI) >28 kg/m2) correlates with severity of fibrosis and risk of cirrhosis. Other risk factorsinclude necroinflammatory activity with ALT >2¥ normal and/orAST/ALT >1, age, elevated triglycerides, insulin resistance and/ordiabetes mellitus, and systemic hypertension.39 It is uncertainwhether these features are comparable across the spectrum of dis-orders associated with NASH, including obesity with insulin-resist-ance, JI (jejuno-ileal) bypass, total parenteral nutrition and rapidweight loss, among others. Whether these factors represent surro-gates for other risk factors (i.e. reduced antioxidant levels in olderpatients, increased renin–angiotensin activity in hypertensives) isunknown. Ratziu and colleagues40 have reported a clinicobio-logicalscore that combines age, BMI, triglycerides and ALT and whichreportedly has 100% negative predictive value for excluding signifi-cant fibrosis.
REVERSIBILITY OF FIBROSIS AND CIRRHOSISThere is now clear evidence that fibrosis and even cirrhosis can bereversible. The feature common to all cases of cirrhosis improve-ment is the elimination of the underlying cause of liver disease,whether due to eradication of HBV,41 delta hepatitis15 or HCV,42
decompression of biliary obstruction in chronic pancreatitis,43 or toimmunosuppressive treatment of autoimmune liver disease.44 More-over, there is ample evidence of reversibility in animal models,which provide vital clues to underlying mechanisms.45
Earlier studies demonstrated that fibrosis improves with treat-ment of HCV,46 and even cirrhosis can regress following HCV eradication with a-interferon/ribavirin.42 Among a large cohort ofpatients successfully treated with this combination there were 150with cirrhosis, half of whom had a reduction in their fibrosis scoreaccording to METAVIR staging, with several regressing by two ormore stages. Because fibrosis in HCV typically progresses over threedecades, one might anticipate an equally slow but steady regressionof fibrosis following viral clearance.
It remains unclear what distinguishes those patients whose cir-rhosis is reversible from those in whom it is fixed. Potential factorsinfluencing reversibility probably include: (1) a prolonged period ofestablished cirrhosis, which could reflect a longer period of cross-linking of collagen, rendering this collagen less sensitive to degrada-tion by enzymes over time. Animal studies now clearly support thispossibility;47 (2) total content of collagen and other scar molecules,which might lead to a large mass of scar that is physically inacces-sible to degradative enzymes; (3) reduced expression of enzymesthat degrade matrix, or sustained elevation of proteins that inhibitthe function of these degradative enzymes, in particular elevatedlevels of tissue inhibitors of metalloproteinases (TIMPs), whichblock matrix proteases and also prevent apoptosis of activated stellate cells.48,49 All three scenarios highlight the dynamic processof collagen deposition and degradation.
PATHOPHYSIOLOGY OF HEPATICFIBROSIS AND CIRRHOSISEXTRACELLULAR MATRIX (ECM) IN THE NORMALAND THE FIBROTIC LIVERExtracellular matrix refers to the array of macromolecules that com-prise the scaffolding of normal and fibrotic liver. These macromol-ecules consist of three main families: collagens, glycoproteins andproteoglycans (see 10 for review). The number of collagens identi-fied in liver is rapidly growing, and includes collagen XVIII, whichis a precursor to the molecule angiostatin. Glycoproteins includefibronectin, laminin, merosin, tenascin, nidogen, and hyaluronicacid, among others. Proteoglycans include heparan, dermatan sul-fates, chondroitin sulfates, perlecan dystroglycan syndecan, biglycanand decorin. There is tremendous heterogeneity of these matrixmacromolecules with respect to their different isoforms, variablecombinations within different tissue regions, and changes related to age.
In normal liver the subendothelial space of Disse separates theepithelium (hepatocytes) from the sinusoidal endothelium. Thisspace contains a basement membrane-like matrix which, unlike thetypical basement membrane, is not electron dense. The hepaticbasement membrane is composed of non-fibril-forming collagens,including types IV, VI and XIV, glycoproteins and proteoglycans.This normal subendothelial ECM is critical for maintaining the dif-ferentiated functions of resident liver cells, including hepatocytes,stellate cells and sinusoidal endothelium.
In contrast to basement membrane-type matrix, in normal liverthe so-called interstitial ECM is largely confined to the capsule,around large vessels, and in the portal areas. It is composed of fibril-forming collagens (e.g. types I and III) together with cellular (EDA)fibronectin, undulin, and other glycoconjugates.
As the liver becomes fibrotic, the total content of collagens andnon-collagenous components increases three- to fivefold, accompa-nied by a shift in the type of ECM in the subendothelial space fromthe normal low-density basement membrane-like matrix to inter-stitial-type matrix (see 10 for review). This ‘capillarization’ leads tothe loss of hepatocyte microvilli and the disappearance of endothe-lial fenestration (Figure 6-1).
90
Ch006-X2998.qxd 3/15/06 5:21 PM Page 90

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
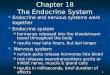
The outcome of fibrogenesis is the conversion of normal low-density basement membrane-like matrix to high-density interstitial-type matrix. A number of components are responsible for ECMremodeling (see 49,50 for reviews) (Figure 6.2). These include afamily of zinc-dependent enzymes matrix metalloproteinases(MMPs),51 their inhibitors (tissue inhibitor of metalloproteinases,TIMP), and several converting enzymes (MT1-MMP, andstromelysin, for example).
In human liver diseases there is down-regulation of MMP1 (inter-stitial collagenase, collagenase I) and up-regulation of MMP2 (gelati-nase A) and MMP9 (gelatinase B). Based on the differing substratespecificities of these enzymes, the result is increased degradation ofbasement membrane collagen and decreased degradation of inter-stitial collagens. These activated MMPs are regulated in part by theirtissue inhibitors, the so-called TIMPs. TIMP1 and TIMP2 are up-regulated relative to MMP1 in progressive experimental liver fibro-sis, which may explain the decreased degradation of interstitial-typematrix observed in experimental and human liver injury. In contrast,during the resolution of experimental liver injury TIMP-1 and TIMP-2 expression is decreased whereas collagenase expression isunchanged, resulting in a net increase in collagenase activity andincreased resorption of scar matrix.
Stellate cells are a key source of MMP-2 and stromelysin. Theyalso express TIMP-1 and TIMP-2 mRNAs and produce TIMP-1 andMT1-MMP MMP-9, which is a type IV collagenase locally secretedby Kupffer cells, and may also be produced by stellate cells in
response to interleukin-1.52 The source of MMP-1, which plays acrucial role in degrading the excess interstitial matrix in advancedliver disease, is still uncertain.53 However, interstitial collagenaseactivity in liver may be attributable to either MT1-MMP or evenMMP-2, although further studies are required.
ECM–CELL INTERACTIONSChanges in the microenvironment of the space of Disse result inphenotypic changes in all resident liver cells. Hepatic stellate cellsare activated by the surrounding increase in interstitial matrix.54
Sinusoidal endothelial cells produce cellular fibronectin in very earlyliver injury, which also contributes to stellate cell activation. In addi-tion, endothelial cells produce type IV collagen, proteoglycans andfactors (e.g. urokinase-type plasminogen activator) that participatein the activation of latent cytokines such as TGF-b1. ActivatedKupffer cells release cytokines and reactive oxygen intermediatesthat may stimulate stellate cells in a paracrine manner.55 Plateletsare also an abundant source of cytokines upon injury, producing arich array of important growth factors. Hepatocytes, the most abun-dant cells in the liver, generate lipid peroxides following injury thatlead to stellate cell activation, a prerequisite for fibrogenesis (seebelow).
The dynamic interactions between fibrogenic cells in liver and theECM is an important determinant of fibrogenesis. The ECM is areservoir for growth factors, for example platelet-derived growthfactor (PDGF).10 Like all cytokines, PDGF signals by binding to
91
Activated stellate cell
Apoptotic stellate cell
Normal ECM
MT1-MMPMMP-2TIMP-2
Early pathologicaldegradation
MMP-1MMP-13Other MMPs
Regression
TIMP-1TIMP-2
Progression
Kupffer cell
Figure 6-2. Emerging Mechanisms of Early Pathologic Matrix Degradation, Fibrosis Progression & Fibrosis Resolution in Chronic Liver Disease. Activa-tion of stellate cells (top left panel) is a key event in hepatic fibrosis, and is associated with pathologic matrix degradation due to increased production of mem-brane type matrix metalloproteinase 1 (MT1-MMP), matrix metalloproteinase-2 (MMP-2), and tissue inhibitors of metalloproteinases (TIMPs), leading toreplacement by interstitial collagen or scar matrix. As fibrosis progresses (middle panel), sustained expression of TIMPs prevents matrix degradation and apop-tosis of activated stellate cells. Regression of fibrosis (upper right panel) is associated with increased apoptosis of activated stellate cells. Apoptosis requiresdecreased expression of tissue inhibitor of metalloproteinase-1 (TIMP-1), yielding a net increase in protease activity. These events may occur coincident with pro-duction of matrix metalloproteinases, which could include MMP-1 (in humans) and/or MMP-13 (in rodents), although cellular sources of these enzymes (possi-bly including Kupffer cells), and clear evidence of their induction in vivo are still lacking. Validation of these events and further elucidation of mechanismsunderlying fibrosis regression represent key challenges for future studies.147a
Ch006-X2998.qxd 3/15/06 5:21 PM Page 91

Section I. Pathophysiology of the Liver
membrane receptors. The PDGF receptor belongs to a receptorfamily known as receptor tyrosine kinases, which collectively are keytransducers for many important cytokines, including hepatocytegrowth factor (HGF), epidermal growth factor (EGF), vascularendothelial growth factor (VEGF) and fibroblast growth factor(FGF). Interestingly, a new subclass of receptor tyrosine kinases, so-called discoidin domain receptors (DDR), has been identified; thisgroup of receptors signal in response to fibrillar collagens rather thanpeptide ligands.56 Indeed, stellate cell activation is accompanied byup-regulation of DDR2 receptors, and increased signaling is associ-ated with altered MMP-2 expression.57,58 Intracellular signaling cas-cades downstream of receptor tyrosine kinases and other receptorsare pervasive (see 59 for review).
Integrins are another type of membrane receptor that transduceextracellular signals in liver. These are heterodimeric transmem-brane proteins composed of an a and a b subunit whose ligands arematrix molecules rather than cytokines. Several integrins and theirdownstream effectors have been identified in stellate cells, includ-ing a1b1, a2b1, a5b1, avb1, avb3 and a6b4.6,60,61 Integrins mayalso complex with other receptor families in mediating cell motilityand fibrogenesis, for example the tetraspanin family of receptors.62
HEPATIC STELLATE CELL ACTIVATION – THECOMMON PATHWAY LEADING TO HEPATICFIBROSISThe identification of stellate cells as the key cellular source of extra-cellular matrix in liver has been a major advance. This distinct cellpopulation, located in subendothelial space of Disse between hepa-tocytes and sinusoidal endothelial cells (Figure 6-1), represents one-third of the non-parenchymal population or about 15% of the totalnumber of resident cells in normal liver.63 In normal liver they arethe principal storage site for retinoids (vitamin A metabolites),
which accounts for 40–70% of retinoids in the body. Most of theretinoids are in the form of retinyl esters and are confined to cyto-plasmic droplets. Preferential expression of ECM genes in stellatecells has been confirmed in mechanistically distinct experimentmodels of injury.
Recent studies have emphasized the heterogeneity of mesenchy-mal populations in the liver, with variable expression of neural,64
angiogenic,65 contractile,66 and even bone marrow-derived67
markers. Moreover, experimental genetic ‘marking’ of stellate cellsby the expression of fluorescent proteins downstream of eitherfibrogenic or contractile gene promoters illustrates the plasticity offibrogenic populations in vivo.68 In view of this capacity for ‘trans-differentiation’ between different mesenchymal cell lineages, andpossibly even from epithelium,69 the key issue is whether fibrogeniccells express target molecules such as receptors or cytokines in suf-ficient concentrations in vivo to merit their targeting by diagnosticagents or antifibrotic compounds.
Following liver injury of any etiology, stellate cells undergo aprocess known as ‘activation’, which is characterized by the transi-tion of quiescent vitamin A-rich cells into proliferative, fibrogenic,and contractile myofibroblasts.54 Stellate cell activation is typicallya result of complex interplay among ECM (Figure 6.2) and cellular(Figure 6.3) elements found in the local environment. It should benoted that activation most often occurs in the setting of hepatocel-lular injury and subsequent inflammation. Activation can be con-ceptually viewed as a two-stage process: initiation (also referred toas ‘preinflammatory’) and perpetuation54 (Figure 6-4). Initiationrefers to early changes in gene expression and phenotype that renderthe cells responsive to other cytokines and stimuli, whereas perpet-uation results from the effects of these stimuli on maintaining theactivated phenotype and generating fibrosis. Initiation is largely dueto paracrine stimulation, whereas perpetuation involves autocrine aswell as paracrine loops.
92
Inciting injury
Recruitment of inflammatory cells
T-cell
NK cell
Hepatocyte
Activated stellate cell
Expression of cytokines
Kupffer cell
Stellate cell
Stellate cell activation
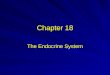
Figure 6-3. Cellular response to wound healing.Most forms of liver injury result in hepatocyte injuryfollowed by inflammation, which in turn leads toactivation of hepatic stellate cells. Inflammatoryeffectors are multiple and include T cells, NK and NKT cells as well as Kupffer cells. These cells produce growth factors, cytokines, andchemokines that play an important role in stellatecell activation. Additionally, injury leads to disrup-tion of the normal cellular environment, and also tostellate cell activation (right upper panel). Onceactivated, stellate cells themselves produce avariety of compounds, including growth factors,cytokines, chemokines, and vasoactive peptides.These substances have pleotropic effects in thelocal environment, including many which haveautocrine effects on stellate cells themselves. Oneof the major results of stellate cell activation isextracellular matrix synthesis, as well as the pro-duction of matrix degrading enzymes.
Ch006-X2998.qxd 3/15/06 5:21 PM Page 92

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
93
InitiationOxidant stress may be an early determinant of stellate cell activa-tion. In hepatic injury, whether subclinical or overt, there is a per-turbation of normal liver homeostasis, with extracellular release ofeither free radicals (i.e. ‘oxidant stress’), intracellular constituents,and/or cytokines and signaling molecules. Sources of these media-tors may be circulating (i.e. endocrine), paracrine or autocrine. Inparticular, oxidant stress-mediated necrosis leading to stellate cellactivation may underlie a variety of liver diseases, includinghemachromatosis, alcoholic liver disease, viral hepatitis and non-alcoholic steatohepatitis (NASH).55,70,71 Liver injury is typically asso-ciated with infiltration of inflammatory cells, but even in theirabsence the liver contains sufficient resident macrophages (Kupffercells) and natural killer cells (pit cells) to initiate local inflammationprior to the arrival of extrahepatic cells. In addition to oxidant stress,following early injury endothelial cells produce a splice variant ofcellular fibronectin that is able to stimulate stellate activation.
Endothelial cells in early injury may also participate in the conver-sion of latent TGF-b1 to its active, profibrogenic form through theactivation of plasmin.
Whereas necrosis is considered a classic inflammatory and fibro-genic stimulus, recent findings also suggest that apoptosis mayprovoke a fibrogenic response in stellate cells. Apoptotic fragmentsreleased from hepatocytes are fibrogenic towards cultured stellatecells,72 and Fas-mediated hepatocyte apoptosis in vivo in experi-mental animals is also fibrogenic.73
Platelets in injured liver are a potent source of paracrine stimuliby generating multiple potentially important mediators, includingPDGF, TGF-b1, and epidermal growth factor (EGF). Additionally,activated stellate cells have also been observed in primary andmetastatic human tumors, as well as a murine model of metastaticmelanoma to liver.74
In recent years, increasing interest has been focused on the molec-ular regulation of gene expression during early stellate cell activa-
PROLIFERATION CONTRACTILITY
PERPETUATION
INITIATION
RESOLUTION
REVERSION?
APOPTOSIS
LEUKOCYTE CHEMOTAXIS
MCP-1
PDGF
PDGF
TGF-β1
MMP-2
ET-1
PDGF MCP-1
RETINOID LOSS
CHEMOTAXIS
MATRIX DEGRADATION
FIBROGENESIS
Figure 6-4. Stellate cell activation. Stellate cell activation is a key pathogenic feature underlying liver fibrosis and cirrhosis. Multiple and varied stimuli contributeto the induction and maintenance of activation, including (but not limited to) cytokines, peptides, and the extracellular matrix itself. Key phenotypic features ofactivation include the production of extracellular matrix, loss of retinoids, proliferation, of up-regulation of smooth muscle proteins, secretion of peptides andcytokines (which have autocrine effects), and up-regulation of various cytokine and peptide receptors. Reprinted with permission from ref 54a.
Ch006-X2998.qxd 3/15/06 5:21 PM Page 93

Section I. Pathophysiology of the Liver
tion. There have been many advances in dissecting pathways ofmembrane and intracellular signaling and transcriptional gene regu-lation in activated hepatic stellate cells that are too numerous todetail here.75 A growing number of transcription factors may regu-late stellate cell behavior, including peroxisomal proliferator-acti-vated receptors (PPAR) a, b and g,76 retinoid receptors,77 NF-kB,78,79
Jun D,75 Krüppel-like factor 6 (previously called ‘Zf9’),80 Foxf1,81
and CRP282 among others.
PerpetuationAfter initiation, activated stellate cells undergo a series of pheno-typic changes that collectively lead to the accumulation of ECM.These include proliferation; contractility; fibrogenesis; chemotaxis;matrix degradation; retinoid loss; and proinflammatory responsesand cytokine release. The following sections detail the mechanismsunderlying each of these events.
ProliferationAn increase in the number of stellate cells has been documentedafter both human and experimental liver injury, in large part due tolocal proliferation. Following liver injury, many mitogenic factors as well as their cognate tyrosine kinase receptors are unregulated,primariliy through receptor tyrosine kinases.59 PDGF is the best-characterized and most potent mitogen towards stellate cells. Up-regulation of PDGF receptor following liver injury enhances theresponsiveness to autocrine PDGF, whose expression is alsoincreased. The downstream signaling pathways involve ERK/MAPkinase, phosphoinositol 3 kinase (PI 3-kinase) and STAT-1 (signaltransducers and activators of transcription) (see 3 for review).PDGF-induced proliferation correlates with increased intracellularCa2+ and pH, raising the possibility that calcium channel blockersmight modulate stellate cell mitogenesis or activation. Other stellate cell mitogens include endothelin-1 (ET-1),83,84 thrombin,85
FGF,86 and IGF,87,88 among others (see 89,90 for reviews). A recentstudy has documented increased sensitivity to ET-1 during activa-tion,91 suggesting potentiation of autocrine/paracrine stimulation.
ContractilityContraction by stellate cells may be a major determinant of earlyand late increases in portal resistance during liver fibrosis. Activatedstellate cells impede hepatic blood flow both by constricting individual sinusoids and by contracting the cirrhotic liver, as the col-lagenous bands typical of end-stage cirrhosis contain large numbersof activated stellate cells (see 66 for review). A key contractile stimulus towards stellate cells is ET-1.66 Other contractile agonistsinclude arginine vasopressin, adrenomedullin, and eicosanoids.66
The regulation of stellate cell contraction is complex. Theendothelium-derived relaxing factor nitric oxide (NO) appears to bean important relaxing factor in the sinusoid (although other factors,such as carbon monoxide, also play a role). The net contractile activ-ity of stellate cells in vivo therefore reflects the relative strength ofeach of these opposing activities. Current evidence suggests thatintrahepatic portal hypertension probably results from diminishedNO (and/or other vasodilators) activity as well as increased stimu-lation by ET-1 (or other constrictors).66
The expression of smooth muscle a actin is increased during stellate cell activation. ET-1 and other vasoactive mediators increasetheir expression.83 Thus studies of contractile proteins in stellatecells may yield a therapeutic target for the treatment of intrahepaticportal hypertension.
FibrogenesisFibrogenesis is perhaps the key component of the stellate cell’s con-tribution to hepatic fibrosis. TGF-b1 is the most potent fibrogenicfactor, with some fibrogenic activity documented for interleukin-1b,TNF, lipid peroxides, acetaldehyde, and others (see 2,6 for reviews).
Because of its importance, TGF-b1 regulation has received con-siderable attention. TGF-b1 is up-regulated in experimental andhuman hepatic fibrosis. Although sources of this cytokine are many,autocrine expression is among the most important (see 2 for review).Several mechanisms underlie the increase in TGF-b1 expression bystellate cells during liver injury, including TGF-b transcriptional up-regulation, activation of latent TGF-b1, increased TGF-b receptorexpression, and up-regulation of TGF-b signaling components.92–96
ChemotaxisStellate cells may accumulate both through proliferation and viadirected migration into regions of injury, or chemotaxis. PDGF, the leukocyte chemoattractant MCP-1, and a growing family ofchemokines have been identified as key stellate cell chemoattrac-tants.97 In addition to tyrosine kinase receptors, new agents havebeen implicated in stellate cell migration, in particular tetraspaninreceptors.3,62
Matrix DegradationA greater understanding of matrix degradation in liver is emerging.Quantitative and qualitative changes in the activity of MMPs andtheir inhibitors play a vital role in extracellular matrix remodelingin liver fibrogenesis (see ECM in the normal and fibrotic liver and Figure 6.2 above). As noted above, the net effect of changes in matrix degradation is the conversion of the low-density sub-endothelial matrix to one rich in interstitial collagens.
Retinoid LossStellate cell activation is accompanied by loss of their characteristicperinuclear retinoid (vitamin A) droplets. Although the intracellu-lar form is largely retinyl esters, when retinol is exported from thecell during activation it is primarily as retinol, suggesting the possi-bility of intracellular hydrolysis of esters before being exported.Several nuclear retinoid receptors that bind intracellular retinoidligands have been identified and their effects characterized in stellate cells.77,98
Proinflammatory Responses and Cytokine ReleaseHepatic stellate cells and sinusoidal endothelial cells have emergedas inflammatory effectors. Sinusoidal endothelial cells, normally fenestrated to allow rapid bidirectional transport of solutes betweensinusoidal blood and parenchymal cells, may rapidly lose their fenestrations upon injury and express proinflammatory molecules,including ICAM-1, VEGF and adhesion molecules.74,99 Togetherwith stellate cells, they activate angiogenic pathways in response tohypoxia associated with local injury or malignancy.74,97,100,101
94
Ch006-X2998.qxd 3/15/06 5:21 PM Page 94

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
Key inflammatory pathways converge on stellate cells, leading tofibrosis (see Figure 6-3). Thus, the cell type is a central mediator ininflammation, rather than just a passive target. Upon activation, theyrelease chemokines97,102 and other leukocyte chemoattractants, proteinase-activated receptors,103 and up-regulate expression of keyinflammatory receptors, including ICAM-1,104 chemokine recep-tors,105 and those mediating lipopolysaccharide (LPS) signaling,including Toll-like receptor 4.78 Stellate cells may also contribute tointrahepatic apoptosis of T lymphocytes.106
Remarkably, little attention has focused on the contribution of different lymphocyte subsets to hepatic fibrogenesis. Interest hasincreased recently, in part because of the observation that patientswith HCV who are co-infected with HIV, as well as those who areimmunosuppressed following liver transplantation, have acceleratedfibrosis rates, implicating the immune system as a determinant offibrogenesis. These observations have been supported by animalstudies demonstrating that the immune phenotype regulates fibro-genesis independent of effects on injury, which in turn have led toefforts to map the genetic loci accounting for these differences.22
Most recently, CD8 lymphocytes have emerged as potential pro-fibrogenic cells, based on their ability to induce early fibrogenesis following adoptive transfer to naïve SCID mice from animals withliver injury.107
Autocrine cytokines play vital roles in regulating the activationprocess of stellate cells. These cytokines include TGF-b1, PDGF,FGF, HGF, PAF, stem cell factor and ET-1, among others.59,90,97,108
Furthermore, stellate cells release neutrophil and monocytechemoattractants, which can amplify inflammation in liver injury.These chemokines include colony-stimulating factor, monocytechemotactic protein-1 (MCP-1), and cytokine-induced neutrophilchemoattractant (CINC).97
Anti-inflammatory cytokines produced by stellate cells have alsobeen identified. Up-regulation of interleukin-10 (IL-10) occurs inearly stellate cell activation. The anti-inflammatory effects of thiscytokine are demonstrated by its ability to down-regulate TNF-aproduction from macrophages. Knockout mice lacking IL-10 havemore severe hepatic fibrosis following CCl4 administration, andtransgenic mice expressing IL-10 in liver have reduced fibrosis.107
Based on the consistent antifibrotic effect of IL-10 in experimentalliver disease, a clinical trial was undertaken which failed to show anantifibrotic effect in patients with HCV infection, possibly becauseof marked increases in HCV replication109 (see Therapy of hepaticfibrosis, below).
DISEASE-SPECIFIC MECHANISMS REGULATINGHEPATIC FIBROSIS – HCV AND NASHIn addition to generic mechanisms of fibrogenesis common to allexperimental and human liver disease, there has been progress inelucidating disease-specific mechanisms, in particular in hepatitis C(HCV) and NASH (non-alcoholic steatohepatitis). In HCV, stellatecells might be infectable by the virus because they express putativeHCV receptors.104,110 Moreover, adenoviral transduction of HCVnon-structural and core proteins induces stellate cell proliferationand the release of inflammatory signals.104 In HCV-infected liverchemokines and their receptors are up-regulated, stimulating lym-phocyte recruitment.111 HCV proteins may also interact directlywith sinusoidal endothelium.112
The increasing prevalence of obesity in the US and westernEurope is associated with an alarming increase in NASH,39 leadingto advanced fibrosis and cirrhosis. Leptin, a circulating adipogenichormone that is proportionate to adipose mass in circulating blood,has been clearly linked to stellate cell fibrogenesis.113–115 Sources arelikely to be both endocrine and autocrine, associated with enhancedsignaling through the leptin receptor, which is up-regulated duringstellate cell activation.113 Concurrently, down-regulation of adipo-nectin, a counterregulatory hormone, in obesity may amplify thefibrogenic activity of leptin. This possibility is supported by findingsin mice lacking adiponectin, which have enhanced fibrosis followingtoxic liver injury.116
RESOLUTION OF LIVER FIBROSIS AND THE FATEOF ACTIVATED STELLATE CELLSDuring recovery from acute human and experimental liver injurythe number of activated stellate cells decreases as tissue integrity isrestored. Either reversion of stellate cell activation, or selectiveclearance of activated stellate cells by apoptosis, may explain theloss of activated cells in resolving liver injury. To date, evidence isstrongest for stellate cell apoptosis in this setting.
Apoptosis of stellate cells probably accounts for the decrease ofactivated stellate cells during resolution of hepatic fibrosis.49 Fol-lowing injury, apoptosis may be inhibited by soluble factors andmatrix components that are present during injury, whereas an apop-totic pathway otherwise represents a ‘default’ mode. Furthermore,cell death ligands, including TRAIL and fas, are expressed in liverinjury, and activated stellate cells are more susceptible to TRAIL-mediated apoptosis.73,117,118 Another death receptor, nerve growthfactor receptor (NGFR), is also expressed by activated stellate cells,and its stimulation with ligand drives apoptosis.119
Survival factors also regulate the net activity of stellate cell apop-tosis. IGF-I promotes stellate cell survival via the PI3-K/c-Aktpathway and TNF-a has the same effect, but utilizes the NF-kBpathway.120,121
Molecules regulating matrix degradation appear closely linked tosurvival and apoptosis. Active MMP2 correlates closely with apop-tosis, and in fact may be stimulated by it.122 Inhibition of MMP2activity by TIMP-1 blocks apoptosis in response to a number ofapoptotic stimuli.123
Interactions between stellate cells and the surrounding matrix alsoinfluence their propensity towards apoptosis, and this might partlyexplain the antiapoptotic activity of TIMP-1. Moreover, the fibroticmatrix may provide important survival signals to activated stellatecells. For example, animals expressing a mutant collagen I resistantto degradation have more sustained fibrosis and less stellate cellapoptosis following liver injury,48 and transgenic animals expressingTIMP-1 in liver have delayed resolution of fibrosis.124 Studies usinggliotoxin,125 a fungal toxin that induces apoptosis in stellate cells,emphasize the role of this pathway in stellate cell removal duringresolution of liver fibrosis.
It is unknown whether an activated stellate cell can revert to aquiescent state in vivo, although it has been observed in culture.When stellate cells are grown on a basement membrane substratum(Matrigel) they remain quiescent, and plating of highly activatedcells on this substratum down-regulates stellate cell activation.58,126
95
Ch006-X2998.qxd 3/15/06 5:21 PM Page 95

Section I. Pathophysiology of the Liver
METHODS TO MEASURE FIBROSISOVERVIEWMeasurement of fibrosis not only helps to stage the severity ofdisease, it allows serial determination of disease progression. Thelevel of fibrosis may play an important role in clinical managementand determine patients’ prognosis. For example, aggressive therapyis more appropriate in HCV-infected patients with advanced fibro-sis. Further, the fibrosis progression rate is an important predictorof the time to develop cirrhosis.18
It is essential to measure fibrosis accurately, given the growingprospect of antifibrotic therapies and the need to track their effi-cacy. Moreover, with growing evidence that fibrosis is reversible,methods will need to assess both progression and regression accu-rately. For example, specific therapy leads to a reduction in fibrosisin a number of diseases, including autoimmune liver disease, hepa-titis C, hepatitis B, and others.34,35,42,44,127–129
Percutaneous liver biopsy has traditionally been considered to bethe gold standard test to assess liver fibrosis. However, a variety ofnon-invasive tests have been advanced as potential alternatives tobiopsy. These include clinical signs, routine laboratory tests, quanti-tative assays of liver function, markers of extracellular matrix syn-thesis and/or degradation, and radiologic imaging studies. In additionto individual indicators of fibrosis, combination tests, and a numberof models for predicting liver fibrosis have been developed. Indi-vidual and combination tests are discussed below.
The ideal method to measure fibrosis would be simple, non-invasive, reproducible, inexpensive, accurate, and readily available.Unfortunately, none of the currently available approaches fulfills all of these criteria.
BEDSIDE DIAGNOSTIC TOOLSClinical signs and symptoms of liver disease are frequently high-lighted in assessing patients with liver disease, but these are of littlevalue in detecting early, precirrhotic stages of liver fibrosis. In con-trast, a number of clinical features can be utilized to assess whethercirrhosis with portal hypertension may be present. Signs of cirrho-sis include spider angiomata, distension of abdominal wall veins,ascites, splenomegaly, muscle wasting, Dupuytren’s contractures(especially with ethanol-associated cirrhosis), gynecomastia and tes-ticular atrophy in males, and palmar erythema. However, it is impor-tant to emphasize that even in patients with histologic cirrhosis, andin those with portal hypertension, these physical signs may not bepresent.
NON-INVASIVE MARKERS OF FIBROSISBlood-Based Markers – OverviewA wide variety of blood, serum, or plasma ‘markers’ for fibrosis havebeen proposed. There are several categories of marker or test. Forexample, some detect abnormalities in serum chemistries. Includedin these types of test are aspartate aminotransferase (AST), alanineaminotransferase (ALT), g-glutamyl transferase (GGT), bilirubin,albumin, and a2-macroglobulin, among others. Moreover, some ofthese individual tests have been incorporated into simple and/orcomplex mathematical models or algorithms (see below).
Another major category of test includes those that are basedspecifically on the pathogenesis of fibrosis (see above). For example,proteins that are produced as a result of the fibrogenic process itselfthat have been studied as markers of fibrosis include procollagen I,fibronectin, tenascin, laminin, hyaluronic acid and others. Othermarkers have included cytokines (i.e. TGF-b1), connective tissuegrowth factor (CTGF), PDGF and others, matrix degradingenzymes (i.e. TIMP1), and others (Table 6-1).
Finally, groups of tests, including those that utilize markers offibrosis in combination with each other or in combination with othertypes of test, have been advanced in an attempt to detect andmeasure fibrosis.
Ideally, a blood-based test should have both high sensitivity andhigh specificity. Many of the available tests have a high specificity(>95%) for advanced fibrosis. However, few (including algorithms)have great sensitivity to detect moderate levels of fibrosis. More-over, a serum-based assay ideally should be linear over the full rangeof fibrosis, follow the natural history, and accurately reflect theeffect of treatment.
Routine Laboratory TestsA number of studies have used routine laboratory tests in an attemptto determine whether a patient may have advanced liver disease, in particular to exclude or confirm portal hypertension and/oresophageal varices.130,131 Although tests such as the prothrombintime, albumin level, and portal vein diameter (measured by ultra-sound) have all been associated with varices, studies have beenremarkably consistent in their identification of the platelet count as
96
Table 6-1. Cytokines, Growth Factors, Peptides, Proteases, and otherComponents Important in Hepatic Fibrogenesis
Cytokines Growth factors Peptides
Transforming Transforming growth factor-b Endothelin-1growth factor-b
Transforming Transforming growth factor-a Norepinephrinegrowth factor-a
Interleukin-1 *Insulin-like growth factor (I, II) Angiotensin IIInterleukin-4 *Platelet-derived growth factor*Interleukin-6 *Fibroblast growth factorInterleukin-10 Vascular endothelial growth factorInterleukin-13 Hepatocyte growth factor*Monocyte Connective tissue growth factor
chemotactic factor
Proteases and their inhibitors MiscellaneousMatrix-metalloproteinase-1 (interstitial Thrombospondin (1,2)
collagenase) LeptinMatrix-metalloproteinase-2 (gelatinase A) Activin AMatrix-metalloproteinase-3 (stromelysin-1) *ThrombinMatrix-metalloproteinase-7 (matrilysin) OsteopontinMatrix-metalloproteinase-8Matrix-metalloproteinase-9 (gelatinase B)Matrix-metalloproteinase-10 (stromelysin-2)Tissue inhibitor of metalloproteinase-1
Agents may have direct effects on hepatic stellate cells, or indirect effects in the woundingenvironment.*Compounds whose effect is largely via stimulation of proliferation.
Ch006-X2998.qxd 3/15/06 5:21 PM Page 96

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
the best single predictor of esophageal varices. For example, in onestudy, cirrhotics without splenomegaly on physical examination andwith a platelet count >88000/mm3 had a risk of large esophagealvarices of 7.2%, whereas the risk was 28% if the platelet count wasless than 88000/mm3.130
An AST/ALT ratio >1 has been proposed to indicate the presenceof cirrhosis.132 In one study of patients with HCV, a ratio >1 had100% specificity and positive predictive value for distinguishing cir-rhotic from non-cirrhotic patients, with a 53.2% sensitivity and80.7% negative predictive value.133 In addition, the ratio correlatedpositively with the stage of fibrosis, but not with the grade of activ-ity or other biochemical indices. Of cirrhotic patients, 17% had noclinical or biochemical evidence of chronic liver disease except foran elevated AST/ALT ratio. In another study, the AST/ALT ratiohad 81.3% sensitivity and 55.3% specificity in identifying cirrhoticpatients who died within 1 year of follow-up.132,134
In a further attempt to develop non-invasive tools for the meas-urement of liver fibrosis, Forns and coworkers developed a modelusing data from HCV patients that included age, GGT, cholesterol,and platelet count.135 This model was developed with the intentionto differentiate patients with significant fibrosis from those without.The sensitivity for detecting METAVIR F2–F4 fibrosis was 94%, andthe presence of significant F2–F4 fibrosis could be excluded withhigh accuracy (negative predictive value of 96%).135
Likewise, Wai et al.136 constructed a simple model utilizing routinelaboratory data (Table 6-2). The authors devised a novel index,termed the AST to platelet ratio index, or APRI, which is the ASTlevel/upper limit of normal (ULN) divided by the platelet count(109/l) multiplied by 100. The sensitivity and specificity for fibro-sis of the APRI value depended on the cut-offs used. Using an APRIvalue of 1.50, the positive and negative predictive values for signif-icant fibrosis (Ishak score = 3) were 91% and 65%, respectively,whereas for cirrhosis and an APRI of 2.00, the positive and negativepredictive values were 65% and 95%, respectively. Thus for a hypo-thetical patient, if the AST was 90 IU/l (and the ULN 45) andplatelet count was 100 ¥ 109/l, then the APRI would be 2.00. Thismeans that the patient has essentially a 90% chance of having sig-nificant fibrosis, and somewhat less likelihood of having cirrhosis.However, cirrhosis could not be excluded with certainty. Althoughthe APRI is attractive because of its simplicity, it can neither defin-itively diagnose nor exclude cirrhosis, and it will not identify patientswith early fibrosis.
Other simple quantitative systems based on routine laboratoryvalues have been developed. One early example was the ‘PGAindex’, which combined prothrombin time, GGT and apolipo-protein A1 (Table 6-2); this test was examined in patients with alcoholic cirrhosis.137 The diagnostic accuracy of this index was laterimproved by the addition of a2-macroglobulin (and hence termedthe ‘PGAA index’).138 The test characteristics of many of these indirect assays have been derived from datasets, but have not beenvalidated on independent datasets.
More complicated algorithms based on commonly available labo-ratory tests include the ‘Fibrotest,’ reported by the French MUL-TIVIRC group.25 This group used mathematical modeling to developan algorithm including five different markers to predict fibrosis (the markers selected were a2-macroglobulin, haptoglobin, GGT,apolipoprotein A1, and total bilirubin). This index predicted a spe-
cific biopsy category in 46% of patients139 and has been validated ina number of hepatitis C patient cohorts, having been found to havean area under the receiver operator characteristic (AUROC) curveof 0.73–0.87.140 The addition of ALT to the marker panel allows forprediction of METAVIR necroinflammatory activity.140 The panelhas also been examined in other liver disease cohorts.141,142 Limita-tions of this panel in fibrosis include false positive results due toincreases in bilirubin or decreases in haptoglobin, for example fromhemolysis secondary to ribavirin therapy. Likewise, false positiveresults may also occur in situations where there is hyperbilirubine-mia, such as Gilbert’s disease and cholestasis. Acute inflammationmay also affect the results of the test owing to changes in a2-macroglobulin or increases in haptoglobin. Currently, it is unclearwhether the ‘fibrotest’ assay meets sufficiently rigorous criteria,given a predictive value of only 46%, for routine clinical use.
Tests Using Extracellular Matrix/Fibrosis MarkersAnalyses of serum markers of extracellular matrix/fibrosis includemany proteins important in fibrogenesis, ECM constituents (i.e.fibronectin, collagen I, collagen IV, collagen VI, amino terminalpropeptide of type III collagen (PIIINP), tenascin, and hyaluronicacid, metalloproteinases (including many of those listed in Table 6-1), inhibitors of matrix metalloproteinases (i.e. TIMP-1, TIMP-2),and other proteins, peptides, and cytokines, as highlighted in Table 6-1. Although many tests have been studied individually, theyare generally not sensitive for detection of fibrosis143,144 (see 145 forreview).
Tests Using Combinations of Extracellular Matrixand/or Routine MarkersA combination test including hyaluronic acid, TIMP1, and a2-macroglobulin was examined in a cohort of 294 patients with HCVinfection and subsequently validated in a second cohort of 402patients146 (‘Fibrospect’, Table 6-2). This had a combined AUROCof 0.831 for METAVIR F2–F4 fibrosis. The positive and negativepredictive values were 74.3% and 75.8%, respectively, with an accu-racy of 75%. This three-marker panel thus may help differentiate
97
Table 6-2. Combined Panels of Blood Markers used to Detect Liver Fibrosis
Panel Components References
AST/ALT AST/ALT 132–134§Forns Platelets, GGT, cholesterol 135APRI AST, Platelets 136 PGA index Platelets, GGT, apolipoprotein A 137–138Fibrotest GGT, haptoglobin, bilirubin,
apolipoprotein A, a2-macroglobulin 25, 139–142Fibrospect Hyaluronic acid, TIMP-1, a2-macroglobulin 146*ELF ECM proteins 147FPI AST, cholesterol, HOMA-IR
ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, g-glutamyltranspeptidase; APRI, AST to platelet ratio index; TIMP-1, tissue inhibitor of metallopro-teinase 1; ECM, extracellular matrix; ELF, European liver fibrosis; FPI, fibrosis probabilityindex; HOMA-IR, insulin resistance by the homeostasis model assessment.§Also includes age in the panel.*Components tested include collagen IV, collagen VI, amino terminal propeptide of typeIII collagen (PIIINP), matrix metalloproteinase 2 (MMP-2), matrix metalloproteinase 9(MMP-9), tissue inhibitor of matrix metalloproteinase 1 (TIMP-1), tenascin, laminin, andhyaluronic acid (HA).
Ch006-X2998.qxd 3/15/06 5:21 PM Page 97

Section I. Pathophysiology of the Liver
patients with HCV infection with moderate/severe fibrosis fromthose with no/mild fibrosis, although it was not possible to differ-entiate specific stages accurately.
Another combination test was developed by the European LiverFibrosis (ELF) Study Group.147 This group examined collagen IV,collagen VI, PIIINP, matrix metalloproteinase 2 (MMP-2), matrixmetalloproteinase 9 (MMP-9), TIMP-1, tenascin, laminin, andhyaluronic acid (HA). The study was unique in that it examinedpatients with a wide variety of liver diseases, including those withchronic hepatitis C virus infection (n = 496), alcoholic liver disease(n = 64), non-alcoholic fatty liver disease (n = 61), chronic hepati-tis B virus infection (n = 61), primary biliary cirrhosis or primarysclerosing cholangitis (n = 53), recurrent liver disease post ortho-topic liver transplantation (n = 48), autoimmune hepatitis (n = 45),hemochromatosis (n = 32), cryptogenic cirrhosis (n = 19), both hep-atitis B and C (n = 4), and other or no known diagnosis (n = 138);the cohort also had a wide distribution of fibrosis stages (Scheuerfibrosis stages were as follows: stage 0 = 24.6%; stage 1 = 35.5%;stage 2 = 13.4%; stage 3 = 14.9%; and stage 4 = 11.8%). An algo-rithm was developed that detected the upper third of fibrosis groups(Scheuer stages 2, 3, and 4) with a sensitivity of 90% and accuratelydetected the absence of fibrosis (Scheuer stages 0, 1), with a nega-tive predictive value for this level of fibrosis of 92%. The AUC of areceiver operating characteristic (ROC) plot was 0.804. Interest-ingly, the addition of clinical chemistry tests including liver functiontests, or hematological indices including platelet count and prothrombin time, did not improve test performance. The testappeared to be best in patients with hepatitis C, non-alcoholic fattyliver disease and alcoholic liver disease. The inclusion of patientswith multiple etiologies of liver disease, although appealing, has the potential to limit the accuracy of these and other panels, as thecharacteristics of specific assays may be disease specific.
Another model, including AST, cholesterol, and insulin resistance(as well as age and an estimate of past alcohol intake) in patientswith HCV147a found that the sensitivity for detection of advancedfibrosis depended on the index value used. At a low probabilityindex, the sensitivity for predicting significant fibrosis was high, butspecificity was low, while at a high probability index, sensitivity forsignificant fibrosis was low, but specificity was high.
ProteomicsWith the recent explosion in proteomics, proteomic approacheshave attempted to identify unique protein fingerprints in patientswith liver disease. Various platforms are available, including thosethat measure protein expression, protein–protein interactions, oreven enzymatic activity. The majority of approaches have used high-throughput technologies to identify novel protein expression pat-terns. For example, a recent study in 46 patients with chronichepatitis B identified 30 proteomic features predictive of significantfibrosis (Ishak stage = 3) and cirrhosis. The AUROC for this analy-sis was 0.906 and 0.921, for advanced fibrosis and cirrhosis, respec-tively.148 Another study in 193 patients with chronic hepatitis Cidentified eight peaks that differentiated METAVIR fibrosis stageswith an AUROC of 0.88; this was compared to an AUROC 0.81for the Fibrotest.149 Another report in patients with HCV fibrosisidentified several serum proteins to be differentially regulated.150 In
this study, patients with advanced fibrosis had elevated levels of a2-macroglobulin, haptoglobin, and albumin, but apolipoprotein AI,apolipoprotein A-IV, complement C4, and serum retinol-bindingprotein were reduced.
Another approach has included measurement of labeled N-glycans found in serum.151 The technique exploits the ability toanalyze the desialylated total serum N-glycome on a DNA analyzer.The authors focused on cirrhosis (primarily ethanol induced),demonstrating unique patterns of serum N-glycans in those with cirrhosis compared to those with chronic liver disease alone. It waspostulated that in cirrhotic livers characteristic N-glycans with abisecting GlcNAc residue were prominent. In normal liver, theenzyme responsible for this modification, N-acetylglucosaminyltransferase III (GnT-III), is found only in non-parenchymal cells,but in regenerating liver (two-thirds partial hepatectomy) thisenzyme is produced in hepatocytes. Thus, GnT-III expression is pre-sumably a manifestation of hepatocellular regeneration, reflected byregenerative nodules. This approach was most sensitive for thedetection of cirrhosis and was also able to exclude cirrhosis withgreat accuracy. When combined with the commercially availableFibrotest this test had 100% specificity and 75% sensitivity for diag-nosing compensated cirrhosis.151
Summary of Blood-based MarkersA key advantage of serum markers to detect fibrosis is their non-invasiveness. Additionally, it has been argued that serum markersovercome sampling problems associated with liver biopsy. However,these approaches have several drawbacks. First, most of the studiesexamining serum markers have been performed in cohorts ofpatients that have been biased toward advanced fibrosis/cirrhosis. Afurther problem is that the currently proposed serum marker algo-rithms use dichotomous rather than continuous scales. The dichoto-mous nature of these variables would be less problematic if therewere clear clinical associations, for example if prognosis or treat-ment response were highly linked to stage 0–1 versus stages 2–4. Inthe absence of clinical correlates between dichotomous variables andoutcomes, it remains important to diagnose the different stages offibrosis accurately (0–4). Unfortunately, current tests and algo-rithms are unable to do this, and perhaps most importantly, the testsdo not differentiate between intermediate levels of fibrosis. Thus,although assessments of fibrosis with approaches that use serummarkers have great appeal, and indeed, in some areas the tests havebegun to replace liver biopsy. Further investigation is required tooptimize these tests.
Imaging TestsA wide variety of radiographic tests have been used to image patientswith fibrosis/cirrhosis. Included in this group are ultrasound, CT,and MRI. In general, these tests are capable of detecting evidenceof portal hypertension, thus they have the ability to detect advanceddisease. As currently used in clinical practice, however, they areinsensitive for the detection of moderate degrees of fibrosis.
Transient elastography, which uses pulse-echo ultrasound acquisi-tions to measure liver stiffness and predict fibrosis stage, has gainedinterest as a method to quantify fibrosis as it appears that liver ‘stiff-ness’ may accompany the fibrogenic response.152 In a prospectivemulticenter study of 327 chronic HCV patients, the AUROCs for
98
Ch006-X2998.qxd 3/15/06 5:21 PM Page 98

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
METAVIR stage F2–F4 and cirrhosis were 0.79 and 0.97, respec-tively.153 In a separate study of 183 chronic HCV patients, transientelastography compared favorably with the Fibrotest and APRI(AUROC for F2–F4 = 0.83, 0.85 and 0.78, for transient transientelastography, Fibrotest and APRI, respectively).154 When transientelastography was combined with the Fibrotest, the predictive valuefor fibrosis stage F2–F4 was improved, with an AUROC of 0.88.154
Transient elastography (Fibroscan) reportedly offers good repro-ducibility with low inter- and intraobserver variability. The proce-dure is performed by obtaining multiple validated measurements ineach patient, further reducing the potential for sampling errors. Thedepth of measurement from the skin surface is between 25 and65mm, raising the possibility that this technique may be difficult touse in obese patients or those with ascites. However, newer probesare being developed for obese patients, and further investigation isexpected.
Finally, it would theoretically be desirable to utilize advances inthe molecular understanding of liver fibrosis to image the liver. Forexample, the number of activated stellate cells, which reflect fibro-genic activity, might be identified by tagging them with cell-specificmarkers.155 Alternatively, matrix or matrix turnover could be labeledusing molecular tools. Although such approaches are appealing, theyremain experimental at present.
Tests of Liver FunctionA variety of bona fide liver function tests have been used to assessliver fibrosis and cirrhosis. Such tests generally measure advanceddisease and several depend on perfusion, such as indocyanine green,sorbitol and galactose clearance tests, or tests such as the 13C–galactose breath test and the 13C–aminopyrine breath test thatdepend on the functional capacity of the liver.156–158 Another test,the MEGX test, which measures monoethylglycinexylidide(MEGX) formation after the administration of lidocaine, dependsupon the activity hepatic cytochrome P450 3A4 isoenzyme (whichcatalyzes oxidative N-de-ethylation of lidocaine to MEGX.159 TheMEGX test has a sensitivity and specificity in the 80% range for distinguishing chronic hepatitis from cirrhosis in comparison to standard liver tests.159 Unfortunately, although the MEGX test andother function tests may predict prognosis in cirrhotic patients, theyare insensitive for quantifying fibrosis in patients with less advanceddisease.156–158
Liver BiopsyPercutaneous liver biopsy has traditionally been considered to be thegold standard test to measure fibrosis. Although there is great expe-rience with liver biopsy, this procedure is time consuming, incon-venient, uncomfortable, invasive, and makes both patients andphysicians anxious. Further, liver biopsy can be associated with sub-stantial sampling-error (see Chapter 12 for further details aboutliver biopsy). In a recent study in which 124 patients with chronicHCV infection underwent laparoscopy-guided biopsy of each theright and left hepatic lobes, 33.1% had a difference of at least onehistologic stage (modified Scheuer system) between the twolobes.160 Furthermore, in 18 study subjects a stage consistent withcirrhosis was found in one lobe, whereas stage 3 fibrosis was reported
in the other. Finally, in 10% of subjects, stage 0–2 disease was identified in one lobe and stage 3–4 fibrosis was found in the other.Similar variability was reported in another study in patients withfatty liver disease.161
There are several other limitations of liver biopsy. Quantificationof fibrosis in biopsies is subject to significant interobserver variation.In chronic hepatitis C, for example, standardized grading systems,including Knodell, METAVIR, Scheuer or Ishak, are concordant inonly 70–80% of samples. Specimen quality is very important, withsmaller samples leading to an underestimation of disease severity.162
A recent study created digitized virtual image biopsy specimens ofvarying length from large liver sections, and revealed that 75% of25-mm biopsy specimens were correctly classified using theMETAVIR staging system, compared to only 65% for biopsies15mm long.163 Interestingly, a recent study noted that the experi-ence of the pathologist may have more influence on interobserveragreement than specimen length.164
Another major problem with using liver biopsy or serum markersto quantify fibrosis is that all of the currently utilized gradingsystems use a simple linear numerical scoring approach, implyingthat they represent linear changes in fibrosis content. Such an infer-ence is highly inaccurate, as METAVIR stage 4 fibrosis does not represent twice as much fibrosis as stage 2, but rather a 5–20-folddifference.
TREATMENT OF FIBROSISSpecific therapy for the treatment of liver fibrosis is attractivebecause the scarring response leads to many if not all of the com-plications of chronic liver disease, in particular impaired syntheticfunction, liver failure, and perhaps hepatocellular cancer. Fibrosis,particularly in its advanced stages, may also contribute to portalhypertension, by preventing blood flow through fibrotic nodules.Although attempts have been made previously to treat specificallythe ‘fibrosis’ component of liver disease, these approaches have gen-erally been unsuccessful. Thus, there remains a major unmet needfor novel and effective antifibrotic therapy. Advances in elucidatingthe pathogenesis of fibrosis have led to renewed efforts in this area.Additionally, data indicating that fibrosis is reversible have helpedfuel this effort (Figure 6.5).
Although fibrosis is commonly accepted as the precursor to cirrhosis, it is not clear that mortality risk increases directly with thestage of fibrosis, until the patient actually becomes cirrhotic. Evenwith established cirrhosis, in a cohort of patients with chronic HCVinfection Fattovich and colleagues demonstrated that complicationsof cirrhosis developed over prolonged periods, and only when com-plications occurred was mortality increased.7
The most effective ‘antifibrotic’ therapies are currently those thattreat or remove the underlying stimulus to fibrogenesis (Table 6-3).In addition, preclinical and human clinical studies have highlighteda number of therapies that may abrogate fibrogenesis without affect-ing the underlying disease, by targeting specific steps in the fibro-genic response. Anti-inflammatory therapies have been based on theknowledge that inflammation drives the fibrogenic cascade. Othertreatments have attempted to inhibit cellular injury or focused onstellate cell activation, whereas others have targeted collagen syn-
99
Ch006-X2998.qxd 3/15/06 5:21 PM Page 99

Section I. Pathophysiology of the Liver
thesis and matrix deposition. The following section highlightshuman studies in these areas.
THERAPIES DIRECTED AT THE UNDERLYING DISEASEIn many forms of liver disease treatment of the underlying incitinglesion leads to an improvement in fibrosis (Table 6-4). For example,eradication or inhibition of HBV33,34,129 or HCV replication42 leadsto reversion of fibrosis, even in patients with histological cirrhosis.Fibrosis reverts in patients with hemochromatosis during iron deple-tion,165,166 after corticosteroid therapy in autoimmune hepatitis,165,166
and in patients with secondary biliary cirrhosis after decompressionof bile duct obstruction.43 In a preliminary report in patients withnon-alcoholic steatohepatitis (NASH) treated with the peroxisomalproliferator active receptor (PPAR)-g agonist rosiglitazone bothsteatosis and fibrosis were reduced.167
ANTI-INFLAMMATORY COMPOUNDSMany liver diseases, such as HCV disease, have an important inflam-matory component. Inflammation in these disorders typically drivesstellate cell activation and fibrogenesis, and it is these diseases inparticular that have been studied in order to evaluate the efficacyof anti-inflammatory drugs.
CorticosteroidsClassic examples of the benefits of steroids include autoimmunehepatitis and alcoholic hepatitis. In patients with autoimmune hep-
atitis who respond to medical treatment (prednisone or equivalent)advanced fibrosis and cirrhosis are reversible.44 Fibrosis may improvein patients with alcoholic liver disease who respond to corticos-teroids.168,169 Thus, corticosteroids appear to have antifibrotic effectsin patients with certain liver disorders.
Interleukin-10 (IL-10)Interleukin (IL)-10 has both anti-inflammatory and immunosup-pressive effects. IL-10 has been shown to reduce the production ofproinflammatory cytokines, such as TNF-a, IL-1, interferon-g, andIL-2 from T cells. These cytokines belong to the Th1 family. Endoge-nous IL-10 reduces the intrahepatic inflammatory response, shiftsthe cytokine milieu towards a Th2 predominance, and reduces fibro-sis in several in vivo models of liver injury.170 It was hypothesizedthat in vivo administration of IL-10 in patients with hepatitis C virusinfection may have an anti-inflammatory and hence an antifibroticeffect.109 Therefore, 30 patients with advanced HCV-mediatedfibrosis who had failed standard interferon-a-based antiviral therapywere enrolled in a 12-month treatment trial of IL-10 given daily orthrice weekly subcutaneously. In 13 of 28 of these patients thehepatic inflammation score decreased by at least two points (Ishakscore) and 11 of 28 had a reduction in fibrosis score (mean changefrom 5.0 ± 0.2 to 4.5 ± 0.3, p < 0.05). However, serum HCV RNAlevels increased during therapy (mean HCV RNA at day 0: 12.3 ±3.0 mEq/ml; and at 12 months: 38 mEq/ml; p < 0.05). Changes inliver histology and HCV RNA levels were accompanied by an appar-ent shift in toward a Th2-predominant lymphocyte phenotype, as had been originally hypothesized. Long-term therapy with
100
Table 6-3. Approaches to Treat Liver Fibrosis
Approach Example
Remove injurious agent Eradication of HBVAnti-inflammatory agents Corticosteroids in AIHAntioxidants PPC in alcoholic hepatitisCytoprotective agents Ursodeoxycholic acid Inhibit stellate cell activation Interferon-gInhibit stellate cell activation Colchicine
phenotypes (fibrogenesis)
Note: some approaches have not been demonstrated to be successful.AIH, autoimmune hepatitis; PPC, polyenylphosphatidylcholine.
Table 6-4. Diseases and Therapies in which there is Strong Evidence thatTreatment Reduces Liver Fibrosis
Disease Therapy References
Hepatitis B Lamivudine 33–35,129Hepatitis C Interferon-a* 42Bile duct obstruction Surgical decompression 43Autoimmune hepatitis Corticosteroids 44Hemochromatosis Iron depletion 165,166Alcoholic hepatitis Corticosteroids 168,169
*or PEG-interferon-a, with or without ribavirin.MTX, methotrexate; PPAR, peroxisomal proliferator-activated receptor.
A
B
C
Inset in A
Figure 6-5. Reversal of fibrosis. An example ofreversal of advanced fibrosis (cirrhosis in this situa-tion) is depicted. A liver biopsy prior to lamivudinetreatment is shown (upper panel and left panel).After treatment with lamivudine, liver biopsy wasrepeated and reveals almost complete dissolutionof fibrosis. Data similar to these have been pub-lished in autoimmune liver disease, hepatitis C, alco-holic hepatitis, hepatitis B, and others. (Reprintedwith permission, Wanless, et al: Arch Pathol Lab Med2001;124:1599–1607.)
Ch006-X2998.qxd 3/15/06 5:21 PM Page 100

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
IL-10 decreased hepatic inflammatory activity and appeared to havean inhibitory overall effect on fibrosis. Thus, although IL-10 appearsto reduce inflammation and fibrosis, it has not been pursued as anantifibrotic compound because of putative detrimental virologiceffects.
Miscellaneous Anti-inflammatory DrugsA number of other anti-inflammatory approaches have gained atten-tion as therapies for fibrosis. Because TNF-a drives inflammation inmany diseases, and because TNF-a is up-regulated in liver diseases(such as alcoholic hepatitis), an anti-TNF-a compound should theoretically reduce inflammation and hence the stimulus for fibro-sis.171–174 Preliminary analyses from a study of anti-TNF-a therapysuggest an improvement in inflammation which presumably pre-cedes fibrosis in patients with alcoholic hepatitis,173 although therewas little effect of anti-TNF-a on hepatic fibrosis. Such data, in addi-tion to the favorable effects of the TNF-a inhibitor pentoxifyllineon mortality, provide the rationale for future study in patients withalcoholic hepatitis. These approaches and others that broadly inhibitinflammation must be considered cautiously because of the con-cern about disruption of the immune system, with increased risk ofinfection.
Penicillamine is a heavy metal chelating compound that has beenproposed to have anti-inflammatory and thus antifibrogeniceffects.175 However, this compound had no effect on fibrogenesis inpatients with primary biliary cirrhosis.176,177
Metrothrexate is thought to have anti-inflammatory properties,but interestingly has typically been considered to be profibrogenicin the liver for patients receiving methotrexate for treatment ofrheumatologic diseases178 (although it is noteworthy that the risk of fibrosis progression may be less prominent than typicallybelieved178,179). Metrothrexate has been studied in patients withprimary biliary cirrhosis. Although some investigators have reportedhighly favorable effects in this disease, including improvement ofthe disease and reversion of fibrosis,180 the majority of the data onmethotrexate have either been negative181,182 or show that the drug’seffects have been marginal, either alone181 or in combination withcolchicine.183 It is important to emphasize that if methotrexate isused to treat patients with primary biliary cirrhosis, this must beundertaken by an experienced hepatologist.
ANTIOXIDANT AGENTSOxidative stress is thought to play an important role in injury, stel-late cell activation, and the stimulation of extracellular matrix pro-duction, as discussed above. Thus, a wide variety of antioxidantshave received attention as potential antifibrotics.
PolyenylphosphatidylcholinePolyenylphosphatidylcholine is a mixture of polyunsaturated phos-phatidylcholines, extracted from soybeans. This compound hasantioxidant properties and oxidant stress (see above) is thought tobe important in the inflammatory and fibrogenic response to injury,particularly in alcoholic liver disease. As oxidative stress leads tolipid peroxidation, and lipid peroxidation is injurious at the level ofthe cell membrane, phosphatidylcholine has been proposed to beprotective against injury to cell membranes, resulting in reduced cellular injury and fibrogenesis.184
A VA cooperative multicenter clinical trial examined the effectof polyenylphosphatidylcholine in 789 patients with alcoholic hepatitis who had a very high daily average alcohol intake (16drinks/day).185 Subjects were randomized to either polyenylphos-phatidylcholine or placebo for 2 years. The long period of treatmentis noteworthy as it is likely that long periods of treatment will berequired to effect changes in the liver fibrosis. Many subjects sub-stantially reduced their ethanol consumption during the trial, whichprobably accounted for improvement in fibrosis in the control group,making it difficult to demonstrate an improvement in fibrosis in thepolyenylphosphatidylcholine group. Thus, overall, polyenylphos-phatidylcholine failed to lead to significant improvement in fibrosis.
SilymarinSilymarin is derived from the milk thistle Silybum marianum. Thisextract has been shown to reduce lipid peroxidation and inhibitfibrogenesis in rodent animal models,186,187 as well as in baboons.188
It has been tested in several carefully performed human clinicaltrials, although fibrosis was not used as an endpoint. The compoundhas been found to be safe, but reportedly has mixed effects.189,190
In one study examining silymarin in alcoholics189 mortality wasreduced; in addition, patients with early stages of cirrhosis alsoappeared to benefit. However, in another study in alcoholics no sur-vival benefit could be identified.190 In both of these trials, silymarinappeared to be safe. Thus, although the agent is safe and is com-monly used by patients with fibrosing liver disease, there is limitedevidence of its efficacy.
Other AntioxidantsAntioxidants such as vitamin E have been examined in animalmodels191 as well as in humans.192–195 A vitamin E precursor, D-a-tocopherol (1200 IU/day for 8 weeks), was studied in six patientswith hepatitis C virus infection who failed to respond to interferontherapy,192 and was found to inhibit stellate cell activation but didnot affect fibrosis. A randomized controlled trial examined vitaminE in patients with mild to moderate alcoholic hepatitis and foundthat vitamin E reduced serum hyaluronic acid, but did not lead toa change in type III collagen.194 Combined antioxidant therapy,including vitamin E, had no effect on outcome in patients withsevere alcoholic hepatitis, although fibrosis was not specificallyaddressed.195
Malotilate is another potential cytoprotective agent, perhapsacting via inhibition of cytochrome P450 2E1; in addition, this compound may have anti-inflammatory properties. In patients withprimary biliary cirrhosis, although it was found to diminish plasmacell and lymphocytic infiltrate and piecemeal necrosis, it had no significant effect on fibrogenesis.196
Another agent used to antagonize oxidative stress is S-adenosyl-methionine; this compound is important in the synthesis of theantioxidant glutathione. The enzyme (methionine adenosyltrans-ferase) responsible for its synthesis is reduced in the injured liver;197
thus it has been hypothesized that if S-adenosylmethionine werereplaced, then injury and fibrogenesis might be slowed. S-adenosyl-methionine has been tested in a large randomized trial in patientswith alcoholic cirrhosis.198 There was an improvement in overallmortality/need for liver transplantation in the treatment arm, espe-
101
Ch006-X2998.qxd 3/15/06 5:21 PM Page 101

Section I. Pathophysiology of the Liver
cially in patients with Child’s A/B cirrhosis, although histologicassessment of fibrosis was not specifically assessed.198
Propylthiouracil is an antithyroid drug that reacts with some ofthe oxidizing species derived from the respiratory burst and maythus be protective in alcoholic liver disease, a disease in which anincrease in hepatic oxygen consumption may predispose the liver toischemic injury. Thus, propylthiouracil has been tested in a numberof randomized clinical trials in patients with alcoholic liver disease.Unfortunately, a systematic review and meta-analysis found thatpropylthiouracil had no benefit in fibrosis, or in any other outcomemeasured.199
CYTOPROTECTIVE AGENTSUrsodeoxycholic AcidUrsodeoxycholic acid binds to hepatocyte membranes, where it pre-sumably stabilizes them and is thus cytoprotective. This cytopro-tective action in turn theoretically reduces inflammation and may inturn have a beneficial effect on fibrogenesis.200 Neither experimen-tal data nor human studies indicate a primary antifibrotic effect ofursodeoxycholic acid in the liver, but the compound has been exam-ined extensively.201–209
Ursodeoxycholic acid has been studied in patients with cysticfibrosis, primary biliary injury (primary biliary cirrhosis, primarysclerosing cholangitis and progressive familial intrahepatic cholesta-sis), and miscellaneous liver diseases. Results with ursodeoxycholicacid in these conditions have been mixed. Both symptomatic andbiochemical improvement has been observed in these diseases, inparticular the biliary diseases, but data on histologic improvement(and survival) have not been consistent. For example, in a random-ized controlled trial in patients with primary biliary cirrhosis,ursodeoxycholic acid led to reduced fibrosis in those with milddisease but had no effect on those with severe disease.202 In anotherstudy, survival was improved in patients treated with ursodeoxy-cholic acid but fibrosis was not improved.206 Further, in a histopatho-logic study of 54 patients with primary biliary cirrhosis and pairedliver biopsies, 4 years of ursodeoxycholic acid therapy was associ-ated with a significant decrease in the prevalence of florid interlob-ular bile duct lesions, lobular inflammation, and necrosis. Worseningof fibrosis was observed in 14 patients (the majority had only a one-grade progression in fibrosis score), whereas stabilization was notedin the 40 remaining patients.207 A recent combined analysis of thehistologic effect of ursodeoxycholic acid on paired liver biopsiesincluding a total of 367 patients (200 ursodeoxycholic acid and 167placebo) revealed that subpopulations of patients with initial early-stage disease may benefit from therapy.208 Results of meta-analysesexamining ursodeoxycholic acid have been mixed, and have largelyreported that ursodeoxycholic acid is not effective in primary biliarycirrhosis.205 The aggregate data suggest that ursodeoxycholic acidmay impede the progression of fibrosis in primary biliary cirrhosisvia effects on (bile duct) inflammation, particularly if given early inthe disease course. It should be emphasized that so far as we know,ursodeoxycholic acid is extremely safe. Thus, although it is alsoexpensive, the available data justify its use as an antifibrotic inpatients with primary biliary cirrhosis.
Ursodeoxycholic acid has also been studied in children with pro-gressive familial intrahepatic cholestasis,203 where it appeared to
improve fibrogenesis. Additionally, a small series indicated thatseven of 10 patients with cystic fibrosis treated with ursodeoxy-cholic acid had a reduction in liver fibrosis.204 Although these effectsare promising, it should be emphasized that the numbers of patientsstudied has been small. Finally, in a large randomized controlled trialof ursodeoxycholic acid in patients with non-alcoholic steatohepati-tis over 2 years, including 107 subjects who had paired biopsy data,there was no improvement in fibrosis.209
MISCELLANEOUSAnabolic–androgenic steroids such as oxandrolone have been exam-ined in randomized trials including patients with alcoholic liverdisease, but have not been found to have significant effects on fibro-sis (or other outcomes).210
Stellate Cell-Specific CompoundsInterferon-gA wealth of data supports the antifibrotic potential of interferon-g.The interferons consist of a family of three major isoforms, a, b andg. These isoforms are unique, not only in structure but also in theirbiologic actions. Interferons-a and -b bind to the same receptor,whereas interferon-g binds to a different receptor. Interferon-a hasmore potent antiviral effects than does interferon-g, and interferon-g has been shown to specifically inhibit extracellular matrix synthesis in isolated cells, including stellate cells.211,212 Interferon-gpotently inhibits multiple aspects of stellate cell activation,211,212 andappears to have antifibrotic effects in patients with pulmonary fibro-sis.213 Such data have generated considerable enthusiasm about theuse of interferon-g in patients with hepatic fibrosis, although thereis theoretical concern about its use because it is proinflammatory,and moreover its overexpression in the liver leads to chronic hepa-titis.214 None the less, it has now been tested in humans with fibros-ing liver disease, and appears to be safe.215 Although this pilot studyprovides a firm foundation highlighting the potential use of inter-feron-g in patients, larger studies are needed to prove a therapeuticbenefit.
COMPOUNDS THAT INHIBIT FIBROGENESISColchicineColchicine is a plant alkaloid that inhibits polymerization of micro-tubules, a process that in turn is believed to be required for colla-gen secretion. Based on this concept, colchicine has been advancedas an antifibrotic agent. A sizeable body of literature indicates thatcolchicine has antifibrotic properties in experimental animalmodels.216 This work has led to a number of human clinicaltrials.217–220 A wide variety of liver diseases has been studied, includ-ing primary biliary cirrhosis, alcoholic cirrhosis, cryptogenic cirrho-sis, and miscellaneous other liver diseases. In a double-blindrandomized controlled trial examining colchicine in primary biliarycirrhosis improvements were noted in a number of biochemicalmarkers, but the drug failed to reduce fibrosis.217 In an often-citedpopularized double-blind randomized controlled trial of colchicineversus placebo in patients with various liver diseases, colchicine ledto improved fibrosis as well as a dramatic improvement in survival.218
However, this study has been extended to clinical practice withgreat caution because of a variety of methodological concerns. First,
102
Ch006-X2998.qxd 3/15/06 5:21 PM Page 102

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
many patients were lost to follow-up, and in addition there was sub-stantial unexplained excess mortality in the control group (unrelatedto liver disease). In a recent large VA cooperative multicenter studyinvolving 549 patients comparing colchicine (0.6mg orally b.i.d.) toplacebo in patients with alcoholic liver disease, there was no appar-ent effect of active treatment on survival. Histologic data that mighthave provided information on the anti-inflammatory effects ofcolchicine were not obtained.219 A meta-analysis including 1138 sub-jects found that colchicine had no effect on hepatic fibrosis or mor-tality.220 In summary, the data surrounding colchicine suggest thatthis compound is safe but likely to be ineffective.
FUTURE ANTIFIBROTICSGiven the major effort in understanding the biology of hepatic fibro-genesis, it is not surprising that numerous pathways have been tar-geted as having therapeutic potential. Many compounds have beenstudied in experimental models and have been shown to have anti-fibrotic properties, including several with great potential in humanliver disease (Table 6-5).
Several important pathways merit discussion. One of the mostimportant examples is the TGF-b pathway, as it plays a central rolein the fibrogenic cascade. Several approaches to inhibit the actionof TGF-g have been proposed and include the use of molecules suchas decorin, the protein core component of proteoglycan, which bindsand inactivates TGF-b,221 antibodies directed against TGF-b1, andsoluble receptors which typically encode for sequences that bindactive TGF-b and prevent it from binding to its cognate receptors.The concept has been well established experimentally; indeed, theeffect of inhibition of TGF-b in animal models of liver injury andfibrogenesis has been striking.222,223 A limitation of approaches thattarget TGF-b is that the cytokine potently inhibits cellular prolifer-ation, and inhibition of its effects in vivo could predispose to malig-nant transformation.
Another critical pathway involves PDGF. PDGF is the mostpotent stellate cell mitogen known,3,224 and in addition stimulatesstellate cell migration.225 A number of approaches have been usedto inhibit the effect of PDGF. For example, kinase inhibitors thatspecifically inhibit PDGF signaling might be useful,226 as could thosewith more general effects on tyrosine kinase receptors.
Additionally, stellate cells express angiotensin and endothelinreceptors and their cognate ligands appear to be overproduced inthe liver; further, stimulation of stellate cells with their respectiveligands leads to stellate cell activation.66 Thus, inhibition of theirbinding may be clinically beneficial.
Among others agents, compounds such as pirfenidone,227 peroxi-somal proliferator-activated receptor (PPAR)-g ligands,76,228 andhalofuginone229 appear to have direct effects on stellate cells and
thus could evolve into effective antifibrotic compounds. Manyothers have been highlighted (see 5 for review).
SUMMARY AND FUTUREDIRECTIONS FOR ANTIFIBROTICTHERAPYThe explosion of information about the pathogenesis of fibro-genesis has spawned a field dedicated to antifibrotics focused on theactivation of hepatic stellate cells. Stellate cell activation is charac-terized by a number of important features, including enhancedmatrix synthesis and a prominent contractile phenotype, processesthat each contribute to the dysfunction of the liver typically foundin advanced disease. It should be emphasized that the control ofactivation is multifactorial, and thus several potential therapeuticinterventions are possible. A further critical concept is that fibrosis,in particular the ECM component of fibrosis, is dynamic, and theaccumulation of fibrosis may be inhibited. It is likely that fibrosis,including even advanced fibrosis, may be reversible under the appro-priate conditions. Currently, effective therapy for hepatic fibrogen-esis exists for several diseases in which the cause of the underlyingdisease is removed. In contrast, specific therapy directed only at thefibrotic lesion is not currently available; the most effective therapieswill most likely be directed at the stellate cell. Additionally,approaches that regulate matrix remodeling (i.e. by enhancingmatrix degradation or inhibiting factors that prevent matrix break-down) will be attractive. Thus, multiple potential targets have beenidentified, and it is highly likely that candidates will emerge. Theideal antifibrotic compound will be specific, effective, safe, and inexpensive.
REFERENCES1. Kim WR, Brown RS Jr, Terrault NA, El-Serag H. Burden of
liver disease in the United States: summary of a workshop.Hepatology 2002;36:227–242.
2. Gressner AM, Weiskirchen R, Breitkopf K, Dooley S. Roles ofTGF-beta in hepatic fibrosis. Front Biosci 2002;7:D793–807.
3. Pinzani M. PDGF and signal transduction in hepatic stellatecells. Front Biosci 2002;7:d1720–1726.
4. Friedman SL. Liver fibrosis – from bench to bedside. J Hepatol2003;38(Suppl 1):S38–53.
5. Rockey DC. Antifibrotic therapy in chronic liver disease. ClinGastroenterol Hepatol 2005;3:95–107.
6. Bataller R, Brenner DA. Liver fibrosis. J Clin Invest2005;115:209–218.
7. Fattovich G, Giustina G, Degos F, et al. Morbidity andmortality in compensated cirrhosis type C: a retrospectivefollow-up study of 384 patients. Gastroenterology1997;112:463–472.
8. El-Serag HB. Hepatocellular carcinoma and hepatitis C in theUnited States. Hepatology 2002;36(Suppl 1):S74–83.
9. Bruix J, Boix L, Sala M, Llovet JM. Focus on hepatocellularcancer. Cancer Cell 2004;5:215–219.
10. Schuppan D, Ruehl M, Somasundaram R, Hahn EG. Matrix asmodulator of stellate cell and hepatic fibrogenesis. Semin LiverDis 2001;21:351–372.
11. Jarnagin WR, Rockey DC, Koteliansky VE, et al. Expression ofvariant fibronectins in wound healing: cellular source and
103
Table 6-5. New Potential Antifibrotic Targets in Humans
Agent Comments
Anti-TGF-b Blocks stellate cell fibrogenesisAnti-PDGF Blocks stellate cell proliferationInterferon-g Inhibits multiple features of stellate cell activationPPAR ligands ? Stellate cell-specific effects
Ch006-X2998.qxd 3/15/06 5:21 PM Page 103

Section I. Pathophysiology of the Liver
biological activity of the EIIIA segment in rat hepaticfibrogenesis. J Cell Biol 1994;127:2037–2048.
12. Bedossa P, Ferlicot S, Paradis V, et al. Dystroglycan expressionin hepatic stellate cells: role in liver fibrosis. Lab Invest2002;82:1053–1061.
13. Schiano TD, Kim-Schluger L, Gondolesi G, Miller CM. Adultliving donor liver transplantation: the hepatologist’s perspective.Hepatology 2001;33:3–9.
14. Benhamou Y, Di Martino V, Bochet M, et al. Factors affectingliver fibrosis in human immunodeficiency virus- and hepatitis Cvirus-coinfected patients: impact of protease inhibitor therapy.Hepatology 2001;34:283–287.
15. Farci P, Roskams T, Chessa L, et al. Long-term benefit ofinterferon alpha therapy of chronic hepatitis D: regression ofadvanced hepatic fibrosis. Gastroenterology2004;126:1740–1749.
16. Wiesner RH, McDiarmid SV, Kamath PS, et al. MELD andPELD: application of survival models to liver allocation. LiverTranspl 2001;7:567–580.
17. Kamath PS, Wiesner RH, Malinchoc M, et al. A model topredict survival in patients with end-stage liver disease.Hepatology 2001;33:464–470.
18. Poynard T, Ratziu V, Charlotte F, et al. Rates and risk factors ofliver fibrosis progression in patients with chronic hepatitis C. J Hepatol 2001;34:730–739.
19. Powell EE, Edwards-Smith CJ, Hay JL, et al. Host geneticfactors influence disease progression in chronic hepatitis C.Hepatology 2000;31:828–833.
20. Huang H, et al. Hepatology 2004;40:230A.21. Shi Z, Wakil AE, Rockey DC. Strain-specific differences in
mouse hepatic wound healing are mediated by divergent Thelper cytokine responses. Proc Natl Acad Sci USA1997;94:10663–10668.
22. Hillebrandt S, Goos C, Matern S, Lammert F. Genome-wideanalysis of hepatic fibrosis in inbred mice identifies thesusceptibility locus Hfib1 on chromosome 15. Gastroenterology2002;123:2041–2051.
23. Monto A, Patel K, Bostrom A, et al. Risks of a range of alcoholintake on hepatitis C-related fibrosis. Hepatology 2004;39:826–834.
24. Patton HM, Patel K, Behling C, et al. The impact of steatosison disease progression and early and sustained treatmentresponse in chronic hepatitis C patients. J Hepatol2004;40:484–490.
25. Poynard T, Bedossa P, Opolon P. Natural history of liver fibrosisprogression in patients with chronic hepatitis C. TheOBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups.Lancet 1997;349:825–832.
26. de Torres M, Poynard T. Risk factors for liver fibrosisprogression in patients with chronic hepatitis C. Ann Hepatol2003;2:5–11.
27. Wright TL. Treatment of patients with hepatitis C andcirrhosis. Hepatology 2002;36(Suppl 1):S185–194.
28. Arenas JI, Vargas HE. Hepatitis C virus antiviral therapy inpatients with cirrhosis. Gastroenterol Clin North Am2004;33:549–562, ix.
29. Lindh M, Horal P, Dhillon AP, Norkrans G. Hepatitis B virusDNA levels, precore mutations, genotypes and histologicalactivity in chronic hepatitis B. J Viral Hepatol 2000;7:258–267.
30. Merican I, Guan R, Amarapuka D, et al. Chronic hepatitis Bvirus infection in Asian countries. J Gastroenterol Hepatol2000;15:1356–1361.
31. Kobayashi M, Arase Y, Ikeda K, et al. Clinical characteristics ofpatients infected with hepatitis B virus genotypes A, B, and C. J Gastroenterol 2002;37:35–39.
32. Chen CH, Chen PJ, Chu JS, et al. Fibrosing cholestatichepatitis in a hepatitis B surface antigen carrier after renaltransplantation. Gastroenterology 1994;107:1514–1518.
33. Lai CL, Chien RN, Leung NW, et al. A one-year trial oflamivudine for chronic hepatitis B. Asia Hepatitis LamivudineStudy Group [see comments]. N Engl J Med 1998;339:61–68.
34. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Adefovirdipivoxil for the treatment of hepatitis B e antigen-negativechronic hepatitis B. N Engl J Med 2003;348:800–807.
35. Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patientswith chronic hepatitis B and advanced liver disease. N Engl JMed 2004;351:1521–1531.
36. Raynard B, Balian A, Fallik D, et al. Risk factors of fibrosis inalcohol-induced liver disease. Hepatology 2002;35:635–638.
37. Falck-Ytter Y, Younossi ZM, Marchesini G, McCullough AJ.Clinical features and natural history of nonalcoholic steatosissyndromes. Semin Liver Dis 2001;21:17–26.
38. Brunt EM. Nonalcoholic steatohepatitis: definition andpathology. Semin Liver Dis 2001;21:3–16.
39. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med2002;346:1221–1231.
40. Ratziu V, Giral P, Charlotte F, et al. Liver fibrosis in overweightpatients. Gastroenterology 2000;118:1117–1123.
41. Kweon YO, Goodman ZD, Dienstag JL, et al. Decreasingfibrogenesis: an immunohistochemical study of paired liverbiopsies following lamivudine therapy for chronic hepatitis B. J Hepatol 2001;35:749–755.
42. Poynard T, McHutchison J, Manns M, et al. Impact ofpegylated interferon alfa-2b and ribavirin on liver fibrosis inpatients with chronic hepatitis C. Gastroenterology2002;122:1303–1313.
43. Hammel P, Couvelard A, O’Toole D, et al. Regression of liverfibrosis after biliary drainage in patients with chronicpancreatitis and stenosis of the common bile duct. N Engl JMed 2001;344:418–423.
44. Dufour JF, DeLellis R, Kaplan MM. Reversibility of hepaticfibrosis in autoimmune hepatitis. Ann Intern Med1997;127:981–985.
45. Iredale JP, Benyon RC, Pickering J, et al. Mechanisms ofspontaneous resolution of rat liver fibrosis. Hepatic stellate cellapoptosis and reduced hepatic expression of metalloproteinaseinhibitors. J Clin Invest 1998;102:538–549.
46. Shiratori Y, Imazeki F, Moriyama M, et al. Histologicimprovement of fibrosis in patients with hepatitis C who havesustained response to interferon therapy. Ann Intern Med2000;132:517–524.
47. Issa R, Zhou X, Constandinou CM, et al. Spontaneous recoveryfrom micronodular cirrhosis: Evidence for incompleteresolution associated with matrix cross-linking.Gastroenterology 2004;126:1795–1808.
48. Issa R, Williams E, Trim N, et al. Apoptosis of hepatic stellatecells: involvement in resolution of biliary fibrosis and regulationby soluble growth factors. Gut 2001;48:548–557.
49. Iredale JP. Stellate cell behavior during resolution of liver injury.Semin Liver Dis 2001;21:427–436.
50. Arthur MJ. Fibrogenesis II. Metalloproteinases and theirinhibitors in liver fibrosis. Am J Physiol Gastrointest LiverPhysiol 2000;279:G245–249.
51. Schaefer B, Rivas-Estilla AM, Meraz-Cruz N, et al. Reciprocalmodulation of matrix metalloproteinase-13 and type I collagengenes in rat hepatic stellate cells. Am J Pathol2003;162:1771–1780.
52. Han YP, Zhou L, Wang J, et al. Essential role of matrixmetalloproteinases in interleukin-1-induced myofibroblasticactivation of hepatic stellate cell in collagen. J Biol Chem2004;279:4820–4828.
53. Benyon D, Arthur MJP. Extracellular matrix degradation andthe role of stellate cells. Semin Liver Dis 2001;21:373–384.
54. Friedman SL. Molecular regulation of hepatic fibrosis, anintegrated cellular response to tissue injury. J Biol Chem2000;275:2247–2250.
104
Ch006-X2998.qxd 3/15/06 5:21 PM Page 104

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
54a. Friedman SL, Arthur MJD. Reversing hepatic fibrosis. Scienceand Medicine 2002;8:194–205.
55. Tsukamoto H. Redox regulation of cytokine expression inKupffer cells. Antioxid Redox Signal 2002;4:741–748.
56. Vogel W, Gish GD, Alves F, Pawson T. The discoidin domainreceptor tyrosine kinases are activated by collagen. Mol Cell1997;1:13–23.
57. Ikeda K, Wang LH, Torres R, et al. Discoidin domain receptor2 interacts with Src and Shc following its activation by type Icollagen. J Biol Chem 2002;277:19206–19212.
58. Olaso E, Ikeda K, Eng FJ, et al. DDR2 receptor promotesMMP-2-mediated proliferation and invasion by hepatic stellatecells. J Clin Invest 2001;108:1369–1378.
59. Pinzani M, Marra F. Cytokine receptors and signaling in hepaticstellate cells. Semin Liver Dis 2001;21:397–416.
60. Racine-Samson L, Rockey DC, Bissell DM. The role ofalpha1beta1 integrin in wound contraction. A quantitativeanalysis of liver myofibroblasts in vivo and in primary culture. J Biol Chem 1997;272:30911–30917.
61. Gao R, Brigstock DR. Connective tissue growth factor (CCN2)induces adhesion of rat activated hepatic stellate cells bybinding of its C-terminal domain to integrin alpha(v)beta(3)and heparan sulfate proteoglycan. J Biol Chem2004;279:8848–8855.
62. Mazzocca A, Carloni V, Sciammetta S, et al. Expression oftransmembrane 4 superfamily (TM4SF) proteins and their rolein hepatic stellate cell motility and wound healing migration. J Hepatol 2002;37:322–330.
63. Geerts A. History, heterogeneity, developmental biology, andfunctions of quiescent hepatic stellate cells. Semin Liver Dis2001;21:311–335.
64. Cassiman D, Libbrecht L, Desmet V, et al. Hepatic stellatecell/myofibroblast subpopulations in fibrotic human and ratlivers. J Hepatol 2002;36:200–209.
65. Corpechot C, Barbu V, Wendum D, et al. Hypoxia-inducedVEGF and collagen I expressions are associated withangiogenesis and fibrogenesis in experimental cirrhosis.Hepatology 2002;35:1010–1021.
66. Rockey DC. Vascular mediators in the injured liver. Hepatology2003;37:4–12.
67. Forbes SJ, Russo FP, Rey V, et al. A significant proportion ofmyofibroblasts are of bone marrow origin in human liverfibrosis. Gastroenterology 2004;126:955–963.
68. Magness ST, Bataller R, Yang L, Brenner DA. A dual reportergene transgenic mouse demonstrates heterogeneity in hepatic fibrogenic cell populations. Hepatology 2004;40:1151–1159.
69. Kalluri R, Neilson EG. Epithelial–mesenchymal transition and its implications for fibrosis. J Clin Invest 2003;112:1776–1784.
70. Tuma DJ. Role of malondialdehyde–acetaldehyde adducts inliver injury. Free Radic Biol Med 2002;32:303–308.
71. Bataller R, Schwabe RF, Choi YH, et al. NADPH oxidase signaltransduces angiotensin II in hepatic stellate cells and is criticalin hepatic fibrosis. J Clin Invest 2003;112:1383–1394.
72. Canbay A, Taimr P, Torok N, et al. Apoptotic body engulfmentby a human stellate cell line is profibrogenic. Lab Invest2003;83:655–663.
73. Canbay A, Higuchi H, Bronk SF, et al. Fas enhancesfibrogenesis in the bile duct ligated mouse: a link betweenapoptosis and fibrosis. Gastroenterology 2002;123:1323–1330.
74. Olaso E, Salado C, Egilegor E, et al. Proangiogenic role oftumor-activated hepatic stellate cells in experimental melanomametastasis. Hepatology 2003;37:674–685.
75. Mann DA, Smart DE. Transcriptional regulation of hepaticstellate cell activation. Gut 2002;50:891–896.
76. Marra F, Efsen E, Romanelli RG, et al. Ligands of peroxisomeproliferator-activated receptor gamma modulate profibrogenic
and proinflammatory actions in hepatic stellate cells.Gastroenterology 2000;119:466–478.
77. Hellemans K, Verbuyst P, Quartier E, et al. Differentialmodulation of rat hepatic stellate phenotype by natural andsynthetic retinoids. Hepatology 2004;39:97–108.
78. Paik YH, Schwabe RF, Bataller R, et al. Toll-like receptor 4mediates inflammatory signaling by bacterial lipopolysaccharidein human hepatic stellate cells. Hepatology2003;37:1043–1055.
79. Rippe RA, Schrum LW, Stefanovic B, et al. NF-kappaB inhibitsexpression of the alpha1(I) collagen gene. DNA Cell Biol1999;18:751–761.
80. Ratziu V, Lalazar A, Wong L, et al. Zf9, a Kruppel-liketranscription factor up-regulated in vivo during early hepaticfibrosis. Proc Natl Acad Sci USA 1998;95:9500–9505.
81. Kalinichenko VV, Bhattacharyya D, Zhou Y, et al. Foxf1 +/–mice exhibit defective stellate cell activation and abnormal liverregeneration following CCl4 injury. Hepatology2003;37:107–117.
82. Weiskirchen R, Moser M, Weiskirchen S, et al. LIM-domainprotein cysteine- and glycine-rich protein 2 (CRP2) is a novelmarker of hepatic stellate cells and binding partner of theprotein inhibitor of activated STAT1. Biochem J 2001;359(Pt3):485–496.
83. Rockey DC, Fouassier L, Chung JJ, et al. Cellular localizationof endothelin-1 and increased production in liver injury in therat: potential for autocrine and paracrine effects on stellatecells. Hepatology 1998;27:472–480.
84. Pinzani M, Milani S, De Franco R, et al. Endothelin 1 isoverexpressed in human cirrhotic liver and exerts multipleeffects on activated hepatic stellate cells. Gastroenterology1996;110:534–548.
85. Marra F, Grandaliano G, Valente AJ, Abboud HE. Thrombinstimulates proliferation of liver fat-storing cells and expressionof monocyte chemotactic protein-1: potential role in liverinjury. Hepatology 1995;22:780–787.
86. Rosenbaum J, Blazejewski S, Preaux AM, et al. Fibroblastgrowth factor 2 and transforming growth factor beta 1interactions in human liver myofibroblasts. Gastroenterology1995;109:1986–1996.
87. Skrtic S, Wallenius V, Ekberg S, et al. Insulin-like growthfactors stimulate expression of hepatocyte growth factor butnot transforming growth factor beta1 in cultured hepaticstellate cells. Endocrinology 1997;138:4683–4689.
88. Pinzani M, Abboud HE, Aron DC. Secretion of insulin-likegrowth factor-I and binding proteins by rat liver fat-storingcells: regulatory role of platelet-derived growth factor.Endocrinology 1990;127:2343–2349.
89. Pinzani M, Marra F, Carloni V. Signal transduction in hepaticstellate cells. Liver 1998;18:2–13.
90. Friedman SL. Cytokines and fibrogenesis. Semin Liver Dis1999;19:129–140.
91. Reinehr RM, Kubitz R, Peters-Regehr T, et al. Activation of rathepatic stellate cells in culture is associated with increasedsensitivity to endothelin 1. Hepatology 1998;28:1566–1577.
92. Schnabl B, Kweon YO, Frederick JP, et al. The role of Smad3in mediating mouse hepatic stellate cell activation. Hepatology2001;34:89–100.
93. Dooley S, Delvoux B, Lahme B, et al. Modulation oftransforming growth factor beta response and signaling duringtransdifferentiation of rat hepatic stellate cells tomyofibroblasts. Hepatology 2000;31:1094–1106.
94. Liu C, Gaca MD, Swenson ES, et al. Smads 2 and 3 aredifferentially activated by transforming growth factor-beta(TGF-beta) in quiescent and activated hepatic stellate cells.Constitutive nuclear localization of Smads in activated cells is TGF-beta-independent. J Biol Chem 2003;278:11721–11728.
105
Ch006-X2998.qxd 3/15/06 5:21 PM Page 105

Section I. Pathophysiology of the Liver
95. Wells RG. Fibrogenesis. V. TGF-beta signaling pathways. Am JPhysiol Gastrointest Liver Physiol 2000;279:G845–850.
96. Wells RG, Kruglov E, Dranoff JA. Autocrine release of TGF-beta by portal fibroblasts regulates cell growth. FEBS Lett2004;559:107–110.
97. Marra F. Chemokines in liver inflammation and fibrosis. FrontBiosci 2002;7:d1899–914.
98. Ohata M, Yamauchi M, Takeda K, et al. RAR and RXRexpression by Kupffer cells. Exp Mol Pathol 2000;68:13–20.
99. LeCouter J, Moritz DR, Li B, et al. Angiogenesis-independentendothelial protection of liver: role of VEGFR-1. Science2003;299:890–893.
100. Yoshiji H, Kuriyama S, Yoshii J, et al. Vascular endothelialgrowth factor and receptor interaction is a prerequisite formurine hepatic fibrogenesis. Gut 2003;52:1347–1354.
101. Ankoma-Sey V, Wang Y, Dai Z. Hypoxic stimulation of vascularendothelial growth factor expression in activated rat hepaticstellate cells. Hepatology 2000;31:141–148.
102. Schwabe RF, Bataller R, Brenner DA. Human hepatic stellatecells express CCR5 and RANTES to induce proliferation andmigration. Am J Physiol Gastrointest Liver Physiol2003;285:G949–958.
103. Gaca MD, Zhou X, Benyon RC. Regulation of hepatic stellatecell proliferation and collagen synthesis by proteinase-activatedreceptors. J Hepatol 2002;36:362–369.
104. Bataller R, Paik YH, Lindquist JN, et al. Hepatitis C virus coreand nonstructural proteins induce fibrogenic effects in hepaticstellate cells. Gastroenterology 2004;126:529–540.
105. Efsen E, Grappone C, DeFranco RM, et al. Up-regulatedexpression of fractalkine and its receptor CX3CR1 during liverinjury in humans. J Hepatol 2002;37:39–47.
106. Kobayashi S, Seki S, Kawada N, et al. Apoptosis of T cells inthe hepatic fibrotic tissue of the rat: a possible inducing role ofhepatic myofibroblast-like cells. Cell Tissue Res2003;311:353–364.
107. Safadi R, Ohta M, Alvarez CE, et al. Immune stimulation ofhepatic fibrogenesis by CD8 cells and attenuation by transgenicinterleukin-10 from hepatocytes. Gastroenterology 2004;127:870–882.
108. Gaca MD, Pickering JA, Arthur MJ, Benyon RC. Human andrat hepatic stellate cells produce stem cell factor: a possiblemechanism for mast cell recruitment in liver fibrosis. J Hepatol1999;30:850–858.
109. Nelson DR, Tu Z, Soldevila-Pico C, et al. Long-terminterleukin 10 therapy in chronic hepatitis C patients has aproviral and anti-inflammatory effect. Hepatology2003;38:859–868.
110. Mazzocca A, Sciammetta SC, Carloni V, et al. Binding ofhepatitis C virus envelope protein E2 to CD81 up-regulatesmatrix metalloproteinase-2 in human hepatic stellate cells. JBiol Chem 2005;280:11329–11339.
111. Bonacchi A, Petrai I, Defranco RM, et al. The chemokineCCL21 modulates lymphocyte recruitment and fibrosis inchronic hepatitis C. Gastroenterology 2003;125:1060–1076.
112. Pohlmann S, Zhang J, Baribaud F, et al. Hepatitis C virusglycoproteins interact with DC-SIGN and DC-SIGNR. J Virol2003;77:4070–4080.
113. Ikejima K, Takei Y, Honda H, et al. Leptin receptor-mediatedsignaling regulates hepatic fibrogenesis and remodeling ofextracellular matrix in the rat. Gastroenterology2002;122:1399–1410.
114. Leclercq IA, Farrell GC, Schriemer R, Robertson GR. Leptin isessential for the hepatic fibrogenic response to chronic liverinjury. J Hepatol 2002;37:206–213.
115. Saxena NK, Saliba G, Floyd JJ, Anania FA. Leptin inducesincreased alpha2(I) collagen gene expression in cultured rathepatic stellate cells. J Cell Biochem 2003;89:311–320.
116. Kamada Y, Tamura S, Kiso S, et al. Enhanced carbontetrachloride-induced liver fibrosis in mice lacking adiponectin.Gastroenterology 2003;125:1796–1807.
117. Canbay A, Friedman S, Gores GJ. Apoptosis: the nexus of liverinjury and fibrosis. Hepatology 2004;39:273–278.
118. Taimr P, Higuchi H, Kocova E, et al. Activated stellate cellsexpress the TRAIL receptor-2/death receptor-5 and undergoTRAIL-mediated apoptosis. Hepatology 2003;37:87–95.
119. Trim N, Morgan S, Evans M, et al. Hepatic stellate cellsexpress the low affinity nerve growth factor receptor p75 andundergo apoptosis in response to nerve growth factorstimulation. Am J Pathol 2000;156:1235–1243.
120. Lang A, Schoonhoven R, Tuvia S, et al. Nuclear factor kappaBin proliferation, activation, and apoptosis in rat hepatic stellatecells. J Hepatol 2000;33:49–58.
121. Reif S, Lang A, Lindquist JN, et al. The role of focal adhesionkinase-phosphatidylinositol 3-kinase-akt signaling in hepaticstellate cell proliferation and type I collagen expression. J BiolChem 2003;278:8083–8090.
122. Preaux AM, D’Ortho MP, Bralet MP, et al. Apoptosis of humanhepatic myofibroblasts promotes activation of matrixmetalloproteinase-2. Hepatology 2002;36:615–622.
123. Li L, Tao J, Davaille J, et al. 15-deoxy-delta 12,14-prostaglandin J2 induces apoptosis of human hepaticmyofibroblasts. A pathway involving oxidative stressindependently of peroxisome-proliferator-activated receptors. J Biol Chem 2001;276:38152–38158.
124. Yoshiji H, Kuriyama S, Yoshii J, et al. Tissue inhibitor ofmetalloproteinases-1 attenuates spontaneous liver fibrosisresolution in the transgenic mouse. Hepatology2002;36:850–860.
125. Wright MC, Issa R, Smart DE, et al. Gliotoxin stimulates theapoptosis of human and rat hepatic stellate cells and enhancesthe resolution of liver fibrosis in rats. Gastroenterology2001;121:685–698.
126. Sohara N, Znoyko I, Levy MT, et al. Reversal of activation ofhuman myofibroblast-like cells by culture on a basementmembrane-like substrate. J Hepatol 2002;37:214–221.
127. Lin SM, Sheen IS, Chien RN, et al. Long-term beneficial effectof interferon therapy in patients with chronic hepatitis B virusinfection. Hepatology 1999;29:971–975.
128. Wanless IR, Nakashima E, Sherman M. Regression of humancirrhosis. Morphologic features and the genesis of incompleteseptal cirrhosis. Arch Pathol Lab Med 2000;124:1599–1607.
129. Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil forthe treatment of hepatitis B e antigen-positive chronic hepatitisB. N Engl J Med 2003;348:808–816.
130. Chalasani N, Imperiale TF, Ismail A, et al. Predictors of largeesophageal varices in patients with cirrhosis. Am JGastroenterol 1999;94:3285–3291.
131. Zaman A, Becker T, Lapidus J, Benner K. Risk factors for the presence of varices in cirrhotic patients without a history of variceal hemorrhage. Arch Intern Med 2001;161:2564–2570.
132. Giannini E, Risso D, Botta F, et al. Validity and clinical utilityof the aspartate aminotransferase–alanine aminotransferase ratioin assessing disease severity and prognosis in patients withhepatitis C virus-related chronic liver disease. Arch Intern Med2003;163:218–224.
133. Sheth SG, Flamm SL, Gordon FD, Chopra S. AST/ALT ratiopredicts cirrhosis in patients with chronic hepatitis C virusinfection. Am J Gastroenterol 1998;93:44–48.
134. Giannini E, Testa R. Noninvasive diagnosis of fibrosis: the truthis rarely pure and never simple. Hepatology2003;38:1312–1313; author reply 3.
135. Forns X, Ampurdanes S, Llovet JM, et al. Identification ofchronic hepatitis C patients without hepatic fibrosis by a simplepredictive model. Hepatology 2002;36:986–992.
106
Ch006-X2998.qxd 3/15/06 5:21 PM Page 106

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
136. Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasiveindex can predict both significant fibrosis and cirrhosis inpatients with chronic hepatitis C. Hepatology 2003;38:518–526.
137. Poynard T, Aubert A, Bedossa P, et al. A simple biological indexfor detection of alcoholic liver disease in drinkers.Gastroenterology 1991;100:1397–1402.
138. Naveau S, Poynard T, Benattar C, Bedossa P, Chaput JC.Alpha-2-macroglobulin and hepatic fibrosis. Diagnostic interest.Dig Dis Sci 1994;39:2426–2432.
139. Imbert-Bismut F, Ratziu V, Pieroni L, et al. Biochemicalmarkers of liver fibrosis in patients with hepatitis C virusinfection: a prospective study. Lancet 2001;357:1069–1075.
140. Poynard T, Imbert-Bismut F, Munteanu M, et al. Overview ofthe diagnostic value of biochemical markers of liver fibrosis(FibroTest, HCV FibroSure) and necrosis (ActiTest) in patientswith chronic hepatitis C. Comp Hepatol 2004;3:8.
141. Myers RP, Tainturier MH, Ratziu V, et al. Prediction of liverhistological lesions with biochemical markers in patients withchronic hepatitis B. J Hepatol 2003;39:222–230.
142. Naveau S, Raynard B, Ratziu V, et al. Biomarkers for theprediction of liver fibrosis in patients with chronic alcoholicliver disease. Clin Gastroenterol Hepatol 2005;3:167–174.
143. Colombo M, Annoni G, Donato MF, et al. Serum type IIIprocollagen peptide in alcoholic liver disease and idiopathichemochromatosis: its relationship to hepatic fibrosis, activity ofthe disease and iron overload. Hepatology 1985;5:475–479.
144. Tsutsumi M, Takase S, Urashima S, et al. Serum markers forhepatic fibrosis in alcoholic liver disease: which is the bestmarker, type III procollagen, type IV collagen, laminin, tissueinhibitor of metalloproteinase, or prolyl hydroxylase? AlcoholClin Exp Res 1996;20:1512–1517.
145. Afdhal NH, Nunes D. Evaluation of liver fibrosis: a concisereview. Am J Gastroenterol 2004;99:1160–1174.
146. Patel K, Gordon SC, Jacobson I, et al. Evaluation of a panel ofnon-invasive serum markers to differentiate mild frommoderate-to-advanced liver fibrosis in chronic hepatitis Cpatients. J Hepatol 2004;41:935–942.
147. Rosenberg WM, Voelker M, Thiel R, et al. Serum markersdetect the presence of liver fibrosis: a cohort study.Gastroenterology 2004;127:1704–1713.
147a. Sud A, Hui JM, Farrell GC, et al. Improved prediction offibrosis in chronic hepatitis C using measures of insulinresistance in a probability index. Hepatology2004;39:1239–1247.
148. Poon TC, Hui AY, Chan HL, et al. Prediction of liver fibrosisand cirrhosis in chronic hepatitis B infection by serumproteomic fingerprinting: a pilot study. Clin Chem2005;51:328–335.
149. Bora R, Ratziu V, Bedossa P, et al. Diagnostic value ofbiochemical markers, fibrotest–actitest–HCV–fibrosurecompared with serum protein profiling by seldi-TOF, for thediagnosis of bridging fibrosis in patients with chronic hepatitisC. Hepatology 2004;40:517A.
150. Dev A, White I, Symonds W, et al. Serum proteomic analysisin hepatitis C patients with and without fibrosis. J Hepatol2005;42(suppl 2):117A.
151. Callewaert N, Van Vlierberghe H, Van Hecke A, et al.Noninvasive diagnosis of liver cirrhosis using DNA sequencer-based total serum protein glycomics. Nature Med2004;10:429–434.
152. Wells RG. The role of matrix stiffness in hepatic stellate cellactivation and liver fibrosis. J Clin Gastroenterol2005;39:S158–161.
153. Ziol M, Handra-Luca A, Kettaneh A, et al. Noninvasiveassessment of liver fibrosis by measurement of stiffness inpatients with chronic hepatitis C. Hepatology 2005;41:48–54.
154. Castera L, Vergniol J, Foucher J, et al. Prospective comparisonof transient elastography, Fibrotest, APRI, and liver biopsy forthe assessment of fibrosis in chronic hepatitis C.Gastroenterology 2005;128:343–350.
155. Beljaars L, Meijer DK, Poelstra K. Targeting hepatic stellatecells for cell-specific treatment of liver fibrosis. Front Biosci2002;7:e214–222.
156. Adler M, Verset D, Bouhdid H, et al. Prognostic evaluation ofpatients with parenchymal cirrhosis. Proposal of a new simplescore. J Hepatol 1997;26:642–649.
157. Giannini EG, Testa R. 13C-breath tests and liver fibrosis. EurRev Med Pharmacol Sci 2004;8:51–54.
158. Giannini EG, Fasoli A, Borro P, et al. 13C-galactose breath testand 13C-aminopyrine breath test for the study of liver functionin chronic liver disease. Clin Gastroenterol Hepatol 2005;3:279–285.
159. Testa R, Caglieris S, Risso D, et al. Monoethylglycinexylidideformation measurement as a hepatic function test to assessseverity of chronic liver disease. Am J Gastroenterol1997;92:2268–2273.
160. Regev A, Berho M, Jeffers LJ, et al. Sampling error andintraobserver variation in liver biopsy in patients with chronicHCV infection. Am J Gastroenterol 2002;97:2614–2618.
161. Ratziu V, Charlotte F, Heurtier A, et al. Sampling variability ofliver biopsy in nonalcoholic fatty liver disease. Gastroenterology2005;128:1898–1906.
162. Colloredo G, Guido M, Sonzogni A, Leandro G. Impact ofliver biopsy size on histological evaluation of chronic viralhepatitis: the smaller the sample, the milder the disease. JHepatol 2003;39:239–244.
163. Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003;38:1449–1457.
164. Rousselet MC, Michalak S, Dupre F, et al. Sources ofvariability in histological scoring of chronic viral hepatitis.Hepatology 2005;41:257–264.
164a. Wanless IR, Nakashima E, Sherman M. Regression of humancirrhosis. Morphologic features and the genesis of incompleteseptal cirrhosis. Arch Pathol Lab Med 2000;124:1599–1607.
165. Powell LW, Kerr JF. Reversal of ‘cirrhosis’ in idiopathichaemochromatosis following long-term intensive venesectiontherapy. Australas Ann Med 1970;19:54–57.
166. Blumberg RS, Chopra S, Ibrahim R, et al. Primaryhepatocellular carcinoma in idiopathic hemochromatosis afterreversal of cirrhosis. Gastroenterology 1988;95: 1399–1402.
167. Neuschwander-Tetri BA, Brunt EM, Wehmeier KR, et al.Improved nonalcoholic steatohepatitis after 48 weeks oftreatment with the PPAR-gamma ligand rosiglitazone.Hepatology 2003;38:1008–1017.
168. Ramond MJ, Poynard T, Rueff B, et al. A randomized trial ofprednisolone in patients with severe alcoholic hepatitis. N EnglJ Med 1992;326:507–512.
169. Spahr L, Rubbia-Brandt L, Pugin J, et al. Rapid changes inalcoholic hepatitis histology under steroids: correlation withsoluble intercellular adhesion molecule-1 in hepatic venousblood. J Hepatol 2001;35:582–589.
170. Thompson K, Maltby J, Fallowfield J, et al. Interleukin-10expression and function in experimental murine liverinflammation and fibrosis [see comments]. Hepatology1998;28:1597–1606.
171. Akriviadis E, Botla R, Briggs W, et al. Pentoxifylline improvesshort-term survival in severe acute alcoholic hepatitis: a double-blind, placebo-controlled trial. Gastroenterology2000;119:1637–1648.
172. Spahr L, Rubbia-Brandt L, Frossard JL, et al. Combination ofsteroids with infliximab or placebo in severe alcoholic hepatitis:a randomized controlled pilot study. J Hepatol2002;37:448–455.
107
Ch006-X2998.qxd 3/15/06 5:21 PM Page 107

Section I. Pathophysiology of the Liver
173. Tilg H, Jalan R, Kaser A, et al. Anti-tumor necrosis factor-alphamonoclonal antibody therapy in severe alcoholic hepatitis. JHepatol 2003;38:419–425.
174. Menon KV, Stadheim L, Kamath PS, et al. A pilot study of thesafety and tolerability of etanercept in patients with alcoholichepatitis. Am J Gastroenterol 2004;99:255–260.
175. Schaff Z, Lapis K, Szende B, et al. The effect of D-penicillamine on CCl4-induced experimental liver cirrhosis.Exp Pathol 1991;43:111–120.
176. Bodenheimer HC Jr, Schaffner F, Sternlieb I, et al. Aprospective clinical trial of D-penicillamine in the treatment ofprimary biliary cirrhosis. Hepatology 1985;5:1139–1142.
177. Dickson ER, Fleming TR, Wiesner RH, et al. Trial ofpenicillamine in advanced primary biliary cirrhosis. N Engl JMed 1985;312:1011–1015.
178. Aithal GP, Haugk B, Das S, et al. Monitoring methotrexate-induced hepatic fibrosis in patients with psoriasis: are serialliver biopsies justified? Aliment Pharmacol Ther2004;19:391–399.
179. Te HS, Schiano TD, Kuan SF, et al. Hepatic effects of long-term methotrexate use in the treatment of inflammatory boweldisease. Am J Gastroenterol 2000;95:3150–3156.
180. Kaplan MM, DeLellis RA, Wolfe HJ. Sustained biochemical and histologic remission of primary biliary cirrhosis in response to medical treatment. Ann Intern Med 1997;126:682–688.
181. Hendrickse MT, Rigney E, Giaffer MH, et al. Low-dosemethotrexate is ineffective in primary biliary cirrhosis: long-term results of a placebo-controlled trial [see comments].Gastroenterology 1999;117:400–407.
182. Bach N, Bodian C, Bodenheimer H, et al. Methotrexatetherapy for primary biliary cirrhosis. Am J Gastroenterol2003;98:187–193.
183. Kaplan MM, Cheng S, Price LL, Bonis PA. A randomizedcontrolled trial of colchicine plus ursodiol versus methotrexateplus ursodiol in primary biliary cirrhosis: ten-year results.Hepatology 2004;39:915–923.
184. Aleynik SI, Leo MA, Ma X, et al. Polyenylphosphatidylcholineprevents carbon tetrachloride-induced lipid peroxidation whileit attenuates liver fibrosis. J Hepatol 1997;27:554–561.
185. Lieber CS, Weiss DG, Groszmann R, et al. II. Veterans AffairsCooperative Study of Polyenylphosphatidylcholine in AlcoholicLiver Disease. Alcohol Clin Exp Res 2003;27:1765–1772.
186. Boigk G, Stroedter L, Herbst H, et al. Silymarin retardscollagen accumulation in early and advanced biliary fibrosissecondary to complete bile duct obliteration in rats. Hepatology1997;26:643–649.
187. Jia JD, Bauer M, Cho JJ, et al. Antifibrotic effect of silymarinin rat secondary biliary fibrosis is mediated by downregulationof procollagen alpha1(I) and TIMP-1. J Hepatol2001;35:392–398.
188. Lieber CS, Leo MA, Cao Q, et al. Silymarin retards theprogression of alcohol-induced hepatic fibrosis in baboons. JClin Gastroenterol 2003;37:336–339.
189. Ferenci P, Dragosics B, Dittrich H, et al. Randomizedcontrolled trial of silymarin treatment in patients with cirrhosisof the liver. J Hepatol 1989;9:105–113.
190. Pares A, Planas R, Torres M, et al. Effects of silymarin inalcoholic patients with cirrhosis of the liver: results of acontrolled, double-blind, randomized and multicenter trial [seecomments]. J Hepatol 1998;28:615–621.
191. Brown KE, Poulos JE, Li L, et al. Effect of vitamin Esupplementation on hepatic fibrogenesis in chronic dietary ironoverload. Am J Physiol 1997;272:G116–123.
192. Houglum K, Venkataramani A, Lyche K, Chojkier M. A pilotstudy of the effects of d-alpha-tocopherol on hepatic stellatecell activation in chronic hepatitis C. Gastroenterology1997;113:1069–1073.
193. Hasegawa T, Yoneda M, Nakamura K, et al. Plasmatransforming growth factor-beta1 level and efficacy of alpha-tocopherol in patients with non-alcoholic steatohepatitis: a pilotstudy. Aliment Pharmacol Ther 2001;15:1667–1672.
194. Mezey E, Potter J, Rennie-Tankersley L, et al. A randomizedplacebo controlled trial of vitamin E in alcoholic hepatitis.Hepatology 2003;38:264A.
195. Stewart S, Prince M, Bassendine M, et al. A trial of antioxidanttherapy alone or with corticosteroids in acute alcoholichepatitis. J Hepatol 2002;36(S):16.
196. Anon. The results of a randomized double blind controlled trialevaluating malotilate in primary biliary cirrhosis. A Europeanmulticentre study group. J Hepatol 1993;17:227–235.
197. Lu SC, Tsukamoto H, Mato JM. Role of abnormal methioninemetabolism in alcoholic liver injury. Alcohol 2002;27:155–162.
198. Mato JM, Camara J, Fernandez de Paz J, et al. S-adenosylmethionine in alcoholic liver cirrhosis: a randomized,placebo-controlled, double-blind, multicenter clinical trial. J Hepatol 1999;30:1081–1089.
199. Rambaldi A, Gluud C. Meta-analysis of propylthiouracil foralcoholic liver disease – a Cochrane Hepato-Biliary GroupReview. Liver 2001;21:398–404.
200. Nava-Ocampo AA, Suster S, Muriel P. Effect of colchiceine andursodeoxycholic acid on hepatocyte and erythrocytemembranes and liver histology in experimentally inducedcarbon tetrachloride cirrhosis in rats. Eur J Clin Invest1997;27:77–84.
201. Stiehl A. Ursodeoxycholic acid in the treatment of primarysclerosing cholangitis. Ann Med 1994;26:345–349.
202. Combes B, Carithers RL Jr, Maddrey WC, et al. A randomized,double-blind, placebo-controlled trial of ursodeoxycholic acid inprimary biliary cirrhosis. Hepatology 1995;22:759–766.
203. Jacquemin E, Hermans D, Myara A, et al. Ursodeoxycholicacid therapy in pediatric patients with progressive familialintrahepatic cholestasis. Hepatology 1997;25:519–523.
204. Lindblad A, Glaumann H, Strandvik B. A two-year prospectivestudy of the effect of ursodeoxycholic acid on urinary bile acidexcretion and liver morphology in cystic fibrosis-associated liverdisease. Hepatology 1998;27:166–174.
205. Goulis J, Leandro G, Burroughs AK. Randomised controlledtrials of ursodeoxycholic-acid therapy for primary biliarycirrhosis: a meta-analysis. Lancet 1999;354:1053–1060.
206. Poupon RE, Bonnand AM, Chretien Y, Poupon R. Ten-yearsurvival in ursodeoxycholic acid-treated patients with primarybiliary cirrhosis. The UDCA-PBC Study Group. Hepatology1999;29:1668–1671.
207. Degott C, Zafrani ES, Callard P, et al. Histopathological studyof primary biliary cirrhosis and the effect of ursodeoxycholicacid treatment on histology progression. Hepatology1999;29:1007–1012.
208. Poupon RE, Lindor KD, Pares A, et al. Combined analysis ofthe effect of treatment with ursodeoxycholic acid on histologicprogression in primary biliary cirrhosis. J Hepatol2003;39:12–16.
209. Lindor KD, Kowdley KV, Heathcote EJ, et al. Ursodeoxycholicacid for treatment of nonalcoholic steatohepatitis: results of arandomized trial. Hepatology 2004;39:770–778.
210. Rambaldi A, Iaquinto G, Gluud C. Anabolic–androgenicsteroids for alcoholic liver disease: a Cochrane review. Am JGastroenterol 2002;97:1674–1681.
211. Rockey DC, Maher JJ, Jarnagin WR, et al. Inhibition of rathepatic lipocyte activation in culture by interferon-gamma.Hepatology 1992;16:776–784.
212. Rockey DC, Chung JJ. Interferon gamma inhibits lipocyteactivation and extracellular matrix mRNA expression duringexperimental liver injury: implications for treatment of hepaticfibrosis. J Invest Med 1994;42:660–670.
108
Ch006-X2998.qxd 3/15/06 5:21 PM Page 108

Chapter 6
HEPATIC FIBROSIS AND CIRRHOSIS
213. Ziesche R, Hofbauer E, Wittman K, et al. A preliminary studyof long-term treatment with interferon gamma-1b and low-doseprednisolone in patients with idiopathic pulmonary fibrosis. N Engl J Med 1999;341:1264–1269.
214. Toyonaga T, Hino O, Sugai S, et al. Chronic active hepatitis in transgenic mice expressing interferon-gamma in the liver.Proc Natl Acad Sci USA 1994;91:614–618.
215. Muir AJ, Sylvestre PB, Rockey DC. Interferon gamma-1b forthe treatment of chronic hepatitis C infection. J Viral Hepatitis2006; in press.
216. Rodriguez L, Cerbon-Ambriz J, Munoz ML. Effects ofcolchicine and colchiceine in a biochemical model of liverinjury and fibrosis. Arch Med Res 1998;29:109–116.
217. Kaplan MM, Alling DW, Zimmerman HJ, et al. A prospectivetrial of colchicine for primary biliary cirrhosis. N Engl J Med1986;315:1448–1454.
218. Kershenobich D, Vargas F, Garcia-Tsao G, et al. Colchicine inthe treatment of cirrhosis of the liver. N Engl J Med1988;318:1709–1713.
219. Morgan TR, Nemchausky B, Schiff ER, et al. Colchicine doesnot prolong life in patients with advanced alcoholic cirrhosis:results of a prospective, randomized, placebo-controlled trial.Gastroenterology 2002;122:641A.
220. Rambaldi A, Gluud C. Colchicine for alcoholic and non-alcoholic liver fibrosis or cirrhosis. Liver 2001;21:129–136.
221. Isaka Y, Brees DK, Ikegaya K, et al. Gene therapy by skeletalmuscle expression of decorin prevents fibrotic disease in ratkidney. Nature Med 1996;2:418–423.
222. George J, Roulot D, Koteliansky VE, Bissell DM. In vivoinhibition of rat stellate cell activation by soluble TGF beta
type II receptor: a potential new therapy for hepatic fibrosis.Proc Natl Acad Sci USA 1999;96:12719–12724.
223. Yata Y, Gotwals P, Koteliansky V, Rockey DC. Dose-dependentinhibition of hepatic fibrosis in mice by a TGF-beta solublereceptor: implications for antifibrotic therapy. Hepatology2002;35:1022–1030.
224. Pinzani M, Milani S, Herbst H, et al. Expression of platelet-derived growth factor and its receptors in normal human liverand during active hepatic fibrogenesis. Am J Pathol1996;148:785–800.
225. Ikeda K, Wakahara T, Wang YQ, et al. In vitro migratorypotential of rat quiescent hepatic stellate cells and itsaugmentation by cell activation. Hepatology1999;29:1760–1767.
226. Kinnman N, Francoz C, Barbu V, et al. The myofibroblasticconversion of peribiliary fibrogenic cells distinct from hepaticstellate cells is stimulated by platelet-derived growth factorduring liver fibrogenesis. Lab Invest 2003;83:163–173.
227. Di Sario A, Bendia E, Svegliati Baroni G, et al. Effect ofpirfenidone on rat hepatic stellate cell proliferation and collagenproduction. J Hepatol 2002;37:584–591.
228. Miyahara T, Schrum L, Rippe R, et al. Peroxisome proliferator-activated receptors and hepatic stellate cell activation. J BiolChem 2000;275:35715–35722.
229. Bruck R, Genina O, Aeed H, et al. Halofuginone to preventand treat thioacetamide-induced liver fibrosis in rats.Hepatology 2001;33:379–386.
109
Ch006-X2998.qxd 3/15/06 5:21 PM Page 109

Ch006-X2998.qxd 3/15/06 5:21 PM Page 110